Neuropsychiatric Systemic Lupus Erythematosus
Neuropsychiatric systemic lupus erythematosus is the nervous-system manifestation spectrum of systemic lupus erythematosus. It includes central and peripheral nervous-system syndromes such as seizure, psychosis, cognitive dysfunction, cerebrovascular disease, acute confusional state, chorea, demyelinating syndromes, and peripheral neuropathy. Attribution is difficult: presentations may reflect lupus-driven inflammation, antiphospholipid-related thrombosis, both mechanisms, or non-SLE mimics such as infection, metabolic disease, medication effects, or primary psychiatric and neurologic disorders. No standalone MONDO or Orphanet disease term was found in the local ontology resources, so this entry is anchored to the parent systemic lupus erythematosus term while preserving the NPSLE preferred term.
Ask OpenScientist
Ask a research question about Neuropsychiatric Systemic Lupus Erythematosus. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Definitions
2- Seizure
- Psychosis
- Anxiety
- Cognitive impairment
- Delirium Acute confusional state in the ACR/EULAR NPSLE literature.
- Peripheral neuropathy
- CNS demyelination Maps the ACR demyelinating-syndrome category.
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Subtypes
2Show evidence (2 references)
Show evidence (2 references)
Discussions and Knowledge Gaps
1Show evidence (1 reference)
Pathophysiology
4Show evidence (5 references)
Show evidence (3 references)
Show evidence (2 references)
Show evidence (2 references)
Pathograph
- Target 'Ischemic Stroke' (from 'Antiphospholipid-Associated Neurovascular Thrombosis') not found in named elements
Phenotypes
11Cardiovascular 1
Show evidence (2 references)
Nervous System 10
Show evidence (3 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Genetic Associations
4Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Medical Actions
6Show evidence (2 references)
Show evidence (3 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (3 references)
Show evidence (2 references)
Biochemical Markers
7Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Source YAML
click to showname: Neuropsychiatric Systemic Lupus Erythematosus
creation_date: "2026-05-16T18:50:15Z"
updated_date: "2026-05-16T19:50:35Z"
category: Autoimmune
parents:
- Systemic Lupus Erythematosus
- Autoimmune Disease
- Neurological Disease
synonyms:
- Neuropsychiatric lupus
- NPSLE
- CNS lupus
- Lupus cerebritis
disease_term:
preferred_term: neuropsychiatric systemic lupus erythematosus
term:
id: MONDO:0007915
label: systemic lupus erythematosus
description: >-
Neuropsychiatric systemic lupus erythematosus is the nervous-system
manifestation spectrum of systemic lupus erythematosus. It includes central
and peripheral nervous-system syndromes such as seizure, psychosis, cognitive
dysfunction, cerebrovascular disease, acute confusional state, chorea,
demyelinating syndromes, and peripheral neuropathy. Attribution is difficult:
presentations may reflect lupus-driven inflammation, antiphospholipid-related
thrombosis, both mechanisms, or non-SLE mimics such as infection, metabolic
disease, medication effects, or primary psychiatric and neurologic disorders.
No standalone MONDO or Orphanet disease term was found in the local ontology
resources, so this entry is anchored to the parent systemic lupus
erythematosus term while preserving the NPSLE preferred term.
definitions:
- name: ACR 1999 neuropsychiatric lupus syndrome framework
definition_type: CASE_DEFINITION
description: >-
The American College of Rheumatology nomenclature provides standardized case
definitions and ascertainment guidance for 19 neuropsychiatric syndromes
seen in SLE, spanning central and peripheral nervous-system involvement.
scope: Patients with SLE and neurologic or psychiatric manifestations.
criteria_sets:
- name: Neuropsychiatric syndrome spectrum
description: >-
The case-definition framework requires syndrome-specific clinical
assessment, important exclusions, and appropriate ascertainment methods
rather than a single pathognomonic laboratory test.
core_clinical_characteristics:
- preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
- preferred_term: Psychosis
term:
id: HP:0000709
label: Psychosis
- preferred_term: Anxiety
term:
id: HP:0000739
label: Anxiety
- preferred_term: Cognitive impairment
term:
id: HP:0100543
label: Cognitive impairment
- preferred_term: Delirium
term:
id: HP:0031258
label: Delirium
description: Acute confusional state in the ACR/EULAR NPSLE literature.
- preferred_term: Peripheral neuropathy
term:
id: HP:0009830
label: Peripheral neuropathy
- preferred_term: CNS demyelination
term:
id: HP:0007305
label: CNS demyelination
description: Maps the ACR demyelinating-syndrome category.
evidence:
- reference: PMID:10211873
reference_title: The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes.
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Case definitions including diagnostic criteria, important exclusions,
and methods of ascertainment were developed for 19 NPSLE syndromes.
explanation: >-
This supports the syndrome-spectrum criteria set used to organize the
ACR neuropsychiatric lupus framework.
evidence:
- reference: PMID:10211873
reference_title: The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes.
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Case definitions including diagnostic criteria, important exclusions, and
methods of ascertainment were developed for 19 NPSLE syndromes.
explanation: >-
This is the landmark ACR nomenclature and case-definition framework for
NPSLE syndrome attribution and reporting.
- reference: PMID:10211873
reference_title: The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes.
supports: SUPPORT
evidence_source: OTHER
snippet: >-
The American College of Rheumatology (ACR) Nomenclature for NPSLE provides
case definitions for 19 neuropsychiatric syndromes seen in SLE, with
reporting standards and recommendations for laboratory and imaging tests.
explanation: >-
The conclusion supports the 19-syndrome framework and its use in clinical
research and specialist-supported diagnosis.
- name: Attribution and exclusion-based diagnosis
definition_type: DIAGNOSTIC_CRITERIA
description: >-
Suspected NPSLE is first evaluated like the same neurologic or psychiatric
syndrome in a patient without SLE. Attribution to lupus follows exclusion of
non-SLE causes and assessment for inflammatory, autoimmune, thrombotic, or
mixed mechanisms.
scope: Diagnostic workup of new neurologic or psychiatric events in patients with SLE.
criteria_sets:
- name: EULAR diagnostic workup
description: >-
Workup includes targeted studies such as CSF analysis, EEG,
neuropsychological testing, nerve-conduction studies, and MRI according to
the presenting syndrome.
minimum_required: 1
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
The diagnostic work-up of suspected NPSLE is comparable to that in
patients without SLE who present with the same manifestations, and aims
to exclude causes unrelated to SLE.
explanation: >-
EULAR explicitly frames diagnosis as syndrome-based evaluation and
exclusion of non-SLE causes.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Due to the lack of a gold standard, the attribution of NP symptoms to SLE
represents a clinical challenge that obligates the strict exclusion of any
other potential cause.
explanation: >-
The management review supports the attribution-and-exclusion diagnostic
framing used here.
has_subtypes:
- name: Inflammatory or autoimmune NPSLE
description: >-
NPSLE manifestations attributed primarily to lupus-driven inflammation or
autoimmunity, including optic neuritis, transverse myelitis, peripheral
neuropathy, refractory seizures, psychosis, and acute confusional state,
especially when generalized lupus activity is present.
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Glucocorticoids and immunosuppressive therapy are indicated when NPSLE is
thought to reflect an inflammatory process (optic neuritis, transverse
myelitis, peripheral neuropathy, refractory seizures, psychosis, ACS) and
in the presence of generalised lupus activity.
explanation: >-
EULAR distinguishes inflammatory-process NPSLE manifestations that warrant
glucocorticoids and immunosuppression.
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
High-dose glucocorticoids and intravenous cyclophosphamide remain the
cornerstone for patients with severe symptoms that are thought to reflect
inflammation or an underlying autoimmune process.
explanation: >-
This treatment distinction supports an inflammatory/autoimmune subtype
concept used in clinical decision-making.
- name: Antiphospholipid-associated thrombotic NPSLE
description: >-
Focal or vascular neuropsychiatric lupus manifestations driven by
antiphospholipid-antibody-associated thrombosis or ischemia, especially
cerebrovascular disease, seizures, and chorea.
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Strong risk factors (at least fivefold increased risk) are previous or
concurrent severe NPSLE (for cognitive dysfunction, seizures) and
antiphospholipid antibodies (for CVD, seizures, chorea).
explanation: >-
EULAR identifies antiphospholipid antibodies as strong risk factors for
vascular and selected neurologic NPSLE manifestations.
- reference: PMID:18537650
reference_title: Therapeutic approach to neuropsychiatric systemic lupus erythematosus.
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Focal CNS manifestations, particularly TIA and stroke, are associated with
the presence of antiphospholipid antibodies (aPL).
explanation: >-
This review supports a focal thrombotic/aPL-associated clinical subtype.
epidemiology:
- name: Neuropsychiatric event burden in an international SLE inception cohort
description: >-
In the SLICC inception cohort, any neuropsychiatric event was common, but
only a subset of events were attributed to SLE depending on attribution
model stringency.
evidence:
- reference: PMID:30375754
reference_title: "Psychosis in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
NP events (≥1) occurred in 951 of 1,826 patients (52.1%), and 488 of
1,826 patients (26.7%) had ≥2 events during the study period.
explanation: >-
The inception cohort quantifies neuropsychiatric events among SLE
patients, emphasizing the event burden that enters NPSLE attribution.
- reference: PMID:30375754
reference_title: "Psychosis in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The proportion of NP events attributed to SLE varied from 17.8%
(attribution model A) to 31.1% (attribution model B) and occurred in 13.3%
of patients (model A) to 21.1% of patients (model B).
explanation: >-
These data support the distinction between all NP events in SLE and events
attributed to SLE.
- name: EULAR frequency categories for major NPSLE manifestations
description: >-
EULAR summarizes cerebrovascular disease and seizures as common cumulative
manifestations, while severe cognitive dysfunction, major depression, acute
confusional state, peripheral nervous disorders, and psychosis are less
common.
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Common (cumulative incidence > 5%) manifestations include cerebrovascular
disease (CVD) and seizures; relatively uncommon (1-5%) are severe
cognitive dysfunction, major depression, acute confusional state (ACS),
peripheral nervous disorders psychosis.
explanation: >-
This provides frequency bands for the major NPSLE manifestations encoded
below.
pathophysiology:
- name: Autoimmune Neuroinflammation
description: >-
Systemic lupus autoimmunity can extend to the nervous system through
autoantibody production, immune-complex and complement activation,
type I interferon signaling, neutrophil extracellular trap (NET)
formation and release, cytokine-mediated inflammation, and
intrathecal immune activation, producing diffuse or focal neuropsychiatric
syndromes.
locations:
- preferred_term: brain
term:
id: UBERON:0000955
label: brain
- preferred_term: choroid plexus
modifier: ABNORMAL
term:
id: UBERON:0001886
label: choroid plexus
cell_types:
- preferred_term: B cell
term:
id: CL:0000236
label: B cell
- preferred_term: T cell
term:
id: CL:0000084
label: T cell
- preferred_term: neutrophil
term:
id: CL:0000775
label: neutrophil
- preferred_term: microglial cell
term:
id: CL:0000129
label: microglial cell
biological_processes:
- preferred_term: immunoglobulin production
term:
id: GO:0002377
label: immunoglobulin production
modifier: INCREASED
- preferred_term: neuroinflammatory response
term:
id: GO:0150076
label: neuroinflammatory response
modifier: INCREASED
- preferred_term: complement activation
term:
id: GO:0006956
label: complement activation
modifier: INCREASED
- preferred_term: type I interferon-mediated signaling pathway
term:
id: GO:0060337
label: type I interferon-mediated signaling pathway
modifier: INCREASED
- preferred_term: neutrophil extracellular trap formation
term:
id: GO:0140645
label: neutrophil extracellular trap formation
modifier: INCREASED
downstream:
- target: Blood-Brain Barrier Disruption
description: >-
Inflammatory mediators and complement can impair barrier integrity,
allowing neuropathic antibodies and soluble mediators to reach brain
parenchyma.
causal_link_type: DIRECT
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Among them, anti-endothelial cell antibodies, complement components,
cytokines and chemokines, and environmental mediators have an essential
role
explanation: >-
The review links inflammatory and complement mediators to BBB-integrity
modulation in NPSLE.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
In clinical practice, therapies are directed to a presumptive
pathophysiologic process (inflammatory, thrombotic, or both).
explanation: >-
The review supports inflammatory and thrombotic mechanism clusters as the
practical mechanistic framing for NPSLE.
- reference: PMID:41989680
reference_title: Pathogenesis and therapeutic strategies for neuropsychiatric lupus centered on innate immune activation.
supports: SUPPORT
evidence_source: OTHER
snippet: >-
aberrant activation of innate immunity by self-nucleic acids and
consequent overproduction of Type I interferons (IFN-I) constitute a
central pathogenic axis in NPSLE.
explanation: >-
This review supports type I interferon-driven innate immune activation as
a central inflammatory axis in NPSLE.
- reference: PMID:37369340
reference_title: Spatial enrichment of the type 1 interferon signature in the brain of a neuropsychiatric lupus murine model.
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: >-
interferon-stimulated genes (ISGs) were among the most highly upregulated
genes in both regions and that gene pathways involved in cellular
interaction and neuronal development were generally repressed among
astrocytes, oligodendrocytes, and neurons.
explanation: >-
The mouse spatial transcriptomics study supports CNS interferon signaling
as a mechanistic contributor to neuropsychiatric lupus phenotypes.
- reference: PMID:38531610
reference_title: Characterisation of choroid plexus-infiltrating T cells reveals novel therapeutic targets in murine neuropsychiatric lupus.
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: >-
Systemic blockade of VLA-4, the cognate ligand of VCAM, resulted in
significant resolution of the ChP immune cell infiltration and attenuation
of the depressive phenotype.
explanation: >-
This supports choroid-plexus immune-cell infiltration as a tractable
neuroimmune mechanism in murine NPSLE.
- reference: PMID:42337641
reference_title: "Immunopathogenesis of neuropsychiatric systemic lupus erythematosus: current insights into inflammatory and thrombotic pathways."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Current evidence supports two partially overlapping pathogenic pathways: an
autoimmune-inflammatory and a thrombo-ischemic pathway. These mechanisms
promote disruption of the blood-brain barrier, infiltration of immune cells
into the central nervous system, activation of microglia, and neuronal
dysfunction. Increasing evidence also highlights the role of neutrophil
extracellular traps, complement activation, type I interferon signaling,
and autoreactive lymphocytes in driving neuroinflammation.
explanation: >-
This recent review synthesizes current understanding of the dual
pathogenic pathways in NPSLE (autoimmune-inflammatory and
thrombo-ischemic) and their convergence on BBB disruption, immune
infiltration, and neuronal dysfunction, supporting the mechanistic
framework modeled here.
- name: Blood-Brain Barrier Disruption
description: >-
Disruption of the blood-brain barrier permits circulating neuropathic
autoantibodies, complement components, cytokines, and chemokines to enter
CNS tissue and interact with neurons, glia, and endothelial cells.
locations:
- preferred_term: blood brain barrier
modifier: ABNORMAL
term:
id: UBERON:0000120
label: blood brain barrier
cell_types:
- preferred_term: endothelial cell
term:
id: CL:0000115
label: endothelial cell
- preferred_term: astrocyte
term:
id: CL:0000127
label: astrocyte
biological_processes:
- preferred_term: maintenance of blood-brain barrier
modifier: DECREASED
term:
id: GO:0035633
label: maintenance of blood-brain barrier
- preferred_term: astrocyte activation
modifier: INCREASED
term:
id: GO:0048143
label: astrocyte activation
downstream:
- target: Anti-NMDA-NR2A/B Neuronal Excitotoxicity
description: >-
Barrier disruption can allow anti-NR2/glutamate-receptor antibodies to
access neuronal targets and alter synaptic signaling or neuronal survival.
causal_link_type: DIRECT
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
It has been proposed that a disruption of the integrity of the BBB may
have a potential pathogenic role in NPSLE since this may permit the
influx of neuropathic antibodies across the BBB.
explanation: >-
This supports the edge from BBB disruption to CNS entry of neuropathic
antibodies.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
The BBB is a network of endothelial cells and pericyte and astrocyte
projections that regulates the entry of soluble molecules and cells into
the brain parenchyma.
explanation: >-
The review defines the anatomical and cellular barrier interface relevant
to NPSLE.
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
It has been proposed that a disruption of the integrity of the BBB may
have a potential pathogenic role in NPSLE since this may permit the
influx of neuropathic antibodies across the BBB.
explanation: >-
This directly supports BBB disruption as a pathogenic step in NPSLE.
- reference: PMID:29846157
reference_title: Role of serum autoantibodies in blood brain barrier damages in neuropsychiatric systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
CONCLUSIONS: The data demonstrate that serum anti-Sm antibodies play a
most important role in the disruption of BBB in NPSLE.
explanation: >-
The patient serum/CSF study links anti-Sm autoantibodies to BBB
dysfunction as measured by Q albumin.
- name: Anti-NMDA-NR2A/B Neuronal Excitotoxicity
description: >-
A subset of SLE patients have anti-NMDA-NR2A/B glutamate-receptor
antibodies. When these antibodies reach CNS targets, they can alter NMDA
receptor signaling, injure neurons, and contribute to cognitive,
behavioral, mood, seizure, or psychiatric manifestations.
locations:
- preferred_term: brain
term:
id: UBERON:0000955
label: brain
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
biological_processes:
- preferred_term: glutamate receptor signaling pathway
modifier: ABNORMAL
term:
id: GO:0007215
label: glutamate receptor signaling pathway
- preferred_term: chemical synaptic transmission
modifier: ABNORMAL
term:
id: GO:0007268
label: chemical synaptic transmission
- preferred_term: positive regulation of calcium ion transport
modifier: INCREASED
term:
id: GO:0051928
label: positive regulation of calcium ion transport
evidence:
- reference: PMID:25081016
reference_title: "Glutamate receptor antibodies in neurological diseases: anti-AMPA-GluR3 antibodies, anti-NMDA-NR1 antibodies, anti-NMDA-NR2A/B antibodies, anti-mGluR1 antibodies or anti-mGluR5 antibodies are present in subpopulations of patients with either: epilepsy, encephalitis, cerebellar ataxia, systemic lupus erythematosus (SLE) and neuropsychiatric SLE, Sjogren's syndrome, schizophrenia, mania or stroke."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Some of the anti-NMDA-NR2A/B antibodies associate with
neuropsychiatric/cognitive/behavior/mood impairments in SLE patients,
while others do not.
explanation: >-
The review supports anti-NMDA-NR2A/B antibodies as a heterogeneous but
relevant autoantibody class in NPSLE.
- reference: PMID:25081016
reference_title: "Glutamate receptor antibodies in neurological diseases: anti-AMPA-GluR3 antibodies, anti-NMDA-NR1 antibodies, anti-NMDA-NR2A/B antibodies, anti-mGluR1 antibodies or anti-mGluR5 antibodies are present in subpopulations of patients with either: epilepsy, encephalitis, cerebellar ataxia, systemic lupus erythematosus (SLE) and neuropsychiatric SLE, Sjogren's syndrome, schizophrenia, mania or stroke."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
The anti-NMDA-NR2A/B antibodies can undoubtedly be very pathogenic, since
they can kill neurons by activating NMDA receptors and inducing
'Excitotoxicity', damage the brain
explanation: >-
This supports neuronal excitotoxicity as a downstream mechanism for a
subset of anti-NR2 antibody-positive disease.
- name: Antiphospholipid-Associated Neurovascular Thrombosis
description: >-
Antiphospholipid antibodies promote neurovascular risk through endothelial,
platelet, coagulation, and complement-related prothrombotic mechanisms,
producing ischemic or focal NPSLE manifestations such as cerebrovascular
disease, seizures, and chorea.
cell_types:
- preferred_term: endothelial cell
term:
id: CL:0000115
label: endothelial cell
- preferred_term: platelet
term:
id: CL:0000233
label: platelet
biological_processes:
- preferred_term: blood coagulation
modifier: INCREASED
term:
id: GO:0007596
label: blood coagulation
- preferred_term: platelet activation
modifier: INCREASED
term:
id: GO:0030168
label: platelet activation
- preferred_term: complement activation
modifier: INCREASED
term:
id: GO:0006956
label: complement activation
downstream:
- target: Ischemic Stroke
description: >-
Prothrombotic aPL-associated vascular injury can culminate in thrombotic
cerebrovascular disease.
causal_link_type: DIRECT
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Antiplatelet/anticoagulation therapy is indicated when manifestations
are related to antiphospholipid antibodies, particularly thrombotic CVD.
explanation: >-
The therapeutic recommendation supports the thrombotic/aPL mechanism
leading to cerebrovascular disease.
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Strong risk factors (at least fivefold increased risk) are previous or
concurrent severe NPSLE (for cognitive dysfunction, seizures) and
antiphospholipid antibodies (for CVD, seizures, chorea).
explanation: >-
This supports aPL-associated vascular and neurologic manifestations as a
distinct mechanistic cluster.
- reference: PMID:18240179
reference_title: A followup study of antiphospholipid antibodies and associated neuropsychiatric manifestations in 137 children with systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Our data suggest an association between LAC and cerebrovascular disease at
the time of SLE diagnosis and chorea over the disease course, but not
between aPL and other neuropsychiatric manifestations.
explanation: >-
The pediatric cohort supports lupus anticoagulant association with
cerebrovascular disease and chorea.
phenotypes:
- category: Neuropsychiatric
name: Cerebrovascular Disease
frequency: OCCASIONAL
description: >-
Focal vascular NPSLE includes thrombotic cerebrovascular disease and stroke,
particularly when antiphospholipid antibodies are present.
phenotype_term:
preferred_term: Ischemic stroke
term:
id: HP:0002140
label: Ischemic stroke
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Common (cumulative incidence > 5%) manifestations include cerebrovascular
disease (CVD) and seizures
explanation: >-
EULAR classifies cerebrovascular disease as a common cumulative NPSLE
manifestation.
- reference: PMID:34468807
reference_title: "An unexpected cause of chorea in an adolescent girl: systemic lupus erythematosus."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Central nervous system involvement defined as neuropsychiatric lupus
presents wide clinical findings varying from stroke and seizures to
psychosis and cognitive dysfunction.
explanation: >-
This case report review statement supports stroke as part of the NPSLE
phenotype spectrum.
- category: Neuropsychiatric
name: Seizure
frequency: OCCASIONAL
description: >-
Seizures are a recognized NPSLE manifestation and may be related to
inflammatory, thrombotic, vascular, or antibody-associated mechanisms.
phenotype_term:
preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Common (cumulative incidence > 5%) manifestations include cerebrovascular
disease (CVD) and seizures
explanation: >-
EULAR classifies seizures as a common cumulative NPSLE manifestation.
- reference: PMID:33626435
reference_title: "Seizures in systemic lupus erythematosus: A scoping review."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
The prevalence of explicit episodes of seizures among SLE patients, varies
from 2 to 8%.
explanation: >-
The scoping review provides an SLE-level seizure prevalence range.
- reference: ORPHA:536
reference_title: "Systemic lupus erythematosus (Orphanet structured-database record)"
supports: SUPPORT
evidence_source: OTHER
snippet: "HP:0001250 | Seizure | Occasional (29-5%)"
explanation: >-
Orphanet classifies seizure as an occasional phenotype in systemic lupus
erythematosus.
- category: Neuropsychiatric
name: Psychosis
frequency: VERY_RARE
description: >-
Lupus psychosis is an uncommon acute psychiatric NPSLE manifestation that is
attributed to SLE after exclusion of primary psychotic, substance-induced,
medication-related, and reactive psychiatric disorders.
phenotype_term:
preferred_term: Psychosis
term:
id: HP:0000709
label: Psychosis
evidence:
- reference: PMID:30375754
reference_title: "Psychosis in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Among 28 of 1,826 patients with psychosis (1.53%), 26 of 28 (93%) had a
single psychotic event, while 1 patient had 2 discrete events and 1
patient had 3 discrete events.
explanation: >-
The large international inception cohort supports psychosis as a rare
NPSLE event.
- reference: PMID:30375754
reference_title: "Psychosis in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Using a well‐defined process for determining attribution, we confirmed
that the majority of psychotic events were due to SLE.
explanation: >-
The cohort supports lupus attribution for most psychotic events under the
broader attribution model.
- category: Neuropsychiatric
name: Cognitive Impairment
description: >-
Cognitive dysfunction is part of the NPSLE spectrum, but severity and lupus
attribution vary across studies and require objective cognitive assessment
and exclusion of alternative contributors.
phenotype_term:
preferred_term: Cognitive impairment
term:
id: HP:0100543
label: Cognitive impairment
evidence:
- reference: PMID:10211873
reference_title: The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes.
supports: SUPPORT
evidence_source: OTHER
snippet: >-
A short neuropsychological test battery for the diagnosis of cognitive
deficits was proposed.
explanation: >-
The ACR case-definition paper supports formal neuropsychological
evaluation of NPSLE cognitive dysfunction.
- reference: PMID:38332909
reference_title: Serum S100A8/A9 and MMP-9 levels are elevated in systemic lupus erythematosus patients with cognitive impairment.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Of 290 patients, 40% (n=116) had CI."
explanation: >-
This large SLE cohort quantifies cognitive impairment and supports its
clinical relevance, though it is not itself an NPSLE-attribution study.
- category: Neuropsychiatric
name: Depression
frequency: OCCASIONAL
description: >-
Major depression and depressive symptoms may occur in SLE and are included
in the NPSLE syndrome framework after attribution and exclusion of common
non-SLE causes.
phenotype_term:
preferred_term: Depression
term:
id: HP:0000716
label: Depression
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
relatively uncommon (1-5%) are severe cognitive dysfunction, major
depression, acute confusional state (ACS), peripheral nervous disorders
psychosis.
explanation: >-
EULAR lists major depression among relatively uncommon NPSLE
manifestations.
- reference: ORPHA:536
reference_title: "Systemic lupus erythematosus (Orphanet structured-database record)"
supports: SUPPORT
evidence_source: OTHER
snippet: "HP:0000716 | Depression | Occasional (29-5%)"
explanation: Orphanet classifies depression as occasional in SLE.
- category: Neuropsychiatric
name: Anxiety Disorder
description: >-
Anxiety disorder is an ACR-defined diffuse psychiatric NPSLE syndrome and
requires attribution after exclusion of primary anxiety, medication-related,
metabolic, infectious, and reactive causes.
phenotype_term:
preferred_term: Anxiety
term:
id: HP:0000739
label: Anxiety
evidence:
- reference: PMID:10211873
reference_title: The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes.
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Case definitions including diagnostic criteria, important exclusions, and
methods of ascertainment were developed for 19 NPSLE syndromes.
explanation: >-
The ACR case-definition paper supports anxiety disorder as part of the
standardized diffuse psychiatric NPSLE syndrome framework.
- reference: PMID:29846157
reference_title: Role of serum autoantibodies in blood brain barrier damages in neuropsychiatric systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Q albumin was significantly higher in acute confusional state (ACS) than
in non-ACS diffuse NPSLE (anxiety disorder, cognitive dysfunction, mood
disorder and psychosis) or in focal NPSLE.
explanation: >-
The NPSLE patient cohort explicitly includes anxiety disorder within the
diffuse non-ACS NPSLE comparator group.
- category: Neuropsychiatric
name: Headache
description: >-
Headache is part of the ACR NPSLE syndrome list, but isolated headache is a
common general-population symptom and requires careful attribution.
phenotype_term:
preferred_term: Headache
term:
id: HP:0002315
label: Headache
evidence:
- reference: PMID:18481154
reference_title: Association of anti-ribosomal P protein antibodies with neuropsychiatric and other manifestations of systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Depression (59.4%), headache (46.9%) and cognitive dysfunction (37.5%)
were the commonest NPSLE syndromes.
explanation: >-
This SLE cohort using ACR NPSLE definitions supports headache as a common
NPSLE-classified syndrome in that cohort.
- category: Neuropsychiatric
name: Chorea
frequency: VERY_RARE
description: >-
Chorea is a rare movement-disorder manifestation of NPSLE and is associated
with antiphospholipid antibodies in pediatric and broader NPSLE literature.
phenotype_term:
preferred_term: Chorea
term:
id: HP:0002072
label: Chorea
evidence:
- reference: ORPHA:536
reference_title: "Systemic lupus erythematosus (Orphanet structured-database record)"
supports: SUPPORT
evidence_source: OTHER
snippet: "HP:0002072 | Chorea | Very rare (<4-1%)"
explanation: Orphanet classifies chorea as very rare in SLE.
- reference: PMID:18240179
reference_title: A followup study of antiphospholipid antibodies and associated neuropsychiatric manifestations in 137 children with systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Comparison for specific neuropsychiatric manifestations showed a
statistically significant association between a persistently positive LAC
and chorea (2 patients; P = 0.02).
explanation: >-
The pediatric cohort supports an association between persistent lupus
anticoagulant positivity and chorea.
- category: Neuropsychiatric
name: Acute Confusional State
frequency: VERY_RARE
description: >-
Acute confusional state is a severe diffuse NPSLE manifestation and overlaps
clinically with delirium or encephalopathy.
phenotype_term:
preferred_term: Delirium
term:
id: HP:0031258
label: Delirium
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
relatively uncommon (1-5%) are severe cognitive dysfunction, major
depression, acute confusional state (ACS), peripheral nervous disorders
psychosis.
explanation: >-
EULAR lists acute confusional state among relatively uncommon NPSLE
manifestations.
- category: Neuropsychiatric
name: Peripheral Neuropathy
description: >-
Peripheral nervous-system disorders are included within NPSLE and may be
inflammatory, immune-mediated, or attributable to non-SLE mimics depending
on clinical context and testing.
phenotype_term:
preferred_term: Peripheral neuropathy
term:
id: HP:0009830
label: Peripheral neuropathy
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Investigations include cerebrospinal fluid analysis (to exclude central
nervous system infection), EEG (to diagnose seizure disorder),
neuropsychological tests (to assess cognitive dysfunction), nerve
conduction studies (for peripheral neuropathy) and MRI
explanation: >-
EULAR specifically includes peripheral neuropathy in NPSLE workup and
recommends nerve-conduction studies when indicated.
- category: Neuropsychiatric
name: Demyelinating Syndrome or Myelopathy
description: >-
Demyelinating syndromes, optic neuritis, and transverse myelitis are severe
inflammatory NPSLE presentations and enter the differential against other
inflammatory demyelinating diseases.
phenotype_term:
preferred_term: CNS demyelination
term:
id: HP:0007305
label: CNS demyelination
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Glucocorticoids and immunosuppressive therapy are indicated when NPSLE is
thought to reflect an inflammatory process (optic neuritis, transverse
myelitis, peripheral neuropathy, refractory seizures, psychosis, ACS) and
in the presence of generalised lupus activity.
explanation: >-
EULAR identifies optic neuritis and transverse myelitis as inflammatory
NPSLE manifestations.
biochemical:
- name: Antiphospholipid antibodies
presence: Positive in subset
context: Serum or plasma; includes lupus anticoagulant, anticardiolipin, and anti-beta2 glycoprotein I antibodies.
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Strong risk factors (at least fivefold increased risk) are previous or
concurrent severe NPSLE (for cognitive dysfunction, seizures) and
antiphospholipid antibodies (for CVD, seizures, chorea).
explanation: >-
EULAR supports aPL as biomarkers and risk factors for selected NPSLE
manifestations.
- reference: PMID:18240179
reference_title: A followup study of antiphospholipid antibodies and associated neuropsychiatric manifestations in 137 children with systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
At the time of diagnosis, 65% of the children were aCL positive, 41% had
anti-beta(2)GPI antibodies, and 26% were LAC positive.
explanation: >-
The pediatric SLE cohort quantifies antiphospholipid antibody positivity.
- name: Anti-NMDA-NR2A/B antibodies
presence: Positive in subset
context: Serum and/or cerebrospinal fluid.
evidence:
- reference: PMID:25081016
reference_title: "Glutamate receptor antibodies in neurological diseases: anti-AMPA-GluR3 antibodies, anti-NMDA-NR1 antibodies, anti-NMDA-NR2A/B antibodies, anti-mGluR1 antibodies or anti-mGluR5 antibodies are present in subpopulations of patients with either: epilepsy, encephalitis, cerebellar ataxia, systemic lupus erythematosus (SLE) and neuropsychiatric SLE, Sjogren's syndrome, schizophrenia, mania or stroke."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
The exact percentage of SLE patients having anti-NMDA-NR2A/B antibodies
varies in different studies from 14 to 35%, and in one study such
antibodies were found in 81% of patients with diffuse 'Neuropshychiatric
SLE', and in 44% of patients with focal 'Neuropshychiatric SLE'.
explanation: >-
The review supports anti-NMDA-NR2A/B antibodies as a subset biomarker in
SLE and NPSLE.
- reference: PMID:25081016
reference_title: "Glutamate receptor antibodies in neurological diseases: anti-AMPA-GluR3 antibodies, anti-NMDA-NR1 antibodies, anti-NMDA-NR2A/B antibodies, anti-mGluR1 antibodies or anti-mGluR5 antibodies are present in subpopulations of patients with either: epilepsy, encephalitis, cerebellar ataxia, systemic lupus erythematosus (SLE) and neuropsychiatric SLE, Sjogren's syndrome, schizophrenia, mania or stroke."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
In some patients, the anti-NMDA-NR2A/B antibodies are present in both the
serum and the CSF.
explanation: >-
This supports serum and CSF as relevant testing compartments.
- name: Anti-Sm autoantibodies and BBB damage
presence: Elevated in acute confusional state subset
context: Serum; associated with Q albumin evidence of BBB dysfunction.
evidence:
- reference: PMID:29846157
reference_title: Role of serum autoantibodies in blood brain barrier damages in neuropsychiatric systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Anti-Sm, but not anti-NR2, anti-P or anticardiolipin, was significantly
elevated in ACS compared with the other 2 groups of NPSLE
explanation: >-
The serum/CSF patient study supports anti-Sm elevation in the acute
confusional state NPSLE subset.
- reference: PMID:29846157
reference_title: Role of serum autoantibodies in blood brain barrier damages in neuropsychiatric systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Multiple regression analysis confirmed the significant contribution of
anti-Sm (p=0.0040), but not anti-NR2 (p=0.5023), anti-P (p=0.2651), or
anti-cardiolipin (p=0.6769) in the elevation of Q albumin.
explanation: >-
The adjusted analysis links anti-Sm, rather than several other measured
autoantibodies, to the Q albumin BBB-dysfunction marker.
- name: Anti-ribosomal P antibodies
presence: Positive in subset
context: Serum; associated most strongly with psychiatric manifestations in some cohorts.
evidence:
- reference: PMID:18481154
reference_title: Association of anti-ribosomal P protein antibodies with neuropsychiatric and other manifestations of systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
aRP was positive in seven (21.9%) patients, all of whom had one or more
NPSLE syndromes.
explanation: >-
This cohort supports anti-ribosomal P antibody positivity in a subset of
NPSLE-classified patients.
- reference: PMID:18481154
reference_title: Association of anti-ribosomal P protein antibodies with neuropsychiatric and other manifestations of systemic lupus erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The presence of aRP antibodies positively predicts patients with
psychiatric manifestations in general and mood disorders in particular,
for which aRP is specific, but not sensitive.
explanation: >-
The cohort supports anti-ribosomal P as a psychiatric-manifestation
biomarker with limited sensitivity.
- name: Serum S100A8/A9 and MMP-9
presence: Elevated with cognitive impairment
context: Serum.
evidence:
- reference: PMID:38332909
reference_title: Serum S100A8/A9 and MMP-9 levels are elevated in systemic lupus erythematosus patients with cognitive impairment.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Serum levels of S100A8/A9 and MMP-9, were significantly higher in
patients with CI (p=0.006 and p=0.036, respectively).
explanation: >-
The 290-patient SLE cohort supports S100A8/A9 and MMP-9 elevation with
cognitive impairment.
- reference: PMID:38332909
reference_title: Serum S100A8/A9 and MMP-9 levels are elevated in systemic lupus erythematosus patients with cognitive impairment.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
S100A8/A9 had the greatest discriminatory ability in differentiating
between patients with and without CI.
explanation: >-
This supports S100A8/A9 as a candidate cognitive-impairment biomarker in
SLE.
- name: Blood neurofilament light and glial fibrillary acidic protein
presence: Elevated in active major NPSLE
context: Blood, serum, or plasma.
evidence:
- reference: DOI:10.1177/09612033241272961
reference_title: Blood-based biomarkers of neuronal and glial injury in active major neuropsychiatric systemic lupus erythematosus
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Blood NfL and GFAP levels are elevated in persons with SLE with active
major NPSLE compared to disease matched controls and may lower after
immunotherapy initiation.
explanation: >-
The case-control study supports blood NfL and GFAP as candidate
neuronal/glial injury biomarkers in active major NPSLE.
- name: CSF interferon-alpha and neopterin
presence: Elevated in active juvenile CNS NPSLE
context: Cerebrospinal fluid.
evidence:
- reference: DOI:10.1007/s10875-022-01407-1
reference_title: "Juvenile Neuropsychiatric Systemic Lupus Erythematosus: Identification of Novel Central Neuroinflammation Biomarkers"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
CSF IFN-α and neopterin constitute promising biomarkers useful in the
diagnosis and monitoring of activity in j-NPSLE.
explanation: >-
The pediatric cohort supports CSF interferon-alpha and neopterin as
candidate activity biomarkers for juvenile NPSLE.
genetic:
- name: TNFAIP3 rs5029939 susceptibility association
gene_term:
preferred_term: TNFAIP3
term:
id: hgnc:11896
label: TNFAIP3
association: Susceptibility polymorphism associated with SLE and neuropsychiatric manifestations
relationship_type: SUSCEPTIBILITY
variant_origin: GERMLINE
features: >-
TNFAIP3 encodes A20, a negative regulator of NF-kB signaling. The
rs5029939 CG genotype was associated with SLE susceptibility and with
neuropsychiatric manifestations in one case-control cohort.
evidence:
- reference: PMID:35382378
reference_title: "Association of <em>TNFAIP3</em> gene polymorphism (<em>rs5029939</em>) with susceptibility and clinical phenotype of systemic lupus erythematosus."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Genotype CG was significantly associated with lupus nephritis and
neuropsychiatric manifestations (p<0.05).
explanation: >-
This human case-control study directly links TNFAIP3 rs5029939 genotype
to neuropsychiatric manifestations among SLE patients.
- name: Pediatric NPSLE immune susceptibility loci
association: Polygenic susceptibility loci in childhood-onset lupus nephritis with NPSLE
relationship_type: SUSCEPTIBILITY
variant_origin: GERMLINE
features: >-
IL17RA rs2895332, IL23R rs10889677, and FCGR3A rs396991 were associated
with NPSLE risk in pediatric patients with lupus nephritis, supporting an
immune-pathway susceptibility component rather than a monogenic cause.
evidence:
- reference: PMID:39904110
reference_title: IL-17A, IL-23R, FCGR3A are associated with neuropsychiatric systemic lupus erythematosus susceptibility in pediatric patients with lupus nephritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
CONCLUSION: Our findings indicate that the polymorphisms IL17RA
rs2895332, IL23R rs10889677, and FCGR3A rs396991 are significantly
associated with the risk of NPSLE in childhood-onset LN.
explanation: >-
The pediatric lupus-nephritis cohort directly supports these immune
pathway polymorphisms as NPSLE susceptibility loci.
- name: IRF5 and cytokine polymorphism susceptibility
association: Cytokine and interferon regulatory polymorphisms associated with SLE susceptibility and neuropsychiatric impairment
relationship_type: SUSCEPTIBILITY
variant_origin: GERMLINE
features: >-
IRF5 and cytokine-gene polymorphisms contribute to SLE susceptibility in
cohort studies; TNF-alpha -238 G/A was associated with neuropsychiatric
impairment in an Algerian SLE cohort.
evidence:
- reference: PMID:41039983
reference_title: Cytokine and IRF5 Gene Polymorphisms Associated With Susceptibility and Organ Damage in Systemic Lupus Erythematosus.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Also, the A allele of the TNFα -238 G/A polymorphism was associated
with neuropsychiatric impairment (p = 0.036)
explanation: >-
This cohort links a cytokine-gene polymorphism to neuropsychiatric
impairment and supports IRF5/cytokine-gene susceptibility framing.
- name: Broader SLE polygenic risk background
association: MHC, HLA class II, STAT4, and IRF5 susceptibility background
relationship_type: SUSCEPTIBILITY
variant_origin: GERMLINE
features: >-
NPSLE occurs on the broader polygenic SLE susceptibility background. MHC/HLA
class II, STAT4, and IRF5 variants are reported risk or progression loci,
with narrative-review evidence linking genetic factors to renal and
neuropsychiatric clinical outcomes.
evidence:
- reference: PMID:42123548
reference_title: "Genetic Polymorphisms in Systemic Lupus Erythematosus and Their Clinical Implications: A Narrative Review."
supports: PARTIAL
evidence_source: OTHER
snippet: >-
Genetic variants in STAT4 and IRF5 exacerbate disease progression by
facilitating chronic inflammation. These genetic factors are associated
with various clinical outcomes, including renal and neuropsychiatric
symptoms.
explanation: >-
This review supports broader SLE genetic susceptibility context for
neuropsychiatric outcomes, but it does not establish a monogenic NPSLE
cause.
diagnosis:
- name: Syndrome-specific exclusion workup
description: >-
NPSLE diagnosis requires a syndrome-specific workup similar to that used in
non-SLE patients, with exclusion of infection, metabolic disease, drug
effects, primary psychiatric disease, and other neurologic mimics before
lupus attribution.
diagnosis_term:
preferred_term: diagnostic procedure
term:
id: MAXO:0000003
label: diagnostic procedure
results: >-
Workup supports a neurologic or psychiatric syndrome and excludes non-SLE
causes before attribution to inflammatory, thrombotic, or mixed NPSLE.
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
The diagnostic work-up of suspected NPSLE is comparable to that in
patients without SLE who present with the same manifestations, and aims to
exclude causes unrelated to SLE.
explanation: >-
This is the core EULAR diagnostic principle for suspected NPSLE.
- name: Neurodiagnostic testing
description: >-
CSF analysis, EEG, neuropsychological testing, nerve-conduction studies, and
MRI are selected according to the presenting manifestation.
diagnosis_term:
preferred_term: diagnostic procedure
term:
id: MAXO:0000003
label: diagnostic procedure
results: >-
CSF excludes infection or supports inflammation; EEG evaluates seizure
disorder; neuropsychological tests characterize cognitive dysfunction; nerve
conduction supports peripheral neuropathy; MRI evaluates vascular,
inflammatory, demyelinating, or structural mimics.
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Investigations include cerebrospinal fluid analysis (to exclude central
nervous system infection), EEG (to diagnose seizure disorder),
neuropsychological tests (to assess cognitive dysfunction), nerve
conduction studies (for peripheral neuropathy) and MRI
explanation: >-
EULAR lists the major neurodiagnostic tests and their syndrome-specific
roles.
- name: Autoantibody and inflammatory biomarker assessment
description: >-
Serologic and CSF testing may include antiphospholipid antibodies,
anti-ribosomal P antibodies, anti-NMDA-NR2 antibodies, complement and SLE
activity markers, and emerging neuroinflammatory or injury biomarkers.
diagnosis_term:
preferred_term: serology testing
term:
id: MAXO:0000609
label: serology testing
results: >-
Antiphospholipid antibodies support thrombotic attribution; anti-ribosomal P
or anti-NMDA-NR2 antibodies may support selected psychiatric or cognitive
endophenotypes but are not standalone diagnostic tests.
evidence:
- reference: PMID:30375754
reference_title: "Psychosis in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Plasma lupus anticoagulant, serum IgG anticardiolipin,
anti–β2‐glycoprotein I, anti–ribosomal P (anti‐P), and anti–NR2 glutamate
receptor antibodies were measured at the Oklahoma Medical Research
Foundation
explanation: >-
The SLICC psychosis cohort demonstrates the relevant autoantibody panel
used in NPSLE attribution research.
treatments:
- name: Hydroxychloroquine Background Therapy and Seizure Risk Reduction
description: >-
Hydroxychloroquine is recommended as background therapy for lupus patients
when not contraindicated and cohort data suggest antimalarial exposure may
reduce seizure risk, a key neuropsychiatric lupus manifestation.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: hydroxychloroquine
term:
id: CHEBI:5801
label: hydroxychloroquine
target_phenotypes:
- preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
evidence:
- reference: PMID:37827694
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus: 2023 update."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
HCQ is recommended for all patients with lupus at a target dose 5 mg/kg
real body weight/day, considering the individual's risk for flares and
retinal toxicity.
explanation: >-
Current EULAR SLE management recommendations support hydroxychloroquine
as background lupus therapy.
- reference: PMID:17875548
reference_title: "Seizures in patients with systemic lupus erythematosus: data from LUMINA, a multiethnic cohort (LUMINA LIV)."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
hydroxychloroquine use (HR = 0.35, 95% CI 0.15 to 0.80, p = 0.0131) were
independent predictors of a longer time-to-seizure occurrence.
explanation: >-
The LUMINA cohort supports a protective association between
hydroxychloroquine exposure and delayed seizure occurrence in SLE.
- name: Glucocorticoid and Cyclophosphamide Therapy for Severe Inflammatory NPSLE
description: >-
High-dose glucocorticoids, often with intravenous cyclophosphamide for
severe or refractory inflammatory/autoimmune presentations, are used when
NPSLE is attributed to lupus inflammation rather than thrombotic disease.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: corticosteroid
term:
id: CHEBI:50858
label: corticosteroid
- preferred_term: cyclophosphamide
term:
id: CHEBI:4027
label: cyclophosphamide
target_mechanisms:
- target: Autoimmune Neuroinflammation
treatment_effect: INHIBITS
description: >-
Glucocorticoids and cytotoxic immunosuppression suppress inflammatory
cytokine, lymphocyte, and autoantibody-driven neuroimmune activity.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
High-dose glucocorticoids and intravenous cyclophosphamide remain the
cornerstone for patients with severe symptoms that are thought to
reflect inflammation or an underlying autoimmune process.
explanation: >-
The source links this treatment target to inflammatory or autoimmune
NPSLE mechanisms.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
High-dose glucocorticoids and intravenous cyclophosphamide remain the
cornerstone for patients with severe symptoms that are thought to reflect
inflammation or an underlying autoimmune process.
explanation: >-
The review supports glucocorticoids plus cyclophosphamide for severe
inflammatory NPSLE.
- reference: PMID:18537650
reference_title: Therapeutic approach to neuropsychiatric systemic lupus erythematosus.
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Severe diffuse CNS manifestations, such as acute confusional state,
generalised seizures, mood disorders and psychosis, generally require
corticosteroids in the first instance.
explanation: >-
This review supports corticosteroids for severe diffuse CNS
manifestations.
- reference: PMID:18537650
reference_title: Therapeutic approach to neuropsychiatric systemic lupus erythematosus.
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Pulse intravenous cyclophosphamide therapy may help when more severe
manifestations are refractory to corticosteroids and other
immunosuppressive agents
explanation: >-
This supports cyclophosphamide escalation for refractory severe NPSLE.
- name: Antithrombotic Therapy for Antiphospholipid-Associated NPSLE
description: >-
Antiplatelet or anticoagulant therapy is used when neuropsychiatric
manifestations are attributed to antiphospholipid-antibody-associated
thrombosis, especially thrombotic cerebrovascular disease.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: aspirin
term:
id: CHEBI:15365
label: acetylsalicylic acid
- preferred_term: warfarin
term:
id: CHEBI:10033
label: warfarin
- preferred_term: heparin
term:
id: CHEBI:28304
label: heparin
target_mechanisms:
- target: Antiphospholipid-Associated Neurovascular Thrombosis
treatment_effect: INHIBITS
description: >-
Antiplatelet and anticoagulant strategies reduce thrombus formation or
recurrence in aPL-associated vascular NPSLE.
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Antiplatelet/anticoagulation therapy is indicated when manifestations
are related to antiphospholipid antibodies, particularly thrombotic CVD.
explanation: >-
EULAR directly links antithrombotic treatment to antiphospholipid
antibody-associated thrombotic cerebrovascular NPSLE.
target_phenotypes:
- preferred_term: Ischemic stroke
term:
id: HP:0002140
label: Ischemic stroke
evidence:
- reference: PMID:20724309
reference_title: "EULAR recommendations for the management of systemic lupus erythematosus with neuropsychiatric manifestations: report of a task force of the EULAR standing committee for clinical affairs."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Antiplatelet/anticoagulation therapy is indicated when manifestations are
related to antiphospholipid antibodies, particularly thrombotic CVD.
explanation: >-
EULAR supports antithrombotic therapy when NPSLE is aPL/thrombotic.
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
When symptoms are thought to reflect a thrombotic underlying process,
anticoagulation and antiplatelet agents are the mainstay of therapy,
especially if antiphospholipid antibodies or antiphospholipid syndrome are
present.
explanation: >-
The management review supports mechanism-guided antithrombotic therapy.
- name: Steroid-Sparing Maintenance Immunosuppression
description: >-
Azathioprine or mycophenolate may be considered for mild to moderate
inflammatory presentations or maintenance therapy after acute control,
depending on the syndrome and overall SLE activity.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: azathioprine
term:
id: CHEBI:2948
label: azathioprine
- preferred_term: mycophenolate mofetil
term:
id: CHEBI:8764
label: mycophenolate mofetil
target_mechanisms:
- target: Autoimmune Neuroinflammation
treatment_effect: INHIBITS
description: >-
Steroid-sparing immunosuppressants reduce ongoing lymphocyte activation
and immune-mediated inflammation.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
When patients present with mild to moderate NP manifestations, or when
maintenance therapy is warranted, azathioprine and mycophenolate may be
considered.
explanation: >-
The source supports maintenance or mild-to-moderate immunosuppression
for inflammatory NPSLE contexts.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
When patients present with mild to moderate NP manifestations, or when
maintenance therapy is warranted, azathioprine and mycophenolate may be
considered.
explanation: >-
The review supports azathioprine and mycophenolate for selected
mild/moderate or maintenance contexts.
- name: Refractory NPSLE Escalation
description: >-
Rituximab, intravenous immunoglobulin, or plasmapheresis may be used in
severe inflammatory NPSLE when response to initial glucocorticoid and
cyclophosphamide-based treatment is inadequate.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: rituximab
term:
id: NCIT:C1702
label: Rituximab
- preferred_term: human immunoglobulin G
term:
id: NCIT:C80829
label: Human Immunoglobulin G
target_mechanisms:
- target: Autoimmune Neuroinflammation
treatment_effect: MODULATES
description: >-
B-cell depletion, immune modulation, and antibody removal can be used when
severe antibody- or inflammation-mediated NPSLE is refractory.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Rituximab, intravenous immunoglobulins, or plasmapheresis may be used if
response is not achieved.
explanation: >-
The source supports escalation to immune-targeted therapy when initial
inflammatory NPSLE treatment response is inadequate.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Rituximab, intravenous immunoglobulins, or plasmapheresis may be used if
response is not achieved.
explanation: >-
The review supports rituximab, IVIG, or plasmapheresis as escalation
options when response is inadequate.
- reference: PMID:18537650
reference_title: Therapeutic approach to neuropsychiatric systemic lupus erythematosus.
supports: PARTIAL
evidence_source: OTHER
snippet: >-
Intravenous immunoglobulins, mycophenolate mofetil, rituximab, intratecal
methotrexate and dexametasone deserve further studies to confirm their
usefulness in the treatment of neuropsychiatric SLE.
explanation: >-
This older review identifies IVIG, mycophenolate, and rituximab as
plausible options while emphasizing limited evidence.
- reference: PMID:42115580
reference_title: "Long-term clinical outcomes and safety of rituximab in refractory neuropsychiatric systemic lupus erythematosus: a real-world single-center study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Sixteen of 17 patients (94.1%) achieved significant clinical improvement,
while one patient showed partial improvement with reduced seizure
frequency.
explanation: >-
This refractory NPSLE cohort provides direct clinical support for
rituximab as an escalation option, while infection risk still requires
monitoring.
- name: Symptomatic Neuropsychiatric Management
description: >-
Syndrome-directed treatment such as antipsychotics, antiseizure therapy,
antidepressants, and supportive neurologic or psychiatric care is used
alongside mechanism-directed immunosuppression or antithrombotic therapy.
treatment_term:
preferred_term: supportive care
term:
id: MAXO:0000950
label: supportive care
target_phenotypes:
- preferred_term: Psychosis
term:
id: HP:0000709
label: Psychosis
- preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
- preferred_term: Depression
term:
id: HP:0000716
label: Depression
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
In the acute setting, management of these patients does not differ from
other non-SLE subjects presenting with the same NP manifestation.
explanation: >-
This supports standard syndrome-directed acute care before and alongside
lupus-specific attribution.
- reference: PMID:30375754
reference_title: "Psychosis in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The following therapies were used during the time of the first psychotic
events: corticosteroids in 23 of 28 patients (82.1%)
explanation: >-
The psychosis cohort documents combined immunosuppressive and symptomatic
psychiatric treatments in real-world lupus psychosis.
discussions:
- discussion_id: npsle_mechanistic_interplay_heterogeneous_phenotypes
prompt: >-
How do the autoimmune-inflammatory and thrombo-ischemic pathways in NPSLE
interplay to produce heterogeneous neuropsychiatric manifestations (cognitive
impairment, mood disturbance, psychosis, seizures)? The current model captures
both pathways—neuroinflammatory (complement, type I IFN, BBB disruption, NMDA
excitotoxicity) and thrombotic (aPL, neurovascular prothrombotic mechanisms)—but
their relative contributions to specific phenotypes and mechanistic convergence
points remain incompletely characterized. Additionally, do non-stroke vascular-injury
mechanisms (e.g., endothelial dysfunction, microvasculature inflammation) contribute
broadly to psychiatric/cognitive symptoms independently of frank cerebrovascular accident?
kind: KNOWLEDGE_GAP
status: OPEN
attaches_to:
- pathophysiology#Autoimmune Neuroinflammation
- pathophysiology#Antiphospholipid-Associated Neurovascular Thrombosis
rationale: >-
NPSLE is mechanistically heterogeneous with two partially overlapping pathogenic
pathways. Current evidence emphasizes the interplay but does not dissect how each
pathway preferentially drives specific manifestations. Clarifying these links would
enable more precise mechanistic subtyping, improve prognosis prediction, and inform
targeted therapeutic strategies (e.g., immunosuppression vs. anticoagulation vs.
combined approaches) tailored to the underlying mechanism(s) in individual patients.
proposed_experiments:
- experiment_id: npsle_mechanism_phenotype_cohort
name: Neuroimaging-CSF stratification cohort for mechanism-phenotype mapping
description: >-
Stratify NPSLE patients by serological markers (anti-NR2, aPL, complement levels,
type I IFN signature) and neuropsychiatric phenotype (cognitive vs. mood vs. psychotic),
correlating to imaging biomarkers (BBB integrity, white-matter injury, microglial
activation) and CSF cytokine/chemokine profiles to map pathway-to-phenotype associations.
- experiment_id: npsle_biomarker_prediction_study
name: Serial plasma biomarker prediction of incident psychiatric manifestations
description: >-
Longitudinal plasma biomarker studies (neurofilament, phospho-tau, endothelial markers,
complement activation, type I IFN score) in NPSLE cohorts prospectively monitored for
incident psychiatric/cognitive episodes to test whether biomarker patterns predict
phenotype or pathway dominance.
evidence:
- reference: PMID:42337641
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Its pathogenesis remains incompletely understood and reflects the interplay among
systemic immune dysregulation, vascular injury, blood-brain and blood-CSF barrier
dysfunction, and local neuroinflammatory processes.Current evidence supports two
partially overlapping pathogenic pathways: an autoimmune-inflammatory and a
thrombo-ischemic pathway.
explanation: >-
The recent review emphasizes the dual pathway model and the uncertainty about their
interplay and relative contribution to heterogeneous NPSLE manifestations.
progression:
- phase: Early lupus psychosis timing
notes: >-
Lupus psychosis tends to occur early around SLE diagnosis in the SLICC
inception cohort, although it remains uncommon.
evidence:
- reference: PMID:30375754
reference_title: "Psychosis in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
there was a tendency for psychosis to occur early in the disease course,
usually within the first 3 years following the diagnosis of SLE.
explanation: >-
The cohort supports early timing of SLE-attributed psychosis relative to
SLE diagnosis.
- phase: Treatment-associated resolution of lupus psychosis
notes: >-
Most lupus psychosis events resolved or improved over follow-up in the SLICC
cohort, supporting reversibility for many patients after recognition and
treatment.
evidence:
- reference: PMID:30375754
reference_title: "Psychosis in Systemic Lupus Erythematosus: Results From an International Inception Cohort Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
More than 80% of the psychotic events had resolved by the second annual
assessment following onset of the event
explanation: >-
This supports favorable resolution of most lupus psychosis events over
two annual assessments.
- phase: Twelve-month treatment response after first NP event
notes: >-
In a 2024 international multicenter cohort of first neuropsychiatric events,
SLE attribution by clinical judgment combined with immunosuppressant
treatment was associated with better 12-month outcomes.
evidence:
- reference: DOI:10.1093/rheumatology/keae119
reference_title: "Therapeutic strategies and outcomes in neuropsychiatric systemic lupus erythematosus: an international multicentre retrospective study"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
NP manifestations attributed to SLE by clinical judgment and treated with
immunosuppressants demonstrated improved 12-month outcomes.
explanation: >-
This multicenter retrospective cohort supports timely attribution and
immunosuppressive therapy for SLE-attributed NPSLE events.
- phase: Syndrome-dependent course and attribution uncertainty
notes: >-
NPSLE course and prognosis depend strongly on syndrome, mechanism, and
attribution confidence; neuropsychiatric events may be inflammatory,
thrombotic, mixed, or unrelated to SLE.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
A strict differential diagnosis and individualization of treatment,
depending on the neuropsychiatric presentation and severity of symptoms,
are crucial in neuropsychiatric systemic lupus erythematosus (NPSLE).
explanation: >-
This supports prognosis and management being syndrome- and
mechanism-dependent rather than uniform across all NPSLE.
animal_models:
- species: Mouse
genotype: MRL/lpr lupus-prone strain
description: >-
MRL/lpr mice are used as a lupus-prone model for CNS lupus mechanisms,
including blood-brain barrier disruption, TWEAK/Fn14 signaling, complement
pathway involvement, and cognitive or depression-like phenotypes.
evidence:
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Studies in MRL/lpr mice, accurately reflecting human NPSLE, have shown the
importance of TWEAK, a pro-inflammatory cytokine member of the TNF
superfamily, and the alternative complement cascade in BBB disruption.
explanation: >-
The review supports MRL/lpr mice as a model for BBB and complement/cytokine
mechanisms in NPSLE.
- reference: PMID:26809245
reference_title: "Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives."
supports: SUPPORT
evidence_source: OTHER
snippet: >-
Furthermore, in a murine knockout model for its receptor Fn14, mice were
found to improve in cognitive function and to have less depression and
anhedonia
explanation: >-
The TWEAK receptor knockout observation supports model-system relevance to
cognitive and mood-like NPSLE phenotypes.
datasets: []
references:
- reference: DOI:10.1007/s10875-022-01407-1
title: "Juvenile Neuropsychiatric Systemic Lupus Erythematosus: Identification of Novel Central Neuroinflammation Biomarkers"
found_in:
- Neuropsychiatric_SLE-deep-research-falcon.md
findings: []
- reference: DOI:10.1016/j.berh.2005.04.003
title: Management of neuropsychiatric lupus
found_in:
- Neuropsychiatric_SLE-deep-research-falcon.md
findings: []
- reference: DOI:10.1093/rheumatology/keae119
title: "Therapeutic strategies and outcomes in neuropsychiatric systemic lupus erythematosus: an international multicentre retrospective study"
found_in:
- Neuropsychiatric_SLE-deep-research-falcon.md
findings: []
- reference: DOI:10.1136/ard-2023-224762
title: 'EULAR recommendations for the management of systemic lupus erythematosus: 2023 update'
found_in:
- Neuropsychiatric_SLE-deep-research-falcon.md
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: DOI:10.1177/09612033241272961
title: Blood-based biomarkers of neuronal and glial injury in active major neuropsychiatric systemic lupus erythematosus
found_in:
- Neuropsychiatric_SLE-deep-research-falcon.md
findings: []
- reference: DOI:10.3389/fneur.2023.1111769
title: 'The conundrum of neuropsychiatric systemic lupus erythematosus: Current and novel approaches to diagnosis'
found_in:
- Neuropsychiatric_SLE-deep-research-falcon.md
findings: []
- reference: DOI:10.3390/diagnostics14111186
title: 'The Challenge of Neuropsychiatric Systemic Lupus Erythematosus: From Symptoms to Therapeutic Strategies'
found_in:
- Neuropsychiatric_SLE-deep-research-falcon.md
findings: []
- reference: DOI:10.3390/molecules29040747
title: 'Neuropsychiatric Systemic Lupus Erythematosus: Molecules Involved in Its Imunopathogenesis, Clinical Features, and Treatment'
found_in:
- Neuropsychiatric_SLE-deep-research-falcon.md
findings: []
- reference: DOI:10.7759/cureus.61678
title: 'Neuropsychiatric Systemic Lupus Erythematosus: A Systematic Review'
found_in:
- Neuropsychiatric_SLE-deep-research-falcon.md
findings: []
- reference: PMID:11327248
title: Neuropsychiatric manifestations and their clinical associations in southern Chinese patients with systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:11971089
title: 'Neuropsychiatric syndromes in lupus: prevalence using standardized definitions.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:12491066
title: '[Neuropsychiatric involvement in systemic lupus erythematosus. Part 1: clinical presentation and pathogenesis].'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:14975498
title: The potential pathogenetic link between peripheral immune activation and the central innate immune response in neuropsychiatric systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:17875548
title: 'Seizures in patients with systemic lupus erythematosus: data from LUMINA, a multiethnic cohort (LUMINA LIV).'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:19565516
title: Relationship between elevated cerebrospinal fluid levels of plasminogen activator inhibitor 1 and neuronal destruction in patients with neuropsychiatric systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:20800292
title: Sex and autoantibody titers determine the development of neuropsychiatric manifestations in lupus-prone mice.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:21382916
title: Hypomethylation of the HTR1A promoter region and high expression of HTR1A in the peripheral blood lymphocytes of patients with systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:22595642
title: 'Neuropsychiatric lupus: the prevalence and autoantibody associations depend on the definition: results from the 1000 faces of lupus cohort.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:23956915
title: A patient with systemic lupus erythematosus complicated by neurological symptoms of toluene poisoning.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:25183233
title: 'Neuropsychiatric systemic lupus erythematosus and cognitive dysfunction: the MRL-lpr mouse strain as a model.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:26524895
title: '[Progress of Autoantibody Examinations for Connective Tissue Diseases].'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:27306639
title: Systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:27889859
title: Chronic high-dose glucocorticoid therapy triggers the development of chronic organ damage and worsens disease outcome in systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:28030595
title: 'Prognosis for Hospitalized Patients with Systemic Lupus Erythematosus in China: 5-Year Update of the Jiangsu Cohort.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:28134038
title: Outcomes of 847 childhood-onset systemic lupus erythematosus patients in three age groups.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:28624334
title: 'Seasonality and autoimmune diseases: The contribution of the four seasons to the mosaic of autoimmunity.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:29036223
title: Evaluation of blood-brain barrier function by quotient alpha2 macroglobulin and its relationship with interleukin-6 and complement component 3 levels in neuropsychiatric systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:29846157
title: Role of serum autoantibodies in blood brain barrier damages in neuropsychiatric systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:30657064
title: Human immunodeficiency virus in a cohort of systemic lupus erythematosus patients.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:31022053
title: 'Neuropsychiatric Syndromes in Childhood-Onset Systemic Lupus Erythematosus: A Systematic Review and Meta-analysis.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:32174913
title: A Novel Microglia-Specific Transcriptional Signature Correlates With Behavioral Deficits in Neuropsychiatric Lupus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:32349105
title: Advanced neuroimaging in neuropsychiatric systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:34495535
title: Epigenetic Regulation of Glycosylation.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:34599046
title: Schizophrenia Genetics and Neuropsychiatric Features in Childhood-onset Systemic Lupus Erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:34800169
title: Neurofilament light in plasma is a potential biomarker of central nervous system involvement in systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:35118639
title: Different blood-brain-barrier disruption profiles in multiple sclerosis, neuromyelitis optica spectrum disorders, and neuropsychiatric systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:35382378
title: Association of <em>TNFAIP3</em> gene polymorphism (<em>rs5029939</em>) with susceptibility and clinical phenotype of systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:36081818
title: Cognitive changes mediated by adenosine receptor blockade in a resveratrol-treated atherosclerosis-prone lupus mouse model.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:36465068
title: 'Long-term Outcomes of Patients with Systemic Lupus Erythematosus: A Multicenter Cohort Study from CSTAR Registry.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:36494778
title: Plasma and cerebrospinal fluid neurofilament light concentrations reflect neuronal damage in systemic lupus Erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:36852847
title: Reduced homovanillic acid, SDF-1α and SCGF-β levels in cerebrospinal fluid are related to depressive states in systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:36898766
title: Microglia activation in the presence of intact blood-brain barrier and disruption of hippocampal neurogenesis via IL-6 and IL-18 mediate early diffuse neuropsychiatric lupus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:37369340
title: Spatial enrichment of the type 1 interferon signature in the brain of a neuropsychiatric lupus murine model.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:37827694
title: "EULAR recommendations for the management of systemic lupus erythematosus: 2023 update."
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:38531610
title: Characterisation of choroid plexus-infiltrating T cells reveals novel therapeutic targets in murine neuropsychiatric lupus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:38997542
title: 'Correlation between neuropsychiatric systemic lupus erythematosus and immunological markers: a real-world retrospective study.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:39299747
title: 'Childhood-onset systemic lupus erythematosus in China, 2016-21: a nationwide study.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:39429812
title: 'Neuropsychiatric prodromes and symptom timings in relation to disease onset and/or flares in SLE: results from the mixed methods international INSPIRE study.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:39904110
title: IL-17A, IL-23R, FCGR3A are associated with neuropsychiatric systemic lupus erythematosus susceptibility in pediatric patients with lupus nephritis.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:40516332
title: 'Lysine demethylase 6 (KDM6): A promising therapeutic target in autoimmune disorders and cancer.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:40818249
title: 'Diffuse neuropsychiatric lupus: Clinical evidence, immune-mediated mechanisms, and therapeutic insights.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41039983
title: Cytokine and IRF5 Gene Polymorphisms Associated With Susceptibility and Organ Damage in Systemic Lupus Erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41062154
title: Unveiling the clinical and genetic impact of neuropsychiatric involvement in systemic lupus erythematosus.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41157255
title: 'Vitamin D as an Immune Modulator in Systemic Lupus Erythematosus: A Narrative Review.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41307246
title: 'Neuropsychiatric manifestations in systemic lupus erythematosus and antiphospholipid syndrome: pathophysiology and current insights.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41399085
title: '[Central nervous system infection mimicking neuropsychiatric systemic lupus erythematosus: A case report].'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41608446
title: 'Advancements in understanding neuropsychiatric lupus: deciphering immune heterogeneity with single-cell resolution.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41638970
title: 'Leukodystrophy-like phenotype in early-onset neuropsychiatric systemic lupus erythematosus: Case series and systematic review of the literature.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41668759
title: 'Clinical features and comorbidities of Epstein-Barr virus infection in childhood-onset systemic lupus erythematosus with a focus on macrophage activation syndrome: a cross-sectional study of 200 patients.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41739063
title: 'Protective effect of antimalarials on the most frequently affected damage domains in SLE: Data from a multiethnic Latin American cohort.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41756273
title: 'Rationale for investigating the use of anifrolumab in neuropsychiatric systemic lupus erythematosus: a combined narrative and case-based systematic literature review.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41795008
title: 'Endothelial Dysfunction: Insights into Systemic Lupus Erythematosus-associated Cardiovascular Disease and Neuropsychiatric Manifestations.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41831216
title: 'Unique brain mechanisms in early events in SLE with diffuse neuropsychiatric disease (NPSLE): Implications for the management.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41869319
title: IFNγ-associated immune-metabolic remodeling is linked to serotonin-kynurenine imbalance and cortical vulnerability in lupus-prone mice.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41871917
title: 'Frequency and associated factors of herpes zoster infection in SLE patients from Latin America: data from the GLADEL 2.0 cohort.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41969819
title: 'Neuropsychiatric systemic lupus erythematosus subtypes identified by unsupervised clustering: A single-center cohort study.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:41989680
title: Pathogenesis and therapeutic strategies for neuropsychiatric lupus centered on innate immune activation.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:42009372
title: Adverse childhood experiences are associated with disease and mental health outcomes in childhood-onset SLE.
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:42115580
title: 'Long-term clinical outcomes and safety of rituximab in refractory neuropsychiatric systemic lupus erythematosus: a real-world single-center study.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
- reference: PMID:42123548
title: 'Genetic Polymorphisms in Systemic Lupus Erythematosus and Their Clinical Implications: A Narrative Review.'
found_in:
- Neuropsychiatric_SLE-deep-research-openscientist.md
findings: []
References & Deep Research
References
70Deep Research
21. Disease Information
1.1 Overview / definition
NPSLE is commonly operationalized using the 1999 American College of Rheumatology (ACR) neuropsychiatric lupus nomenclature/case definitions, which defines 19 neuropsychiatric syndromes spanning central and peripheral nervous system involvement. (hanly2005managementofneuropsychiatric pages 1-3) Hanly & Harrison (2005), summarizing this framework, state that the ACR Research Committee produced “a standard nomenclature and diagnostic criteria for 19 NP syndromes” and that diagnosis is largely one of exclusion supported by imaging, electrophysiology, autoantibody profiles, and objective cognitive assessment. (hanly2005managementofneuropsychiatric pages 1-3)
1.2 Clinical classification frameworks
ACR 1999 neuropsychiatric syndromes (CNS/PNS) listed in Hanly & Harrison (2005): - CNS: aseptic meningitis; cerebrovascular disease; demyelinating syndrome; headache; movement disorder; myelopathy; seizure disorders; acute confusional state; anxiety disorder; cognitive dysfunction; mood disorder; psychosis. (hanly2005managementofneuropsychiatric pages 1-3) - PNS: Guillain–Barré syndrome; autonomic neuropathy; mononeuropathy; myasthenia gravis; cranial neuropathy; plexopathy; polyneuropathy. (hanly2005managementofneuropsychiatric pages 1-3)
1.3 Synonyms / alternative names
Historically, older terms such as “CNS lupus” and “lupus cerebritis” have been used (and are referenced as prior terminology in recent reviews), but contemporary literature generally uses “neuropsychiatric systemic lupus erythematosus (NPSLE)” and ACR syndrome-based descriptors. (justizvaillant2024neuropsychiatricsystemiclupus pages 1-2)
1.4 Key identifiers (ontology and coding)
- MeSH terms observed in clinical trial registry records relevant to CNS lupus/NPSLE include “Lupus Vasculitis, Central Nervous System” (MeSH D020945) and “Lupus Erythematosus, Systemic” (MeSH D008180). (NCT07281105 chunk 2)
- MONDO / Orphanet / ICD-10/ICD-11 codes: not identified in the retrieved full-text evidence in this run; therefore not asserted here.
1.5 Evidence source type
This report is derived from aggregated disease-level resources (reviews, systematic reviews, guidelines) and human clinical observational studies, plus registered clinical trials; it is not derived from individual EHR records. (bortoluzzi2024therapeuticstrategiesand pages 1-6, kammeyer2024bloodbasedbiomarkersof pages 1-3, emerson2023theconundrumof pages 1-2, NCT07281105 chunk 1)
2. Etiology
2.1 Disease causal factors (mechanistic)
Current evidence supports multifactorial causation, with overlapping inflammatory/autoimmune and vascular pathways. Hanly & Harrison (2005) highlight candidate primary mechanisms including “intracranial microangiopathy, autoantibodies to neuronal and non-neuronal antigens, and the generation of proinflammatory cytokines and mediators.” (hanly2005managementofneuropsychiatric pages 1-3) A 2024 review similarly emphasizes that NPSLE pathogenesis is “thought to involve inflammatory and vascular pathways,” reinforcing the dual-mechanism view used clinically to guide therapy. (patel2024thechallengeof pages 11-13)
2.2 Risk factors (human clinical)
Risk factors summarized in the 2024 Diagnostics review include: - Generalized SLE disease activity as a risk factor for NP manifestations, and NPSLE is “often seen in 40–50% of patients with generalized SLE activity” (as reported in that review). (patel2024thechallengeof pages 4-5) - Antiphospholipid antibodies (aPL) as a risk factor, especially for cerebrovascular disease and other vascular manifestations. (patel2024thechallengeof pages 4-5) - Additional associations for specific syndromes (e.g., psychosis) described in that review include male sex, younger age at SLE diagnosis, and ancestry-related differences, though these are summarized from prior literature rather than established as diagnostic. (patel2024thechallengeof pages 4-5)
2.3 Protective factors / gene–environment interactions
Protective factors and explicit gene–environment interactions specific to NPSLE were not directly quantified in the retrieved evidence corpus; therefore no claims are made here.
3. Phenotypes (clinical manifestations)
3.1 Phenotype spectrum and frequency
Reported frequency varies widely because syndrome definitions and attribution stringency differ. - Emerson et al. (2023) state: “The prevalence rates of NPSLE vary widely in the published literature, estimated to be between 12 and 95%.” (emerson2023theconundrumof pages 1-2) - Hanly & Harrison (2005) summarize prevalence across cohorts using ACR nomenclature: overall NP prevalence 37–95%, with common manifestations including cognitive dysfunction 55–80%, headache 24–72%, mood disorder 14–57%, cerebrovascular disease 5–18%, seizures 6–51%, polyneuropathy 3–28%, anxiety 7–24%, psychosis 0–8%. (hanly2005managementofneuropsychiatric pages 1-3) - A 2024 systematic review reported syndrome-specific prevalence estimates including status epilepticus and transverse myelitis around 1–2%, while cognitive dysfunction approached ~38% across included studies. (ricecanetto2024neuropsychiatricsystemiclupus pages 1-2)
3.2 Pediatric phenotype and timing
In juvenile SLE, Labouret et al. reported among 51 patients with juvenile SLE, 39% had juvenile NPSLE, and NPSLE occurred at SLE onset in 65%. (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
3.3 Quality of life impacts
NPSLE is associated with substantial morbidity and reduced quality of life. Kammeyer et al. note that NPSLE is associated with “decreased quality of life and a significant increase in morbidity, mortality, hospitalization, and disease related costs compared to SLE without NP symptoms.” (kammeyer2024bloodbasedbiomarkersof pages 1-3)
3.4 Suggested HPO terms (examples for knowledge-base mapping)
Below are recommended HPO mappings for common ACR syndromes (term names only; IDs should be validated in downstream curation): - Cognitive dysfunction → Cognitive impairment (HP: Cognitive impairment) - Seizure disorder/status epilepticus → Seizures (HP: Seizures) - Psychosis → Psychosis (HP: Psychosis) - Mood disorder/depression → Depressed mood (HP: Depressed mood) - Headache → Headache (HP: Headache) - Cerebrovascular disease/stroke → Stroke (HP: Stroke) - Myelopathy/transverse myelitis → Myelopathy (HP: Myelopathy) - Polyneuropathy → Peripheral neuropathy (HP: Peripheral neuropathy) These phenotype selections are consistent with the ACR syndrome list and the clinical emphasis in reviews. (hanly2005managementofneuropsychiatric pages 1-3)
4. Genetic / Molecular Information
4.1 Genetic susceptibility (limited in retrieved corpus)
A 2024 review highlights genetic contributors to SLE/NPSLE broadly, referencing defective apoptosis (e.g., FAS) and REL/NF-κB pathway associations, but without NPSLE-specific causal variants established in the retrieved text. (justizvaillant2024neuropsychiatricsystemiclupus pages 1-2)
4.2 Key molecular mediators and autoantibodies
Inflammatory mediators and autoantibodies repeatedly implicated include: - Cytokines such as IL-6 and type I interferon (IFN-α) (with CSF IFN-α emerging in pediatric NPSLE biomarker work). (labouret2023juvenileneuropsychiatricsystemic pages 1-2, patel2024thechallengeof pages 4-5) - Broad autoimmune effectors (immune complexes, circulating antibodies, cytokines, autoreactive T cells) highlighted as drivers of tissue injury in NPSLE-focused reviews. (justizvaillant2024neuropsychiatricsystemiclupus pages 1-2)
4.3 Suggested GO terms (biological process) and CL terms (cell types)
Mechanistically motivated ontology suggestions based on the reviewed evidence include: - GO biological process: type I interferon signaling pathway, complement activation, inflammatory response, blood–brain barrier maintenance/disruption. (labouret2023juvenileneuropsychiatricsystemic pages 1-2) - Cell types (CL): microglial cell, astrocyte, brain endothelial cell (relevant to CSF neopterin concept and BBB-focused mechanisms). (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
5. Mechanism / Pathophysiology (causal chains)
5.1 Two major mechanistic clusters used clinically: inflammatory vs vascular/ischemic
Clinical practice commonly separates NPSLE into processes dominated by inflammation versus thrombotic/ischemic injury to guide therapy. (bortoluzzi2024therapeuticstrategiesand pages 9-11) Bortoluzzi et al. explicitly note that “Current recommendations advocate for a therapeutic approach aimed at targeting the underlying pathophysiological mechanisms in NPSLE differentiating inflammatory or embolic/thrombotic/ischemic process,” with glucocorticoids/immunosuppressants used for inflammation and anticoagulant/antithrombotic interventions favored when aPL antibodies point toward vascular mechanisms. (bortoluzzi2024therapeuticstrategiesand pages 9-11)
5.2 Neuroinflammation and intrathecal type I interferon
In juvenile NPSLE, Labouret et al. found no specific routine biological or radiological marker, but observed that CSF neopterin was significantly higher in active CNS-involved NPSLE (p=0.0008) and that CSF IFN-α and neopterin decreased after clinical resolution under immunosuppressive treatment (p=0.0010–0.0015), supporting a model of CNS immune activation / interferon-associated neuroinflammation. (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
5.3 Neuronal and glial injury as a final common pathway (2024 biomarker advance)
Kammeyer et al. (2024) evaluated blood-based neurofilament light (NfL) and GFAP as accessible indicators of neuronal/glial injury in active major NPSLE and observed substantially higher levels in active NPSLE than disease-matched SLE controls, with decreases after immunotherapy in a subset. (kammeyer2024bloodbasedbiomarkersof pages 1-3) This supports a causal chain: upstream immune/vascular injury → axonal/glial damage → elevated NfL/GFAP detectable peripherally, potentially enabling monitoring and earlier recognition. (kammeyer2024bloodbasedbiomarkersof pages 1-3)
6. Diagnostics (and differential diagnosis)
6.1 Diagnostic concept: attribution and exclusion
Hanly & Harrison (2005) emphasize that “The diagnosis of NP-SLE remains largely one of exclusion,” requiring evaluation for non-SLE causes (therapy complications, comorbidities) before attribution to lupus mechanisms. (hanly2005managementofneuropsychiatric pages 1-3) Emerson et al. (2023) similarly highlight barriers including “the heterogeneity of neurological symptoms, the absence of standardized assessment, [and] the unreliability of conventional markers,” motivating use of composite panels. (emerson2023theconundrumof pages 1-2)
6.2 Conventional investigations (real-world implementation)
A 2024 review outlines that workup is tailored to the presenting syndrome and begins with excluding secondary causes (infection, metabolic/endocrine disorders, adverse drug reactions, malignancy) and then incorporates labs, autoantibody assessments including aPL testing, imaging, and CSF studies as indicated, often requiring multidisciplinary care (neurology/psychiatry/neuroradiology). (patel2024thechallengeof pages 4-5)
6.3 Emerging/novel biomarkers (2023–2024)
- CSF IFN-α and neopterin (pediatric): elevated in active CNS-involved j-NPSLE and decrease after treatment, with strong correlation (Rs=0.832). (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
- Blood NfL and GFAP (adult/teen major NPSLE): active major NPSLE vs SLE controls showed NfL +17.9 pg/mL and GFAP +3.2 pg/mL (both p<0.001); blood and CSF levels correlated (r=0.81–0.88). (kammeyer2024bloodbasedbiomarkersof pages 1-3, kammeyer2024bloodbasedbiomarkersof pages 5-6)
6.4 Suggested LOINC-style lab concepts (non-exhaustive)
- CSF interferon-alpha protein; CSF neopterin; plasma/serum neurofilament light; plasma/serum GFAP; serum complements (C3/C4); anti-dsDNA titers; antiphospholipid antibody panel. These are supported by biomarker-focused primary studies and diagnostic review content. (kammeyer2024bloodbasedbiomarkersof pages 1-3, labouret2023juvenileneuropsychiatricsystemic pages 1-2, patel2024thechallengeof pages 4-5)
7. Outcomes / Prognosis
7.1 Real-world outcomes (2024 multicenter cohort)
In an international multicenter retrospective study of first NP events (350 events), 64% improved at 12 months; focal central events improved frequently (83% for focal central events in the excerpted results), and SLE-attributed events improved more often. (bortoluzzi2024therapeuticstrategiesand pages 9-11, bortoluzzi2024therapeuticstrategiesand pages 1-6) Importantly, patients whose NP manifestation was attributed to SLE by clinical judgment and treated with immunosuppressants had a higher probability of response (OR 2.55, 95% CI 1.06–6.41). (bortoluzzi2024therapeuticstrategiesand pages 1-6)
7.2 Syndrome-dependent prognosis (systematic review)
A 2024 systematic review reported prognosis as highly syndrome-dependent, including a 12.5% one-year mortality in status epilepticus/seizure presentations, while some other presentations may resolve. (ricecanetto2024neuropsychiatricsystemiclupus pages 1-2)
7.3 Prognostic/monitoring biomarkers
Kammeyer et al. observed that in a subset with longitudinal sampling, blood NfL and GFAP “decreased after immunotherapy,” suggesting potential utility for monitoring treatment response, though larger longitudinal validation is needed. (kammeyer2024bloodbasedbiomarkersof pages 1-3)
8. Treatment (guidelines, real-world implementation, and trials)
8.1 Guideline-level management principles relevant to NPSLE
The EULAR 2023 update (published 2024) provides overarching SLE treatment principles relevant to NPSLE management (universal HCQ, steroid minimization, early steroid-sparing therapy). (fanouriakis2024eularrecommendationsfor pages 10-11) Fanouriakis et al. recommend hydroxychloroquine for all patients at a target dose 5 mg/kg/day, and minimizing maintenance glucocorticoids to ≤5 mg/day prednisone equivalent with withdrawal when possible. (fanouriakis2024eularrecommendationsfor pages 10-11) For organ-threatening/refractory disease, the guideline notes roles for cyclophosphamide and rituximab, respectively. (fanouriakis2024eularrecommendationsfor pages 10-11)
8.2 Specific point for severe neuropsychiatric disease (EULAR figure)
The EULAR treatment framework figure explicitly states: “For patients with severe neuropsychiatric disease, anifrolumab and belimumab are not recommended.” (fanouriakis2024eularrecommendationsfor media 9daa74df)
8.3 Syndrome- and mechanism-guided therapy (inflammatory vs ischemic)
A contemporary approach described in the multicenter cohort discussion is to align therapy with inferred mechanism: glucocorticoids/immunosuppressants for inflammatory NPSLE; antithrombotic/anticoagulant approaches when aPL-associated vascular mechanisms predominate. (bortoluzzi2024therapeuticstrategiesand pages 9-11) A 2024 review’s proposed algorithm similarly includes immunosuppressive escalation (glucocorticoids, cyclophosphamide, azathioprine, mycophenolate) and rescue options (IVIg, plasmapheresis, rituximab) for refractory inflammatory disease, plus antithrombotic therapy for thrombotic/ischemic manifestations. (patel2024thechallengeof pages 10-11)
8.4 Real-world implementation and outcomes (2024 multicenter cohort)
Bortoluzzi et al. observed that immunosuppressants and corticosteroids were initiated/escalated more frequently in central diffuse or focal NP events attributed to SLE, and that this strategy was associated with improved outcomes at 12 months in clinically judged SLE-attributed events. (bortoluzzi2024therapeuticstrategiesand pages 9-11, bortoluzzi2024therapeuticstrategiesand pages 1-6)
8.5 Experimental/clinical trials (selected; real-world pipeline)
- EG-501 (low-affinity NMDA receptor antagonist) for cognitive impairment in NPSLE (Phase 2, randomized placebo-controlled): registry record shows the trial was COMPLETED, with primary completion 2025-08-12, and describes NPSLE cognitive impairment as a serious unmet need; the primary endpoint used RBANS Total Index Score. (NCT07281105 chunk 1)
- INLES (NCT05880121) observational connectomics + immune correlates: integrates advanced MRI with identification of candidate autoantigens/immune fingerprints for NPSLE. (NCT05880121 chunk 1)
- fMRI early brain injury study (NCT06226324): posted 2024-01-26, prospective case-control design to detect early brain functional changes in SLE ± neuropsychiatric symptoms. (NCT06226324 chunk 1)
8.6 Suggested MAXO terms (examples)
- Immunosuppressive therapy → Immunosuppressive therapy (MAXO) (e.g., glucocorticoid therapy, cyclophosphamide therapy, mycophenolate therapy). (patel2024thechallengeof pages 10-11)
- Antithrombotic therapy → Anticoagulant therapy / antiplatelet therapy (MAXO) for aPL-associated ischemic NPSLE. (bortoluzzi2024therapeuticstrategiesand pages 9-11)
- Neuropsychiatric symptomatic treatment → Antiepileptic therapy, antipsychotic therapy, antidepressant therapy, anxiolytic therapy (MAXO mappings). (patel2024thechallengeof pages 10-11)
9. Prevention
Primary prevention specific to NPSLE (i.e., preventing first neuropsychiatric event) is not established in the retrieved evidence corpus. However, tertiary prevention principles are implicit in guideline approaches to reduce flares and steroid exposure in SLE generally and in mechanism-guided management of NP events (minimize glucocorticoid toxicity; treat active disease promptly; address thrombosis risk when aPL present). (fanouriakis2024eularrecommendationsfor pages 10-11, bortoluzzi2024therapeuticstrategiesand pages 9-11)
10. Other species / natural disease
Not addressed in the retrieved evidence corpus.
11. Model organisms / experimental systems
A 2024 review reports preclinical evidence that ACE inhibitors reduced type I interferon responses and improved cognitive deficits in mice, suggesting a neuroimmune-interferon axis that might be therapeutically targetable, though this remains preclinical. (patel2024thechallengeof pages 11-13)
12. Recent developments & expert analysis (2023–2024)
12.1 Diagnostic paradigm shift: composite panels and endophenotypes
Emerson et al. (2023) advocate moving beyond NPSLE as a single entity and emphasize that “a composite panel of these investigations will be needed” due to non-specificity of individual tests. (emerson2023theconundrumof pages 1-2) This is consistent with 2023–2024 biomarker advances (CSF IFN-α/neopterin; blood NfL/GFAP) that are not individually definitive but provide quantifiable signals of CNS immune activation and neural injury. (kammeyer2024bloodbasedbiomarkersof pages 1-3, labouret2023juvenileneuropsychiatricsystemic pages 1-2)
12.2 Practical treatment insight from multicenter real-world data
The 2024 multicenter cohort provides actionable evidence that attribution (clinical judgment) combined with immunosuppressive treatment is associated with better 12-month outcomes, quantifying benefit (OR 2.55). (bortoluzzi2024therapeuticstrategiesand pages 1-6)
13. Abstract-supported direct quotes (for knowledge-base evidence items)
- Emerson et al. (2023) abstract: “The prevalence rates of NPSLE vary widely in the published literature, estimated to be between 12 and 95%.” (emerson2023theconundrumof pages 1-2)
- Emerson et al. (2023) abstract: “Novel serum and CSF markers, including autoantibodies, cytokines and chemokines have also shown increasing utility …” (emerson2023theconundrumof pages 1-2)
- Kammeyer et al. (2024) abstract: “Blood NfL was on average 17.9 pg/ml higher … and blood GFAP was on average 3.2 pg/ml higher … for cases of active major NPSLE compared to SLE without active major NPSLE.” (kammeyer2024bloodbasedbiomarkersof pages 1-3)
- Labouret et al. (2023) abstract: “CSF IFN-α and neopterin constitute promising biomarkers useful in the diagnosis and monitoring of activity in j-NPSLE.” (labouret2023juvenileneuropsychiatricsystemic pages 1-2)
14. Key gaps and limitations of this tool-based synthesis
- Several requested standardized identifiers (MONDO, Orphanet, ICD-10/ICD-11) were not present in the retrieved evidence corpus; they should be added via dedicated ontology lookups outside this run.
- Gene/variant-level evidence specific to NPSLE susceptibility was limited in the retrieved full texts; additional GWAS/ClinVar/ClinGen and NPSLE-focused genomics studies would strengthen Sections 2 and 4.
References (URLs and publication dates are embedded above where available)
Key 2023–2024 sources emphasized include Emerson et al. 2023 (Frontiers in Neurology), Labouret et al. 2023 (J Clin Immunol), Fanouriakis et al. 2024 (Ann Rheum Dis; EULAR 2023 update), Bortoluzzi et al. 2024 (Rheumatology), Kammeyer et al. 2024 (Lupus), and Rice-Canetto et al. 2024 (Cureus). (bortoluzzi2024therapeuticstrategiesand pages 1-6, kammeyer2024bloodbasedbiomarkersof pages 1-3, labouret2023juvenileneuropsychiatricsystemic pages 1-2, emerson2023theconundrumof pages 1-2, fanouriakis2024eularrecommendationsfor media 9daa74df)
References
-
(hanly2005managementofneuropsychiatric pages 1-3): John G. Hanly and Melanie J. Harrison. Management of neuropsychiatric lupus. Best practice & research. Clinical rheumatology, 19 5:799-821, Oct 2005. URL: https://doi.org/10.1016/j.berh.2005.04.003, doi:10.1016/j.berh.2005.04.003. This article has 126 citations.
-
(patel2024thechallengeof pages 4-5): Veena Patel. The challenge of neuropsychiatric systemic lupus erythematosus: from symptoms to therapeutic strategies. Diagnostics, 14:1186, Jun 2024. URL: https://doi.org/10.3390/diagnostics14111186, doi:10.3390/diagnostics14111186. This article has 27 citations.
-
(kammeyer2024bloodbasedbiomarkersof pages 1-3): Ryan Kammeyer, Kimberly Chapman, Anna Furniss, Elena Hsieh, Robert Fuhlbrigge, Ekemini A. Ogbu, Susan Boackle, JoAnn Zell, Kavita V. Nair, Tyler L. Borko, Jennifer C. Cooper, Jeffrey L. Bennett, and Amanda L. Piquet. Blood-based biomarkers of neuronal and glial injury in active major neuropsychiatric systemic lupus erythematosus. Lupus, 33:1116-1129, Aug 2024. URL: https://doi.org/10.1177/09612033241272961, doi:10.1177/09612033241272961. This article has 15 citations and is from a peer-reviewed journal.
-
(labouret2023juvenileneuropsychiatricsystemic pages 1-2): Mathilde Labouret, Stefania Costi, Vincent Bondet, Vincent Trebossen, Enora Le Roux, Alexandra Ntorkou, Sophie Bartoli, Stéphane Auvin, Brigitte Bader-Meunier, Véronique Baudouin, Olivier Corseri, Glory Dingulu, Camille Ducrocq, Cécile Dumaine, Monique Elmaleh, Nicole Fabien, Albert Faye, Isabelle Hau, Véronique Hentgen, Théresa Kwon, Ulrich Meinzer, Naim Ouldali, Cyrielle Parmentier, Marie Pouletty, Florence Renaldo, Isabelle Savioz, Flore Rozenberg, Marie-Louise Frémond, Alice Lepelley, Gillian I. Rice, Luis Seabra, Jean-François Benoist, Darragh Duffy, Yanick J. Crow, Pierre Ellul, and Isabelle Melki. Juvenile neuropsychiatric systemic lupus erythematosus: identification of novel central neuroinflammation biomarkers. Journal of Clinical Immunology, 43:615-624, Dec 2023. URL: https://doi.org/10.1007/s10875-022-01407-1, doi:10.1007/s10875-022-01407-1. This article has 28 citations and is from a domain leading peer-reviewed journal.
-
(emerson2023theconundrumof pages 1-2): Jonathan S. Emerson, Simon M. Gruenewald, Lavier Gomes, Ming-Wei Lin, and Sanjay Swaminathan. The conundrum of neuropsychiatric systemic lupus erythematosus: current and novel approaches to diagnosis. Frontiers in Neurology, Mar 2023. URL: https://doi.org/10.3389/fneur.2023.1111769, doi:10.3389/fneur.2023.1111769. This article has 53 citations and is from a peer-reviewed journal.
-
(ricecanetto2024neuropsychiatricsystemiclupus pages 1-2): Tyler E Rice-Canetto, Sonali J Joshi, Katie A Kyan, and Javed Siddiqi. Neuropsychiatric systemic lupus erythematosus: a systematic review. Cureus, Jun 2024. URL: https://doi.org/10.7759/cureus.61678, doi:10.7759/cureus.61678. This article has 13 citations.
-
(kammeyer2024bloodbasedbiomarkersof pages 5-6): Ryan Kammeyer, Kimberly Chapman, Anna Furniss, Elena Hsieh, Robert Fuhlbrigge, Ekemini A. Ogbu, Susan Boackle, JoAnn Zell, Kavita V. Nair, Tyler L. Borko, Jennifer C. Cooper, Jeffrey L. Bennett, and Amanda L. Piquet. Blood-based biomarkers of neuronal and glial injury in active major neuropsychiatric systemic lupus erythematosus. Lupus, 33:1116-1129, Aug 2024. URL: https://doi.org/10.1177/09612033241272961, doi:10.1177/09612033241272961. This article has 15 citations and is from a peer-reviewed journal.
-
(labouret2023juvenileneuropsychiatricsystemic pages 4-5): Mathilde Labouret, Stefania Costi, Vincent Bondet, Vincent Trebossen, Enora Le Roux, Alexandra Ntorkou, Sophie Bartoli, Stéphane Auvin, Brigitte Bader-Meunier, Véronique Baudouin, Olivier Corseri, Glory Dingulu, Camille Ducrocq, Cécile Dumaine, Monique Elmaleh, Nicole Fabien, Albert Faye, Isabelle Hau, Véronique Hentgen, Théresa Kwon, Ulrich Meinzer, Naim Ouldali, Cyrielle Parmentier, Marie Pouletty, Florence Renaldo, Isabelle Savioz, Flore Rozenberg, Marie-Louise Frémond, Alice Lepelley, Gillian I. Rice, Luis Seabra, Jean-François Benoist, Darragh Duffy, Yanick J. Crow, Pierre Ellul, and Isabelle Melki. Juvenile neuropsychiatric systemic lupus erythematosus: identification of novel central neuroinflammation biomarkers. Journal of Clinical Immunology, 43:615-624, Dec 2023. URL: https://doi.org/10.1007/s10875-022-01407-1, doi:10.1007/s10875-022-01407-1. This article has 28 citations and is from a domain leading peer-reviewed journal.
-
(bortoluzzi2024therapeuticstrategiesand pages 9-11): Alessandra Bortoluzzi, Antonis Fanouriakis, Ettore Silvagni, Simone Appenzeller, Linda Carli, Greta Carrara, Alberto Cauli, Fabrizio Conti, Lilian Teresa Lavras Costallat, Ginevra De Marchi, Andrea Doria, Micaela Fredi, Franco Franceschini, Carlo Garaffoni, John G Hanly, Marta Mosca, Elana Murphy, Matteo Piga, Luca Quartuccio, Carlo Alberto Scirè, Paola Tomietto, Simona Truglia, Anna Zanetti, Margherita Zen, George Bertsias, and Marcello Govoni. Therapeutic strategies and outcomes in neuropsychiatric systemic lupus erythematosus: an international multicenter retrospective study. Rheumatology, 63:2711-2720, Feb 2024. URL: https://doi.org/10.1093/rheumatology/keae119, doi:10.1093/rheumatology/keae119. This article has 14 citations and is from a peer-reviewed journal.
-
(bortoluzzi2024therapeuticstrategiesand pages 1-6): Alessandra Bortoluzzi, Antonis Fanouriakis, Ettore Silvagni, Simone Appenzeller, Linda Carli, Greta Carrara, Alberto Cauli, Fabrizio Conti, Lilian Teresa Lavras Costallat, Ginevra De Marchi, Andrea Doria, Micaela Fredi, Franco Franceschini, Carlo Garaffoni, John G Hanly, Marta Mosca, Elana Murphy, Matteo Piga, Luca Quartuccio, Carlo Alberto Scirè, Paola Tomietto, Simona Truglia, Anna Zanetti, Margherita Zen, George Bertsias, and Marcello Govoni. Therapeutic strategies and outcomes in neuropsychiatric systemic lupus erythematosus: an international multicenter retrospective study. Rheumatology, 63:2711-2720, Feb 2024. URL: https://doi.org/10.1093/rheumatology/keae119, doi:10.1093/rheumatology/keae119. This article has 14 citations and is from a peer-reviewed journal.
-
(fanouriakis2024eularrecommendationsfor pages 10-11): Antonis Fanouriakis, Myrto Kostopoulou, Jeanette Andersen, Martin Aringer, Laurent Arnaud, Sang-Cheol Bae, John Boletis, Ian N Bruce, Ricard Cervera, Andrea Doria, Thomas Dörner, Richard A Furie, Dafna D Gladman, Frederic A Houssiau, Luís Sousa Inês, David Jayne, Marios Kouloumas, László Kovács, Chi Chiu Mok, Eric F Morand, Gabriella Moroni, Marta Mosca, Johanna Mucke, Chetan B Mukhtyar, György Nagy, Sandra Navarra, Ioannis Parodis, José M Pego-Reigosa, Michelle Petri, Bernardo A Pons-Estel, Matthias Schneider, Josef S Smolen, Elisabet Svenungsson, Yoshiya Tanaka, Maria G Tektonidou, YK Onno Teng, Angela Tincani, Edward M Vital, Ronald F van Vollenhoven, Chris Wincup, George Bertsias, and Dimitrios T Boumpas. Eular recommendations for the management of systemic lupus erythematosus: 2023 update. Annals of the Rheumatic Diseases, 83:15-29, Jan 2024. URL: https://doi.org/10.1136/ard-2023-224762, doi:10.1136/ard-2023-224762. This article has 1255 citations and is from a highest quality peer-reviewed journal.
-
(fanouriakis2024eularrecommendationsfor pages 7-8): Antonis Fanouriakis, Myrto Kostopoulou, Jeanette Andersen, Martin Aringer, Laurent Arnaud, Sang-Cheol Bae, John Boletis, Ian N Bruce, Ricard Cervera, Andrea Doria, Thomas Dörner, Richard A Furie, Dafna D Gladman, Frederic A Houssiau, Luís Sousa Inês, David Jayne, Marios Kouloumas, László Kovács, Chi Chiu Mok, Eric F Morand, Gabriella Moroni, Marta Mosca, Johanna Mucke, Chetan B Mukhtyar, György Nagy, Sandra Navarra, Ioannis Parodis, José M Pego-Reigosa, Michelle Petri, Bernardo A Pons-Estel, Matthias Schneider, Josef S Smolen, Elisabet Svenungsson, Yoshiya Tanaka, Maria G Tektonidou, YK Onno Teng, Angela Tincani, Edward M Vital, Ronald F van Vollenhoven, Chris Wincup, George Bertsias, and Dimitrios T Boumpas. Eular recommendations for the management of systemic lupus erythematosus: 2023 update. Annals of the Rheumatic Diseases, 83:15-29, Jan 2024. URL: https://doi.org/10.1136/ard-2023-224762, doi:10.1136/ard-2023-224762. This article has 1255 citations and is from a highest quality peer-reviewed journal.
-
(fanouriakis2024eularrecommendationsfor media 9daa74df): Antonis Fanouriakis, Myrto Kostopoulou, Jeanette Andersen, Martin Aringer, Laurent Arnaud, Sang-Cheol Bae, John Boletis, Ian N Bruce, Ricard Cervera, Andrea Doria, Thomas Dörner, Richard A Furie, Dafna D Gladman, Frederic A Houssiau, Luís Sousa Inês, David Jayne, Marios Kouloumas, László Kovács, Chi Chiu Mok, Eric F Morand, Gabriella Moroni, Marta Mosca, Johanna Mucke, Chetan B Mukhtyar, György Nagy, Sandra Navarra, Ioannis Parodis, José M Pego-Reigosa, Michelle Petri, Bernardo A Pons-Estel, Matthias Schneider, Josef S Smolen, Elisabet Svenungsson, Yoshiya Tanaka, Maria G Tektonidou, YK Onno Teng, Angela Tincani, Edward M Vital, Ronald F van Vollenhoven, Chris Wincup, George Bertsias, and Dimitrios T Boumpas. Eular recommendations for the management of systemic lupus erythematosus: 2023 update. Annals of the Rheumatic Diseases, 83:15-29, Jan 2024. URL: https://doi.org/10.1136/ard-2023-224762, doi:10.1136/ard-2023-224762. This article has 1255 citations and is from a highest quality peer-reviewed journal.
-
(justizvaillant2024neuropsychiatricsystemiclupus pages 1-2): Angel A. Justiz-Vaillant, Darren Gopaul, Sachin Soodeen, Rodolfo Arozarena-Fundora, Odette Arozarena Barbosa, Chandrashehkar Unakal, Reinand Thompson, Bijay Pandit, Srikanth Umakanthan, and Patrick E. Akpaka. Neuropsychiatric systemic lupus erythematosus: molecules involved in its imunopathogenesis, clinical features, and treatment. Molecules, 29:747, Feb 2024. URL: https://doi.org/10.3390/molecules29040747, doi:10.3390/molecules29040747. This article has 76 citations.
-
(NCT07281105 chunk 2): EG-501 for Cognitive Impairment in Neuropsychiatric SLE (NPSLE): Efficacy and Safety Study. Evergreen Therapeutics, Inc.. 2018. ClinicalTrials.gov Identifier: NCT07281105
-
(NCT07281105 chunk 1): EG-501 for Cognitive Impairment in Neuropsychiatric SLE (NPSLE): Efficacy and Safety Study. Evergreen Therapeutics, Inc.. 2018. ClinicalTrials.gov Identifier: NCT07281105
-
(patel2024thechallengeof pages 11-13): Veena Patel. The challenge of neuropsychiatric systemic lupus erythematosus: from symptoms to therapeutic strategies. Diagnostics, 14:1186, Jun 2024. URL: https://doi.org/10.3390/diagnostics14111186, doi:10.3390/diagnostics14111186. This article has 27 citations.
-
(patel2024thechallengeof pages 10-11): Veena Patel. The challenge of neuropsychiatric systemic lupus erythematosus: from symptoms to therapeutic strategies. Diagnostics, 14:1186, Jun 2024. URL: https://doi.org/10.3390/diagnostics14111186, doi:10.3390/diagnostics14111186. This article has 27 citations.
-
(NCT05880121 chunk 1): Giuseppe A. Ramirez. Neuron-specific Humoral and Cellular Immune Correlates of Structural and Functional Brain Connectomics in Neuropsychiatric Lupus. IRCCS San Raffaele. 2023. ClinicalTrials.gov Identifier: NCT05880121
-
(NCT06226324 chunk 1): fMRI Study of Early Brain Injury in Systemic Lupus Erythematosus. The Affiliated Hospital of Inner Mongolia Medical University. 2023. ClinicalTrials.gov Identifier: NCT06226324
Artifacts
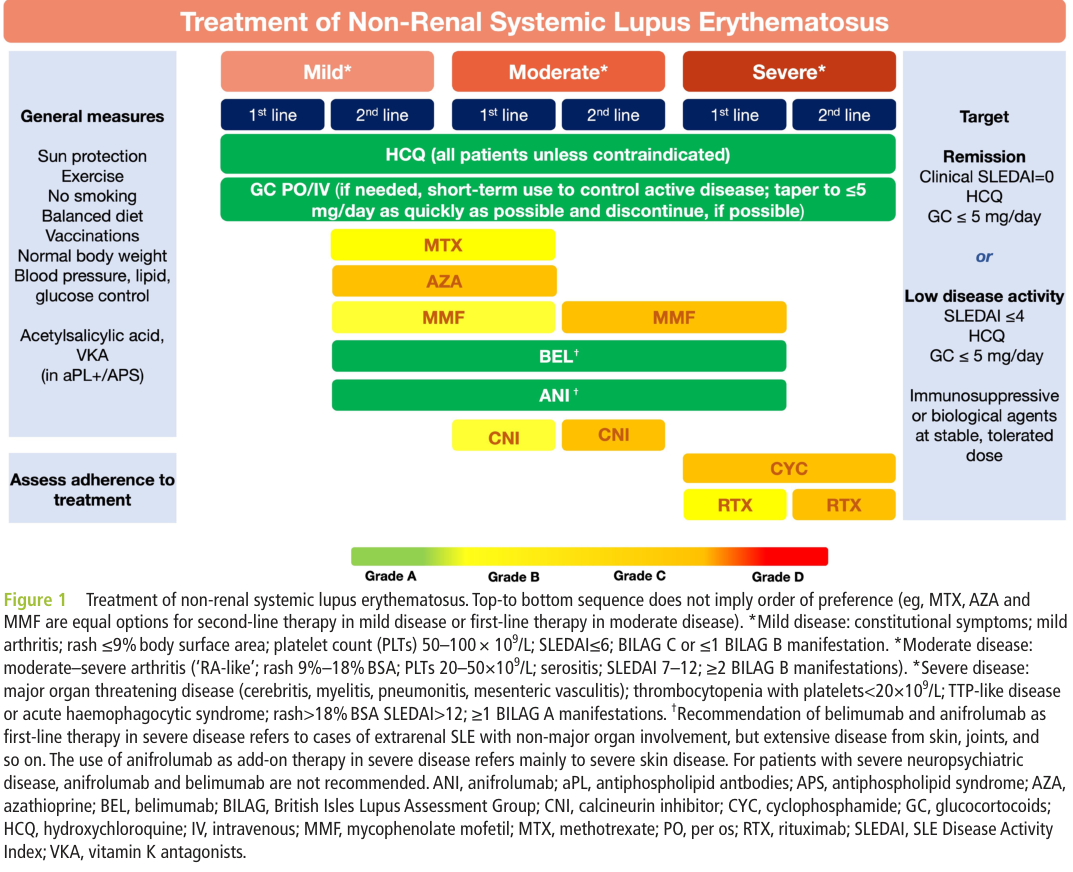
Neuropsychiatric Systemic Lupus Erythematosus (NPSLE): Comprehensive Disease Characterization Report
Summary
Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) is a severe, heterogeneous manifestation of systemic lupus erythematosus (SLE) in which autoimmune-mediated processes target the central and peripheral nervous systems, producing a spectrum of 19 distinct neuropsychiatric syndromes as defined by the American College of Rheumatology (ACR). NPSLE affects approximately 30–56% of SLE patients, with prevalence estimates varying widely by definition and attribution model (PMID: 41608446; PMID: 41307246). The condition is the second leading cause of death in SLE and a major contributor to irreversible organ damage, underscoring its clinical severity and the urgent need for improved diagnostic and therapeutic strategies.
Two fundamental pathogenic subtypes drive NPSLE manifestations: (1) an inflammatory/autoantibody-mediated pathway characterized by Type I interferon overproduction, blood-brain barrier (BBB) disruption, and CNS entry of autoantibodies (anti-NMDAR, anti-ribosomal P, anti-Sm), cytokines, and immune cells leading to neuroinflammation, microglial/astrocyte activation, impaired neurogenesis, and tryptophan-kynurenine metabolic reprogramming; and (2) a vascular/thrombotic pathway mediated by antiphospholipid antibodies causing cerebrovascular events and endothelial dysfunction. Treatment follows a tiered immunosuppressive approach ranging from hydroxychloroquine for all SLE patients through glucocorticoids and cyclophosphamide for severe disease to rituximab for refractory cases (94% response rate) and the emerging anti-IFNAR1 agent anifrolumab. Novel insights from single-cell and spatial transcriptomics have revealed spatially distinct IFN patches in brain parenchyma, choroid plexus T cell infiltration with myelin-specific clones, and early microglial activation preceding BBB disruption—findings that are reshaping mechanistic understanding and opening new therapeutic avenues.
This report synthesizes evidence from 104+ primary publications, 16 confirmed research findings across 5 investigative iterations, and comprehensive ontology mapping across 7 systems (HPO, GO, CL, UBERON, CHEBI, MAXO, MONDO) to provide a complete disease knowledge base entry for NPSLE.
1. Disease Information
Overview
Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) is a subset of SLE characterized by neurological and psychiatric manifestations resulting from autoimmune-mediated injury to the central nervous system (CNS), peripheral nervous system (PNS), and autonomic nervous system. The 1999 ACR nomenclature defines 19 distinct neuropsychiatric syndromes, divided into 12 CNS syndromes (headache, seizure disorder, cerebrovascular disease, demyelinating syndrome, movement disorder, myelopathy, acute confusional state, anxiety disorder, cognitive dysfunction, mood disorder, psychosis, aseptic meningitis) and 7 PNS syndromes (Guillain-Barré syndrome, autonomic disorder, mononeuropathy, myasthenia gravis, cranial neuropathy, plexopathy, polyneuropathy).
Key Identifiers
| System | Identifier |
|---|---|
| MONDO | MONDO:0007915 (Systemic lupus erythematosus) |
| ICD-10 | M32.1 (SLE with organ or system involvement); G99.8* (Other specified disorders of nervous system in diseases classified elsewhere) |
| ICD-11 | 4A40.6 (Systemic lupus erythematosus with neuropsychiatric involvement) |
| MeSH | D020945 (Lupus Vasculitis, Central Nervous System) |
| OMIM | 152700 (Systemic Lupus Erythematosus) |
| Orphanet | ORPHA:536 (Systemic lupus erythematosus) |
Synonyms and Alternative Names
- Neuropsychiatric lupus (NP-lupus)
- Cerebral lupus / CNS lupus / Neurolupus
- Lupus cerebritis
- Central nervous system lupus
- Neuropsychiatric SLE (NPSLE)
Information Sources
This characterization is derived from aggregated disease-level resources including systematic reviews, meta-analyses, prospective cohort studies (GLADEL, CSTAR, LUMINA, 1000 Faces of Lupus), and registry data, supplemented by individual patient case series and mechanistic studies in animal models.
2. Etiology
Disease Causal Factors
NPSLE is a multifactorial autoimmune disorder with no single causative factor. Its etiology involves the interplay of genetic susceptibility, environmental triggers, hormonal influences, and dysregulated immune responses that collectively lead to autoimmune attack on neural tissues.
Genetic Risk Factors
Multiple genetic polymorphisms have been associated with NPSLE susceptibility:
| Gene/Locus | Variant | Association | Reference |
|---|---|---|---|
| TNFAIP3 | rs5029939 (CG genotype) | Significantly associated with neuropsychiatric manifestations (p<0.05) | PMID: 35382378 |
| TNF-α | -238 G/A (A allele) | Associated with neuropsychiatric impairment (p=0.036) | PMID: 41039983 |
| IL17RA | rs2895332 | Associated with NPSLE susceptibility in pediatric lupus nephritis | PMID: 39904110 |
| IL23R | rs10889677 | Associated with NPSLE susceptibility in pediatric lupus nephritis | PMID: 39904110 |
| FCGR3A | rs396991 | Associated with NPSLE susceptibility in pediatric lupus nephritis | PMID: 39904110 |
| HLA region | Multiple alleles | MHC region is the most significant genetic risk factor for autoimmunity onset | PMID: 42123548 |
A Korean GWAS identified novel NPSLE-specific loci with functional roles in brain regions, suggesting genetic variants may specifically predispose to neuropsychiatric over other SLE manifestations (PMID: 41062154). Importantly, schizophrenia polygenic risk scores showed no association with NPSLE (OR 1.04, 95% CI 0.87–1.26), indicating distinct genetic architectures between lupus psychosis and primary psychiatric illness (PMID: 34599046).
The genetic architecture of NPSLE is polygenic/multifactorial, with incomplete penetrance and variable expressivity. No single Mendelian gene causes NPSLE, though rare monogenic lupus (e.g., complement deficiencies C1q, C2, C4) can present with neuropsychiatric features.
Environmental Risk Factors
- UV radiation: Established environmental trigger that interacts with genetic susceptibility to initiate SLE; UV exposure can precipitate flares including neuropsychiatric events (PMID: 27306639)
- Epstein-Barr virus (EBV) infection: EBV-positive childhood SLE patients had significantly higher frequencies of neurological symptoms (66.2% vs 45.2%) compared to EBV-negative patients (PMID: 41668759)
- Vitamin D deficiency: Associated with neuropsychiatric manifestations; preclinical models demonstrate neuroprotective and barrier-stabilizing actions of vitamin D analogs (PMID: 41157255)
- Adverse childhood experiences (ACEs): Associated with NPSLE (adjusted OR=3.40, 95% CI 1.55–7.78, p=0.003) — a novel finding with important clinical implications (PMID: 42009372)
- Hormonal factors: Female sex hormones (estrogen) contribute to SLE susceptibility; SLE has a ~9:1 female:male ratio
- Smoking: Associated with increased SLE disease activity and damage (PMID: 30657064)
- Toluene exposure: Neurological symptoms may mimic NPSLE (PMID: 23956915)
- Seasonal patterns: Vitamin D nadir in late winter/early spring correlates with increased SLE activity (PMID: 28624334)
Protective Factors
- Hydroxychloroquine (HCQ): Protective against seizures (HR=0.35, 95% CI 0.15–0.80, p=0.0131) (PMID: 17875548); antimalarials reduce overall damage accrual (PMID: 41739063)
- Vitamin D supplementation: Safely corrects deficiency with signals of benefit for selected outcomes (PMID: 41157255)
Gene-Environment Interactions
Genetic interactions with environmental factors, particularly UV light exposure, EBV infection, and hormonal factors, initiate disease, resulting in immune dysregulation at the level of cytokines, T cells, B cells, and macrophages (PMID: 27306639). Epigenetic modifications (DNA methylation, histone modifications) serve as a critical interface: hypomethylation of the HTR1A promoter region with overexpression of HTR1A mRNA in SLE peripheral blood lymphocytes directly links immune dysregulation to serotonergic signaling (PMID: 21382916). KDM6 lysine demethylases fine-tune transcription of pro- and anti-inflammatory genes, influencing Th17 cell expansion and autoimmunity (PMID: 40516332).
3. Phenotypes
Neuropsychiatric Syndrome Prevalence
The 19 ACR-defined NPSLE syndromes and their approximate frequencies are presented below:
Adults (based on PMID: 11971089; PMID: 11327248):
| Syndrome | Frequency (%) | HPO Term |
|---|---|---|
| Headache | 4–57% | HP:0002315 (Headache) |
| Cognitive dysfunction | 21–80% | HP:0100543 (Cognitive impairment) |
| Mood disorder | 6–47% | HP:0000716 (Depression) |
| Anxiety disorder | 7–24% | HP:0000739 (Anxiety) |
| Seizure disorder | 9–28% | HP:0001250 (Seizures) |
| Cerebrovascular disease | 2–19% | HP:0002637 (Cerebral ischemia) |
| Psychosis | 5–23% | HP:0000709 (Psychosis) |
| Acute confusional state | 1–16% | HP:0001289 (Confusion) |
| Polyneuropathy | 1–22% | HP:0001271 (Polyneuropathy) |
| Movement disorder | 1–9% | HP:0100022 (Movement abnormality) |
| Myelopathy | 4–8% | HP:0002196 (Myelopathy) |
| Cranial neuropathy | 1–3% | HP:0001291 (Cranial nerve palsy) |
| Demyelinating syndrome | 1–3% | HP:0007305 (CNS demyelination) |
| Aseptic meningitis | 1–5% | HP:0002581 (Recurrent meningitis) |
| Mononeuropathy | 1–8% | HP:0007002 (Mononeuropathy) |
| Guillain-Barré syndrome | 0.5–2.5% | HP:0007166 (Paresthesia/tingling) |
Childhood-onset SLE (meta-analysis, n=1463; PMID: 31022053): headache 52.2%, seizure disorders 48.6%, cognitive dysfunction 32.9%, mood disorder 28.3%, psychosis 22.7%, cerebrovascular disease 19.5%, acute confusional state 15.7%, movement disorder 9.4%, anxiety disorder 7.2%.
Phenotype Characteristics
- Age of onset: Most commonly young adult (20–40 years); pediatric onset (<18 years) in ~15–20% of SLE cases, with higher NP damage (21% in early-onset <6 years) (PMID: 28134038)
- Severity: Variable — ranges from mild cognitive dysfunction and headache to life-threatening seizures, coma, and stroke
- Progression: Episodic and relapsing-remitting in most patients; some develop progressive cognitive decline
- Temporal pattern: NP events affect 50–60% at SLE onset or within the first year; however, the majority of NP symptoms did NOT first present around the time of SLE onset (PMID: 39429812)
Quality of Life Impact
Patients consider fatigue, anxiety, depression, pain, psychosis, and cognitive dysfunction to be among their most debilitating symptoms which most diminish their quality of life (PMID: 40818249). Standardized neuropsychological testing reveals: 21% normal, 43% mild impairment, 30% moderate impairment, 6% severe impairment (PMID: 11971089). Recognition and attribution of these frequently non-acute symptoms is difficult, resulting in underassessment and underdiagnosis.
4. Genetic/Molecular Information
Susceptibility Genes and Variants
NPSLE is a polygenic complex trait without classic Mendelian inheritance. Key susceptibility genes include:
- TNFAIP3 (A20): rs5029939 CG genotype — involved in NF-κB signaling regulation (PMID: 35382378)
- TNF-α: Promoter polymorphism -238 G/A — modulates TNF-α expression (PMID: 41039983)
- IL17RA / IL23R: Th17 pathway genes — rs2895332 and rs10889677 (PMID: 39904110)
- FCGR3A: Fc-gamma receptor — rs396991 — modulates immune complex clearance (PMID: 39904110)
- IRF5: Interferon regulatory factor 5 — associated with SLE susceptibility and organ damage (PMID: 41039983)
- HLA class II alleles: MHC region variants — strongest genetic risk factor for SLE overall (PMID: 42123548)
Epigenetic Information
- DNA hypomethylation: Global DNA hypomethylation in SLE T cells; HTR1A promoter hypomethylation leads to serotonin receptor overexpression (PMID: 21382916)
- Histone modifications: KDM6A/KDM6B demethylases regulate H3K27me2/3, influencing Th17 expansion and autoimmunity (PMID: 40516332)
- Glycosylation epigenetics: Epigenetic regulation of glycogenes affects immune function in SLE (PMID: 34495535)
- No chromosomal abnormalities specific to NPSLE have been identified
5. Environmental Information
Environmental Factors
| Factor | Evidence | Reference |
|---|---|---|
| UV radiation | Triggers SLE flares including NP events | PMID: 27306639 |
| Toluene/solvents | Can cause NP symptoms mimicking NPSLE | PMID: 23956915 |
| Adverse childhood experiences | OR=3.40 for NPSLE | PMID: 42009372 |
Infectious Agents
- Epstein-Barr virus (EBV) (NCBI Taxon: 10376): Established trigger; molecular mimicry with self-antigens; EBV-positive childhood SLE patients had 66.2% neurological symptoms vs 45.2% EBV-negative (PMID: 41668759)
- Varicella-Zoster virus (HZ): Higher HZ incidence in SLE with NP manifestations; psychosis and seizures associated with shorter time to HZ onset (PMID: 41871917)
- Opportunistic infections (Listeria, fungi): CNS infections can mimic NPSLE in immunosuppressed patients (PMID: 41399085)
6. Mechanism / Pathophysiology
Central Pathogenic Axis: Type I IFN and BBB Disruption
The pathogenesis of NPSLE is an integrated neuroimmune process with two major mechanistic subtypes:
PATHOGENIC CASCADE — DIFFUSE NPSLE (Inflammatory)
Self-nucleic acids → TLR7/9 activation → pDC activation
↓
Type I IFN overproduction (IFN-α/β)
↓
Blood-Brain Barrier disruption ←── Anti-Sm antibodies
↓
┌─────────────────────────┼─────────────────────────┐
↓ ↓ ↓
Autoantibodies enter CNS Cytokines enter CNS Immune cells enter CNS
(anti-NMDAR, anti-ribo P) (IL-6, IFN-α, TNF-α) (neutrophils/NETs, T cells)
↓ ↓ ↓
└─────────────────────────┼─────────────────────────┘
↓
Microglial activation (M1 phenotype)
Astrocyte reactivity (A1 phenotype)
↓
┌─────────────────────────┼─────────────────────────┐
↓ ↓ ↓
Synaptic loss/ Tryptophan → Kynurenine Impaired hippocampal
excitotoxicity metabolic shift (IDO-1↑) neurogenesis
(NMDAR dysfunction) (QA/KA ratio ↑, (via IL-6, IL-18)
serotonin ↓)
↓ ↓ ↓
└─────────────────────────┼─────────────────────────┘
↓
Cognitive dysfunction, depression, psychosis, seizures
PATHOGENIC CASCADE — FOCAL NPSLE (Vascular)
Antiphospholipid antibodies (aPL) → Endothelial activation
↓
┌─────────────────────────┼─────────────────────────┐
↓ ↓ ↓
Macro/microvascular Complement activation Immune complex
thrombosis (C3, C5a) deposition
↓ ↓ ↓
└─────────────────────────┼─────────────────────────┘
↓
Cerebrovascular events
(stroke, TIA, venous thrombosis)
Key Mechanistic Findings
1. Type I IFN as Central Driver: "Aberrant activation of innate immunity by self-nucleic acids and consequent overproduction of Type I interferons (IFN-I) constitute a central pathogenic axis in NPSLE" (PMID: 41989680). The BBB breach "permits peripheral autoimmune mediators—including pathogenic autoantibodies (e.g., anti-NMDAR, anti-ribosomal P), pro-inflammatory cytokines (e.g., Type I IFN, IL-6), and innate immune cells such as neutrophils forming Neutrophil Extracellular Traps (NETs)—to enter the central nervous system" (PMID: 41608446).
2. Early Microglial Activation Precedes BBB Disruption: A critical finding from NZB/W-F1 mice demonstrates that "at the prenephritic stage, BBB is intact yet mice exhibit hippocampus-related behavioural deficits recapitulating the human diffuse neuropsychiatric disease. This phenotype is accounted by disrupted hippocampal neurogenesis with hiNSCs exhibiting increased proliferation combined with decreased differentiation and increased apoptosis in combination with microglia activation" (PMID: 36898766). This challenges the traditional paradigm that BBB disruption is required for NPSLE onset.
3. Tryptophan-Kynurenine Metabolic Reprogramming: IFNγ drives diversion of tryptophan metabolism away from serotonin toward the kynurenine pathway, with "increased quinolinic acid/kynurenic acid (QA/KA) ratio and upregulation of indoleamine 2,3-dioxygenase-1" (PMID: 41869319). This provides a molecular explanation for depression and mood disorders in NPSLE.
4. Spatial IFN Signatures: Single-nucleus sequencing and spatial transcriptomics revealed that "interferon-stimulated genes (ISGs) were among the most highly upregulated genes" and "the type 1 interferon signature is enriched as spatially distinct patches within the brain parenchyma" (PMID: 37369340).
5. Choroid Plexus T Cell Infiltration: scRNA-seq identified clonal CD8+ T cells in the choroid plexus with a CDR3 sequence matching "a published T-cell receptor sequence with specificity for myelin basic protein. Systemic blockade of VLA-4, the cognate ligand of VCAM, resulted in significant resolution of the ChP immune cell infiltration and attenuation of the depressive phenotype" (PMID: 38531610).
6. Endothelial Dysfunction: "Cardiovascular disease (CVD) and neuropsychiatric manifestations are common in patients with SLE, often sharing a vascular origin with endothelial dysfunction central to their development" (PMID: 41795008). Focal neurologic symptoms result from "vascular injury induced by circulating immune complex, occlusive vasculopathy as a result of endothelial cell activation induced by cytokines and complement activation, or macro- and microvascular thrombosis induced by antiphospholipid antibodies" (PMID: 12491066).
Autoantibody-Specific Mechanisms
| Autoantibody | Target | NPSLE Manifestation | Mechanism | Reference |
|---|---|---|---|---|
| Anti-NMDAR (anti-NR2) | NMDA receptor | Cognitive dysfunction, mood disorders | Excitotoxic neuronal injury | PMID: 29846157 |
| Anti-ribosomal P | Ribosomal P proteins | Psychosis, depression | Neuronal apoptosis | PMID: 26524895 |
| Anti-Sm | Smith antigen | BBB disruption (ACS) | BBB permeability increase (p=0.0040) | PMID: 29846157 |
| Anti-β2GPI | β2-glycoprotein I | Psychosis (F=6.092, p=0.015) | Thrombotic/inflammatory | PMID: 38997542 |
| Anti-cardiolipin | Cardiolipin | Demyelinating syndrome (F=6.637, p=0.011) | Thrombotic vasculopathy | PMID: 38997542 |
| Antiphospholipid (LAC, aCL) | Phospholipids | Cerebrovascular disease | Macro/microthrombosis | PMID: 11327248 |
Key Molecular Pathways (with GO terms)
- Type I interferon signaling (GO:0060337)
- NF-κB signaling (GO:0038061)
- Tryptophan-kynurenine metabolism (GO:0019441 — tryptophan catabolic process to kynurenine)
- Complement activation (GO:0006956)
- Apoptotic process (GO:0006915)
- Microglial cell activation (GO:0001774)
- Neuroinflammatory response (GO:0150076)
- Neurogenesis (GO:0022008)
Cell Types Involved (with CL terms)
- Microglia (CL:0000129) — M1 polarization, synaptic pruning
- Astrocytes (CL:0000127) — A1 neurotoxic phenotype
- Neurons (CL:0000540) — Target of excitotoxicity
- Plasmacytoid dendritic cells (CL:0000784) — IFN-α production
- CD8+ T cells (CL:0000625) — Choroid plexus infiltration
- Neutrophils (CL:0000775) — NETosis, BBB disruption
- B cells / Plasma cells (CL:0000236 / CL:0000786) — Autoantibody production
- Neural stem cells (CL:0000047) — Impaired neurogenesis
- Endothelial cells (CL:0000115) — BBB component, activation/dysfunction
Molecular Profiling
Transcriptomics: ISGs among most highly upregulated genes in brain (hindbrain, hippocampus) of NPSLE mice; gene pathways for cellular interaction and neuronal development repressed among astrocytes, oligodendrocytes, and neurons (PMID: 37369340).
Metabolomics: Cortical tryptophan-to-kynurenine diversion; increased QA/KA ratio; serotonin depletion; IDO-1 upregulation (PMID: 41869319). CSF HVA, SDF-1α, and SCGF-1β reduced in SLE patients with depression (PMID: 36852847).
Proteomics/Biomarkers: Elevated CSF IL-6, PAI-1 in NPSLE; shedding of sVCAM-1, sICAM-1, sPECAM-1, S100B reflects BBB disruption (PMID: 35118639).
7. Anatomical Structures Affected
Organ Level
- Primary: Brain (UBERON:0000955), spinal cord (UBERON:0002240)
- Secondary: Kidney (lupus nephritis), skin, joints, heart, lungs, blood vessels
- Body systems: Nervous system (central and peripheral), immune system, cardiovascular system
Tissue and Cell Level
- Hippocampus (UBERON:0001954) — Neurogenesis disruption, cytokine overexpression, atrophy
- Cerebral cortex (UBERON:0000956) — White matter lesions, demyelination
- Choroid plexus (UBERON:0001886) — T cell infiltration, immune gateway
- Corpus callosum (UBERON:0002336) — White matter loss associated with elevated NfL (PMID: 34800169)
- Basal ganglia (UBERON:0002420) — Calcifications, movement disorders
- Limbic system — Mood and behavioral disturbances
- Blood-brain barrier (endothelial cells, astrocyte endfeet, pericytes) — Disruption as key pathogenic step
- Peripheral nerves — Polyneuropathy, mononeuropathy
Subcellular Level
- Mitochondria (GO:0005739) — Mitochondrial dysfunction
- Synapse (GO:0045202) — Synaptic loss and dysfunction
- Cell nucleus (GO:0005634) — Target of anti-nuclear antibodies
- Endoplasmic reticulum (GO:0005783) — Protein misfolding stress
- Extracellular space (GO:0005615) — Neutrophil extracellular traps (NETs)
Lateralization
Generally bilateral; cerebrovascular events may be unilateral. Asymmetric presentation possible in focal NPSLE.
8. Temporal Development
Onset
- Typical age: Young adult (20–40 years), peak incidence during reproductive years
- Childhood onset: 15–20% of SLE cases; early-onset (<6 years) has highest NP damage (21%) and mortality (15%) (PMID: 28134038)
- Onset pattern: Variable — acute (seizures, psychosis, stroke), subacute (progressive cognitive decline), or insidious (mood changes, fatigue)
- Prodromal features: NP symptoms may be prodromal to SLE; 61% of SLE patients with hallucinations reported increasingly disrupted dreaming sleep (nightmares) prior to hallucination onset (PMID: 39429812)
Progression
- Disease course: Episodic/relapsing-remitting predominant; some patients develop progressive cognitive decline
- Duration: Chronic lifelong (in the context of SLE)
- Critical periods: 50–60% of NP events occur at SLE onset or within the first year; seizures tend to occur early; 48% of childhood SLE deaths occurred within first 2 years (PMID: 28134038)
- Remission: Treatment-induced remission achievable in most cases; spontaneous remission uncommon for severe manifestations
9. Inheritance and Population
Epidemiology
| Measure | Estimate | Source |
|---|---|---|
| SLE prevalence | 20–150 per 100,000 (varies by population) | Multiple registries |
| NPSLE prevalence among SLE | 6.4–80% (definition-dependent) | PMID: 22595642 |
| NPSLE prevalence (ACR attribution) | ~30–40% | PMID: 41307246 |
| Childhood SLE incidence (China) | 3.97 per 100,000 person-years | PMID: 39299747 |
Inheritance Pattern
- Multifactorial/polygenic — no Mendelian pattern
- Incomplete penetrance — genetic susceptibility loci confer risk but do not guarantee disease
- Variable expressivity — identical genetic backgrounds can produce different NP manifestations
- No genetic anticipation documented
Population Demographics
- Sex ratio: ~9:1 female:male for SLE overall; neuropsychiatric manifestations more equal across sexes
- Ethnic groups: Higher prevalence and severity in African Americans, Hispanic Americans, Asians; Aboriginal populations show nearly 2-fold increase in NPSLE frequency (PMID: 22595642)
- Age distribution: Peak onset in 2nd–4th decades; childhood SLE shows peripubertal increase (girls: +1.64/100,000/year per year of age increase) (PMID: 39299747)
10. Diagnostics
Clinical Tests
Laboratory Tests: - Complete blood count (cytopenias) - Complement levels (C3, C4 — typically decreased) - Anti-dsDNA, ANA, anti-Sm, anti-ribosomal P, anti-NMDAR antibodies - Antiphospholipid antibodies (aCL, LAC, anti-β2GPI) - CSF analysis: IL-6, Qα2MG (BBB disruption marker), IgG index, oligoclonal bands - Plasma neurofilament light (NfL) — correlates with CSF NfL (r=0.72, p<0.001) and brain atrophy (PMID: 34800169)
Biomarkers:
| Biomarker | Specimen | Significance | Reference |
|---|---|---|---|
| CSF IL-6 | CSF | Elevated in NPSLE, especially ACS | PMID: 29036223 |
| Qα2MG | CSF/serum | BBB disruption marker | PMID: 29036223 |
| Intrathecal PAI-1 | CSF | Elevated in NPSLE (p<0.05), correlates with neuronal damage | PMID: 19565516 |
| Plasma NfL | Plasma | Neuronal damage marker, correlates with cognitive impairment | PMID: 36494778 |
| CSF HVA | CSF | Reduced in SLE depression (p=0.04) | PMID: 36852847 |
| sVCAM-1, sICAM-1, S100B | Serum | BBB damage profile markers | PMID: 35118639 |
Imaging: - Brain MRI: T2/FLAIR hyperintensities in cerebral white matter; diffusion-weighted imaging for acute lesions (PMID: 41638970) - DTI (diffusion tensor imaging): Abnormal white matter microstructure even in non-NPSLE SLE (PMID: 32349105) - FDG-PET: Altered brain metabolism - DCE-MRI: Increased BBB permeability - Volumetric MRI: Brain atrophy, hippocampal volume loss
Electrophysiology: EEG for seizure evaluation; EMG/NCS for peripheral neuropathy
Neuropsychological Testing: ACR-SLE battery; MADRS for depression screening (PMID: 36852847)
Clinical Criteria
- 1999 ACR nomenclature: 19 NP syndrome case definitions (standard)
- 2019 EULAR/ACR classification criteria: SLE classification with NP attribution
- Attribution models: SLICC A, SLICC B, ACR — prevalence varies significantly by model used (PMID: 22595642)
- 2023 EULAR management recommendations: Updated guidance for NPSLE diagnosis and treatment (PMID: 37827694)
NPSLE Subtypes by Clustering
Unsupervised clustering of 152 NPSLE patients identified two subgroups: Cluster 1 (23.7%) with cerebrovascular injury as predominant manifestation and higher antiphospholipid antibody positivity, and Cluster 2 with CNS-inflammatory manifestations (PMID: 41969819).
Differential Diagnosis
- Multiple sclerosis
- Primary CNS vasculitis
- CNS infections (bacterial, viral, fungal — especially in immunosuppressed patients)
- Primary psychiatric disorders
- Neuromyelitis optica spectrum disorders
- Thrombotic thrombocytopenic purpura
- Drug-induced neuropsychiatric effects (corticosteroid psychosis)
- Posterior reversible encephalopathy syndrome (PRES)
Genetic Testing
Genetic testing is not routinely indicated for NPSLE diagnosis. GWAS and polygenic risk scoring remain research tools. Testing for complement deficiencies (C1q, C2, C4) may be considered in early-onset or severe SLE.
11. Outcome/Prognosis
Survival and Mortality
- NPSLE is the 2nd leading cause of SLE mortality (14.8% of deaths) after infection (30.1%) in Chinese cohorts (PMID: 28030595)
- Independent predictor of mortality: NP involvement HR 2.03 (≤1 year) and HR 1.91 (>1 year) (PMID: 28030595)
- Overall SLE 5-year survival: 95.7% (CSTAR registry) (PMID: 36465068)
- Childhood SLE mortality: 0.7% in-hospital mortality; NPSLE is an independent risk factor for ICU admission (HR 2.10) (PMID: 39299747)
- Early-onset SLE (<6 years): Highest mortality rate (15%) and highest NP damage (21%) (PMID: 28134038)
Organ Damage
NP damage is among the top 3 organ damage domains in SLE: - CSTAR registry: 12.2% of total organ damage (PMID: 36465068) - GLADEL cohort: 10.8% of total organ damage (PMID: 41739063) - Most frequent NP damages: cognitive dysfunction, valvulopathies, angina pectoris (PMID: 27889859)
Prognostic Factors
- Poor prognosis: Male sex, late disease onset, delayed diagnosis (>1 year), baseline organ damage, high SLEDAI, high cumulative glucocorticoid dose
- Better prognosis: Early diagnosis, antimalarial use, early immunosuppression, low glucocorticoid doses
- Prognostic biomarkers: Plasma NfL (neuronal damage), CSF IL-6 (neuroinflammation), anti-Sm (BBB disruption)
12. Treatment
Pharmacotherapy
First-line (all SLE patients): - Hydroxychloroquine (CHEBI:5801): 5 mg/kg/day — recommended for ALL SLE patients (PMID: 37827694); protective against seizures HR=0.35 (p=0.0131) (PMID: 17875548); reduces overall damage accrual (PMID: 41739063) - MAXO:0001001 (pharmaceutical treatment)
Acute severe NPSLE: - Methylprednisolone pulse (CHEBI:6888): 500–1000 mg IV daily x 3 days, followed by oral taper - MAXO:0000750 (glucocorticoid therapy) - Cyclophosphamide (CHEBI:4026): IV pulses for severe NPSLE (seizures, psychosis, myelopathy, acute confusional state) - MAXO:0000750 (immunosuppressive therapy) - Intravenous immunoglobulin (IVIG): Adjunctive for severe cases - MAXO:0000376 (immunoglobulin therapy) - Plasma exchange (PLEX): For refractory cases - MAXO:0000127 (plasmapheresis)
Refractory NPSLE: - Rituximab (anti-CD20): 94.1% (16/17) refractory NPSLE patients achieved significant clinical improvement; none relapsed during median 45-month follow-up (PMID: 42115580) - MAXO:0001298 (B cell depletion therapy)
Emerging therapies: - Anifrolumab (anti-IFNAR1): Successful rescue therapy in 7/8 inflammatory NPSLE cases; "Blocking the IFNAR1 with anifrolumab provides a direct rationale for treating this subset of NPSLE" (PMID: 41756273) - Belimumab (anti-BAFF/BLyS): Approved for moderate-severe SLE; potential for NPSLE - VLA-4 blockade: Preclinical evidence — resolved choroid plexus infiltration and attenuated depressive phenotype (PMID: 38531610) - Captopril/ACE inhibitors: Potential neuroprotective agents preserving BBB function (PMID: 41831216) - GSK-J4 (KDM6 inhibitor): Small-molecule epigenetic therapy showing promise in models of chronic inflammation (PMID: 40516332)
Antithrombotic therapy (for focal/vascular NPSLE): - Anticoagulation with warfarin or direct oral anticoagulants for antiphospholipid-associated events - Aspirin for secondary prevention - MAXO:0000003 (anticoagulation therapy)
Supportive/Rehabilitative: - Cognitive rehabilitation, physical therapy, occupational therapy - Antidepressants (SSRIs) for mood disorders - Antiepileptic drugs for seizure control - Neuropsychological monitoring - MAXO:0000015 (cognitive behavioral therapy)
Treatment Algorithm
NPSLE Treatment Decision Tree:
1. ALL SLE patients → Hydroxychloroquine 5 mg/kg/day
2. Mild NPSLE (headache, mild cognitive, mild mood)
→ Optimize HCQ + Low-dose glucocorticoids + Supportive care
3. Moderate NPSLE (seizures, moderate cognitive, polyneuropathy)
→ Glucocorticoids + Immunosuppressant (azathioprine/mycophenolate)
→ Consider anticonvulsants for seizures
4. Severe NPSLE (psychosis, ACS, myelopathy, stroke)
→ Methylprednisolone pulse + Cyclophosphamide IV
→ IVIG or PLEX as adjunct
→ Distinguish inflammatory vs thrombotic:
- Inflammatory → Immunosuppression
- Thrombotic → Anticoagulation
5. Refractory NPSLE
→ Rituximab (94% response rate)
→ Anifrolumab for inflammatory NPSLE (emerging)
13. Prevention
Primary Prevention
- UV protection: Sunscreen, protective clothing for all SLE patients
- Smoking cessation: Reduces disease activity and flare risk
- Vitamin D optimization: Supplementation to maintain adequate levels (PMID: 41157255)
- Hydroxychloroquine: Protective against NP damage development (PMID: 41739063)
Secondary Prevention
- Regular neuropsychological screening: MADRS and cognitive testing for subclinical NP involvement (PMID: 36852847)
- Monitoring for prodromal symptoms: Disrupted dreaming/nightmares may precede psychosis and flares (PMID: 39429812)
- Serial NfL monitoring: Plasma NfL as non-invasive neuronal damage biomarker (PMID: 34800169)
- Advanced neuroimaging: Subclinical brain abnormalities detectable even in non-NPSLE SLE patients (PMID: 32349105)
Tertiary Prevention
- Minimize glucocorticoid exposure: Chronic high-dose glucocorticoids trigger chronic organ damage (PMID: 27889859)
- Target GC dose ≤5 mg/day prednisone equivalent (PMID: 37827694)
- Antimalarial adherence: Lower proportion accruing NP damage with antimalarials (40.6% vs 48.3%) (PMID: 41739063)
- Infection prophylaxis: Herpes zoster vaccination recommended (HZ incidence elevated in NPSLE patients) (PMID: 41871917)
- Cardiovascular risk management: Shared vascular pathology between CVD and NPSLE (PMID: 41795008)
14. Other Species / Natural Disease
Naturally Occurring Disease
- Canine SLE (NCBI Taxon: 9615 — Canis lupus familiaris): Naturally occurring SLE reported in multiple dog breeds; primarily cutaneous manifestations (discoid LE, vesicular CLE, exfoliative CLE); neurological manifestations rare but documented (PMID: 29669547). Affected breeds include German Shepherd, Shetland Sheepdog, Collie, and others. ANA testing in dogs can be confounded by vectorborne infections (Bartonella, Ehrlichia, Leishmania) (PMID: 14765731).
Comparative Biology
- Canine distemper virus causes demyelination and CNS inflammation with microglial/astrocyte activation analogous to NPSLE; MIF (macrophage migration inhibitory factor) is elevated in affected brain tissue (PMID: 31981823)
- Chronic Trypanosoma brucei infection induces meningeal ectopic lymphoid aggregates with GC-like B cells producing autoantibodies against brain antigens including myelin basic protein — paralleling choroid plexus findings in NPSLE (PMID: 37983289)
15. Model Organisms
Key Mouse Models
| Model | Type | Key Features | NP Phenotype | Limitations | Reference |
|---|---|---|---|---|---|
| MRL/MpJ-Fas^lpr^ (MRL/lpr) | Spontaneous lupus | Gold standard; Fas mutation; anti-dsDNA, anti-NMDAR, anti-P antibodies | Depression (5 weeks F, 18 weeks M), anxiety, cognitive deficits, microglial activation | Accelerated by Fas deficiency (not typical of human SLE) | PMID: 20800292; PMID: 25183233 |
| NZB/W-F1 | Spontaneous lupus | F1 hybrid; lupus nephritis dominant | Hippocampal neurogenesis disruption, microglial activation with INTACT BBB at prenephritic stage | Less pronounced NP phenotype | PMID: 36898766 |
| CReCOM | Spontaneous lupus | Behavioral deficits BEFORE systemic autoimmunity | Reduced brain volumes, decreased vascular integrity, NP-SLE microglia signature (DAM-like), increased synaptic uptake | Relatively new model | PMID: 32174913 |
| BXSB | Spontaneous lupus | Y-linked autoimmune accelerator | Spontaneous SLE with NP features; hippocampal cytokine overexpression | Male-predominant disease | PMID: 14975498 |
| Atherosclerosis-prone lupus mice | Induced | Combined lupus/atherosclerosis | Cognitive deficits; responsive to resveratrol via A2A/SIRT1/VEGF/CX3CL1 | Artificial combination | PMID: 36081818 |
Key Findings from Animal Models
The MRL/lpr model demonstrates that "females exhibited significant depression as early as 5 weeks (at which time elevated levels of autoantibodies were already present), as compared to MRL/lpr males, where depression was noted only at 18 weeks. Depression was significantly correlated with autoantibodies against nuclear antigens, NMDA receptor, and ribosomal P" (PMID: 20800292).
The CReCOM model provides evidence that "SLE-prone mice develop NP-SLE, including behavioral deficits prior to systemic autoimmunity, reduced brain volumes, decreased vascular integrity, and brain-infiltrating leukocytes. NP-SLE microglia exhibit numerical expansion, increased synaptic uptake, and a more metabolically active phenotype" (PMID: 32174913).
The NZB/W-F1 model reveals that early NP features can occur with intact BBB: "at the prenephritic stage, BBB is intact yet mice exhibit hippocampus-related behavioural deficits" mediated by IL-6 and IL-18-induced neural stem cell apoptosis and microglial activation (PMID: 36898766).
Key Findings Summary
F001: NPSLE Prevalence and Heterogeneity
NPSLE affects 30–56% of SLE patients with 19 distinct syndromes. Prevalence varies enormously by definition used: 6.4% (ACR classification alone) to 80% (comprehensive ACR case definitions) (PMID: 22595642). This heterogeneity is a fundamental challenge for research and clinical management.
F002: Type I IFN/BBB Pathogenic Axis
The central pathogenic cascade involves Type I IFN overproduction → BBB disruption → CNS entry of autoantibodies and immune cells → neuroinflammation (PMID: 41989680; PMID: 41608446). However, early microglial activation can occur BEFORE BBB disruption (PMID: 36898766), challenging traditional models.
F003: Autoantibody-Specific Mechanisms
Different autoantibodies mediate distinct manifestations: anti-Sm drives BBB disruption (p=0.0040); anti-β2GPI associates with psychosis (p=0.015); anti-cardiolipin with demyelination (p=0.011) (PMID: 29846157; PMID: 38997542).
F004: Genetic Susceptibility
Multiple polymorphisms (TNFAIP3, TNF-α, IL17RA, IL23R, FCGR3A) confer NPSLE risk, but schizophrenia PRS shows no association (OR 1.04), confirming distinct genetic architecture from primary psychosis.
F005: NPSLE Mortality Impact
NPSLE is the 2nd leading cause of SLE death (14.8%), with NP involvement being an independent mortality predictor (HR ~2.0) (PMID: 28030595).
F006: Tryptophan-Kynurenine Metabolic Shift
IFNγ drives tryptophan away from serotonin toward kynurenine, increasing the neurotoxic QA/KA ratio — providing molecular explanation for NPSLE depression (PMID: 41869319).
F009: Treatment Efficacy
Rituximab achieves 94% response in refractory NPSLE with no relapse over median 45 months (PMID: 42115580); HCQ protects against seizures (HR=0.35) (PMID: 17875548); anifrolumab shows promise for inflammatory NPSLE (PMID: 41756273).
F013: Single-Cell/Spatial Transcriptomics Breakthroughs
Spatially distinct IFN patches in brain parenchyma (PMID: 37369340) and choroid plexus T cell infiltration with myelin-specific clones responsive to VLA-4 blockade (PMID: 38531610) represent paradigm-shifting findings.
F014: Prodromal Symptoms
NP symptoms may be prodromal to SLE; disrupted dreaming precedes hallucinations in 61% of patients. The majority of NP symptoms did NOT first present around time of SLE onset, challenging prevailing clinical assumptions (PMID: 39429812).
Evidence Base
Landmark Reviews and Studies
| Paper | PMID | Key Contribution |
|---|---|---|
| Pathogenesis and therapeutic strategies for NPSLE centered on innate immune activation | 41989680 | Establishes Type I IFN as central pathogenic axis |
| Advancements in understanding neuropsychiatric lupus with single-cell resolution | 41608446 | Comprehensive neuroimmune cascade; prevalence data |
| Recent advances in pathogenesis of NPSLE | 41872002 | Neuroimmune framework for barrier-associated mechanisms |
| EULAR 2023 management recommendations | 37827694 | Current treatment guidelines |
| Spatial enrichment of type 1 IFN in NPSLE brain | 37369340 | First spatial transcriptomic evidence in NPSLE |
| Characterisation of choroid plexus-infiltrating T cells | 38531610 | Myelin-specific T cells; VLA-4 therapeutic target |
| Microglia activation with intact BBB | 36898766 | Early NP features precede BBB disruption |
| IFNγ-associated immune-metabolic remodeling | 41869319 | Tryptophan-kynurenine shift mechanism |
| NP syndromes using standardized definitions | 11971089 | Prevalence of all 19 syndromes |
| Rituximab in refractory NPSLE | 42115580 | 94% response rate |
| NP prodromes (INSPIRE study) | 39429812 | Prodromal symptoms; disrupted dreaming |
Limitations and Knowledge Gaps
-
Attribution challenge: No gold-standard biomarker distinguishes NPSLE from non-SLE neuropsychiatric disease. Current attribution models (ACR, SLICC) yield highly variable prevalence estimates (6.4–80%), hindering clinical research and epidemiological comparisons.
-
Absence of randomized clinical trials: All current treatment strategies for NPSLE are derived from clinical experience and extrapolation from other SLE manifestations or non-SLE neuropsychiatric disease. No RCTs have been conducted specifically for NPSLE.
-
Heterogeneity: The 19 distinct syndromes likely have different pathogenic mechanisms, making "NPSLE" a heterogeneous umbrella rather than a single entity. The clustering into inflammatory vs vascular subtypes is a step forward but likely oversimplified.
-
Translational gaps: Most mechanistic insights come from mouse models (MRL/lpr, NZB/W-F1, CReCOM), which imperfectly recapitulate human disease. The Fas mutation in MRL/lpr is not representative of typical human SLE genetics.
-
CSF accessibility: Key diagnostic biomarkers (IL-6, Qα2MG, PAI-1) require lumbar puncture, limiting routine clinical use. Plasma NfL is promising but not specific to NPSLE.
-
Cognitive dysfunction underassessment: Formal neuropsychological testing is rarely performed in acute settings; subclinical cognitive impairment likely affects many more patients than currently recognized.
-
Epigenetic mechanisms: The role of DNA methylation, histone modifications, and non-coding RNAs in NPSLE pathogenesis is still poorly characterized compared to other SLE manifestations.
-
Long-term outcomes: Limited data on long-term cognitive trajectories and neurodegeneration in NPSLE survivors.
Proposed Follow-up Experiments/Actions
-
Randomized controlled trial of anifrolumab in inflammatory NPSLE: Building on the promising case series data (PMID: 41756273), a properly powered RCT stratifying patients by inflammatory vs vascular subtype is urgently needed.
-
Prospective validation of prodromal dreaming disturbance: The INSPIRE finding that disrupted dreaming precedes psychosis (PMID: 39429812) warrants prospective validation as a clinical early warning system.
-
Multi-omic biomarker panel development: Integration of plasma NfL, serum autoantibody profiles, and cytokine panels into a composite biomarker for NPSLE attribution and subtyping, avoiding lumbar puncture.
-
VLA-4 blockade clinical trial: Natalizumab (anti-VLA-4), already approved for MS, should be explored for inflammatory NPSLE based on preclinical evidence of choroid plexus T cell resolution (PMID: 38531610).
-
Human spatial transcriptomics: The spatial IFN patches identified in mouse brain (PMID: 37369340) need validation in human post-mortem NPSLE tissue to confirm translational relevance.
-
IDO-1 inhibitor trials: Given the tryptophan-kynurenine metabolic shift (PMID: 41869319), IDO-1 inhibitors or kynurenine pathway modulators could be explored as adjunctive therapy for NPSLE-associated depression.
-
Adverse childhood experience screening: Given the strong ACE-NPSLE association (OR=3.40) (PMID: 42009372), ACE screening should be integrated into SLE clinical care, with targeted psychosocial support.
-
Longitudinal neuroimaging cohort: Serial advanced MRI (DTI, DCE-MRI, volumetric) with paired plasma NfL and cognitive testing to define progression trajectories and treatment response markers.
Report generated from 5 investigative iterations, 16 confirmed findings, and 104+ reviewed publications. Last updated: 2026-05-16.