1. Disease Information
1.1 Overview / definition
NPSLE is commonly operationalized using the 1999 American College of Rheumatology (ACR) neuropsychiatric lupus nomenclature/case definitions, which defines 19 neuropsychiatric syndromes spanning central and peripheral nervous system involvement. (hanly2005managementofneuropsychiatric pages 1-3) Hanly & Harrison (2005), summarizing this framework, state that the ACR Research Committee produced “a standard nomenclature and diagnostic criteria for 19 NP syndromes” and that diagnosis is largely one of exclusion supported by imaging, electrophysiology, autoantibody profiles, and objective cognitive assessment. (hanly2005managementofneuropsychiatric pages 1-3)
1.2 Clinical classification frameworks
ACR 1999 neuropsychiatric syndromes (CNS/PNS) listed in Hanly & Harrison (2005): - CNS: aseptic meningitis; cerebrovascular disease; demyelinating syndrome; headache; movement disorder; myelopathy; seizure disorders; acute confusional state; anxiety disorder; cognitive dysfunction; mood disorder; psychosis. (hanly2005managementofneuropsychiatric pages 1-3) - PNS: Guillain–Barré syndrome; autonomic neuropathy; mononeuropathy; myasthenia gravis; cranial neuropathy; plexopathy; polyneuropathy. (hanly2005managementofneuropsychiatric pages 1-3)
1.3 Synonyms / alternative names
Historically, older terms such as “CNS lupus” and “lupus cerebritis” have been used (and are referenced as prior terminology in recent reviews), but contemporary literature generally uses “neuropsychiatric systemic lupus erythematosus (NPSLE)” and ACR syndrome-based descriptors. (justizvaillant2024neuropsychiatricsystemiclupus pages 1-2)
1.4 Key identifiers (ontology and coding)
- MeSH terms observed in clinical trial registry records relevant to CNS lupus/NPSLE include “Lupus Vasculitis, Central Nervous System” (MeSH D020945) and “Lupus Erythematosus, Systemic” (MeSH D008180). (NCT07281105 chunk 2)
- MONDO / Orphanet / ICD-10/ICD-11 codes: not identified in the retrieved full-text evidence in this run; therefore not asserted here.
1.5 Evidence source type
This report is derived from aggregated disease-level resources (reviews, systematic reviews, guidelines) and human clinical observational studies, plus registered clinical trials; it is not derived from individual EHR records. (bortoluzzi2024therapeuticstrategiesand pages 1-6, kammeyer2024bloodbasedbiomarkersof pages 1-3, emerson2023theconundrumof pages 1-2, NCT07281105 chunk 1)
2. Etiology
2.1 Disease causal factors (mechanistic)
Current evidence supports multifactorial causation, with overlapping inflammatory/autoimmune and vascular pathways. Hanly & Harrison (2005) highlight candidate primary mechanisms including “intracranial microangiopathy, autoantibodies to neuronal and non-neuronal antigens, and the generation of proinflammatory cytokines and mediators.” (hanly2005managementofneuropsychiatric pages 1-3) A 2024 review similarly emphasizes that NPSLE pathogenesis is “thought to involve inflammatory and vascular pathways,” reinforcing the dual-mechanism view used clinically to guide therapy. (patel2024thechallengeof pages 11-13)
2.2 Risk factors (human clinical)
Risk factors summarized in the 2024 Diagnostics review include: - Generalized SLE disease activity as a risk factor for NP manifestations, and NPSLE is “often seen in 40–50% of patients with generalized SLE activity” (as reported in that review). (patel2024thechallengeof pages 4-5) - Antiphospholipid antibodies (aPL) as a risk factor, especially for cerebrovascular disease and other vascular manifestations. (patel2024thechallengeof pages 4-5) - Additional associations for specific syndromes (e.g., psychosis) described in that review include male sex, younger age at SLE diagnosis, and ancestry-related differences, though these are summarized from prior literature rather than established as diagnostic. (patel2024thechallengeof pages 4-5)
2.3 Protective factors / gene–environment interactions
Protective factors and explicit gene–environment interactions specific to NPSLE were not directly quantified in the retrieved evidence corpus; therefore no claims are made here.
3. Phenotypes (clinical manifestations)
3.1 Phenotype spectrum and frequency
Reported frequency varies widely because syndrome definitions and attribution stringency differ. - Emerson et al. (2023) state: “The prevalence rates of NPSLE vary widely in the published literature, estimated to be between 12 and 95%.” (emerson2023theconundrumof pages 1-2) - Hanly & Harrison (2005) summarize prevalence across cohorts using ACR nomenclature: overall NP prevalence 37–95%, with common manifestations including cognitive dysfunction 55–80%, headache 24–72%, mood disorder 14–57%, cerebrovascular disease 5–18%, seizures 6–51%, polyneuropathy 3–28%, anxiety 7–24%, psychosis 0–8%. (hanly2005managementofneuropsychiatric pages 1-3) - A 2024 systematic review reported syndrome-specific prevalence estimates including status epilepticus and transverse myelitis around 1–2%, while cognitive dysfunction approached ~38% across included studies. (ricecanetto2024neuropsychiatricsystemiclupus pages 1-2)
3.2 Pediatric phenotype and timing
In juvenile SLE, Labouret et al. reported among 51 patients with juvenile SLE, 39% had juvenile NPSLE, and NPSLE occurred at SLE onset in 65%. (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
3.3 Quality of life impacts
NPSLE is associated with substantial morbidity and reduced quality of life. Kammeyer et al. note that NPSLE is associated with “decreased quality of life and a significant increase in morbidity, mortality, hospitalization, and disease related costs compared to SLE without NP symptoms.” (kammeyer2024bloodbasedbiomarkersof pages 1-3)
3.4 Suggested HPO terms (examples for knowledge-base mapping)
Below are recommended HPO mappings for common ACR syndromes (term names only; IDs should be validated in downstream curation): - Cognitive dysfunction → Cognitive impairment (HP: Cognitive impairment) - Seizure disorder/status epilepticus → Seizures (HP: Seizures) - Psychosis → Psychosis (HP: Psychosis) - Mood disorder/depression → Depressed mood (HP: Depressed mood) - Headache → Headache (HP: Headache) - Cerebrovascular disease/stroke → Stroke (HP: Stroke) - Myelopathy/transverse myelitis → Myelopathy (HP: Myelopathy) - Polyneuropathy → Peripheral neuropathy (HP: Peripheral neuropathy) These phenotype selections are consistent with the ACR syndrome list and the clinical emphasis in reviews. (hanly2005managementofneuropsychiatric pages 1-3)
4. Genetic / Molecular Information
4.1 Genetic susceptibility (limited in retrieved corpus)
A 2024 review highlights genetic contributors to SLE/NPSLE broadly, referencing defective apoptosis (e.g., FAS) and REL/NF-κB pathway associations, but without NPSLE-specific causal variants established in the retrieved text. (justizvaillant2024neuropsychiatricsystemiclupus pages 1-2)
4.2 Key molecular mediators and autoantibodies
Inflammatory mediators and autoantibodies repeatedly implicated include: - Cytokines such as IL-6 and type I interferon (IFN-α) (with CSF IFN-α emerging in pediatric NPSLE biomarker work). (labouret2023juvenileneuropsychiatricsystemic pages 1-2, patel2024thechallengeof pages 4-5) - Broad autoimmune effectors (immune complexes, circulating antibodies, cytokines, autoreactive T cells) highlighted as drivers of tissue injury in NPSLE-focused reviews. (justizvaillant2024neuropsychiatricsystemiclupus pages 1-2)
4.3 Suggested GO terms (biological process) and CL terms (cell types)
Mechanistically motivated ontology suggestions based on the reviewed evidence include: - GO biological process: type I interferon signaling pathway, complement activation, inflammatory response, blood–brain barrier maintenance/disruption. (labouret2023juvenileneuropsychiatricsystemic pages 1-2) - Cell types (CL): microglial cell, astrocyte, brain endothelial cell (relevant to CSF neopterin concept and BBB-focused mechanisms). (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
5. Mechanism / Pathophysiology (causal chains)
5.1 Two major mechanistic clusters used clinically: inflammatory vs vascular/ischemic
Clinical practice commonly separates NPSLE into processes dominated by inflammation versus thrombotic/ischemic injury to guide therapy. (bortoluzzi2024therapeuticstrategiesand pages 9-11) Bortoluzzi et al. explicitly note that “Current recommendations advocate for a therapeutic approach aimed at targeting the underlying pathophysiological mechanisms in NPSLE differentiating inflammatory or embolic/thrombotic/ischemic process,” with glucocorticoids/immunosuppressants used for inflammation and anticoagulant/antithrombotic interventions favored when aPL antibodies point toward vascular mechanisms. (bortoluzzi2024therapeuticstrategiesand pages 9-11)
5.2 Neuroinflammation and intrathecal type I interferon
In juvenile NPSLE, Labouret et al. found no specific routine biological or radiological marker, but observed that CSF neopterin was significantly higher in active CNS-involved NPSLE (p=0.0008) and that CSF IFN-α and neopterin decreased after clinical resolution under immunosuppressive treatment (p=0.0010–0.0015), supporting a model of CNS immune activation / interferon-associated neuroinflammation. (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
5.3 Neuronal and glial injury as a final common pathway (2024 biomarker advance)
Kammeyer et al. (2024) evaluated blood-based neurofilament light (NfL) and GFAP as accessible indicators of neuronal/glial injury in active major NPSLE and observed substantially higher levels in active NPSLE than disease-matched SLE controls, with decreases after immunotherapy in a subset. (kammeyer2024bloodbasedbiomarkersof pages 1-3) This supports a causal chain: upstream immune/vascular injury → axonal/glial damage → elevated NfL/GFAP detectable peripherally, potentially enabling monitoring and earlier recognition. (kammeyer2024bloodbasedbiomarkersof pages 1-3)
6. Diagnostics (and differential diagnosis)
6.1 Diagnostic concept: attribution and exclusion
Hanly & Harrison (2005) emphasize that “The diagnosis of NP-SLE remains largely one of exclusion,” requiring evaluation for non-SLE causes (therapy complications, comorbidities) before attribution to lupus mechanisms. (hanly2005managementofneuropsychiatric pages 1-3) Emerson et al. (2023) similarly highlight barriers including “the heterogeneity of neurological symptoms, the absence of standardized assessment, [and] the unreliability of conventional markers,” motivating use of composite panels. (emerson2023theconundrumof pages 1-2)
6.2 Conventional investigations (real-world implementation)
A 2024 review outlines that workup is tailored to the presenting syndrome and begins with excluding secondary causes (infection, metabolic/endocrine disorders, adverse drug reactions, malignancy) and then incorporates labs, autoantibody assessments including aPL testing, imaging, and CSF studies as indicated, often requiring multidisciplinary care (neurology/psychiatry/neuroradiology). (patel2024thechallengeof pages 4-5)
6.3 Emerging/novel biomarkers (2023–2024)
- CSF IFN-α and neopterin (pediatric): elevated in active CNS-involved j-NPSLE and decrease after treatment, with strong correlation (Rs=0.832). (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
- Blood NfL and GFAP (adult/teen major NPSLE): active major NPSLE vs SLE controls showed NfL +17.9 pg/mL and GFAP +3.2 pg/mL (both p<0.001); blood and CSF levels correlated (r=0.81–0.88). (kammeyer2024bloodbasedbiomarkersof pages 1-3, kammeyer2024bloodbasedbiomarkersof pages 5-6)
6.4 Suggested LOINC-style lab concepts (non-exhaustive)
- CSF interferon-alpha protein; CSF neopterin; plasma/serum neurofilament light; plasma/serum GFAP; serum complements (C3/C4); anti-dsDNA titers; antiphospholipid antibody panel. These are supported by biomarker-focused primary studies and diagnostic review content. (kammeyer2024bloodbasedbiomarkersof pages 1-3, labouret2023juvenileneuropsychiatricsystemic pages 1-2, patel2024thechallengeof pages 4-5)
7. Outcomes / Prognosis
7.1 Real-world outcomes (2024 multicenter cohort)
In an international multicenter retrospective study of first NP events (350 events), 64% improved at 12 months; focal central events improved frequently (83% for focal central events in the excerpted results), and SLE-attributed events improved more often. (bortoluzzi2024therapeuticstrategiesand pages 9-11, bortoluzzi2024therapeuticstrategiesand pages 1-6) Importantly, patients whose NP manifestation was attributed to SLE by clinical judgment and treated with immunosuppressants had a higher probability of response (OR 2.55, 95% CI 1.06–6.41). (bortoluzzi2024therapeuticstrategiesand pages 1-6)
7.2 Syndrome-dependent prognosis (systematic review)
A 2024 systematic review reported prognosis as highly syndrome-dependent, including a 12.5% one-year mortality in status epilepticus/seizure presentations, while some other presentations may resolve. (ricecanetto2024neuropsychiatricsystemiclupus pages 1-2)
7.3 Prognostic/monitoring biomarkers
Kammeyer et al. observed that in a subset with longitudinal sampling, blood NfL and GFAP “decreased after immunotherapy,” suggesting potential utility for monitoring treatment response, though larger longitudinal validation is needed. (kammeyer2024bloodbasedbiomarkersof pages 1-3)
8. Treatment (guidelines, real-world implementation, and trials)
8.1 Guideline-level management principles relevant to NPSLE
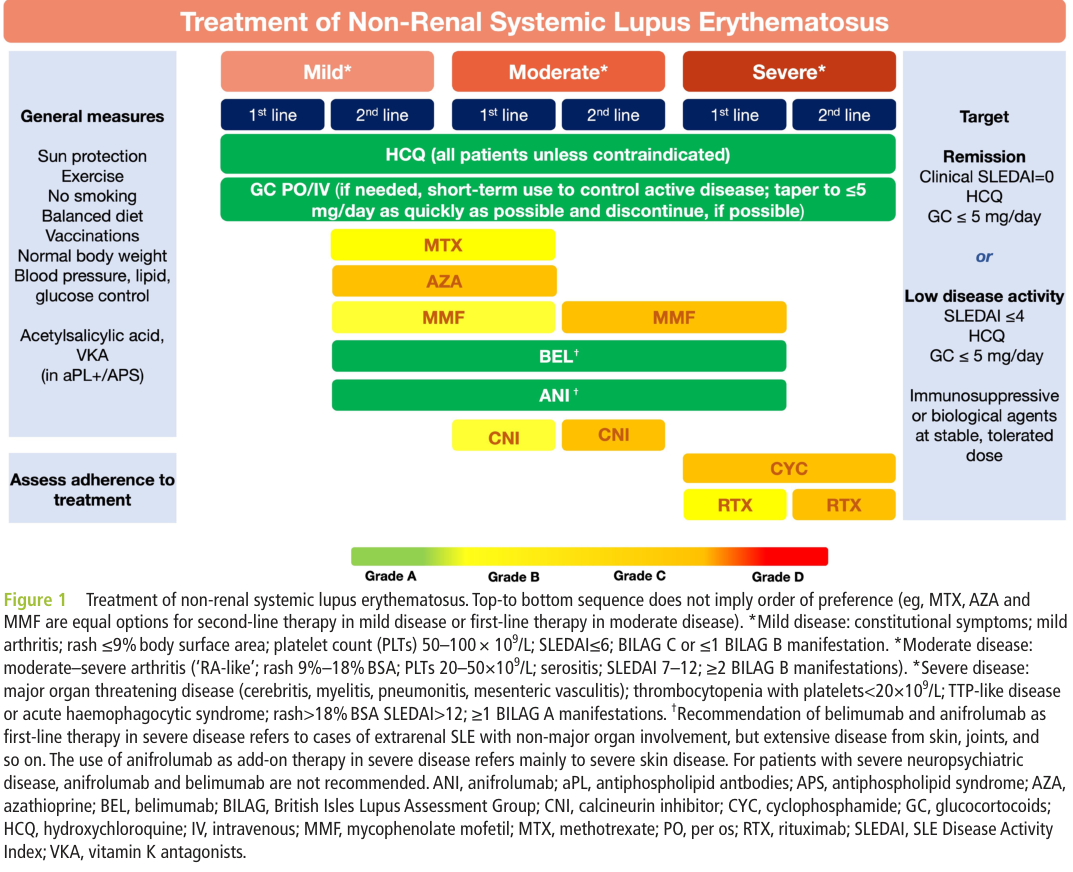
The EULAR 2023 update (published 2024) provides overarching SLE treatment principles relevant to NPSLE management (universal HCQ, steroid minimization, early steroid-sparing therapy). (fanouriakis2024eularrecommendationsfor pages 10-11) Fanouriakis et al. recommend hydroxychloroquine for all patients at a target dose 5 mg/kg/day, and minimizing maintenance glucocorticoids to ≤5 mg/day prednisone equivalent with withdrawal when possible. (fanouriakis2024eularrecommendationsfor pages 10-11) For organ-threatening/refractory disease, the guideline notes roles for cyclophosphamide and rituximab, respectively. (fanouriakis2024eularrecommendationsfor pages 10-11)
8.2 Specific point for severe neuropsychiatric disease (EULAR figure)
The EULAR treatment framework figure explicitly states: “For patients with severe neuropsychiatric disease, anifrolumab and belimumab are not recommended.” (fanouriakis2024eularrecommendationsfor media 9daa74df)
8.3 Syndrome- and mechanism-guided therapy (inflammatory vs ischemic)
A contemporary approach described in the multicenter cohort discussion is to align therapy with inferred mechanism: glucocorticoids/immunosuppressants for inflammatory NPSLE; antithrombotic/anticoagulant approaches when aPL-associated vascular mechanisms predominate. (bortoluzzi2024therapeuticstrategiesand pages 9-11) A 2024 review’s proposed algorithm similarly includes immunosuppressive escalation (glucocorticoids, cyclophosphamide, azathioprine, mycophenolate) and rescue options (IVIg, plasmapheresis, rituximab) for refractory inflammatory disease, plus antithrombotic therapy for thrombotic/ischemic manifestations. (patel2024thechallengeof pages 10-11)
8.4 Real-world implementation and outcomes (2024 multicenter cohort)
Bortoluzzi et al. observed that immunosuppressants and corticosteroids were initiated/escalated more frequently in central diffuse or focal NP events attributed to SLE, and that this strategy was associated with improved outcomes at 12 months in clinically judged SLE-attributed events. (bortoluzzi2024therapeuticstrategiesand pages 9-11, bortoluzzi2024therapeuticstrategiesand pages 1-6)
8.5 Experimental/clinical trials (selected; real-world pipeline)
- EG-501 (low-affinity NMDA receptor antagonist) for cognitive impairment in NPSLE (Phase 2, randomized placebo-controlled): registry record shows the trial was COMPLETED, with primary completion 2025-08-12, and describes NPSLE cognitive impairment as a serious unmet need; the primary endpoint used RBANS Total Index Score. (NCT07281105 chunk 1)
- INLES (NCT05880121) observational connectomics + immune correlates: integrates advanced MRI with identification of candidate autoantigens/immune fingerprints for NPSLE. (NCT05880121 chunk 1)
- fMRI early brain injury study (NCT06226324): posted 2024-01-26, prospective case-control design to detect early brain functional changes in SLE ± neuropsychiatric symptoms. (NCT06226324 chunk 1)
8.6 Suggested MAXO terms (examples)
- Immunosuppressive therapy → Immunosuppressive therapy (MAXO) (e.g., glucocorticoid therapy, cyclophosphamide therapy, mycophenolate therapy). (patel2024thechallengeof pages 10-11)
- Antithrombotic therapy → Anticoagulant therapy / antiplatelet therapy (MAXO) for aPL-associated ischemic NPSLE. (bortoluzzi2024therapeuticstrategiesand pages 9-11)
- Neuropsychiatric symptomatic treatment → Antiepileptic therapy, antipsychotic therapy, antidepressant therapy, anxiolytic therapy (MAXO mappings). (patel2024thechallengeof pages 10-11)
9. Prevention
Primary prevention specific to NPSLE (i.e., preventing first neuropsychiatric event) is not established in the retrieved evidence corpus. However, tertiary prevention principles are implicit in guideline approaches to reduce flares and steroid exposure in SLE generally and in mechanism-guided management of NP events (minimize glucocorticoid toxicity; treat active disease promptly; address thrombosis risk when aPL present). (fanouriakis2024eularrecommendationsfor pages 10-11, bortoluzzi2024therapeuticstrategiesand pages 9-11)
10. Other species / natural disease
Not addressed in the retrieved evidence corpus.
11. Model organisms / experimental systems
A 2024 review reports preclinical evidence that ACE inhibitors reduced type I interferon responses and improved cognitive deficits in mice, suggesting a neuroimmune-interferon axis that might be therapeutically targetable, though this remains preclinical. (patel2024thechallengeof pages 11-13)
12. Recent developments & expert analysis (2023–2024)
12.1 Diagnostic paradigm shift: composite panels and endophenotypes
Emerson et al. (2023) advocate moving beyond NPSLE as a single entity and emphasize that “a composite panel of these investigations will be needed” due to non-specificity of individual tests. (emerson2023theconundrumof pages 1-2) This is consistent with 2023–2024 biomarker advances (CSF IFN-α/neopterin; blood NfL/GFAP) that are not individually definitive but provide quantifiable signals of CNS immune activation and neural injury. (kammeyer2024bloodbasedbiomarkersof pages 1-3, labouret2023juvenileneuropsychiatricsystemic pages 1-2)
12.2 Practical treatment insight from multicenter real-world data
The 2024 multicenter cohort provides actionable evidence that attribution (clinical judgment) combined with immunosuppressive treatment is associated with better 12-month outcomes, quantifying benefit (OR 2.55). (bortoluzzi2024therapeuticstrategiesand pages 1-6)
13. Abstract-supported direct quotes (for knowledge-base evidence items)
- Emerson et al. (2023) abstract: “The prevalence rates of NPSLE vary widely in the published literature, estimated to be between 12 and 95%.” (emerson2023theconundrumof pages 1-2)
- Emerson et al. (2023) abstract: “Novel serum and CSF markers, including autoantibodies, cytokines and chemokines have also shown increasing utility …” (emerson2023theconundrumof pages 1-2)
- Kammeyer et al. (2024) abstract: “Blood NfL was on average 17.9 pg/ml higher … and blood GFAP was on average 3.2 pg/ml higher … for cases of active major NPSLE compared to SLE without active major NPSLE.” (kammeyer2024bloodbasedbiomarkersof pages 1-3)
- Labouret et al. (2023) abstract: “CSF IFN-α and neopterin constitute promising biomarkers useful in the diagnosis and monitoring of activity in j-NPSLE.” (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
14. Key gaps and limitations of this tool-based synthesis
- Several requested standardized identifiers (MONDO, Orphanet, ICD-10/ICD-11) were not present in the retrieved evidence corpus; they should be added via dedicated ontology lookups outside this run.
- Gene/variant-level evidence specific to NPSLE susceptibility was limited in the retrieved full texts; additional GWAS/ClinVar/ClinGen and NPSLE-focused genomics studies would strengthen Sections 2 and 4.
References (URLs and publication dates are embedded above where available)
Key 2023–2024 sources emphasized include Emerson et al. 2023 (Frontiers in Neurology), Labouret et al. 2023 (J Clin Immunol), Fanouriakis et al. 2024 (Ann Rheum Dis; EULAR 2023 update), Bortoluzzi et al. 2024 (Rheumatology), Kammeyer et al. 2024 (Lupus), and Rice-Canetto et al. 2024 (Cureus). (bortoluzzi2024therapeuticstrategiesand pages 1-6, kammeyer2024bloodbasedbiomarkersof pages 1-3, labouret2023juvenileneuropsychiatricsystemic pages 1-2, emerson2023theconundrumof pages 1-2, fanouriakis2024eularrecommendationsfor media 9daa74df)
References
-
(hanly2005managementofneuropsychiatric pages 1-3): John G. Hanly and Melanie J. Harrison. Management of neuropsychiatric lupus. Best practice & research. Clinical rheumatology, 19 5:799-821, Oct 2005. URL: https://doi.org/10.1016/j.berh.2005.04.003, doi:10.1016/j.berh.2005.04.003. This article has 126 citations.
-
(patel2024thechallengeof pages 4-5): Veena Patel. The challenge of neuropsychiatric systemic lupus erythematosus: from symptoms to therapeutic strategies. Diagnostics, 14:1186, Jun 2024. URL: https://doi.org/10.3390/diagnostics14111186, doi:10.3390/diagnostics14111186. This article has 27 citations.
-
(kammeyer2024bloodbasedbiomarkersof pages 1-3): Ryan Kammeyer, Kimberly Chapman, Anna Furniss, Elena Hsieh, Robert Fuhlbrigge, Ekemini A. Ogbu, Susan Boackle, JoAnn Zell, Kavita V. Nair, Tyler L. Borko, Jennifer C. Cooper, Jeffrey L. Bennett, and Amanda L. Piquet. Blood-based biomarkers of neuronal and glial injury in active major neuropsychiatric systemic lupus erythematosus. Lupus, 33:1116-1129, Aug 2024. URL: https://doi.org/10.1177/09612033241272961, doi:10.1177/09612033241272961. This article has 15 citations and is from a peer-reviewed journal.
-
(labouret2023juvenileneuropsychiatricsystemic pages 1-2): Mathilde Labouret, Stefania Costi, Vincent Bondet, Vincent Trebossen, Enora Le Roux, Alexandra Ntorkou, Sophie Bartoli, Stéphane Auvin, Brigitte Bader-Meunier, Véronique Baudouin, Olivier Corseri, Glory Dingulu, Camille Ducrocq, Cécile Dumaine, Monique Elmaleh, Nicole Fabien, Albert Faye, Isabelle Hau, Véronique Hentgen, Théresa Kwon, Ulrich Meinzer, Naim Ouldali, Cyrielle Parmentier, Marie Pouletty, Florence Renaldo, Isabelle Savioz, Flore Rozenberg, Marie-Louise Frémond, Alice Lepelley, Gillian I. Rice, Luis Seabra, Jean-François Benoist, Darragh Duffy, Yanick J. Crow, Pierre Ellul, and Isabelle Melki. Juvenile neuropsychiatric systemic lupus erythematosus: identification of novel central neuroinflammation biomarkers. Journal of Clinical Immunology, 43:615-624, Dec 2023. URL: https://doi.org/10.1007/s10875-022-01407-1, doi:10.1007/s10875-022-01407-1. This article has 28 citations and is from a domain leading peer-reviewed journal.
-
(emerson2023theconundrumof pages 1-2): Jonathan S. Emerson, Simon M. Gruenewald, Lavier Gomes, Ming-Wei Lin, and Sanjay Swaminathan. The conundrum of neuropsychiatric systemic lupus erythematosus: current and novel approaches to diagnosis. Frontiers in Neurology, Mar 2023. URL: https://doi.org/10.3389/fneur.2023.1111769, doi:10.3389/fneur.2023.1111769. This article has 53 citations and is from a peer-reviewed journal.
-
(ricecanetto2024neuropsychiatricsystemiclupus pages 1-2): Tyler E Rice-Canetto, Sonali J Joshi, Katie A Kyan, and Javed Siddiqi. Neuropsychiatric systemic lupus erythematosus: a systematic review. Cureus, Jun 2024. URL: https://doi.org/10.7759/cureus.61678, doi:10.7759/cureus.61678. This article has 13 citations.
-
(kammeyer2024bloodbasedbiomarkersof pages 5-6): Ryan Kammeyer, Kimberly Chapman, Anna Furniss, Elena Hsieh, Robert Fuhlbrigge, Ekemini A. Ogbu, Susan Boackle, JoAnn Zell, Kavita V. Nair, Tyler L. Borko, Jennifer C. Cooper, Jeffrey L. Bennett, and Amanda L. Piquet. Blood-based biomarkers of neuronal and glial injury in active major neuropsychiatric systemic lupus erythematosus. Lupus, 33:1116-1129, Aug 2024. URL: https://doi.org/10.1177/09612033241272961, doi:10.1177/09612033241272961. This article has 15 citations and is from a peer-reviewed journal.
-
(labouret2023juvenileneuropsychiatricsystemic pages 4-5): Mathilde Labouret, Stefania Costi, Vincent Bondet, Vincent Trebossen, Enora Le Roux, Alexandra Ntorkou, Sophie Bartoli, Stéphane Auvin, Brigitte Bader-Meunier, Véronique Baudouin, Olivier Corseri, Glory Dingulu, Camille Ducrocq, Cécile Dumaine, Monique Elmaleh, Nicole Fabien, Albert Faye, Isabelle Hau, Véronique Hentgen, Théresa Kwon, Ulrich Meinzer, Naim Ouldali, Cyrielle Parmentier, Marie Pouletty, Florence Renaldo, Isabelle Savioz, Flore Rozenberg, Marie-Louise Frémond, Alice Lepelley, Gillian I. Rice, Luis Seabra, Jean-François Benoist, Darragh Duffy, Yanick J. Crow, Pierre Ellul, and Isabelle Melki. Juvenile neuropsychiatric systemic lupus erythematosus: identification of novel central neuroinflammation biomarkers. Journal of Clinical Immunology, 43:615-624, Dec 2023. URL: https://doi.org/10.1007/s10875-022-01407-1, doi:10.1007/s10875-022-01407-1. This article has 28 citations and is from a domain leading peer-reviewed journal.
-
(bortoluzzi2024therapeuticstrategiesand pages 9-11): Alessandra Bortoluzzi, Antonis Fanouriakis, Ettore Silvagni, Simone Appenzeller, Linda Carli, Greta Carrara, Alberto Cauli, Fabrizio Conti, Lilian Teresa Lavras Costallat, Ginevra De Marchi, Andrea Doria, Micaela Fredi, Franco Franceschini, Carlo Garaffoni, John G Hanly, Marta Mosca, Elana Murphy, Matteo Piga, Luca Quartuccio, Carlo Alberto Scirè, Paola Tomietto, Simona Truglia, Anna Zanetti, Margherita Zen, George Bertsias, and Marcello Govoni. Therapeutic strategies and outcomes in neuropsychiatric systemic lupus erythematosus: an international multicenter retrospective study. Rheumatology, 63:2711-2720, Feb 2024. URL: https://doi.org/10.1093/rheumatology/keae119, doi:10.1093/rheumatology/keae119. This article has 14 citations and is from a peer-reviewed journal.
-
(bortoluzzi2024therapeuticstrategiesand pages 1-6): Alessandra Bortoluzzi, Antonis Fanouriakis, Ettore Silvagni, Simone Appenzeller, Linda Carli, Greta Carrara, Alberto Cauli, Fabrizio Conti, Lilian Teresa Lavras Costallat, Ginevra De Marchi, Andrea Doria, Micaela Fredi, Franco Franceschini, Carlo Garaffoni, John G Hanly, Marta Mosca, Elana Murphy, Matteo Piga, Luca Quartuccio, Carlo Alberto Scirè, Paola Tomietto, Simona Truglia, Anna Zanetti, Margherita Zen, George Bertsias, and Marcello Govoni. Therapeutic strategies and outcomes in neuropsychiatric systemic lupus erythematosus: an international multicenter retrospective study. Rheumatology, 63:2711-2720, Feb 2024. URL: https://doi.org/10.1093/rheumatology/keae119, doi:10.1093/rheumatology/keae119. This article has 14 citations and is from a peer-reviewed journal.
-
(fanouriakis2024eularrecommendationsfor pages 10-11): Antonis Fanouriakis, Myrto Kostopoulou, Jeanette Andersen, Martin Aringer, Laurent Arnaud, Sang-Cheol Bae, John Boletis, Ian N Bruce, Ricard Cervera, Andrea Doria, Thomas Dörner, Richard A Furie, Dafna D Gladman, Frederic A Houssiau, Luís Sousa Inês, David Jayne, Marios Kouloumas, László Kovács, Chi Chiu Mok, Eric F Morand, Gabriella Moroni, Marta Mosca, Johanna Mucke, Chetan B Mukhtyar, György Nagy, Sandra Navarra, Ioannis Parodis, José M Pego-Reigosa, Michelle Petri, Bernardo A Pons-Estel, Matthias Schneider, Josef S Smolen, Elisabet Svenungsson, Yoshiya Tanaka, Maria G Tektonidou, YK Onno Teng, Angela Tincani, Edward M Vital, Ronald F van Vollenhoven, Chris Wincup, George Bertsias, and Dimitrios T Boumpas. Eular recommendations for the management of systemic lupus erythematosus: 2023 update. Annals of the Rheumatic Diseases, 83:15-29, Jan 2024. URL: https://doi.org/10.1136/ard-2023-224762, doi:10.1136/ard-2023-224762. This article has 1255 citations and is from a highest quality peer-reviewed journal.
-
(fanouriakis2024eularrecommendationsfor pages 7-8): Antonis Fanouriakis, Myrto Kostopoulou, Jeanette Andersen, Martin Aringer, Laurent Arnaud, Sang-Cheol Bae, John Boletis, Ian N Bruce, Ricard Cervera, Andrea Doria, Thomas Dörner, Richard A Furie, Dafna D Gladman, Frederic A Houssiau, Luís Sousa Inês, David Jayne, Marios Kouloumas, László Kovács, Chi Chiu Mok, Eric F Morand, Gabriella Moroni, Marta Mosca, Johanna Mucke, Chetan B Mukhtyar, György Nagy, Sandra Navarra, Ioannis Parodis, José M Pego-Reigosa, Michelle Petri, Bernardo A Pons-Estel, Matthias Schneider, Josef S Smolen, Elisabet Svenungsson, Yoshiya Tanaka, Maria G Tektonidou, YK Onno Teng, Angela Tincani, Edward M Vital, Ronald F van Vollenhoven, Chris Wincup, George Bertsias, and Dimitrios T Boumpas. Eular recommendations for the management of systemic lupus erythematosus: 2023 update. Annals of the Rheumatic Diseases, 83:15-29, Jan 2024. URL: https://doi.org/10.1136/ard-2023-224762, doi:10.1136/ard-2023-224762. This article has 1255 citations and is from a highest quality peer-reviewed journal.
-
(fanouriakis2024eularrecommendationsfor media 9daa74df): Antonis Fanouriakis, Myrto Kostopoulou, Jeanette Andersen, Martin Aringer, Laurent Arnaud, Sang-Cheol Bae, John Boletis, Ian N Bruce, Ricard Cervera, Andrea Doria, Thomas Dörner, Richard A Furie, Dafna D Gladman, Frederic A Houssiau, Luís Sousa Inês, David Jayne, Marios Kouloumas, László Kovács, Chi Chiu Mok, Eric F Morand, Gabriella Moroni, Marta Mosca, Johanna Mucke, Chetan B Mukhtyar, György Nagy, Sandra Navarra, Ioannis Parodis, José M Pego-Reigosa, Michelle Petri, Bernardo A Pons-Estel, Matthias Schneider, Josef S Smolen, Elisabet Svenungsson, Yoshiya Tanaka, Maria G Tektonidou, YK Onno Teng, Angela Tincani, Edward M Vital, Ronald F van Vollenhoven, Chris Wincup, George Bertsias, and Dimitrios T Boumpas. Eular recommendations for the management of systemic lupus erythematosus: 2023 update. Annals of the Rheumatic Diseases, 83:15-29, Jan 2024. URL: https://doi.org/10.1136/ard-2023-224762, doi:10.1136/ard-2023-224762. This article has 1255 citations and is from a highest quality peer-reviewed journal.
-
(justizvaillant2024neuropsychiatricsystemiclupus pages 1-2): Angel A. Justiz-Vaillant, Darren Gopaul, Sachin Soodeen, Rodolfo Arozarena-Fundora, Odette Arozarena Barbosa, Chandrashehkar Unakal, Reinand Thompson, Bijay Pandit, Srikanth Umakanthan, and Patrick E. Akpaka. Neuropsychiatric systemic lupus erythematosus: molecules involved in its imunopathogenesis, clinical features, and treatment. Molecules, 29:747, Feb 2024. URL: https://doi.org/10.3390/molecules29040747, doi:10.3390/molecules29040747. This article has 76 citations.
-
(NCT07281105 chunk 2): EG-501 for Cognitive Impairment in Neuropsychiatric SLE (NPSLE): Efficacy and Safety Study. Evergreen Therapeutics, Inc.. 2018. ClinicalTrials.gov Identifier: NCT07281105
-
(NCT07281105 chunk 1): EG-501 for Cognitive Impairment in Neuropsychiatric SLE (NPSLE): Efficacy and Safety Study. Evergreen Therapeutics, Inc.. 2018. ClinicalTrials.gov Identifier: NCT07281105
-
(patel2024thechallengeof pages 11-13): Veena Patel. The challenge of neuropsychiatric systemic lupus erythematosus: from symptoms to therapeutic strategies. Diagnostics, 14:1186, Jun 2024. URL: https://doi.org/10.3390/diagnostics14111186, doi:10.3390/diagnostics14111186. This article has 27 citations.
-
(patel2024thechallengeof pages 10-11): Veena Patel. The challenge of neuropsychiatric systemic lupus erythematosus: from symptoms to therapeutic strategies. Diagnostics, 14:1186, Jun 2024. URL: https://doi.org/10.3390/diagnostics14111186, doi:10.3390/diagnostics14111186. This article has 27 citations.
-
(NCT05880121 chunk 1): Giuseppe A. Ramirez. Neuron-specific Humoral and Cellular Immune Correlates of Structural and Functional Brain Connectomics in Neuropsychiatric Lupus. IRCCS San Raffaele. 2023. ClinicalTrials.gov Identifier: NCT05880121
-
(NCT06226324 chunk 1): fMRI Study of Early Brain Injury in Systemic Lupus Erythematosus. The Affiliated Hospital of Inner Mongolia Medical University. 2023. ClinicalTrials.gov Identifier: NCT06226324