Optic Neuritis
Optic neuritis is an inflammatory optic neuropathy in which immune-mediated injury of the optic nerve causes acute or subacute visual dysfunction. Modern classification treats optic neuritis as a heterogeneous syndrome: it can be isolated, multiple sclerosis-associated, MOG-IgG-associated, AQP4-IgG neuromyelitis optica spectrum disorder-associated, or linked to other systemic, infectious, or inflammatory disorders. Accurate etiologic attribution at the first attack is clinically important because acute treatment, relapse prevention, and prognosis differ across subgroups.
Ask OpenScientist
Ask a research question about Optic Neuritis. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Mappings
Definitions
3- optic neuritis
- visual loss
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Subtypes
6Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Pathophysiology
4Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Pathograph
- Target 'Optic Nerve Conduction Delay' (from 'Immune-mediated optic nerve inflammation') not found in named elements
- Target 'Visual Dysfunction' (from 'Immune-mediated optic nerve inflammation') not found in named elements
- Target 'Visual Evoked Potential Latency Prolongation' (from 'Inflammatory demyelinating optic neuropathy') not found in named elements
- Target 'Inflammatory Demyelinating Optic Neuropathy' (from 'MOG-IgG-mediated demyelinating optic neuritis') not found in named elements
- Target 'Secondary Demyelination and Neuronal Injury' (from 'AQP4-IgG astrocytopathic optic neuritis') not found in named elements
- ... and 1 more
Phenotypes
13Eye 6
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Constitutional 1
Show evidence (1 reference)
Other 6
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Medical Actions
4Show evidence (3 references)
Show evidence (4 references)
Show evidence (1 reference)
Show evidence (1 reference)
Biochemical Markers
3Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Differential Diagnoses
3Conditions with similar clinical presentations that must be differentiated from Optic Neuritis:
- Often painless sudden vision loss rather than subacute painful inflammatory visual loss.
- Optic disc findings and vascular risk profile may favor ischemic neuropathy.
Show evidence (1 reference)
- Normal objective afferent visual pathway findings argue against optic neuritis.
- A single symptom such as eye pain should not substitute for optic nerve evidence.
Show evidence (1 reference)
- Systemic symptoms, uveitis, granulomatous disease, vascular inflammation, or infectious exposure can redirect evaluation.
- Etiology-specific treatment may be required beyond acute corticosteroids.
Show evidence (1 reference)
Clinical Trials
6Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Source YAML
click to showname: Optic Neuritis
creation_date: "2026-05-16T16:31:33Z"
updated_date: "2026-05-16T16:44:27Z"
category: Neurological Disorder
parents:
- Autoimmune Disorder
- Demyelinating Disease
- Eye disorder
disease_term:
preferred_term: optic neuritis
term:
id: MONDO:0005885
label: optic neuritis
mappings:
mondo_mappings:
- term:
id: MONDO:0005885
label: optic neuritis
mapping_predicate: skos:exactMatch
mapping_source: MONDO
mapping_justification: >-
Primary MONDO disease term for the broad optic neuritis entry.
description: >-
Optic neuritis is an inflammatory optic neuropathy in which immune-mediated
injury of the optic nerve causes acute or subacute visual dysfunction. Modern
classification treats optic neuritis as a heterogeneous syndrome: it can be
isolated, multiple sclerosis-associated, MOG-IgG-associated, AQP4-IgG
neuromyelitis optica spectrum disorder-associated, or linked to other systemic,
infectious, or inflammatory disorders. Accurate etiologic attribution at the
first attack is clinically important because acute treatment, relapse
prevention, and prognosis differ across subgroups.
external_assertions:
- name: Orphanet isolated optic neuritis disease record
source: Orphanet
assertion_type: structured_disease_record
external_id: ORPHA:499096
url: https://www.orpha.net/en/disease/detail/499096
description: >-
Orphanet ORPHA:499096 is a structured record for isolated optic neuritis, a
narrower disorder within the broader optic neuritis syndrome curated here.
The record provides an isolated-disease definition, ICD-10/ICD-11
cross-references, MONDO:0044688 exact mapping, and HPO phenotype
annotations used for isolated optic neuritis features.
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "MONDO:0044688 | Exact"
explanation: >-
Orphanet maps the isolated optic neuritis record to MONDO:0044688, which
is represented as an isolated subtype rather than the broad disease term.
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "A rare inflammatory optic neuropathy"
explanation: >-
Orphanet defines isolated optic neuritis as an inflammatory optic
neuropathy.
- name: Orphanet single isolated optic neuritis subtype record
source: Orphanet
assertion_type: structured_subtype_record
external_id: ORPHA:659626
url: http://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=en&Expert=659626
description: >-
Orphanet records single isolated optic neuritis as a clinical subtype of
isolated optic neuritis and maps it exactly to MONDO:0971049.
evidence:
- reference: ORPHA:659626
reference_title: Single isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "MONDO:0971049 | Exact"
explanation: >-
The Orphanet subtype record provides an exact MONDO mapping for single
isolated optic neuritis.
- name: Orphanet relapsing isolated optic neuritis subtype record
source: Orphanet
assertion_type: structured_subtype_record
external_id: ORPHA:659634
url: http://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=en&Expert=659634
description: >-
Orphanet records relapsing isolated optic neuritis as a clinical subtype of
isolated optic neuritis and maps it exactly to MONDO:0971050.
evidence:
- reference: ORPHA:659634
reference_title: Relapsing isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "MONDO:0971050 | Exact"
explanation: >-
The Orphanet subtype record provides an exact MONDO mapping for relapsing
isolated optic neuritis.
definitions:
- name: Autoimmune optic neuritis spectrum
definition_type: CASE_DEFINITION
description: >-
Autoimmune optic neuritis is a heterogeneous inflammatory optic-nerve
syndrome spanning multiple sclerosis, NMOSD, MOGAD, isolated optic neuritis,
and other etiologies. First-attack attribution should combine clinical red
flags with orbital MRI, antibody assays, OCT, visual evoked potentials, and
selected fluid biomarkers.
criteria_sets:
- name: Multimodal first-attack attribution
core_clinical_characteristics:
- preferred_term: optic neuritis
term:
id: HP:0100653
label: Optic neuritis
- preferred_term: visual loss
term:
id: HP:0000572
label: Visual loss
evidence:
- reference: PMID:41688447
reference_title: An update on the developments and challenges with the diagnosis and classification of autoimmune optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Early and accurate attribution at the first attack is clinically decisive
explanation: >-
The 2026 review frames autoimmune optic neuritis as a heterogeneous
spectrum whose first-attack attribution affects treatment choice.
- name: International optic neuritis diagnostic-classification framework
definition_type: DIAGNOSTIC_CRITERIA
description: >-
The 2022 international framework begins with clinical features sufficient
for possible optic neuritis, then uses paraclinical tests including brain,
orbital, and retinal imaging, antibody testing, and protein biomarkers to
support definite optic neuritis and classify disease subgroups.
evidence:
- reference: PMID:36179757
reference_title: Diagnosis and classification of optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
developed diagnostic criteria for optic neuritis and a classification of
optic neuritis subgroups
explanation: >-
Petzold et al. provide the consensus classification framework used to
distinguish optic neuritis subgroups.
- name: Orphanet isolated optic neuritis definition
definition_type: OTHER
description: >-
Isolated optic neuritis consists of single or recurrent optic neuritis
episodes not associated with another neurologic or systemic disease.
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: >-
isolated episodes (either single or recurrent) of optic neuritis
explanation: >-
Orphanet defines the isolated subtype by single or recurrent attacks in
the absence of another neurologic or systemic disorder.
has_subtypes:
- name: Isolated optic neuritis
description: >-
Optic neuritis occurring as isolated single or recurrent attacks without
another neurologic or systemic disease explaining the presentation.
subtype_term:
preferred_term: isolated optic neuritis
term:
id: MONDO:0044688
label: isolated optic neuritis
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: >-
not associated with other neurological or systemic disease
explanation: >-
Orphanet explicitly defines isolated optic neuritis by absence of an
associated neurologic or systemic disease.
- name: Single isolated optic neuritis
description: >-
A monophasic isolated optic neuritis attack without recurrent optic neuritis
during follow-up.
subtype_term:
preferred_term: single isolated optic neuritis
term:
id: MONDO:0971049
label: single isolated optic neuritis
evidence:
- reference: ORPHA:659626
reference_title: Single isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "Single isolated optic neuritis"
explanation: >-
Orphanet records single isolated optic neuritis as a clinical subtype of
isolated optic neuritis.
- name: Relapsing isolated optic neuritis
description: >-
Recurrent isolated optic neuritis attacks without another identified
neurologic or systemic disease driver.
subtype_term:
preferred_term: relapsing isolated optic neuritis
term:
id: MONDO:0971050
label: relapsing isolated optic neuritis
evidence:
- reference: ORPHA:659634
reference_title: Relapsing isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "Relapsing isolated optic neuritis"
explanation: >-
Orphanet records relapsing isolated optic neuritis as a clinical subtype
of isolated optic neuritis.
- reference: PMID:30612145
reference_title: Incidence and timing of recurrence of optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
monitoring for recurrence is needed even in patients with a single
episode
explanation: >-
Adult follow-up data support recurrence as a clinically important course
pattern after a first optic neuritis episode.
- name: Multiple sclerosis-associated optic neuritis
description: >-
Optic neuritis attributable to multiple sclerosis, often a first
demyelinating event requiring MS-specific prognostic assessment and
disease-modifying treatment decisions.
evidence:
- reference: PMID:36179757
reference_title: Diagnosis and classification of optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
timely treatment of individuals with multiple sclerosis
explanation: >-
The international classification paper identifies multiple sclerosis as a
key etiologic subgroup requiring early attribution.
- name: MOG-IgG-associated optic neuritis
description: >-
Optic neuritis occurring within MOG antibody-associated disease, commonly
presenting as acute optic neuritis and often requiring MOGAD-specific
relapse-risk assessment.
evidence:
- reference: PMID:36706773
reference_title: "Diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease: International MOGAD Panel proposed criteria."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
MOGAD is typically associated with acute disseminated encephalomyelitis,
optic neuritis, or transverse myelitis
explanation: >-
The international MOGAD criteria establish optic neuritis as a typical
MOGAD phenotype.
- reference: PMID:38783085
reference_title: MOG antibody-associated optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "MOGAD most frequently presents with optic neuritis"
explanation: >-
The MOG-ON review supports optic neuritis as the most frequent MOGAD
presentation and describes bilateral involvement, disc swelling, and
longitudinally extensive optic nerve hyperintensity as distinguishing
features.
- name: AQP4-IgG/NMOSD-associated optic neuritis
description: >-
Optic neuritis caused by AQP4-IgG-positive neuromyelitis optica spectrum
disorder. Attacks can be severe, may involve long optic-nerve segments or
the chiasm, and should prompt NMOSD-specific relapse prevention.
evidence:
- reference: PMID:26092914
reference_title: International consensus diagnostic criteria for neuromyelitis optica spectrum disorders.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
clinical syndromes or MRI findings related to optic nerve
explanation: >-
The NMOSD criteria identify optic-nerve involvement as a core clinical
characteristic in AQP4-IgG-positive disease.
epidemiology:
- name: Colombian national incidence, 2015-2019
description: >-
Population-based estimate from the Colombian national health registry using
ICD-10 optic neuritis coding.
minimum_value: 1.56
unit: cases per 100000 inhabitants per year
notes: >-
The cohort identified 2,463 new cases from 2015 to 2019; 66% of patients
were female.
evidence:
- reference: PMID:38133944
reference_title: "Colombian Ocular Inflammatory Diseases Epidemiology Study (COIDES): Optic Neuritis Incidence Between 2015-2020."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
overall 5-year incidence rate was 1.56 cases per 100,000 inhabitants per
year
explanation: >-
COIDES provides a recent national population-based incidence estimate for
optic neuritis.
- name: Afro-descendant Martinique cohort incidence, 2018-2022
description: >-
Retrospective cohort estimate from Martinique using the 2022 Lancet optic
neuritis criteria after neuro-ophthalmologic evaluation.
minimum_value: 1.61
unit: cases per 100000 person-years
notes: >-
Final diagnoses included MS-associated, MOG-associated, NMOSD-associated,
single isolated, relapsing isolated, and unclassified optic neuritis.
evidence:
- reference: PMID:39963868
reference_title: "Incidence of optic neuritis among Afro-descendant, a cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The overall incidence was 1.61"
explanation: >-
The Martinique cohort provides a population estimate in an
Afro-descendant population and applies the 2022 criteria.
pathophysiology:
- name: Immune-mediated optic nerve inflammation
description: >-
Optic neuritis is driven by inflammatory injury within the optic nerve,
producing acute or subacute visual dysfunction. The broad syndrome includes
isolated inflammatory optic neuropathy as well as disease-specific immune
mechanisms in MS, MOGAD, NMOSD, and systemic inflammatory disease.
locations:
- preferred_term: cranial nerve II
term:
id: UBERON:0000941
label: cranial nerve II
biological_processes:
- preferred_term: inflammatory response
term:
id: GO:0006954
label: inflammatory response
modifier: INCREASED
- preferred_term: neuroinflammatory response
term:
id: GO:0150076
label: neuroinflammatory response
modifier: INCREASED
downstream:
- target: Optic Nerve Conduction Delay
description: >-
Inflammation and demyelination delay optic pathway conduction, which can
be measured with visual evoked potentials.
- target: Visual Dysfunction
description: >-
Optic nerve inflammation causes visual acuity loss, dyschromatopsia,
visual field defects, and reduced contrast sensitivity.
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "A rare inflammatory optic neuropathy"
explanation: >-
The Orphanet structured record anchors the isolated form as inflammatory
optic neuropathy.
- reference: PMID:41688447
reference_title: An update on the developments and challenges with the diagnosis and classification of autoimmune optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Autoimmune optic neuritis (ON) is a heterogeneous spectrum
explanation: >-
The 2026 review supports heterogeneous immune-mediated etiologies for
optic neuritis.
- name: Inflammatory demyelinating optic neuropathy
description: >-
Many optic neuritis attacks are demyelinating optic neuropathies. Loss or
dysfunction of optic nerve myelin slows visual pathway conduction and is
reflected by prolonged visual evoked potential latency; retinal and optic
nerve structural injury can be followed by OCT.
locations:
- preferred_term: cranial nerve II
term:
id: UBERON:0000941
label: cranial nerve II
cell_types:
- preferred_term: oligodendrocyte
term:
id: CL:0000128
label: oligodendrocyte
biological_processes:
- preferred_term: myelination
term:
id: GO:0042552
label: myelination
modifier: DECREASED
cellular_components:
- preferred_term: myelin sheath
term:
id: GO:0043209
label: myelin sheath
modifier: DECREASED
downstream:
- target: Visual Evoked Potential Latency Prolongation
description: >-
Demyelinating injury slows optic nerve conduction and prolongs P100 or
full-field VEP latency.
evidence:
- reference: clinicaltrials:NCT01524250
reference_title: "Recovery of Demyelinating Optic Neuritis After Treatment With Equivalent High Doses of Oral vs. Intravenous Corticosteroids: a Randomized Single Blinded Clinical Trial"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "acute demyelinating optic neuritis"
explanation: >-
The randomized oral-versus-intravenous corticosteroid trial record
specifically enrolled acute demyelinating optic neuritis.
- reference: PMID:28229892
reference_title: "Safety and efficacy of opicinumab in acute optic neuritis (RENEW): a randomised, placebo-controlled, phase 2 trial."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
measured as recovery of affected optic nerve conduction latency
explanation: >-
RENEW used optic nerve conduction latency recovery as a remyelination
endpoint, linking optic neuritis to demyelinating conduction delay.
- name: MOG-IgG-mediated demyelinating optic neuritis
description: >-
In MOGAD-associated optic neuritis, antibodies to conformational MOG
epitopes identify a demyelinating disease that is distinct from MS and
AQP4-IgG NMOSD. MOG-IgG effector mechanisms include complement-dependent
cytotoxicity, antibody-dependent cellular cytotoxicity, and T-cell supported
CNS inflammation.
biological_processes:
- preferred_term: complement activation
term:
id: GO:0006956
label: complement activation
modifier: INCREASED
- preferred_term: T cell mediated immunity
term:
id: GO:0002456
label: T cell mediated immunity
modifier: INCREASED
downstream:
- target: Inflammatory Demyelinating Optic Neuropathy
description: >-
MOG-IgG effector mechanisms converge on oligodendrocyte/myelin injury in
optic neuritis attacks.
evidence:
- reference: PMID:36706773
reference_title: "Diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease: International MOGAD Panel proposed criteria."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Serum antibodies directed against myelin oligodendrocyte glycoprotein
explanation: >-
International criteria establish serum MOG-IgG as the defining biomarker
for MOGAD, a common optic neuritis etiology.
- reference: PMID:40088708
reference_title: "Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD): Insights into pathogenesis and biomarkers of prognosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
MOG-IgG-mediated demyelination occurs via complement-dependent
cytotoxicity
explanation: >-
The review describes antibody effector mechanisms relevant to MOGAD optic
neuritis.
- name: AQP4-IgG astrocytopathic optic neuritis
description: >-
In AQP4-IgG-positive NMOSD, optic neuritis reflects astrocyte-targeted
autoimmunity with complement-mediated injury and secondary demyelination.
This mechanism differs from primary MS-type demyelination and from MOGAD.
genes:
- preferred_term: AQP4
term:
id: hgnc:637
label: AQP4
cell_types:
- preferred_term: astrocyte
term:
id: CL:0000127
label: astrocyte
biological_processes:
- preferred_term: complement activation, classical pathway
term:
id: GO:0006958
label: complement activation, classical pathway
modifier: INCREASED
downstream:
- target: Secondary Demyelination and Neuronal Injury
description: >-
Complement-mediated astrocyte injury propagates demyelinating and axonal
damage in optic pathways.
evidence:
- reference: PMID:26092914
reference_title: International consensus diagnostic criteria for neuromyelitis optica spectrum disorders.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
associated with serum aquaporin-4 immunoglobulin G antibodies
explanation: >-
The NMOSD consensus criteria establish AQP4-IgG as the defining
serologic marker for the AQP4-positive optic neuritis subgroup.
phenotypes:
- name: Optic Neuritis
description: >-
Inflammation of the optic nerve with acute or subacute visual symptoms.
category: Ophthalmologic
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: optic neuritis
term:
id: HP:0100653
label: Optic neuritis
evidence:
- reference: PMID:36179757
reference_title: Diagnosis and classification of optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "diagnostic criteria for optic neuritis"
explanation: >-
Optic neuritis is the defining phenotype and the target of the
diagnostic classification framework.
- name: Bilateral Optic Neuritis
description: >-
Bilateral optic nerve involvement is a distinguishing clinical pattern in
MOG-IgG-associated optic neuritis and may also occur in some NMOSD and
pediatric presentations. HPO lacks a specific bilateral optic neuritis term,
so the base optic neuritis phenotype is used with a bilateral preferred
term.
category: Ophthalmologic
subtype: MOG-IgG-associated optic neuritis
frequency: FREQUENT
phenotype_term:
preferred_term: bilateral optic neuritis
term:
id: HP:0100653
label: Optic neuritis
evidence:
- reference: PMID:38783085
reference_title: MOG antibody-associated optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Bilateral involvement, disc swelling clinically and radiologically
explanation: >-
The 2024 MOG-ON review identifies bilateral involvement and disc swelling
as characteristic features that help distinguish MOG-associated optic
neuritis from other etiologies.
- name: Visual Loss
description: >-
Acute or subacute visual loss is a key presenting manifestation, ranging
from blurred vision to severe loss of acuity depending on etiology and
attack severity.
category: Ophthalmologic
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: visual loss
term:
id: HP:0000572
label: Visual loss
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "subacute unilateral loss of vision"
explanation: >-
Orphanet lists subacute unilateral visual loss as a typical presentation
of isolated optic neuritis.
- name: Eye Movement-Induced Pain
description: >-
Periocular pain, often worsened by eye movement, is a common symptom and may
precede visual symptoms.
category: Ophthalmologic
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: Eye movement-induced pain
term:
id: HP:0030857
label: Eye movement-induced pain
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "pain on eye movement"
explanation: >-
Orphanet annotates eye movement-induced pain as very frequent in isolated
optic neuritis.
- name: Ocular Pain
description: >-
Ocular or periocular pain is a frequent presenting symptom.
category: Ophthalmologic
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: Ocular pain
term:
id: HP:0200026
label: Ocular pain
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "periocular pain"
explanation: >-
Orphanet annotates ocular pain as very frequent in isolated optic
neuritis.
- name: Dyschromatopsia
description: >-
Abnormal color vision is common and can be disproportionate to visual acuity
loss.
category: Ophthalmologic
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: Dyschromatopsia
term:
id: HP:0007641
label: Dyschromatopsia
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "abnormal color vision"
explanation: >-
Orphanet annotates dyschromatopsia as very frequent in isolated optic
neuritis.
- name: Visual Field Defect
description: >-
Visual field loss is a common objective manifestation of optic nerve
dysfunction.
category: Ophthalmologic
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: Visual field defect
term:
id: HP:0001123
label: Visual field defect
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "Visual field defect"
explanation: >-
Orphanet annotates visual field defect as very frequent in isolated optic
neuritis.
- name: Central Scotoma
description: >-
Central visual field loss may occur because optic neuritis often affects
fibers serving central vision.
category: Ophthalmologic
frequency: FREQUENT
phenotype_term:
preferred_term: Central scotoma
term:
id: HP:0000603
label: Central scotoma
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "Central scotoma"
explanation: >-
Orphanet annotates central scotoma as frequent in isolated optic
neuritis.
- name: Reduced Contrast Sensitivity
description: >-
Reduced contrast sensitivity can persist even when high-contrast visual
acuity improves.
category: Ophthalmologic
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: Reduced contrast sensitivity
term:
id: HP:0032036
label: Reduced contrast sensitivity
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "reduced contrast sensitivity"
explanation: >-
Orphanet annotates reduced contrast sensitivity as very frequent in
isolated optic neuritis.
- name: Marcus Gunn Pupil
description: >-
A relative afferent pupillary defect can occur with unilateral or asymmetric
optic nerve dysfunction.
category: Ophthalmologic
frequency: FREQUENT
phenotype_term:
preferred_term: Marcus Gunn pupil
term:
id: HP:0200057
label: Marcus Gunn pupil
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "relative afferent pupillary defect"
explanation: >-
Orphanet lists relative afferent pupillary defect and annotates Marcus
Gunn pupil as frequent.
- name: Optic Disc Swelling
description: >-
Optic disc edema or papillitis may be present, particularly in some
pediatric, MOG-associated, and isolated optic neuritis presentations.
category: Ophthalmologic
frequency: FREQUENT
phenotype_term:
preferred_term: Optic disc edema
term:
id: HP:0012795
label: Abnormal optic disc morphology
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "optic disc appears swollen"
explanation: >-
Orphanet lists swollen optic disc as a frequent isolated optic neuritis
feature; HP:0012795 is used as the closest HPO parent because papilledema
specifically denotes optic disc swelling from raised intracranial
pressure.
- name: Photopsia
description: >-
Light flashes with eye movement can occur in a minority of patients.
category: Ophthalmologic
frequency: OCCASIONAL
phenotype_term:
preferred_term: Photopsia
term:
id: HP:0030786
label: Photopsia
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "light flashes on eye movement"
explanation: >-
Orphanet annotates photopsia as occasional in isolated optic neuritis.
- name: Abnormal Visual Evoked Potentials
description: >-
Visual evoked potential latency can be prolonged by demyelinating optic
nerve injury and can be used as an objective functional measure.
category: Electrophysiologic
phenotype_term:
preferred_term: Abnormality of visual evoked potentials
term:
id: HP:0000649
label: Abnormality of visual evoked potentials
evidence:
- reference: PMID:29507942
reference_title: "Effect of Treating Acute Optic Neuritis With Bioequivalent Oral vs Intravenous Corticosteroids: A Randomized Clinical Trial."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "P100 component of the visual evoked potential"
explanation: >-
The randomized corticosteroid trial used VEP P100 latency recovery as a
primary optic nerve function outcome.
biochemical:
- name: MOG-IgG seropositivity
presence: PRESENT
context: >-
Serum MOG-IgG identifies MOGAD-associated optic neuritis and should be
interpreted with assay quality, titer, and phenotype in mind.
evidence:
- reference: PMID:36706773
reference_title: "Diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease: International MOGAD Panel proposed criteria."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "presence of MOG-IgG is a core criterion"
explanation: >-
International MOGAD criteria define MOG-IgG as a core diagnostic
criterion for MOGAD-associated optic neuritis.
- name: AQP4-IgG seropositivity
presence: PRESENT
context: >-
Serum AQP4-IgG identifies NMOSD-associated optic neuritis and strongly
changes relapse-prevention and acute-attack management.
evidence:
- reference: PMID:26092914
reference_title: International consensus diagnostic criteria for neuromyelitis optica spectrum disorders.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "NMOSD with or without AQP4-IgG"
explanation: >-
The NMOSD consensus framework stratifies disease by AQP4-IgG serostatus.
- name: Serum neurofilament light chain and serum GFAP
presence: INCREASED
context: >-
Serum neurofilament light chain and serum glial fibrillary acidic protein
are emerging injury biomarkers that may help refine risk estimates,
particularly in seronegative or diagnostically gray-zone optic neuritis.
evidence:
- reference: PMID:41688447
reference_title: An update on the developments and challenges with the diagnosis and classification of autoimmune optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
may refine risk estimates, especially in seronegative cases
explanation: >-
The 2026 review identifies sNfL and sGFAP as emerging adjunct biomarkers
for risk estimation in autoimmune optic neuritis.
diagnosis:
- name: Multimodal optic neuritis classification workup
description: >-
Diagnostic evaluation should establish optic neuritis and then attribute the
attack to the correct subgroup using clinical pattern, brain/orbital/retinal
imaging, antibody testing, VEP, and selected protein biomarkers.
results: >-
Supports classification into isolated, MS-associated, MOGAD-associated,
NMOSD-associated, systemic inflammatory, infectious, or unclassified optic
neuritis.
diagnosis_term:
preferred_term: diagnostic procedure
term:
id: MAXO:0000003
label: diagnostic procedure
evidence:
- reference: PMID:36179757
reference_title: Diagnosis and classification of optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
brain, orbital, and retinal imaging, together with antibody and other
protein biomarker data
explanation: >-
The international framework supports a multimodal diagnostic process for
definite optic neuritis and subgroup classification.
- name: Orbital and brain MRI
description: >-
MRI documents optic nerve enhancement or T2 signal abnormality, screens for
MS-type brain lesions, and helps identify NMOSD or MOGAD red flags such as
long optic-nerve involvement, chiasmal extension, or associated myelitis.
results: >-
MRI supports diagnosis and etiologic classification when interpreted with
clinical pattern and serology.
diagnosis_term:
preferred_term: magnetic resonance imaging procedure
term:
id: MAXO:0000424
label: magnetic resonance imaging procedure
evidence:
- reference: PMID:41688447
reference_title: An update on the developments and challenges with the diagnosis and classification of autoimmune optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
standardized diagnostic pathways integrating orbital magnetic resonance
imaging
explanation: >-
The 2026 review identifies orbital MRI as a key component of standardized
diagnostic pathways.
- name: Optical coherence tomography
description: >-
OCT measures retinal nerve fiber layer and ganglion cell complex injury,
helping quantify structural damage and follow recovery or atrophy after an
attack.
results: >-
OCT provides retinal structural markers that complement MRI, VEP, and
serologic testing.
diagnosis_term:
preferred_term: optical coherence tomography
term:
id: MAXO:0000969
label: optical coherence tomography
evidence:
- reference: PMID:41688447
reference_title: An update on the developments and challenges with the diagnosis and classification of autoimmune optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "antibody assays, OCT, and visual evoked potentials"
explanation: >-
The 2026 review lists OCT among tools needed for standardized autoimmune
optic neuritis diagnosis.
- reference: PMID:36810323
reference_title: Diagnostic value of intereye difference metrics for optic neuritis in aquaporin-4 antibody seropositive neuromyelitis optica spectrum disorders
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Results support the validation of the IED metrics
explanation: >-
This multicenter AQP4+ NMOSD study validates OCT intereye-difference
metrics for optic neuritis in an antibody-defined subgroup.
- reference: PMID:39231384
reference_title: Diagnostic Value of Inter-Eye Difference Metrics on OCT for Myelin Oligodendrocyte Glycoprotein Antibody-Associated Optic Neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
diagnostic accuracy of OCT-based IED metrics for ON was high
explanation: >-
This multicenter MOG-ON study validates OCT intereye-difference metrics,
especially macular ganglion cell and inner plexiform layer percentage
difference.
- name: Visual evoked potential procedure
description: >-
Visual evoked potentials assess optic pathway conduction delay and can
provide functional evidence of demyelinating optic nerve injury.
results: >-
Prolonged VEP latency supports optic nerve conduction slowing and can be
tracked during recovery.
diagnosis_term:
preferred_term: visual evoked potential procedure
term:
id: MAXO:0035097
label: visual evoked potential procedure
evidence:
- reference: PMID:29507942
reference_title: "Effect of Treating Acute Optic Neuritis With Bioequivalent Oral vs Intravenous Corticosteroids: A Randomized Clinical Trial."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "recovery of the latency of the P100 component"
explanation: >-
VEP latency recovery was used as a functional optic nerve outcome in a
randomized optic neuritis treatment trial.
- name: AQP4-IgG and MOG-IgG antibody testing
description: >-
Serum antibody testing is central for distinguishing MOGAD-associated and
AQP4-IgG NMOSD-associated optic neuritis from MS-associated, isolated, and
other inflammatory optic neuritis.
results: >-
Positive MOG-IgG or AQP4-IgG redirects the diagnosis to an antibody-defined
demyelinating disease subgroup.
diagnosis_term:
preferred_term: diagnostic procedure
term:
id: MAXO:0000003
label: diagnostic procedure
evidence:
- reference: PMID:41688447
reference_title: An update on the developments and challenges with the diagnosis and classification of autoimmune optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "high-quality antibody assays"
explanation: >-
The 2026 review emphasizes high-quality antibody assays in standardized
diagnostic pathways.
differential_diagnoses:
- name: Nonarteritic anterior ischemic optic neuropathy
description: >-
Ischemic optic neuropathy is a common optic neuritis mimic in referred
patients and should be considered when age, vascular risk factors, disc
appearance, pain pattern, and imaging are atypical for inflammatory optic
neuritis.
distinguishing_features:
- Often painless sudden vision loss rather than subacute painful inflammatory visual loss.
- Optic disc findings and vascular risk profile may favor ischemic neuropathy.
evidence:
- reference: PMID:29222573
reference_title: Incidence and Causes of Overdiagnosis of Optic Neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
other optic neuropathies, particularly nonarteritic anterior ischemic
optic neuropathy
explanation: >-
The overdiagnosis study identifies nonarteritic anterior ischemic optic
neuropathy as a frequent alternative diagnosis.
- name: Headache, ocular pain, and functional visual loss mimics
description: >-
Headache syndromes, eye pain without optic nerve inflammation, and
functional visual loss can be misclassified as optic neuritis when isolated
history items are overweighted.
distinguishing_features:
- Normal objective afferent visual pathway findings argue against optic neuritis.
- A single symptom such as eye pain should not substitute for optic nerve evidence.
evidence:
- reference: PMID:29222573
reference_title: Incidence and Causes of Overdiagnosis of Optic Neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
headache and eye pain, functional visual loss
explanation: >-
These were among the most common alternative diagnoses in patients
referred with suspected acute optic neuritis.
- name: Infectious and systemic inflammatory optic neuropathies
description: >-
Infectious optic neuropathies and systemic inflammatory diseases such as
sarcoidosis, SLE, Behcet disease, and vasculitis can produce optic neuritis
or optic neuropathy and require targeted evaluation when clinical context or
imaging is atypical for MS, MOGAD, NMOSD, or isolated optic neuritis.
distinguishing_features:
- Systemic symptoms, uveitis, granulomatous disease, vascular inflammation, or infectious exposure can redirect evaluation.
- Etiology-specific treatment may be required beyond acute corticosteroids.
evidence:
- reference: PMID:41688447
reference_title: An update on the developments and challenges with the diagnosis and classification of autoimmune optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "and other etiologies"
explanation: >-
The 2026 review frames autoimmune optic neuritis as a spectrum that
includes other etiologies beyond MS, NMOSD, and MOGAD.
progression:
- phase: Acute attack
subtype: Isolated optic neuritis
notes: >-
Visual loss typically evolves subacutely over days to two weeks and is often
accompanied by periocular pain, eye movement pain, dyschromatopsia, and
reduced contrast sensitivity.
duration_days: "1-14"
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: >-
progressing over several days to two weeks
explanation: >-
Orphanet provides the typical isolated optic neuritis time course.
- phase: Recurrence risk after first optic neuritis episode
notes: >-
Recurrence risk continues over long-term follow-up, especially in patients
with early relapse or AQP4-IgG positivity.
evidence:
- reference: PMID:30612145
reference_title: Incidence and timing of recurrence of optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
recurrence in either eye was 26% at 1 year
explanation: >-
The adult follow-up cohort quantified recurrence after first optic
neuritis and supports long-term monitoring.
- phase: Multiple sclerosis risk stratification after undifferentiated optic neuritis
notes: >-
At first presentation with undifferentiated optic neuritis, demographic
variables plus an MS genetic risk score can improve prediction of later
multiple sclerosis diagnosis.
evidence:
- reference: PMID:38418465
reference_title: Applying a genetic risk score model to enhance prediction of future multiple sclerosis diagnosis at first presentation with optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
one standard deviation of MS-GRS increased the Hazard of MS 1.3-fold
explanation: >-
This UK Biobank, Geisinger, and FinnGen analysis supports genetic-risk
stratification as an emerging prognostic tool after first optic neuritis.
- phase: Pediatric presentation
notes: >-
Children, especially those younger than 10 years, more often have bilateral
optic neuritis; pediatric workup must consider ADEM, MOGAD, NMOSD, MS,
infection, and post-infectious or post-vaccination contexts.
evidence:
- reference: PMID:27572862
reference_title: Pediatric optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
younger children (<10 years of age) are more likely to present with
bilateral ON
explanation: >-
The pediatric review supports age-dependent differences in bilateral
presentation.
- reference: PMID:28941527
reference_title: Pediatric Optic Neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
higher rate of bilaterality, poor visual acuity on presentation, and
papillitis
explanation: >-
This pediatric review summarizes major clinical differences from adult
optic neuritis.
treatments:
- name: Acute high-dose corticosteroids
description: >-
High-dose corticosteroids, usually intravenous methylprednisolone or a
bioequivalent high-dose oral regimen, accelerate recovery in acute optic
neuritis. Low-dose oral prednisone alone, as used in the original ONTT, is
not equivalent and increased new optic neuritis episodes.
treatment_term:
preferred_term: systemic corticosteroid therapy
term:
id: NCIT:C122080
label: Systemic Corticosteroid Therapy
therapeutic_agent:
- preferred_term: corticosteroid
term:
id: CHEBI:50858
label: corticosteroid
target_mechanisms:
- target: Immune-mediated optic nerve inflammation
treatment_effect: INHIBITS
description: >-
High-dose corticosteroids suppress acute inflammatory optic nerve injury
and speed visual recovery.
evidence:
- reference: PMID:1734247
reference_title: "A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Visual function recovered faster in the group receiving intravenous
methylprednisolone
explanation: >-
ONTT supports high-dose intravenous methylprednisolone for faster visual
recovery in acute optic neuritis.
- reference: PMID:29507942
reference_title: "Effect of Treating Acute Optic Neuritis With Bioequivalent Oral vs Intravenous Corticosteroids: A Randomized Clinical Trial."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
bioequivalent doses of oral corticosteroids may be used as an alternative
to IV corticosteroids
explanation: >-
This randomized trial supports bioequivalent high-dose oral
corticosteroids as an alternative route to high-dose IV therapy.
- reference: PMID:1734247
reference_title: "A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group."
supports: REFUTE
evidence_source: HUMAN_CLINICAL
snippet: >-
Oral prednisone alone, as prescribed in this study, is an ineffective
treatment
explanation: >-
The ONTT finding distinguishes high-dose steroid treatment from low-dose
oral prednisone monotherapy.
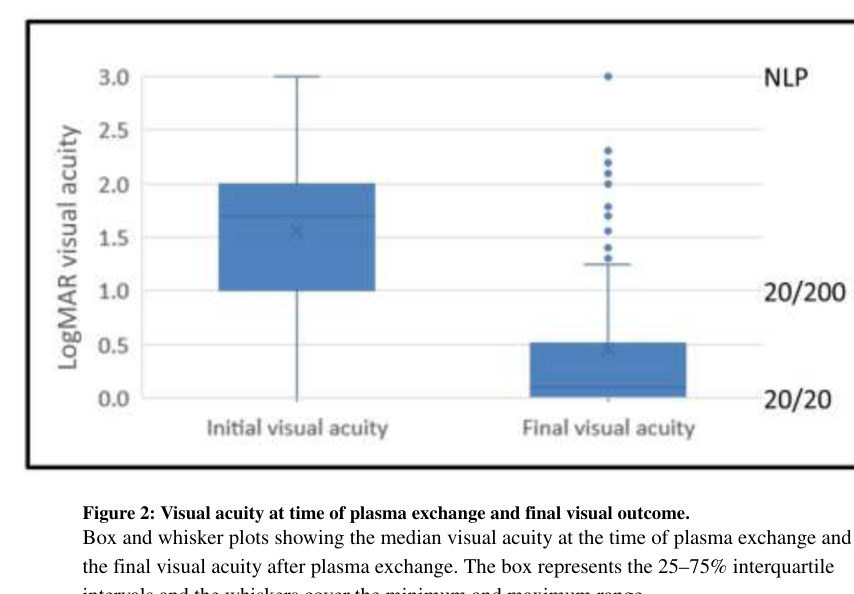
- name: Plasma exchange escalation for severe or steroid-refractory optic neuritis
description: >-
Therapeutic plasma exchange is considered for severe or steroid-refractory
optic neuritis, especially in NMOSD/AQP4-associated attacks. Evidence is
strongest in observational NMO/NMOSD relapse cohorts, while aggregate data
specific to acute NMO/NMOSD optic neuritis remain limited.
treatment_term:
preferred_term: plasmapheresis
term:
id: NCIT:C15304
label: Plasmapheresis
target_mechanisms:
- target: AQP4-IgG/NMOSD-associated optic neuritis
treatment_effect: INHIBITS
description: >-
Plasma exchange removes circulating pathogenic antibodies and complement
mediators during severe antibody-associated attacks.
evidence:
- reference: PMID:25921047
reference_title: "Treatment of acute relapses in neuromyelitis optica: Steroids alone versus steroids plus plasma exchange."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
PLEX+IVMP are more likely to improve EDSS after NMO relapses
explanation: >-
This NMO/NMOSD relapse cohort supports adding plasma exchange to
high-dose steroids, including relapses involving the optic nerves.
- reference: PMID:36822570
reference_title: "Visual Outcomes Following Plasma Exchange for Optic Neuritis: An International Multicenter Retrospective Analysis of 395 Optic Neuritis Attacks."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Most ON attacks improved with PLEX"
explanation: >-
The 395-attack international cohort supports PLEX as a clinically useful
escalation therapy for severe optic neuritis and identifies delayed PLEX
as a poor-outcome predictor.
- reference: PMID:15452303
reference_title: "Plasma exchange for severe optic neuritis: treatment of 10 patients."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
PE may be beneficial as an escalating treatment
explanation: >-
This severe optic neuritis case series supports plasma exchange as an
escalation option when high-dose steroids are insufficient.
- reference: PMID:37387119
reference_title: "Plasma exchange for acute optic neuritis in neuromyelitis optica or neuromyelitis optica spectrum disorder: a systematic review."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: >-
inadequate data to determine whether PLEX effectively treats acute ON
explanation: >-
The systematic review supports clinical plausibility but cautions that
definitive evidence for acute NMO/NMOSD optic neuritis remains limited.
- name: Maintenance intravenous immunoglobulin for relapsing MOGAD-associated optic neuritis
description: >-
Maintenance IVIG is used as a relapse-prevention option in relapsing MOGAD,
including patients whose MOGAD phenotype includes optic neuritis. Evidence is
retrospective and subtype-specific rather than a general treatment for all
optic neuritis.
treatment_term:
preferred_term: intravenous immunoglobulin therapy
term:
id: MAXO:0001480
label: immunoglobulin infusion therapy
target_mechanisms:
- target: MOG-IgG-mediated demyelinating optic neuritis
treatment_effect: INHIBITS
description: >-
IVIG is used to reduce relapsing MOG-IgG-associated inflammatory
demyelinating attacks.
evidence:
- reference: PMID:35377395
reference_title: Association of Maintenance Intravenous Immunoglobulin With Prevention of Relapse in Adult Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
maintenance IVIG was associated with a reduction in disease relapse
explanation: >-
This international adult MOGAD cohort supports maintenance IVIG as a
relapse-prevention strategy relevant to relapsing MOG-associated optic
neuritis.
- name: Eculizumab relapse prevention for AQP4-IgG/NMOSD-associated optic neuritis
description: >-
Complement C5 blockade with eculizumab reduces relapse risk in
AQP4-IgG-positive NMOSD; this is relevant to optic neuritis when optic nerve
attacks occur as part of AQP4-IgG/NMOSD-associated disease.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: eculizumab
term:
id: NCIT:C48386
label: Eculizumab
target_mechanisms:
- target: AQP4-IgG astrocytopathic optic neuritis
treatment_effect: INHIBITS
description: >-
C5 blockade reduces terminal complement-mediated astrocyte injury in
AQP4-IgG-positive NMOSD.
evidence:
- reference: PMID:31050279
reference_title: Eculizumab in Aquaporin-4-Positive Neuromyelitis Optica Spectrum Disorder.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Adjudicated relapses occurred in 3 of 96 patients (3%) in the eculizumab
group and 20 of 47 (43%) in the placebo group
explanation: >-
The PREVENT trial supports eculizumab for relapse prevention in
AQP4-IgG-positive NMOSD, including prevention of recurrent optic neuritis
attacks in that subtype context.
clinical_trials:
- name: NCT00000146
phase: PHASE_III
status: UNKNOWN
description: >-
Historic Optic Neuritis Treatment Trial evaluating corticosteroid treatment,
natural history, and MS risk after optic neuritis.
evidence:
- reference: clinicaltrials:NCT00000146
reference_title: Optic Neuritis Treatment Trial (ONTT)
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
To assess the beneficial and adverse effects of corticosteroid treatment
for optic neuritis.
explanation: >-
The ClinicalTrials.gov record documents the ONTT corticosteroid treatment
and natural-history objectives.
- reference: PMID:1734247
reference_title: "A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
randomly assigned 457 patients with acute optic neuritis
explanation: >-
The NEJM publication reports the pivotal ONTT corticosteroid trial.
- name: NCT01524250
phase: PHASE_III
status: COMPLETED
description: >-
Randomized single-blind trial comparing bioequivalent high-dose oral versus
intravenous corticosteroids for acute demyelinating optic neuritis.
evidence:
- reference: clinicaltrials:NCT01524250
reference_title: "Recovery of Demyelinating Optic Neuritis After Treatment With Equivalent High Doses of Oral vs. Intravenous Corticosteroids: a Randomized Single Blinded Clinical Trial"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
randomized to receive equivalent doses of either intravenous (IV) or oral
corticosteroid treatment
explanation: >-
The trial record documents the randomized oral-versus-IV corticosteroid
comparison.
- reference: PMID:29507942
reference_title: "Effect of Treating Acute Optic Neuritis With Bioequivalent Oral vs Intravenous Corticosteroids: A Randomized Clinical Trial."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
no significant difference between groups
explanation: >-
The published trial found no significant recovery difference between
bioequivalent oral and IV high-dose corticosteroids.
- name: NCT01721161
phase: PHASE_II
status: COMPLETED
description: >-
RENEW randomized placebo-controlled phase 2 trial of BIIB033/opicinumab
after first unilateral acute optic neuritis, evaluating remyelination by
visual evoked potential latency recovery.
evidence:
- reference: clinicaltrials:NCT01721161
reference_title: "A Randomized, Double-Blind, Parallel-Group, Placebo Controlled Study to Assess the Efficacy, Safety, Tolerability, and Pharmacokinetics of BIIB033 in Subjects With First Episode of Acute Optic Neuritis"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
evaluate the efficacy of BIIB033 in subjects with their first episode of
unilateral acute optic neuritis
explanation: >-
The trial record documents the RENEW acute optic neuritis study.
- reference: PMID:28229892
reference_title: "Safety and efficacy of opicinumab in acute optic neuritis (RENEW): a randomised, placebo-controlled, phase 2 trial."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: >-
Remyelination did not differ significantly between the opicinumab and
placebo groups
explanation: >-
RENEW was mechanistically important but did not meet the primary
intention-to-treat remyelination endpoint.
- name: NCT02657915
phase: PHASE_II
status: COMPLETED
description: >-
RENEWED follow-up study assessing long-term electrophysiologic and clinical
outcomes in participants from the RENEW opicinumab acute optic neuritis
trial.
evidence:
- reference: clinicaltrials:NCT02657915
reference_title: "A Multicenter, Follow-Up Study to Assess Long-Term Electrophysiologic and Clinical Outcomes in Subjects Previously Enrolled in Study 215ON201"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
assess full-field visual evoked potential (FF-VEP) latency
explanation: >-
The trial record documents the long-term VEP follow-up endpoint.
- reference: PMID:39662163
reference_title: "RENEWED: A follow-up study of the opicinumab phase 2 RENEW study in participants with acute optic neuritis."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: >-
VEP latency and clinical data in RENEWED should be interpreted with
caution
explanation: >-
The follow-up study provides longer-term data but emphasizes limitations
from study design and sample size.
- name: NCT03586557
phase: NOT_APPLICABLE
status: UNKNOWN
description: >-
Randomized study of high-dose intravenous corticosteroids with or without
plasma exchange for severe acute AQP4-IgG-positive optic neuritis.
evidence:
- reference: clinicaltrials:NCT03586557
reference_title: Effectiveness of Plasma Exchange in Treating With Severe Acute AQP4-Ab Positive Optic Neuritis
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
acute aquaporin-4 immunoglobulin G antibodies (AQP4-IgG) positive optic
neuritis
explanation: >-
The trial record documents a randomized study focused on plasma exchange
in severe acute AQP4-IgG-positive optic neuritis.
- name: NCT04762017
phase: PHASE_II
status: COMPLETED
description: >-
ACUITY phase 2 randomized double-blind placebo-controlled study of OCS-05
added to standard-of-care corticosteroids for acute optic neuritis.
evidence:
- reference: clinicaltrials:NCT04762017
reference_title: "A Randomized, Double-blind, Placebo-controlled Study to Evaluate the Safety and Tolerability of OCS-05 in Patients With Acute Optic Neuritis"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
safety and tolerability of OCS-05 compared to placebo
explanation: >-
The ClinicalTrials.gov record documents the acute optic neuritis OCS-05
phase 2 safety/tolerability trial.
datasets: []
references:
- reference: ORPHA:499096
title: Isolated optic neuritis
findings:
- statement: Orphanet defines isolated optic neuritis and provides phenotype annotations.
supporting_text: A rare inflammatory optic neuropathy
evidence:
- reference: ORPHA:499096
reference_title: Isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "A rare inflammatory optic neuropathy"
explanation: >-
Supports the isolated optic neuritis subtype and its phenotype
annotations.
- reference: ORPHA:659626
title: Single isolated optic neuritis
findings:
- statement: Orphanet maps single isolated optic neuritis to MONDO:0971049.
supporting_text: "MONDO:0971049 | Exact"
evidence:
- reference: ORPHA:659626
reference_title: Single isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "MONDO:0971049 | Exact"
explanation: >-
Supports the single isolated optic neuritis subtype term.
- reference: ORPHA:659634
title: Relapsing isolated optic neuritis
findings:
- statement: Orphanet maps relapsing isolated optic neuritis to MONDO:0971050.
supporting_text: "MONDO:0971050 | Exact"
evidence:
- reference: ORPHA:659634
reference_title: Relapsing isolated optic neuritis
supports: SUPPORT
evidence_source: OTHER
snippet: "MONDO:0971050 | Exact"
explanation: >-
Supports the relapsing isolated optic neuritis subtype term.
- reference: PMID:41688447
title: An update on the developments and challenges with the diagnosis and classification of autoimmune optic neuritis.
findings:
- statement: Autoimmune optic neuritis is heterogeneous and needs standardized first-attack attribution.
supporting_text: >-
Early and accurate attribution at the first attack is clinically decisive
evidence:
- reference: PMID:41688447
reference_title: An update on the developments and challenges with the diagnosis and classification of autoimmune optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Early and accurate attribution at the first attack is clinically
decisive
explanation: >-
Supports the diagnostic framing and the need for multimodal workup.
- reference: PMID:36179757
title: Diagnosis and classification of optic neuritis.
findings:
- statement: International consensus criteria classify optic neuritis subgroups using clinical and paraclinical data.
supporting_text: >-
diagnostic criteria for optic neuritis and a classification of optic
neuritis subgroups
evidence:
- reference: PMID:36179757
reference_title: Diagnosis and classification of optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
diagnostic criteria for optic neuritis and a classification of optic
neuritis subgroups
explanation: >-
Supports use of the Petzold et al. framework for subgroup curation.
- reference: PMID:29222573
title: Incidence and Causes of Overdiagnosis of Optic Neuritis.
findings:
- statement: Overdiagnosis is common in referral cohorts, especially due to mimics.
supporting_text: >-
nearly 60% ... of patients referred for optic neuritis have an alternative
diagnosis
evidence:
- reference: PMID:29222573
reference_title: Incidence and Causes of Overdiagnosis of Optic Neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
patients referred for optic neuritis have an alternative diagnosis
explanation: >-
Supports the differential-diagnosis section and diagnostic caution.
- reference: PMID:1734247
title: "A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group."
findings:
- statement: High-dose IV methylprednisolone accelerates visual recovery, while low-dose oral prednisone alone is not effective.
supporting_text: Visual function recovered faster
evidence:
- reference: PMID:1734247
reference_title: "A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Visual function recovered faster"
explanation: >-
Supports acute high-dose corticosteroid therapy.
- reference: PMID:29507942
title: "Effect of Treating Acute Optic Neuritis With Bioequivalent Oral vs Intravenous Corticosteroids: A Randomized Clinical Trial."
findings:
- statement: Bioequivalent high-dose oral corticosteroids can be an alternative to IV corticosteroids.
supporting_text: >-
bioequivalent doses of oral corticosteroids may be used as an alternative
evidence:
- reference: PMID:29507942
reference_title: "Effect of Treating Acute Optic Neuritis With Bioequivalent Oral vs Intravenous Corticosteroids: A Randomized Clinical Trial."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
bioequivalent doses of oral corticosteroids may be used as an
alternative
explanation: >-
Supports high-dose oral corticosteroid equivalence to IV dosing.
- reference: PMID:37387119
title: "Plasma exchange for acute optic neuritis in neuromyelitis optica or neuromyelitis optica spectrum disorder: a systematic review."
findings:
- statement: Evidence for plasma exchange in acute NMO/NMOSD optic neuritis remains limited.
supporting_text: inadequate data to determine whether PLEX effectively treats acute ON
evidence:
- reference: PMID:37387119
reference_title: "Plasma exchange for acute optic neuritis in neuromyelitis optica or neuromyelitis optica spectrum disorder: a systematic review."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: >-
inadequate data to determine whether PLEX effectively treats acute ON
explanation: >-
Captures the treatment-evidence limitation for plasma exchange.
- reference: PMID:39963868
title: "Incidence of optic neuritis among Afro-descendant, a cohort study."
findings:
- statement: A 2018-2022 Martinique cohort estimated optic neuritis incidence and etiologic distribution.
supporting_text: The overall incidence was 1.61
evidence:
- reference: PMID:39963868
reference_title: "Incidence of optic neuritis among Afro-descendant, a cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The overall incidence was 1.61"
explanation: >-
Supports epidemiology and subtype distribution.
- reference: PMID:38783085
title: MOG antibody-associated optic neuritis.
findings:
- statement: MOGAD most frequently presents with optic neuritis and has characteristic clinical and radiologic features.
supporting_text: MOGAD most frequently presents with optic neuritis
evidence:
- reference: PMID:38783085
reference_title: MOG antibody-associated optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "MOGAD most frequently presents with optic neuritis"
explanation: >-
Supports MOG-IgG-associated optic neuritis as a major antibody-defined
subtype.
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: PMID:35377395
title: Association of Maintenance Intravenous Immunoglobulin With Prevention of Relapse in Adult Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease.
findings:
- statement: Maintenance IVIG was associated with reduced relapse activity in adult MOGAD.
supporting_text: >-
maintenance IVIG was associated with a reduction in disease relapse
evidence:
- reference: PMID:35377395
reference_title: Association of Maintenance Intravenous Immunoglobulin With Prevention of Relapse in Adult Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
maintenance IVIG was associated with a reduction in disease relapse
explanation: >-
Supports maintenance IVIG as relapse prevention for relapsing
MOG-IgG-associated disease, including MOG-associated optic neuritis.
- reference: PMID:36810323
title: Diagnostic value of intereye difference metrics for optic neuritis in aquaporin-4 antibody seropositive neuromyelitis optica spectrum disorders
findings:
- statement: OCT intereye-difference metrics are validated diagnostic parameters in AQP4-positive NMOSD optic neuritis.
supporting_text: Results support the validation of the IED metrics
evidence:
- reference: PMID:36810323
reference_title: Diagnostic value of intereye difference metrics for optic neuritis in aquaporin-4 antibody seropositive neuromyelitis optica spectrum disorders
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Results support the validation of the IED metrics
explanation: >-
Supports OCT intereye-difference metrics as diagnostic support in
AQP4-positive NMOSD-associated optic neuritis.
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: PMID:39231384
title: Diagnostic Value of Inter-Eye Difference Metrics on OCT for Myelin Oligodendrocyte Glycoprotein Antibody-Associated Optic Neuritis.
findings:
- statement: OCT intereye-difference metrics have high diagnostic accuracy for MOG-IgG-associated optic neuritis.
supporting_text: diagnostic accuracy of OCT-based IED metrics for ON was high
evidence:
- reference: PMID:39231384
reference_title: Diagnostic Value of Inter-Eye Difference Metrics on OCT for Myelin Oligodendrocyte Glycoprotein Antibody-Associated Optic Neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
diagnostic accuracy of OCT-based IED metrics for ON was high
explanation: >-
Supports OCT intereye-difference metrics as diagnostic support in
MOG-IgG-associated optic neuritis.
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: PMID:38418465
title: Applying a genetic risk score model to enhance prediction of future multiple sclerosis diagnosis at first presentation with optic neuritis.
findings:
- statement: MS genetic risk score plus demographics improves MS prediction after undifferentiated optic neuritis.
supporting_text: one standard deviation of MS-GRS increased the Hazard of MS 1.3-fold
evidence:
- reference: PMID:38418465
reference_title: Applying a genetic risk score model to enhance prediction of future multiple sclerosis diagnosis at first presentation with optic neuritis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
one standard deviation of MS-GRS increased the Hazard of MS 1.3-fold
explanation: >-
Supports genetic-risk-score stratification as an emerging prognostic
approach after first optic neuritis.
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: PMID:36822570
title: "Visual Outcomes Following Plasma Exchange for Optic Neuritis: An International Multicenter Retrospective Analysis of 395 Optic Neuritis Attacks."
findings:
- statement: A large international cohort found most severe optic neuritis attacks improved with PLEX.
supporting_text: Most ON attacks improved with PLEX
evidence:
- reference: PMID:36822570
reference_title: "Visual Outcomes Following Plasma Exchange for Optic Neuritis: An International Multicenter Retrospective Analysis of 395 Optic Neuritis Attacks."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Most ON attacks improved with PLEX"
explanation: >-
Supports plasma exchange as escalation therapy in severe optic neuritis
while preserving timing and severity as prognostic factors.
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: PMID:31050279
title: Eculizumab in Aquaporin-4-Positive Neuromyelitis Optica Spectrum Disorder.
findings:
- statement: Eculizumab substantially reduced relapse risk in AQP4-IgG-positive NMOSD.
supporting_text: >-
Adjudicated relapses occurred in 3 of 96 patients (3%) in the eculizumab
group and 20 of 47 (43%) in the placebo group
evidence:
- reference: PMID:31050279
reference_title: Eculizumab in Aquaporin-4-Positive Neuromyelitis Optica Spectrum Disorder.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Adjudicated relapses occurred in 3 of 96 patients (3%) in the eculizumab
group and 20 of 47 (43%) in the placebo group
explanation: >-
Supports complement C5 blockade as relapse prevention for
AQP4-IgG-positive NMOSD, including the NMOSD-associated optic neuritis
subtype context.
- reference: DOI:10.1016/j.ajo.2023.02.013
title: "Visual Outcomes Following Plasma Exchange for Optic Neuritis: An International Multicenter Retrospective Analysis of 395 Optic Neuritis Attacks"
findings: []
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: DOI:10.1038/s41433-024-03108-y
title: MOG antibody-associated optic neuritis
findings: []
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: DOI:10.1038/s41467-024-44917-9
title: Applying a genetic risk score model to enhance prediction of future multiple sclerosis diagnosis at first presentation with optic neuritis
findings: []
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: DOI:10.1136/jnnp-2022-330608
title: Diagnostic value of intereye difference metrics for optic neuritis in aquaporin-4 antibody seropositive neuromyelitis optica spectrum disorders
findings: []
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: DOI:10.1177/13524585231224683
title: Prevalence of neuromyelitis optica spectrum disorder in the United States
findings: []
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: DOI:10.1212/nxi.0000000000200214
title: Acute Optic Neuropathy in Older Adults
findings: []
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: DOI:10.1212/nxi.0000000000200291
title: Diagnostic Value of Inter-Eye Difference Metrics on OCT for Myelin Oligodendrocyte Glycoprotein Antibody-Associated Optic Neuritis
findings: []
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: DOI:10.3390/ijms242115986
title: "Beyond Myelin Oligodendrocyte Glycoprotein and Aquaporin-4 Antibodies: Alternative Causes of Optic Neuritis"
findings: []
found_in:
- Optic_Neuritis-deep-research-falcon.md
- reference: DOI:10.7759/cureus.56094
title: "A Comparative Review of Typical and Atypical Optic Neuritis: Advancements in Treatments, Diagnostics, and Prognosis"
findings: []
found_in:
- Optic_Neuritis-deep-research-falcon.md
References & Deep Research
References
26Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Deep Research
1Question: You are an expert researcher providing comprehensive, well-cited information.
Provide detailed information focusing on: 1. Key concepts and definitions with current understanding 2. Recent developments and latest research (prioritize 2023-2024 sources) 3. Current applications and real-world implementations 4. Expert opinions and analysis from authoritative sources 5. Relevant statistics and data from recent studies
Format as a comprehensive research report with proper citations. Include URLs and publication dates where available. Always prioritize recent, authoritative sources and provide specific citations for all major claims.
Disease Characteristics Research Template
Target Disease
- Disease Name: Optic Neuritis
- MONDO ID: (if available)
- Category: Neurological Disorder
Research Objectives
Please provide a comprehensive research report on Optic Neuritis covering all of the disease characteristics listed below. This report will be used to populate a disease knowledge base entry. Be thorough and cite primary literature (PMID preferred) for all claims.
For each section, suggested databases/resources are listed. These are the first places you should search for information on each topic.
1. Disease Information
Search first: OMIM, Orphanet, ICD-10/ICD-11, MeSH, PubMed
- What is the disease? Provide a concise overview.
- What are the key identifiers? (OMIM, Orphanet, ICD-10/ICD-11, MeSH, Mondo)
- What are the common synonyms and alternative names?
- Is the information derived from individual patients (e.g., EHR) or aggregated disease-level resources?
2. Etiology
- Disease Causal Factors: What are the primary causes? (genetic, environmental, infectious, mechanistic)
- Risk Factors:
Search first: PubMed, Cochrane Library, UpToDate, clinical guidelines, ClinVar, ClinGen, GWAS Catalog, PheGenI, CTD, CDC, WHO, epidemiological databases
- Genetic risk factors (causal variants, susceptibility loci, modifier genes)
- Environmental risk factors (toxins, lifestyle, occupational exposures, age, sex, family history)
- Protective Factors:
Search first: PubMed, Cochrane Library, clinical trial databases, GWAS Catalog, gnomAD, WHO, CDC, nutrition databases
- Genetic protective factors (protective variants, modifier alleles)
- Environmental protective factors (diet, lifestyle, exposures that reduce risk)
- Gene-Environment Interactions: How do genetic and environmental factors interact to influence disease?
Search first: CTD, PubMed, PheGenI, GxE databases
3. Phenotypes
Search first: HPO (Human Phenotype Ontology), OMIM, Orphanet, PubMed, clinicaltrials.gov, MedDRA, SNOMED CT, DECIPHER, LOINC
For each phenotype, provide: - Phenotype type: symptoms, clinical signs, physical manifestations, behavioral changes, or laboratory abnormalities
For symptoms/signs: HPO, OMIM, Orphanet, PubMed For behavioral changes: HPO, DSM, RDoC (Research Domain Criteria), PubMed For laboratory abnormalities: LOINC, SNOMED CT, LabTests Online, PubMed - Phenotype characteristics: Search first: OMIM, Orphanet, HPO, PubMed - Age of symptom onset (neonatal, childhood, adult-onset, late-onset) - Symptom severity (mild, moderate, severe, variable) - Symptom progression (stable, progressive, episodic, fluctuating) - Frequency among affected individuals (percentage or qualitative) - Quality of life impact: Effects on daily functioning and well-being (per-phenotype when possible) Search first: EQ-5D database, SF-36, WHO QOL databases, PubMed - Suggest HPO (Human Phenotype Ontology) terms for each phenotype
4. Genetic/Molecular Information
- Causal Genes: Gene mutations or chromosomal abnormalities responsible for disease (gene symbols, OMIM IDs)
Search first: OMIM, ClinVar, HGMD, Ensembl, NCBI Gene
- Pathogenic Variants:
- Affected genes (gene symbols, HGNC IDs) > Search first: OMIM, NCBI Gene, Ensembl, HGNC, UniProt, GeneCards
- Variant classification (pathogenic, likely pathogenic, VUS per ACMG/AMP guidelines) > Search first: ClinVar, ClinGen, ACMG/AMP guidelines, VarSome
- Variant type/class (missense, frameshift, nonsense, splice-site, structural)
- Allele frequency in population databases > Search first: gnomAD, 1000 Genomes, ExAC, TOPMed, dbSNP
- Somatic vs germline origin > Search first: COSMIC (somatic), ClinVar, ICGC, TCGA
- Functional consequences (loss of function, gain of function, dominant negative)
- Modifier Genes: Genes that modify disease severity or expression
- Epigenetic Information: DNA methylation, histone modifications, chromatin changes affecting disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Chromosomal Abnormalities: Large-scale genetic changes (aneuploidy, translocations, inversions)
Search first: DECIPHER, ClinVar, ECARUCA, UCSC Genome Browser
5. Environmental Information
- Environmental Factors: Non-genetic contributing factors (toxins, radiation, pollution, occupational exposure)
Search first: CTD (Comparative Toxicogenomics Database), TOXNET, PubMed, EPA databases
- Lifestyle Factors: Behavioral factors (smoking, diet, exercise, alcohol consumption)
Search first: CDC databases, WHO, PubMed, NHANES
- Infectious Agents: If applicable, pathogens causing or triggering disease (bacteria, viruses, fungi, parasites)
Search first: NCBI Taxonomy, ViPR, BV-BRC, MicrobeDB, GIDEON
6. Mechanism / Pathophysiology
- Molecular Pathways: Specific signaling cascades or biochemical pathways involved (Wnt, MAPK, mTOR, PI3K-AKT, etc.)
Search first: KEGG, Reactome, WikiPathways, PathBank, BioCyc
- Cellular Processes: Cell-level mechanisms (apoptosis, autophagy, cell cycle dysregulation, inflammation, etc.)
Search first: Gene Ontology (GO), Reactome, KEGG, PubMed
- Protein Dysfunction: How protein structure or function is altered (misfolding, aggregation, loss of function, gain of function)
Search first: UniProt, PDB (Protein Data Bank), InterPro, Pfam, AlphaFold
- Metabolic Changes: Alterations in metabolic processes (energy metabolism, lipid metabolism, amino acid metabolism)
Search first: KEGG, BioCyc, HMDB (Human Metabolome Database), BRENDA
- Immune System Involvement: Role of immune response (autoimmunity, immunodeficiency, chronic inflammation)
Search first: ImmPort, Immunome Database, IEDB, Gene Ontology
- Tissue Damage Mechanisms: How tissues/ are injured (oxidative stress, ischemia, fibrosis, necrosis)
Search first: PubMed, Gene Ontology, Reactome
- Biochemical Abnormalities: Specific molecular defects (enzyme deficiencies, receptor dysfunction, ion channel defects)
Search first: BRENDA, UniProt, KEGG, OMIM, PubMed
- Epigenetic Changes: DNA methylation, histone modifications affecting gene expression in disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Molecular Profiling (if available):
- Transcriptomics/gene expression changes > Search first: GEO (Gene Expression Omnibus), ArrayExpress, GTEx, Human Cell Atlas, SRA
- Proteomics findings > Search first: PRIDE, ProteomeXchange, Human Protein Atlas, STRING, BioGRID
- Metabolomics signatures > Search first: MetaboLights, Metabolomics Workbench, HMDB, METLIN
- Lipidomics alterations > Search first: LIPID MAPS, SwissLipids, LipidHome, Metabolomics Workbench
- Genomic structural features > Search first: UCSC Genome Browser, Ensembl, NCBI, dbVar, DGV
- Advanced Technologies (if applicable):
- Single-cell analysis findings (cell-type specific mechanisms, cellular heterogeneity) > Search first: Human Cell Atlas, Single Cell Portal, GEO, CELLxGENE
- Spatial transcriptomics findings > Search first: GEO, Spatial Research, Vizgen, 10x Genomics data
- Multi-omics integration results > Search first: TCGA, ICGC, cBioPortal, LinkedOmics, PubMed
- Functional genomics screens (CRISPR, RNAi) > Search first: DepMap, GenomeRNAi, PubMed, BioGRID ORCS
For each mechanism, describe: - The causal chain from initial trigger to clinical manifestation - Which mechanisms are upstream vs downstream - What cell types and biological processes are involved - Suggest GO terms for biological processes and CL terms for cell types
7. Anatomical Structures Affected
- Organ Level:
- Primary organs directly affected
- Secondary organ involvement (complications, secondary effects)
- Body systems involved (cardiovascular, nervous, digestive, respiratory, endocrine, etc.)
Search first: Uberon, FMA (Foundational Model of Anatomy), OMIM, HPO, ICD-11, MeSH, SNOMED CT
- Tissue and Cell Level:
- Specific tissue types affected (epithelial, connective, muscle, nervous)
- Specific cell populations targeted (with Cell Ontology terms)
Search first: Uberon, Human Protein Atlas, Cell Ontology, Human Cell Atlas, CellMarker, PanglaoDB
- Subcellular Level:
- Cellular compartments involved (mitochondria, nucleus, ER, lysosomes) (with GO Cellular Component terms)
Search first: Gene Ontology (Cellular Component), UniProt, Human Protein Atlas
- Localization:
- Specific anatomical sites (with UBERON terms) > Search first: FMA, Uberon, NeuroNames (for brain), SNOMED CT
- Lateralization (unilateral, bilateral, asymmetric) > Search first: HPO, clinical literature, imaging databases
8. Temporal Development
- Onset:
- Typical age of onset (congenital, pediatric, adult, geriatric)
- Onset pattern (acute, subacute, chronic, insidious)
Search first: OMIM, Orphanet, HPO, PubMed
- Progression:
- Disease stages (early, intermediate, advanced, end-stage) > Search first: Cancer Staging Manual (AJCC), WHO classifications, PubMed
- Progression rate (rapid, slow, variable)
- Disease course pattern (episodic, relapsing-remitting, progressive, stable)
- Disease duration (self-limited, chronic lifelong)
Search first: Disease registries, longitudinal cohort databases, natural history studies, PubMed, Orphanet, OMIM
- Patterns:
- Remission patterns (spontaneous, treatment-induced) > Search first: Clinical trial databases, disease registries, PubMed
- Critical periods (time windows of vulnerability or opportunity for intervention) > Search first: PubMed, developmental biology databases, clinical guidelines
9. Inheritance and Population
- Epidemiology:
- Prevalence (cases per 100,000 at given time)
- Incidence (new cases per 100,000 per year)
Search first: Orphanet, CDC, WHO, GBD (Global Burden of Disease), national registries, SEER, disease registries
- For Genetic Etiology:
- Inheritance pattern (AD, AR, X-linked, mitochondrial, multifactorial, polygenic) > Search first: OMIM, Orphanet, ClinVar, GTR (Genetic Testing Registry)
- Penetrance (complete, incomplete, age-dependent) > Search first: ClinVar, OMIM, PubMed, ClinGen
- Expressivity (variable, consistent) > Search first: OMIM, ClinVar, PubMed
- Genetic anticipation (increasing severity in successive generations) > Search first: OMIM, PubMed (especially for repeat expansion disorders)
- Germline mosaicism > Search first: ClinVar, OMIM, genetic counseling literature, PubMed
- Founder effects (population-specific mutations) > Search first: gnomAD, population genetics databases, PubMed
- Consanguinity role > Search first: OMIM, population studies, genetic counseling resources
- Carrier frequency > Search first: gnomAD, carrier screening databases, GeneReviews, GTR
- Population Demographics:
- Affected populations (ethnic or demographic groups with higher prevalence) > Search first: gnomAD, 1000 Genomes, PAGE Study, PubMed, population registries
- Geographic distribution (endemic areas, regional variation) > Search first: WHO, CDC, GBD, Orphanet, geographic epidemiology databases
- Geographic distribution of specific variants
- Sex ratio (male:female) > Search first: Disease registries, OMIM, PubMed, epidemiological databases
- Age distribution of affected individuals > Search first: CDC, disease registries, SEER, Orphanet
10. Diagnostics
- Clinical Tests:
- Laboratory tests (blood, urine, tissue chemistry, specific enzyme assays) > Search first: LOINC, LabTests Online, PubMed
- Biomarkers (proteins, metabolites, genetic markers, circulating biomarkers) > Search first: FDA Biomarker List, BEST (Biomarkers, EndpointS, and other Tools), PubMed
- Imaging studies (X-ray, CT, MRI, PET, ultrasound) > Search first: RadLex, DICOM, Radiopaedia, imaging databases
- Functional tests (pulmonary function, cardiac stress tests) > Search first: LOINC, clinical guidelines, PubMed
- Electrophysiology (EEG, EMG, ECG, nerve conduction studies) > Search first: LOINC, clinical neurophysiology databases, PubMed
- Biopsy findings (histopathology, immunohistochemistry) > Search first: SNOMED CT, College of American Pathologists resources, PubMed
- Pathology findings (microscopic examination) > Search first: SNOMED CT, Digital Pathology databases, PubMed
- Genetic Testing:
Search first: GTR (Genetic Testing Registry), GeneReviews, ClinGen
- Overview of recommended genetic testing approach
- Whole genome sequencing (WGS) utility > Search first: GTR, ClinVar, GEL (Genomics England), gnomAD
- Whole exome sequencing (WES) utility > Search first: GTR, ClinVar, OMIM, GeneMatcher
- Gene panels (which panels, which genes) > Search first: GTR, ClinVar, laboratory-specific databases
- Single gene testing > Search first: GTR, ClinVar, OMIM, GeneReviews
- Chromosomal microarray (CMA) > Search first: DECIPHER, ClinVar, dbVar, ECARUCA
- Karyotyping > Search first: Chromosome Abnormality Database, ClinVar, cytogenetics resources
- FISH > Search first: ClinVar, cytogenetics databases, PubMed
- Mitochondrial DNA testing > Search first: MITOMAP, MSeqDR, ClinVar, GTR
- Repeat expansion testing > Search first: GTR, ClinVar, repeat expansion databases, PubMed
- Omics-Based Diagnostics (if applicable):
- RNA sequencing / transcriptomics > Search first: GEO, ArrayExpress, GTEx, RNA-seq databases
- Proteomics > Search first: PRIDE, ProteomeXchange, FDA Biomarker database
- Metabolomics > Search first: MetaboLights, Metabolomics Workbench, HMDB
- Epigenomics > Search first: GEO, ENCODE, Roadmap Epigenomics, MethBase
- Liquid biopsy > Search first: COSMIC, ClinVar, liquid biopsy databases, PubMed
- Clinical Criteria:
- Standardized diagnostic criteria (DSM, ICD, society guidelines) > Search first: DSM-5, ICD-11, clinical society guidelines, UpToDate
- Differential diagnosis (other conditions to rule out, with distinguishing features) > Search first: DynaMed, UpToDate, clinical decision support systems
- Screening:
- Screening methods for asymptomatic individuals (newborn screening, carrier screening, cascade screening) > Search first: ACMG recommendations, CDC newborn screening, GTR
11. Outcome/Prognosis
- Survival and Mortality:
- Survival rate (5-year, 10-year, overall) > Search first: SEER, cancer registries, disease-specific registries, PubMed
- Life expectancy (with and without treatment if applicable) > Search first: Orphanet, disease registries, actuarial databases, PubMed
- Mortality rate > Search first: CDC, WHO, GBD, national mortality databases
- Disease-specific mortality (deaths directly attributable to disease) > Search first: Disease registries, CDC Wonder, GBD, PubMed
- Morbidity and Function:
- Morbidity (disease-related disability and health impacts) > Search first: GBD, WHO, disability databases, PubMed
- Disability outcomes (long-term functional impairments) > Search first: ICF (International Classification of Functioning), disability registries
- Quality of life measures (EQ-5D, SF-36, PROMIS, disease-specific tools) > Search first: EQ-5D database, SF-36, PROMIS, PubMed
- Disease Course:
- Complications (secondary problems: infections, organ failure, etc.) > Search first: ICD codes, disease registries, clinical databases, PubMed
- Recovery potential (likelihood and extent of recovery, with vs without treatment) > Search first: Natural history studies, rehabilitation databases, PubMed
- Prediction:
- Prognostic factors (age, disease severity, biomarkers, treatment response) > Search first: Prognostic models databases, clinical calculators, PubMed
- Prognostic biomarkers (molecular markers predicting disease course) > Search first: FDA Biomarker database, PubMed, cancer prognostic databases
12. Treatment
- Pharmacotherapy:
- Pharmacological treatments (drug names, drug classes, mechanisms of action) > Search first: DrugBank, RxNorm, ATC classification, DailyMed, FDA databases
- Pharmacogenomics (how genetic variants affect drug metabolism, efficacy, toxicity) > Search first: PharmGKB, CPIC (Clinical Pharmacogenetics), FDA Table of PGx Biomarkers
- Advanced Therapeutics:
- Gene therapy (viral vectors, CRISPR, gene replacement, gene editing) > Search first: ClinicalTrials.gov, FDA gene therapy database, ASGCT resources
- Cell therapy (stem cell transplant, CAR-T, cellular therapeutics) > Search first: ClinicalTrials.gov, FDA cell therapy database, FACT standards
- RNA-based therapies (ASOs, siRNA, mRNA therapies) > Search first: ClinicalTrials.gov, FDA approvals, PubMed
- Targeted therapies (treatments directed at specific molecular targets) > Search first: My Cancer Genome, OncoKB, ClinicalTrials.gov, FDA approvals
- Immunotherapies (checkpoint inhibitors, monoclonal antibodies) > Search first: Cancer Immunotherapy Database, FDA approvals, ClinicalTrials.gov
- Surgical and Interventional:
- Surgical interventions (types of surgery, timing, outcomes) > Search first: CPT codes, surgical registries, clinical guidelines, PubMed
- Supportive and Rehabilitative:
- Supportive care (symptom management, pain control, nutrition) > Search first: Clinical guidelines, Cochrane Library, PubMed
- Rehabilitation (physical therapy, occupational therapy, speech therapy) > Search first: Rehabilitation medicine databases, clinical guidelines, PubMed
- Experimental:
- Experimental treatments in clinical trials (with NCT identifiers if available) > Search first: ClinicalTrials.gov, EU Clinical Trials Register, WHO ICTRP
- Treatment Outcomes:
- Treatment response rates > Search first: Clinical trial databases, FDA reviews, systematic reviews, PubMed
- Side effects and adverse events > Search first: FDA Adverse Event Reporting System (FAERS), MedWatch, PubMed
- Treatment Strategy:
- Treatment algorithms (clinical pathways, decision trees) > Search first: Clinical practice guidelines, NCCN Guidelines, UpToDate
- Combination therapies > Search first: ClinicalTrials.gov, treatment guidelines, PubMed
- Personalized medicine approaches (genotype-guided treatment) > Search first: My Cancer Genome, CIViC, PharmGKB, precision medicine databases
For each treatment, suggest MAXO (Medical Action Ontology) terms where applicable.
13. Prevention
- Prevention Levels:
- Primary prevention (preventing disease occurrence: vaccination, risk factor modification) > Search first: CDC, WHO, USPSTF recommendations, Cochrane Library
- Secondary prevention (early detection and treatment: screening programs, early intervention) > Search first: USPSTF, CDC screening guidelines, WHO
- Tertiary prevention (preventing complications in those with disease) > Search first: Clinical guidelines, disease management protocols, PubMed
- Immunization: Vaccine strategies (if applicable)
Search first: CDC vaccine schedules, WHO immunization, FDA vaccine database
- Screening and Early Detection:
- Screening programs (population-based: newborn screening, cancer screening) > Search first: CDC screening programs, USPSTF, cancer screening databases
- Genetic screening (carrier screening, preimplantation genetic diagnosis, prenatal testing) > Search first: ACMG recommendations, ACOG guidelines, GTR
- Risk stratification (identifying high-risk individuals for targeted prevention) > Search first: Risk prediction models, clinical calculators, PubMed
- Behavioral Interventions: Lifestyle modifications to reduce risk
Search first: CDC, WHO, behavioral intervention databases, Cochrane Library
- Counseling: Genetic counseling (risk assessment, family planning guidance)
Search first: NSGC resources, ACMG guidelines, GeneReviews
- Public Health:
- Public health interventions (sanitation, vector control, health education) > Search first: CDC, WHO, public health databases, PubMed
- Environmental interventions (reducing environmental risk factors) > Search first: EPA databases, WHO environmental health, PubMed
- Prophylaxis: Preventive medications or procedures
Search first: Clinical guidelines, FDA approvals, PubMed
14. Other Species / Natural Disease
- Taxonomy: Species affected (with NCBI Taxon identifiers)
Search first: NCBI Taxonomy
- Breed: Specific breeds affected (with VBO identifiers if applicable)
Search first: VBO (Vertebrate Breed Ontology)
- Gene: Orthologous genes in other species (with NCBI Gene IDs)
Search first: NCBI Gene
- Natural Disease:
- Naturally occurring disease in other species (companion animals, wildlife) > Search first: OMIA (Online Mendelian Inheritance in Animals), VetCompass, PubMed
- Veterinary relevance and importance in animal health > Search first: OMIA, veterinary databases, PubMed
- Comparative Biology:
- Comparative pathology (similarities and differences across species) > Search first: OMIA, comparative pathology databases, PubMed
- Evolutionary conservation of disease mechanisms > Search first: HomoloGene, OrthoMCL, Alliance of Genome Resources
- Transmission (if applicable):
- Zoonotic potential > Search first: CDC zoonotic diseases, WHO zoonoses, GIDEON
- Cross-species susceptibility > Search first: NCBI Taxonomy, veterinary databases, PubMed
15. Model Organisms
- Model Types:
- Model organism type (mammalian, invertebrate, cellular, in vitro) > Search first: Alliance of Genome Resources, model organism databases
- Specific model systems (mouse, rat, zebrafish, Drosophila, C. elegans, yeast, cell lines, organoids, iPSCs) > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, SGD, ATCC, Cellosaurus
- Induced models (drug treatment, surgical intervention, environmental manipulation) > Search first: MGI, model organism databases, PubMed
- Genetic Models:
- Types available (knockout, knock-in, transgenic, conditional, humanized) > Search first: MGI, IMPC, KOMP, EuMMCR, IMSR
- Model Characteristics:
- Phenotype recapitulation (how well model reproduces human disease features) > Search first: Model organism databases, comparative studies, PubMed
- Model limitations (aspects of human disease not captured) > Search first: Model organism databases, PubMed, review articles
- Applications:
- Research applications (what aspects of disease can be studied) > Search first: Model organism databases, PubMed
- Resources:
- Model databases > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, IMSR, EMMA, MMRRC
Citation Requirements
- Cite primary literature (PMID preferred) for all mechanistic and clinical claims
- Prioritize recent reviews and landmark papers
- Include direct quotes from abstracts where possible to support key statements
- Distinguish evidence source types: human clinical, model organism, in vitro, computational
Output Format
Structure your response as a comprehensive narrative organized by the sections above. For each section, provide: - Factual content with specific details (numbers, percentages, gene names, variant nomenclature) - Ontology term suggestions (HPO, GO, CL, UBERON, CHEBI, MAXO, MONDO) where applicable - Evidence citations with PMIDs - Direct quotes from abstracts to support key claims - Clear indication when information is not available or not applicable for this disease
This report will be used to populate a disease knowledge base entry with: - Pathophysiology descriptions with causal chains - Gene/protein annotations (HGNC, GO terms) - Phenotype associations (HP terms) with frequencies - Cell type involvement (CL terms) - Anatomical locations (UBERON terms) - Chemical entities (CHEBI terms) - Treatment annotations (MAXO terms) - Evidence items with PMIDs and exact abstract quotes - Epidemiology, prognosis, diagnostic, and prevention information - Animal model descriptions with phenotype recapitulation details
Optic Neuritis (ON): Disease Characteristics Research Report (Neurological Disorder)
Executive summary (current understanding)
Optic neuritis (ON) is an inflammatory optic neuropathy characterized clinically by acute/subacute visual loss with features such as impaired color/contrast vision and (in many cases) pain on eye movements; it is a common first manifestation of immune-mediated CNS demyelination and can also occur with antibody-mediated diseases (AQP4-IgG NMOSD; MOG-IgG–associated disease), infections, and systemic inflammatory disorders. A major 2022 international Delphi consensus (ICON) proposed standardized diagnostic criteria and a hierarchical classification to reduce misdiagnosis and to support subtype-specific management. (petzold2022diagnosisandclassification pages 1-3, petzold2022diagnosisandclassification pages 5-8)
Report scope and evidence sources
This report prioritizes 2022–2024 consensus, cohort, and multicenter studies retrieved in the current evidence set. Where key ontology identifiers (e.g., ICD-10, MeSH) were requested but not retrievable from the present corpus, the gap is explicitly flagged.
1. Disease information
1.1 What is the disease?
The ICON 2022 consensus addresses ON as a clinical syndrome requiring defined clinical features plus supportive paraclinical evidence (MRI/OCT/biomarkers) to establish definite ON; the work was motivated by frequent misdiagnosis and the expanding set of immune-mediated ON subtypes. (petzold2022diagnosisandclassification pages 1-3, petzold2022diagnosisandclassification pages 5-8)
Direct abstract quote (ICON 2022): “We have developed diagnostic criteria for optic neuritis and a classification of optic neuritis subgroups.” (petzold2022diagnosisandclassification pages 1-3)
1.2 Key identifiers
- OpenTargets/EFO: optic neuritis EFO_0007405 (OpenTargets Search: optic neuritis)
- MONDO: autoimmune optic neuritis MONDO_0031013 (OpenTargets Search: optic neuritis)
- ICD-10 / ICD-11 / MeSH / OMIM / Orphanet: not retrieved in current evidence corpus (gap).
A consolidated identifiers/synonyms table is provided below.
| Preferred name | MONDO / EFO / other supported ID | ICD-10 / MeSH | Key related entities / subtype context | Common synonyms / alternative names | Source URL(s) and publication date(s) |
|---|---|---|---|---|---|
| Optic neuritis | EFO: EFO_0007405 (OpenTargets); MONDO not retrieved in current evidence | not retrieved in current evidence | Umbrella entity including MS-associated ON, MOG antibody-associated ON, and AQP4-IgG/NMOSD-associated ON (OpenTargets Search: optic neuritis, petzold2022diagnosisandclassification pages 1-3, petzold2022diagnosisandclassification pages 5-8) | optic nerve inflammation; inflammatory optic neuropathy; demyelinating optic neuritis (spillers2024acomparativereview pages 1-2, petzold2022diagnosisandclassification pages 1-3) | OpenTargets disease association context: no standalone public URL retrieved in current evidence, context-based ID mapping from OpenTargets (OpenTargets Search: optic neuritis); Petzold et al., Lancet Neurol 2022-09, https://doi.org/10.1016/S1474-4422(22)00200-9 (petzold2022diagnosisandclassification pages 1-3, petzold2022diagnosisandclassification pages 5-8) |
| Autoimmune optic neuritis | MONDO: MONDO_0031013 | not retrieved in current evidence | Level-1/level-2 classification concept covering relapsing autoimmune ON subgroups such as AQP4-ON, MOG-ON, MS-ON, CRMP5-ON, RION/CRION (OpenTargets Search: optic neuritis, petzold2022diagnosisandclassification pages 5-8) | autoimmune ON; relapsing autoimmune optic neuritis (petzold2022diagnosisandclassification pages 5-8) | OpenTargets context for MONDO mapping: no standalone public URL retrieved in current evidence (OpenTargets Search: optic neuritis); Petzold et al., Lancet Neurol 2022-09, https://doi.org/10.1016/S1474-4422(22)00200-9 (petzold2022diagnosisandclassification pages 1-3, petzold2022diagnosisandclassification pages 5-8) |
| Myelin oligodendrocyte glycoprotein antibody-associated optic neuritis | No MONDO/EFO identifier retrieved in current evidence for this exact subtype | not retrieved in current evidence | MOG-ON; subtype of MOGAD; often bilateral, disc swelling, longitudinally extensive optic nerve lesion/perineuritis, steroid responsive but relapse-prone (jeyakumar2024mogantibodyassociatedoptic pages 1-2) | MOG-ON; MOG antibody-associated optic neuritis; MOG-IgG-associated optic neuritis (jeyakumar2024mogantibodyassociatedoptic pages 1-2) | Jeyakumar et al., Eye 2024-05, https://doi.org/10.1038/s41433-024-03108-y (jeyakumar2024mogantibodyassociatedoptic pages 1-2); Volpe et al., Neurol Neuroimmunol Neuroinflamm 2024-11, https://doi.org/10.1212/NXI.0000000000200291 (volpe2024diagnosticvalueof pages 1-2) |
| Aquaporin-4 antibody-associated optic neuritis / NMOSD-associated optic neuritis | Related disease in OpenTargets: EFO: EFO_0004256 for neuromyelitis optica; exact ON subtype identifier not retrieved in current evidence | not retrieved in current evidence | AQP4-ON; NMOSD-ON; severe visual loss, poorer recovery, often relapsing autoimmune ON (greco2023beyondmyelinoligodendrocyte pages 1-2, oertel2023diagnosticvalueof pages 1-2, briggs2024prevalenceofneuromyelitis pages 1-3) | AQP4-ON; AQP4-IgG optic neuritis; NMOSD-associated optic neuritis; neuromyelitis optica spectrum disorder optic neuritis (greco2023beyondmyelinoligodendrocyte pages 1-2, oertel2023diagnosticvalueof pages 1-2) | Briggs & Shaia, Mult Scler 2024-01, https://doi.org/10.1177/13524585231224683 (briggs2024prevalenceofneuromyelitis pages 1-3); Oertel et al., J Neurol Neurosurg Psychiatry 2023-02, https://doi.org/10.1136/jnnp-2022-330608 (oertel2023diagnosticvalueof pages 1-2) |
| Multiple sclerosis-associated optic neuritis | Related disease in OpenTargets: EFO: EFO_0003929 for relapsing-remitting multiple sclerosis; exact ON subtype identifier not retrieved in current evidence | not retrieved in current evidence | MS-ON; typical optic neuritis phenotype; often unilateral, painful, relatively favorable visual recovery (spillers2024acomparativereview pages 4-5, spillers2024acomparativereview pages 1-2, loginovic2024applyingagenetic pages 1-2) | MS-ON; typical optic neuritis; multiple sclerosis-related optic neuritis (spillers2024acomparativereview pages 4-5, spillers2024acomparativereview pages 1-2) | Loginovic et al., Nat Commun 2024-02, https://doi.org/10.1038/s41467-024-44917-9 (loginovic2024applyingagenetic pages 1-2, loginovic2024applyingagenetic pages 2-4); Petzold et al., Lancet Neurol 2022-09, https://doi.org/10.1016/S1474-4422(22)00200-9 (petzold2022diagnosisandclassification pages 1-3, petzold2022diagnosisandclassification pages 5-8) |
Table: This table summarizes disease identifiers and commonly used names for optic neuritis and its major biomarker-defined or disease-associated subtypes, limited to identifiers explicitly supported by the retrieved evidence. It is useful for harmonizing terminology in a disease knowledge base while flagging identifier gaps not resolved in the current evidence set.
1.3 Synonyms and alternative names
Examples supported in the current corpus include “inflammatory optic neuropathy” and “demyelinating optic neuritis” in the context of typical (MS-associated) ON and biomarker-defined ON subtypes. (spillers2024acomparativereview pages 1-2, petzold2022diagnosisandclassification pages 1-3)
1.4 Evidence provenance (individual vs aggregated)
- ICON diagnostic criteria and classification are aggregated expert consensus using a Delphi process across multiple specialties and regions. (petzold2022diagnosisandclassification pages 3-5, petzold2022diagnosisandclassification pages 5-8)
- Plasma exchange outcomes and OCT diagnostic metrics are aggregated multicenter cohort evidence. (chen2023visualoutcomesfollowing pages 1-3, oertel2023diagnosticvalueof pages 1-2, volpe2024diagnosticvalueof pages 1-2)
2. Etiology
ON is etiologically heterogeneous. ICON emphasizes that “more than 60 conditions can be the subsequent diagnosis after an initial episode of optic neuritis or cause optic neuritis at any time during the disease” and proposes a top-level dichotomy to guide management: autoimmune (often relapsing) versus infectious/systemic (often monophasic). (petzold2022diagnosisandclassification pages 5-8)
2.1 Major immune-mediated causes
- Multiple sclerosis–associated ON (MS-ON): A prototypical “typical” ON phenotype in many neurology/neuro-ophthalmology teaching datasets. A 2024 review summarizes that ON is the first demyelinating event in ~20% of MS and that ~50% of MS patients develop ON at some point. (spillers2024acomparativereview pages 4-5)
- AQP4-IgG neuromyelitis optica spectrum disorder–associated ON (AQP4-ON / NMOSD-ON): NMOSD is a CNS demyelinating autoimmune disease that predominantly affects optic nerves and spinal cord, with near 80% having detectable anti–AQP4-IgG in one recent US EHR study’s background statement. (briggs2024prevalenceofneuromyelitis pages 1-3)
- MOG-IgG–associated disease optic neuritis (MOG-ON): A 2024 MOG-ON review states MOGAD is distinct from MS and AQP4-NMOSD and that MOG-ON has characteristic clinical/MRI features (bilateral involvement, disc swelling, longitudinally extensive optic nerve hyperintensity and perineuritis); serum MOG-IgG detection by live cell-based assays in compatible phenotypes is described as highly specific. (jeyakumar2024mogantibodyassociatedoptic pages 1-2)
2.2 Infectious/systemic and other causes
ICON’s level-1 classification explicitly includes infectious ON, post-infectious ON, post-vaccination ON, and systemic conditions as typically monophasic groups, contrasted with autoimmune relapsing categories. (petzold2022diagnosisandclassification pages 5-8)
2.3 Genetic susceptibility and risk stratification (MS after ON)
A 2024 Nature Communications study reports that at first presentation with undifferentiated ON, combining an MS genetic risk score (MS-GRS) with demographic factors improved prediction of subsequent MS; one SD increase in MS-GRS increased the hazard of MS by ~1.3-fold and predicted-risk quartiles showed incident MS rates from 4% to 41%. (loginovic2024applyingagenetic pages 1-2, loginovic2024applyingagenetic pages 2-4)
Direct abstract quote (Loginovic 2024): “Optic neuritis (ON) is associated with numerous immune-mediated inflammatory diseases, but 50% patients are ultimately diagnosed with multiple sclerosis (MS).” (loginovic2024applyingagenetic pages 1-2)
2.4 Risk and protective factors
Risk-factor statements in general reviews (e.g., obesity, smoking, latitude) are mentioned but are not consistently quantified with primary-study effect sizes within the current evidence corpus; the only well-quantified, ON-specific risk stratification evidence in the present corpus is the MS-GRS model for post-ON MS diagnosis risk. (spillers2024acomparativereview pages 1-2, loginovic2024applyingagenetic pages 1-2)
3. Phenotypes (clinical presentation)
3.1 Core symptom complex
ICON clinical criteria define ON presentations as: - A (classic): “Monocular, sub-acute loss of vision associated with orbital pain worsening on eye movements, reduced contrast and colour vision, and relative afferent pupillary deficit (RAPD).” (petzold2022diagnosisandclassification pages 5-8) - B: painless variant with remaining A features (petzold2022diagnosisandclassification pages 5-8) - C: binocular vision loss with A/B features (petzold2022diagnosisandclassification pages 5-8)
A 2024 review summarizing ONTT reports pain with eye movement in ~90% and emphasizes generally favorable long-term visual outcomes in typical ON. (spillers2024acomparativereview pages 4-5)
3.2 Typical vs atypical phenotype patterns (examples with statistics)
From a 2023 review of serostatus-informed ON differentials: - NMOSD/AQP4-ON: severe visual loss and poorer recovery; bilateral involvement ~20%; chiasmal lesions up to ~two thirds in some series. (greco2023beyondmyelinoligodendrocyte pages 1-2) - MOG-ON: optic disc edema ~80%; bilateral involvement ~50%; often steroid-responsive. (greco2023beyondmyelinoligodendrocyte pages 1-2)
From a multicenter OCT study differentiating older-adult unilateral MOGAD-ON from NAION: - Eye pain strongly associated with MOGAD-ON (OR ~32.9); visual outcomes show worse nadir but better recovery in MOGAD-ON than NAION. (tisavipat2024acuteopticneuropathy pages 1-2)
3.3 Suggested HPO phenotype terms (non-exhaustive; for knowledge-base seeding)
(These are ontology suggestions; HPO IDs are not retrieved in current evidence and should be verified against HPO.) - Subacute vision loss; decreased visual acuity - Eye pain / pain with eye movement - Dyschromatopsia (acquired color vision deficit) - Reduced contrast sensitivity - Relative afferent pupillary defect - Optic disc edema / optic disc swelling - Visual field defect - Bilateral optic neuritis (in MOG-ON and some NMOSD-ON)
3.4 Quality of life impact
The US NMOSD prevalence study notes that lasting neurological deficits that impact quality of life are common in NMOSD, which frequently includes optic neuritis attacks. (briggs2024prevalenceofneuromyelitis pages 1-3)
4. Genetic / molecular information
4.1 Causal genes vs biomarker-defined disease
Classic ON is not typically monogenic; instead, modern practice emphasizes biomarker-defined autoimmune ON subtypes and associated autoimmune mechanisms.
4.2 Key biomarkers in ICON classification (Level 2)
ICON Level-2 autoimmune ON subtypes include: - AQP4-ON, MOG-ON, CRMP5-ON, MS-ON, and clinical entities such as SION/RION/CRION. (petzold2022diagnosisandclassification pages 5-8)
4.3 Target/therapy linkage (knowledge-base enrichment)
OpenTargets association evidence in this corpus links optic neuritis and related demyelinating diseases to therapy targets used in practice (e.g., NR3C1 reflecting glucocorticoid pathway for acute therapy; and NMOSD targets including C5, IL6R, CD19 reflecting approved relapse-prevention therapies). (OpenTargets Search: optic neuritis)
5. Environmental information
ICON’s level-1 framework explicitly includes post-infectious and post-vaccination ON categories (typically monophasic), supporting infection/immune-trigger environmental contributions in subsets. (petzold2022diagnosisandclassification pages 5-8)
A specific infectious trigger example in the current corpus (observational) includes optic neuritis temporally associated with mild COVID-19 more often in MOG-ON than AQP4-ON, with detailed timing statistics. (jeyakumar2024mogantibodyassociatedoptic pages 1-2)
6. Mechanism / pathophysiology
6.1 Mechanistic framing (ICON 2022)
ICON highlights that advances in autoantibody diagnostics, imaging, and OCT have changed ON phenotyping, and that timely identification of relapsing autoimmune subtypes is clinically critical because delayed or wrong treatment can be catastrophic for vision. (petzold2022diagnosisandclassification pages 5-8)
6.2 Antibody-mediated vs oligodendrocyte-mediated paradigms
- AQP4-IgG NMOSD: conceptualized as antibody-mediated astrocytopathy in many expert sources; in the present evidence set, NMOSD is characterized by anti–AQP4-IgG seropositivity in the majority of cases and severe acute deficits. (briggs2024prevalenceofneuromyelitis pages 1-3, spillers2024acomparativereview pages 4-5)
- MOGAD/MOG-ON: described as an oligodendrogliopathy, with characteristic radiology and frequent steroid-responsiveness but relapse risk with rapid tapering. (jeyakumar2024mogantibodyassociatedoptic pages 1-2)
6.3 Suggested GO biological process terms (conceptual; verify against GO)
- Immune-mediated demyelination
- Complement activation (especially NMOSD)
- Leukocyte migration / neuroinflammation
- Axon degeneration / neuronal death
6.4 Suggested Cell Ontology (CL) terms (conceptual; verify)
- Oligodendrocyte
- Astrocyte
- Microglia
- Retinal ganglion cell
7. Anatomical structures affected
7.1 Organ/system level
- Primary: optic nerve (cranial nerve II) (spillers2024acomparativereview pages 1-2)
- CNS/visual pathway involvement varies by etiology (MS, NMOSD, MOGAD). (spillers2024acomparativereview pages 4-5, jeyakumar2024mogantibodyassociatedoptic pages 1-2)
7.2 Suggested UBERON structures (conceptual; verify)
- Optic nerve
- Retina (particularly retinal nerve fiber layer and ganglion cell layer measured by OCT)
- Optic chiasm (notably in NMOSD-associated patterns) (greco2023beyondmyelinoligodendrocyte pages 1-2)
7.3 Lateralization/localization patterns
- Typical ON often unilateral; MOG-ON frequently bilateral at onset; NMOSD can be bilateral in a minority and can involve chiasm. (greco2023beyondmyelinoligodendrocyte pages 1-2, jeyakumar2024mogantibodyassociatedoptic pages 1-2)
8. Temporal development
ICON operationalizes time windows for interpretation of clinical/paraclinical evidence and provides definitions for acute/subacute/chronic presentations; paraclinical criteria differ in acute versus ≥3-month phases. (petzold2022diagnosisandclassification pages 5-8)
MOGAD shows a biphasic age distribution with peaks in childhood (5–10 years) and young/middle adulthood (20–45 years). (jeyakumar2024mogantibodyassociatedoptic pages 1-2)
9. Inheritance and population
9.1 Epidemiology of ON and related diseases
- General ON incidence (UK/USA): A 2024 genetic risk-stratification study cites population-based incidence of 3.7–5.1 per 100,000 person-years in the UK and USA. (loginovic2024applyingagenetic pages 1-2)
- MOGAD epidemiology: incidence ~1.6–4.8 per million/year, prevalence 1.3–2.5 per 100,000. (jeyakumar2024mogantibodyassociatedoptic pages 1-2)
- NMOSD (US 2022 prevalence): 6.88/100,000, with higher prevalence in Black individuals (12.99/100,000) and Asian individuals (9.41/100,000), and female predominance. (briggs2024prevalenceofneuromyelitis pages 1-3)
9.2 Sex and demographic patterns
- NMOSD female prevalence 9.48/100,000 vs male 3.52/100,000; female:male ~3.5:1 in US EHR data. (briggs2024prevalenceofneuromyelitis pages 1-3)
- ON cohorts and classic ON teaching often emphasize young adult predominance and female predominance. (spillers2024acomparativereview pages 1-2, loginovic2024applyingagenetic pages 1-2)
10. Diagnostics
10.1 ICON 2022 diagnostic criteria (key concepts)
ICON defines definite ON based on clinical pattern plus paraclinical support. (petzold2022diagnosisandclassification pages 5-8)
Paraclinical tests and thresholds (ICON Panel 1): - OCT: optic disc swelling acutely or inter-eye difference mGCIPL >4% or >4 μm or pRNFL >5% or >5 μm within ≥3 months after onset (petzold2022diagnosisandclassification pages 5-8) - MRI: optic nerve/sheath contrast enhancement acutely or intrinsic optic nerve signal increase within ≥3 months (petzold2022diagnosisandclassification pages 5-8) - Biomarkers: AQP4-IgG, MOG-IgG, CRMP5-IgG seropositivity, or CSF oligoclonal bands (intrathecal IgG) (petzold2022diagnosisandclassification pages 5-8)
10.2 Recent (2023–2024) validation and practical implementation of OCT criteria
- In AQP4+ NMOSD, inter-eye OCT difference metrics showed excellent discrimination between unilateral NMOSD-ON and controls (AUC up to 0.96 with sensitivity/specificity ~75–98% depending on metric). (oertel2023diagnosticvalueof pages 1-2)
- In MOG-ON, the mGCIP inter-eye percentage difference was highly sensitive (92%), with notably lower sensitivity in bilateral ON compared with unilateral ON. (volpe2024diagnosticvalueof pages 1-2)
10.3 Differential diagnosis (selected, evidence-backed examples)
- Older adults: differentiating MOGAD-ON from NAION using eye pain, optic disc anatomy, and OCT swelling patterns; caution regarding low-titer false-positive MOG-IgG in NAION (8% among those tested at Mayo in one cohort). (tisavipat2024acuteopticneuropathy pages 1-2)
11. Outcome / prognosis
11.1 Visual recovery in typical ON and MS risk
- Typical ON generally has favorable long-term vision; a 2024 review summarizing ONTT reports ~72% maintained 20/20 vision in both eyes at 15 years and pain with eye movement ~90% in typical ON. (spillers2024acomparativereview pages 4-5)
- MS conversion risk after undifferentiated ON can be stratified using MS-GRS models (4% to 41% MS incidence across risk quartiles). (loginovic2024applyingagenetic pages 1-2)
11.2 Outcomes with plasma exchange (PLEX) for severe ON (2023 multicenter data)
A large 2023 international multicenter retrospective cohort (395 attacks) reported median final VA ~20/25 after PLEX but with substantial residual severe vision loss in a subset (20.5% ≤20/200). Outcomes varied by etiology: MOGAD-ON had the best outcomes (median 20/20; 1% ≤20/200), while AQP4+ NMOSD had higher proportions with poor final VA (≈31% ≤20/200). Time-to-PLEX was associated with outcomes (median 2.4 vs 3.3 weeks in good vs poor outcome groups; p<0.001). (chen2023visualoutcomesfollowing pages 5-6, chen2023visualoutcomesfollowing pages 18-25)
The PLEX paper’s tables/figures supporting these outcome stratifications were retrieved as document images (Figures 2–4; Tables 1–3). (chen2023visualoutcomesfollowing media 1c706b2b)
12. Treatment
12.1 Acute attack treatment (general)
ICON’s framing and recent reviews emphasize that acute treatment should be time-sensitive, especially for atypical/autoimmune cases at risk of irreversible injury. (petzold2022diagnosisandclassification pages 5-8, spillers2024acomparativereview pages 1-2)
Common acute strategies discussed in current reviews include: - High-dose IV glucocorticoids (e.g., IV methylprednisolone) - Escalation to plasma exchange (PLEX) for severe and/or steroid-refractory attacks - IVIG in selected situations (evidence base remains incomplete) (spillers2024acomparativereview pages 6-7)
12.2 Evidence for PLEX in severe ON
The 2023 multicenter retrospective analysis supports meaningful recovery in many severe cases treated with PLEX and suggests improved outcomes compared with matched severe ONTT subsets (e.g., final VA worse than 20/40: 12% PLEX vs 33% ONTT IVMP without PLEX; p=0.04). (chen2023visualoutcomesfollowing pages 1-3, chen2023visualoutcomesfollowing pages 6-8)
12.3 Treatment considerations by subtype
- MOG-ON: described as largely corticosteroid-responsive, but relapse risk is common with early/rapid tapering, motivating research on steroid-sparing relapse prevention. (jeyakumar2024mogantibodyassociatedoptic pages 1-2)
- AQP4+ NMOSD: relapse prevention is central; the present evidence set includes real-world effectiveness/safety data for complement inhibition with eculizumab (attack-free 88% during therapy; systemic infection risks and vaccine-timing issues). (spillers2024acomparativereview pages 8-9)
12.4 Suggested MAXO terms (conceptual; verify)
- High-dose intravenous glucocorticoid therapy
- Therapeutic plasma exchange
- Intravenous immunoglobulin therapy
- Long-term immunosuppression / immunomodulation (subtype-specific)
13. Prevention
No primary prevention is established for idiopathic/typical ON. Secondary/tertiary prevention is subtype-driven: - Prevent relapse and disability in NMOSD/MOGAD via appropriate long-term therapy and monitoring. (petzold2022diagnosisandclassification pages 5-8, jeyakumar2024mogantibodyassociatedoptic pages 1-2)
14. Other species / natural disease
Not resolved in the current evidence corpus.
15. Model organisms
Not resolved with citeable model-organism primary literature in the current evidence corpus. (Preclinical ON/EAE papers were retrieved during search but were not converted into citeable evidence snippets in this run; therefore they are not included as claims here.)
Recent developments (2022–2024) and real-world implementation highlights
The following table compiles the most actionable, recent quantitative evidence for clinical implementation (ICON 2022 criteria; OCT thresholds validation in AQP4+ NMOSD and MOG-ON; PLEX outcomes; NMOSD prevalence; MS genetic risk stratification).
| Topic | Key finding/statistic | Population/study design | Publication (authors, journal) | Year/month | DOI/URL | Evidence type |
|---|---|---|---|---|---|---|
| Diagnostic criteria (ICON/International Consensus) | Clinical criteria: A = monocular, subacute vision loss with orbital pain on eye movement, reduced contrast/color vision, RAPD; B = painless with all other features of A; C = binocular loss with features of A or B. Paraclinical thresholds: OCT mGCIPL inter-eye difference >4% or >4 μm or pRNFL >5% or >5 μm within ≥3 months after onset; MRI symptomatic optic nerve/sheath contrast enhancement acutely or intrinsic T2 signal increase within ≥3 months; biomarkers: AQP4, MOG, CRMP5 seropositivity or CSF oligoclonal bands. Definite ON: A + 1 paraclinical test; B + 2 tests of different modality; C + MRI + 1 other paraclinical test (petzold2022diagnosisandclassification pages 5-8) | International Delphi consensus diagnostic/classification framework for optic neuritis | Petzold et al., Lancet Neurology | 2022/Sep | 10.1016/S1474-4422(22)00200-9; https://doi.org/10.1016/S1474-4422(22)00200-9 | Guideline/consensus (human expert Delphi) |
| OCT thresholds validated in AQP4+ NMOSD-ON | Proposed thresholds tested: pRNFL IEAD 5 μm, IEPD 5%; GCIPL IEAD 4 μm, IEPD 4%. NMOSD-ON vs healthy controls: pRNFL IEAD AUC 0.95, specificity 82%, sensitivity 86%; GCIPL IEAD AUC 0.93, specificity 98%, sensitivity 75%; pRNFL IEPD AUC 0.96, specificity 87%, sensitivity 89%; GCIPL IEPD AUC 0.94, specificity 96%, sensitivity 82%. NMOSD-ON vs NMOSD-NON: pRNFL IEAD AUC 0.92, specificity 77%, sensitivity 86%; GCIPL IEAD AUC 0.87, specificity 85%, sensitivity 75%; pRNFL IEPD AUC 0.94, specificity 82%, sensitivity 89%; GCIPL IEPD AUC 0.88, specificity 82%, sensitivity 82% (oertel2023diagnosticvalueof pages 1-2) | Multicenter study of 28 AQP4+ NMOSD unilateral ON, 45 AQP4+ NMOSD without ON history, 62 healthy controls | Oertel et al., JNNP | 2023/Feb | 10.1136/jnnp-2022-330608; https://doi.org/10.1136/jnnp-2022-330608 | Human multicenter diagnostic cohort |
| OCT thresholds validated in MOG-ON | Using ICON-related published cutoffs (>4% or >4 μm mGCIP; >5% or >5 μm pRNFL), pooled MOG-ON analysis showed mGCIP IEPD sensitivity 92%, mGCIP IEAD 88%, pRNFL 84%; specificity: mGCIP IEPD 82%, mGCIP IEAD 82%, pRNFL IEPD 82%, pRNFL IEAD 79%. In unilateral ON, diagnostic sensitivity was >99% for all metrics; in bilateral ON, sensitivity fell to 61%–78% (volpe2024diagnosticvalueof pages 1-2) | Multicenter validation study of 66 participants (33 MOG-ON, 33 controls) | Volpe et al., Neurology Neuroimmunology & Neuroinflammation | 2024/Nov | 10.1212/NXI.0000000000200291; https://doi.org/10.1212/NXI.0000000000200291 | Human multicenter diagnostic cohort |
| PLEX outcomes in severe ON | 395 ON attacks in 317 patients; median time from vision loss onset to PLEX 2.6 weeks (IQR 1.4–4.0); median VA at PLEX count fingers (IQR 20/200–hand motion); median final VA 20/25 (IQR 20/20–20/60); 81 attacks (20.5%) ended with final VA 20/200 or worse. Poorer outcomes associated with older age (p=0.002), worse VA at PLEX (p<0.001), and longer delay to PLEX (p<0.001). In matched comparison, final VA worse than 20/40 occurred in 12% (6/50) of PLEX-treated attacks vs 33% (6/18) in ONTT IVMP without PLEX (p=0.04) (chen2023visualoutcomesfollowing pages 1-3) | International multicenter retrospective analysis; etiologies included MS (108), MOGAD (92), AQP4+ NMOSD (75), seronegative NMOSD (34), idiopathic (83) | Chen et al., American Journal of Ophthalmology | 2023/Aug | 10.1016/j.ajo.2023.02.013; https://doi.org/10.1016/j.ajo.2023.02.013 | Human multicenter retrospective cohort |
| MOGAD / MOG-ON epidemiology and phenotype | MOGAD incidence ~1.6–4.8 per million/year; prevalence 1.3–2.5 per 100,000; biphasic onset peaks at 5–10 years and 20–45 years. Optic neuritis is the commonest adult presentation (~30–60%). Distinctive features include frequent bilateral onset, optic disc swelling, headache, longitudinally extensive optic nerve hyperintensity, and optic perineuritis on MRI; serum live cell-based assay MOG-IgG is highly specific (jeyakumar2024mogantibodyassociatedoptic pages 1-2) | Narrative review synthesizing cohort/registry data on MOG antibody-associated optic neuritis | Jeyakumar et al., Eye | 2024/May | 10.1038/s41433-024-03108-y; https://doi.org/10.1038/s41433-024-03108-y | Human review of cohort/registry evidence |
| NMOSD prevalence in the US | 2022 prevalence 6.88/100,000 from 1,772 patients among 25,743,039 EHR patients. By race: Black 12.99/100,000, Asian 9.41/100,000, White 5.58/100,000. Among females, prevalence 9.48/100,000; Black and Asian females had 2.65× and 1.94× higher prevalence than White females. Male prevalence 3.52/100,000; female:male ratio about 3.5:1. Estimated US burden: 15,413 females and 6,233 males (~22,000 total) (briggs2024prevalenceofneuromyelitis pages 1-3) | Cross-sectional prevalence study using nationwide aggregated EHR data from 55 healthcare organizations | Briggs & Shaia, Multiple Sclerosis Journal | 2024/Jan | 10.1177/13524585231224683; https://doi.org/10.1177/13524585231224683 | Human population-based EHR epidemiology |
| MS risk stratification after ON using genetics | In undifferentiated ON, one SD increase in MS genetic risk score (MS-GRS) increased hazard of MS 1.3-fold; multivariable HR 1.29 (95% CI 1.07–1.55, P=0.0067). Predicted-risk quartiles developed incident MS at rates from 4% (95% CI 0.5–7%, lowest quartile) to 41% (95% CI 33–49%, highest quartile). Background rates in study: ON incidence cited as 3.7–5.1 per 100,000 person-years in UK/USA; by 5 years, about 20% of undifferentiated ON diagnosed with MS; by 15 years, up to 50% of ON (excluding bilateral presentation) diagnosed with MS. In UK Biobank, among 545 undifferentiated ON cases, 124 (22.8%) developed MS during median 18.4 years follow-up (loginovic2024applyingagenetic pages 1-2, loginovic2024applyingagenetic pages 2-4) | UK Biobank primary analysis with replication in Geisinger and FinnGen; genetic risk modeling in ON | Loginovic et al., Nature Communications | 2024/Feb | 10.1038/s41467-024-44917-9; https://doi.org/10.1038/s41467-024-44917-9 | Human genomic cohort / prognostic modeling |
Table: This table compiles high-yield quantitative findings from 2022-2024 on optic neuritis diagnostic criteria, imaging thresholds, outcomes, epidemiology, and MS risk prediction. It is useful as a compact evidence summary for knowledge-base curation and citation-backed reporting.
Limitations and evidence gaps (important for knowledge-base curation)
- ICD-10/ICD-11, MeSH, OMIM, and Orphanet identifiers were not retrievable from the current corpus and should be added from dedicated ontology sources in a subsequent retrieval step.
- HPO/GO/UBERON/CL/MAXO term mappings are provided as suggestions and require ontology-validated IDs.
- Animal model evidence was retrieved in searches but not captured as citeable evidence snippets in the current run; therefore, the model-organism section is left as “not resolved” rather than inferred.
References
-
(petzold2022diagnosisandclassification pages 1-3): Axel Petzold, Clare L Fraser, Mathias Abegg, Raed Alroughani, Daniah Alshowaeir, Regina Alvarenga, Cécile Andris, Nasrin Asgari, Yael Barnett, Roberto Battistella, Raed Behbehani, Thomas Berger, Mukharram M Bikbov, Damien Biotti, Valerie Biousse, Antonella Boschi, Milan Brazdil, Andrei Brezhnev, Peter A Calabresi, Monique Cordonnier, Fiona Costello, Franz M Cruz, Leonardo Provetti Cunha, Smail Daoudi, Romain Deschamps, Jerome De Seze, Ricarda Diem, Masoud Etemadifar, Jose Flores-Rivera, Pedro Fonseca, Jette Frederiksen, Elliot Frohman, Teresa Frohman, Caroline Froment Tilikete, Kazuo Fujihara, Alberto Gálvez, Riadh Gouider, Fernando Gracia, Nikolaos Grigoriadis, José M Guajardo, Mario Habek, Marko Hawlina, Elena H Martínez-Lapiscina, Juzar Hooker, Jyh Yung Hor, William Howlett, Yumin Huang-Link, Zhannat Idrissova, Zsolt Illes, Jasna Jancic, Panitha Jindahra, Dimitrios Karussis, Emilia Kerty, Ho Jin Kim, Wolf Lagrèze, Letizia Leocani, Netta Levin, Petra Liskova, Yaou Liu, Youssoufa Maiga, Romain Marignier, Chris McGuigan, Dália Meira, Harold Merle, Mário L R Monteiro, Anand Moodley, Frederico Moura, Silvia Muñoz, Sharik Mustafa, Ichiro Nakashima, Susana Noval, Carlos Oehninger, Olufunmilola Ogun, Afekhide Omoti, Lekha Pandit, Friedemann Paul, Gema Rebolleda, Stephen Reddel, Konrad Rejdak, Robert Rejdak, Alfonso J Rodriguez-Morales, Marie-Bénédicte Rougier, Maria Jose Sa, Bernardo Sanchez-Dalmau, Deanna Saylor, Ismail Shatriah, Aksel Siva, Hadas Stiebel-Kalish, Gabriella Szatmary, Linh Ta, Silvia Tenembaum, Huy Tran, Yevgen Trufanov, Vincent Van Pesch, An-Guor Wang, Mike P Wattjes, Ernest Willoughby, Magd Zakaria, Jasmin Zvornicanin, Laura Balcer, and Gordon T Plant. Diagnosis and classification of optic neuritis. The Lancet Neurology, 21:1120-1134, Sep 2022. URL: https://doi.org/10.1016/s1474-4422(22)00200-9, doi:10.1016/s1474-4422(22)00200-9. This article has 345 citations and is from a highest quality peer-reviewed journal.
-
(petzold2022diagnosisandclassification pages 5-8): Axel Petzold, Clare L Fraser, Mathias Abegg, Raed Alroughani, Daniah Alshowaeir, Regina Alvarenga, Cécile Andris, Nasrin Asgari, Yael Barnett, Roberto Battistella, Raed Behbehani, Thomas Berger, Mukharram M Bikbov, Damien Biotti, Valerie Biousse, Antonella Boschi, Milan Brazdil, Andrei Brezhnev, Peter A Calabresi, Monique Cordonnier, Fiona Costello, Franz M Cruz, Leonardo Provetti Cunha, Smail Daoudi, Romain Deschamps, Jerome De Seze, Ricarda Diem, Masoud Etemadifar, Jose Flores-Rivera, Pedro Fonseca, Jette Frederiksen, Elliot Frohman, Teresa Frohman, Caroline Froment Tilikete, Kazuo Fujihara, Alberto Gálvez, Riadh Gouider, Fernando Gracia, Nikolaos Grigoriadis, José M Guajardo, Mario Habek, Marko Hawlina, Elena H Martínez-Lapiscina, Juzar Hooker, Jyh Yung Hor, William Howlett, Yumin Huang-Link, Zhannat Idrissova, Zsolt Illes, Jasna Jancic, Panitha Jindahra, Dimitrios Karussis, Emilia Kerty, Ho Jin Kim, Wolf Lagrèze, Letizia Leocani, Netta Levin, Petra Liskova, Yaou Liu, Youssoufa Maiga, Romain Marignier, Chris McGuigan, Dália Meira, Harold Merle, Mário L R Monteiro, Anand Moodley, Frederico Moura, Silvia Muñoz, Sharik Mustafa, Ichiro Nakashima, Susana Noval, Carlos Oehninger, Olufunmilola Ogun, Afekhide Omoti, Lekha Pandit, Friedemann Paul, Gema Rebolleda, Stephen Reddel, Konrad Rejdak, Robert Rejdak, Alfonso J Rodriguez-Morales, Marie-Bénédicte Rougier, Maria Jose Sa, Bernardo Sanchez-Dalmau, Deanna Saylor, Ismail Shatriah, Aksel Siva, Hadas Stiebel-Kalish, Gabriella Szatmary, Linh Ta, Silvia Tenembaum, Huy Tran, Yevgen Trufanov, Vincent Van Pesch, An-Guor Wang, Mike P Wattjes, Ernest Willoughby, Magd Zakaria, Jasmin Zvornicanin, Laura Balcer, and Gordon T Plant. Diagnosis and classification of optic neuritis. The Lancet Neurology, 21:1120-1134, Sep 2022. URL: https://doi.org/10.1016/s1474-4422(22)00200-9, doi:10.1016/s1474-4422(22)00200-9. This article has 345 citations and is from a highest quality peer-reviewed journal.
-
(OpenTargets Search: optic neuritis): Open Targets Query (optic neuritis, 18 results). Buniello, A. et al. (2025). Open Targets Platform: facilitating therapeutic hypotheses building in drug discovery. Nucleic Acids Research.
-
(spillers2024acomparativereview pages 1-2): Noah J Spillers, Patrick M Luther, Norris C Talbot, Evan J Kidder, Connor A Doyle, Salim C Lutfallah, Alyssa G Derouen, Sridhar Tirumala, Shahab Ahmadzadeh, Sahar Shekoohi, Alan D Kaye, and Giustino Varrassi. A comparative review of typical and atypical optic neuritis: advancements in treatments, diagnostics, and prognosis. Cureus, Mar 2024. URL: https://doi.org/10.7759/cureus.56094, doi:10.7759/cureus.56094. This article has 11 citations.
-
(jeyakumar2024mogantibodyassociatedoptic pages 1-2): Niroshan Jeyakumar, Magdalena Lerch, Russell C. Dale, and Sudarshini Ramanathan. Mog antibody-associated optic neuritis. Eye, 38:2289-2301, May 2024. URL: https://doi.org/10.1038/s41433-024-03108-y, doi:10.1038/s41433-024-03108-y. This article has 69 citations and is from a peer-reviewed journal.
-
(volpe2024diagnosticvalueof pages 1-2): Giulio Volpe, Neringa Jurkute, Gabriela Girafa, Hanna G. Zimmermann, Seyedamirhosein Motamedi, Charlotte Bereuter, Lekha Pandit, Anitha D'Cunha, Michael R. Yeaman, Terry J. Smith, Lawrence J. Cook, Alexander U. Brandt, Friedemann Paul, Axel Petzold, and Frederike C. Oertel. Diagnostic value of inter-eye difference metrics on oct for myelin oligodendrocyte glycoprotein antibody-associated optic neuritis. Neurology Neuroimmunology & Neuroinflammation, Nov 2024. URL: https://doi.org/10.1212/nxi.0000000000200291, doi:10.1212/nxi.0000000000200291. This article has 11 citations.
-
(greco2023beyondmyelinoligodendrocyte pages 1-2): Giacomo Greco, Elena Colombo, Matteo Gastaldi, Lara Ahmad, Eleonora Tavazzi, Roberto Bergamaschi, and Eleonora Rigoni. Beyond myelin oligodendrocyte glycoprotein and aquaporin-4 antibodies: alternative causes of optic neuritis. International Journal of Molecular Sciences, 24:15986, Nov 2023. URL: https://doi.org/10.3390/ijms242115986, doi:10.3390/ijms242115986. This article has 15 citations.
-
(oertel2023diagnosticvalueof pages 1-2): Frederike Cosima Oertel, Hanna G Zimmermann, Seyedamirhosein Motamedi, Claudia Chien, Orhan Aktas, Philipp Albrecht, Marius Ringelstein, Anitha Dcunha, Lekha Pandit, Elena H Martinez-Lapiscina, Bernardo Sanchez-Dalmau, Pablo Villoslada, Jacqueline Palace, Adriana Roca-Fernández, Maria Isabel Leite, Srilakshmi M Sharma, Letizia Leocani, Marco Pisa, Marta Radaelli, Marco Aurélio Lana-Peixoto, Mariana Andrade Fontenelle, Joachim Havla, Fereshteh Ashtari, Rahele Kafieh, Alireza Dehghani, Mohsen Pourazizi, Romain Marignier, Alvaro Cobo-Calvo, Nasrin Asgari, Anu Jacob, Saif Huda, Yang Mao-Draayer, Ari J Green, Rachel Kenney, Michael R Yeaman, Terry J Smith, Lawrence Cook, Alexander U Brandt, Friedemann Paul, and Axel Petzold. Diagnostic value of intereye difference metrics for optic neuritis in aquaporin-4 antibody seropositive neuromyelitis optica spectrum disorders. Journal of Neurology, Neurosurgery, and Psychiatry, 94:560-566, Feb 2023. URL: https://doi.org/10.1136/jnnp-2022-330608, doi:10.1136/jnnp-2022-330608. This article has 7 citations.
-
(briggs2024prevalenceofneuromyelitis pages 1-3): Farren B S Briggs and Jacqueline Shaia. Prevalence of neuromyelitis optica spectrum disorder in the united states. Multiple Sclerosis Journal, 30:316-324, Jan 2024. URL: https://doi.org/10.1177/13524585231224683, doi:10.1177/13524585231224683. This article has 26 citations.
-
(spillers2024acomparativereview pages 4-5): Noah J Spillers, Patrick M Luther, Norris C Talbot, Evan J Kidder, Connor A Doyle, Salim C Lutfallah, Alyssa G Derouen, Sridhar Tirumala, Shahab Ahmadzadeh, Sahar Shekoohi, Alan D Kaye, and Giustino Varrassi. A comparative review of typical and atypical optic neuritis: advancements in treatments, diagnostics, and prognosis. Cureus, Mar 2024. URL: https://doi.org/10.7759/cureus.56094, doi:10.7759/cureus.56094. This article has 11 citations.
-
(loginovic2024applyingagenetic pages 1-2): Pavel Loginovic, Feiyi Wang, Jiang Li, Lauric Ferrat, Uyenlinh L. Mirshahi, H. Shanker Rao, Axel Petzold, Jessica Tyrrell, Harry D. Green, Michael N. Weedon, Andrea Ganna, Tiinamaija Tuomi, David J. Carey, Richard A. Oram, and Tasanee Braithwaite. Applying a genetic risk score model to enhance prediction of future multiple sclerosis diagnosis at first presentation with optic neuritis. Nature Communications, Feb 2024. URL: https://doi.org/10.1038/s41467-024-44917-9, doi:10.1038/s41467-024-44917-9. This article has 14 citations and is from a highest quality peer-reviewed journal.
-
(loginovic2024applyingagenetic pages 2-4): Pavel Loginovic, Feiyi Wang, Jiang Li, Lauric Ferrat, Uyenlinh L. Mirshahi, H. Shanker Rao, Axel Petzold, Jessica Tyrrell, Harry D. Green, Michael N. Weedon, Andrea Ganna, Tiinamaija Tuomi, David J. Carey, Richard A. Oram, and Tasanee Braithwaite. Applying a genetic risk score model to enhance prediction of future multiple sclerosis diagnosis at first presentation with optic neuritis. Nature Communications, Feb 2024. URL: https://doi.org/10.1038/s41467-024-44917-9, doi:10.1038/s41467-024-44917-9. This article has 14 citations and is from a highest quality peer-reviewed journal.
-
(petzold2022diagnosisandclassification pages 3-5): Axel Petzold, Clare L Fraser, Mathias Abegg, Raed Alroughani, Daniah Alshowaeir, Regina Alvarenga, Cécile Andris, Nasrin Asgari, Yael Barnett, Roberto Battistella, Raed Behbehani, Thomas Berger, Mukharram M Bikbov, Damien Biotti, Valerie Biousse, Antonella Boschi, Milan Brazdil, Andrei Brezhnev, Peter A Calabresi, Monique Cordonnier, Fiona Costello, Franz M Cruz, Leonardo Provetti Cunha, Smail Daoudi, Romain Deschamps, Jerome De Seze, Ricarda Diem, Masoud Etemadifar, Jose Flores-Rivera, Pedro Fonseca, Jette Frederiksen, Elliot Frohman, Teresa Frohman, Caroline Froment Tilikete, Kazuo Fujihara, Alberto Gálvez, Riadh Gouider, Fernando Gracia, Nikolaos Grigoriadis, José M Guajardo, Mario Habek, Marko Hawlina, Elena H Martínez-Lapiscina, Juzar Hooker, Jyh Yung Hor, William Howlett, Yumin Huang-Link, Zhannat Idrissova, Zsolt Illes, Jasna Jancic, Panitha Jindahra, Dimitrios Karussis, Emilia Kerty, Ho Jin Kim, Wolf Lagrèze, Letizia Leocani, Netta Levin, Petra Liskova, Yaou Liu, Youssoufa Maiga, Romain Marignier, Chris McGuigan, Dália Meira, Harold Merle, Mário L R Monteiro, Anand Moodley, Frederico Moura, Silvia Muñoz, Sharik Mustafa, Ichiro Nakashima, Susana Noval, Carlos Oehninger, Olufunmilola Ogun, Afekhide Omoti, Lekha Pandit, Friedemann Paul, Gema Rebolleda, Stephen Reddel, Konrad Rejdak, Robert Rejdak, Alfonso J Rodriguez-Morales, Marie-Bénédicte Rougier, Maria Jose Sa, Bernardo Sanchez-Dalmau, Deanna Saylor, Ismail Shatriah, Aksel Siva, Hadas Stiebel-Kalish, Gabriella Szatmary, Linh Ta, Silvia Tenembaum, Huy Tran, Yevgen Trufanov, Vincent Van Pesch, An-Guor Wang, Mike P Wattjes, Ernest Willoughby, Magd Zakaria, Jasmin Zvornicanin, Laura Balcer, and Gordon T Plant. Diagnosis and classification of optic neuritis. The Lancet Neurology, 21:1120-1134, Sep 2022. URL: https://doi.org/10.1016/s1474-4422(22)00200-9, doi:10.1016/s1474-4422(22)00200-9. This article has 345 citations and is from a highest quality peer-reviewed journal.
-
(chen2023visualoutcomesfollowing pages 1-3): John J. Chen, Eoin P. Flanagan, Sean J. Pittock, Nicole Caroline Stern, Nanthaya Tisavipat, M. Tariq Bhatti, Kevin D. Chodnicki, Deena A. Tajfirouz, Sepideh Jamali, Amy Kunchok, Eric R. Eggenberger, Marie A. Di Nome, Elias S. Sotirchos, Eleni S. Vasileiou, Amanda D. Henderson, Anthony C. Arnold, Laura Bonelli, Heather E. Moss, Sylvia Elizabeth Villarreal Navarro, Tanyatuth Padungkiatsagul, Hadas Stiebel-Kalish, Itay Lotan, Adi Wilf-Yarkoni, Helen Danesh-Meyer, Stefan Ivanov, Saif Huda, Mirasol Forcadela, David Hodge, Pascale Poullin, Julie Rode, Caroline Papeix, Samir Saheb, Marine Boudot de la Motte, Catherine Vignal, Yael Hacohen, Julie Pique, Elisabeth Maillart, Romain Deschamps, Bertrand Audoin, and Romain Marignier. Visual outcomes following plasma exchange for optic neuritis: an international multicenter retrospective analysis of 395 optic neuritis attacks. American Journal of Ophthalmology, 252:213-224, Aug 2023. URL: https://doi.org/10.1016/j.ajo.2023.02.013, doi:10.1016/j.ajo.2023.02.013. This article has 78 citations and is from a domain leading peer-reviewed journal.
-
(tisavipat2024acuteopticneuropathy pages 1-2): Nanthaya Tisavipat, Hadas Stiebel-Kalish, Dahlia Palevski, Omer Y. Bialer, Heather E. Moss, Pareena Chaitanuwong, Tanyatuth Padungkiatsagul, Amanda D. Henderson, Elias S. Sotirchos, Shonar Singh, Abdul-Rahman Salman, Deena A. Tajfirouz, Kevin D. Chodnicki, Sean J. Pittock, Eoin P. Flanagan, and John J. Chen. Acute optic neuropathy in older adults. Neurology Neuroimmunology & Neuroinflammation, May 2024. URL: https://doi.org/10.1212/nxi.0000000000200214, doi:10.1212/nxi.0000000000200214. This article has 17 citations.
-
(chen2023visualoutcomesfollowing pages 5-6): John J. Chen, Eoin P. Flanagan, Sean J. Pittock, Nicole Caroline Stern, Nanthaya Tisavipat, M. Tariq Bhatti, Kevin D. Chodnicki, Deena A. Tajfirouz, Sepideh Jamali, Amy Kunchok, Eric R. Eggenberger, Marie A. Di Nome, Elias S. Sotirchos, Eleni S. Vasileiou, Amanda D. Henderson, Anthony C. Arnold, Laura Bonelli, Heather E. Moss, Sylvia Elizabeth Villarreal Navarro, Tanyatuth Padungkiatsagul, Hadas Stiebel-Kalish, Itay Lotan, Adi Wilf-Yarkoni, Helen Danesh-Meyer, Stefan Ivanov, Saif Huda, Mirasol Forcadela, David Hodge, Pascale Poullin, Julie Rode, Caroline Papeix, Samir Saheb, Marine Boudot de la Motte, Catherine Vignal, Yael Hacohen, Julie Pique, Elisabeth Maillart, Romain Deschamps, Bertrand Audoin, and Romain Marignier. Visual outcomes following plasma exchange for optic neuritis: an international multicenter retrospective analysis of 395 optic neuritis attacks. American Journal of Ophthalmology, 252:213-224, Aug 2023. URL: https://doi.org/10.1016/j.ajo.2023.02.013, doi:10.1016/j.ajo.2023.02.013. This article has 78 citations and is from a domain leading peer-reviewed journal.
-
(chen2023visualoutcomesfollowing pages 18-25): John J. Chen, Eoin P. Flanagan, Sean J. Pittock, Nicole Caroline Stern, Nanthaya Tisavipat, M. Tariq Bhatti, Kevin D. Chodnicki, Deena A. Tajfirouz, Sepideh Jamali, Amy Kunchok, Eric R. Eggenberger, Marie A. Di Nome, Elias S. Sotirchos, Eleni S. Vasileiou, Amanda D. Henderson, Anthony C. Arnold, Laura Bonelli, Heather E. Moss, Sylvia Elizabeth Villarreal Navarro, Tanyatuth Padungkiatsagul, Hadas Stiebel-Kalish, Itay Lotan, Adi Wilf-Yarkoni, Helen Danesh-Meyer, Stefan Ivanov, Saif Huda, Mirasol Forcadela, David Hodge, Pascale Poullin, Julie Rode, Caroline Papeix, Samir Saheb, Marine Boudot de la Motte, Catherine Vignal, Yael Hacohen, Julie Pique, Elisabeth Maillart, Romain Deschamps, Bertrand Audoin, and Romain Marignier. Visual outcomes following plasma exchange for optic neuritis: an international multicenter retrospective analysis of 395 optic neuritis attacks. American Journal of Ophthalmology, 252:213-224, Aug 2023. URL: https://doi.org/10.1016/j.ajo.2023.02.013, doi:10.1016/j.ajo.2023.02.013. This article has 78 citations and is from a domain leading peer-reviewed journal.
-
(chen2023visualoutcomesfollowing media 1c706b2b): John J. Chen, Eoin P. Flanagan, Sean J. Pittock, Nicole Caroline Stern, Nanthaya Tisavipat, M. Tariq Bhatti, Kevin D. Chodnicki, Deena A. Tajfirouz, Sepideh Jamali, Amy Kunchok, Eric R. Eggenberger, Marie A. Di Nome, Elias S. Sotirchos, Eleni S. Vasileiou, Amanda D. Henderson, Anthony C. Arnold, Laura Bonelli, Heather E. Moss, Sylvia Elizabeth Villarreal Navarro, Tanyatuth Padungkiatsagul, Hadas Stiebel-Kalish, Itay Lotan, Adi Wilf-Yarkoni, Helen Danesh-Meyer, Stefan Ivanov, Saif Huda, Mirasol Forcadela, David Hodge, Pascale Poullin, Julie Rode, Caroline Papeix, Samir Saheb, Marine Boudot de la Motte, Catherine Vignal, Yael Hacohen, Julie Pique, Elisabeth Maillart, Romain Deschamps, Bertrand Audoin, and Romain Marignier. Visual outcomes following plasma exchange for optic neuritis: an international multicenter retrospective analysis of 395 optic neuritis attacks. American Journal of Ophthalmology, 252:213-224, Aug 2023. URL: https://doi.org/10.1016/j.ajo.2023.02.013, doi:10.1016/j.ajo.2023.02.013. This article has 78 citations and is from a domain leading peer-reviewed journal.
-
(spillers2024acomparativereview pages 6-7): Noah J Spillers, Patrick M Luther, Norris C Talbot, Evan J Kidder, Connor A Doyle, Salim C Lutfallah, Alyssa G Derouen, Sridhar Tirumala, Shahab Ahmadzadeh, Sahar Shekoohi, Alan D Kaye, and Giustino Varrassi. A comparative review of typical and atypical optic neuritis: advancements in treatments, diagnostics, and prognosis. Cureus, Mar 2024. URL: https://doi.org/10.7759/cureus.56094, doi:10.7759/cureus.56094. This article has 11 citations.
-
(chen2023visualoutcomesfollowing pages 6-8): John J. Chen, Eoin P. Flanagan, Sean J. Pittock, Nicole Caroline Stern, Nanthaya Tisavipat, M. Tariq Bhatti, Kevin D. Chodnicki, Deena A. Tajfirouz, Sepideh Jamali, Amy Kunchok, Eric R. Eggenberger, Marie A. Di Nome, Elias S. Sotirchos, Eleni S. Vasileiou, Amanda D. Henderson, Anthony C. Arnold, Laura Bonelli, Heather E. Moss, Sylvia Elizabeth Villarreal Navarro, Tanyatuth Padungkiatsagul, Hadas Stiebel-Kalish, Itay Lotan, Adi Wilf-Yarkoni, Helen Danesh-Meyer, Stefan Ivanov, Saif Huda, Mirasol Forcadela, David Hodge, Pascale Poullin, Julie Rode, Caroline Papeix, Samir Saheb, Marine Boudot de la Motte, Catherine Vignal, Yael Hacohen, Julie Pique, Elisabeth Maillart, Romain Deschamps, Bertrand Audoin, and Romain Marignier. Visual outcomes following plasma exchange for optic neuritis: an international multicenter retrospective analysis of 395 optic neuritis attacks. American Journal of Ophthalmology, 252:213-224, Aug 2023. URL: https://doi.org/10.1016/j.ajo.2023.02.013, doi:10.1016/j.ajo.2023.02.013. This article has 78 citations and is from a domain leading peer-reviewed journal.
-
(spillers2024acomparativereview pages 8-9): Noah J Spillers, Patrick M Luther, Norris C Talbot, Evan J Kidder, Connor A Doyle, Salim C Lutfallah, Alyssa G Derouen, Sridhar Tirumala, Shahab Ahmadzadeh, Sahar Shekoohi, Alan D Kaye, and Giustino Varrassi. A comparative review of typical and atypical optic neuritis: advancements in treatments, diagnostics, and prognosis. Cureus, Mar 2024. URL: https://doi.org/10.7759/cureus.56094, doi:10.7759/cureus.56094. This article has 11 citations.