1. Disease Information
1.1 What is the disease? (concise overview)
Perivascular epithelioid cell tumors (PEComas) are rare mesenchymal neoplasms composed of distinctive perivascular epithelioid cells with characteristic dual immunophenotype (melanocytic and smooth-muscle markers) and a spectrum of behavior from benign to malignant. (testa2023systemictreatmentsand pages 1-2, amante2024hepaticperivascularepithelioid pages 1-2)
A commonly cited WHO-style definition (as quoted in a 2024 clinicopathology editorial) is: “a mesenchymal tumor which shows a local association with vessel walls and usually expresses melanocyte and smooth muscle markers.” (amante2024hepaticperivascularepithelioid pages 1-2)
1.2 Key identifiers (OMIM, Orphanet, ICD-10/11, MeSH, MONDO)
- OMIM/Orphanet/ICD-10/ICD-11/MeSH/MONDO codes: Not reliably extractable using the available tools from the retrieved full-text corpus; therefore not populated here and should be filled from the relevant ontology portals directly.
1.3 Synonyms / alternative names
Commonly used names in the clinical and pathology literature include: - PEComa - Perivascular epithelioid cell tumor - Perivascular epithelioid cell neoplasm - PEComa-NOS (not otherwise specified)
The PEComa “family” includes related entities often discussed together, such as angiomyolipoma (AML), lymphangioleiomyomatosis (LAM), and pulmonary clear cell “sugar” tumor. (amante2024hepaticperivascularepithelioid pages 1-2, ji2024hepaticperivascularepithelioid pages 1-2)
1.4 Evidence source type
The information summarized here is derived from: - Aggregated disease-level resources (systematic reviews, narrative reviews, WHO-referenced definitions). (amante2024hepaticperivascularepithelioid pages 1-2, dong2024comprehensiveinsightsinto pages 1-2, levin2024gynecologicperivascularepithelioid pages 1-3) - Human clinical evidence (prospective phase II trial; retrospective cohort/series). (wagner2021nabsirolimusforpatients pages 1-2, ji2024hepaticperivascularepithelioid pages 1-2, testa2023systemictreatmentsand pages 1-2)
2. Etiology
2.1 Disease causal factors
PEComas are primarily driven by molecular alterations affecting the mTOR pathway, most classically through loss-of-function of TSC1 or TSC2, and by a biologically distinct subset with TFE3 gene fusions. (wagner2021nabsirolimusforpatients pages 1-2, nikolova2026pecomasrevisitedmtordriven pages 2-4, dong2024comprehensiveinsightsinto pages 1-2)
Abstract-supported mechanistic statement (direct quote): a 2025 case report reviewing core biology states PEComas are “molecularly characterized by TSC2 inactivation driving mammalian target of rapamycin (mTOR) pathway activation.” (nikolova2026pecomasrevisitedmtordriven pages 1-2)
2.2 Risk factors
Genetic risk factors / predisposition: - Association with tuberous sclerosis complex (TSC) is a recognized context for PEComa-family tumors, reflecting germline TSC1/TSC2 pathway dysfunction; however, most PEComa patients do not have clinical TSC in summarized reviews. (dong2024comprehensiveinsightsinto pages 1-2)
Demographic factors: - Female sex is a consistent epidemiologic feature across anatomic sites. (wagner2021nabsirolimusforpatients pages 1-2, dong2024comprehensiveinsightsinto pages 1-2)
Environmental/infectious risk factors: - No specific environmental or infectious causal factors were identified in the retrieved evidence.
2.3 Protective factors
No validated protective genetic or environmental factors were identified in the retrieved evidence.
2.4 Gene–environment interactions
No gene–environment interaction evidence was identified in the retrieved evidence.
3. Phenotypes
3.1 Core clinical phenotype (typical presentation)
Phenotype depends strongly on organ site; across sites, PEComas often present as an incidental mass lesion or with nonspecific symptoms. In a 2024 hepatic PEComa cohort (n=36), 72.2% (26/36) were diagnosed incidentally with non-specific symptoms. (ji2024hepaticperivascularepithelioid pages 1-2)
3.2 Histopathology phenotype (defining)
Direct quote: “The diagnosis of a PEComa is based on its pathological features” with characteristic epithelioid forms and perivascular association. (amante2024hepaticperivascularepithelioid pages 1-2)
Key histologic patterns include epithelioid to spindle cells with clear to eosinophilic cytoplasm, sometimes arranged around thick-walled vessels. (amante2024hepaticperivascularepithelioid pages 1-2, dong2024comprehensiveinsightsinto pages 1-2)
3.3 Immunophenotype phenotype (diagnostic marker expression)
Common IHC features: - Melanocytic markers: HMB45, Melan-A, often MiTF (variable by site). (amante2024hepaticperivascularepithelioid pages 1-2, ji2024hepaticperivascularepithelioid pages 1-2) - Myoid markers: SMA, ± desmin, caldesmon. (amante2024hepaticperivascularepithelioid pages 1-2, ji2024hepaticperivascularepithelioid pages 1-2)
Example quantitative IHC data from hepatic PEComa (2024, n=36): HMB-45 97.2% (35/36), Melan-A 97.1% (34/35), SMA 88.5% (23/26), CD34 86.7% (26/30). (ji2024hepaticperivascularepithelioid pages 1-2)
3.4 Suggested HPO terms (examples; site-dependent)
Because PEComa is a tumor entity spanning sites, HPO terms are best captured at the level of mass lesions and site-specific symptoms. Suggested high-level HPO terms: - Neoplasm (HP:0002664) - Abdominal mass (HP:0001541) (for retroperitoneal/hepatic/pelvic presentations) - Abnormality of the uterus (HP:0000130) (for uterine PEComa) - Pulmonary nodules (HP:0025179) / Metastatic neoplasm (HP:0033109) (when metastatic)
Frequency and severity are highly site- and subtype-dependent; robust cross-site phenotype frequencies were not available in the retrieved texts.
3.5 Quality of life impact
No disease-specific QoL instrument outcomes (e.g., EQ-5D/SF-36) were identified in the retrieved evidence.
4. Genetic / Molecular Information
4.1 Causal genes and major molecular subtypes
Two clinically meaningful molecular groupings recur in contemporary reviews and clinical trial biomarker analyses:
1) mTOR-pathway–altered PEComa - Typically via TSC1/TSC2 inactivation and sometimes MTOR mutations, producing constitutive mTORC1 signaling. (wagner2021nabsirolimusforpatients pages 1-2, dong2024comprehensiveinsightsinto pages 1-2) - A 2024 renal-focused review summarizes that “mutations in TSC1/TSC2 disrupt the TSC, leading to unchecked cell proliferation due to deregulation of the mTOR pathway.” (dong2024comprehensiveinsightsinto pages 1-2) - The same review reports approximate alteration frequencies: “close to 70% show TSC2 mutations and 20% exhibit TSC1 mutations.” (dong2024comprehensiveinsightsinto pages 1-2)
2) TFE3-rearranged PEComa - Defined by TFE3 gene fusions and strong TFE3 expression; may show distinct clinicopathologic features and potentially different therapy sensitivity. (nikolova2026pecomasrevisitedmtordriven pages 2-4, amante2024hepaticperivascularepithelioid pages 1-2)
Additional genes mentioned as potentially involved (context-dependent, not necessarily causal across all PEComa): TP53, and rare mentions of FLCN truncating mutations in WHO-referenced discussion. (amante2024hepaticperivascularepithelioid pages 1-2, dong2024comprehensiveinsightsinto pages 1-2)
4.2 Pathogenic variants and origin (somatic vs germline)
The dominant actionable alterations described in the retrieved PEComa evidence are somatic TSC1/TSC2 alterations in malignant PEComa cohorts and trials (tumor profiling), with germline TSC1/TSC2 variants relevant in the context of tuberous sclerosis complex. (wagner2021nabsirolimusforpatients pages 1-2, dong2024comprehensiveinsightsinto pages 1-2)
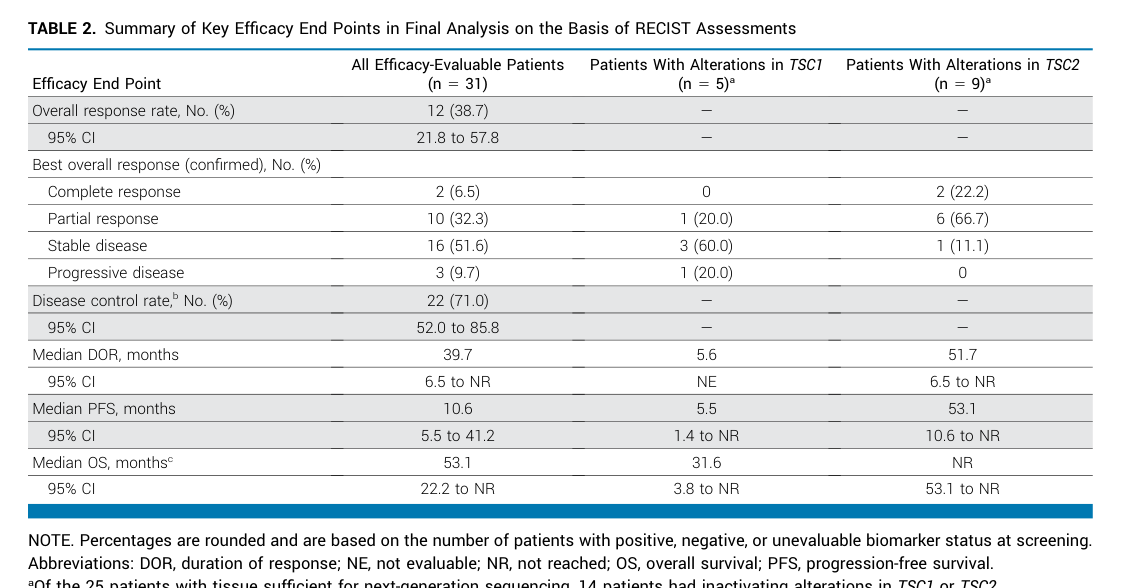
Example trial biomarker result: in AMPECT tumor mutation profiling, 8/9 (89%) patients with a TSC2 mutation achieved a confirmed response to nab-sirolimus vs 2/16 (13%) without TSC2 mutation. (wagner2021nabsirolimusforpatients pages 1-2)
Population allele frequencies and ClinVar/ACMG classifications were not available in the retrieved evidence.
4.3 Modifier genes / epigenetics / chromosomal abnormalities
No validated modifier genes or epigenetic signatures were identified in the retrieved evidence. TFE3 rearrangements are the primary structural alteration discussed. (nikolova2026pecomasrevisitedmtordriven pages 2-4)
5. Environmental Information
No specific toxins, lifestyle, or infectious triggers were identified in the retrieved evidence as contributing environmental factors for PEComa.
6. Mechanism / Pathophysiology
6.1 Core pathways
mTORC1 activation via TSC1/TSC2 loss is the central mechanistic axis for a major PEComa subset. - In malignant PEComa, the AMPECT trial background states PEComas commonly harbor TSC1/TSC2 loss-of-function and show evidence of mTORC1 activation, including phosphorylation of p70S6K and ribosomal protein S6 by IHC. (wagner2021nabsirolimusforpatients pages 1-2)
Causal chain (mTOR-driven subtype): 1. TSC1/TSC2 inactivation → disruption of hamartin–tuberin tumor-suppressor complex. (dong2024comprehensiveinsightsinto pages 1-2) 2. Loss of inhibition of mTORC1 signaling → increased downstream phosphorylation (e.g., S6K/S6) and growth/proliferation programs. (wagner2021nabsirolimusforpatients pages 1-2, dong2024comprehensiveinsightsinto pages 1-2) 3. Clinical phenotype: tumor growth across multiple anatomical sites; in advanced disease, metastatic spread. (wagner2021nabsirolimusforpatients pages 1-2)
TFE3-rearranged subtype: A gynecologic PEComa review describes a TFE3-associated subtype with “heightened transcriptional activity of TFE3,” and notes downstream pro-oncogenic pathway activation (including “c-Met, AKT, and mTOR”). (levin2024gynecologicperivascularepithelioid pages 5-6)
6.2 Suggested GO biological process terms (examples)
- mTOR signaling (GO:0031929)
- Regulation of cell growth (GO:0001558)
- Positive regulation of cell proliferation (GO:0008284)
- Autophagy regulation (GO:0010506) (mTOR-linked, though PEComa-specific omics were not retrieved)
6.3 Suggested Cell Ontology (CL) terms (best-effort)
The neoplastic “perivascular epithelioid cell” has no universally agreed normal counterpart. Reviews state PEComas have “no known normal counterpart.” (nikolova2026pecomasrevisitedmtordriven pages 1-2) - Suggested CL mapping is therefore uncertain; as a pragmatic knowledge-base approach, represent the tumor cell as a mesenchymal neoplastic cell (custom/local class) with smooth muscle-like and melanocytic marker expression.
6.4 Molecular profiling (transcriptomics/proteomics/metabolomics/single-cell/spatial)
No PEComa-specific multi-omics datasets were identified in the retrieved evidence.
7. Anatomical Structures Affected
7.1 Organ level
PEComas can arise in many organs; commonly cited visceral sites include kidney, uterus, gastrointestinal tract, and others (liver, lung, retroperitoneum). (wagner2021nabsirolimusforpatients pages 1-2, dong2024comprehensiveinsightsinto pages 1-2)
Suggested UBERON terms (examples): - Kidney (UBERON:0002113) - Uterus (UBERON:0000995) - Liver (UBERON:0002107) - Lung (UBERON:0002048) - Retroperitoneal space (UBERON:0003684)
7.2 Tissue/cell level
- Mesenchymal tumor with perivascular growth pattern and immunophenotypic overlap with smooth muscle and melanocytic differentiation. (amante2024hepaticperivascularepithelioid pages 1-2, dong2024comprehensiveinsightsinto pages 1-2)
7.3 Subcellular level
No specific subcellular compartment abnormalities were described in the retrieved evidence.
8. Temporal Development
8.1 Onset
PEComas occur predominantly in adults, with some subsets (e.g., TFE3-rearranged) suggested to occur in younger patients in review discussions; detailed age-of-onset distributions were not comprehensively retrievable. (nikolova2026pecomasrevisitedmtordriven pages 2-4)
8.2 Progression / disease course
Clinical behavior ranges from indolent to aggressive metastatic malignancy. (wagner2021nabsirolimusforpatients pages 1-2, amante2024hepaticperivascularepithelioid pages 1-2)
9. Inheritance and Population
9.1 Epidemiology
Malignant PEComa is ultra-rare; an estimated annual incidence of ~1 per 1,000,000 is cited in trial and retrospective-series contexts. (wagner2021nabsirolimusforpatients pages 1-2, testa2023systemictreatmentsand pages 1-2)
9.2 Sex ratio and demographics
Female predominance is consistent across multiple sources. - A 2024 review reports female:male ratio outside sex-linked organs as ~1.6- to 5-fold higher in females. (dong2024comprehensiveinsightsinto pages 1-2) - Hepatic series: 29 female / 7 male; median age 47.8 years. (ji2024hepaticperivascularepithelioid pages 1-2)
9.3 Inheritance pattern
PEComa as a tumor diagnosis is not typically described as a Mendelian inherited disease; however, tuberous sclerosis complex (autosomal dominant TSC1/TSC2) predisposes to PEComa-family tumors in some individuals. (dong2024comprehensiveinsightsinto pages 1-2)
Penetrance/expressivity/carrier frequency/founder effects were not retrievable for PEComa specifically from the current evidence.
10. Diagnostics
10.1 Clinical and imaging tests
Imaging can be non-specific, and diagnostic accuracy may be low. - In hepatic PEComa, only 19.4% (7/36) were correctly diagnosed by imaging; vascular enhancement was frequent (75%, 27/36). (ji2024hepaticperivascularepithelioid pages 1-2)
10.2 Biopsy and pathology
Pathologic diagnosis is central. - Direct quote: “The diagnosis of a PEComa is based on its pathological features.” (amante2024hepaticperivascularepithelioid pages 1-2)
Key immunohistochemistry: - Direct quote: lesions are “typically … positive for HMB45, Melan-A, and smooth muscle actin (SMA) in decreasing order,” with advice to “evaluate immunoreactivity for TFE3.” (amante2024hepaticperivascularepithelioid pages 1-2)
10.3 Molecular diagnostics
Molecular profiling is increasingly relevant for subtype assignment and therapy selection. - AMPECT included tumor mutation profiling and demonstrated strong association of TSC2 mutation with response to nab-sirolimus. (wagner2021nabsirolimusforpatients pages 1-2)
10.4 Differential diagnosis
Not comprehensively extractable from the retrieved evidence; in practice, differentials are site-specific and include smooth muscle tumors and melanocytic tumors, among others (not detailed quantitatively in retrieved sources).
11. Outcome / Prognosis
11.1 General prognosis and prognostic factors
PEComa prognosis varies widely by site, resectability, and malignant risk features.
Risk stratification (Folpe-type criteria): A commonly used framework (endorsed in 2024 discussion) is Folpe’s criteria to categorize PEComa as benign, malignant, or uncertain malignant potential. (amante2024hepaticperivascularepithelioid pages 1-2)
A review excerpt summarizes Folpe features (used in practice): tumor size >5 cm; infiltrative growth; high nuclear grade/cellularity; mitotic activity >1/50 HPF; necrosis; vascular invasion; and tumors with ≥2 features are often considered malignant. (nikolova2026pecomasrevisitedmtordriven pages 1-2)
Biomarker-associated prognosis: In a 2023 advanced PEComa retrospective analysis (n=29), TFE3 overexpression correlated with higher risk of death (HR 11.8, P=0.04) and shorter median overall survival. (testa2023systemictreatmentsand pages 1-2)
11.2 Survival / disease control data
- Advanced malignant PEComa, AMPECT trial: median OS 40.8 months in primary report; updated median OS 53.1 months at trial completion. (wagner2021nabsirolimusforpatients pages 1-2, wagner2024phaseiitrial media 6536d2a4)
- Hepatic PEComa series: during follow-up (2–81 months), three malignant patients died within 6 months; most others had no recurrence/metastasis, with one intrahepatic recurrence. (ji2024hepaticperivascularepithelioid pages 1-2)
12. Treatment
12.1 Local therapy
Surgical resection is the cornerstone for localized disease; organ-specific alternatives (e.g., ablation, TACE) may be used when surgery is contraindicated. - Hepatic PEComa management distribution: resection 67.7% (24/36), radiofrequency ablation 16.7% (6/36), TACE 2.7% (1/36). (ji2024hepaticperivascularepithelioid pages 1-2)
Suggested MAXO terms (examples): - Surgical excision (MAXO:0001067) (term label may vary by ontology release) - Tumor ablation therapy (MAXO:0000756) - Transarterial chemoembolization (MAXO:0000936)
12.2 Systemic pharmacotherapy (current standard and recent developments)
nab-Sirolimus (albumin-bound sirolimus; FYARRO) — AMPECT trial
nab-sirolimus is described as approved in the US for metastatic or locally advanced malignant PEComa based on AMPECT trial results. (wagner2024phaseiitrial media 6536d2a4)
Primary report (JCO 2021): - ORR 39% (12/31; 95% CI 22–58) with 1 CR and 11 PR; stable disease 52%; progressive disease 10%. (wagner2021nabsirolimusforpatients pages 1-2) - Median PFS 10.6 months; median OS 40.8 months; median DOR not reached at primary analysis; responses rapid (67% by week 6) and durable. (wagner2021nabsirolimusforpatients pages 1-2) - Biomarker effect: 8/9 (89%) with TSC2 mutation responded vs 2/16 (13%) without (P<.001). (wagner2021nabsirolimusforpatients pages 1-2)
Long-term update (JCO 2024; data cutoff April 29, 2022): - Confirmed ORR 38.7%; median DOR 39.7 months; median PFS 10.6 months; median OS 53.1 months. (wagner2024phaseiitrial media 6536d2a4) - Most common TRAEs: stomatitis 82.4%, fatigue 61.8%, rash 61.8%; no grade ≥4 TRAEs. (wagner2024phaseiitrial media 6536d2a4)
Real-world implementation notes: The 2023 retrospective series emphasizes that nab-sirolimus is the only FDA-approved therapy for advanced malignant PEComa and that mTOR inhibitors are often preferred when possible due to chemotherapy morbidity and similar observed efficacy in retrospective comparisons. (testa2023systemictreatmentsand pages 1-2)
Image evidence: The 2024 JCO update includes Table 2 (efficacy outcomes) and Figure 1 (response waterfall/spider plots) supporting the above quantitative outcomes. (wagner2024phaseiitrial media 6536d2a4, wagner2024phaseiitrial media c9372bd3)
Other mTOR inhibitors (sirolimus, everolimus, temsirolimus)
Multiple reviews and retrospective analyses indicate clinical activity of mTOR inhibitors in PEComa, consistent with mTOR pathway dependence in TSC-altered tumors. (testa2023systemictreatmentsand pages 1-2, dong2024comprehensiveinsightsinto pages 1-2)
12.3 Immunotherapy and other targeted approaches
Evidence in the retrieved corpus is insufficient to summarize PEComa-specific immunotherapy efficacy beyond general mention in retrospective comparisons; robust response-rate data were not available. (testa2023systemictreatmentsand pages 1-2)
13. Prevention
No primary prevention strategies are established for sporadic PEComa given its ultra-rare incidence. In the context of tuberous sclerosis complex, surveillance for TSC-associated tumors is clinically relevant, but PEComa-specific preventive guidelines were not retrievable from the current evidence. (dong2024comprehensiveinsightsinto pages 1-2)
14. Other Species / Natural Disease
No naturally occurring PEComa disease burden in non-human species was identified in the retrieved evidence.
15. Model Organisms
No PEComa-specific engineered animal models were identified in the retrieved evidence. Mechanistic studies of TSC1/TSC2 and mTOR biology exist broadly (oncology and TSC field), but explicit PEComa model organism details were not retrievable here. (dong2024comprehensiveinsightsinto pages 1-2)
Recent developments (2023–2024 prioritized): key points
- Durable efficacy of nab-sirolimus confirmed with longer follow-up: median DOR ~39.7 months and median OS ~53.1 months in the 2024 AMPECT update. (wagner2024phaseiitrial media 6536d2a4)
- Continued emphasis on molecular stratification (mTOR/TSC-altered vs TFE3-rearranged) in 2024 reviews of renal and gynecologic PEComa. (levin2024gynecologicperivascularepithelioid pages 5-6, dong2024comprehensiveinsightsinto pages 1-2)
- Clinical characterization in organ-specific series (e.g., hepatic PEComa n=36) providing contemporary diagnostic yield and IHC frequency data (HMB45/Melan-A/SMA). (ji2024hepaticperivascularepithelioid pages 1-2)
- Prognostic signal for TFE3 overexpression in advanced PEComa retrospective analysis (worse OS; HR 11.8). (testa2023systemictreatmentsand pages 1-2)
Ongoing and recent clinical trials (selected)
(Records summarized are limited to information present in retrieved ClinicalTrials.gov chunks.)
- NCT02494570 (AMPECT): Phase 2 nab-sirolimus (ABI-009) in advanced malignant PEComa; multi-center; excludes LAM; publications report outcomes above. URL: https://clinicaltrials.gov/study/NCT02494570 (NCT02494570 chunk 2, wagner2021nabsirolimusforpatients pages 1-2)
- NCT03817515: Expanded access program for ABI-009 (sirolimus albumin-bound nanoparticles) in advanced PEComa and other mTOR-activated malignancies; status APPROVED_FOR_MARKETING. URL: https://clinicaltrials.gov/study/NCT03817515 (NCT03817515 chunk 1)
- NCT01690871: Phase II BEZ235 monotherapy (PI3K/mTOR inhibitor) in metastatic/unresectable malignant PEComa; WITHDRAWN; primary endpoint ORR (RECIST 1.1). URL: https://clinicaltrials.gov/study/NCT01690871 (NCT01690871 chunk 1)
Other PEComa-related trials were retrieved as metadata but not sufficiently detailed in the accessible text chunks to summarize endpoints accurately.
Limitations of this report
- Ontology identifiers (MONDO/Orphanet/ICD/MeSH) were not extractable from the currently retrieved full-text evidence via available tools; these should be programmatically filled from the ontology portals.
- PEComa is ultra-rare; many clinical inferences rely on case reports/small series and subtype/site heterogeneity.
References
-
(amante2024hepaticperivascularepithelioid pages 1-2): Marcelo Fabián Amante. Hepatic perivascular epithelioid cell tumors: benign, malignant, and uncertain malignant potential. World Journal of Gastroenterology, 30:2374-2378, May 2024. URL: https://doi.org/10.3748/wjg.v30.i18.2374, doi:10.3748/wjg.v30.i18.2374. This article has 18 citations.
-
(wagner2021nabsirolimusforpatients pages 1-2): Andrew J. Wagner, Vinod Ravi, Richard F. Riedel, Kristen Ganjoo, Brian A. Van Tine, Rashmi Chugh, Lee Cranmer, Erlinda M. Gordon, Jason L. Hornick, Heng Du, Berta Grigorian, Anita N. Schmid, Shihe Hou, Katherine Harris, David J. Kwiatkowski, Neil P. Desai, and Mark A. Dickson. nab-sirolimus for patients with malignant perivascular epithelioid cell tumors. Journal of Clinical Oncology, 39:3660-3670, Nov 2021. URL: https://doi.org/10.1200/jco.21.01728, doi:10.1200/jco.21.01728. This article has 181 citations and is from a highest quality peer-reviewed journal.
-
(testa2023systemictreatmentsand pages 1-2): Stefano Testa, Nam Q. Bui, and Kristen N. Ganjoo. Systemic treatments and molecular biomarkers for perivascular epithelioid cell tumors: a single-institution retrospective analysis. Cancer Research Communications, 3:1212-1223, Jul 2023. URL: https://doi.org/10.1158/2767-9764.crc-23-0139, doi:10.1158/2767-9764.crc-23-0139. This article has 18 citations and is from a peer-reviewed journal.
-
(dong2024comprehensiveinsightsinto pages 1-2): Bao Nan Dong, Hui Zhan, Ting Luan, and Jian Song Wang. Comprehensive insights into renal perivascular epithelioid cell neoplasms: from molecular mechanisms to clinical practice. World Journal of Oncology, 15:372-381, Jun 2024. URL: https://doi.org/10.14740/wjon1794, doi:10.14740/wjon1794. This article has 10 citations.
-
(nikolova2026pecomasrevisitedmtordriven pages 2-4): D Nikolova, B Terzyiski, and S Slavov. Pecomas revisited: mtor-driven and tfe3-rearranged tumors as distinct biological entities. Unknown journal, 2026.
-
(cohen2022cutaneousperivascularepithelioid pages 1-25): Philip R Cohen, Shumei M Kato, Christof P Erickson, Antoanella Calame, and Razelle Kurzrock. Cutaneous perivascular epithelioid cell tumor (pecoma): case report and world literature review of clinical and molecular characteristics. Dermatology Online Journal, Apr 2022. URL: https://doi.org/10.5070/d328157058, doi:10.5070/d328157058. This article has 13 citations and is from a peer-reviewed journal.
-
(nikolova2026pecomasrevisitedmtordriven pages 1-2): D Nikolova, B Terzyiski, and S Slavov. Pecomas revisited: mtor-driven and tfe3-rearranged tumors as distinct biological entities. Unknown journal, 2026.
-
(wagner2024phaseiitrial media 6536d2a4): Andrew J. Wagner, Vinod Ravi, Richard F. Riedel, Kristen Ganjoo, Brian A. Van Tine, Rashmi Chugh, Lee Cranmer, Erlinda M. Gordon, Jason L. Hornick, Heng Du, Li Ding, Anita N. Schmid, Willis H. Navarro, David J. Kwiatkowski, and Mark A. Dickson. Phase ii trial of nab-sirolimus in patients with advanced malignant perivascular epithelioid cell tumors (ampect): long-term efficacy and safety update. May 2024. URL: https://doi.org/10.1200/jco.23.02266, doi:10.1200/jco.23.02266. This article has 51 citations and is from a highest quality peer-reviewed journal.
-
(wagner2024phaseiitrial media c9372bd3): Andrew J. Wagner, Vinod Ravi, Richard F. Riedel, Kristen Ganjoo, Brian A. Van Tine, Rashmi Chugh, Lee Cranmer, Erlinda M. Gordon, Jason L. Hornick, Heng Du, Li Ding, Anita N. Schmid, Willis H. Navarro, David J. Kwiatkowski, and Mark A. Dickson. Phase ii trial of nab-sirolimus in patients with advanced malignant perivascular epithelioid cell tumors (ampect): long-term efficacy and safety update. May 2024. URL: https://doi.org/10.1200/jco.23.02266, doi:10.1200/jco.23.02266. This article has 51 citations and is from a highest quality peer-reviewed journal.
-
(ji2024hepaticperivascularepithelioid pages 1-2): Min Ji, Yuchen Zhang, Shuaibing Liu, Menghui Zhang, and Bingbing Qiao. Hepatic perivascular epithelioid cell tumor: a retrospective analysis of 36 cases. Frontiers in Oncology, Aug 2024. URL: https://doi.org/10.3389/fonc.2024.1416254, doi:10.3389/fonc.2024.1416254. This article has 9 citations.
-
(levin2024gynecologicperivascularepithelioid pages 1-3): Gabriel Levin, Mariana Pilon Capella, Raanan Meyer, Yoav Brezinov, and Walter H Gotlieb. Gynecologic perivascular epithelioid cell tumors (pecomas): a review of recent evidence. Archives of Gynecology and Obstetrics, 309:2381-2386, Apr 2024. URL: https://doi.org/10.1007/s00404-024-07510-5, doi:10.1007/s00404-024-07510-5. This article has 17 citations and is from a peer-reviewed journal.
-
(levin2024gynecologicperivascularepithelioid pages 5-6): Gabriel Levin, Mariana Pilon Capella, Raanan Meyer, Yoav Brezinov, and Walter H Gotlieb. Gynecologic perivascular epithelioid cell tumors (pecomas): a review of recent evidence. Archives of Gynecology and Obstetrics, 309:2381-2386, Apr 2024. URL: https://doi.org/10.1007/s00404-024-07510-5, doi:10.1007/s00404-024-07510-5. This article has 17 citations and is from a peer-reviewed journal.
-
(NCT02494570 chunk 2): A Phase 2 Study of Nab-sirolimus (ABI-009) in Patients With Advanced Malignant PEComa. Aadi Bioscience, Inc.. 2015. ClinicalTrials.gov Identifier: NCT02494570
-
(NCT03817515 chunk 1): Expanded Access for ABI-009 in Patients With Advanced PEComa and Patients With a Malignancy With Relevant Genetic Mutations or mTOR Pathway Activation. Aadi Bioscience, Inc.. ClinicalTrials.gov Identifier: NCT03817515
-
(NCT01690871 chunk 1): A Phase II Study of Orally Administered BEZ235 Monotherapy in Patients With Metastatic or Unresectable Malignant PEComa. Novartis Pharmaceuticals. 2012. ClinicalTrials.gov Identifier: NCT01690871