Fragile X-Associated Tremor Ataxia Syndrome
Fragile X-associated tremor/ataxia syndrome (FXTAS) is a late-onset, progressive neurodegenerative disorder of FMR1 premutation carriers (55-200 CGG repeats in the FMR1 5' UTR). It is mechanistically and clinically distinct from full-mutation fragile X syndrome: rather than FMR1 silencing and FMRP loss, FXTAS is driven by an RNA toxic gain-of-function from elevated CGG-repeat FMR1 mRNA (sequestration of RNA-binding proteins) together with repeat-associated non-AUG (RAN) translation that produces a toxic polyglycine protein, FMRpolyG. The neuropathological hallmark is ubiquitin-positive intranuclear inclusions in neurons and astrocytes. Core clinical features are adult-onset intention/action tremor and cerebellar gait ataxia, with parkinsonism, executive dysfunction and dementia, peripheral neuropathy, and dysautonomia; the radiologic hallmark is increased T2 signal in the middle cerebellar peduncles (the MCP sign).
Ask OpenScientist
Ask a research question about Fragile X-Associated Tremor Ataxia Syndrome. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Inheritance
1Show evidence (2 references)
Mechanistic Hypotheses
1Show evidence (2 references)
Pathophysiology
9Show evidence (2 references)
Show evidence (2 references)
Show evidence (3 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Pathograph
Phenotypes
10Nervous System 8
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Other 2
Show evidence (1 reference)
Show evidence (1 reference)
Genetic Associations
1Show evidence (2 references)
Medical Actions
5Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Clinical Trials
2Show evidence (1 reference)
Show evidence (1 reference)
Source YAML
click to showname: Fragile X-Associated Tremor Ataxia Syndrome
creation_date: "2026-06-04T12:00:00Z"
category: Mendelian
parents:
- Trinucleotide Repeat Disorder
- X-linked Cerebellar Ataxia
description: >-
Fragile X-associated tremor/ataxia syndrome (FXTAS) is a late-onset, progressive
neurodegenerative disorder of FMR1 premutation carriers (55-200 CGG repeats in the
FMR1 5' UTR). It is mechanistically and clinically distinct from full-mutation fragile
X syndrome: rather than FMR1 silencing and FMRP loss, FXTAS is driven by an RNA
toxic gain-of-function from elevated CGG-repeat FMR1 mRNA (sequestration of
RNA-binding proteins) together with repeat-associated non-AUG (RAN) translation that
produces a toxic polyglycine protein, FMRpolyG. The neuropathological hallmark is
ubiquitin-positive intranuclear inclusions in neurons and astrocytes. Core clinical
features are adult-onset intention/action tremor and cerebellar gait ataxia, with
parkinsonism, executive dysfunction and dementia, peripheral neuropathy, and
dysautonomia; the radiologic hallmark is increased T2 signal in the middle cerebellar
peduncles (the MCP sign).
disease_term:
preferred_term: Fragile X-Associated Tremor Ataxia Syndrome
term:
id: MONDO:0010382
label: fragile X-associated tremor/ataxia syndrome
inheritance:
- name: X-linked inheritance
inheritance_term:
preferred_term: X-linked inheritance
term:
id: HP:0001417
label: X-linked inheritance
description: >-
FXTAS is transmitted in an X-linked manner via FMR1 premutation alleles, with
age-dependent reduced penetrance. Penetrance is higher among hemizygous male
carriers (~40% of males >50) than heterozygous female carriers (~16-20%).
evidence:
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "FMR1 disorders are inherited in an X-linked manner."
explanation: GeneReviews establishes X-linked inheritance for FMR1 disorders, including FXTAS.
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "Age of onset is typically between 60 and 65 years and is more common among males who are hemizygous for the premutation (40%) than among females who are heterozygous for the premutation (16%-20%)."
explanation: GeneReviews documents the sex-differential, age-dependent penetrance of FXTAS among premutation carriers.
mechanistic_hypotheses:
- hypothesis_group_id: canonical_fmr1_premutation_rna_gof_ran_translation_model
hypothesis_label: Canonical FMR1 Premutation RNA Gain-of-Function / RAN-Translation (FMRpolyG) Model
status: CANONICAL
description: >-
FXTAS arises from a 55-200 CGG repeat premutation expansion in the FMR1 5' UTR.
Unlike the full mutation (which silences FMR1 and causes fragile X syndrome via
FMRP loss), the premutation is transcribed at elevated levels and is pathogenic
through two non-exclusive gain-of-function routes: (1) RNA toxicity, in which the
expanded CGG-repeat FMR1 mRNA sequesters CGG-repeat-binding proteins (e.g., Pur
alpha, hnRNP A2/B1) into RNA foci, depleting them from their normal functions; and
(2) repeat-associated non-AUG (RAN) translation, which produces a toxic polyglycine
protein, FMRpolyG, that drives ubiquitin-proteasome system impairment. These
converge on ubiquitin-positive intranuclear inclusions in neurons and astrocytes,
proteostasis/autophagy failure, mitochondrial dysfunction and oxidative stress, and
glial/white-matter disruption, culminating in cerebellar and fronto-subcortical
circuit degeneration.
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The pathogenic mechanism is related to overexpression and toxicity of the FMR1 mRNA per se."
explanation: The landmark clinical/genetics review establishes the FMR1 mRNA toxic gain-of-function as the core mechanism distinguishing FXTAS from fragile X syndrome.
- reference: PMID:25954027
reference_title: "RAN translation at CGG repeats induces ubiquitin proteasome system impairment in models of fragile X-associated tremor ataxia syndrome."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "the repeat also elicits production of a toxic polyglycine protein, FMRpolyG, via repeat-associated non-AUG (RAN)-initiated translation"
explanation: This adds RAN translation of FMRpolyG as a parallel toxic gain-of-function arm of the canonical model.
pathophysiology:
- name: FMR1 premutation CGG expansion and elevated FMR1 mRNA
description: >-
The initiating lesion is a premutation-range (55-200 CGG) trinucleotide repeat
expansion in the FMR1 5' UTR. In contrast to the full mutation, the premutation
allele is not silenced; it is transcribed at elevated levels, producing an
expanded CGG-repeat FMR1 mRNA that is the substrate for downstream RNA toxicity
and RAN translation. Human postmortem single-nucleus RNA-seq shows the magnitude
of FMR1 upregulation in brain is more modest (~1.3-fold in some glia) than the
4-8-fold reported in peripheral blood, implicating tissue- and cell-type-specific
toxicity.
gene:
preferred_term: FMR1
modifier: INCREASED
term:
id: hgnc:3775
label: FMR1
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
- preferred_term: glial cell
term:
id: CL:0000125
label: glial cell
biological_processes:
- preferred_term: gene expression
term:
id: GO:0010467
label: gene expression
modifier: INCREASED
downstream:
- target: RNA toxic gain-of-function and protein sequestration
causal_link_type: DIRECT
description: >-
Elevated expanded-repeat FMR1 mRNA forms RNA foci that sequester
CGG-repeat-binding proteins, initiating RNA gain-of-function toxicity.
- target: RAN translation and FMRpolyG production
causal_link_type: DIRECT
description: >-
The expanded CGG repeat is a substrate for repeat-associated non-AUG (RAN)
translation, producing the toxic polyglycine protein FMRpolyG.
- target: Glial and oligodendrocyte dysregulation
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
description: >-
Premutation-range FMR1 expansion and elevated FMR1 mRNA drive cell-type- and
region-specific glial and oligodendrocyte-lineage transcriptional dysregulation,
an upstream facet of premutation brain pathophysiology.
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "FXTAS is caused by moderate expansions (55-200 repeats; premutation range) of a CGG trinucleotide in the fragile X mental retardation 1 (FMR1) gene, the same gene which causes fragile X syndrome when in the full mutation range (200 or greater CGG repeats)."
explanation: Establishes the premutation-range CGG expansion in FMR1 as the causal genetic lesion of FXTAS, distinct from the full mutation.
- reference: PMID:37252957
reference_title: "Glial dysregulation in the human brain in fragile X-associated tremor/ataxia syndrome."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "We found only modest upregulation (~1.3-fold) of FMR1 in some glial populations associated with premutation expansions."
explanation: Human brain single-nucleus RNA-seq quantifies the modest tissue-level FMR1 upregulation, refining the RNA-overexpression model.
- name: RNA toxic gain-of-function and protein sequestration
description: >-
The expanded CGG-repeat FMR1 mRNA forms nuclear RNA foci that bind and sequester
specific RNA-binding proteins, including Pur alpha and hnRNP A2/B1, away from their
normal functions. In a Drosophila model, transcribed premutation repeats alone are
sufficient to cause neurodegeneration, and Pur alpha overexpression suppresses this
toxicity, supporting a sequestration mechanism. Pur alpha is also found within the
intranuclear inclusions of FXTAS patient brains.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
biological_processes:
- preferred_term: protein-RNA complex assembly (RNA foci sequestering RNA-binding proteins)
term:
id: GO:0022618
label: protein-RNA complex assembly
modifier: INCREASED
downstream:
- target: Ubiquitin-positive intranuclear inclusion formation
causal_link_type: INDIRECT_KNOWN_INTERMEDIATES
intermediate_mechanisms:
- RNA foci formation
- Sequestration of RNA-binding proteins
description: >-
Sequestered proteins and dysregulated proteostasis contribute to the formation
of intranuclear inclusions.
- target: Mitochondrial dysfunction and oxidative stress
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
description: >-
Expanded FMR1 mRNA toxicity is associated with downstream mitochondrial
dysfunction and oxidative stress, amplifying neuronal injury.
- target: Neurodegeneration and neuronal cell death
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
description: >-
Loss of normal function of sequestered RNA-binding proteins contributes to
neuronal dysfunction and death.
evidence:
- reference: PMID:17698009
reference_title: "Pur alpha binds to rCGG repeats and modulates repeat-mediated neurodegeneration in a Drosophila model of fragile X tremor/ataxia syndrome."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "transcribed premutation repeats alone are sufficient to cause neurodegeneration, suggesting that rCGG-repeat-binding proteins (RBPs) may be sequestered from their normal function by rCGG binding"
explanation: The Drosophila model directly supports RNA gain-of-function via sequestration of RNA-binding proteins as a driver of neurodegeneration.
- reference: PMID:17698009
reference_title: "Pur alpha binds to rCGG repeats and modulates repeat-mediated neurodegeneration in a Drosophila model of fragile X tremor/ataxia syndrome."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "Overexpression of Pur alpha in Drosophila could suppress rCGG-mediated neurodegeneration in a dose-dependent manner. Furthermore, Pur alpha is also present in the inclusions of FXTAS patient brains."
explanation: Identifies Pur alpha as a sequestered RNA-binding protein whose restoration rescues toxicity and which co-localizes with FXTAS inclusions.
- name: RAN translation and FMRpolyG production
description: >-
The expanded CGG repeat undergoes repeat-associated non-AUG (RAN) translation,
generating a toxic polyglycine-containing protein, FMRpolyG. FMRpolyG accumulates
within the characteristic intranuclear inclusions and impairs the
ubiquitin-proteasome system. In cell models, driving FMRpolyG expression enhances
UPS impairment, whereas preventing RAN translation attenuates it.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
biological_processes:
- preferred_term: translation
term:
id: GO:0006412
label: translation
modifier: INCREASED
downstream:
- target: Ubiquitin-proteasome system and autophagy impairment
causal_link_type: DIRECT
description: >-
FMRpolyG impairs the ubiquitin-proteasome system and contributes to proteostasis
failure.
- target: Ubiquitin-positive intranuclear inclusion formation
causal_link_type: DIRECT
description: >-
FMRpolyG accumulates within the ubiquitin-positive intranuclear inclusions that
define FXTAS neuropathology.
evidence:
- reference: PMID:25954027
reference_title: "RAN translation at CGG repeats induces ubiquitin proteasome system impairment in models of fragile X-associated tremor ataxia syndrome."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "In transfected mammalian cells, CGG repeat expression triggered accumulation of a UPS reporter in a length-dependent fashion."
explanation: Cell-based data show CGG-repeat expression impairs the ubiquitin-proteasome system in a length-dependent manner.
- reference: PMID:25954027
reference_title: "RAN translation at CGG repeats induces ubiquitin proteasome system impairment in models of fragile X-associated tremor ataxia syndrome."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "In Drosophila, ubiquitin proteasome system (UPS) impairment led to enhancement of CGG-repeat-induced degeneration, whereas overexpression of the chaperone protein HSP70 suppressed this toxicity."
explanation: The Drosophila model demonstrates a genetic interaction between UPS impairment and CGG-repeat toxicity, supporting proteostasis failure as a driver of degeneration.
- reference: PMID:26060190
reference_title: "Reversibility of neuropathology and motor deficits in an inducible mouse model for FXTAS."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "8 weeks of dox exposure was sufficient to induce the formation of ubiquitin-positive intranuclear inclusions, which also stain positive for the RAN translation product FMRpolyG."
explanation: An inducible mouse model confirms FMRpolyG is a component of the FXTAS-type ubiquitin-positive intranuclear inclusions.
- name: Ubiquitin-proteasome system and autophagy impairment
description: >-
FXTAS inclusions are enriched for components of the protein-degradation machinery.
Nearly 200 proteins have been identified in FXTAS inclusions, with SUMO2, ubiquitin,
and p62/SQSTM1 among the most abundant. Postmortem FXTAS brains are positive for
SUMO2/3 conjugates and show transcriptional upregulation of SUMOylation, while
patient fibroblasts accumulate p62 and autophagosomes with downregulation of
autophagy-related gene-ontology terms, indicating impaired autophagic flux.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
- preferred_term: astrocyte
term:
id: CL:0000127
label: astrocyte
biological_processes:
- preferred_term: ubiquitin-dependent protein catabolic process
term:
id: GO:0006511
label: ubiquitin-dependent protein catabolic process
modifier: DECREASED
- preferred_term: protein sumoylation
term:
id: GO:0016925
label: protein sumoylation
modifier: INCREASED
- preferred_term: autophagy
term:
id: GO:0006914
label: autophagy
modifier: DECREASED
downstream:
- target: Ubiquitin-positive intranuclear inclusion formation
causal_link_type: DIRECT
description: >-
Failure of proteostasis and autophagy promotes accumulation of misfolded and
modified proteins into intranuclear inclusions.
evidence:
- reference: PMID:37830578
reference_title: "Exploration of SUMO2/3 Expression Levels and Autophagy Process in Fragile X-Associated Tremor/Ataxia Syndrome."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Nearly 200 different proteins have been identified in FXTAS inclusions, being the small ubiquitin-related modifier 2 (SUMO2), ubiquitin and p62 the most highly abundant."
explanation: Identifies the protein-degradation-machinery composition of FXTAS inclusions, supporting proteostasis dysfunction.
- reference: PMID:37830578
reference_title: "Exploration of SUMO2/3 Expression Levels and Autophagy Process in Fragile X-Associated Tremor/Ataxia Syndrome."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "the analysis of the autophagy flux showed the accumulation of p62 protein levels and autophagosomes in skin fibroblasts from FXTAS patients. Similarly, gene set analysis evidenced a significant downregulation in gene ontology terms related to autophagy in FXTAS samples."
explanation: Patient fibroblast and transcriptomic data support impaired autophagic flux as part of FXTAS proteostasis failure.
- name: Mitochondrial dysfunction and oxidative stress
description: >-
Mitochondrial dysfunction is a convergent downstream mechanism in FXTAS, including
impaired mitochondrial protein import, altered morphology, disrupted calcium
handling, reduced respiratory-chain activity, and elevated reactive oxygen species
with lipid peroxidation and protein carbonylation. These changes amplify neuronal
injury and have motivated antioxidant and mitochondrial-nutrient therapeutic
strategies.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
- preferred_term: astrocyte
term:
id: CL:0000127
label: astrocyte
biological_processes:
- preferred_term: response to oxidative stress
term:
id: GO:0006979
label: response to oxidative stress
modifier: INCREASED
- preferred_term: mitochondrion organization
term:
id: GO:0007005
label: mitochondrion organization
modifier: ABNORMAL
downstream:
- target: Neurodegeneration and neuronal cell death
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
description: >-
Oxidative stress and bioenergetic failure contribute to progressive neuronal
injury and death.
evidence:
- reference: PMID:38578387
reference_title: "Mitochondrial dysfunction in Fragile X syndrome and Fragile X-associated tremor/ataxia syndrome."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "FXTAS is associated with elevated levels of FMR1 mRNA, leading to neurodegenerative manifestations such as tremors and ataxia.Mounting evidence suggests a link between both syndromes and mitochondrial dysfunction (MDF)."
explanation: This minireview links the FMR1 premutation mRNA toxicity in FXTAS to mitochondrial dysfunction as a downstream mechanism.
- name: Glial and oligodendrocyte dysregulation
description: >-
Human postmortem single-nucleus RNA-seq of frontal cortex and cerebellum implicates
glial dysregulation as a critical, upstream facet of premutation pathophysiology,
with cell-type- and region-specific dysregulation of FMR1 protein-target gene
networks, decreased cortical astrocyte proportions, and notable perturbation of the
cortical oligodendrocyte lineage, consistent with the white-matter pathology seen
radiologically.
cell_types:
- preferred_term: oligodendrocyte
term:
id: CL:0000128
label: oligodendrocyte
- preferred_term: astrocyte
term:
id: CL:0000127
label: astrocyte
biological_processes:
- preferred_term: oligodendrocyte differentiation
term:
id: GO:0048709
label: oligodendrocyte differentiation
modifier: ABNORMAL
- preferred_term: myelination
term:
id: GO:0042552
label: myelination
modifier: ABNORMAL
downstream:
- target: White matter disease and middle cerebellar peduncle pathology
causal_link_type: INDIRECT_KNOWN_INTERMEDIATES
intermediate_mechanisms:
- Oligodendrocyte-lineage transcriptional dysregulation
- Impaired myelination
description: >-
Glial and oligodendrocyte dysregulation contributes to the white-matter disease
that is characteristic of FXTAS.
evidence:
- reference: PMID:37252957
reference_title: "Glial dysregulation in the human brain in fragile X-associated tremor/ataxia syndrome."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "we identified cell type-specific and region-specific patterns of FMR1 protein target gene dysregulation unique to premutation cases, with notable network dysregulation in the cortical oligodendrocyte lineage."
explanation: Human brain transcriptomics implicate oligodendrocyte-lineage glial dysregulation as central to premutation pathophysiology and white-matter disease.
- name: Ubiquitin-positive intranuclear inclusion formation
description: >-
The defining neuropathological feature of FXTAS is the presence of ubiquitin-positive
intranuclear inclusions in neurons and astrocytes in broad distribution throughout
the brain and brainstem. Inclusions contain ubiquitin, SUMO2, p62, FMRpolyG, and
sequestered RNA-binding proteins, representing the convergence of RNA toxicity, RAN
translation, and proteostasis failure.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
- preferred_term: astrocyte
term:
id: CL:0000127
label: astrocyte
biological_processes:
- preferred_term: inclusion body assembly
term:
id: GO:0070841
label: inclusion body assembly
modifier: INCREASED
downstream:
- target: Neurodegeneration and neuronal cell death
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
description: >-
Inclusion formation accompanies and marks progressive neuronal dysfunction and
degeneration.
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The major neuropathological feature of FXTAS is the presence of intranuclear, neuronal, and astrocytic, inclusions in broad distribution throughout the brain and brainstem."
explanation: Establishes intranuclear neuronal and astrocytic inclusions as the defining FXTAS neuropathology.
- name: White matter disease and middle cerebellar peduncle pathology
description: >-
FXTAS produces progressive cerebral and cerebellar white-matter disease. The
radiologic hallmark is increased T2 signal in the middle cerebellar peduncles (the
MCP sign), with similar signal change in deep and subependymal cerebral white matter
and general cortical and subcortical atrophy.
cell_types:
- preferred_term: oligodendrocyte
term:
id: CL:0000128
label: oligodendrocyte
biological_processes:
- preferred_term: myelination
term:
id: GO:0042552
label: myelination
modifier: DECREASED
downstream:
- target: Neurodegeneration and neuronal cell death
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
description: >-
White-matter disease and cerebellar peduncle pathology underlie the cerebellar
and fronto-subcortical circuit dysfunction producing FXTAS symptoms.
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Magnetic Resonance Imaging studies in FXTAS demonstrate increased T2 signal intensity in the middle cerebellar peduncles (MCP sign) in the majority of patients."
explanation: Establishes the middle cerebellar peduncle white-matter sign as the radiologic hallmark of FXTAS.
- name: Neurodegeneration and neuronal cell death
description: >-
The convergent mechanisms of RNA toxicity, RAN-translated FMRpolyG, proteostasis and
autophagy failure, mitochondrial dysfunction, and glial/white-matter disruption
culminate in cerebellar and fronto-subcortical neurodegeneration that produces the
clinical syndrome of progressive tremor, ataxia, parkinsonism, cognitive decline,
neuropathy, and dysautonomia.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
- preferred_term: Purkinje cell
term:
id: CL:0000121
label: Purkinje cell
biological_processes:
- preferred_term: positive regulation of neuron apoptotic process
term:
id: GO:0043525
label: positive regulation of neuron apoptotic process
modifier: INCREASED
downstream:
- target: Intention/Action Tremor
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
description: Cerebellar circuit degeneration produces the characteristic intention/action tremor.
- target: Cerebellar Gait Ataxia
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
description: Cerebellar degeneration produces progressive gait ataxia.
- target: Cognitive Decline and Dementia
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
description: Fronto-subcortical degeneration produces executive dysfunction and dementia.
evidence:
- reference: PMID:26060190
reference_title: "Reversibility of neuropathology and motor deficits in an inducible mouse model for FXTAS."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "FXTAS is characterized by progressive development of intention tremor, ataxia, parkinsonism and neuropsychological problems. The disease is thought to be caused by a toxic RNA gain-of-function mechanism, and the major hallmark of the disease is ubiquitin-positive intranuclear inclusions in neurons and astrocytes."
explanation: Links the toxic gain-of-function mechanism and inclusion neuropathology to the progressive neurodegenerative clinical syndrome.
phenotypes:
- name: Intention/Action Tremor
category: Neurological
diagnostic: true
description: >-
Intention and action (kinetic) tremor is a core motor feature and usually the first
major motor symptom of FXTAS, with median onset around age 60 in male carriers.
phenotype_term:
preferred_term: Intention tremor
clinical_course: PROGRESSIVE
term:
id: HP:0002080
label: Intention tremor
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Fragile X-associated tremor/ataxia syndrome (FXTAS) is a neurodegenerative disorder with core features of action tremor and cerebellar gait ataxia."
explanation: Establishes action/intention tremor as a defining core feature of FXTAS.
- reference: PMID:17133502
reference_title: "Progression of tremor and ataxia in male carriers of the FMR1 premutation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "tremor usually occurs first, with median onset at approximately 60 years of age."
explanation: Supports tremor as the typically first motor sign with adult-onset timing.
- name: Cerebellar Gait Ataxia
category: Neurological
diagnostic: true
description: >-
Progressive cerebellar gait ataxia is a core sign of FXTAS, typically following
tremor and leading to imbalance, falls, and eventual walking-aid dependence.
phenotype_term:
preferred_term: Gait ataxia
clinical_course: PROGRESSIVE
term:
id: HP:0002066
label: Gait ataxia
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Fragile X-associated tremor/ataxia syndrome (FXTAS) is a neurodegenerative disorder with core features of action tremor and cerebellar gait ataxia."
explanation: Establishes cerebellar gait ataxia as a defining core feature of FXTAS.
- reference: PMID:17133502
reference_title: "Progression of tremor and ataxia in male carriers of the FMR1 premutation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "From the onset of the initial motor sign, median delay of onset of ataxia was 2 years; onset of falls, 6 years; dependence on a walking aid, 15 years"
explanation: Documents the progressive course of ataxia and falls in FXTAS.
- name: Parkinsonism
category: Neurological
description: >-
Parkinsonian features (bradykinesia, rigidity, rest tremor) occur in roughly a third
of FXTAS patients and contribute to the differential diagnosis with Parkinson disease
and multiple system atrophy.
phenotype_term:
preferred_term: Parkinsonism
term:
id: HP:0001300
label: Parkinsonism
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Frequent associated findings include parkinsonism, executive function deficits and dementia, neuropathy, and dysautonomia."
explanation: Lists parkinsonism as a frequent associated finding in FXTAS.
- name: Cognitive Decline and Dementia
category: Neurological
description: >-
FXTAS produces a progressive fronto-subcortical cognitive disorder; a substantial
proportion of affected males develop frontal-subcortical dementia/major
neurocognitive disorder.
phenotype_term:
preferred_term: Dementia
clinical_course: PROGRESSIVE
term:
id: HP:0000726
label: Dementia
evidence:
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "FXTAS occurs in individuals who have an FMR1 premutation and is characterized by late-onset, progressive cerebellar ataxia and intention tremor followed by cognitive impairment."
explanation: GeneReviews documents progressive cognitive impairment following the motor syndrome in FXTAS.
- reference: PMID:41940304
reference_title: "Comprehensive, multidisciplinary care for fragile X-associated tremor/ataxia syndrome."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Patients often develop fronto-subcortical dementia/major neurocognitive disorder (MNCD), leading to significant functional decline (particularly in males)."
explanation: Supports progression to fronto-subcortical dementia/major neurocognitive disorder in FXTAS.
- name: Executive Dysfunction
category: Neurological
description: >-
Executive function deficits are a characteristic cognitive feature of FXTAS and a
minor diagnostic criterion, reflecting fronto-subcortical involvement.
phenotype_term:
preferred_term: Impaired executive functioning
term:
id: HP:0033051
label: Impaired executive functioning
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Frequent associated findings include parkinsonism, executive function deficits and dementia, neuropathy, and dysautonomia."
explanation: Lists executive function deficits as a frequent associated finding in FXTAS.
- name: Peripheral Neuropathy
category: Neurological
description: >-
Peripheral neuropathy with distal sensory loss, reduced reflexes, and impaired
vibration sense is a frequent associated finding; lower-extremity neuropathy is a
minor diagnostic criterion.
phenotype_term:
preferred_term: Peripheral neuropathy
term:
id: HP:0009830
label: Peripheral neuropathy
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Frequent associated findings include parkinsonism, executive function deficits and dementia, neuropathy, and dysautonomia."
explanation: Lists neuropathy as a frequent associated finding in FXTAS.
- name: Impaired Vibratory Sensation
category: Neurological
description: >-
Reduced vibration sense in the lower extremities is a common sensory manifestation of
the FXTAS peripheral neuropathy.
phenotype_term:
preferred_term: Impaired vibratory sensation
term:
id: HP:0002495
label: Impaired vibratory sensation
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Frequent associated findings include parkinsonism, executive function deficits and dementia, neuropathy, and dysautonomia."
explanation: The FXTAS-associated neuropathy includes distal sensory deficits such as impaired vibration sense; this item is scoped under the documented neuropathy finding.
- name: Dysautonomia
category: Neurological
description: >-
Autonomic dysfunction is a frequent associated finding in FXTAS, including orthostatic
hypotension, erectile dysfunction, and progressive bowel/bladder dysfunction.
phenotype_term:
preferred_term: Abnormal autonomic nervous system physiology
term:
id: HP:0012332
label: Abnormal autonomic nervous system physiology
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Frequent associated findings include parkinsonism, executive function deficits and dementia, neuropathy, and dysautonomia."
explanation: Lists dysautonomia as a frequent associated finding in FXTAS; manifestations include orthostatic hypotension, erectile dysfunction, and bowel/bladder dysfunction.
- name: Psychiatric Symptoms
category: Behavioral
description: >-
Psychiatric disorders are common in FXTAS and premutation carriers, including
depression, anxiety, irritability, and apathy; neuropsychiatric features may precede
the overt motor syndrome, especially in female carriers.
phenotype_term:
preferred_term: Depression
term:
id: HP:0000716
label: Depression
evidence:
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "Psychiatric disorders are common."
explanation: GeneReviews documents psychiatric disorders as common in FXTAS.
- name: White Matter Hyperintensities (MCP Sign)
category: Neurological
diagnostic: true
description: >-
The radiologic hallmark of FXTAS is increased T2 signal in the middle cerebellar
peduncles (the MCP sign) on brain MRI, with similar signal change in deep and
subependymal cerebral white matter and accompanying cortical/subcortical atrophy.
phenotype_term:
preferred_term: Middle cerebellar peduncle and cerebral white matter T2/FLAIR hyperintensity (MCP sign)
clinical_course: PROGRESSIVE
term:
id: HP:0030890
label: Hyperintensity of cerebral white matter on MRI
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Similar signal alterations are seen in deep and subependymal cerebral white matter, as is general cortical and subcortical atrophy."
explanation: Documents the cerebral white-matter signal hyperintensity (alongside the MCP sign) that is the radiologic hallmark of FXTAS.
genetic:
- name: FMR1
gene_term:
preferred_term: FMR1
term:
id: hgnc:3775
label: FMR1
association: Causative premutation CGG repeat expansion (55-200 repeats)
relationship_type: CAUSATIVE
variant_origin: GERMLINE
notes: >-
FXTAS is caused by a premutation-range CGG repeat expansion (55-200 repeats) in the
FMR1 5' UTR. Unlike the full mutation (>200 repeats) that silences FMR1 and causes
fragile X syndrome, the premutation allele is expressed at elevated levels and is
pathogenic via RNA toxic gain-of-function and RAN translation of FMRpolyG.
variants:
- name: FMR1 premutation CGG repeat expansion
description: >-
Premutation-range expansion of the FMR1 5' UTR CGG repeat to 55-200 repeats,
producing elevated expanded-repeat FMR1 mRNA with toxic gain-of-function and RAN
translation rather than gene silencing.
gene:
preferred_term: FMR1
term:
id: hgnc:3775
label: FMR1
type: trinucleotide repeat expansion
clinical_significance: PATHOGENIC
evidence:
- reference: PMID:17618523
reference_title: "Fragile X-associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "FXTAS is caused by moderate expansions (55-200 repeats; premutation range) of a CGG trinucleotide in the fragile X mental retardation 1 (FMR1) gene, the same gene which causes fragile X syndrome when in the full mutation range (200 or greater CGG repeats)."
explanation: Establishes FMR1 premutation CGG expansion as the causal variant class of FXTAS, distinct from the full mutation.
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "the diagnosis of FXTAS or FXPOI is associated with a premutation-sized repeat (55-200 CGG repeats)."
explanation: GeneReviews confirms the premutation-sized (55-200 CGG) repeat as the FXTAS-associated allele class.
prevalence:
- population: FMR1 premutation carriers (general population)
notes: >-
FXTAS occurs specifically in FMR1 premutation carriers; not all carriers develop
FXTAS. General-population premutation carrier frequency is commonly cited as
roughly 1 in 250-300 females and 1 in 800 males, but a quantitative source is not
cited here for those specific figures.
evidence:
- reference: PMID:41940304
reference_title: "Comprehensive, multidisciplinary care for fragile X-associated tremor/ataxia syndrome."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "a neurodegenerative disorder affecting FMR1 premutation carriers (55-200 CCG repeats)"
explanation: Confirms FXTAS occurs specifically in FMR1 premutation carriers.
- population: Male premutation carriers over age 50
percentage: "~40%"
notes: >-
Age-dependent penetrance of FXTAS is higher in male (40%) than female (16-20%)
premutation carriers (GeneReviews).
evidence:
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "more common among males who are hemizygous for the premutation (40%) than among females who are heterozygous for the premutation (16%-20%)."
explanation: GeneReviews documents the higher FXTAS penetrance in male than female premutation carriers.
progression:
- phase: Onset
age_range: Typically age 60-65 (after age 50)
notes: >-
FXTAS is a late-onset disorder; tremor usually appears first, with median onset
around age 60 in male carriers.
evidence:
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "Age of onset is typically between 60 and 65 years"
explanation: GeneReviews documents the late-adult typical age of onset of FXTAS.
- reference: PMID:17133502
reference_title: "Progression of tremor and ataxia in male carriers of the FMR1 premutation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "tremor usually occurs first, with median onset at approximately 60 years of age."
explanation: Cohort natural-history data support tremor as the first motor sign at median age ~60.
- phase: Progression and survival
notes: >-
Median intervals from first motor sign: ataxia 2 years, falls 6 years, walking-aid
dependence 15 years, and death 21 years; reported survival after onset is variable
(5-25 years).
evidence:
- reference: PMID:17133502
reference_title: "Progression of tremor and ataxia in male carriers of the FMR1 premutation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "From the onset of the initial motor sign, median delay of onset of ataxia was 2 years; onset of falls, 6 years; dependence on a walking aid, 15 years; and death, 21 years. Preliminary data on life expectancy are variable, with a range from 5 to 25 years."
explanation: Provides cohort-based progression milestones and survival range for FXTAS.
treatments:
- name: Symptomatic and Supportive Care
description: >-
There is no disease-modifying therapy for FXTAS; management is symptomatic and
supportive, tailored to the individual, and ideally delivered through coordinated
multidisciplinary care.
treatment_term:
preferred_term: supportive care
term:
id: MAXO:0000950
label: supportive care
evidence:
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "FXTAS: symptomatic and supportive and should be tailored to the individual."
explanation: GeneReviews defines FXTAS management as symptomatic and supportive.
- name: Tremor Pharmacotherapy
description: >-
Pharmacologic management of FXTAS tremor commonly uses agents such as primidone,
beta-blockers, and gabapentin/pregabalin.
therapeutic_modality: SMALL_MOLECULE
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
evidence:
- reference: PMID:41940304
reference_title: "Comprehensive, multidisciplinary care for fragile X-associated tremor/ataxia syndrome."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "A holistic, person-centered approach coordinated by the primary care clinician with multispecialty and multidisciplinary collaboration is recommended to address the complex needs of FXTAS patients and their support networks."
explanation: The multidisciplinary care review supports symptomatic pharmacologic and coordinated management of FXTAS, including tremor.
- name: Physical, Occupational, and Speech Therapy
description: >-
Rehabilitation (physical, occupational, and speech-language therapy) supports
mobility, function, fall prevention, and communication as the disorder progresses.
treatment_term:
preferred_term: physical therapy
term:
id: MAXO:0000011
label: physical therapy
evidence:
- reference: PMID:41940304
reference_title: "Comprehensive, multidisciplinary care for fragile X-associated tremor/ataxia syndrome."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "A multispecialty and multidisciplinary team of authors with backgrounds in psychiatry, pediatrics, clinical psychology, speech and language pathology, and neurosciences."
explanation: The review supports a multidisciplinary rehabilitative approach including speech-language pathology for FXTAS.
- name: Genetic Counseling
description: >-
Genetic counseling and cascade testing are recommended once an FMR1 premutation or
other fragile X-associated condition is identified in a family.
treatment_term:
preferred_term: Genetic Counseling
term:
id: NCIT:C15240
label: Genetic Counseling
evidence:
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "Prenatal testing for a pregnancy at increased risk and preimplantation genetic testing are possible once an expanded (or altered) FMR1 allele has been identified in a family member."
explanation: GeneReviews supports genetic counseling and family testing in FMR1 disorders including FXTAS.
- name: Avoidance of Aggravating Agents
description: >-
GeneReviews lists agents/circumstances to avoid in FXTAS: typical and atypical
antipsychotics with significant anti-dopaminergic effects and metoclopramide (can
exacerbate parkinsonism); anticholinergic agents (can exacerbate cognitive
complaints); excessive alcohol (can enhance cerebellar dysfunction and postural
instability); and agents with known cerebellar toxicity.
treatment_term:
preferred_term: supportive care
term:
id: MAXO:0000950
label: supportive care
evidence:
- reference: PMID:20301558
reference_title: "FMR1 Disorders."
supports: SUPPORT
evidence_source: OTHER
snippet: "Agents/circumstances to avoid: FXTAS: typical and atypical antipsychotics with significant anti-dopaminergic effects and metoclopramide, which can exacerbate parkinsonism; anticholinergic agents, which can exacerbate cognitive complaints; excessive alcohol, which can enhance cerebellar dysfunction and postural instability; agents with known cerebellar toxicity or side effects."
explanation: GeneReviews specifies drug-safety warnings (Agents/Circumstances to Avoid) for FXTAS.
clinical_trials:
- name: NCT00584948
phase: PHASE_II
status: COMPLETED
description: >-
Randomized, double-blind, placebo-controlled trial of memantine in FMR1 premutation
carriers with FXTAS, assessing executive function and intention tremor over one year.
target_phenotypes:
- preferred_term: Intention tremor
term:
id: HP:0002080
label: Intention tremor
- preferred_term: Impaired executive functioning
term:
id: HP:0033051
label: Impaired executive functioning
evidence:
- reference: clinicaltrials:NCT00584948
reference_title: "Characterization and Treatment of CNS Abnormalities in Premutation Carriers: A Double-Blind Placebo-Controlled Trial of Memantine"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The purpose of this study is to determine if memantine is effective in treating symptoms of Fragile X-associated Tremor Ataxia Syndrome."
explanation: ClinicalTrials.gov documents the memantine treatment trial in FXTAS.
- name: NCT02603926
phase: PHASE_II
status: COMPLETED
description: >-
Open-label phase 2 trial of intravenous allopregnanolone in FMR1 premutation carriers
with FXTAS, assessing cognitive, tremor, and MRI outcomes.
target_phenotypes:
- preferred_term: Dementia
term:
id: HP:0000726
label: Dementia
evidence:
- reference: clinicaltrials:NCT02603926
reference_title: "Treatment of Fragile-X Associated Tremor/Ataxia Syndrome (FXTAS) With Allopregnanolone"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The purpose of this study is to examine the safety and efficacy of Allopregnanolone as a possible treatment for symptoms of Fragile X-associated Tremor/Ataxia Syndrome (FXTAS)."
explanation: ClinicalTrials.gov documents the allopregnanolone treatment trial in FXTAS.
datasets: []
references:
- reference: PMID:20301558
title: "FMR1 Disorders."
tags:
- GeneReviews
References & Deep Research
References
1Deep Research
1Fragile X–Associated Tremor/Ataxia Syndrome (FXTAS) — Disease Characteristics Research Report
Target Disease
- Disease name: Fragile X–associated tremor/ataxia syndrome (FXTAS)
- Category: Mendelian / repeat-expansion disorder (X-linked; FMR1 premutation)
- MONDO ID: MONDO:0010382 (OpenTargets) (OpenTargets Search: Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS)
Executive overview (current understanding)
FXTAS is a late-onset, progressive neurodegenerative disorder that occurs in carriers of FMR1 premutation alleles and is classically characterized by action/intention tremor and cerebellar gait ataxia, with frequent cognitive decline and neuropsychiatric symptoms. The canonical genetic definition used in clinical trials and reviews is 55–200 CGG repeats in the 5′ untranslated region (5′UTR) of FMR1, with pathogenesis primarily attributed to toxic gain-of-function of elevated FMR1 mRNA and additional contributions from repeat-associated non-AUG (RAN) translation (e.g., FMRpolyG) and downstream proteostasis, mitochondrial, and glial/white-matter dysfunction (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, bourgeois2026comprehensivemultidisciplinarycare pages 1-2, tassone2023insightandrecommendations pages 6-8).
1. Disease information
1.1 Definition / overview
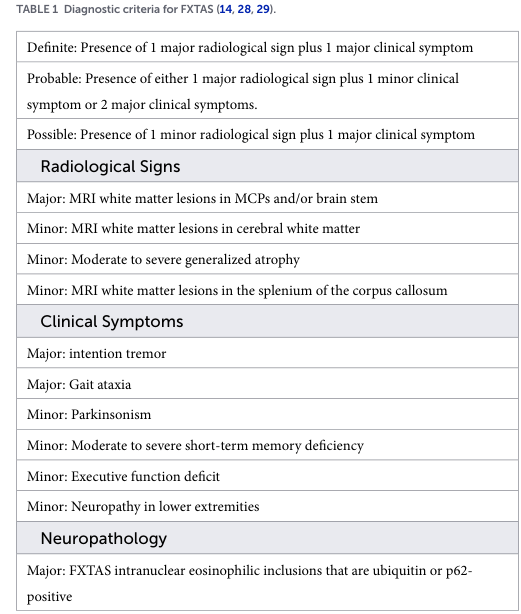
- Landmark clinical/genetic testing guidance describes FXTAS as “a neurodegenerative disorder with core features of action tremor and cerebellar gait ataxia” with frequent associated parkinsonism and executive dysfunction/dementia; MRI often shows the middle cerebellar peduncle (MCP) sign; neuropathology shows ubiquitin-positive intranuclear inclusions in neurons and astrocytes (Berry-Kravis et al., 2007; DOI: https://doi.org/10.1002/mds.21493; Oct 2007) (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8).
1.2 Key identifiers
A structured identifier summary is provided here:
| Identifier system | Identifier/code | Preferred name | Synonyms/aliases | Source URL | Publication date (if source is a paper) | Notes |
|---|---|---|---|---|---|---|
| MONDO | MONDO_0010382 | fragile X-associated tremor/ataxia syndrome | FXTAS; fragile X-associated tremor ataxia syndrome; fragile X tremor ataxia syndrome | https://platform.opentargets.org/disease/MONDO_0010382 | — | Disease identifier and FMR1 association retrieved via OpenTargets disease-target evidence; useful for ontology mapping in knowledge bases (OpenTargets Search: Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS) |
| OMIM | OMIM #300623 | Fragile X-associated tremor/ataxia syndrome | FXTAS | https://omim.org/entry/300623 | 2023 (paper citing OMIM) | OMIM number explicitly stated in 2023 FXTAS papers/reviews: “FXTAS, OMIM# 300623” (eliasmas2023evaluationofaqp4 pages 1-2, alvarezmora2023explorationofsumo23 pages 1-2) |
| MeSH / registry labeling | “Fragile X Tremor Ataxia Syndrome” | Fragile X Tremor Ataxia Syndrome | FXTAS | https://clinicaltrials.gov/study/NCT02936531 | 2016 | MeSH-style disease label present in ClinicalTrials.gov record for BNA/gait-posture study; included as a practical nomenclature source rather than a definitive MeSH browser record (NCT02936531 chunk 2, NCT02936531 chunk 1) |
| Gene (causal) | FMR1 | fragile X messenger ribonucleoprotein 1 | fragile X mental retardation 1; FMR1 premutation gene context | https://platform.opentargets.org/target/ENSG00000102081 | — | Only disease-associated target returned by OpenTargets for FXTAS; premutation range in FXTAS is 55–200 CGG repeats in the 5′ UTR (OpenTargets Search: Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS, berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, bourgeois2026comprehensivemultidisciplinarycare pages 1-2) |
| Variant class | FMR1 premutation, 55–200 CGG repeats | FMR1 premutation-associated FXTAS | premutation carrier state | https://doi.org/10.1002/mds.21493 | 2007 | Canonical molecular definition from landmark review; still used in recent reviews and trial records for diagnosis/testing guidance (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, NCT02936531 chunk 1, bourgeois2026comprehensivemultidisciplinarycare pages 1-2) |
| Disease name (preferred clinical usage) | — | Fragile X-associated tremor/ataxia syndrome | FXTAS | https://doi.org/10.3389/fnagi.2022.1073258 | 2023 | Modern preferred disease name used in recent primary literature and reviews; adult-onset neurodegenerative disorder of FMR1 premutation carriers (eliasmas2023evaluationofaqp4 pages 1-2, dias2023glialdysregulationin pages 1-2) |
| Alternate spelling | — | Fragile-X-associated tremor/ataxia syndrome | Fragile-X associated tremor/ataxia syndrome | https://doi.org/10.3390/ijms26062825 | 2025 | Hyphenated form appears in recent literature; nomenclature variant only, same disease concept (liani2025premutationfemaleswith pages 4-6) |
| Historical/abbreviated disease label | FXTAS | FXTAS | fragile X-associated tremor/ataxia syndrome | https://doi.org/10.3389/fneur.2026.1746002 | 2026 | Widely used abbreviation across clinical reviews, management papers, and trials; recommended to store as exact synonym (bourgeois2026comprehensivemultidisciplinarycare pages 1-2, bourgeois2026comprehensivemultidisciplinarycare pages 6-7) |
Table: This table summarizes key identifiers and naming conventions for fragile X-associated tremor/ataxia syndrome, including ontology and OMIM references plus the causal gene. It is useful for harmonizing disease records across clinical, genomic, and knowledge-base resources.
Notes on missing codes: Orphanet, ICD-10/ICD-11, and an authoritative MeSH-browser identifier were not retrievable from the full-text/trial-record evidence available in this run; these should be added from dedicated ontology services in a separate curation step.
1.3 Synonyms / alternative names
Common synonyms used in the scientific and clinical-trial literature include: - Fragile X tremor ataxia syndrome - Fragile X-associated tremor ataxia syndrome - FXTAS (OpenTargets Search: Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS, NCT02936531 chunk 2).
1.4 Evidence sources (patient-level vs aggregated)
- Aggregated disease resources / reviews: e.g., Movement Disorders testing guidelines (2007) and later expert reviews/consensus statements (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, tassone2023insightandrecommendations pages 6-8).
- Primary human data: postmortem molecular profiling (snRNA-seq) (dias2023glialdysregulationin pages 1-2), postmortem pathology/biochemistry (alvarezmora2023explorationofsumo23 pages 1-2).
- Clinical trial registry records: interventional and observational trial metadata (NCT records) (NCT00584948 chunk 1, NCT02603926 chunk 1).
2. Etiology
2.1 Primary causal factors
- Genetic cause: FXTAS occurs in FMR1 premutation carriers, typically defined as 55–200 CGG repeats in the 5′UTR of FMR1 (Berry-Kravis et al., 2007; DOI: https://doi.org/10.1002/mds.21493) (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2) and reiterated in clinical trial descriptions (NCT02936531 chunk 1).
- Core mechanistic etiology: an early synthesis states “The pathogenic mechanism is related to overexpression and toxicity of the FMR1 mRNA per se.” (Berry-Kravis et al., 2007; DOI: https://doi.org/10.1002/mds.21493) (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2).
2.2 Risk factors
Non-modifiable - Age: typical onset ~60 years in males, later in females; male penetrance rises steeply with age (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, bourgeois2026comprehensivemultidisciplinarycare pages 1-2). - Sex: males are more frequently and more severely affected (bourgeois2026comprehensivemultidisciplinarycare pages 1-2). - Repeat size: higher CGG repeat number is associated with earlier onset in classic clinical synthesis (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2).
Potential genetic modifiers - AQP4 variants: a 2023 case-control modifier study found no significant association between common AQP4 SNPs/haplotypes and FXTAS development in 95 FXTAS vs 65 no-FXTAS premutation carriers (Frontiers in Aging Neuroscience; Jan 2023; DOI: https://doi.org/10.3389/fnagi.2022.1073258) (eliasmas2023evaluationofaqp4 pages 1-2). - Somatic instability / DNA repair genes: A 2023 premutation consensus report highlights somatic expansion processes and notes DNA repair genes such as FAN1 and MSH3 can modify expansion risk in premutation-associated conditions, contributing to phenotypic variability and informing counseling (Cells; Sep 2023; DOI: https://doi.org/10.3390/cells12182330) (tassone2023insightandrecommendations pages 6-8).
Environmental / exposure modifiers (limited evidence in retrieved set) - A multidisciplinary review notes exposures such as excessive alcohol and/or opioids can worsen white-matter hyperintensities (WMH) (bourgeois2026comprehensivemultidisciplinarycare pages 3-4).
2.3 Protective factors
Robust protective factors are not established in the retrieved primary literature. Some experimental/early therapeutic approaches aim to mitigate downstream oxidative/mitochondrial stress (see Treatment section), but these are not proven protective factors at the population level (pagano2024mitochondrialdysfunctionin pages 1-2).
2.4 Gene–environment interactions
Direct gene–environment interaction studies were not present in the retrieved evidence. The available review-level evidence suggests that toxic exposures may exacerbate white matter injury in genetically susceptible premutation carriers (bourgeois2026comprehensivemultidisciplinarycare pages 3-4).
3. Phenotypes
A structured phenotype table with HPO suggestions, onset/course, and numeric notes is provided here:
| Phenotype | HPO term suggestion(s) | Typical onset | Course | Frequency/notes with numeric estimates | Key evidence citation IDs |
|---|---|---|---|---|---|
| Intention/action tremor | HP:0002080 Tremor; HP:0002068 Action tremor; HP:0002345 Intention tremor | Usually adult-onset after age 50; mean onset ~60.2 years in males | Progressive; often first major motor symptom | Core feature of FXTAS; male premutation-carrier penetrance rises with age: 17% (50–59), 38% (60–69), 47% (70–79), 75% (80+); overall ~40% of male carriers >50 affected; female risk lower (~16–20%) (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, NCT02936531 chunk 1, bourgeois2026comprehensivemultidisciplinarycare pages 1-2, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8) | (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, NCT02936531 chunk 1, bourgeois2026comprehensivemultidisciplinarycare pages 1-2, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8) |
| Gait ataxia | HP:0002066 Ataxia; HP:0001288 Gait disturbance; HP:0002317 Unsteady gait | Usually begins after tremor in later adulthood; often around the 60s | Progressive; balance impairment worsens, leading to falls and walking-aid dependence | Major clinical sign in diagnostic criteria; family-based natural history reported median delay from tremor to ataxia of 2 years and to falls of 6 years; progression to walking-aid dependence around 15 years after onset (bourgeois2026comprehensivemultidisciplinarycare pages 3-4, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8) | (bourgeois2026comprehensivemultidisciplinarycare pages 3-4, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8) |
| Parkinsonism | HP:0001300 Parkinsonism; HP:0001336 Bradykinesia; HP:0000736 Rigidity | Later adult onset, usually after tremor/ataxia emerge | Progressive, variable severity | Approximately 30% of FXTAS patients have parkinsonian symptoms; considered a minor clinical criterion and relevant differential with Parkinson disease/MSA-C (bourgeois2026comprehensivemultidisciplinarycare pages 3-4, bourgeois2026comprehensivemultidisciplinarycare pages 4-6) | (bourgeois2026comprehensivemultidisciplinarycare pages 3-4, bourgeois2026comprehensivemultidisciplinarycare pages 4-6) |
| Peripheral neuropathy | HP:0009830 Peripheral neuropathy; HP:0003443 Decreased vibratory sense; HP:0002528 Areflexia | Adult onset, often after or alongside motor syndrome | Progressive sensory and reflex abnormalities | Frequent associated finding; includes distal sensory loss, decreased reflexes, impaired vibration sense; lower-extremity neuropathy is a minor clinical diagnostic criterion (bourgeois2026comprehensivemultidisciplinarycare pages 3-4, berry‐kravis2007fragilex‐associatedtremorataxia pages 2-4) | (bourgeois2026comprehensivemultidisciplinarycare pages 3-4, berry‐kravis2007fragilex‐associatedtremorataxia pages 2-4) |
| Cognitive/executive dysfunction / dementia | HP:0002185 Neurocognitive decline; HP:0000734 Executive dysfunction; HP:0001268 Dementia; HP:0002354 Memory impairment | Usually later than motor onset, often in the 60s–70s | Progressive fronto-subcortical pattern; may advance to major neurocognitive disorder | Executive dysfunction and short-term memory deficiency are minor diagnostic criteria; ~50% of males with FXTAS may develop frontal-subcortical dementia/MNCD; cognitive impairment correlates with MCP sign and disease progression (bourgeois2026comprehensivemultidisciplinarycare pages 2-3, bourgeois2026comprehensivemultidisciplinarycare pages 3-4, berry‐kravis2007fragilex‐associatedtremorataxia pages 2-4, bourgeois2026comprehensivemultidisciplinarycare pages 4-6) | (bourgeois2026comprehensivemultidisciplinarycare pages 2-3, bourgeois2026comprehensivemultidisciplinarycare pages 3-4, berry‐kravis2007fragilex‐associatedtremorataxia pages 2-4, bourgeois2026comprehensivemultidisciplinarycare pages 4-6) |
| Psychiatric symptoms (depression/anxiety/apathy) | HP:0000716 Depression; HP:0000739 Anxiety; HP:0000741 Apathy | Can precede or accompany motor symptoms; often prominent in females/preFXTAS | Chronic/progressive with disease burden; may worsen with cognitive decline | Common comorbidities include depression, anxiety, irritability, and apathy; female premutation carriers may show earlier neuropsychiatric manifestations than overt motor syndrome (bourgeois2026comprehensivemultidisciplinarycare pages 2-3, NCT02936531 chunk 1, liani2025premutationfemaleswith pages 4-6) | (bourgeois2026comprehensivemultidisciplinarycare pages 2-3, NCT02936531 chunk 1, liani2025premutationfemaleswith pages 4-6) |
| Autonomic dysfunction | HP:0001284 Orthostatic hypotension; HP:0000011 Neurogenic bladder; HP:0000047 Urinary incontinence; HP:0004383 Erectile dysfunction | Adult onset, usually after established neurologic disease | Progressive, contributes to disability and complications | Frequent associated finding; reported manifestations include orthostatic hypotension, impotence, and progressive bowel/bladder dysfunction (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, berry‐kravis2007fragilex‐associatedtremorataxia pages 2-4) | (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, berry‐kravis2007fragilex‐associatedtremorataxia pages 2-4) |
| White matter lesions / MCP sign (imaging phenotype) | HP:0012707 Abnormality of cerebral white matter; HP:0002500 Abnormal cerebral MRI white matter signal intensity; HP:0025437 Middle cerebellar peduncle hyperintensity | Usually detected in symptomatic adults; may occasionally precede overt tremor/ataxia | Progressive radiologic white matter disease and atrophy | Major radiologic hallmark; MCP sign = increased T2/FLAIR signal in middle cerebellar peduncles. Observed only in premutation carriers in one cohort and present in 52% of carriers aged ≥45 vs 0% controls; recent review notes MCP hyperintensities in ~60% of male FXTAS patients; asymptomatic carriers with MCP sign have been reported (bourgeois2026comprehensivemultidisciplinarycare pages 3-4, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8, bourgeois2026comprehensivemultidisciplinarycare pages 4-6, bourgeois2026comprehensivemultidisciplinarycare media 7c781a75) | (bourgeois2026comprehensivemultidisciplinarycare pages 3-4, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8, bourgeois2026comprehensivemultidisciplinarycare pages 4-6, bourgeois2026comprehensivemultidisciplinarycare media 7c781a75) |
Table: This table summarizes the main clinical and imaging phenotypes of fragile X-associated tremor/ataxia syndrome, with suggested HPO mappings, typical onset and progression, and key numeric estimates useful for knowledge-base curation.
3.1 Natural history and progression (key data)
A cohort analysis reported the typical progression sequence and timing (male premutation carriers with FXTAS), with median times from first motor symptom: ataxia 2 years, falls 6 years, walking-aid dependence 15 years, death 21 years (Leehey et al., Movement Disorders; Jan 2007; DOI: https://doi.org/10.1002/mds.21252) (leehey2007progressionoftremor pages 2-4). The same progression metrics are reiterated in testing-guideline synthesis (berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8).
3.2 Quality-of-life impact (high-level)
FXTAS progression leads to increasing gait instability, falls, need for assistive devices, and frequent evolution to major neurocognitive disorder/dementia in a substantial proportion of males, implying major impacts on independence and caregiver burden (bourgeois2026comprehensivemultidisciplinarycare pages 2-3, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8).
4. Genetic / molecular information
4.1 Causal gene
- FMR1 (fragile X messenger ribonucleoprotein 1) is the primary and essentially exclusive established disease gene for FXTAS in OpenTargets disease-target evidence (OpenTargets Search: Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS).
4.2 Pathogenic variant class
- Repeat expansion (trinucleotide): premutation 55–200 CGG repeats in the 5′UTR (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, NCT02936531 chunk 1).
- Mechanistic consequence: increased FMR1 mRNA with toxic gain-of-function; inclusions in neurons and astrocytes (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, bourgeois2026comprehensivemultidisciplinarycare pages 3-4).
4.3 Epigenetics / chromatin effects (selected primary/model evidence)
A Drosophila and patient-cell study reported increased histone acetylation at the FMR1 locus in premutation carriers and showed that chromatin-modifying interventions can suppress CGG-repeat induced neurodegeneration in models: “overexpressing any of three histone deacetylases (HDACs 3, 6, or 11) suppresses CGG repeat–induced neurodegeneration” and HAT inhibitors repressed FMR1 mRNA and extended fly lifespan (PLoS Genet; Dec 2010; DOI: https://doi.org/10.1371/journal.pgen.1001240) (todd2010histonedeacetylasessuppress pages 1-2).
4.4 Modifier genes
- Negative evidence: AQP4 common variants not associated with FXTAS development (eliasmas2023evaluationofaqp4 pages 1-2).
- Premutation consensus: DNA repair genes (e.g., FAN1, MSH3) may influence somatic repeat instability and thereby modulate phenotype variability (tassone2023insightandrecommendations pages 6-8).
5. Environmental information
FXTAS is not infectious and has no known infectious trigger in the retrieved evidence. Potential exposure-related worsening of white matter changes is noted in review-level evidence (excessive alcohol/opioids) (bourgeois2026comprehensivemultidisciplinarycare pages 3-4). More systematic environmental epidemiology for FXTAS was not available in the retrieved corpus.
6. Mechanism / pathophysiology
A structured mechanism table with GO/CL/UBERON suggestions is provided here:
| Mechanism | Key molecular players | Evidence type | Key findings/statistics | Suggested GO biological process terms | Suggested cell type (CL) and anatomical (UBERON) terms | Key citation IDs |
|---|---|---|---|---|---|---|
| RNA toxicity | FMR1 premutation RNA (55–200 CGG repeats), RNA-binding proteins, reduced FMRP | Human clinical/review; human postmortem transcriptomics | FXTAS is driven in part by elevated FMR1 mRNA with toxic gain-of-function; early foundational review states the mechanism is related to “overexpression and toxicity of the FMR1 mRNA per se.” In human brain snRNA-seq, FMR1 upregulation was modest in some glial populations (~1.3-fold rather than 4–8-fold reported in blood), supporting tissue- and cell-type-specific RNA toxicity; study analyzed 7 premutation carriers vs 6 controls and >120,000 nuclei from frontal cortex and cerebellum (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, dias2023glialdysregulationin pages 1-2, bourgeois2026comprehensivemultidisciplinarycare pages 1-2) | GO:0006396 RNA processing; GO:0009451 RNA modification; GO:0034645 cellular macromolecule biosynthetic process; GO:0010467 gene expression | CL:0000125 glial cell; CL:0000630 neuron; UBERON:0001870 frontal lobe; UBERON:0002037 cerebellum | (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, dias2023glialdysregulationin pages 1-2, bourgeois2026comprehensivemultidisciplinarycare pages 1-2) |
| RAN translation / FMRpolyG toxicity | Expanded CGG repeat, FMRpolyG, translational machinery, sequestered proteins | Review/human disease synthesis | Recent multidisciplinary review lists production of toxic FMRpolyG among major pathogenic mechanisms, alongside RNA toxicity, reduced FMRP, oxidative stress, and calcium dysregulation. Evidence in the retrieved context is primarily review-level rather than quantitative primary clinical statistics (bourgeois2026comprehensivemultidisciplinarycare pages 1-2) | GO:0006412 translation; GO:0031126 cytoplasmic translational initiation; GO:0031047 gene silencing by RNA; GO:0061684 chaperone-mediated autophagy | CL:0000630 neuron; CL:0000127 astrocyte; UBERON:0000955 brain; UBERON:0002037 cerebellum | (bourgeois2026comprehensivemultidisciplinarycare pages 1-2) |
| Inclusion formation / SUMOylation–autophagy dysfunction | SUMO2/3, ubiquitin, p62/SQSTM1, autophagosomes, proteostasis machinery | Human postmortem brain; patient-derived skin fibroblasts; RNA-seq/gene-set analysis | Neuropathologic hallmark is intranuclear inclusions in neurons and astrocytes. Nearly 200 proteins have been identified in FXTAS inclusions, with SUMO2, ubiquitin, and p62 among the most abundant. 2023 study found FXTAS postmortem brains positive for SUMO2/3 conjugates; RNA-seq indicated SUMOylation upregulated; fibroblasts showed p62 accumulation and autophagosome accumulation; gene-set analysis showed downregulation of autophagy-related GO terms (alvarezmora2023explorationofsumo23 pages 1-2, bourgeois2026comprehensivemultidisciplinarycare pages 3-4) | GO:0016567 protein ubiquitination; GO:0016925 protein sumoylation; GO:0006914 autophagy; GO:0006511 ubiquitin-dependent protein catabolic process | CL:0000630 neuron; CL:0000127 astrocyte; UBERON:0000955 brain; UBERON:0002037 cerebellum | (alvarezmora2023explorationofsumo23 pages 1-2, bourgeois2026comprehensivemultidisciplinarycare pages 3-4) |
| Mitochondrial dysfunction / oxidative stress | Mitochondria, VDAC, ER-mitochondria contact sites, ROS, respiratory-chain complexes, calcium homeostasis | Review of human/model/cell evidence; small open-label therapeutic signal | 2024 review links FXTAS to impaired mitochondrial protein import/transport, altered mitochondrial morphology, disrupted calcium handling, reduced respiratory-chain activity, elevated ROS/lipid peroxidation/protein carbonylation, and impaired antioxidant defenses. A small 12-week open-label allopregnanolone study in 6 males reportedly reduced oxidative stress and improved mitochondrial function (pagano2024mitochondrialdysfunctionin pages 1-2) | GO:0005739 mitochondrion; GO:0006979 response to oxidative stress; GO:0007005 mitochondrion organization; GO:0006874 cellular calcium ion homeostasis; GO:0006119 oxidative phosphorylation | CL:0000127 astrocyte; CL:0000630 neuron; UBERON:0000955 brain; UBERON:0002037 cerebellum | (pagano2024mitochondrialdysfunctionin pages 1-2) |
| Glial / oligodendrocyte dysregulation | FMR1/FMRP networks, oligodendrocyte-lineage genes, glial transcriptional programs | Human postmortem single-nucleus RNA-seq | PNAS 2023 identified cell type–, disease type–, and region-specific transcriptional perturbations, with notable network dysregulation in the cortical oligodendrocyte lineage. Pseudotime analyses suggested altered early oligodendrocyte gene expression, implicating glial dysfunction as an upstream contributor to white-matter pathology. Dataset: 7 premutation carriers, 6 controls, >120,000 nuclei from frontal cortex and cerebellum (dias2023glialdysregulationin pages 1-2) | GO:0042552 myelination; GO:0048709 oligodendrocyte differentiation; GO:0007268 synaptic transmission; GO:0014003 oligodendrocyte development | CL:0000128 oligodendrocyte; CL:0000127 astrocyte; UBERON:0001870 frontal lobe; UBERON:0002037 cerebellum | (dias2023glialdysregulationin pages 1-2) |
| White matter disease / cerebellar peduncle pathology | Middle cerebellar peduncles (MCP), corpus callosum splenium, dentate nucleus, iron dysregulation, CGG repeat size | MRI biomarker studies; clinical-radiologic correlation; review | MRI hallmark is the MCP sign (T2 hyperintensity in middle cerebellar peduncles). Among premutation carriers aged ≥45 years, MCP sign was seen in 52% of carriers and 0% of controls; it associated with impaired motor and executive function. Review evidence notes MCP hyperintensities in about 60% of male FXTAS cases and progressive white-matter lesion burden/atrophy correlating with stage and cognition. MCP width may be an early biomarker and was reduced in premutation carriers who later converted to FXTAS (bourgeois2026comprehensivemultidisciplinarycare pages 4-6, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8, berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2) | GO:0042552 myelination; GO:0007417 central nervous system development; GO:0007601 visual perception; GO:0051962 positive regulation of nervous system development | CL:0000128 oligodendrocyte; CL:0000540 neuron of cerebellum; UBERON:0001950 middle cerebellar peduncle; UBERON:0002037 cerebellum; UBERON:0001885 corpus callosum | (bourgeois2026comprehensivemultidisciplinarycare pages 4-6, berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8, berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2) |
Table: This table summarizes the main proposed pathophysiologic mechanisms in fragile X-associated tremor/ataxia syndrome, linking molecular players to evidence type, quantitative findings, and suggested ontology terms. It is useful for building structured disease knowledge-base entries across mechanism, cell type, and anatomy fields.
6.1 Recent developments (prioritizing 2023–2024)
Human brain cell-type evidence (2023): - A PNAS study performed single-nucleus RNA-seq of >120,000 nuclei from frontal cortex and cerebellum in 7 premutation carriers vs 6 controls, identifying cell-type-, region-, and disease-specific transcriptional perturbations with notable dysregulation in the cortical oligodendrocyte lineage (May 2023; DOI: https://doi.org/10.1073/pnas.2300052120) (dias2023glialdysregulationin pages 1-2).
Proteostasis/autophagy and inclusion biology (2023): - A Cells study examined human postmortem brain and patient fibroblasts, reporting SUMO2/3 conjugate positivity in FXTAS brains and findings consistent with impaired autophagic flux (p62/autophagosome accumulation) and downregulated autophagy-related GO terms (Sep 2023; DOI: https://doi.org/10.3390/cells12192364) (alvarezmora2023explorationofsumo23 pages 1-2).
Mitochondrial dysfunction / oxidative stress (2024): - A 2024 minireview highlights mitochondrial dysfunction as a convergent mechanism in FXTAS and discusses antioxidants/mitochondrial nutrients (ALA, carnitine, CoQ10) as therapeutic candidates; it notes a small open-label allopregnanolone study in six males showing reduced oxidative stress and improved mitochondrial function (Apr 2024; DOI: https://doi.org/10.1007/s11033-024-09415-7) (pagano2024mitochondrialdysfunctionin pages 1-2).
Consensus mechanistic framework (2023 conference synthesis): - A 2023 conference consensus article summarizes three nonexclusive upstream mechanisms for premutation-associated conditions: R-loops, RNA gain-of-function (RNA foci/gelation and sequestration of CGG-binding proteins), and RAN translation yielding potentially toxic proteins; it states these “contribute to subsequent consequences, including mitochondrial dysfunction and neuronal death” (Sep 2023; DOI: https://doi.org/10.3390/cells12182330) (tassone2023insightandrecommendations pages 6-8).
6.2 Causal chain (high-level)
A coherent causal chain supported by the retrieved evidence is: 1) FMR1 CGG premutation expansion → 2) elevated/abnormal FMR1 mRNA and/or RAN translation products (FMRpolyG) → 3) protein sequestration, nuclear inclusions, UPS/autophagy impairment, mitochondrial dysfunction/oxidative stress and glial/white-matter disruption → 4) cerebellar and fronto-subcortical circuit dysfunction → 5) clinical syndrome of tremor, ataxia, executive dysfunction/dementia, neuropsychiatric symptoms, neuropathy/autonomic dysfunction (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, alvarezmora2023explorationofsumo23 pages 1-2, dias2023glialdysregulationin pages 1-2, todd2010histonedeacetylasessuppress pages 1-2).
7. Anatomical structures affected
Primary system: nervous system (brain; cerebellar and white-matter tracts). - Key neuroanatomy / UBERON suggestions: - Cerebellum (UBERON:0002037) - Middle cerebellar peduncle (UBERON:0001950) - Corpus callosum (UBERON:0001885) - Frontal lobe/cortex (UBERON:0001870)
Imaging and neuropathology emphasize white matter disease and the MCP sign, with broad distribution of neuronal and astrocytic inclusions (berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8, bourgeois2026comprehensivemultidisciplinarycare media 7c781a75).
8. Temporal development
- Typical onset: after age 50, commonly around ~60 years in males (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2, NCT02936531 chunk 1).
- Course: progressive; cohort-based milestone progression includes falls and eventual dependence and death over a multi-year to multi-decade course (leehey2007progressionoftremor pages 2-4).
- Staging: A six-stage framework (from subtle symptoms to profound disability) is presented in the multidisciplinary review’s staging table (Table 2), with diagnostic categorization in Table 1 (bourgeois2026comprehensivemultidisciplinarycare media 7c781a75, bourgeois2026comprehensivemultidisciplinarycare media 4ec0dbb2).
9. Inheritance and population
9.1 Inheritance pattern
- X-linked via FMR1 premutation alleles; FXTAS manifests in premutation carriers with reduced penetrance, especially in females (bourgeois2026comprehensivemultidisciplinarycare pages 1-2).
9.2 Epidemiology and penetrance (statistics)
Premutation carrier frequency (population): - Estimated premutation prevalence reported as approximately 1 in 148–200 females and 1 in 290–855 males (Frontiers in Neurology review; Mar 2026; DOI: https://doi.org/10.3389/fneur.2026.1746002) (bourgeois2026comprehensivemultidisciplinarycare pages 1-2). - Earlier clinical synthesis reported carrier frequencies around 1/259 females and 1/813 males (Movement Disorders 2007) (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2).
FXTAS penetrance among premutation carriers: - A widely cited estimate: about 40% of male carriers >50 develop FXTAS; age-stratified male penetrance reported as 17% (50–59), 38% (60–69), 47% (70–79), 75% (80+) (berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2). - Female penetrance is lower (often cited ~14–20% depending on cohort/source) (bourgeois2026comprehensivemultidisciplinarycare pages 1-2, tassone2023insightandrecommendationsa pages 18-20).
Disease prevalence in general population: - FXTAS prevalence has been estimated at ~2–4 per 100,000, based on cohort synthesis (leehey2007progressionoftremor pages 1-2).
10. Diagnostics
10.1 Genetic testing
- Diagnosis relies on DNA-based FMR1 CGG repeat sizing; the same fragile X DNA test is used in FXS and FXTAS evaluation (berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8).
10.2 Clinical criteria (radiologic + clinical)
- A commonly used scheme defines Definite / Probable / Possible FXTAS based on combinations of major/minor radiologic signs (notably MCP/brainstem white-matter lesions) and clinical signs (notably intention tremor and gait ataxia). The multidisciplinary review reproduces these criteria in Table 1 (bourgeois2026comprehensivemultidisciplinarycare media 7c781a75).
10.3 Imaging
- MCP sign: “increased T2 signal intensity in the middle cerebellar peduncles” is a key radiologic hallmark (berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8) and illustrated in the review’s MRI figure (bourgeois2026comprehensivemultidisciplinarycare media d690cd70).
10.4 Differential diagnosis
FXTAS is frequently mistaken for essential tremor, Parkinson disease, multiple system atrophy-cerebellar type (MSA-C), or spinocerebellar ataxias; testing guidelines recommend considering FMR1 testing in unexplained adult-onset tremor/ataxia or suggestive MRI findings (berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8, eliasmas2023evaluationofaqp4 pages 1-2).
11. Outcomes / prognosis
- Progression milestones: median 2y to ataxia, 6y to falls, 15y to walking aid dependence, and 21y to death from initial motor symptom in cohort analysis (leehey2007progressionoftremor pages 2-4).
- Survival variability: survival after onset reported as variable (5–25 years) in the same synthesis (leehey2007progressionoftremor pages 2-4).
Complications include recurrent falls, progressive disability, and cognitive decline/dementia in a substantial fraction of males (bourgeois2026comprehensivemultidisciplinarycare pages 2-3, leehey2007progressionoftremor pages 2-4).
12. Treatment
12.1 Current clinical management (real-world implementation)
There is no established disease-modifying therapy in the retrieved evidence; care is largely symptom- and function-focused with multidisciplinary involvement. A multidisciplinary care review lists commonly used symptomatic agents (e.g., primidone, gabapentin/pregabalin, beta blockers for tremor; carbidopa/levodopa for parkinsonism; acetylcholinesterase inhibitors or memantine for cognitive symptoms) and emphasizes PT/OT/SLP, exercise, delirium-risk minimization, and caregiver support (Frontiers in Neurology; Mar 2026; DOI: https://doi.org/10.3389/fneur.2026.1746002) (bourgeois2026comprehensivemultidisciplinarycare pages 6-7).
MAXO suggestions (examples): - MAXO:0000004 pharmacotherapy - MAXO:0000015 physical therapy - MAXO:0000016 occupational therapy - MAXO:0000017 speech therapy - MAXO:0000757 genetic counseling
12.2 Clinical trials / experimental interventions
A structured trial table is provided here:
| Intervention | NCT ID | Phase | Design | Status | Enrollment | Population | Primary outcomes | Key notes (e.g., timepoints) | Source citation IDs |
|---|---|---|---|---|---|---|---|---|---|
| Memantine | NCT00584948 | NA | Randomized, parallel, quadruple-masked, placebo-controlled | Completed | 94 | FMR1 premutation carriers (55–200 CGG repeats) with FXTAS stage 1–5 | Change from baseline in executive function (BDS-II) over 1 year; change in intention tremor by CATSYS at 1 year | Dosing titrated from 5 mg to 10 mg twice daily by week 4; started Sep 2007, completed Sep 2012; derived publication cited as Seritan et al. 2014 (PMID 24345444) | (NCT00584948 chunk 1) |
| Allopregnanolone | NCT02603926 | Phase 2 | Single-group, open-label interventional trial | Completed | 6 | Fragile X premutation carriers (55–200 CGG repeats) with FXTAS | CVLT-II Trial 1–5 raw score; secondary outcomes included BDS-2, CATSYS Dot-to-Dot Tremor Intensity, hippocampal volume MRI | Weekly IV infusions for 12 total infusions; dose escalation 2.0 → 4.0 → 6.0 mg, highest tolerated dose maintained; outcomes measured baseline and 14 weeks/post-treatment | (NCT02603926 chunk 1) |
| Sulforaphane | NCT05233579 | NA | Open-label interventional trial | Completed | 15 | Adults age 50–85 with diagnosed FXTAS and FMR1 premutation (55–200 CGG repeats) | FXTAS-RS clinical stage; structural MRI volumetrics; FLAIR hyperintensity volume; multiple cognitive, gait, motor, and QoL measures | Scheduled assessments at baseline and 6 months; measures included Neuro-QoL, MoCA, MMSE, BDS-2, COWAT, CANTAB, GAITRite, Purdue Pegboard, Kinesia One; preclinical rationale cited from Napoli et al. 2021 | (NCT05233579 chunk 2) |
| Citicoline | NCT02197104 | Phase 2 | Interventional trial | Completed | 10 | FXTAS participants | Not available in current context | Trial listed in ClinicalTrials.gov search results, but detailed outcome fields were not retrieved in the available context | (OpenTargets Search: Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS) |
| Diaphragmatic breathing and heart-rate variability training | NCT03816540 | Phase 3 | Interventional trial | Completed | 20 | Individuals with fragile X-associated tremor/ataxia | Not available in current context | Trial listed in ClinicalTrials.gov search results as targeting hypertension in FXTAS; detailed outcome fields not retrieved in available context | (OpenTargets Search: Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS) |
| Treadmill training | NCT04428567 | NA | Interventional rehabilitation trial | Terminated | 3 | Adults age ≥50 with FXTAS able to stand and walk without support for 2 minutes | Cognitive outcomes (MoCA, SDMT, COWAT, STROOP, Digit Span); QoL (Neuro-QoL); mood/sleep/anxiety (CES-D, PSQI, BAI); physical activity and exertion | Time frames included 6 weeks and 6 months; site at Rush University Medical Center; exclusion criteria included dementia and major neurologic/musculoskeletal disease | (NCT04428567 chunk 2, OpenTargets Search: Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS) |
| Brain network activation and gait/posture biomarkers | NCT02936531 | Not provided | Observational | Unknown | 150 | FXTAS participants age 50–80 | Biomarker-oriented study of electrophysiological BNA/ERP with gait/posture phenotyping | Trial background notes FXTAS features and MRI findings; not a treatment study but relevant real-world biomarker implementation | (NCT02936531 chunk 1) |
| Symptomatic multidisciplinary care (real-world implementation) | Not applicable | Not applicable | Clinical management approach | In clinical use/recommended | Not applicable | Patients with FXTAS, especially multisystem disease and caregiver burden | Not trial-based; symptom control and function-focused management | Recommended agents include primidone, levetiracetam, gabapentin/pregabalin, beta-blockers, carbidopa/levodopa; cognitive agents such as acetylcholinesterase inhibitors or memantine may be tried; PT/OT/SLP, cardiovascular exercise, delirium-risk minimization emphasized | (bourgeois2026comprehensivemultidisciplinarycare pages 6-7) |
Table: This table summarizes the main FXTAS interventional and observational studies available in the retrieved ClinicalTrials.gov context, along with a real-world multidisciplinary management row. It is useful for quickly comparing study design, enrollment, outcomes, and implementation details across current FXTAS interventions.
Key trials with retrievable registry details include: - Memantine RCT (NCT00584948; completed; n=94; primary outcomes BDS-II executive function and CATSYS tremor) (NCT00584948 chunk 1). - Allopregnanolone (NCT02603926; open-label phase 2; completed; n=6; cognitive/tremor/MRI outcomes) (NCT02603926 chunk 1). - Sulforaphane (NCT05233579; open-label; completed; n=15; includes MRI lesion volumetrics and functional outcomes) (NCT05233579 chunk 2).
13. Prevention
Primary prevention of FXTAS is not currently possible in premutation carriers, but secondary/tertiary prevention strategies include: - Genetic counseling and cascade testing when FXTAS or other fragile X–associated conditions are identified in a family (berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8). - Risk factor mitigation for complications (e.g., fall prevention, management of psychiatric symptoms, and avoidance of exposures that may worsen white-matter disease per expert review) (bourgeois2026comprehensivemultidisciplinarycare pages 3-4).
14. Other species / natural disease
Naturally occurring FXTAS as a spontaneous veterinary condition was not identified in the retrieved evidence.
15. Model organisms (key systems)
FXTAS is extensively studied in Drosophila, mouse (CGG knock-in and inducible CGG-expression models), and cell-based systems.
15.1 Drosophila models
- A Neuron study reported that “transcribed premutation repeats alone are sufficient to cause neurodegeneration” and that Purα overexpression “could suppress rCGG-mediated neurodegeneration in a dose-dependent manner” (Aug 2007; DOI: https://doi.org/10.1016/j.neuron.2007.07.020) (jin2007purαbinds pages 1-2).
- Epigenetic modulation in flies: overexpressing HDAC3/6/11 suppresses CGG-repeat neurodegeneration and HAT inhibitors reduce FMR1 mRNA in premutation cells and extend fly lifespan (Dec 2010; DOI: https://doi.org/10.1371/journal.pgen.1001240) (todd2010histonedeacetylasessuppress pages 1-2).
15.2 Mouse models
- A 2014 review summarizes that mouse models recapitulate elevated Fmr1 mRNA, reduced FMRP, ubiquitin-positive intranuclear inclusions, dendritic abnormalities, memory and motor deficits, and RAN-translation-related pathology; it provides population-frequency and penetrance estimates for context (Jul 2014; DOI: https://doi.org/10.1186/1866-1955-6-25) (berman2014mousemodelsof pages 1-3).
- An inducible mouse model study reported that stopping expanded-CGG expression early could reverse inclusion formation and ameliorate motor phenotypes; it also reports inclusions stain for FMRpolyG (Jun 2015; DOI: https://doi.org/10.1093/hmg/ddv216) (hukema2015reversibilityofneuropathology pages 1-2).
15.3 Cell-based / iPSC-derived systems
- A mechanistic study in models links RAN translation → FMRpolyG → UPS impairment, with suppression by HSP70 and attenuation by preventing RAN translation (May/Aug 2015; DOI: https://doi.org/10.1093/hmg/ddv165) (oh2015rantranslationat pages 1-2).
Evidence gaps and curation notes
- ICD-10/ICD-11, Orphanet (ORPHA), and authoritative MeSH ID: not retrievable from the current evidence set; should be added via dedicated ontology services.
- 2023–2024 interventional outcomes: ClinicalTrials.gov records in this run provide trial structure but not full numeric efficacy results; linking to results publications (e.g., Seritan et al. 2014 for memantine) is recommended for outcome extraction (NCT00584948 chunk 1).
Key figure/table evidence used
- Diagnostic criteria and staging tables, and MRI example of MCP sign were retrieved from the multidisciplinary review (bourgeois2026comprehensivemultidisciplinarycare media 7c781a75, bourgeois2026comprehensivemultidisciplinarycare media 4ec0dbb2, bourgeois2026comprehensivemultidisciplinarycare media d690cd70).
References
-
(OpenTargets Search: Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS): Open Targets Query (Fragile X-associated tremor/ataxia syndrome,fragile X-associated tremor ataxia syndrome,FXTAS, 3 results). Buniello, A. et al. (2025). Open Targets Platform: facilitating therapeutic hypotheses building in drug discovery. Nucleic Acids Research.
-
(berry‐kravis2007fragilex‐associatedtremorataxia pages 1-2): Elizabeth Berry‐Kravis, Liane Abrams, Sarah M. Coffey, Deborah A. Hall, Claudia Greco, Louise W. Gane, Jim Grigsby, James A. Bourgeois, Brenda Finucane, Sebastien Jacquemont, James A. Brunberg, Lin Zhang, Janet Lin, Flora Tassone, Paul J. Hagerman, Randi J. Hagerman, and Maureen A. Leehey. Fragile x‐associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines. Movement Disorders, 22:2018-2030, Oct 2007. URL: https://doi.org/10.1002/mds.21493, doi:10.1002/mds.21493. This article has 399 citations and is from a highest quality peer-reviewed journal.
-
(bourgeois2026comprehensivemultidisciplinarycare pages 1-2): James A. Bourgeois, Andrea Schneider, Jessica Klusek, Thomas R. Christensen, Ellie Levin, Kendall Gardner, Ariel A. Jacobi, and Randi J. Hagerman. Comprehensive, multidisciplinary care for fragile x-associated tremor/ataxia syndrome. Frontiers in Neurology, Mar 2026. URL: https://doi.org/10.3389/fneur.2026.1746002, doi:10.3389/fneur.2026.1746002. This article has 0 citations and is from a peer-reviewed journal.
-
(tassone2023insightandrecommendations pages 6-8): Flora Tassone, Dragana Protic, Emily Graves Allen, Alison D Archibald, Anna Baud, Ted W Brown, Dejan B Budimirovic, Jonathan Cohen, Brett Dufour, Rachel Eiges, Nicola Elvassore, Lidia V Gabis, Samantha J Grudzien, Deborah A Hall, David Hessl, Abigail Hogan, Jessica Ezzell Hunter, Peng Jin, Poonnada Jiraanont, Jessica Klusek, R Frank Kooy, Claudine M Kraan, Cecilia Laterza, Andrea Lee, Karen Lipworth, Molly Losh, Danuta Loesch-Mdzewska, Reymundo Lozano, Marsha R Mailick, Apostolos Manolopoulos, Veronica Martinez-Cerdeno, Yingratana McLennan, Robert M Miller, Federica Alice Maria Montanaro, Matthew W Mosconi, Sarah Nelson Potter, Melissa Raspa, Susan M Rivera, Katharine Shelly, Peter K Todd, Katarzyna Tutak, Jun Yi Wang, Anne Wheeler, Tri Indah Winarni, Marwa Zafarullah, and Randi J Hagerman. Insight and recommendations for fragile x-premutation-associated conditions from the fifth international conference on fmr1 premutation. Cells, Sep 2023. URL: https://doi.org/10.3390/cells12182330, doi:10.3390/cells12182330. This article has 81 citations.
-
(berry‐kravis2007fragilex‐associatedtremorataxia pages 7-8): Elizabeth Berry‐Kravis, Liane Abrams, Sarah M. Coffey, Deborah A. Hall, Claudia Greco, Louise W. Gane, Jim Grigsby, James A. Bourgeois, Brenda Finucane, Sebastien Jacquemont, James A. Brunberg, Lin Zhang, Janet Lin, Flora Tassone, Paul J. Hagerman, Randi J. Hagerman, and Maureen A. Leehey. Fragile x‐associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines. Movement Disorders, 22:2018-2030, Oct 2007. URL: https://doi.org/10.1002/mds.21493, doi:10.1002/mds.21493. This article has 399 citations and is from a highest quality peer-reviewed journal.
-
(eliasmas2023evaluationofaqp4 pages 1-2): Andrea Elias-Mas, Miriam Potrony, Jaume Bague, David J. Cutler, Maria Isabel Alvarez-Mora, Teresa Torres, Tamara Barcos, Joan Anton Puig-Butille, Marta Rubio, Irene Madrigal, Susana Puig, Emily G. Allen, and Laia Rodriguez-Revenga. Evaluation of aqp4 functional variants and its association with fragile x-associated tremor/ataxia syndrome. Frontiers in Aging Neuroscience, Jan 2023. URL: https://doi.org/10.3389/fnagi.2022.1073258, doi:10.3389/fnagi.2022.1073258. This article has 6 citations and is from a peer-reviewed journal.
-
(alvarezmora2023explorationofsumo23 pages 1-2): Maria Isabel Alvarez-Mora, Glòria Garrabou, Laura Molina-Porcel, Ruben Grillo-Risco, Francisco Garcia-Garcia, Tamara Barcos, Judith Cantó-Santos, and Laia Rodriguez-Revenga. Exploration of sumo2/3 expression levels and autophagy process in fragile x-associated tremor/ataxia syndrome: addressing study limitations and insights for future research. Cells, 12:2364, Sep 2023. URL: https://doi.org/10.3390/cells12192364, doi:10.3390/cells12192364. This article has 4 citations.
-
(NCT02936531 chunk 2): Dr. Sharon Hassin. Brain Network Activation and Gait and Posture in FXTAS. Sheba Medical Center. 2016. ClinicalTrials.gov Identifier: NCT02936531
-
(NCT02936531 chunk 1): Dr. Sharon Hassin. Brain Network Activation and Gait and Posture in FXTAS. Sheba Medical Center. 2016. ClinicalTrials.gov Identifier: NCT02936531
-
(dias2023glialdysregulationin pages 1-2): Caroline M. Dias, Biju Issac, Liang Sun, Abigail Lukowicz, Maya Talukdar, Shyam K. Akula, Michael B. Miller, Katherine Walsh, Shira Rockowitz, and Christopher A. Walsh. Glial dysregulation in the human brain in fragile x-associated tremor/ataxia syndrome. Proceedings of the National Academy of Sciences of the United States of America, May 2023. URL: https://doi.org/10.1073/pnas.2300052120, doi:10.1073/pnas.2300052120. This article has 26 citations and is from a highest quality peer-reviewed journal.
-
(liani2025premutationfemaleswith pages 4-6): Valentina Liani, Carme Torrents, Elisa Rolleri, Nor Azyati Yusoff, Narueporn Likhitweerawong, Sydney Moore, Flora Tassone, Andrea Schneider, Ellery Santos, Hazel M. B. Biag, James A. Bourgeois, Kathryn E. Unruh, Matthew W. Mosconi, and Randi J. Hagerman. Premutation females with prefxtas. International Journal of Molecular Sciences, 26:2825, Mar 2025. URL: https://doi.org/10.3390/ijms26062825, doi:10.3390/ijms26062825. This article has 10 citations.
-
(bourgeois2026comprehensivemultidisciplinarycare pages 6-7): James A. Bourgeois, Andrea Schneider, Jessica Klusek, Thomas R. Christensen, Ellie Levin, Kendall Gardner, Ariel A. Jacobi, and Randi J. Hagerman. Comprehensive, multidisciplinary care for fragile x-associated tremor/ataxia syndrome. Frontiers in Neurology, Mar 2026. URL: https://doi.org/10.3389/fneur.2026.1746002, doi:10.3389/fneur.2026.1746002. This article has 0 citations and is from a peer-reviewed journal.
-
(NCT00584948 chunk 1): Memantine Treatment in Fragile X-Associated Tremor/Ataxia Syndrome. University of California, Davis. 2007. ClinicalTrials.gov Identifier: NCT00584948
-
(NCT02603926 chunk 1): Randi J. Hagerman, MD. Treatment of Fragile-X Associated Tremor/Ataxia Syndrome (FXTAS) With Allopregnanolone. Randi J. Hagerman, MD. 2015. ClinicalTrials.gov Identifier: NCT02603926
-
(bourgeois2026comprehensivemultidisciplinarycare pages 3-4): James A. Bourgeois, Andrea Schneider, Jessica Klusek, Thomas R. Christensen, Ellie Levin, Kendall Gardner, Ariel A. Jacobi, and Randi J. Hagerman. Comprehensive, multidisciplinary care for fragile x-associated tremor/ataxia syndrome. Frontiers in Neurology, Mar 2026. URL: https://doi.org/10.3389/fneur.2026.1746002, doi:10.3389/fneur.2026.1746002. This article has 0 citations and is from a peer-reviewed journal.
-
(pagano2024mitochondrialdysfunctionin pages 1-2): Giovanni Pagano, Alex Lyakhovich, Federico V. Pallardó, Luca Tiano, Adriana Zatterale, and Marco Trifuoggi. Mitochondrial dysfunction in fragile x syndrome and fragile x-associated tremor/ataxia syndrome: prospect use of antioxidants and mitochondrial nutrients. Molecular Biology Reports, Apr 2024. URL: https://doi.org/10.1007/s11033-024-09415-7, doi:10.1007/s11033-024-09415-7. This article has 12 citations and is from a peer-reviewed journal.
-
(bourgeois2026comprehensivemultidisciplinarycare pages 4-6): James A. Bourgeois, Andrea Schneider, Jessica Klusek, Thomas R. Christensen, Ellie Levin, Kendall Gardner, Ariel A. Jacobi, and Randi J. Hagerman. Comprehensive, multidisciplinary care for fragile x-associated tremor/ataxia syndrome. Frontiers in Neurology, Mar 2026. URL: https://doi.org/10.3389/fneur.2026.1746002, doi:10.3389/fneur.2026.1746002. This article has 0 citations and is from a peer-reviewed journal.
-
(berry‐kravis2007fragilex‐associatedtremorataxia pages 2-4): Elizabeth Berry‐Kravis, Liane Abrams, Sarah M. Coffey, Deborah A. Hall, Claudia Greco, Louise W. Gane, Jim Grigsby, James A. Bourgeois, Brenda Finucane, Sebastien Jacquemont, James A. Brunberg, Lin Zhang, Janet Lin, Flora Tassone, Paul J. Hagerman, Randi J. Hagerman, and Maureen A. Leehey. Fragile x‐associated tremor/ataxia syndrome: clinical features, genetics, and testing guidelines. Movement Disorders, 22:2018-2030, Oct 2007. URL: https://doi.org/10.1002/mds.21493, doi:10.1002/mds.21493. This article has 399 citations and is from a highest quality peer-reviewed journal.
-
(bourgeois2026comprehensivemultidisciplinarycare pages 2-3): James A. Bourgeois, Andrea Schneider, Jessica Klusek, Thomas R. Christensen, Ellie Levin, Kendall Gardner, Ariel A. Jacobi, and Randi J. Hagerman. Comprehensive, multidisciplinary care for fragile x-associated tremor/ataxia syndrome. Frontiers in Neurology, Mar 2026. URL: https://doi.org/10.3389/fneur.2026.1746002, doi:10.3389/fneur.2026.1746002. This article has 0 citations and is from a peer-reviewed journal.
-
(bourgeois2026comprehensivemultidisciplinarycare media 7c781a75): James A. Bourgeois, Andrea Schneider, Jessica Klusek, Thomas R. Christensen, Ellie Levin, Kendall Gardner, Ariel A. Jacobi, and Randi J. Hagerman. Comprehensive, multidisciplinary care for fragile x-associated tremor/ataxia syndrome. Frontiers in Neurology, Mar 2026. URL: https://doi.org/10.3389/fneur.2026.1746002, doi:10.3389/fneur.2026.1746002. This article has 0 citations and is from a peer-reviewed journal.
-
(leehey2007progressionoftremor pages 2-4): Maureen A. Leehey, Elizabeth Berry‐Kravis, Sung‐Joon Min, Deborah A. Hall, Cathlin D. Rice, Lin Zhang, Jim Grigsby, Claudia M. Greco, Ann Reynolds, Rebecca Lara, Jennifer Cogswell, Sebastien Jacquemont, David R. Hessl, Flora Tassone, Randi Hagerman, and Paul J. Hagerman. Progression of tremor and ataxia in male carriers of the fmr1 premutation. Movement Disorders, 22:203-206, Jan 2007. URL: https://doi.org/10.1002/mds.21252, doi:10.1002/mds.21252. This article has 171 citations and is from a highest quality peer-reviewed journal.
-
(todd2010histonedeacetylasessuppress pages 1-2): Peter K. Todd, Seok Yoon Oh, Amy Krans, Udai B. Pandey, Nicholas A. Di Prospero, Kyung-Tai Min, J. Paul Taylor, and Henry L. Paulson. Histone deacetylases suppress cgg repeat–induced neurodegeneration via transcriptional silencing in models of fragile x tremor ataxia syndrome. PLoS Genetics, 6:e1001240, Dec 2010. URL: https://doi.org/10.1371/journal.pgen.1001240, doi:10.1371/journal.pgen.1001240. This article has 114 citations and is from a domain leading peer-reviewed journal.
-
(bourgeois2026comprehensivemultidisciplinarycare media 4ec0dbb2): James A. Bourgeois, Andrea Schneider, Jessica Klusek, Thomas R. Christensen, Ellie Levin, Kendall Gardner, Ariel A. Jacobi, and Randi J. Hagerman. Comprehensive, multidisciplinary care for fragile x-associated tremor/ataxia syndrome. Frontiers in Neurology, Mar 2026. URL: https://doi.org/10.3389/fneur.2026.1746002, doi:10.3389/fneur.2026.1746002. This article has 0 citations and is from a peer-reviewed journal.
-
(tassone2023insightandrecommendationsa pages 18-20): F Tassone, D Protic, E Allen, AD Archibald, and A Baud. Insight and recommendations for fragile x premutation associated conditions from the 5th international conference on fmr1 premutation. Unknown journal, 2023.
-
(leehey2007progressionoftremor pages 1-2): Maureen A. Leehey, Elizabeth Berry‐Kravis, Sung‐Joon Min, Deborah A. Hall, Cathlin D. Rice, Lin Zhang, Jim Grigsby, Claudia M. Greco, Ann Reynolds, Rebecca Lara, Jennifer Cogswell, Sebastien Jacquemont, David R. Hessl, Flora Tassone, Randi Hagerman, and Paul J. Hagerman. Progression of tremor and ataxia in male carriers of the fmr1 premutation. Movement Disorders, 22:203-206, Jan 2007. URL: https://doi.org/10.1002/mds.21252, doi:10.1002/mds.21252. This article has 171 citations and is from a highest quality peer-reviewed journal.
-
(bourgeois2026comprehensivemultidisciplinarycare media d690cd70): James A. Bourgeois, Andrea Schneider, Jessica Klusek, Thomas R. Christensen, Ellie Levin, Kendall Gardner, Ariel A. Jacobi, and Randi J. Hagerman. Comprehensive, multidisciplinary care for fragile x-associated tremor/ataxia syndrome. Frontiers in Neurology, Mar 2026. URL: https://doi.org/10.3389/fneur.2026.1746002, doi:10.3389/fneur.2026.1746002. This article has 0 citations and is from a peer-reviewed journal.
-
(NCT05233579 chunk 2): Open-Label Trial of Sulforaphane in Premutation Carriers With FXTAS. University of California, Davis. 2021. ClinicalTrials.gov Identifier: NCT05233579
-
(NCT04428567 chunk 2): Treadmill Training in Fragile X-associated Tremor/Ataxia Syndrome. Rush University Medical Center. 2019. ClinicalTrials.gov Identifier: NCT04428567
-
(jin2007purαbinds pages 1-2): Peng Jin, Ranhui Duan, Abrar Qurashi, Yunlong Qin, Donghua Tian, Tracie C. Rosser, Huijie Liu, Yue Feng, and Stephen T. Warren. Pur α binds to rcgg repeats and modulates repeat-mediated neurodegeneration in a drosophila model of fragile x tremor/ataxia syndrome. Neuron, 55:556-564, Aug 2007. URL: https://doi.org/10.1016/j.neuron.2007.07.020, doi:10.1016/j.neuron.2007.07.020. This article has 363 citations and is from a highest quality peer-reviewed journal.
-
(berman2014mousemodelsof pages 1-3): Robert F Berman, Ronald AM Buijsen, Karen Usdin, Elizabeth Pintado, Frank Kooy, Dalyir Pretto, Isaac N Pessah, David L Nelson, Zachary Zalewski, Nicholas Charlet-Bergeurand, Rob Willemsen, and Renate K Hukema. Mouse models of the fragile x premutation and fragile x-associated tremor/ataxia syndrome. Journal of Neurodevelopmental Disorders, Jul 2014. URL: https://doi.org/10.1186/1866-1955-6-25, doi:10.1186/1866-1955-6-25. This article has 87 citations and is from a peer-reviewed journal.
-
(hukema2015reversibilityofneuropathology pages 1-2): Renate K. Hukema, Ronald A.M. Buijsen, Martijn Schonewille, Chris Raske, Lies-Anne W.F.M. Severijnen, Ingeborg Nieuwenhuizen-Bakker, Rob F.M. Verhagen, Lisanne van Dessel, Alex Maas, Nicolas Charlet-Berguerand, Chris I. De Zeeuw, Paul J. Hagerman, Robert F. Berman, and Rob Willemsen. Reversibility of neuropathology and motor deficits in an inducible mouse model for fxtas. Human molecular genetics, 24 17:4948-57, Jun 2015. URL: https://doi.org/10.1093/hmg/ddv216, doi:10.1093/hmg/ddv216. This article has 61 citations and is from a domain leading peer-reviewed journal.
-
(oh2015rantranslationat pages 1-2): Seok Yoon Oh, Fang He, Amy Krans, Michelle Frazer, J. Paul Taylor, Henry L. Paulson, and Peter K. Todd. Ran translation at cgg repeats induces ubiquitin proteasome system impairment in models of fragile x-associated tremor ataxia syndrome. Human molecular genetics, 24 15:4317-26, Aug 2015. URL: https://doi.org/10.1093/hmg/ddv165, doi:10.1093/hmg/ddv165. This article has 112 citations and is from a domain leading peer-reviewed journal.