Autoimmune Autonomic Ganglionopathy (AAG) — Comprehensive Disease Characteristics Report
Executive summary
Autoimmune autonomic ganglionopathy (AAG) is a rare, immune-mediated disorder of peripheral autonomic failure affecting sympathetic, parasympathetic, and enteric systems, classically presenting with subacute-onset diffuse dysautonomia (e.g., orthostatic hypotension, anhidrosis, severe gastrointestinal and bladder dysfunction). Roughly half of clinically suspected cases have serum autoantibodies against the ganglionic nicotinic acetylcholine receptor (gAChR; typically α3-containing receptors), and antibody titers correlate with autonomic severity; immunotherapy (plasma exchange, IVIg, corticosteroids and steroid-sparing immunosuppression) can lead to objective improvement in many patients, though controlled trial data remain very limited. (iodice2009efficacyofimmunotherapy pages 1-3, golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2024autoimmuneautonomicneuropathy pages 2-3, koay2021multimodalbiomarkersquantify pages 1-8)
1. Disease information
1.1 Definition and current understanding
- AAG is an immune-mediated disorder with prominent/selective involvement of the peripheral autonomic nervous system, producing generalized autonomic failure and often orthostatic hypotension, anhidrosis, and parasympathetic dysfunction. (iodice2009efficacyofimmunotherapy pages 1-3)
- AAG is commonly described as “a disease of autonomic failure caused by ganglionic acetylcholine receptor (gAChR) autoantibodies” (direct abstract statement). (nakane2024autoimmuneautonomicneuropathy pages 11-12)
1.2 Synonyms / alternative names
Commonly used terms in the literature include: - Autoimmune autonomic ganglionopathy (AAG) (nakane2024autoimmuneautonomicneuropathy pages 11-12, iodice2009efficacyofimmunotherapy pages 1-3) - Autoimmune autonomic neuropathy (umbrella term often including AAG) (nakane2024autoimmuneautonomicneuropathy pages 11-12) - Subacute panautonomic failure / subacute autonomic neuropathy (historical discovery context for ganglionic nAChR antibodies) (vernino1998neuronalnicotinicach pages 4-6, vernino1998neuronalnicotinicach pages 3-4)
1.3 Key identifiers (OMIM/Orphanet/ICD/MeSH/MONDO)
- In the evidence retrieved for this run, explicit OMIM/Orphanet/ICD-10/ICD-11/MeSH/MONDO identifiers were not present in accessible full text excerpts; this entry should be completed by querying those dedicated ontology resources directly. (iodice2009efficacyofimmunotherapy pages 1-3, golden2019autoimmuneautonomicneuropathies pages 1-2)
1.4 Evidence sources
The characterization below is derived from: - Aggregated disease-level clinical cohorts and reviews (e.g., Japanese cohort n=80; seropositive cohort n=13) (nakane2018autoimmuneautonomicganglionopathy pages 6-8, koay2021multimodalbiomarkersquantify pages 1-8) - Primary discovery and pathophysiology studies (Neurology 1998 discovery of neuronal/ganglionic nAChR antibodies) (vernino1998neuronalnicotinicach pages 1-2, vernino1998neuronalnicotinicach pages 3-4) - Interventional/observational clinical evidence and trial registry information (Neurology 2009 immunotherapy case series; ClinicalTrials.gov NCT01522235) (iodice2009efficacyofimmunotherapy pages 1-3, NCT01522235 chunk 1)
2. Etiology
2.1 Primary causal factors (mechanistic)
Autoantibody-mediated ganglionic synaptic failure - The principal autoantigen is the ganglionic nicotinic acetylcholine receptor (gAChR), typically α3-containing receptors (often α3β4). Patient antibodies bind α3 and can reduce receptor currents in vitro, supporting pathogenicity. (golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2024autoimmuneautonomicneuropathy pages 2-3) - A 2024 mechanistic synthesis proposes a three-step pathogenic model: (1) antibody binding, (2) antibody-driven internalization/degradation reducing receptor number, and (3) functional blockade. (nakane2024autoimmuneautonomicneuropathy pages 2-3) - In a 2024 clinical utility review, AAG antibodies are described as acting “by preventing post‑synaptic depolarization, thereby blocking autonomic neurotransmission.” (loser2024autoantibodiesinneuromuscular pages 13-15)
Seronegative disease and heterogeneity - About ~50% of suspected AAG may be seronegative, and some evidence suggests possible antibody- vs cell-mediated subtypes, including steroid-responsive but IVIg/PLEX/rituximab-poorly responsive subsets. (mohapatra2024decodingautoimmuneautonomic pages 4-5, golden2019autoimmuneautonomicneuropathies pages 3-5)
2.2 Risk factors
- Robust genetic susceptibility loci or causal germline variants were not identified in the retrieved evidence; AAG is primarily treated as an acquired autoimmune condition. (golden2019autoimmuneautonomicneuropathies pages 1-2)
- Autoimmune comorbidity is common. In a seropositive cohort (n=13), 8/13 (62%) had other autoimmune diseases (e.g., hypothyroidism, inflammatory bowel disease, Addison’s, pernicious anemia). (koay2021multimodalbiomarkersquantify pages 8-13)
- Antecedent infection or events are reported in subsets (see Temporal Development). (nakane2018autoimmuneautonomicganglionopathy pages 6-8, koay2021multimodalbiomarkersquantify pages 8-13)
2.3 Protective factors / gene–environment interactions
- No protective genetic variants or specific gene–environment interaction evidence was present in the retrieved set; this remains a knowledge gap. (golden2019autoimmuneautonomicneuropathies pages 1-2)
3. Phenotypes
3.1 Core clinical phenotype (multi-domain autonomic failure)
AAG reflects diffuse autonomic failure across sympathetic, parasympathetic, and enteric domains. (iodice2009efficacyofimmunotherapy pages 1-3, golden2019autoimmuneautonomicneuropathies pages 1-2)
Common features and frequencies (cohort evidence) - Japanese seropositive cohort (n=80): - Orthostatic hypotension: 64/80 (80%) - Lower GI symptoms: 59/80 (74%) - Pupillary dysfunction: 21/80 (26%) - Sensory disturbance (dysesthesia/numbness): 37/80 (46%) - Extra-autonomic involvement overall: 67/80 (84%) - Gradual onset predominant: 62/80 (78%) - Antecedent events: 13/80 (16%) (nakane2018autoimmuneautonomicganglionopathy pages 6-8)
- Seropositive multimodal cohort (n=13):
- Impaired pupillary light constriction: 12/13 (92%); cholinergic supersensitivity in tested patients
- Postganglionic sudomotor dysfunction: 7/8 (88%)
- Urinary retention: 9/11 (82%); catheterisation needed 5/13 (38%)
- Xerophthalmia (reduced lacrimation): 9/11 (82%); xerostomia: 6/8 (75%)
- 31% had antecedent infections; 15% antecedent surgery (koay2021multimodalbiomarkersquantify pages 13-17, koay2021multimodalbiomarkersquantify pages 8-13, koay2021multimodalbiomarkersquantify pages 1-8)
3.2 Suggested HPO terms (non-exhaustive; map to patient-level data when available)
- Orthostatic hypotension (HP:0001278)
- Autonomic dysfunction (HP:0004398)
- Anhidrosis / hypohidrosis (HP:0000970 / HP:0000966)
- Urinary retention / neurogenic bladder (HP:0000016 / HP:0000010)
- Gastrointestinal dysmotility / constipation (HP:0002574 / HP:0002019)
- Xerostomia / keratoconjunctivitis sicca (HP:0000217 / HP:0001097)
- Abnormal pupillary light reflex / mydriasis (HP:0000615 / HP:0000611)
- Sensory neuropathy / paresthesia (HP:0000763 / HP:0003401)
(nakane2018autoimmuneautonomicganglionopathy pages 6-8, koay2021multimodalbiomarkersquantify pages 1-8)
3.3 Quality of life impact
Quantitative symptom and QoL instruments are used in AAG cohorts, including COMPASS-31 and SF-36. In one seropositive cohort (n=13), immunotherapy improved COMPASS-31 scores (total 52 → 17, P=.03) and SF-36 physical function (example data in figures), consistent with clinically meaningful functional improvement. (koay2021multimodalbiomarkersquantify pages 1-8, koay2021multimodalbiomarkersquantify pages 17-21)
4. Genetic / molecular information
4.1 Causal genes
- AAG is not primarily described as a Mendelian genetic disorder in retrieved evidence. However, the target receptor comprises subunits including α3 and typically β4; these correspond to receptor subunit genes (e.g., CHRNA3, CHRNB4), but the disease mechanism is autoimmune rather than inherited mutation-based in the cited cohorts/reviews. (golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2024autoimmuneautonomicneuropathy pages 2-3)
4.2 Pathogenic “variants”
- Not applicable as germline pathogenic variants were not implicated as causal in the retrieved clinical literature. (golden2019autoimmuneautonomicneuropathies pages 1-2)
4.3 Epigenetics / modifiers
- Not addressed in retrieved evidence.
5. Environmental information
5.1 Infectious or other triggers
- Antecedent infections/events are reported in subsets of cohorts (e.g., 31% antecedent infections in a seropositive cohort; 16% antecedent events in a Japanese cohort). (koay2021multimodalbiomarkersquantify pages 8-13, nakane2018autoimmuneautonomicganglionopathy pages 6-8)
6. Mechanism / pathophysiology
6.1 Causal chain (antibody-mediated archetype)
1) Immune tolerance break (often idiopathic; sometimes paraneoplastic context in early discovery cohorts) with production of antibodies to ganglionic nAChR (α3-containing receptor). (vernino1998neuronalnicotinicach pages 4-6, golden2019autoimmuneautonomicneuropathies pages 1-2) 2) Antibody binding to extracellular receptor epitopes, with receptor internalization/degradation and functional blockade, reducing ganglionic synaptic transmission. (nakane2024autoimmuneautonomicneuropathy pages 2-3, nakane2018autoimmuneautonomicganglionopathy pages 3-5) 3) Downstream failure of autonomic output across multiple organs (cardiovascular, sudomotor, secretomotor, GI, bladder, pupillary systems), producing “pandysautonomia.” (iodice2009efficacyofimmunotherapy pages 1-3, koay2021multimodalbiomarkersquantify pages 1-8)
6.2 Upstream vs downstream processes
- Upstream: autoantibody generation; in some patients, possibly alternative immune effector mechanisms (cell-mediated) in seronegative disease. (mohapatra2024decodingautoimmuneautonomic pages 4-5, golden2019autoimmuneautonomicneuropathies pages 3-5)
- Downstream: postganglionic sympathetic and parasympathetic failure; reduced catecholamine release; end-organ dysfunction (e.g., impaired sweating, impaired lacrimation). (nakane2024autoimmuneautonomicneuropathy pages 11-12, koay2021multimodalbiomarkersquantify pages 1-8)
6.3 Cell types and GO / CL suggestions
Cell types (CL) – suggested: - Autonomic neuron (sympathetic neuron; parasympathetic neuron) - Postganglionic sympathetic neuron - Postganglionic parasympathetic neuron
Biological processes (GO) – suggested: - Chemical synaptic transmission, cholinergic - Autonomic nervous system development / regulation of autonomic nervous system - Regulation of blood pressure - Regulation of gastrointestinal motility - Regulation of sweating
(These align with receptor localization and physiological deficits described in cohorts and mechanistic studies.) (golden2019autoimmuneautonomicneuropathies pages 1-2, koay2021multimodalbiomarkersquantify pages 1-8)
6.4 Molecular profiling / multi-omics
- No transcriptomic/proteomic/metabolomic signatures were reported in the retrieved evidence.
7. Anatomical structures affected
7.1 Organ and system level
Primary system: peripheral autonomic nervous system (autonomic ganglia and postganglionic fibers). (golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2024autoimmuneautonomicneuropathy pages 11-12) Secondary/target organs include: - Cardiovascular system (orthostatic hypotension) (nakane2018autoimmuneautonomicganglionopathy pages 6-8) - Sweat glands (anhidrosis/hypohidrosis) (koay2021multimodalbiomarkersquantify pages 1-8) - Exocrine glands (lacrimal/salivary; sicca) (koay2021multimodalbiomarkersquantify pages 1-8, golden2019autoimmuneautonomicneuropathies pages 1-2) - GI tract (dysmotility) (nakane2018autoimmuneautonomicganglionopathy pages 6-8) - Urinary tract (neurogenic bladder/retention) (koay2021multimodalbiomarkersquantify pages 13-17) - Eye (pupil dysfunction) (koay2021multimodalbiomarkersquantify pages 13-17)
UBERON suggestions: - Autonomic ganglion; sympathetic ganglion; parasympathetic ganglion - Heart; gastrointestinal tract; urinary bladder; sweat gland; lacrimal gland; salivary gland; iris/pupil
7.2 Subcellular / receptor localization
- Key molecular site: postsynaptic ganglionic nicotinic ACh receptor at autonomic ganglionic synapses. (vernino1998neuronalnicotinicach pages 4-6, loser2024autoantibodiesinneuromuscular pages 13-15)
8. Temporal development
8.1 Onset
- Onset can be acute/subacute or gradual; one cohort defined subacute as peak within 3 months and found gradual onset predominated in seropositive patients. (nakane2018autoimmuneautonomicganglionopathy pages 6-8)
8.2 Course and progression
- Spontaneous improvement occurs in ~one-third of patients but is often incomplete. (iodice2009efficacyofimmunotherapy pages 1-3, golden2019autoimmuneautonomicneuropathies pages 1-2)
- Chronic phenotypes may resemble pure autonomic failure and can represent about half of seropositive patients in review-level synthesis. (golden2019autoimmuneautonomicneuropathies pages 1-2)
9. Inheritance and population
9.1 Epidemiology
- AAG is consistently described as rare; specific population prevalence/incidence rates were not identified in the retrieved evidence. (golden2019autoimmuneautonomicneuropathies pages 1-2)
9.2 Demographics
- Review synthesis: mean ages ~45–61 with ~2:1 female predominance. (golden2019autoimmuneautonomicneuropathies pages 1-2)
- Seropositive multimodal cohort: median age at onset 54 (IQR 31–63), 54% female. (koay2021multimodalbiomarkersquantify pages 8-13)
10. Diagnostics
10.1 Core diagnostic concept
Diagnosis is a combination of: 1) compatible clinical syndrome (diffuse autonomic failure) and 2) objective autonomic testing and 3) supportive biomarkers, especially gAChR antibodies, recognizing limited sensitivity and potential nonspecific low titers. (iodice2009efficacyofimmunotherapy pages 1-3, nakane2024autoimmuneautonomicneuropathy pages 11-12)
10.2 Antibody testing: assays and interpretation
- 2024 synthesis: gAChR antibody testing is “essential” but detection frequency “is not high,” and CBA or RIPA are recommended as the most accurate assays. (nakane2024autoimmuneautonomicneuropathy pages 11-12)
- Threshold interpretation (RIA/RIPA): >1.0 nmol/L high specificity; 0.2–1.0 nmol/L moderate specificity; <0.2 nmol/L nonspecific; low-level positivity can occur in 2–4% of healthy individuals. (loser2024autoantibodiesinneuromuscular pages 12-13, mohapatra2024decodingautoimmuneautonomic pages 4-5)
- Assay landscape includes RIPA/RIA, luciferase immunoprecipitation (LIPS), cell-based assays, immunomodulation assays, and flow cytometry; a 2024 review notes “there are no studies directly comparing the performance metrices of these antibody assays.” (mohapatra2024decodingautoimmuneautonomic pages 4-5)
10.3 Autonomic testing and ancillary diagnostics
Commonly used tests in cohorts/reviews include: - Head-up tilt / orthostatic vitals; Valsalva; heart-rate response to deep breathing - QSART / thermoregulatory sweat testing; plasma catecholamines (resting often reduced) - Schirmer (lacrimation) and Saxon (salivation) tests - Pupillometry / pharmacologic testing (pilocarpine supersensitivity) - Uroflowmetry and post-void residuals - CSF (protein elevation / albuminocytologic dissociation in a substantial minority) - Cardiac 123I-MIBG myocardial scintigraphy (often reduced uptake; may improve after immunotherapy) - Skin biopsy for small-fiber/autonomic denervation and recovery biomarkers (iodice2009efficacyofimmunotherapy pages 3-4, nakane2024autoimmuneautonomicneuropathy pages 11-12, koay2021multimodalbiomarkersquantify pages 1-8, nakane2018autoimmuneautonomicganglionopathy pages 9-10)
10.4 Differential diagnosis
- Differentiation from acute autonomic sensory neuropathy (AASN), pure autonomic failure (PAF), POTS, chronic fatigue syndrome, and long COVID is emphasized, using nerve conduction studies/biopsy, MRI in selected cases, catecholamine patterns, and multimodal autonomic testing. (nakane2024autoimmuneautonomicneuropathy pages 11-12)
11. Outcome / prognosis
- Spontaneous (often incomplete) improvement in ~one-third is described in clinical synthesis. (iodice2009efficacyofimmunotherapy pages 1-3, golden2019autoimmuneautonomicneuropathies pages 1-2)
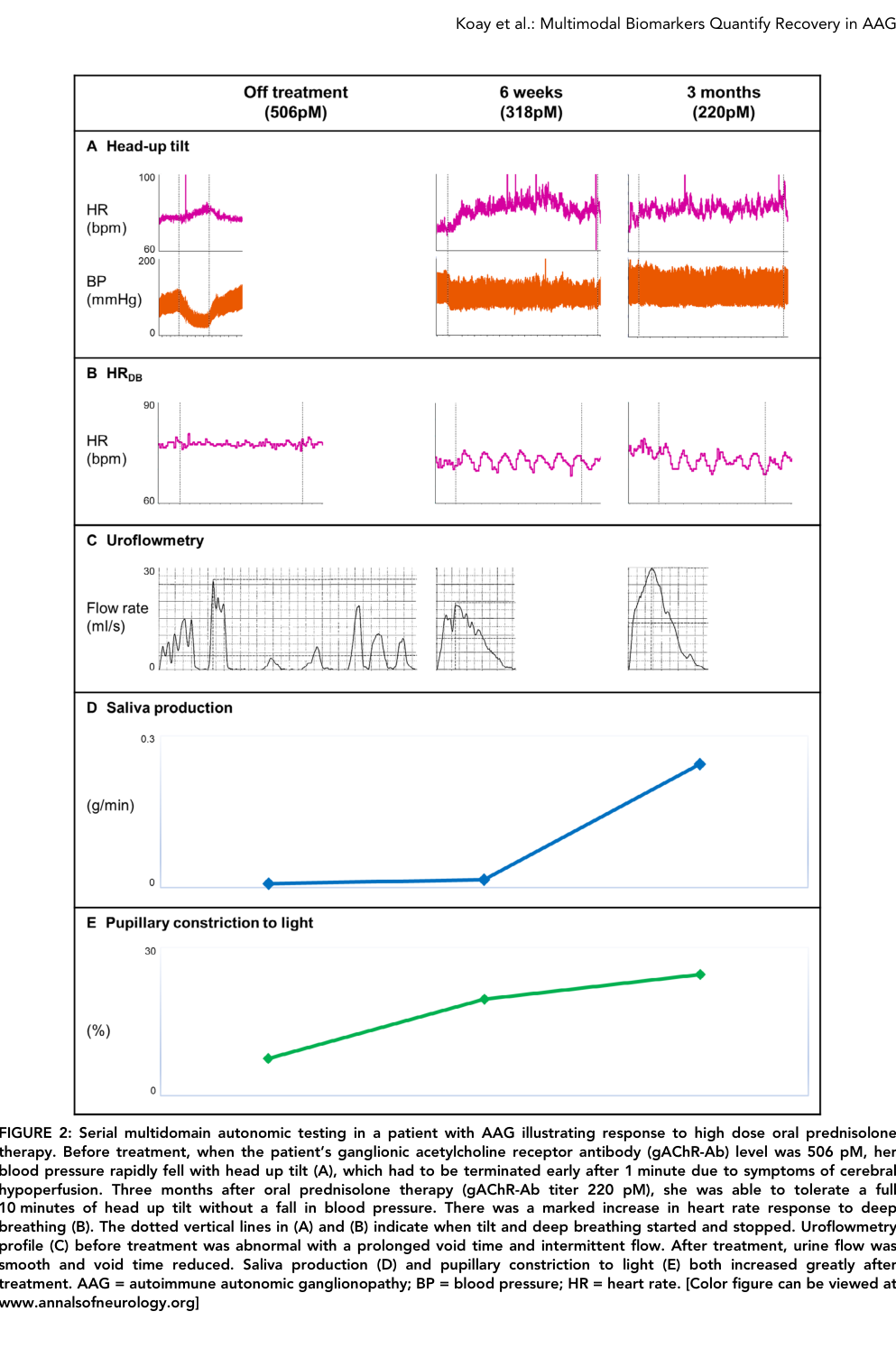
- Long-term recovery can be quantified by biomarker improvement; in a seropositive cohort (n=13) immunotherapy significantly improved orthostatic intolerance ratio, HRDB, pupillary constriction, saliva production and COMPASS-31. (koay2021multimodalbiomarkersquantify pages 1-8, koay2021multimodalbiomarkersquantify media 639533be)
- Mortality rates and life expectancy are not defined in the retrieved evidence; this remains a data gap.
12. Treatment
12.1 Immunotherapy (disease-modifying)
First-line approaches - Reviews commonly describe IVIg and plasma exchange (PLEX) as first-line antibody-directed therapies; corticosteroids are often used in combination. (golden2019autoimmuneautonomicneuropathies pages 5-6, mohapatra2024decodingautoimmuneautonomic pages 4-5, golden2019autoimmuneautonomicneuropathies pages 3-5) - In a Neurology case series (n=6; 4 seropositive, 2 seronegative), all 6 patients improved clinically after immunotherapy; sudomotor measures improved in 4. (iodice2009efficacyofimmunotherapy pages 1-3)
Evidence of objective biomarker response - In a seropositive multimodal cohort (n=13; 11 treated), immunotherapy improved key outcomes, e.g. orthostatic intolerance ratio 33.3 → 5.2 (P=.007), COMPASS-31 52 → 17 (P=.03), and pupillary constriction and salivary measures (cohort-level pre/post comparisons), supported by Figure 2 and Table 5. (koay2021multimodalbiomarkersquantify pages 1-8, koay2021multimodalbiomarkersquantify media 639533be)
Maintenance / refractory therapy - Steroid-sparing agents (e.g., mycophenolate, azathioprine) and B-cell depletion (rituximab) have case-based/series-level support and are used for relapsing or refractory disease. (golden2019autoimmuneautonomicneuropathies pages 5-6, nakane2018autoimmuneautonomicganglionopathy pages 9-10) - A 2024 review notes heterogeneity: a subset can show strong steroid responses with poorer response to IVIg/PLEX/rituximab, consistent with possible cell-mediated forms. (mohapatra2024decodingautoimmuneautonomic pages 4-5)
12.2 Symptomatic/supportive care (real-world implementations)
- Pressor/orthostatic therapies (e.g., midodrine, droxidopa) are used to manage neurogenic orthostatic hypotension in AAG-focused reviews. (nakane2018autoimmuneautonomicganglionopathy pages 9-10)
- Organ-specific supportive care is routinely required (bowel regimen and prokinetic strategies for dysmotility; catheterization/urodynamic-guided care for retention; ocular/oral sicca management). (golden2019autoimmuneautonomicneuropathies pages 1-2, koay2021multimodalbiomarkersquantify pages 13-17)
12.3 Clinical trials
- NCT01522235 (ClinicalTrials.gov): randomized, double-blind, placebo-controlled Phase 2/3 IVIg vs 5% albumin in seropositive AAG; enrollment 6; started Feb 2012; primary completion May 2014; completion Sep 2015; results first posted Jul 2, 2017. Primary endpoint: change in systolic BP during 60° tilt (ΔSBP) at 6 weeks; secondary endpoints included COMPASS, CASS, EQ-5D, orthostatic symptom questionnaire. Outcome numbers were not present in the retrieved excerpts. (NCT01522235 chunk 1, NCT01522235 chunk 2)
- URL: https://clinicaltrials.gov/study/NCT01522235 (trial registry; dates from record in evidence). (NCT01522235 chunk 1)
12.4 Suggested MAXO terms (non-exhaustive)
- Plasma exchange therapy
- Intravenous immunoglobulin therapy
- Systemic glucocorticoid therapy
- B-cell depletion therapy (rituximab)
- Mycophenolate mofetil therapy
- Vasopressor therapy (for neurogenic orthostatic hypotension)
13. Prevention
- No established primary prevention strategies were identified in the retrieved evidence; prevention is largely secondary/tertiary (early recognition and treatment to prevent complications of severe autonomic failure). (nakane2024autoimmuneautonomicneuropathy pages 11-12)
14. Other species / natural disease
- Naturally occurring veterinary analogs were not identified in the retrieved evidence. (golden2019autoimmuneautonomicneuropathies pages 1-2)
15. Model organisms
Multiple experimental systems support the antibody-mediated model: - α3 nAChR subunit knockout mice: profound autonomic failure (bladder distention, GI dysmotility, absent pupillary reflexes; urinary retention and increased mortality in review synthesis). (golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2018autoimmuneautonomicganglionopathy pages 3-5) - Passive transfer models: transfer of patient IgG to mice reduces evoked EPSP amplitudes in autonomic ganglia; EPSPs can recover despite persistent antibodies (suggesting homeostatic plasticity). (nakane2024autoimmuneautonomicneuropathy pages 2-3) - Active immunization models: immunization against ganglionic AChR (including α3 subunit strategies) induces experimental autoimmune dysautonomia/autonomic neuropathy in rabbits and mice. (vernino2009autoimmuneautonomicneuropathy pages 2-4, nakane2024autoimmuneautonomicneuropathy pages 12-14)
Recent developments (prioritizing 2023–2024)
Diagnostics and assay technology
- 2024 review-level consensus: CBA and/or RIPA are preferred for gAChR antibody detection; low sensitivity and limited access motivate new assays and expansion to other autonomic receptor targets. (nakane2024autoimmuneautonomicneuropathy pages 11-12)
- 2024 assay landscape and evidence gap: multiple assay modalities exist, but head-to-head performance comparisons are lacking (“no studies directly comparing…”). (mohapatra2024decodingautoimmuneautonomic pages 4-5)
Phenotyping and biomarkers for treatment response
- Multidomain quantitative biomarker panels (tilt-derived orthostatic intolerance ratio, pupillometry, sweat testing, secretomotor measures, COMPASS-31) are used to quantify response, with significant pre/post immunotherapy changes in seropositive cohorts, and are highlighted as practical tools for monitoring. (koay2021multimodalbiomarkersquantify pages 1-8, koay2021multimodalbiomarkersquantify media 639533be)
Expert opinions / authoritative analysis (from reviews)
- AAG is described as “rare” and clinically heterogeneous, with antibody titers and phenotypic distribution supporting a spectrum ranging from severe pan-dysautonomia to limited phenotypes, and with recognition of potentially distinct seronegative mechanisms. (golden2019autoimmuneautonomicneuropathies pages 1-2, mohapatra2024decodingautoimmuneautonomic pages 4-5)
- Clinical interpretation of autoantibody tests should be contextualized because low titers can be nonspecific, and assay characteristics vary across platforms and laboratories. (loser2024autoantibodiesinneuromuscular pages 12-13, loser2024autoantibodiesinneuromuscular pages 13-15)
Key quantitative statistics (selected)
- Seropositivity: ~50% of suspected AAG cases seropositive for gAChR antibodies. (iodice2009efficacyofimmunotherapy pages 1-3, golden2019autoimmuneautonomicneuropathies pages 1-2)
- Low-titer nonspecificity: <0.2 nmol/L can be nonspecific and seen in ~2–4% of healthy individuals. (mohapatra2024decodingautoimmuneautonomic pages 4-5)
- Japanese cohort symptom frequencies: orthostatic hypotension 80%; lower GI 74%; sensory disturbance 46%; extra-autonomic features 84%. (nakane2018autoimmuneautonomicganglionopathy pages 6-8)
- Seropositive cohort (n=13) domain frequencies: urinary retention 82% (9/11); impaired pupillary constriction 92% (12/13); reduced lacrimation 82% (9/11); postganglionic sudomotor dysfunction 88% (7/8). (koay2021multimodalbiomarkersquantify pages 13-17, koay2021multimodalbiomarkersquantify pages 1-8)
- Immunotherapy response (seropositive cohort): orthostatic intolerance ratio 33.3→5.2 (P=.007); COMPASS-31 52→17 (P=.03). (koay2021multimodalbiomarkersquantify pages 1-8, koay2021multimodalbiomarkersquantify media 639533be)
Evidence table (compact)
Table (click to expand)
| Item | Evidence/Numbers | Source (with DOI/URL when available) | Pub year |
|---|---|---|---|
| Definition | Rare immune-mediated disorder causing diffuse autonomic failure involving sympathetic, parasympathetic, and enteric systems; often considered an antibody-mediated autonomic ganglionopathy/ganglionopathy phenotype (iodice2009efficacyofimmunotherapy pages 1-3, golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2024autoimmuneautonomicneuropathy pages 2-3) | Iodice et al., Neurology doi:10.1212/WNL.0b013e3181a92b52 https://doi.org/10.1212/WNL.0b013e3181a92b52; Golden & Vernino, Clin Auton Res doi:10.1007/s10286-019-00611-1 https://doi.org/10.1007/s10286-019-00611-1; Nakane et al., Int J Mol Sci doi:10.3390/ijms25042296 https://doi.org/10.3390/ijms25042296 | 2009; 2019; 2024 |
| Core autoantigen / autoantibody | Ganglionic nicotinic acetylcholine receptor (gAChR), especially α3-containing receptor; antibodies bind mainly α3 subunit, usually in α3β4 receptor complex (golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2024autoimmuneautonomicneuropathy pages 2-3, vernino1998neuronalnicotinicach pages 1-2) | Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1; Nakane et al., https://doi.org/10.3390/ijms25042296; Vernino et al., Neurology doi:10.1212/WNL.50.6.1806 https://doi.org/10.1212/WNL.50.6.1806 | 2019; 2024; 1998 |
| Pathogenic mechanism | Proposed 3-step model: antibody binding → receptor internalization/degradation → functional blockade; patient IgG reduces ganglionic AChR currents; passive transfer in mice reduces EPSPs (nakane2024autoimmuneautonomicneuropathy pages 2-3, golden2019autoimmuneautonomicneuropathies pages 1-2) | Nakane et al., https://doi.org/10.3390/ijms25042296; Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1 | 2024; 2019 |
| Seropositivity rate | About 50% of clinically suspected AAG patients are seropositive for gAChR antibodies; seronegative disease remains recognized (mohapatra2024decodingautoimmuneautonomic pages 4-5, iodice2009efficacyofimmunotherapy pages 1-3, golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2018autoimmuneautonomicganglionopathy pages 1-3) | Mohapatra et al., Ann Indian Acad Neurol doi:10.4103/aian.aian_394_24 https://doi.org/10.4103/aian.aian_394_24; Iodice et al., https://doi.org/10.1212/WNL.0b013e3181a92b52; Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1; Nakane et al., https://doi.org/10.1080/14737175.2018.1540304 | 2024; 2009; 2019; 2018 |
| Antibody threshold: classic RIPA positivity | Upper lab limit reported as 0.05 nmol/L in one major clinical series; antibody-positive AAG defined at or above this threshold (iodice2009efficacyofimmunotherapy pages 3-4, golden2019autoimmuneautonomicneuropathies pages 3-5) | Iodice et al., https://doi.org/10.1212/WNL.0b013e3181a92b52; Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1 | 2009; 2019 |
| Antibody titer interpretation | >0.20 nmol/L fairly specific for AAG; high titers correlate with more severe dysautonomia/cholinergic failure; ≥1.0 nmol/L associated with severe pan-dysautonomia; <0.2 nmol/L often nonspecific and seen in ~2%–4% of healthy people (golden2019autoimmuneautonomicneuropathies pages 3-5, mohapatra2024decodingautoimmuneautonomic pages 4-5) | Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1; Mohapatra et al., https://doi.org/10.4103/aian.aian_394_24 | 2019; 2024 |
| LIPS assay thresholds | Anti-gAChRα3 A.I. cutoff 1.0: sensitivity 50.0%, specificity 100%; anti-gAChRβ4 A.I. cutoff 1.0: sensitivity 10.0%, specificity 100% (nakane2018autoimmuneautonomicganglionopathy pages 5-6) | Nakane et al., Expert Rev Neurother doi:10.1080/14737175.2018.1540304 https://doi.org/10.1080/14737175.2018.1540304 | 2018 |
| Typical demographics | Middle age predominance; mean ages reported ~45–61 years with ~2:1 female predominance; in Koay cohort median onset 54 years, 54% female; in Japanese cohort mean age 60±18 years (43M/37F) (golden2019autoimmuneautonomicneuropathies pages 1-2, koay2021multimodalbiomarkersquantify pages 8-13, nakane2018autoimmuneautonomicganglionopathy pages 5-6) | Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1; Koay et al., Ann Neurol doi:10.1002/ana.26018 https://doi.org/10.1002/ana.26018; Nakane et al., https://doi.org/10.1080/14737175.2018.1540304 | 2019; 2021; 2018 |
| Onset / course | Often acute or subacute; spontaneous but usually incomplete recovery in ~one-third; in seropositive Japanese cohort gradual onset predominated 62/80 (78%), antecedent events 13/80 (16%) (iodice2009efficacyofimmunotherapy pages 1-3, golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2018autoimmuneautonomicganglionopathy pages 6-8, nakane2018autoimmuneautonomicganglionopathy pages 1-3) | Iodice et al., https://doi.org/10.1212/WNL.0b013e3181a92b52; Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1; Nakane et al., https://doi.org/10.1080/14737175.2018.1540304 | 2009; 2019; 2018 |
| Common feature: orthostatic hypotension / intolerance | Most common presenting/autonomic feature; 64/80 (80%) in seropositive Japanese cohort; initial symptom in 50/80 (62.5%); all 13/13 in Koay cohort had cardiovascular autonomic failure with orthostatic hypotension (nakane2018autoimmuneautonomicganglionopathy pages 6-8, koay2021multimodalbiomarkersquantify pages 8-13) | Nakane et al., https://doi.org/10.1080/14737175.2018.1540304; Koay et al., https://doi.org/10.1002/ana.26018 | 2018; 2021 |
| Common feature: lower GI dysmotility | Lower GI symptoms in 59/80 (74%) seropositive cases; GI dysfunction is a core cholinergic manifestation (nakane2018autoimmuneautonomicganglionopathy pages 6-8, golden2019autoimmuneautonomicneuropathies pages 1-2, nakane2018autoimmuneautonomicganglionopathy pages 9-10) | Nakane et al., https://doi.org/10.1080/14737175.2018.1540304; Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1 | 2018; 2019 |
| Common feature: urinary dysfunction | Urinary retention 9/11 (82%); catheterisation required in 5/13 (38%); abnormal uroflowmetry in 6/8 (75%) in Koay cohort (koay2021multimodalbiomarkersquantify pages 13-17, koay2021multimodalbiomarkersquantify pages 1-8) | Koay et al., https://doi.org/10.1002/ana.26018 | 2021 |
| Common feature: pupillary dysfunction | Pupillary dysfunction 21/80 (26%) in Japanese cohort; in Koay cohort impaired pupillary constriction 12/13 (92%), cholinergic supersensitivity in 5/5 tested, ptosis 4/13 (31%) (nakane2018autoimmuneautonomicganglionopathy pages 6-8, koay2021multimodalbiomarkersquantify pages 13-17, koay2021multimodalbiomarkersquantify pages 8-13) | Nakane et al., https://doi.org/10.1080/14737175.2018.1540304; Koay et al., https://doi.org/10.1002/ana.26018 | 2018; 2021 |
| Common feature: secretomotor dysfunction | Reduced lacrimation 9/11 (82%), reduced salivary production 6/8 (75%), impaired sweat production 7/8 (88%) in Koay cohort; sicca/anhidrosis also emphasized in reviews (koay2021multimodalbiomarkersquantify pages 13-17, koay2021multimodalbiomarkersquantify pages 1-8, golden2019autoimmuneautonomicneuropathies pages 1-2) | Koay et al., https://doi.org/10.1002/ana.26018; Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1 | 2021; 2019 |
| Extra-autonomic manifestations | Extra-autonomic involvement common: 67/80 (84%) in seropositive Japanese cohort; sensory disturbance/numbness 37/80 (46%); concurrent autoimmune disease in 25/80 (31%); tumors in 11/80 (14%); in Koay cohort other autoimmune diseases in 8/13 (62%) (nakane2018autoimmuneautonomicganglionopathy pages 6-8, nakane2018autoimmuneautonomicganglionopathy pages 8-9, koay2021multimodalbiomarkersquantify pages 8-13) | Nakane et al., https://doi.org/10.1080/14737175.2018.1540304; Koay et al., https://doi.org/10.1002/ana.26018 | 2018; 2021 |
| Catecholamine / imaging biomarkers | Resting plasma catecholamines often low; in Koay cohort plasma noradrenaline mostly 100–200 pg/ml with absent tilt rise; reduced cardiac 123I-MIBG uptake in ~80% of Japanese AAG cohort, and uptake may improve after immunotherapy (nakane2024autoimmuneautonomicneuropathy pages 11-12, koay2021multimodalbiomarkersquantify pages 8-13, nakane2018autoimmuneautonomicganglionopathy pages 9-10) | Nakane et al., https://doi.org/10.3390/ijms25042296; Koay et al., https://doi.org/10.1002/ana.26018; Nakane et al., https://doi.org/10.1080/14737175.2018.1540304 | 2024; 2021; 2018 |
| CSF findings | Elevated CSF protein in 48% and albuminocytologic dissociation in 37% in review summary; another review cites albuminocytologic dissociation in ~40% (nakane2024autoimmuneautonomicneuropathy pages 11-12, mohapatra2024decodingautoimmuneautonomic pages 4-5) | Nakane et al., https://doi.org/10.3390/ijms25042296; Mohapatra et al., https://doi.org/10.4103/aian.aian_394_24 | 2024; 2024 |
| Core diagnostic tests | History and time-course; autonomic reflex screen; head-up tilt; Valsalva; HR response to deep breathing; QSART/TST/sweat testing; plasma catecholamines; Schirmer/Saxon tests; pupillometry; uroflowmetry; GI motility studies; skin biopsy; 123I-MIBG scintigraphy; gAChR antibody testing by RIPA/CBA/LIPS (iodice2009efficacyofimmunotherapy pages 3-4, nakane2024autoimmuneautonomicneuropathy pages 11-12, nakane2018autoimmuneautonomicganglionopathy pages 9-10, koay2021multimodalbiomarkersquantify pages 8-13) | Iodice et al., https://doi.org/10.1212/WNL.0b013e3181a92b52; Nakane et al., https://doi.org/10.3390/ijms25042296; Nakane et al., https://doi.org/10.1080/14737175.2018.1540304; Koay et al., https://doi.org/10.1002/ana.26018 | 2009; 2024; 2018; 2021 |
| Preferred antibody assays | RIPA or live cell-based assay considered most accurate in recent review; LIPS also used with high specificity in Japanese studies (nakane2024autoimmuneautonomicneuropathy pages 11-12, nakane2018autoimmuneautonomicganglionopathy pages 5-6) | Nakane et al., https://doi.org/10.3390/ijms25042296; Nakane et al., https://doi.org/10.1080/14737175.2018.1540304 | 2024; 2018 |
| First-line immunotherapy | IVIG and plasma exchange generally regarded as first-line; corticosteroids commonly added/used in pulse regimens (golden2019autoimmuneautonomicneuropathies pages 5-6, nakane2018autoimmuneautonomicganglionopathy pages 9-10, nakane2018autoimmuneautonomicganglionopathy pages 1-3) | Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1; Nakane et al., https://doi.org/10.1080/14737175.2018.1540304 | 2019; 2018 |
| Maintenance / refractory treatment | Prednisolone, azathioprine, mycophenolate mofetil, rituximab used for sustained control or refractory disease; evidence mainly case reports/series (golden2019autoimmuneautonomicneuropathies pages 5-6, nakane2018autoimmuneautonomicganglionopathy pages 9-10, golden2019autoimmuneautonomicneuropathies pages 3-5) | Golden & Vernino, https://doi.org/10.1007/s10286-019-00611-1; Nakane et al., https://doi.org/10.1080/14737175.2018.1540304 | 2019; 2018 |
| Quantitative response biomarkers after immunotherapy | In Koay cohort, orthostatic intolerance ratio improved 33.3 [17.8–61.3] → 5.2 [1.4–8.2] (P=.007); HR response to deep breathing 1.5 → 4.5 (P=.02); pupillary constriction 12.0% → 19.0% (P=.02); saliva 0.01 → 0.08 g/min (P=.03); COMPASS-31 52 → 17 (P=.03) (koay2021multimodalbiomarkersquantify pages 1-8, koay2021multimodalbiomarkersquantify media 639533be) | Koay et al., https://doi.org/10.1002/ana.26018 | 2021 |
| Clinical trial landscape | Very limited prospective evidence; one identified interventional IVIG study: NCT01522235, completed, phase 2/3, enrollment 6 (clinicaltrials.gov result in tool output) (iodice2009efficacyofimmunotherapy pages 1-3) | Beth Israel Deaconess Medical Center trial listing: NCT01522235 | — |
Table: This table compiles high-yield clinical and mechanistic facts about autoimmune autonomic ganglionopathy, including antibody biology, phenotype frequencies, diagnostics, and treatment patterns. It is designed as a compact evidence summary for rapid knowledge-base ingestion.
Visual evidence from Koay et al. 2021
- Figure and tables demonstrating biomarker improvements and immunotherapy regimens are available from the Koay et al. cohort (Figure 2; Tables 4–5). (koay2021multimodalbiomarkersquantify media 639533be, koay2021multimodalbiomarkersquantify media 2579079a, koay2021multimodalbiomarkersquantify media 172ee738)
Notes on evidence limitations
AAG is rare, and much of the treatment evidence base remains small case series or uncontrolled cohorts; even the registered randomized trial (NCT01522235) enrolled only six participants, and outcome numbers were not available in the excerpts retrieved in this run. Population prevalence/incidence and mortality statistics were not found in the retrieved primary sources and should be filled via rare-disease registries/Orphanet or epidemiologic databases if needed for the knowledge base. (NCT01522235 chunk 1, golden2019autoimmuneautonomicneuropathies pages 1-2)
References
-
(iodice2009efficacyofimmunotherapy pages 1-3): Valeria Iodice, K. Kimpinski, S. Vernino, Paola Sandroni, R. Fealey, and Philip Low. Efficacy of immunotherapy in seropositive and seronegative putative autoimmune autonomic ganglionopathy. Neurology, 72:2002-2008, Jun 2009. URL: https://doi.org/10.1212/wnl.0b013e3181a92b52, doi:10.1212/wnl.0b013e3181a92b52. This article has 107 citations and is from a highest quality peer-reviewed journal.
-
(golden2019autoimmuneautonomicneuropathies pages 1-2): Elisabeth P. Golden and Steven Vernino. Autoimmune autonomic neuropathies and ganglionopathies: epidemiology, pathophysiology, and therapeutic advances. Clinical Autonomic Research, 29:277-288, May 2019. URL: https://doi.org/10.1007/s10286-019-00611-1, doi:10.1007/s10286-019-00611-1. This article has 77 citations and is from a peer-reviewed journal.
-
(nakane2024autoimmuneautonomicneuropathy pages 2-3): Shunya Nakane, Haruki Koike, Tomohiro Hayashi, and Yuji Nakatsuji. Autoimmune autonomic neuropathy: from pathogenesis to diagnosis. International Journal of Molecular Sciences, 25:2296, Feb 2024. URL: https://doi.org/10.3390/ijms25042296, doi:10.3390/ijms25042296. This article has 17 citations.
-
(koay2021multimodalbiomarkersquantify pages 1-8): Shiwen Koay, Ekawat Vichayanrat, Fion Bremner, Jalesh N. Panicker, Bethan Lang, Michael P. Lunn, Laura Watson, Gordon T. Ingle, Ellen Merete Hagen, Patricia McNamara, Leslie Jacobson, Vincenzo Provitera, Maria Nolano, Angela Vincent, Christopher J. Mathias, and Valeria Iodice. Multimodal biomarkers quantify recovery in autoimmune autonomic ganglionopathy. Annals of Neurology, 89:753-768, Feb 2021. URL: https://doi.org/10.1002/ana.26018, doi:10.1002/ana.26018. This article has 30 citations and is from a highest quality peer-reviewed journal.
-
(nakane2024autoimmuneautonomicneuropathy pages 11-12): Shunya Nakane, Haruki Koike, Tomohiro Hayashi, and Yuji Nakatsuji. Autoimmune autonomic neuropathy: from pathogenesis to diagnosis. International Journal of Molecular Sciences, 25:2296, Feb 2024. URL: https://doi.org/10.3390/ijms25042296, doi:10.3390/ijms25042296. This article has 17 citations.
-
(vernino1998neuronalnicotinicach pages 4-6): Steven Vernino, Jill Adamski, Thomas J. Kryzer, Robert D. Fealey, and Vanda A. Lennon. Neuronal nicotinic ach receptor antibody in subacute autonomic neuropathy and cancer‐related syndromes. Neurology, 50:1806-1813, Jun 1998. URL: https://doi.org/10.1212/wnl.50.6.1806, doi:10.1212/wnl.50.6.1806. This article has 277 citations and is from a highest quality peer-reviewed journal.
-
(vernino1998neuronalnicotinicach pages 3-4): Steven Vernino, Jill Adamski, Thomas J. Kryzer, Robert D. Fealey, and Vanda A. Lennon. Neuronal nicotinic ach receptor antibody in subacute autonomic neuropathy and cancer‐related syndromes. Neurology, 50:1806-1813, Jun 1998. URL: https://doi.org/10.1212/wnl.50.6.1806, doi:10.1212/wnl.50.6.1806. This article has 277 citations and is from a highest quality peer-reviewed journal.
-
(nakane2018autoimmuneautonomicganglionopathy pages 6-8): Shunya Nakane, Akihiro Mukaino, Osamu Higuchi, Mari Watari, Yasuhiro Maeda, Makoto Yamakawa, Keiichi Nakahara, Koutaro Takamatsu, Hidenori Matsuo, and Yukio Ando. Autoimmune autonomic ganglionopathy: an update on diagnosis and treatment. Expert Review of Neurotherapeutics, 18:953-965, Nov 2018. URL: https://doi.org/10.1080/14737175.2018.1540304, doi:10.1080/14737175.2018.1540304. This article has 42 citations and is from a peer-reviewed journal.
-
(vernino1998neuronalnicotinicach pages 1-2): Steven Vernino, Jill Adamski, Thomas J. Kryzer, Robert D. Fealey, and Vanda A. Lennon. Neuronal nicotinic ach receptor antibody in subacute autonomic neuropathy and cancer‐related syndromes. Neurology, 50:1806-1813, Jun 1998. URL: https://doi.org/10.1212/wnl.50.6.1806, doi:10.1212/wnl.50.6.1806. This article has 277 citations and is from a highest quality peer-reviewed journal.
-
(NCT01522235 chunk 1): Roy Freeman, MD. Evaluating the Effectiveness of Intravenous Immunoglobulin Therapy in Autoimmune Autonomic Ganglionopathy. Beth Israel Deaconess Medical Center. 2012. ClinicalTrials.gov Identifier: NCT01522235
-
(loser2024autoantibodiesinneuromuscular pages 13-15): Valentin Loser, Alex Vicino, and Marie Théaudin. Autoantibodies in neuromuscular disorders: a review of their utility in clinical practice. Frontiers in Neurology, Nov 2024. URL: https://doi.org/10.3389/fneur.2024.1495205, doi:10.3389/fneur.2024.1495205. This article has 10 citations and is from a peer-reviewed journal.
-
(mohapatra2024decodingautoimmuneautonomic pages 4-5): Prachi Mohapatra, Ayush Agarwal, Divya M Radhakrishnan, Achal Kumar Srivastava, and Divyani Garg. Decoding autoimmune autonomic disorders: a less-recognized overlap. Annals of Indian Academy of Neurology, 27:482-492, Oct 2024. URL: https://doi.org/10.4103/aian.aian_394_24, doi:10.4103/aian.aian_394_24. This article has 1 citations and is from a peer-reviewed journal.
-
(golden2019autoimmuneautonomicneuropathies pages 3-5): Elisabeth P. Golden and Steven Vernino. Autoimmune autonomic neuropathies and ganglionopathies: epidemiology, pathophysiology, and therapeutic advances. Clinical Autonomic Research, 29:277-288, May 2019. URL: https://doi.org/10.1007/s10286-019-00611-1, doi:10.1007/s10286-019-00611-1. This article has 77 citations and is from a peer-reviewed journal.
-
(koay2021multimodalbiomarkersquantify pages 8-13): Shiwen Koay, Ekawat Vichayanrat, Fion Bremner, Jalesh N. Panicker, Bethan Lang, Michael P. Lunn, Laura Watson, Gordon T. Ingle, Ellen Merete Hagen, Patricia McNamara, Leslie Jacobson, Vincenzo Provitera, Maria Nolano, Angela Vincent, Christopher J. Mathias, and Valeria Iodice. Multimodal biomarkers quantify recovery in autoimmune autonomic ganglionopathy. Annals of Neurology, 89:753-768, Feb 2021. URL: https://doi.org/10.1002/ana.26018, doi:10.1002/ana.26018. This article has 30 citations and is from a highest quality peer-reviewed journal.
-
(koay2021multimodalbiomarkersquantify pages 13-17): Shiwen Koay, Ekawat Vichayanrat, Fion Bremner, Jalesh N. Panicker, Bethan Lang, Michael P. Lunn, Laura Watson, Gordon T. Ingle, Ellen Merete Hagen, Patricia McNamara, Leslie Jacobson, Vincenzo Provitera, Maria Nolano, Angela Vincent, Christopher J. Mathias, and Valeria Iodice. Multimodal biomarkers quantify recovery in autoimmune autonomic ganglionopathy. Annals of Neurology, 89:753-768, Feb 2021. URL: https://doi.org/10.1002/ana.26018, doi:10.1002/ana.26018. This article has 30 citations and is from a highest quality peer-reviewed journal.
-
(koay2021multimodalbiomarkersquantify pages 17-21): Shiwen Koay, Ekawat Vichayanrat, Fion Bremner, Jalesh N. Panicker, Bethan Lang, Michael P. Lunn, Laura Watson, Gordon T. Ingle, Ellen Merete Hagen, Patricia McNamara, Leslie Jacobson, Vincenzo Provitera, Maria Nolano, Angela Vincent, Christopher J. Mathias, and Valeria Iodice. Multimodal biomarkers quantify recovery in autoimmune autonomic ganglionopathy. Annals of Neurology, 89:753-768, Feb 2021. URL: https://doi.org/10.1002/ana.26018, doi:10.1002/ana.26018. This article has 30 citations and is from a highest quality peer-reviewed journal.
-
(nakane2018autoimmuneautonomicganglionopathy pages 3-5): Shunya Nakane, Akihiro Mukaino, Osamu Higuchi, Mari Watari, Yasuhiro Maeda, Makoto Yamakawa, Keiichi Nakahara, Koutaro Takamatsu, Hidenori Matsuo, and Yukio Ando. Autoimmune autonomic ganglionopathy: an update on diagnosis and treatment. Expert Review of Neurotherapeutics, 18:953-965, Nov 2018. URL: https://doi.org/10.1080/14737175.2018.1540304, doi:10.1080/14737175.2018.1540304. This article has 42 citations and is from a peer-reviewed journal.
-
(loser2024autoantibodiesinneuromuscular pages 12-13): Valentin Loser, Alex Vicino, and Marie Théaudin. Autoantibodies in neuromuscular disorders: a review of their utility in clinical practice. Frontiers in Neurology, Nov 2024. URL: https://doi.org/10.3389/fneur.2024.1495205, doi:10.3389/fneur.2024.1495205. This article has 10 citations and is from a peer-reviewed journal.
-
(iodice2009efficacyofimmunotherapy pages 3-4): Valeria Iodice, K. Kimpinski, S. Vernino, Paola Sandroni, R. Fealey, and Philip Low. Efficacy of immunotherapy in seropositive and seronegative putative autoimmune autonomic ganglionopathy. Neurology, 72:2002-2008, Jun 2009. URL: https://doi.org/10.1212/wnl.0b013e3181a92b52, doi:10.1212/wnl.0b013e3181a92b52. This article has 107 citations and is from a highest quality peer-reviewed journal.
-
(nakane2018autoimmuneautonomicganglionopathy pages 9-10): Shunya Nakane, Akihiro Mukaino, Osamu Higuchi, Mari Watari, Yasuhiro Maeda, Makoto Yamakawa, Keiichi Nakahara, Koutaro Takamatsu, Hidenori Matsuo, and Yukio Ando. Autoimmune autonomic ganglionopathy: an update on diagnosis and treatment. Expert Review of Neurotherapeutics, 18:953-965, Nov 2018. URL: https://doi.org/10.1080/14737175.2018.1540304, doi:10.1080/14737175.2018.1540304. This article has 42 citations and is from a peer-reviewed journal.
-
(koay2021multimodalbiomarkersquantify media 639533be): Shiwen Koay, Ekawat Vichayanrat, Fion Bremner, Jalesh N. Panicker, Bethan Lang, Michael P. Lunn, Laura Watson, Gordon T. Ingle, Ellen Merete Hagen, Patricia McNamara, Leslie Jacobson, Vincenzo Provitera, Maria Nolano, Angela Vincent, Christopher J. Mathias, and Valeria Iodice. Multimodal biomarkers quantify recovery in autoimmune autonomic ganglionopathy. Annals of Neurology, 89:753-768, Feb 2021. URL: https://doi.org/10.1002/ana.26018, doi:10.1002/ana.26018. This article has 30 citations and is from a highest quality peer-reviewed journal.
-
(golden2019autoimmuneautonomicneuropathies pages 5-6): Elisabeth P. Golden and Steven Vernino. Autoimmune autonomic neuropathies and ganglionopathies: epidemiology, pathophysiology, and therapeutic advances. Clinical Autonomic Research, 29:277-288, May 2019. URL: https://doi.org/10.1007/s10286-019-00611-1, doi:10.1007/s10286-019-00611-1. This article has 77 citations and is from a peer-reviewed journal.
-
(NCT01522235 chunk 2): Roy Freeman, MD. Evaluating the Effectiveness of Intravenous Immunoglobulin Therapy in Autoimmune Autonomic Ganglionopathy. Beth Israel Deaconess Medical Center. 2012. ClinicalTrials.gov Identifier: NCT01522235
-
(vernino2009autoimmuneautonomicneuropathy pages 2-4): S Vernino, PA Low, and VA Lennon. Autoimmune autonomic neuropathy. Encyclopedia of Neuroscience, pages 785-789, Jan 2009. URL: https://doi.org/10.1016/b978-008045046-9.00625-2, doi:10.1016/b978-008045046-9.00625-2. This article has 1 citations.
-
(nakane2024autoimmuneautonomicneuropathy pages 12-14): Shunya Nakane, Haruki Koike, Tomohiro Hayashi, and Yuji Nakatsuji. Autoimmune autonomic neuropathy: from pathogenesis to diagnosis. International Journal of Molecular Sciences, 25:2296, Feb 2024. URL: https://doi.org/10.3390/ijms25042296, doi:10.3390/ijms25042296. This article has 17 citations.
-
(nakane2018autoimmuneautonomicganglionopathy pages 1-3): Shunya Nakane, Akihiro Mukaino, Osamu Higuchi, Mari Watari, Yasuhiro Maeda, Makoto Yamakawa, Keiichi Nakahara, Koutaro Takamatsu, Hidenori Matsuo, and Yukio Ando. Autoimmune autonomic ganglionopathy: an update on diagnosis and treatment. Expert Review of Neurotherapeutics, 18:953-965, Nov 2018. URL: https://doi.org/10.1080/14737175.2018.1540304, doi:10.1080/14737175.2018.1540304. This article has 42 citations and is from a peer-reviewed journal.
-
(nakane2018autoimmuneautonomicganglionopathy pages 5-6): Shunya Nakane, Akihiro Mukaino, Osamu Higuchi, Mari Watari, Yasuhiro Maeda, Makoto Yamakawa, Keiichi Nakahara, Koutaro Takamatsu, Hidenori Matsuo, and Yukio Ando. Autoimmune autonomic ganglionopathy: an update on diagnosis and treatment. Expert Review of Neurotherapeutics, 18:953-965, Nov 2018. URL: https://doi.org/10.1080/14737175.2018.1540304, doi:10.1080/14737175.2018.1540304. This article has 42 citations and is from a peer-reviewed journal.
-
(nakane2018autoimmuneautonomicganglionopathy pages 8-9): Shunya Nakane, Akihiro Mukaino, Osamu Higuchi, Mari Watari, Yasuhiro Maeda, Makoto Yamakawa, Keiichi Nakahara, Koutaro Takamatsu, Hidenori Matsuo, and Yukio Ando. Autoimmune autonomic ganglionopathy: an update on diagnosis and treatment. Expert Review of Neurotherapeutics, 18:953-965, Nov 2018. URL: https://doi.org/10.1080/14737175.2018.1540304, doi:10.1080/14737175.2018.1540304. This article has 42 citations and is from a peer-reviewed journal.
-
(koay2021multimodalbiomarkersquantify media 2579079a): Shiwen Koay, Ekawat Vichayanrat, Fion Bremner, Jalesh N. Panicker, Bethan Lang, Michael P. Lunn, Laura Watson, Gordon T. Ingle, Ellen Merete Hagen, Patricia McNamara, Leslie Jacobson, Vincenzo Provitera, Maria Nolano, Angela Vincent, Christopher J. Mathias, and Valeria Iodice. Multimodal biomarkers quantify recovery in autoimmune autonomic ganglionopathy. Annals of Neurology, 89:753-768, Feb 2021. URL: https://doi.org/10.1002/ana.26018, doi:10.1002/ana.26018. This article has 30 citations and is from a highest quality peer-reviewed journal.
-
(koay2021multimodalbiomarkersquantify media 172ee738): Shiwen Koay, Ekawat Vichayanrat, Fion Bremner, Jalesh N. Panicker, Bethan Lang, Michael P. Lunn, Laura Watson, Gordon T. Ingle, Ellen Merete Hagen, Patricia McNamara, Leslie Jacobson, Vincenzo Provitera, Maria Nolano, Angela Vincent, Christopher J. Mathias, and Valeria Iodice. Multimodal biomarkers quantify recovery in autoimmune autonomic ganglionopathy. Annals of Neurology, 89:753-768, Feb 2021. URL: https://doi.org/10.1002/ana.26018, doi:10.1002/ana.26018. This article has 30 citations and is from a highest quality peer-reviewed journal.