1. Disease Information
Overview (definition; current understanding)
Anal canal adenocarcinoma is a rare malignant epithelial tumor with gland-forming histology arising in the anal canal region and/or adjacent transitional zone, with heterogeneous biology and clinical behavior. Registry-based studies emphasize its rarity and historically limited evidence base for guidelines. (gogna2020clinicopathologicfeaturesand pages 1-2, park2020survivaloutcomesafter pages 1-2)
Key identifiers and coding (available from retrieved sources)
SEER-based studies identify anal canal adenocarcinoma using ICD-O-3 site codes for the anal canal region—C21.0 (anus, NOS), C21.1 (anal canal), C21.2 (cloacogenic zone)—and exclude “overlapping lesion of rectum, anus and anal canal” (C21.8) to avoid misclassification with rectal primaries. (gogna2020clinicopathologicfeaturesand pages 2-3)
Synonyms / alternative names (from literature)
- Anal adenocarcinoma (used interchangeably in case series and registry studies) (tsay2021analadenocarcinomacase pages 2-3, park2020survivaloutcomesafter pages 1-2)
- Fistula-associated mucinous adenocarcinoma (subset arising in chronic anorectal fistula tracts) (koizumi2023acasereport pages 1-3, inoue2023resectionofanorectal pages 1-3)
- Extramucosal anal adenocarcinoma (from anal glands or fistulae) vs colorectal-type (above dentate line) (tsay2021analadenocarcinomacase pages 2-3)
Evidence source type
Most available evidence is aggregated (SEER population registry) and case-based/observational literature due to rarity; prospective randomized data are minimal. (gogna2020clinicopathologicfeaturesand pages 1-2, park2020survivaloutcomesafter pages 1-2, NCT05605873 chunk 1)
2. Etiology
Disease causal factors / mechanistic contexts
Anal canal adenocarcinoma is etiologically heterogeneous and can arise through distinct pathways depending on subtype.
Chronic inflammation and fistula-associated carcinogenesis (mucinous subtype) - A 2023 fistula-associated mucinous adenocarcinoma case report states: “Chronic inflammation in organs is one of the causes of cancer development and proliferation.” (Koizumi et al., Surgical Case Reports, published 2023-09; https://doi.org/10.1186/s40792-023-01743-3). (koizumi2023acasereport pages 1-3) - The same report emphasizes that “A long-standing (over 10 years) anal fistula is considered an etiology of fistula-associated mucinous adenocarcinoma (FAMC)” and notes that malignant transformation may occur faster than expected: “FAMC can develop within fewer than 3 years after the development of a perianal abscess and anal fistula.” (koizumi2023acasereport pages 1-3)
Crohn’s disease and anorectal fistula cancer context A 2023 Crohn’s disease-associated case report highlights diagnostic difficulty and late presentation in anorectal fistula cancers, commonly mucinous histology, and reports that symptom changes (mucus discharge, bleeding, stricture) often trigger diagnosis. (Inoue et al., Surgical Case Reports, published 2023-11; https://doi.org/10.1186/s40792-023-01778-6). (inoue2023resectionofanorectal pages 1-3)
Infectious agents (HPV) and current evidence
Evidence for HPV differs by subtype: - A 2021 literature review/case report states that, unlike anal squamous cell carcinoma, “no such association with anal adenocarcinoma has been established” for HPV. (Tsay et al., BMJ Open Gastroenterology, 2021-07; https://doi.org/10.1136/bmjgast-2021-000661). (tsay2021analadenocarcinomacase pages 2-3) - In contrast, molecular profiling of primary anal canal adenocarcinoma supports HPV-dependent and HPV-independent pathways and reports HPV16/18 restricted to an anal gland/transitional-type subset (see Molecular section). (herfs2018adualisticmodel pages 1-2, herfs2018adualisticmodel pages 8-9)
Risk factors (human clinical evidence)
- Immunosuppression, perianal Crohn’s disease, and older age are proposed/recognized risk factors, though “poorly studied” due to small sample sizes. (tsay2021analadenocarcinomacase pages 2-3)
- Chronic anal fistula / perianal abscess → fistula-associated mucinous adenocarcinoma is supported by case-based evidence and recognized as an etiologic substrate in reviews of extramucosal tumors. (koizumi2023acasereport pages 1-3, tsay2021analadenocarcinomacase pages 2-3, inoue2023resectionofanorectal pages 1-3)
Protective factors / gene–environment interactions
No protective factors or gene–environment interaction evidence specific to anal canal adenocarcinoma were retrievable in the current corpus.
3. Phenotypes
Common clinical presentation (symptoms/signs)
Case reports and fistula-associated cancer reports describe symptomatic presentation including: - Anal pain and palpable perianal/anal mass (koizumi2023acasereport pages 1-3) - Mucus discharge, anal bleeding, and stricturing/stenosis in fistula-cancer contexts (inoue2023resectionofanorectal pages 1-3) - Perianal nodules/papules and chronic anal drainage in an anal adenocarcinoma case report (tsay2021analadenocarcinomacase pages 1-1)
Stage at presentation / temporal development
In a SEER population analysis (1973–2015), anal canal adenocarcinoma presented as: - In situ 6.7%, localized 44.4%, regional 25.8%, distant 13.5% (gogna2020clinicopathologicfeaturesand pages 1-2) This distribution supports a substantial proportion diagnosed beyond localized disease, consistent with diagnostic delay in fistula-associated forms. (inoue2023resectionofanorectal pages 1-3)
Phenotype characteristics and frequencies
Beyond SEER stage distributions, robust phenotype frequency estimates (e.g., percent with bleeding/pain) were not available in retrieved texts.
Suggested HPO terms (non-exhaustive)
- Anal pain — HP:0002043 (mapping suggestion; not validated from retrieved text)
- Hematochezia/rectal bleeding — HP:0002240 (mapping suggestion)
- Tenesmus — HP:0031052 (mapping suggestion)
- Anal fistula — HP:0001930 (mapping suggestion)
- Anal mass — could map to HP:0031976 (mass) with anatomic qualifier (mapping suggestion)
Quality of life impact
Crohn’s-related perianal disease and fistulizing disease is described as disabling with significant quality-of-life impairment in contemporary reviews of perianal IBD, but disease-specific QoL quantification for anal adenocarcinoma itself was not retrievable. (inoue2023resectionofanorectal pages 1-3)
4. Genetic / Molecular Information
Molecular subtypes and lineage markers (primary human tumor profiling)
A multi-institutional cohort study (n=74 primary anal canal adenocarcinomas) supports a dualistic model with two region-specific entities: - Anal gland/transitional-type: 26/74 (35.1%), characterized by diffuse Krt7 expression and absence of Krt20/CDX2 (herfs2018adualisticmodel pages 4-5) - Colorectal-type: 48/74 (64.9%), characterized by Krt20/CDX2 positivity and not Krt7 (herfs2018adualisticmodel pages 4-5)
HPV status and p16INK4a
- HPV16/18 infection was detected in an anal gland/transitional subset: 11/26 (42.3%) (herfs2018adualisticmodel pages 8-9)
- Among HPV-infected tumors, 5/11 (45.5%) had patches of p16 negativity and some showed CDKN2A promoter hypermethylation (herfs2018adualisticmodel pages 9-10, herfs2018adualisticmodel pages 8-9)
Mismatch repair deficiency / MSI
Mismatch repair deficiency/MSI-high appears rare in this tumor type: 1/74 (1.4%) MSI-high reported in the dualistic cohort. (herfs2018adualisticmodel pages 8-9)
Immune microenvironment and checkpoints
Anal gland/transitional-type tumors show greater immune infiltration and higher checkpoint expression; the study highlights higher PD-1/PD-L1 expression and T-cell infiltration relative to colorectal-type tumors. Visual summary of immune-marker differences (PD-L1 tumor cell scoring; PD-1+ immune infiltration) is provided in the retrieved figures. (herfs2018adualisticmodel pages 9-10, herfs2018adualisticmodel media 4416b428)
Actionable alterations and pathway context
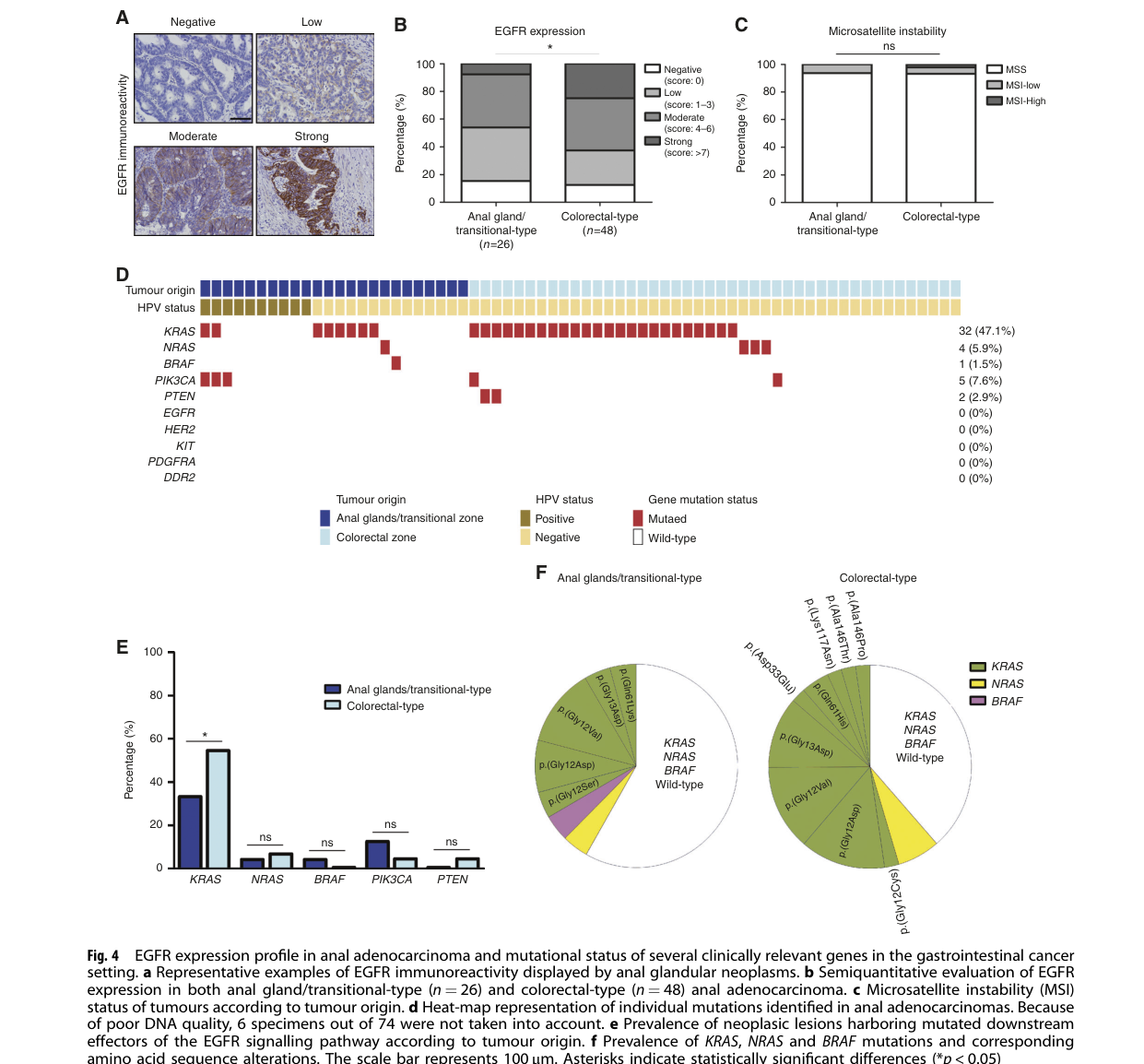
In the 74-case dualistic cohort: - EGFR protein detected by IHC in 64/74 (86.5%) tumors (herfs2018adualisticmodel pages 7-8) - Somatic mutation frequencies included KRAS 47.1%, NRAS 5.9%, PIK3CA 7.6%, PTEN 2.9%, BRAF 1.5%; EGFR, HER2, KIT, PDGFRA, DDR2 mutations were absent in this dataset (herfs2018adualisticmodel pages 7-8) - The subtype comparison and mutation landscape are summarized visually in retrieved figures (heatmap and prevalence plots). (herfs2018adualisticmodel media 502e33fe)
Example case molecular features
A 2021 case report described MSI-high status and KRAS/NRAS/BRAF wild type tumor profiling in an individual patient. (tsay2021analadenocarcinomacase pages 1-2)
Suggested gene/pathway ontologies
- HGNC gene symbols: KRAS, NRAS, PIK3CA, PTEN, BRAF, EGFR, CDKN2A (herfs2018adualisticmodel pages 7-8, herfs2018adualisticmodel pages 8-9)
- Suggested GO biological process terms (mapping suggestions):
- GO:0008285 negative regulation of cell proliferation (cancer hallmark)
- GO:0007169 transmembrane receptor protein tyrosine kinase signaling pathway (EGFR axis)
- GO:0045087 innate immune response / GO:0006955 immune response (immune infiltration/checkpoints)
Suggested CL (cell types) for mechanism annotation (mapping suggestions)
- CD8+ T cell — CL:0000625 (supported conceptually by T-cell infiltration measures) (herfs2018adualisticmodel pages 9-10)
- Regulatory T cell (Foxp3+) — CL:0000815 (herfs2018adualisticmodel pages 9-10)
- Epithelial cell (glandular) — CL:0000066 (tumor origin) (herfs2018adualisticmodel pages 4-5)
5. Environmental Information
Direct environmental toxin/radiation/lifestyle risk factor quantification specific to anal canal adenocarcinoma was not retrievable in the current corpus. The most consistently described non-genetic drivers relate to chronic inflammation (fistula, IBD) rather than classic environmental exposures. (koizumi2023acasereport pages 1-3, inoue2023resectionofanorectal pages 1-3)
6. Mechanism / Pathophysiology
Causal chains (current evidence-supported models)
Pathway A: Chronic fistula/inflammation → mucinous adenocarcinoma Perianal abscess and fistula represent chronic infectious/inflammatory processes; persistent inflammation and epithelial dysplasia within fistula tracts can progress to mucinous adenocarcinoma, often recognized only after symptom change or mass formation. (koizumi2023acasereport pages 1-3, inoue2023resectionofanorectal pages 1-3)
Pathway B: Dualistic anal canal adenocarcinoma model (HPV-dependent vs independent) Primary anal canal adenocarcinoma comprises at least two lineages with distinct etiologies and immune/mutational features. Anal gland/transitional tumors can be HPV16/18-associated and show increased PD-1/PD-L1 and T-cell infiltration, while colorectal-type tumors more closely resemble colorectal mucosal cancers and show different mutation patterns. (herfs2018adualisticmodel pages 1-2, herfs2018adualisticmodel pages 8-9)
Upstream vs downstream processes
- Upstream: chronic inflammation (fistula/IBD), HPV infection in a subset (koizumi2023acasereport pages 1-3, herfs2018adualisticmodel pages 8-9)
- Downstream: oncogenic signaling alterations (KRAS/PI3K axis), immune evasion via PD-1/PD-L1, invasion and metastatic spread (herfs2018adualisticmodel pages 7-8, herfs2018adualisticmodel media 4416b428)
7. Anatomical Structures Affected
Primary site
- Anal canal / cloacogenic/transitional zone region (ICD-O-3 C21.1/C21.2 context; anal canal strict localization in molecular cohort) (gogna2020clinicopathologicfeaturesand pages 2-3, herfs2018adualisticmodel pages 7-8)
Suggested UBERON terms (mapping suggestions)
- Anal canal — UBERON:0001052 (mapping suggestion)
- Anus — UBERON:0001245 (mapping suggestion)
- Rectum (lower rectum interface) — UBERON:0001052? (rectum has separate UBERON ID; mapping suggestion)
Local invasion patterns (case evidence)
Advanced fistula-associated tumors may infiltrate adjacent pelvic structures (e.g., prostate/levator ani/internal obturator described in Crohn’s-associated fistula cancer report). (inoue2023resectionofanorectal pages 1-3)
8. Temporal Development
Typical age of onset
Mean age at diagnosis in a SEER analysis was 68.12 ± 14.02 years. (gogna2020clinicopathologicfeaturesand pages 1-2)
Course/progression patterns
- Fistula-associated cancers can emerge after long-standing disease (>10 years) but may also develop within a few years after perianal abscess/fistula in some cases, emphasizing variable latency. (koizumi2023acasereport pages 1-3)
9. Inheritance and Population
Epidemiology (registry-based)
A SEER population-based study (1973–2015; n=2,090) reports: - Estimated prevalence 0.0011% (gogna2020clinicopathologicfeaturesand pages 1-2) - Incidence trend: +4.03%/year (1973–1985) followed by −0.32%/year (1986–2015) (gogna2020clinicopathologicfeaturesand pages 2-3) - Sex distribution: 54.8% male, 45.2% female (gogna2020clinicopathologicfeaturesand pages 1-2)
No Mendelian inheritance pattern is established; this is primarily a sporadic malignancy with somatic alterations and inflammatory/viral etiologies in subsets. (herfs2018adualisticmodel pages 1-2, herfs2018adualisticmodel pages 7-8)
10. Diagnostics
Clinical and pathology diagnosis
Diagnosis typically relies on anorectal exam, endoscopic evaluation, and biopsy with histopathology and immunohistochemistry to distinguish anal gland/transitional vs colorectal-type tumors.
Histopathology / IHC (subtype assignment) - The dualistic model uses keratin/CDX2 patterns: Krt7 (anal gland/transitional) vs Krt20/CDX2 (colorectal-type). (herfs2018adualisticmodel pages 4-5)
Imaging Case reports use cross-sectional imaging and/or PET for staging and metastatic evaluation. (tsay2021analadenocarcinomacase pages 1-1)
Molecular testing Somatic profiling may include KRAS/NRAS/BRAF testing and MSI/MMR assessment (MSI-high is rare but clinically actionable for immunotherapy in many GI cancers). (tsay2021analadenocarcinomacase pages 1-2, herfs2018adualisticmodel pages 8-9)
Differential diagnosis
A recurring challenge is distinguishing primary anal canal adenocarcinoma from distal rectal adenocarcinoma extending into the anal canal and from fistula-associated extramucosal lesions. (tsay2021analadenocarcinomacase pages 2-3)
11. Outcome / Prognosis
Survival statistics (SEER population data)
In SEER (n=2,090), overall survival at: - 1 year 76.1%, 2 years 63.4%, 3 years 52.6%, 4 years 47.9%, 5 years 39.6% (gogna2020clinicopathologicfeaturesand pages 2-3) Prognosis varies strongly by stage and grade; metastatic disease showed markedly higher mortality (HR ~6). (gogna2020clinicopathologicfeaturesand pages 2-3)
Prognostic factors
- Older age strongly predicts worse survival (e.g., age >81 mean survival 30.14 ± 1.84 months, HR 3.79). (gogna2020clinicopathologicfeaturesand pages 2-3)
- Localized disease is associated with better survival than distant disease. (gogna2020clinicopathologicfeaturesand pages 2-3)
- In the dualistic molecular cohort, anal gland/transitional-type tumors tended toward worse 5-year DFS/OS than colorectal-type tumors (5-year OS 27.8% vs 50.4%). (herfs2018adualisticmodel pages 7-8)
12. Treatment
Current applications / real-world implementations (population-based evidence)
Because of limited disease-specific guidelines, management often extrapolates from rectal adenocarcinoma paradigms and/or multimodality strategies.
Surgery In a SEER analysis, surgery was associated with longer survival (116.7 months vs 42.7 months, p<0.01). (gogna2020clinicopathologicfeaturesand pages 1-2)
Chemoradiation and combined modality In a SEER cohort of stage I–III patients (2010–2016; n=393), 3-year cause-specific survival differed by initial approach: - RT+CTx 63.9% - RT or CTx 35.7% - Surgery alone 77.7% - Preoperative RT/CTx + surgery 80.3% - Postoperative RT/CTx + surgery 65.8% (P<.001). (Park 2020; https://doi.org/10.1016/j.clcc.2020.04.001). (park2020survivaloutcomesafter pages 1-2) Preoperative RT/CTx plus surgery remained associated with improved cause-specific survival (multivariable P=0.024). (park2020survivaloutcomesafter pages 1-2)
Immunotherapy (evidence level: case-based; biomarker-driven) A 2021 case report described pembrolizumab use in an MSI-high anal adenocarcinoma patient with >1-year survival in follow-up narrative. (tsay2021analadenocarcinomacase pages 1-2) For anal adenocarcinoma overall, immune checkpoint relevance is biologically supported by elevated PD-1/PD-L1 in anal gland/transitional tumors, but prospective efficacy data are not established in the retrieved corpus. (herfs2018adualisticmodel pages 9-10, herfs2018adualisticmodel media 4416b428)
Ongoing / recent clinical research (clinicaltrials.gov)
- NCT05605873 (ProCHADA): Retrospective observational cohort (France), enrollment 46; aims to classify forms of anal adenocarcinoma and estimate prognosis; endpoints include 1-year and 5-year mortality; start date 2022-09-16, estimated completion 2023-12-31. (ClinicalTrials.gov record). (NCT05605873 chunk 1)
Suggested MAXO terms (mapping suggestions)
- Abdominoperineal resection — MAXO:0000445 (mapping suggestion)
- Chemoradiotherapy — MAXO:0000602 (mapping suggestion)
- External beam radiotherapy — MAXO:0000014 (mapping suggestion)
- Immune checkpoint inhibitor therapy — MAXO:0001025 (mapping suggestion)
13. Prevention
Evidence specific to adenocarcinoma prevention is limited in retrieved sources. - For fistula-associated cancers, case literature suggests heightened clinical suspicion and early biopsy when chronic fistula symptoms change or masses develop, as delayed diagnosis contributes to advanced presentation. (koizumi2023acasereport pages 1-3, inoue2023resectionofanorectal pages 1-3) - HPV vaccination and anal cancer screening guidelines are largely developed for anal squamous cell carcinoma risk contexts and cannot be directly assumed for adenocarcinoma, especially given mixed HPV evidence by subtype. (tsay2021analadenocarcinomacase pages 2-3, herfs2018adualisticmodel pages 8-9)
14. Other Species / Natural Disease
No directly analogous naturally occurring non-human disease models of anal canal adenocarcinoma were identified in the retrieved evidence. A canine condition, apocrine gland anal sac adenocarcinoma, is anatomically and biologically distinct (anal sac origin) and should not be treated as a direct model for human anal canal adenocarcinoma. (gogna2020clinicopathologicfeaturesand pages 1-2)
15. Model Organisms
No validated, disease-specific model organism systems (mouse, zebrafish, organoid platforms uniquely representing anal canal adenocarcinoma subtypes) were retrieved from the current corpus.
Key quantitative evidence map
The table below compiles the most actionable numeric findings for knowledge-base fields (epidemiology, stage distribution, survival, subtype proportions, HPV/MMR, and mutation frequencies).
Table (click to expand)
| Domain | Key finding (with numbers) | Population/cohort | Study (first author year) | Publication date | URL/DOI | Evidence citation ID |
|---|---|---|---|---|---|---|
| Epidemiology | Estimated prevalence in SEER: 0.0011%; incidence increased 4.03%/year (1973-1985), then declined 0.32%/year (1986-2015) | 2,090 anal canal adenocarcinoma cases from SEER (1973-2015) | Gogna 2020 | 2020-05-13 | https://doi.org/10.1155/2020/5139236 | (gogna2020clinicopathologicfeaturesand pages 1-2, gogna2020clinicopathologicfeaturesand pages 2-3) |
| Epidemiology | Mean age at diagnosis 68.12 ± 14.02 years; 54.8% male; presentation: 44.4% localized, 25.8% regional, 13.5% distant, 6.7% in situ | 2,090 SEER cases | Gogna 2020 | 2020-05-13 | https://doi.org/10.1155/2020/5139236 | (gogna2020clinicopathologicfeaturesand pages 1-2, gogna2020clinicopathologicfeaturesand pages 2-3) |
| Survival | Overall survival rates at 1, 2, 3, 4, 5 years: 76.1%, 63.4%, 52.6%, 47.9%, 39.6% | 2,090 SEER cases | Gogna 2020 | 2020-05-13 | https://doi.org/10.1155/2020/5139236 | (gogna2020clinicopathologicfeaturesand pages 2-3) |
| Survival | Surgery associated with markedly longer survival: 116.7 months vs 42.7 months without surgery (p < 0.01) | 2,090 SEER cases | Gogna 2020 | 2020-05-13 | https://doi.org/10.1155/2020/5139236 | (gogna2020clinicopathologicfeaturesand pages 1-2) |
| Survival | Age >81 years associated with poorer outcome: mean survival 30.14 ± 1.84 months; HR 3.79 (95% CI 2.65-5.41) | 2,090 SEER cases | Gogna 2020 | 2020-05-13 | https://doi.org/10.1155/2020/5139236 | (gogna2020clinicopathologicfeaturesand pages 2-3) |
| Survival | Metastatic disease associated with ~6-fold higher mortality: HR 6.02 (95% CI 4.55-7.99) | 2,090 SEER cases | Gogna 2020 | 2020-05-13 | https://doi.org/10.1155/2020/5139236 | (gogna2020clinicopathologicfeaturesand pages 2-3) |
| Treatment | 3-year cause-specific survival by initial treatment: 63.9% (RT+CTx), 35.7% (RT or CTx), 77.7% (surgery alone), 80.3% (preop RT/CTx + surgery), 65.8% (postop RT/CTx + surgery); P < .001 | 393 stage I-III cases in SEER (2010-2016) | Park 2020 | 2020-09 | https://doi.org/10.1016/j.clcc.2020.04.001 | (park2020survivaloutcomesafter pages 1-2) |
| Treatment | Preoperative RT/CTx plus surgery associated with improved cause-specific survival on multivariable analysis (P = .024) | 393 stage I-III SEER cases | Park 2020 | 2020-09 | https://doi.org/10.1016/j.clcc.2020.04.001 | (park2020survivaloutcomesafter pages 1-2) |
| Molecular subtype | Two subtypes identified: anal gland/transitional-type 26/74 (35.1%) vs colorectal-type 48/74 (64.9%) | 74 primary anal canal adenocarcinomas | Herfs 2018 | 2018 | Not available in retrieved metadata | (herfs2018adualisticmodel pages 4-5) |
| HPV/MMR | HPV16/18 detected only in anal gland/transitional tumors: 11/26 (42.3%); p16 strong/diffuse staining in 12/26 (46.2%) Krt7-positive tumors | 74 tumors; subtype analysis within 26 gland/transitional tumors | Herfs 2018 | 2018 | Not available in retrieved metadata | (herfs2018adualisticmodel pages 8-9, herfs2018adualisticmodel pages 4-5) |
| HPV/MMR | Among HPV-infected tumors, 5/11 (45.5%) showed patches of p16 negativity; MSI-high/MMR-deficient phenotype observed in only 1/74 (1.4%) tumors | 74 tumors | Herfs 2018 | 2018 | Not available in retrieved metadata | (herfs2018adualisticmodel pages 9-10, herfs2018adualisticmodel pages 8-9) |
| Mutations | EGFR protein detected in 64/74 (86.5%) cancers | 74 tumors | Herfs 2018 | 2018 | Not available in retrieved metadata | (herfs2018adualisticmodel pages 9-10, herfs2018adualisticmodel pages 7-8) |
| Mutations | Mutation frequencies: KRAS 47.1%, NRAS 5.9%, PIK3CA 7.6%, PTEN 2.9%, BRAF 1.5%; EGFR, HER2, KIT, PDGFRA, DDR2 mutations absent | 74 tumors | Herfs 2018 | 2018 | Not available in retrieved metadata | (herfs2018adualisticmodel pages 7-8, herfs2018adualisticmodel media 502e33fe) |
| Immune microenvironment | Anal gland/transitional-type tumors showed higher PD-1/PD-L1 expression and more prominent T-cell infiltration than colorectal-type counterparts | 74 tumors | Herfs 2018 | 2018 | Not available in retrieved metadata | (herfs2018adualisticmodel pages 9-10, herfs2018adualisticmodel pages 1-2, herfs2018adualisticmodel media 4416b428) |
| Prognosis by subtype | In survival subset, 65/74 (87.8%) evaluable; 9/74 (12.2%) metastatic at diagnosis; recurrence 10/24 (41.7%) in anal gland/transitional vs 13/41 (31.7%) in colorectal-type; 5-year DFS 33.1% vs 52.6% and 5-year OS 27.8% vs 50.4% | 65 evaluable for OS/DFS within a 74-case cohort | Herfs 2018 | 2018 | Not available in retrieved metadata | (herfs2018adualisticmodel pages 7-8) |
| Comparative prognosis | Anal adenocarcinoma represented 5%-10% of anal canal malignancies and had worse prognosis than rectal adenocarcinoma and anal squamous carcinoma in comparative SEER analysis | SEER comparative cohort; anal adenocarcinoma subset noted as 1,660 in excerpted review | Tsay 2021 | 2021-07 | https://doi.org/10.1136/bmjgast-2021-000661 | (tsay2021analadenocarcinomacase pages 2-3, tsay2021analadenocarcinomacase pages 1-1) |
Table: This table compiles key numeric findings for anal canal adenocarcinoma across epidemiology, survival, molecular subtype, HPV/MMR status, mutations, and treatment outcomes. It is useful as a quick-reference evidence map for populating structured disease knowledge base fields.
Visual evidence (molecular landscape)
Figures from the dualistic model cohort summarize mutation prevalence by subtype and PD-1/PD-L1/T-cell infiltration patterns. - Mutation/subtype overview: (herfs2018adualisticmodel media 502e33fe) - PD-L1 and immune infiltration overview: (herfs2018adualisticmodel media 4416b428)
Expert synthesis and analysis (authoritative interpretation)
- Anal canal adenocarcinoma is not a single entity: evidence supports at least two biologically distinct subtypes (anal gland/transitional vs colorectal-type) with different HPV associations, immune contexture, and mutational landscapes, which implies that “one-size-fits-all” extrapolation from rectal adenocarcinoma or anal squamous carcinoma is likely suboptimal. (herfs2018adualisticmodel pages 1-2, herfs2018adualisticmodel pages 4-5)
- Inflammation-associated disease contexts (Crohn’s/fistula) are clinically important for a subset of tumors (often mucinous), with notable diagnostic delay; surveillance strategies for high-risk fistulizing disease remain an evidence gap requiring prospective evaluation. (koizumi2023acasereport pages 1-3, inoue2023resectionofanorectal pages 1-3)
- Precision oncology opportunities exist but are constrained by KRAS prevalence (~47% in one cohort), which may limit anti-EGFR strategies in many patients; conversely, PD-1/PD-L1–high immune phenotypes in anal gland/transitional tumors provide a biologic rationale for immunotherapy trials, though MSI-high appears rare (~1.4%). (herfs2018adualisticmodel pages 7-8, herfs2018adualisticmodel pages 8-9, herfs2018adualisticmodel media 4416b428)
Limitations of this report (evidence availability)
- Ontology identifiers (MONDO/MeSH/ICD-10/ICD-11/Orphanet) were not retrievable using available tools and texts; only ICD-O-3 site codes used in SEER studies are provided. (gogna2020clinicopathologicfeaturesand pages 2-3)
- Most adenocarcinoma-specific clinical guidance is based on retrospective cohorts and case reports; several potentially relevant 2024 adenocarcinoma studies were listed as unobtainable in tool search results and thus could not be cited.
References
-
(gogna2020clinicopathologicfeaturesand pages 2-3): Shekhar Gogna, Roberto Bergamaschi, Agon Kajmolli, Mahir Gachabayov, Aram Rojas, David Samson, Rifat Latifi, and Xiang Da Dong. Clinicopathologic features and outcome of adenocarcinoma of the anal canal: a population-based study. International Journal of Surgical Oncology, 2020:1-6, May 2020. URL: https://doi.org/10.1155/2020/5139236, doi:10.1155/2020/5139236. This article has 7 citations.
-
(gogna2020clinicopathologicfeaturesand pages 1-2): Shekhar Gogna, Roberto Bergamaschi, Agon Kajmolli, Mahir Gachabayov, Aram Rojas, David Samson, Rifat Latifi, and Xiang Da Dong. Clinicopathologic features and outcome of adenocarcinoma of the anal canal: a population-based study. International Journal of Surgical Oncology, 2020:1-6, May 2020. URL: https://doi.org/10.1155/2020/5139236, doi:10.1155/2020/5139236. This article has 7 citations.
-
(park2020survivaloutcomesafter pages 1-2): Hyojung Park. Survival outcomes after initial treatment for anal adenocarcinoma: a population-based cohort study. Clinical Colorectal Cancer, 19:e75-e82, Sep 2020. URL: https://doi.org/10.1016/j.clcc.2020.04.001, doi:10.1016/j.clcc.2020.04.001. This article has 6 citations and is from a peer-reviewed journal.
-
(tsay2021analadenocarcinomacase pages 2-3): Cynthia J Tsay, Thomas Pointer, Jocelyn B Chandler, Anil B Nagar, and Petr Protiva. Anal adenocarcinoma: case report, literature review and comparative survival analysis. BMJ Open Gastroenterology, 8:e000661, Jul 2021. URL: https://doi.org/10.1136/bmjgast-2021-000661, doi:10.1136/bmjgast-2021-000661. This article has 6 citations and is from a peer-reviewed journal.
-
(koizumi2023acasereport pages 1-3): Michihiro Koizumi, Akihisa Matsuda, Takeshi Yamada, Koji Morimoto, Itaru Kubota, Yawara Kubota, Shuzo Tamura, Kenta Tominaga, Takashi Sakatani, and Hiroshi Yoshida. A case report of anal fistula-associated mucinous adenocarcinoma developing 3 years after treatment of perianal abscess. Surgical Case Reports, Sep 2023. URL: https://doi.org/10.1186/s40792-023-01743-3, doi:10.1186/s40792-023-01743-3. This article has 15 citations.
-
(inoue2023resectionofanorectal pages 1-3): Takuya Inoue, Yuki Sekido, Takayuki Ogino, Tsuyoshi Hata, Norikatsu Miyoshi, Hidekazu Takahashi, Mamoru Uemura, Tsunekazu Mizushima, Yuichiro Doki, and Hidetoshi Eguchi. Resection of anorectal fistula cancer associated with crohn’s disease after preoperative chemoradiotherapy: a case report. Surgical Case Reports, Nov 2023. URL: https://doi.org/10.1186/s40792-023-01778-6, doi:10.1186/s40792-023-01778-6. This article has 10 citations.
-
(NCT05605873 chunk 1): Clinical, Histological and Prognostic Forms of Adenocarcinoma of the Anus. Fondation Hôpital Saint-Joseph. 2022. ClinicalTrials.gov Identifier: NCT05605873
-
(herfs2018adualisticmodel pages 1-2): M Herfs, P Roncarati, B Koopmansch, O Peulen, D Bruyere, A Lebeau, E Hendrick, and P Hubert. A dualistic model of primary anal canal adenocarcinoma with distinct cellular origins, etiologies, inflammatory microenvironments and mutational signatures …. Unknown journal, 2018.
-
(herfs2018adualisticmodel pages 8-9): M Herfs, P Roncarati, B Koopmansch, O Peulen, D Bruyere, A Lebeau, E Hendrick, and P Hubert. A dualistic model of primary anal canal adenocarcinoma with distinct cellular origins, etiologies, inflammatory microenvironments and mutational signatures …. Unknown journal, 2018.
-
(tsay2021analadenocarcinomacase pages 1-1): Cynthia J Tsay, Thomas Pointer, Jocelyn B Chandler, Anil B Nagar, and Petr Protiva. Anal adenocarcinoma: case report, literature review and comparative survival analysis. BMJ Open Gastroenterology, 8:e000661, Jul 2021. URL: https://doi.org/10.1136/bmjgast-2021-000661, doi:10.1136/bmjgast-2021-000661. This article has 6 citations and is from a peer-reviewed journal.
-
(herfs2018adualisticmodel pages 4-5): M Herfs, P Roncarati, B Koopmansch, O Peulen, D Bruyere, A Lebeau, E Hendrick, and P Hubert. A dualistic model of primary anal canal adenocarcinoma with distinct cellular origins, etiologies, inflammatory microenvironments and mutational signatures …. Unknown journal, 2018.
-
(herfs2018adualisticmodel pages 9-10): M Herfs, P Roncarati, B Koopmansch, O Peulen, D Bruyere, A Lebeau, E Hendrick, and P Hubert. A dualistic model of primary anal canal adenocarcinoma with distinct cellular origins, etiologies, inflammatory microenvironments and mutational signatures …. Unknown journal, 2018.
-
(herfs2018adualisticmodel media 4416b428): M Herfs, P Roncarati, B Koopmansch, O Peulen, D Bruyere, A Lebeau, E Hendrick, and P Hubert. A dualistic model of primary anal canal adenocarcinoma with distinct cellular origins, etiologies, inflammatory microenvironments and mutational signatures …. Unknown journal, 2018.
-
(herfs2018adualisticmodel pages 7-8): M Herfs, P Roncarati, B Koopmansch, O Peulen, D Bruyere, A Lebeau, E Hendrick, and P Hubert. A dualistic model of primary anal canal adenocarcinoma with distinct cellular origins, etiologies, inflammatory microenvironments and mutational signatures …. Unknown journal, 2018.
-
(herfs2018adualisticmodel media 502e33fe): M Herfs, P Roncarati, B Koopmansch, O Peulen, D Bruyere, A Lebeau, E Hendrick, and P Hubert. A dualistic model of primary anal canal adenocarcinoma with distinct cellular origins, etiologies, inflammatory microenvironments and mutational signatures …. Unknown journal, 2018.
-
(tsay2021analadenocarcinomacase pages 1-2): Cynthia J Tsay, Thomas Pointer, Jocelyn B Chandler, Anil B Nagar, and Petr Protiva. Anal adenocarcinoma: case report, literature review and comparative survival analysis. BMJ Open Gastroenterology, 8:e000661, Jul 2021. URL: https://doi.org/10.1136/bmjgast-2021-000661, doi:10.1136/bmjgast-2021-000661. This article has 6 citations and is from a peer-reviewed journal.