Anti-NMDA Receptor Encephalitis
Anti-NMDA receptor encephalitis is an antibody-mediated autoimmune encephalitis caused by IgG autoantibodies against the GluN1/NR1 subunit of the NMDA receptor. It usually presents subacutely with psychiatric or cognitive and speech-language symptoms, seizures, movement disorder, decreased consciousness, autonomic dysfunction, and central hypoventilation. Ovarian teratoma and herpes simplex encephalitis are recognized triggers, CSF antibody testing is a core diagnostic marker, and early immunotherapy plus tumor removal when indicated improves outcome.
Ask OpenScientist
Ask a research question about Anti-NMDA Receptor Encephalitis. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Definitions
1- Psychosis Psychiatric or behavioral syndrome.
- Language impairment Speech or language dysfunction, including reduced speech.
- Seizure
- Dyskinesia Movement disorder including orofacial or choreoathetoid movements.
- Coma Severe decreased level of consciousness.
- Abnormality of the autonomic nervous system
- Central hypoventilation
Show evidence (1 reference)
Show evidence (1 reference)
Subtypes
2Show evidence (2 references)
Show evidence (3 references)
Discussions and Knowledge Gaps
1Show evidence (1 reference)
Pathophysiology
6Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Pathograph
Phenotypes
10Nervous System 7
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Respiratory 1
Show evidence (1 reference)
Other 2
Show evidence (2 references)
Show evidence (1 reference)
Medical Actions
7Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Environmental Factors
4Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Biochemical Markers
3Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Clinical Trials
3Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Source YAML
click to showname: Anti-NMDA Receptor Encephalitis
creation_date: "2026-05-16T06:56:16Z"
updated_date: "2026-05-16T08:02:25Z"
category: Autoimmune
parents:
- Autoimmune Encephalitis
- Neurological Disease
- Autoimmune Disease
synonyms:
- Anti-NMDAR encephalitis
- Anti-NMDA receptor autoimmune encephalitis
- NMDAR encephalitis
- NMDARE
disease_term:
preferred_term: anti-NMDA receptor encephalitis
term:
id: MONDO:0021081
label: anti-NMDA receptor encephalitis
description: >-
Anti-NMDA receptor encephalitis is an antibody-mediated autoimmune
encephalitis caused by IgG autoantibodies against the GluN1/NR1 subunit of
the NMDA receptor. It usually presents subacutely with psychiatric or
cognitive and speech-language symptoms, seizures, movement disorder,
decreased consciousness, autonomic dysfunction, and central hypoventilation.
Ovarian teratoma and herpes simplex encephalitis are recognized triggers, CSF
antibody testing is a core diagnostic marker, and early immunotherapy plus
tumor removal when indicated improves outcome.
has_subtypes:
- name: Teratoma-associated anti-NMDA receptor encephalitis
description: >-
Anti-NMDA receptor encephalitis triggered by an ovarian teratoma or other
tumor expressing nervous-system antigens, most often in young adult women.
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Tumours, usually ovarian teratoma, and herpes simplex encephalitis are known triggers of NMDAR autoimmunity."
explanation: >
The Lancet Neurology update identifies ovarian teratoma as a recognized
trigger for NMDAR autoimmunity.
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Tumors were found in 43 (19.5%) patients: 42 females with ovarian teratomas and 1 male with lung cancer."
explanation: >
This 220-patient prospective Chinese cohort quantifies the tumor-associated
subgroup and shows ovarian teratoma dominated tumor findings in females.
- name: Post-herpes simplex encephalitis anti-NMDA receptor encephalitis
description: >-
Anti-NMDA receptor encephalitis emerging after herpes simplex encephalitis,
typically within weeks, with prominent behavioral change, movement disorder,
and dysautonomia.
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Tumours, usually ovarian teratoma, and herpes simplex encephalitis are known triggers of NMDAR autoimmunity."
explanation: >
The review identifies herpes simplex encephalitis as a known upstream
trigger for NMDAR autoimmunity.
- reference: PMID:39147951
reference_title: "Specific clinical and radiological characteristics of anti-NMDA receptor autoimmune encephalitis following herpes encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The median time between HSE and NMDARE onset was 30 days (21-46)."
explanation: >
The HSE-NMDARE cohort directly characterizes the post-herpetic interval
between herpes encephalitis and anti-NMDAR encephalitis onset.
- reference: PMID:39147951
reference_title: "Specific clinical and radiological characteristics of anti-NMDA receptor autoimmune encephalitis following herpes encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "patients with HSE-NMDARE were more frequently males (7/13, 54% vs 43/198, 22%; p = 0.015) and children < 4 (4/13, 31% vs 14/198, 7%; p = 0.016)"
explanation: >
Post-herpetic NMDARE reverses the young-female predominance of idiopathic
NMDARE, skewing toward males and children under 4 years, marking it as a
demographically distinct subgroup with a poorer long-term prognosis.
definitions:
- name: Probable anti-NMDA receptor encephalitis clinical criteria
definition_type: CASE_DEFINITION
description: >-
Probable anti-NMDA receptor encephalitis can be recognized before antibody
confirmation when a subacute encephalitis syndrome develops multiple
characteristic symptom groups, has supportive EEG or CSF abnormalities, and
alternative disorders are reasonably excluded.
criteria_sets:
- name: Graus-style clinical syndrome
core_clinical_characteristics:
- preferred_term: Psychosis
term:
id: HP:0000709
label: Psychosis
description: Psychiatric or behavioral syndrome.
- preferred_term: Language impairment
term:
id: HP:0002463
label: Language impairment
description: Speech or language dysfunction, including reduced speech.
- preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
- preferred_term: Dyskinesia
term:
id: HP:0100660
label: Dyskinesia
description: Movement disorder including orofacial or choreoathetoid movements.
- preferred_term: Coma
term:
id: HP:0001259
label: Coma
description: Severe decreased level of consciousness.
- preferred_term: Abnormality of the autonomic nervous system
term:
id: HP:0002270
label: Abnormality of the autonomic nervous system
- preferred_term: Central hypoventilation
term:
id: HP:0007110
label: Central hypoventilation
evidence:
- reference: PMID:28972277
reference_title: "High sensitivity and specificity in proposed clinical diagnostic criteria for anti-N-methyl-D-aspartate receptor encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The criteria are satisfied if patients develop four out of six symptom groups within 3 months, together with at least one abnormal investigation (electroencephalography/cerebrospinal fluid) and reasonable exclusion of other disorders."
explanation: >
This pediatric validation study summarizes the practical clinical
criteria used for early recognition before definitive antibody results.
evidence:
- reference: PMID:26906964
reference_title: "A clinical approach to diagnosis of autoimmune encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Because autoantibody test results and response to therapy are not available at disease onset, we based the initial diagnostic approach on neurological assessment and conventional tests that are accessible to most clinicians."
explanation: >
The consensus diagnostic framework supports syndrome-based assessment so
treatment is not delayed while antibody results are pending.
epidemiology:
- name: Age and sex distribution
description: >-
Anti-NMDAR encephalitis predominantly affects young women, with disease onset
concentrated in the second and third decades of life; a large prospective
Chinese cohort reported a female majority and a median age at onset of about
21 years.
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "anti-NMDAR encephalitis is predominantly found in females (65.0%) with the median age at onset of 21 years"
explanation: >-
The 220-patient prospective cohort quantifies the young-female predominance
and median age at onset that characterize the disease.
- name: United States race and ethnicity incidence gradients
description: >-
In Kaiser Permanente Southern California from 2011 through 2022, age- and
sex-standardized incidence varied substantially by race and ethnicity, with
higher incidence estimates among Black, Hispanic, and Asian/Pacific Islander
individuals than among White individuals.
unit: cases per 1 million person-years
evidence:
- reference: PMID:38728608
reference_title: "Racial and Ethnic Disparities in the Incidence of Anti-NMDA Receptor Encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The age-standardized and sex-standardized incidence of anti-NMDAR encephalitis per 1 million person-years was significantly higher in Black (2.94, 95% CI 1.27-4.61), Hispanic (2.17, 95% CI 1.51-2.83), and Asian/Pacific Island persons (2.02, 95% CI 0.77-3.28) compared with White persons (0.40, 95% CI 0.08-0.72)."
explanation: >
The population-based health-system cohort provides standardized incidence
estimates stratified by race and ethnicity.
- name: Geographic and climatic incidence variation
description: >-
A systematic review and meta-analysis found higher reported incidence in
Oceania and South America than in Europe and North America, with latitude
and temperature associations suggesting environmental or geographic risk
modifiers.
unit: cases per 100000 person-years
evidence:
- reference: PMID:37371620
reference_title: "Spatial and Ecological Factors Modulate the Incidence of Anti-NMDAR Encephalitis-A Systematic Review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The reported incidence of anti-NMDAR encephalitis varied considerably among studies and countries, being higher in Oceania and South America (0.2 and 0.16 per 100,000 persons-year, respectively) compared to Europe and North America (0.06 per 100,000 persons-year) (p < 0.01)."
explanation: >
This meta-analysis quantifies regional differences in reported incidence.
pathophysiology:
- name: Triggered Anti-GluN1 Autoimmunity
description: >-
Multiple triggers can initiate B-cell autoimmunity against extracellular
NMDA receptor epitopes, including: tumor antigen exposure from ovarian
teratoma, post-infectious inflammation after herpes simplex encephalitis,
and potentially bacterial infections such as Group A Streptococcus.
cell_types:
- preferred_term: B cell
term:
id: CL:0000236
label: B cell
biological_processes:
- preferred_term: B cell mediated immunity
modifier: INCREASED
term:
id: GO:0019724
label: B cell mediated immunity
downstream:
- target: Intrathecal Anti-NMDAR Antibody Production
description: >
Triggered autoreactive B-cell responses feed local CNS/CSF anti-NMDAR
antibody production.
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Tumours, usually ovarian teratoma, and herpes simplex encephalitis are known triggers of NMDAR autoimmunity."
explanation: >
Tumor or post-infectious triggering supports the upstream edge into
anti-NMDAR antibody production.
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Tumours, usually ovarian teratoma, and herpes simplex encephalitis are known triggers of NMDAR autoimmunity."
explanation: >
The review supports ovarian teratoma and herpes simplex encephalitis as
upstream triggers of anti-NMDAR autoimmunity.
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All teratomas contained nervous tissue; 25 were examined for expression of NMDA receptors, and all were positive (data not shown)."
explanation: >
The original case series supports a mechanistic link between teratoma
neural tissue, NMDA receptor expression, and loss of immune tolerance.
- name: Intrathecal Anti-NMDAR Antibody Production
description: >-
Antibody production is concentrated in the CNS compartment: CSF antibody
levels can exceed serum levels even when the blood-brain barrier is
preserved, supporting intrathecal synthesis by antibody-secreting cells.
cell_types:
- preferred_term: B cell
term:
id: CL:0000236
label: B cell
- preferred_term: plasma cell
term:
id: CL:0000786
label: plasma cell
biological_processes:
- preferred_term: immunoglobulin production
modifier: INCREASED
term:
id: GO:0002377
label: immunoglobulin production
downstream:
- target: Synaptic NMDAR Cluster Loss
description: >
Locally produced antibodies bind extracellular NR1/GluN1 epitopes on
neuronal NMDA receptors.
evidence:
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "Patients’ antibodies labelled nearly all clusters of NMDA receptors (figure 4)."
explanation: >
Patient antibodies directly bind postsynaptic NMDAR clusters, linking
intrathecal antibodies to receptor-cluster effects.
evidence:
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Analysis of normalized concentrations of IgG showed that all 53 patients had higher concentrations of antibodies in CSF than in sera, indicating intrathecal synthesis of antibodies (figure 3)."
explanation: >
Paired CSF/serum analysis supports intrathecal antibody synthesis as part
of the pathogenic cascade.
- reference: PMID:38145121
reference_title: "Anti-NMDAR antibodies, the blood-brain barrier, and anti-NMDAR encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "It is characterized by the existence of antibodies against NMDAR, mainly against the GluN1 subunit, in cerebrospinal fluid (CSF)."
explanation: >
This review identifies CSF anti-GluN1/NMDAR antibodies as the defining
disease marker.
- name: Synaptic NMDAR Cluster Loss
description: >-
Patient IgG binds neuronal surface NMDA receptors and reduces the
cell-surface and postsynaptic receptor cluster pool, producing a selective
and potentially reversible receptor loss rather than fixed neuronal death.
locations:
- preferred_term: brain
term:
id: UBERON:0000955
label: brain
- preferred_term: hippocampal formation
term:
id: UBERON:0002421
label: hippocampal formation
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
biological_processes:
- preferred_term: receptor internalization
modifier: INCREASED
term:
id: GO:0031623
label: receptor internalization
downstream:
- target: Glutamatergic Synaptic Hypofunction
description: >
Reduced surface and postsynaptic NMDAR availability impairs
NMDAR-dependent synaptic signaling.
evidence:
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "Together, these findings show that patients’ antibodies produce a selective and reversible decrease of NMDA-receptor clusters in postsynaptic dendrites."
explanation: >
Reversible postsynaptic NMDAR cluster loss supports downstream synaptic
hypofunction.
evidence:
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "adding patients’ IgG to rat hippocampal neuronal cultures produced a concentration-dependent decrease of the cell-surface fraction of NMDA receptors (figure 5)."
explanation: >
Patient IgG directly reduced cell-surface NMDA receptor availability in
cultured hippocampal neurons.
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "Together, these findings show that patients’ antibodies produce a selective and reversible decrease of NMDA-receptor clusters in postsynaptic dendrites."
explanation: >
The reversibility of postsynaptic NMDAR cluster loss explains why severe
disease can improve after antibody-directed treatment.
- name: Glutamatergic Synaptic Hypofunction
description: >-
Loss of synaptic NMDA receptors disrupts glutamatergic signaling and
synaptic plasticity, providing a mechanistic bridge to psychiatric,
cognitive, seizure, movement, autonomic, and ventilatory manifestations.
locations:
- preferred_term: hippocampal formation
term:
id: UBERON:0002421
label: hippocampal formation
biological_processes:
- preferred_term: glutamate receptor signaling pathway
modifier: DECREASED
term:
id: GO:0007215
label: glutamate receptor signaling pathway
- preferred_term: regulation of synaptic plasticity
modifier: ABNORMAL
term:
id: GO:0048167
label: regulation of synaptic plasticity
downstream:
- target: Neuropsychiatric and Seizure Syndrome
description: >
NMDAR hypofunction maps to the characteristic encephalitis syndrome of
psychiatric symptoms, seizures, movement disorder, coma, autonomic
dysfunction, and hypoventilation.
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "autoantibodies serve as a diagnostic marker and alter NMDAR-related synaptic transmission."
explanation: >
Altered NMDAR-related synaptic transmission is the mechanistic bridge
from receptor hypofunction to the clinical syndrome.
evidence:
- reference: PMID:38145121
reference_title: "Anti-NMDAR antibodies, the blood-brain barrier, and anti-NMDAR encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Recent research suggests that anti-NMDAR antibodies may reduce NMDAR levels in this disorder, compromising synaptic activity in the hippocampus."
explanation: >
The review links anti-NMDAR antibodies to reduced receptor levels and
hippocampal synaptic dysfunction.
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "This feature is compatible with disruption of the mechanisms of synaptic plasticity, thought to underlie learning and memory, in which the NMDA receptors play a key part."
explanation: >
The case series connects persistent amnesia with NMDAR-dependent synaptic
plasticity disruption.
- name: Blood-Brain Barrier and Immune Trafficking
description: >-
Blood-brain barrier function modulates access of antibodies and immune cells
between peripheral and CNS compartments, and inflammatory cytokine findings
support barrier involvement in anti-NMDAR encephalitis.
locations:
- preferred_term: blood brain barrier
modifier: ABNORMAL
term:
id: UBERON:0000120
label: blood brain barrier
biological_processes:
- preferred_term: maintenance of blood-brain barrier
modifier: ABNORMAL
term:
id: GO:0035633
label: maintenance of blood-brain barrier
downstream:
- target: Intrathecal Anti-NMDAR Antibody Production
description: >
Barrier dysfunction may facilitate antibody and immune-cell traffic that
sustains the intrathecal immune compartment.
evidence:
- reference: PMID:38145121
reference_title: "Anti-NMDAR antibodies, the blood-brain barrier, and anti-NMDAR encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The blood-brain barrier (BBB), which separates the brain from the peripheral circulatory system, is crucial for antibodies and immune cells to enter or exit the CNS."
explanation: >
BBB control of antibody and immune-cell traffic supports this edge into
the intrathecal antibody compartment.
evidence:
- reference: PMID:38145121
reference_title: "Anti-NMDAR antibodies, the blood-brain barrier, and anti-NMDAR encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The blood-brain barrier (BBB), which separates the brain from the peripheral circulatory system, is crucial for antibodies and immune cells to enter or exit the CNS."
explanation: >
The review supports BBB involvement as the anatomical interface governing
antibody and immune-cell traffic.
- reference: PMID:38145121
reference_title: "Anti-NMDAR antibodies, the blood-brain barrier, and anti-NMDAR encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The findings of cytokines in this disorder support the involvement of the BBB."
explanation: >
Cytokine findings are cited as evidence that BBB dysfunction participates
in anti-NMDAR encephalitis biology.
- name: Neuropsychiatric and Seizure Syndrome
description: >-
The downstream clinical syndrome reflects reversible NMDAR hypofunction and
encephalitic network dysfunction, with psychiatric symptoms and seizures
most often reported in large cohorts and additional movement, consciousness,
autonomic, and ventilatory involvement in severe disease.
locations:
- preferred_term: brain
term:
id: UBERON:0000955
label: brain
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The identification of anti-NMDA receptor (NMDAR) encephalitis about 12 years ago made it possible to recognise that some patients with rapidly progressive psychiatric symptoms or cognitive impairment, seizures, abnormal movements, or coma of unknown cause, had an autoimmune disease."
explanation: >
The review summarizes the characteristic neurologic and psychiatric
syndrome produced by anti-NMDAR encephalitis.
phenotypes:
- name: Psychosis
category: Psychiatric
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: Psychosis
term:
id: HP:0000709
label: Psychosis
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The most common clinical manifestations of the anti-NMDAR encephalitis were psychosis (182, 82.7%) and seizures (178, 80.9%)."
explanation: >
Psychosis occurred in 82.7% of the 220-patient cohort, placing it in the
VERY_FREQUENT frequency band.
- name: Seizure
category: Neurologic
frequency: VERY_FREQUENT
diagnostic: true
phenotype_term:
preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The most common clinical manifestations of the anti-NMDAR encephalitis were psychosis (182, 82.7%) and seizures (178, 80.9%)."
explanation: >
Seizures occurred in 80.9% of the 220-patient cohort, placing them in the
VERY_FREQUENT frequency band.
- name: Dyskinesia
category: Neurologic
frequency: FREQUENT
phenotype_term:
preferred_term: Dyskinesia
term:
id: HP:0100660
label: Dyskinesia
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Movement disorder presented more often in patients younger than 18 years than adult patients (38/69, 55.1% vs 56/151, 37.1%, p = 0.01)."
explanation: >
The cohort reports movement disorder in 94/220 patients overall, with
higher frequency in children; dyskinesia is used as the HPO-grounded
movement-disorder phenotype.
- name: Memory Impairment
category: Neurologic
frequency: FREQUENT
phenotype_term:
preferred_term: Memory impairment
term:
id: HP:0002354
label: Memory impairment
evidence:
- reference: PMID:39566012
reference_title: "Long-Term Cognitive, Functional, and Patient-Reported Outcomes in Patients With Anti-NMDAR Encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Beyond 36 months (n = 44), 34% of patients had a persistent impairment (z-score <-1.5 SD) and 65% scored below-average (<-1 SD) in 1 or more cognitive domains, despite a \"favorable\" outcome measured by mRS (≤2) in the majority (91%)."
explanation: >
Long-term cognitive impairment persisted in a substantial subset despite
favorable mRS outcomes; memory was among the most affected domains.
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "A characteristic feature of patients who recover from anti-NMDA-receptor encephalitis is a persisting amnesia of the entire process (data not shown)."
explanation: >
The early case series highlights persistent amnesia as a characteristic
recovery-phase cognitive feature.
- name: Speech and Language Dysfunction
category: Neurologic
diagnostic: true
phenotype_term:
preferred_term: Language impairment
term:
id: HP:0002463
label: Language impairment
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "acute onset of 1 or more of the 8 major groups of manifestations: psychosis, memory deficit, speech disturbance, seizures, movement disorder, loss of consciousness, autonomic dysfunction, and central hypoventilation"
explanation: >
Speech disturbance is included among the major clinical manifestation
groups used for anti-NMDAR encephalitis case inclusion in this cohort.
- reference: PMID:39566012
reference_title: "Long-Term Cognitive, Functional, and Patient-Reported Outcomes in Patients With Anti-NMDAR Encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Most affected were memory (mean -0.67 ± 0.89 SD, p = 0.25) and language (-0.75 ± 1.06 SD, p = 0.23)."
explanation: >
Long-term follow-up identifies language as one of the most affected
cognitive domains after anti-NMDAR encephalitis.
- name: Coma
category: Neurologic
phenotype_term:
preferred_term: Coma
term:
id: HP:0001259
label: Coma
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "some patients with rapidly progressive psychiatric symptoms or cognitive impairment, seizures, abnormal movements, or coma of unknown cause, had an autoimmune disease."
explanation: >
Coma is listed among the severe neurologic presentations of anti-NMDAR
encephalitis.
- name: Autonomic Dysfunction
category: Neurologic
frequency: FREQUENT
phenotype_term:
preferred_term: Abnormality of the autonomic nervous system
term:
id: HP:0002270
label: Abnormality of the autonomic nervous system
evidence:
- reference: PMID:33589542
reference_title: "Long-term Functional Outcomes and Relapse of Anti-NMDA Receptor Encephalitis: A Cohort Study in Western China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "We reported that 48.4% of patients displayed autonomic symptoms, and other studies on anti-NMDAR encephalitis also reported elevated incidences of autonomic dysfunction (Titulaer: 37%–48%; Dalmau: 69%)."
explanation: >
The Western China cohort reports autonomic symptoms in nearly half of
patients, placing the phenotype in the FREQUENT frequency band.
- name: Central Hypoventilation
category: Respiratory
phenotype_term:
preferred_term: Central hypoventilation
term:
id: HP:0007110
label: Central hypoventilation
evidence:
- reference: PMID:30578370
reference_title: "A score that predicts 1-year functional status in patients with anti-NMDA receptor encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "movement disorder (p = 0.001), central hypoventilation (p < 0.001), elevated CSF white blood cell count (p < 0.001), elevated CSF protein level (p = 0.027), and abnormal MRI (p = 0.002) were associated with 1-year functional status in univariate analysis."
explanation: >
Central hypoventilation is identified as a clinically important feature
associated with functional outcome.
- name: EEG Abnormality
category: Neurologic
frequency: FREQUENT
phenotype_term:
preferred_term: EEG abnormality
term:
id: HP:0002353
label: EEG abnormality
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Abnormal EEG findings were seen in 113 (51.4%) patients: 102 (46.4%) had slow activity and 14 (6.4%) epileptic discharges."
explanation: >
EEG abnormalities occurred in 51.4% of the 220-patient cohort.
- name: CSF Pleocytosis
category: Neurologic
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: CSF pleocytosis
term:
id: HP:0012229
label: CSF pleocytosis
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Of note, 81.3% of the patients had pleocytosis, the median white blood cell count was 14.0 (IQR 7.0–22.5) × 106/L, and 90.9% were of mononuclear cells (i.e., lymphocyte and monocytes)."
explanation: >
CSF pleocytosis occurred in 81.3% of the prospective cohort, placing it
in the VERY_FREQUENT frequency band.
biochemical:
- name: CSF Anti-NMDAR IgG
presence: Positive
context: Cerebrospinal fluid
notes: IgG antibodies target the GluN1/NR1 subunit of the NMDA receptor.
evidence:
- reference: PMID:38145121
reference_title: "Anti-NMDAR antibodies, the blood-brain barrier, and anti-NMDAR encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "It is characterized by the existence of antibodies against NMDAR, mainly against the GluN1 subunit, in cerebrospinal fluid (CSF)."
explanation: >
CSF anti-GluN1/NMDAR antibodies are the defining diagnostic biomarker.
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients (100%) were positive for anti-NMDAR antibodies in CSF, and 157 (71.4%) were positive in serum."
explanation: >
Paired testing in the 220-patient cohort supports high diagnostic value
of CSF antibody detection relative to serum.
- name: CSF White Blood Cell Count
presence: Elevated
context: Cerebrospinal fluid
evidence:
- reference: PMID:30578370
reference_title: "A score that predicts 1-year functional status in patients with anti-NMDA receptor encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Intensive care unit admission, treatment delay >4 weeks, lack of clinical improvement within 4 weeks, abnormal MRI, and CSF white blood cell count >20 cells/μL were independent predictors for outcome in multivariate regression modeling."
explanation: >
Elevated CSF white blood cell count is both a diagnostic inflammatory
marker and one component of the NEOS prognostic score.
- name: Serum Anti-NMDAR IgG
presence: Positive in subset
context: Serum
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients (100%) were positive for anti-NMDAR antibodies in CSF, and 157 (71.4%) were positive in serum."
explanation: >
Serum antibody positivity is common but less consistently detected than
CSF positivity in paired testing.
environmental:
- name: Ovarian teratoma
description: >
Ovarian teratoma is a recognized tumor trigger and should prompt tumor
screening and removal when identified.
effect: Triggers or sustains NMDAR autoimmunity
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Tumours, usually ovarian teratoma, and herpes simplex encephalitis are known triggers of NMDAR autoimmunity."
explanation: >
The review identifies ovarian teratoma as a common tumor trigger.
- reference: PMID:38728608
reference_title: "Racial and Ethnic Disparities in the Incidence of Anti-NMDA Receptor Encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Ovarian teratomas were found in 58.3% of Black female individuals and 10%-28.6% in other groups."
explanation: >
A US incidence cohort shows ovarian teratoma frequency varies across
female patient groups.
- name: Herpes simplex encephalitis
description: >
Herpes simplex encephalitis can precede anti-NMDAR encephalitis and defines
a post-infectious trigger subgroup with poorer long-term prognosis in
recent cohort data.
effect: Post-infectious trigger of NMDAR autoimmunity
evidence:
- reference: PMID:39147951
reference_title: "Specific clinical and radiological characteristics of anti-NMDA receptor autoimmune encephalitis following herpes encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Herein, patients with HSE-NMDARE have a poorer long-term prognosis than patients with regular NMDARE."
explanation: >
This cohort supports post-HSE anti-NMDAR encephalitis as a clinically
distinct and prognostically important subgroup.
- name: Group A Streptococcus infection
description: >
Streptococcal infection may trigger or exacerbate anti-NMDAR autoimmunity,
though the mechanism and causal relationship remain incompletely
characterized in the literature. When streptococcal infection is identified
concurrent with anti-NMDAR disease, careful evaluation is warranted.
effect: May trigger anti-NMDAR autoimmunity
evidence:
- reference: PMID:42344622
reference_title: "A Case of Ovarian Teratoma-Associated Anti-NMDA Receptor Encephalitis in the Presence of Group A Streptococcus Infection."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "The observed association between Group A Streptococcus infection preceding symptom onset suggests a possible infectious trigger leading to an immunologic response and subsequent anti-NMDAR encephalitis; however, there is limited evidence of a causal relationship in the literature."
explanation: >
A case report documents concurrent Group A Streptococcus infection with
ovarian teratoma-associated anti-NMDAR encephalitis, with temporal
precedence suggesting a possible infectious trigger role.
- name: Geographic and climatic factors
description: >
Latitude, temperature, and ultraviolet exposure have been associated with
reported incidence variation, suggesting environmental modulation of risk.
effect: Modifies disease incidence
evidence:
- reference: PMID:37371620
reference_title: "Spatial and Ecological Factors Modulate the Incidence of Anti-NMDAR Encephalitis-A Systematic Review."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "This study provides the first evidence that geographic and climatic factors including latitude, mean annual temperature, and ultraviolet exposure, might modify disease risk."
explanation: >
Ecologic evidence suggests environmental risk modification, but causality
and individual-level mechanisms remain uncertain.
progression:
- phase: Prodromal and subacute neuropsychiatric onset
notes: >
Patients typically develop a rapidly progressive encephalitic syndrome in
which psychiatric symptoms, cognitive impairment, seizures, abnormal
movements, or coma may precede recognition of autoimmune disease.
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "some patients with rapidly progressive psychiatric symptoms or cognitive impairment, seizures, abnormal movements, or coma of unknown cause, had an autoimmune disease."
explanation: >
The review describes the subacute syndrome that led to recognition of
anti-NMDAR encephalitis.
- phase: Acute severe encephalitis and prognostic assessment
notes: >
Acute severity is captured by ICU admission, treatment delay, early lack of
improvement, abnormal MRI, and CSF WBC elevation; these features compose the
NEOS prognostic score for 1-year functional outcome.
evidence:
- reference: PMID:30578370
reference_title: "A score that predicts 1-year functional status in patients with anti-NMDA receptor encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Intensive care unit admission, treatment delay >4 weeks, lack of clinical improvement within 4 weeks, abnormal MRI, and CSF white blood cell count >20 cells/μL were independent predictors for outcome in multivariate regression modeling."
explanation: >
The NEOS study defines acute predictors that stratify expected 1-year
functional recovery.
- phase: Recovery and relapse risk
notes: >
Recovery often continues for months to years, but relapse occurs in a
clinically important minority and cognitive/psychosocial deficits can
persist after apparently favorable mRS recovery.
evidence:
- reference: PMID:23290630
reference_title: "Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Outcomes continued to improve for up to 18 months after symptom onset."
explanation: >
The 577-patient observational cohort shows prolonged recovery after
disease onset.
- reference: PMID:33589542
reference_title: "Long-term Functional Outcomes and Relapse of Anti-NMDA Receptor Encephalitis: A Cohort Study in Western China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Overall, 15.9% of the patients had one or multiple relapses, with 82.0% experiencing the first relapse within 24 months and 76.9% experiencing relapses that were less severe than the initial episodes."
explanation: >
The Western China cohort quantifies relapse frequency and timing.
- reference: PMID:39566012
reference_title: "Long-Term Cognitive, Functional, and Patient-Reported Outcomes in Patients With Anti-NMDAR Encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Recovery from anti-NMDAR encephalitis may continue for 3 years, with risk of persisting cognitive deficits, notably in memory and language, and sequelae in social functioning, energy levels, and well-being."
explanation: >
Long-term follow-up shows mRS can miss persistent cognitive and
patient-reported impairment.
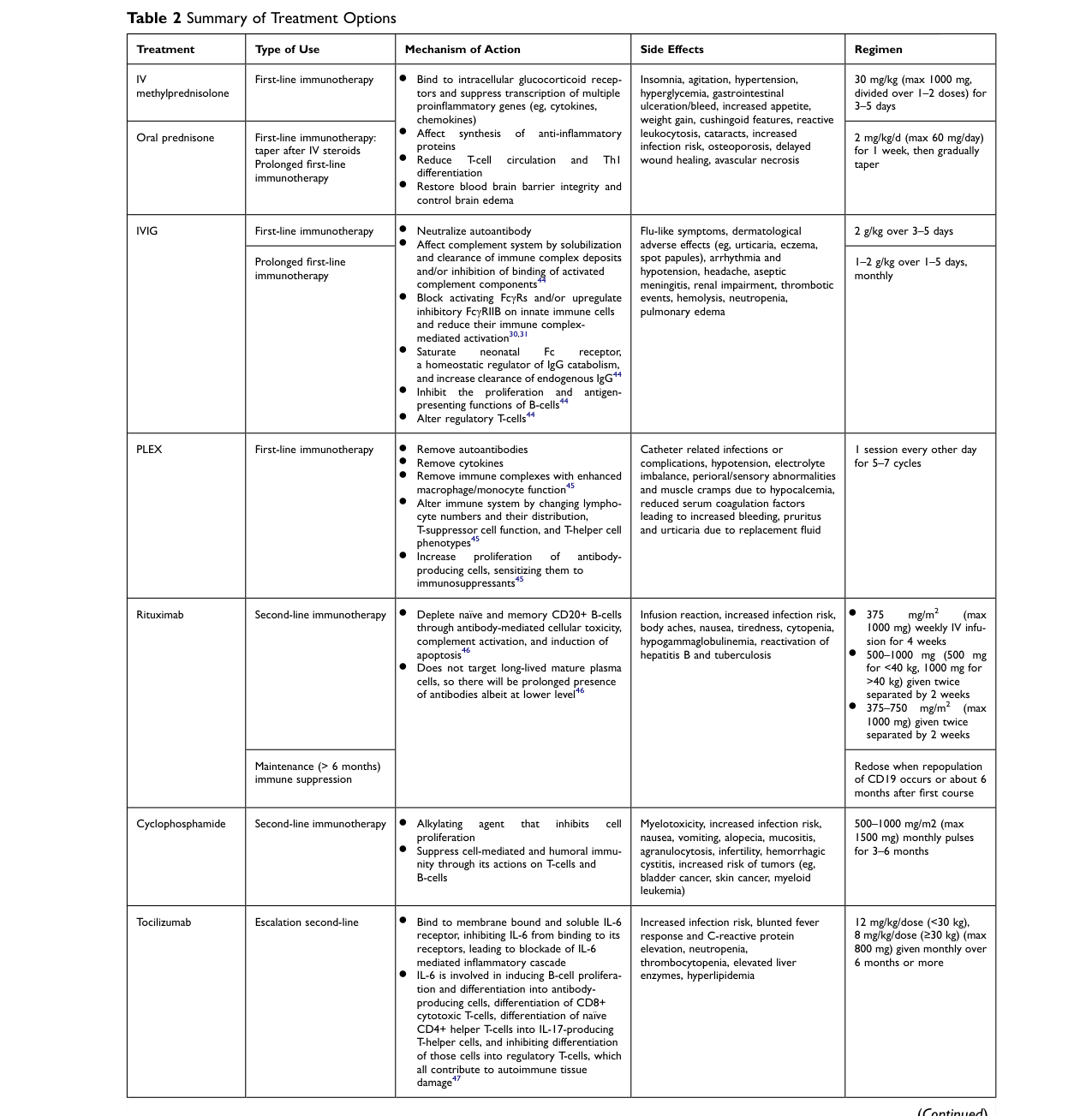
treatments:
- name: First-Line Immunotherapy
description: >
Initial treatment uses corticosteroids, intravenous immunoglobulin, plasma
exchange, or combinations of these therapies, often alongside tumor removal
when a tumor is identified.
treatment_term:
preferred_term: immunotherapy
term:
id: MAXO:0001002
label: immunotherapy procedure
target_mechanisms:
- target: Intrathecal Anti-NMDAR Antibody Production
treatment_effect: INHIBITS
description: >
First-line immunotherapy suppresses the inflammatory antibody-mediated
process and can reduce circulating or intrathecal pathogenic antibody
effects.
evidence:
- reference: PMID:23290630
reference_title: "Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Most patients with anti-NMDAR encephalitis respond to immunotherapy."
explanation: >
Clinical response to immunotherapy supports inhibition of the
antibody-mediated immune process.
evidence:
- reference: PMID:23290630
reference_title: "Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Treatment included first-line immunotherapy (steroids, intravenous immunoglobulin, plasmapheresis), second-line immunotherapy (rituximab, cyclophosphamide), and tumour removal."
explanation: >
The large observational cohort defines the core first-line and
second-line treatment categories used in anti-NMDAR encephalitis.
- reference: PMID:23290630
reference_title: "Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "472 (94%) underwent first-line immunotherapy or tumour removal, resulting in improvement within 4 weeks in 251 (53%)."
explanation: >
Most assessable patients received first-line treatment or tumor removal,
with early improvement in just over half.
- name: High-Dose Corticosteroid Therapy
description: >
Corticosteroids are commonly used in first-line acute immunotherapy,
including pulsed intravenous methylprednisolone in severe disease.
treatment_term:
preferred_term: systemic corticosteroid therapy
term:
id: NCIT:C122080
label: Systemic Corticosteroid Therapy
target_mechanisms:
- target: Triggered Anti-GluN1 Autoimmunity
treatment_effect: INHIBITS
description: Corticosteroids suppress acute CNS and systemic inflammation.
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "A total of 208 (94.5%) patients received steroids, of whom 103 (46.8%) received pulsed IV methylprednisolone."
explanation: >
The cohort documents corticosteroid use as a major acute
immunosuppressive treatment.
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "A total of 208 (94.5%) patients received steroids, of whom 103 (46.8%) received pulsed IV methylprednisolone."
explanation: >
This prospective cohort documents frequent use of corticosteroids and
pulsed IV methylprednisolone in real-world acute treatment.
- name: Plasma Exchange
description: >
Plasma exchange is used as an acute first-line or escalation strategy to
remove pathogenic antibodies.
treatment_term:
preferred_term: plasmapheresis
term:
id: NCIT:C15304
label: Plasmapheresis
target_mechanisms:
- target: Intrathecal Anti-NMDAR Antibody Production
treatment_effect: INHIBITS
description: >
Plasma exchange lowers pathogenic antibody burden, especially the
circulating component.
evidence:
- reference: PMID:23290630
reference_title: "Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Treatment included first-line immunotherapy (steroids, intravenous immunoglobulin, plasmapheresis), second-line immunotherapy (rituximab, cyclophosphamide), and tumour removal."
explanation: >
Plasmapheresis is explicitly included among first-line antibody-directed
immunotherapies.
evidence:
- reference: PMID:23290630
reference_title: "Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Treatment included first-line immunotherapy (steroids, intravenous immunoglobulin, plasmapheresis), second-line immunotherapy (rituximab, cyclophosphamide), and tumour removal."
explanation: >
The cohort explicitly includes plasmapheresis among first-line
immunotherapies.
- name: Intravenous Immunoglobulin
description: >
Intravenous immunoglobulin is a first-line immunotherapy used alone or with
corticosteroids and/or plasma exchange.
treatment_term:
preferred_term: intravenous immunoglobulin therapy
term:
id: NCIT:C121331
label: Intravenous Immunoglobulin Therapy
target_mechanisms:
- target: Triggered Anti-GluN1 Autoimmunity
treatment_effect: MODULATES
description: >
IVIG modulates immune effector pathways and pathogenic autoantibody
activity.
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "IVIG was administered to 199 (90.5%) patients, and 7 (3.2%) patients underwent PE."
explanation: >
High use of IVIG in this cohort supports IVIG as a core immune-modulating
acute therapy.
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "IVIG was administered to 199 (90.5%) patients, and 7 (3.2%) patients underwent PE."
explanation: >
IVIG was used in most patients in this prospective Chinese cohort.
- name: Rituximab or Cyclophosphamide Second-Line Immunotherapy
description: >
Patients who fail first-line therapy may receive rituximab and/or
cyclophosphamide as second-line immunotherapy.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: rituximab
term:
id: NCIT:C1702
label: Rituximab
- preferred_term: cyclophosphamide
term:
id: CHEBI:4027
label: cyclophosphamide
target_mechanisms:
- target: Intrathecal Anti-NMDAR Antibody Production
treatment_effect: INHIBITS
description: >
B-cell depletion or cytotoxic immunosuppression reduces autoreactive
lymphocyte populations driving antibody production.
evidence:
- reference: PMID:23290630
reference_title: "Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Of 221 patients who did not improve with first-line treatment, 125 (57%) received second-line immunotherapy that resulted in a better outcome (mRS 0-2) than those who did not"
explanation: >
Better outcomes after second-line rituximab/cyclophosphamide support
targeting persistent immune antibody production.
evidence:
- reference: PMID:23290630
reference_title: "Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Of 221 patients who did not improve with first-line treatment, 125 (57%) received second-line immunotherapy that resulted in a better outcome (mRS 0-2) than those who did not"
explanation: >
The observational cohort supports second-line immunotherapy for patients
not improving after first-line therapy.
- name: Long-Term Mycophenolate or Azathioprine Immunotherapy
description: >
Mycophenolate mofetil and azathioprine are used as longer-term
immunosuppressive treatment in selected severe, refractory, or relapsing
anti-NMDAR encephalitis cases.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: mycophenolate mofetil
term:
id: CHEBI:8764
label: mycophenolate mofetil
- preferred_term: azathioprine
term:
id: CHEBI:2948
label: azathioprine
target_mechanisms:
- target: Intrathecal Anti-NMDAR Antibody Production
treatment_effect: INHIBITS
description: >
Long-term steroid-sparing immunosuppression is used to suppress ongoing
autoimmune activity and reduce relapse-management burden.
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Long-term immunotherapy was administered mainly in patients who were enrolled later, as an add-on therapy for severe or refractory patients in the acute phase, or as maintenance therapy to prevent and manage relapses."
explanation: >
The cohort describes long-term immunotherapy as an add-on or
maintenance strategy for severe, refractory, or relapsing disease.
evidence:
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Long-term immunotherapy was administered mainly in patients who were enrolled later, as an add-on therapy for severe or refractory patients in the acute phase, or as maintenance therapy to prevent and manage relapses."
explanation: >
This prospective cohort explicitly identifies the treatment phase and
clinical role of long-term immunotherapy.
- reference: PMID:31619447
reference_title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "In general, MMF was administered in 109 (49.5%) patients, 55 of whom at onset and 54 after relapse, and AZA was administered in 8 (3.6%) patients."
explanation: >
Mycophenolate mofetil and azathioprine use is quantified in the cohort,
supporting these agents as long-term immunotherapy options.
- name: Tumor Removal
description: >
Surgical removal of an associated ovarian teratoma or other tumor is part of
standard management when a tumor is identified.
treatment_term:
preferred_term: surgical procedure
term:
id: MAXO:0000004
label: surgical procedure
target_mechanisms:
- target: Triggered Anti-GluN1 Autoimmunity
treatment_effect: INHIBITS
description: >
Removing a teratoma eliminates a potential antigen source sustaining
NMDAR autoimmunity.
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "About 80% of patients improve with immunotherapy and, if needed, tumour removal, but the recovery is slow."
explanation: >
Tumor removal is linked with clinical improvement when tumor-associated
disease is present.
evidence:
- reference: PMID:31326280
reference_title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "About 80% of patients improve with immunotherapy and, if needed, tumour removal, but the recovery is slow."
explanation: >
The review identifies tumor removal as part of effective management when
tumor-associated disease is present.
clinical_trials:
- name: NCT03274375
phase: PHASE_II
status: RECRUITING
description: >
Prospective study of immunoadsorption therapy for severe pediatric
anti-NMDAR encephalitis.
target_phenotypes:
- preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
- preferred_term: Dyskinesia
term:
id: HP:0100660
label: Dyskinesia
evidence:
- reference: clinicaltrials:NCT03274375
reference_title: "Prospective Assessment of Efficacy of Immunoadsorption Therapy in Managing Childhood NMDA-Receptor (NMDAR) Antibodies Encephalitis"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The purpose of the study is to assess the efficacy of immunoadsorption therapy (IA) on improving the neurological status of severe pediatric anti-NMDAR encephalitis patients."
explanation: >
ClinicalTrials.gov describes the trial as testing immunoadsorption in
severe pediatric anti-NMDAR encephalitis.
- name: NCT06183788
status: RECRUITING
description: >
AMENDS study of symptoms, biomarkers, mechanisms, remote follow-up tools,
and cognitive rehabilitation in the prolonged recovery stage.
target_phenotypes:
- preferred_term: Memory impairment
term:
id: HP:0002354
label: Memory impairment
evidence:
- reference: clinicaltrials:NCT06183788
reference_title: "Antibody-mediated NMDA Receptor Encephalitis: Symptoms, Biomarkers, and Mechanisms of the Prolonged Recovery Stage"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "In Aim 1, the post-acute stage will be clinically characterized, tools to remotely follow cognitive, behavioral and psychiatric deficits will be provided, and the impact of cognitive rehabilitation will be assessed."
explanation: >
The trial targets long-term cognitive, behavioral, and psychiatric
deficits after the acute stage.
- name: NCT06023160
status: RECRUITING
description: >
International cohort study developing the NEOSII score to predict long-term
outcome and response to first-line immunotherapy at diagnosis.
evidence:
- reference: clinicaltrials:NCT06023160
reference_title: "Predicting Functional Outcome and Response to Therapy of Anti-NMDAR Encephalitis at Diagnosis: The NEOSII Score"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The goal of this international cohort study is to develop a prediction model for long-term outcome and response to first-line immunotherapy of anti-NMDAR Encephalitis, already at the moment of diagnosis."
explanation: >
The study extends prognostic modeling to diagnosis-time prediction of
long-term outcome and treatment response.
datasets:
references:
- reference: DOI:10.1007/s00415-024-12615-7
title: Specific clinical and radiological characteristics of anti-NMDA receptor autoimmune encephalitis following herpes encephalitis
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1038/s41598-020-67485-6
title: "Influencing electroclinical features and prognostic factors in patients with anti-NMDAR encephalitis: a cohort follow-up study in Chinese patients"
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1111/dmcn.13579
title: High sensitivity and specificity in proposed clinical diagnostic criteria for anti-N-methyl-D-aspartate receptor encephalitis
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1152/physrev.00010.2016
title: Autoantibodies to Synaptic Receptors and Neuronal Cell Surface Proteins in Autoimmune Diseases of the Central Nervous System
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1212/NXI.0000000000000633
title: Anti-NMDAR encephalitis
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1212/NXI.0000000000000958
title: Long-term Functional Outcomes and Relapse of Anti-NMDA Receptor Encephalitis
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1212/NXI.0000000000200255
title: Racial and Ethnic Disparities in the Incidence of Anti-NMDA Receptor Encephalitis
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1212/WNL.0000000000003414
title: NMDA receptor encephalitis and other antibody-mediated disorders of the synapse
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1212/WNL.0000000000006783
title: A score that predicts 1-year functional status in patients with anti-NMDA receptor encephalitis
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1212/WNL.0000000000207221
title: Predictive Value of Serum Neurofilament Light Chain Levels in Anti-NMDA Receptor Encephalitis
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1212/WNL.0000000000210109
title: Long-Term Cognitive, Functional, and Patient-Reported Outcomes in Patients With Anti-NMDAR Encephalitis
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.2147/IJGM.S397429
title: "Anti-NMDA Receptor Autoimmune Encephalitis: Diagnosis and Management Strategies"
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.3389/fneur.2023.1283511
title: Anti-NMDAR antibodies, the blood-brain barrier, and anti-NMDAR encephalitis
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.3390/biomedicines11061525
title: Spatial and Ecological Factors Modulate the Incidence of Anti-NMDAR Encephalitis-A Systematic Review
found_in:
- Anti-NMDA_Receptor_Encephalitis-deep-research-falcon.md
findings: []
- reference: PMID:17262855
title: Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma.
findings: []
- reference: PMID:18851928
title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
findings: []
- reference: PMID:23290630
title: "Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study."
findings: []
- reference: PMID:26906964
title: A clinical approach to diagnosis of autoimmune encephalitis.
findings: []
- reference: PMID:28972277
title: High sensitivity and specificity in proposed clinical diagnostic criteria for anti-N-methyl-D-aspartate receptor encephalitis.
findings: []
- reference: PMID:30578370
title: A score that predicts 1-year functional status in patients with anti-NMDA receptor encephalitis.
findings: []
- reference: PMID:31326280
title: "An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models."
findings: []
- reference: PMID:31619447
title: "Anti-NMDAR encephalitis: A single-center, longitudinal study in China."
findings: []
- reference: PMID:33589542
title: "Long-term Functional Outcomes and Relapse of Anti-NMDA Receptor Encephalitis: A Cohort Study in Western China."
findings: []
- reference: PMID:37371620
title: Spatial and Ecological Factors Modulate the Incidence of Anti-NMDAR Encephalitis-A Systematic Review.
findings: []
- reference: PMID:38145121
title: "Anti-NMDAR antibodies, the blood-brain barrier, and anti-NMDAR encephalitis."
findings: []
- reference: PMID:38728608
title: Racial and Ethnic Disparities in the Incidence of Anti-NMDA Receptor Encephalitis.
findings: []
- reference: PMID:39147951
title: Specific clinical and radiological characteristics of anti-NMDA receptor autoimmune encephalitis following herpes encephalitis.
findings:
- statement: >-
Severity-associated criteria on the initial MRI (extensive lesions and
bilateral diffusion-weighted imaging abnormalities) are more frequent in
HSE-NMDARE than in regular HSE and may help flag patients at higher risk of
developing post-herpetic NMDARE.
supporting_text: "patients with HSE-NMDARE more often achieved severity-associated criteria on initial MRIs, with extensive lesions (11/11, 100% vs 10/21, 48%, p = 0.005) and bilateral diffusion-weighted imaging sequence abnormalities (9/10, 90% vs 6/21, 29%, p = 0.002)"
- reference: PMID:39566012
title: Long-Term Cognitive, Functional, and Patient-Reported Outcomes in Patients With Anti-NMDAR Encephalitis.
findings: []
- reference: PMID:42344622
title: A Case of Ovarian Teratoma-Associated Anti-NMDA Receptor Encephalitis in the Presence of Group A Streptococcus Infection.
findings: []
- reference: clinicaltrials:NCT03274375
title: Prospective Assessment of Efficacy of Immunoadsorption Therapy in Managing Childhood NMDA-Receptor (NMDAR) Antibodies Encephalitis
findings: []
- reference: clinicaltrials:NCT06183788
title: "Antibody-mediated NMDA Receptor Encephalitis: Symptoms, Biomarkers, and Mechanisms of the Prolonged Recovery Stage"
findings: []
- reference: clinicaltrials:NCT06023160
title: "Predicting Functional Outcome and Response to Therapy of Anti-NMDAR Encephalitis at Diagnosis: The NEOSII Score"
findings: []
discussions:
- discussion_id: gap_nmdare_gas_trigger
prompt: >-
Can Group A Streptococcus infection independently trigger anti-NMDAR
autoimmunity, or is co-occurring GAS incidental in teratoma-bearing patients?
kind: KNOWLEDGE_GAP
status: OPEN
attaches_to:
- pathophysiology#Triggered Anti-GluN1 Autoimmunity
rationale: >-
A single case report (PMID:42344622) documents concurrent GAS infection
in a patient with bilateral ovarian teratomas and anti-NMDAR encephalitis,
but the paper's own conclusion notes limited evidence of a causal relationship.
Whether GAS triggers molecular mimicry or epitope spreading against NMDAR
epitopes — analogous to the established post-HSE pathway — remains untested.
proposed_experiments:
- experiment_id: exp_nmdare_gas_serology_cohort
name: GAS serology screening in non-teratoma NMDARE cohorts
description: >-
Systematic screening for GAS serology in non-teratoma NMDARE cohorts to
determine whether GAS infection precedes disease onset independently of
teratoma presence.
- experiment_id: exp_nmdare_gas_cross_reactivity
name: GAS M-protein cross-reactivity testing against GluN1
description: >-
In vitro cross-reactivity testing of GAS M-protein epitopes against GluN1
to evaluate molecular mimicry as a potential mechanistic pathway.
evidence:
- reference: PMID:42344622
reference_title: "A Case of Ovarian Teratoma-Associated Anti-NMDA Receptor Encephalitis in the Presence of Group A Streptococcus Infection."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "The observed association between Group A Streptococcus infection preceding symptom onset suggests a possible infectious trigger leading to an immunologic response and subsequent anti-NMDAR encephalitis; however, there is limited evidence of a causal relationship in the literature."
explanation: >-
Case-level co-occurrence in a teratoma-bearing patient; causal role of GAS
not established.
References & Deep Research
References
32Deep Research
2Asta Literature Retrieval: Pathophysiology and clinical mechanisms of Anti-NMDA Receptor Encephalitis. Core disease mechanisms, molecular and ce...
This report is retrieval-only and is generated directly from Asta results.
- Papers retrieved: 18
- Snippets retrieved: 20
Relevant Papers
[1] Global study of anti-NMDA encephalitis: a bibliometric analysis from 2005 to 2023
- Authors: Xinyue Song, Zixin Luo, Duoqin Huang, Jialian Lv, Li Xiao et al.
- Year: 2024
- Venue: Frontiers in Neurology
- URL: https://www.semanticscholar.org/paper/b57cb6594188ed0e2575076019dd6ad402d87ca0
- DOI: 10.3389/fneur.2024.1387260
- PMID: 38711554
- PMCID: 11070467
- Citations: 4
- Summary: A bibliometric and visualization analysis from 2005 to 2023 shows that the number of studies on anti-NMDA encephalitis is generally increasing year by year, and it is a hot disease pursued by researchers.
- Evidence snippets:
- Snippet 1 (score: 0.553) > Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis is an autoimmune-mediated disease characterized by a complex neuropsychiatric syndrome, and an antibody to cerebrospinal fluid (CSF) targeting the GluN1 subunit of NMDAR exists (14,15), a brain parenchymal inflammation associated with autoimmune-related neurologic dysfunction (16). Anti-NMDA receptor encephalitis was first reported in 2005, when symptoms of psychotic features, memory loss, and altered consciousness were found in four young women with ovarian teratomas (17). In 2007, a study found a new autoantibody in cerebrospinal fluid (CSF) or serum of 12 female patients with an early psychotic This discovery ushered in a new era of diagnostic medicine (18). The etiology of anti-NMDA encephalitis is, for the moment, uncertain, but some studies suggest that it may be able to be triggered by viruses, vaccines or tumors (19,20). IgG antibodies targeting the GluN1 subunit of the NMDA receptor (NMDAR) are key mediators in the pathogenesis of the disease (21). Antibody-mediated NMDAR dysfunction leads to severe psychiatric symptoms, including memory loss (22), dyskinesia (23), psychotic symptoms (24), drowsiness, seizures (25), impaired consciousness, and even coma in severe cases. Early recognition and rapid activation of a range of immunotherapies may be able to improve the prognosis of patients with anti-NMDA encephalitis. Clinical presentation, cerebrospinal fluid examination, neuroimaging, and electroencephalography can be used for diagnostic typing of encephalitis (26), and are important modalities for guiding the clinical approach to treatment and achieving a favorable outcome for patients. As research progresses, relevant animal models have begun to reveal underlying pathogenic mechanisms and will lead to the development of new therapies in addition to immunotherapy (3).
- Snippet 2 (score: 0.406) > However, it is worth noting that there may be some differences between children and adults (33), and we believe that the most common clinical manifestations of anti-NMDA receptor encephalitis in children are epilepsy, movement disorders, and personality changes, as well as the incidence of comorbid tumors in pediatric patients is lower than in adults (17). The younger the age, the lower the likelihood of tumor development, suggesting that the pathogenesis may differ between children and adults (34). Research into potential clinical treatment modalities for anti-NMDA encephalitis has been an outbreak hotspot in recent years. The treatment of anti-NMDA receptor encephalitis mainly relies on searching for the relevant causes and treating the causes as much as possible, including receiving immunotherapy, supportive therapy, Second-line drug therapy, including rituximab and cyclophosphamide, can often be considered when patients with anti-NMDA receptor encephalitis do not respond significantly to first-line drug therapy, but overall immunotherapy for anti-NMDA receptor encephalitis remains the main effective approach at present. This study focuses on a new type of autoimmune encephalitis anti-NMDA encephalitis. And the discovery of NMDA receptor has opened up the research field of anti-NMDA encephalitis which reveals the pathogenesis of anti-NMDA encephalitis and also provides an important theoretical basis for the development of drugs targeting NMDA receptor which brings a new hope for the treatment of patients. Among the six clusters in the keyword timeline graph two are related to anti-NMDA encephalitis and two are related to anti-NMDA receptor just using different forms to convey the same meaning. In addition through the timeline we found that in recent years the research on anti-NMDA encephalitis has gradually shifted from the previous basic research to focus on the clinical direction including its clinical features outcomes and related case reports but there are still fewer research articles suggesting that future scholars can focus on the clinical aspect of the research to explore new manifestations and characteristics.
- Snippet 3 (score: 0.402) > Keyword clustering mapping showed that studies in the field of anti-NMDA encephalitis were mainly centered on its definition, pathogenesis, clinical manifestations, diagnostic indicators, therapeutic modalities, and case reports, and the results confirmed that anti-NMDA encephalitis is an autoimmune-mediated disease manifesting as a complex neuropsychiatric syndrome, which results in a wide range of neurological symptoms, including psychiatric symptoms, movement disorders, memory disorders (14). And according to the clustering results, for cluster 2 we explored the specific clinical manifestations of anti-NMDA encephalitis, suggesting that patients with anti-NMDA receptor encephalitis present a characteristic stage-by-stage clinical course, and according to the course curve of classical anti-NMDAR encephalitis drawn by Kayser and Dalmau (32), we found that patients often have an antecedent infection 2 weeks before the onset of the disease, which leads to the development of certain antecedent symptoms, mainly viral cold symptoms; 1-2 weeks of progression of psychiatric symptoms, such as hallucinations, mania, delusions, anxiety, insomnia; weeks to months of neurological complications: disorders of consciousness, central hypoventilation, and even coma, often accompanied by dyskinesia and seizures; and months to years of neurological symptoms: executive functions, hypoparathyroidism and hyperventilation. Long-term deficits such as executive dysfunction, impulsivity and sleep disturbances are manifested over a period of months to years, and the critical but relatively reversible nature of the disease is an important feature. It was even found that the course of recovery from the disease was consistent with the course of disease progression, i.e., the first symptoms to appear disappeared last. However, it is worth noting that there may be some differences between children and adults (33), and we believe that the most common clinical manifestations of anti-NMDA receptor encephalitis in children are epilepsy, movement disorders, and personality changes, as well as the incidence of comorbid tumors in pediatric patients is lower than in adults (17).
[2] Symptomatologic pathomechanism of N-methyl D-aspartate receptor encephalitis
- Authors: Woo-Jin Lee
- Year: 2021
- Venue: Encephalitis
- URL: https://www.semanticscholar.org/paper/fe42ff1f42de5346c36c54b79c4684a07f88f107
- DOI: 10.47936/encephalitis.2021.00017
- PMID: 37469763
- PMCID: 10295887
- Summary: Those pathomechanistic hypotheses for NMDAR encephalitis support the rationale for the early introduction of combination immunotherapy and the use of adjuvant immunotherapy in patients with persisting symptoms in chronic disease phases.
- Evidence snippets:
- Snippet 1 (score: 0.517) > N-methyl D-aspartate receptor (NMDAR) encephalitis is a well-characterized clinical syndrome. The main molecular mechanism of NMDAR encephalitis is autoantibody-mediated NMDAR hypofunction in the neuronal synapse. Several pathomechanistic hypotheses might explain how NMDAR hypofunction causes the typical symptoms and prognosis of NMDAR encephalitis. Suppression of NMDAR-dependent gamma-aminobutyric acid interneurons provokes an accelerated activation of the positive feedback loops of the dorsolateral prefrontal cortex/subiculum–nucleus accumbens circuit in the striatum, the ventral tegmental area (VTA), and the nucleus reuniens in the thalamus–hippocampus–VTA loop. Dysregulated activation of the VTA and cortex via those positive feedback loops may explain the rapid clinical deterioration at acute stages of the disease and the well-characterized syndrome that includes limbic system dysfunction, intractable seizures, dyskinesia, coma, and the characteristic extreme delta brush. Progressive cerebellar atrophy is correlated with cumulative disease burden and is associated with worse long-term outcomes, which might be explained by the NMDAR-dependent pathways required to maintain neuronal survival. Those pathomechanistic hypotheses for NMDAR encephalitis support the rationale for the early introduction of combination immunotherapy and the use of adjuvant immunotherapy in patients with persisting symptoms in chronic disease phases.
[3] Recent advances in autoimmune encephalitis
- Authors: J. Ferreira, C. Disserol, Bruna de Freitas Dias, Alexandre Coelho Marques, Marina Driemeier Cardoso et al.
- Year: 2024
- Venue: Arquivos de Neuro-Psiquiatria
- URL: https://www.semanticscholar.org/paper/36759fd04ed2757c5112e8fa3f3dec5dfd4a4d47
- DOI: 10.1055/s-0044-1793933
- PMID: 39706227
- PMCID: 11661894
- Citations: 6
- Summary: The clinical spectrum of anti-LGI1, anti-AMPAR, anti-CASPR2, and anti-IgLON5 was expanded, comprising new differential diagnoses, and a diagnostic algorithm was proposed, considering potential mimics and misdiagnosis of autoimmune encephalitis.
- Evidence snippets:
- Snippet 1 (score: 0.516) > Anti-N-methyl-D-aspartate receptor encephalitis is caused by ABs targeting the GluN1 subunit of the NMDA receptor, which causes cross-linking and internalization of those receptors, leading to impaired NMDAR electric currents. 13,14 nimal models showed that anti-NMDAR ABs modify CA1 pyramidal cells' excitability and hippocampal network activity. 15 Additionally, hippocampal proteomics revealed changes in components of glutamatergic, GABAergic, and central hubs of intracellular signaling, providing insights into molecular mechanisms for electrophysiological findings and pathophysiology. 15 ecently, the mean annualized incidence rate of anti-NMDARE was estimated at 1.00/million cases in the Netherlands. 8 Anti-NMDARE predominates in young women, with an ovarian teratoma found in nearly 50% of cases. 16 8][19] Moreover, one recent case series showed that 20% of patients were > 45 years, indicating that late presentation may be more common than previously expected. 10 These late-onset cases were associated with other tumors, mainly carcinomas, were oligosymptomatic, and had worse outcome. 10,16 he classic anti-NMDARE clinical syndrome starts with prodromal symptoms, followed by cognitive or psychiatric manifestations (delusions, psychosis, catatonia), movement disorders (orofacial dyskinesias, choreoathetosis), speech disorder, dysautonomia, seizures, and decreased level of consciousness. 12,16 substantial number of patients require ICU admission for management of status epilepticus, autonomic dysfunction, and mechanical ventilation. 4 Clinical variables from the acute presentation can be used to evaluate disease prognosis. The anti-NMDAR Encephalitis One-Year Functional Status (NEOS) score predicts functional outcomes after 1 year of symptoms onset and includes 5 clinical variables: This score also performed well for children, and preliminary findings indicate that it can also be used for cognitive outcomes. 21 n the post-acute phase, patients may present a neuropsychiatric syndrome that resembles schizophrenia, which improves gradually. 22
[4] First-episode psychosis in a 15 year-old female with clinical presentation of anti-NMDA receptor encephalitis: a case report and review of the literature
- Authors: Maria Moura, Amílcar Silva-Dos-Santos, J. Afonso, M. Talina
- Year: 2016
- Venue: BMC Research Notes
- URL: https://www.semanticscholar.org/paper/1646c9c0933489c5f3308172ec520d0e2a2e1133
- DOI: 10.1186/s13104-016-2180-6
- PMID: 27473459
- PMCID: 4966559
- Citations: 10
- Summary: This case is presented of a 15 year-old female adolescent with first-episode psychosis with anti-NMDA receptor encephalitis not related to tumor, which manifested with delusion, hallucinations, panic attacks, agitation, and neurological symptoms, and later with autonomic instability.
- Evidence snippets:
- Snippet 1 (score: 0.503) > Anti-NMDA receptor encephalitis is an autoimmune disease that was first identified as a paraneoplastic syndrome in young women with ovarian teratomas, and can also occur as a rare manifestation of teratoma of the mediastinum, or due to testicular cancer or small-cell lung carcinoma [7,10]; however it can also be non-paraneoplastic [3,22]. The clinical presentation usually consists of three stages: a prodromal period that lasts up to 1 week with common cold-like symptoms, fever, headache, malaise or gastroenteritis; an intermediate period, lasting 1-3 weeks, with behavioral changes, psychiatric symptoms or mood changes. The most common clinical presentation resembles acute psychosis (anxiety, agitation, paranoia, auditory or visual hallucinations) [7,23], meaning that psychiatrists are usually the first physicians to observe these patients. The third stage can last from weeks to months, and consist of neurological and autonomic symptoms, including alteration in speech, catatonia, and seizures. The common autonomic symptoms include urinary incontinence or sleep dysfunction. The more severe autonomic symptoms, such as hypoventilation, dysrhythmia, tachycardia, and hyperthermia, are not frequent in children [11]. It has been shown that this condition is more frequent in children than was previously thought and that its clinical manifestations in the pediatric population are similar to those of adults [11]. > The exact pathophysiology of anti-NMDA receptor encephalitis is not fully understood. It is believed that NR1 subunits expressed by tumoral neural tissues may break the immune tolerance [10]. However, anti-NMDA receptor encephalitis is not always related to teratoma or other malignancies, and hence, other immunologic mechanisms might be involved. Hypotheses thus far proposed include the concept that there is an immunological response to a flu-like prodromal phase possibly related to a viral infection, and genetic susceptibility [10].
[5] Neuroleptic intolerance in patients with anti-NMDAR encephalitis
- Authors: F. Lejuste, L. Thomas, G. Picard, V. Desestret, F. Ducray et al.
- Year: 2016
- Venue: Neurology® Neuroimmunology & Neuroinflammation
- URL: https://www.semanticscholar.org/paper/9d6905fe5955e78d89679ebecd667546c084bbcc
- DOI: 10.1212/NXI.0000000000000280
- PMID: 27606355
- PMCID: 5004531
- Citations: 150
- Influential citations: 13
- Summary: Several psychiatric presentations were observed in patients with anti-NMDAR encephalitis, although none was specific; however, patients, mostly women, also had discreet neurologic signs that should be carefully assessed as well as signs of antipsychotic intolerance that should raise suspicion for anti- NMDAREncephalitis.
- Evidence snippets:
- Snippet 1 (score: 0.500) > cephalitis. > Our results also outline that emergency physicians, neurologists, and psychiatrists must systematically search for associated discreet neurologic signs and symptoms relevant to encephalitis in young patients with psychiatric symptoms. Indeed, more than half (n 5 24) of the 45 patients hospitalized in psychiatric departments had neurologic signs at the first evaluation. Despite the presence of these comorbid elements, the patients were not correctly diagnosed or hospitalized in an appropriate unit and did not receive the medical investigations required for diagnosis of encephalitis. Many patients had a normal neuroimaging, which was misinterpreted to support a primary psychiatric etiology of symptoms and signs, but neuroimaging is frequently normal in anti-NMDAR encephalitis. 2,11 An interesting observation was the very high rate of possible antipsychotic drug intolerance in our 19 In particular, it should be stressed that one patient presented with 3 previous psychiatric episodes, separated by many years, and for each episode, she had experienced severe intolerance to antipsychotic drugs. DSM-5 20 and DSM-IV 21 do not provide an exact list of criteria for NMS, and we did not have enough information on the 21 patients to strictly confirm the diagnosis of NMS, but the significantly high rate of fever with abnormal biological data in our patients receiving antipsychotic drugs and the absence of such clinical presentation in the group of patients who were not treated with antipsychotic drugs suggests the existence of a pathophysiologic overlap between NMS, malignant catatonia, and anti-NMDAR encephalitis. > Interestingly, hypofunction of glutamatergic neurotransmission has been proposed in the etiology of NMS, 22 although amantadine, a weak NMDA receptor antagonist, improves NMS symptoms in a Parkinson disease model. 23,24 Beyond the apparent contradiction of glutamatergic functioning, the pathophysiologic interplay between the NMDAR and dopaminergic receptors, and more generally monoamine signaling, emerges as a core mechanism in several neuropsychiatric disorders. Any alteration in NMDAR signaling at the neuronal surface (as reported in anti-NMDAR encephalitis 25
[6] Deciphering the molecular landscape of NMDAR-E associated ovarian teratomas: a Multi-Omics approach
- Authors: Lingwei Ma, Xinmeng Sun, Shaohua Zhang, Yinping Xiao, Haiyun Guan et al.
- Year: 2025
- Venue: Journal of Ovarian Research
- URL: https://www.semanticscholar.org/paper/1e51dd97cee96f7970afd788203963afd0ddd878
- DOI: 10.1186/s13048-025-01871-4
- PMID: 41339905
- PMCID: 12676869
- Citations: 1
- Summary: Key genes and proteins involved in ferroptosis and immune activation, including SLC40A1, GGH, FKBP11, CCDC80, and ANK3, showed significant expression differences, and changes were notable at the mRNA and protein levels in ovarian teratomas associated with NMDAR-E.
- Evidence snippets:
- Snippet 1 (score: 0.492) > Anti-N-methyl-D-aspartate receptor encephalitis (NMDAR-E) is an autoimmune disorder often associated with ovarian teratomas. It involves antibodies against the neuronal NMDAr1 subunits of NR1, but the pathogenesis and molecular mechanisms are not fully understood. To identify significantly differentially expressed genes and proteins and investigate the intricate molecular regulatory network underlying anti-NMDA receptor encephalitis (NMDAR-E) associated with ovarian teratomas. This retrospective study analyzed ovarian teratoma samples from patients with and without NMDAR-E. RNA sequencing and iTRAQ coupled LC-MS/MS analysis were used for gene and protein expression profiling. qPCR and western blotting were used to validate the gene and protein expression. We identified 2524 significantly differentially expressed genes and 34 proteins. The changes were notable at the mRNA and protein levels in ovarian teratomas associated with NMDAR-E. Functional enrichment analysis highlighted the extracellular matrix and immune activation pathways. Key genes and proteins involved in ferroptosis and immune activation, including SLC40A1, GGH, FKBP11, CCDC80, and ANK3, showed significant expression differences. Our findings provide preliminary insights into the pathophysiology of NMDAR-E associated with ovarian teratomas. These results may generate hypotheses for future mechanistic studies, and the candidate biomarkers identified warrant further validation before clinical translation.
[7] Simultaneous serum aquaporin-4 antibody and CSF NMDA receptor antibody–positive encephalitis
- Authors: Unknown authors
- Year: 2015
- Venue: Neurology® Neuroimmunology & Neuroinflammation
- URL: https://www.semanticscholar.org/paper/ce7b01bd99ff2ef99c25ece6e5208893b23b7008
- DOI: 10.1212/NXI.0000000000000101
- PMID: 25884011
- PMCID: 4396527
- Citations: 2
- Summary: A 29-year-old Hmong woman presented with 3 months of worsening imbalance and intermittent vertigo followed by right facial numbness, slurred/nonsensical speech, and memory impairment, which revealed impaired short-term memory, expressive aphasia, mild right appendicular ataxia, and profound abulia.
- Evidence snippets:
- Snippet 1 (score: 0.480) > disorder followed by NMDA receptor encephalitis was recently reported in 5 patients. 3 The simultaneous occurrence of these CNS pathogenic antibodies with pathologic findings has not been previously reported. Although we do not know to what extent the anti-NMO/AQP4 and the anti-NMDA receptor autoantibodies contributed to the presentation, the clinical and radiographic features in this case suggest features of both NMO spectrum disorder and NMDA receptor encephalitis. Clinical and radiographic features that could be consistent with NMO include the brainstem syndrome with anorexia and radiographic involvement of the brainstem, hypothalamus, and optic chiasm. Similarly, cognitive impairment and akinesia along with the radiographic features of encephalitis might be due to NMDA receptor antibodies. > Other autoimmune diseases, including systemic lupus erythematosus, Sjögren syndrome, and myasthenia gravis, occur in patients with NMO. Many patients with NMO test seropositive for other autoantibodies. 4 More recently, anti-myelin oligodendrocyte glycoprotein antibodies were associated with a Neurology.org/nn © 2015 American Academy of Neurology 1 clinical presentation consistent with NMO. 5 We speculate that a mechanism underlying a breach in immune tolerance could be shared by CNS autoantibody-mediated diseases, resulting in the sequential occurrence of NMO and NMDA receptor encephalitis and possibly explaining the co-occurrence of these autoantibodies in our patient. An immunodominant AQP4 peptide recognized by T cells in patients with NMO has a high degree of homology to an ABC transporter from Clostridium species, suggesting that molecular mimicry might be involved in NMO pathogenesis. 6 Colonization of Clostridium or other bacterial species in the gut could promote immune responses that cross-react with the AQP4 and NMDA receptor proteins. Alternately, we speculate that NMO-related inflammation could "reveal" CNS antigens to the immune system, resulting in a secondary inflammatory response similar to that proposed for HSV and NMDA There are scattered activated microglia with elongated comma-shaped nuclei (
[8] Immune inflammatory regulation in Anti-NMDAR encephalitis: insights from transcriptome analysis
- Authors: Shan Qiao, Jia Wang, Shanchao Zhang, Aihua Wang, Hai-yun Li et al.
- Year: 2025
- Venue: Frontiers in Neurology
- URL: https://www.semanticscholar.org/paper/cd426a7d25d9ae6141d60961d06697e6de2154d5
- DOI: 10.3389/fneur.2025.1568274
- PMID: 40417115
- PMCID: 12098042
- Citations: 2
- Summary: Background Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis is a critical neurological disorder mediated by autoimmune mechanisms, Previous literature suggests that immune inflammatory responses may be involved in the progression of anti NMDAR encephalitis, but its molecular regulatory mechanisms still remain uncertain. We aimed to identify transcriptome-wide landscape of mRNAs and explore the potential pathogenesis for anti-NMDAR encephalitis. Methods Peripheral blood mononuclear cell...
- Evidence snippets:
- Snippet 1 (score: 0.464) > Background Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis is a critical neurological disorder mediated by autoimmune mechanisms, Previous literature suggests that immune inflammatory responses may be involved in the progression of anti NMDAR encephalitis, but its molecular regulatory mechanisms still remain uncertain. We aimed to identify transcriptome-wide landscape of mRNAs and explore the potential pathogenesis for anti-NMDAR encephalitis. Methods Peripheral blood mononuclear cells were obtained from six patients with anti-NMDAR encephalitis and six controls for RNA extraction and library creation. The Illumina HiSeq platform was used to do transcriptome sequencing. We utilized R software to identify differentially expressed genes (DEGs) and performed a functional enrichment analysis. Furthermore, random forest (RF) and support vector machine-recursive feature elimination (SVM-RFE) were employed to screen for and identify anti-NMDAR encephalitis diagnostic signatures. To verify the findings, we employed quantitative real-time polymerase chain reaction. Receiver operating characteristic curves were utilized to assess the diagnostic values. We evaluated the inflammatory state of anti-NMDAR encephalitis using cell-type identification by computing the relative subsets of RNA transcripts (CIBERSORT) and investigated the relationship between diagnostic biomarkers and immune cell subsets. Results 899 DEGs were identified (568 upregulated and 331 downregulated), of which 78 were immune-related genes. The DEGs were found to be considerably enriched in immunological inflammation-related pathways, according to the functional enrichment analysis. Insulin-like factor 3 [area under the curve (AUC) = 0.917] and tumor protein translationally controlled regulator 1 (AUC = 0.944) were considered potential diagnostic indicator candidates of anti-NMDAR encephalitis, with statistically significant variations in expression. An immune cell analysis of immune cell proportions suggests that monocytes, CD8+ T cells, and T regulatory cells may all be involved in the development of anti-NMDAR encephalitis. Conclusions Transcriptome analysis reveals significant activation of peripheral immune-inflammatory pathways in anti-NMDAR encephalitis. INSL3 and TPT1 may
[9] The neuroinflammation collection: a vision for expanding neuro-immune crosstalk in Brain
- Authors: S. Irani, A. Nath, F. Zipp
- Year: 2021
- Venue: Brain
- URL: https://www.semanticscholar.org/paper/76ab9e302f17b1934b7a7e7440cc35418a9c1f5b
- DOI: 10.1093/brain/awab187
- PMID: 33983376
- PMCID: 8370408
- Citations: 10
- Summary: A vision is offered of how anticipated developments in neuroinflammation are likely to impact the understanding of key elements of neurology, and lead to new treatments as well as some of the most exciting areas within this rapidly expanding, clinically relevant and highly translational field.
- Evidence snippets:
- Snippet 1 (score: 0.461) > The autoantibody-mediated diseases of the nervous system provide perhaps the most direct examples to connect an identified pathogenic agent with the corresponding disease process. In these conditions-ranging from myasthenia gravis and neuromyelitis optica to autoimmune encephalitis-autoantibodies target extracellular domains of neuroglial proteins and patients often show highly distinctive, even unique, clinical features. In autoimmune encephalitis, these include faciobrachial dystonic seizures and multiple frequent focal seizure semiologies in patients with leucine-rich glioma-inactivated 1 (LGI1) antibodies, 1 while a stereotyped multistage progression of inherently complex clinical features characterizes the phenotype of individuals with N-methyl-D-aspartate receptor (NMDAR) antibody encephalitis. 2,3 In these patients, the highly characteristic nature of these-and other-clinical features provides persuasive evidence of a distinctive human pathology directly mediated by these antibodies. Further to these clinical observations, experimental data confirm these autoantibodies fulfil modified Koch's postulates for pathogenicity, both in vitro and in animal models. 4,5 Hence, a logical prediction is that inhibiting their end-target effects will reverse symptoms in patients. > To test this hypothesis at the molecular level, an allosteric modulator of the NMDAR-which crosses the blood-brain barrier-was applied to culture and in vivo model systems prior to application of patient NMDAR antibodies. 6 Administration of this drug to mice subsequently receiving a cerebroventricular transfer of NMDAR antibodies prevented all the antibody-mediated effects: memory alterations, a spatial redistribution of NMDARs and the abrogation of long-term potentiation. Yet, intriguingly, this drug did not fully abrogate NMDAR internalization, which is often characterized as the dominant mechanism of action of the human autoantibodies. However, this study lacked a key experiment: namely the application of the drug after the induction of antibodymediated pathology. Hence, its clinical relevance as a symptomatic therapy, alongside the observationally established value of immunotherapies, remains a key area for future work.
[10] Autoantibodies detection in anti-N-methyl-D-aspartate receptor encephalitis
- Authors: Jiayu Li, Qi Wang, Honghao Wang
- Year: 2021
- Venue: Annals of Translational Medicine
- URL: https://www.semanticscholar.org/paper/47c5272562cd73f4b7e9d0f24fc328e115f23a5a
- DOI: 10.21037/atm-20-2279
- PMID: 37090042
- PMCID: 10116423
- Citations: 7
- Summary: It’s found that IHC got a higher positive rate than CBA in both serum and cerebrospinal fluid (CSF) when screening potential AE, while CBA was more specific.
- Evidence snippets:
- Snippet 1 (score: 0.457) > Autoimmune encephalitis (AE) covers a group of central nervous system diseases with clinical manifestations as neurological and/or psychiatric symptoms. AE is severe but treatable. It has gained increasing attention currently. The body's immune function can be disturbed under certain conditions such as tumor and infection, producing antibodies directed against neuronal autoantigens. Antineuronal antibodies include antibodies against cell surface, synaptic and intraneuronal antigens (1,2). Antibodies against cell surface antigens can directly influence the neurotransmission and excitability by targeting molecules including encephalitis: anti-N-methyl-D-aspartate (NMDA) receptor and α-amino-3-hydroxy-5-methyl-4isoxazolepropionic acid (AMPA) receptors via changing the function of the target protein (2,3). Antibodies may act as either agonist or antagonist on receptors (4), interfere with adjacent molecular interactions or reduce the expression of receptors on cell surface by altering the localization of membrane receptors or causing receptor internalization (i.e., anti-NMDAR antibodies) (5,6). Moreover, they can Review Article lead to the opening of transmembrane ion channels or cell death because of complement deposition and activation of natural killer cells. Antibodies against synaptic antigens are believed to alter the release or responsiveness of neurotransmitters (3). In contrast, antibodies against intraneuronal antigens (i.e., anti-Hu, anti-Yo and anti-Ma) are most likely not directly pathogenic, probably an epiphenomenon of T-cell-mediated immune response and classified as paraneoplastic neurological syndromerelated onconeural antibodies (7,8). Further discoveries showed that these antibodies caused cellular dysfunction or injury through multiple effector mechanisms. Intracellular antigens were not accessible to immune attack in situ; but upregulated major histocompatibility complex class I molecules in a pro-inflammatory cytokine milieu after proteasomal degradation, and then they were accessible to peptide-specific cytotoxic T cells (3).
[11] Anti-NMDA Receptor Encephalitis: A Narrative Review
- Authors: V. Pădureanu, D. Dop, R. Pădureanu, D. Pîrșcoveanu, Gabriela Olaru et al.
- Year: 2025
- Venue: Brain Sciences
- URL: https://www.semanticscholar.org/paper/79ec541ca01050ca7b270282c4e37df10cf3c334
- DOI: 10.3390/brainsci15050518
- PMID: 40426689
- PMCID: 12110449
- Citations: 9
- Influential citations: 2
- Summary: Given its high prevalence, anti-NMDA receptor encephalitis should be included in the differential diagnosis in routine psychiatric treatment, and an overview of the research on the condition is provided.
- Evidence snippets:
- Snippet 1 (score: 0.454) > In light of this, the HLA genetic factors are the autoimmunity core, but the non-HLA genetic factor might influence the genetic risk and therapeutic response. To date, the non-HLA gene's role in anti-NMDAR encephalitis is less characterized. For the first time, recent studies on autoimmune encephalitis genetics report that the non-HLA gene is involved in the diseases' molecular mechanism. Gene mutation, such as single-nucleotide polymorphism (SNP), can increase the risk of developing anti-NMDAR encephalitis. A genome-wide association study (GWAS), aimed at identifying genetic risk factors for anti-NMDA receptor (anti-NMDAR) encephalitis, performed colocalization and gene variant analysis to identify causal genes or gene variants [30]. These variants and genes did not belong to the HLA system. In this genomics study, performed by Tietz and colleagues, two significant genetic loci located on chromosomes 15 and 11 were identified as potential risk factors for anti-NMDAR encephalitis (Table 1). Other genes related to immune system checkpoints or the cytokine signaling pathway which involve BBB could be key factors in anti-NMDAR encephalitis. The lysosomal acid phosphatase 2 (ACP2) gene encodes an enzyme from the lysosomal membrane which hydrolyzes orthophosphoric monoesters to alcohol and phosphate. About 37 single-nucleotide variants (SNVs) of this gene are reported according to clinvar, but no clear pathological association with immune response was found [30]. ACP2 is involved in the interaction between the host and pathogens, such as viruses [36]. The ACP2 gene involved in immune regulation and the inflammatory signaling pathway may influence antigen processing and potentiate autoantigen production. The mutation of the ACP2 gene may be used in personalized therapies and can sustain the potential benefit of antiinflammatory therapy.
[12] Progress in the preparation of an active immunization model of anti-N-methyl-D-aspartate receptor encephalitis in animals
- Authors: Kuikui Zeng, Yuting Liu, Sai Yang, Lingjuan Liu
- Year: 2025
- Venue: Frontiers in Immunology
- URL: https://www.semanticscholar.org/paper/d78fd3dcf8563d324f99f53d2dc4e26157a4c3f4
- DOI: 10.3389/fimmu.2025.1585353
- PMID: 41451196
- PMCID: 12728017
- Summary: This review aims to systematically classify existing active immunization models of anti-NMDAR encephalitis, with detailed discussion on their establishment protocols, respective advantages, current applications, and future prospects.
- Evidence snippets:
- Snippet 1 (score: 0.452) > Usually, antibody-mediated encephalitides are typically characterized by concomitant neuroinflammation and seizure activity. Unlike other neurological disorders or experimental models, these conditions provide direct evidence for synaptic dysfunction and neuronal hyperexcitability through their welldefined mechanisms involving specific antibody binding to synaptic receptors and proteins (41). The GluN1 peptide-induced NMDAR encephalitis model exhibits significant limitations: while linear peptides can directly activate B cells and generate high-titer antibodies, their inability to engage T cell assistance and relevant inflammatory signaling pathways prevents complete recapitulation of human disease pathology. This model fails to reproduce hallmark clinical manifestations of anti-NMDAR encephalitis (including movement disorders, psychiatric symptoms, and spontaneous seizures), while demonstrating marked deficiencies in investigating critical aspects such as disease pathogenesis, inflammatory cytokine networks, and immune cell interactions. These shortcomings substantially constrain the model's utility for comprehensive mechanistic studies of NMDAR encephalitis. > HSV infection of the central nervous system represents a significant trigger for anti-neuronal autoimmunity (42). Current scholarship predominantly supports the view that HSV infection serves as an indirect precipitating factor for anti-NMDAR encephalitis, which may explain the relative scarcity of such models in research. The pathogenic mechanism is not attributable to direct viral neurotoxicity, but rather stems from secondary immune-mediated damage following viral infection (35,43). This pathophysiological process involves three key interrelated mechanisms: First, molecular mimicry occurs between HSV-1 proteins (e.g., glycoprotein B) and human synaptic proteins (e.g., NMDA receptors), leading to cross-reactive autoantibody production (44). Second, viral PAMPs are recognized by microglial TLR3 receptors, triggering innate immune responses characterized by excessive IFN and proinflammatory cytokine (IL-6, TNF-a) release, blood-brain barrier disruption, and CD8+ T cell infiltration (45).
[13] Immuno-psychiatry: an agenda for clinical practice and innovative research
- Authors: M. Leboyer, M. Berk, R. Yolken, R. Tamouza, D. Kupfer et al.
- Year: 2016
- Venue: BMC Medicine
- URL: https://www.semanticscholar.org/paper/9b33161ac3fa0889a188af2fa167cf846ceb2553
- DOI: 10.1186/s12916-016-0712-5
- PMID: 27788673
- PMCID: 5084344
- Citations: 60
- Influential citations: 2
- Summary: The development of bio-signatures will allow clinicians to tailor interventions to the abovementioned biomarker subtypes – a major translational goal for research in this field.
- Evidence snippets:
- Snippet 1 (score: 0.423) > extracted from the above emerging models in derivation studies could serve to design new "educated chips" that will contain immune, neurobiological and genetic markers defining subtypes of patients that could be further refined in validation studies (Fig. 1). > The use of animal models could facilitate exploration of in-depth temporal and molecular pathways linking central and peripheral dysfunctions in psychiatric disorders. For instance, since the discovery that some NMDA receptor (NMDAR) blockers induce schizophrenia-like psychosis, reproducing both positive and negative symptoms, the NMDA glutamatergic model of psychosis and schizophrenia has been increasingly accepted as part of the disease's etiopathology [40]. The dysfunction of NMDAR signalling might originate, among other pathways, from genetic alteration, autoantibodies directed against extracellular epitopes [41][42][43][44][45][46], and/or altered levels of endogenous agonists/antagonists (kynurenine metabolites) [47]. Of note, the recent discovery that autoantibodies against extracellular epitopes of the NMDAR produce major psychosis [41][42][43][44][45][46] provides a unique opportunity to increase our understanding of psychotic disorders at the molecular, cellular and brain imaging levels. For instance, autoantibodies from anti-NMDA encephalitis patients altered NMDAR signalling by preventing molecular interaction and altering membrane trafficking of NMDAR, although without modulating the function of the NMDAR channel [43]. Thus, NMDAR dysfunction-induced psychosis could originate from a blockade of the channel (e.g. phencyclidine) or an altered trafficking of the receptor (e.g. autoantibodies). Future investigations in various psychotic disorders will thus shed new light on the mechanisms underlying these disorders and pave the way for new, innovative therapeutical strategies to restore proper NMDAR signaling. > Could a common dysfunction be at the origin of peripheral disorders? Theoretically, yes. Indeed, it is often forgotten that NMDAR is not only expressed in brain cells but also in many other organs and cell types; for example, NMDAR is expressed in pancreatic islets and in insulin-secreting beta cells whose functional
[14] Pediatric anti-N-methyl-d-aspartate receptor encephalitis in southern China: Analysis of 111 cases.
- Authors: Xiaojing Li, C. Hou, Wen-lin Wu, Hui-ci Liang, Ke-lu Zheng et al.
- Year: 2021
- Venue: Journal of neuroimmunology
- URL: https://www.semanticscholar.org/paper/1906f55fc6403a746429f3c2c2be5ee26c468cfe
- DOI: 10.1016/j.jneuroim.2021.577479
- PMID: 33486307
- Citations: 19
- Summary: Of pediatric anti-NMDAR encephalitis in southern China: median onset age around 7 years; girls more common; boys might have poor outcome than girls; seizure or movement disorder respectively being most common onset or course symptom; a few overlapped with other neuronal autoantibodies; rare combined with tumor.
- Evidence snippets:
- Snippet 1 (score: 0.419) > Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis is a neuroinflammatory disease mainly mediated by autoantibodies against the GluN1 subunit of the receptor (Dalmau, 2016). Since it was first reported in 2007, a series of studies have been conducted on this disease during these years (Dalmau et al. , 2007, Gurrera, 2019. With regards to clinical evidence of inflammation, there are two stages. In the first stage (which has a duration of around 3 months or longer), patients develop severe symptoms (such as psychosis, movement disorders, seizures, dysautonomia, and coma) commonly accompanied by transient magnetic resonance image (MRI) abnormalities or pleocytosis. The second stage (which has a duration of around 6 months or longer) corresponds to the process of recovery. Patients' antibodies crosslink the NMDARs, altering their surface dynamics and interaction with other synaptic proteins, and causing their internalization along with severe impairment of synaptic plasticity and NMDAR network function. The clinical features in patients and animal models resemble those caused by genetic or pharmacological attenuation of NMDAR function (Dalmau, 2016, Lynch et al. , 2018. And regional clinical studies of anti-NMDAR encephalitis may promote the research on its mechanism and enrich the clinical phenotypes. However, regional studies with large samples of children are still limited. > In current study, we reported the clinical features of children recently diagnosed with anti-NMDAR encephalitis in a national regional tertiary medical center from southern China.
[15] Precision Therapeutics in Lennox–Gastaut Syndrome: Targeting Molecular Pathophysiology in a Developmental and Epileptic Encephalopathy
- Authors: Debopam Samanta
- Year: 2025
- Venue: Children
- URL: https://www.semanticscholar.org/paper/455479c1bfbea7b90b73c109228f67c813d13888
- DOI: 10.3390/children12040481
- PMID: 40310132
- PMCID: 12025602
- Citations: 19
- Influential citations: 1
- Summary: A narrative review explores precision therapeutic strategies for LGS based on molecular pathophysiology, including channelopathies, receptor and ligand dysfunction, receptor and ligand dysfunction, cell signaling abnormalities, cell signaling abnormalities, synaptopathies, and the repurposing of existing medications with mechanism-specific effects.
- Evidence snippets:
- Snippet 1 (score: 0.408) > A key advantage of disease-modifying therapies is their potential to target pathogenic mechanisms early in the disease course, potentially preventing the progression of some infantile epileptic encephalopathies to LGS. > This narrative review explores precision therapeutic strategies based on specific monogenic causes and disease mechanisms relevant to LGS. A comprehensive literature search (PubMed, MEDLINE, ClinicalTrials.gov, conference abstracts from the American Academy of Neurology and American Epilepsy Society, and gray literature) was conducted through 19 February 2025 to identify established ASMs, repurposed and novel drugs, as well as various gene therapy approaches with potential relevance to LGS. Given that over 900 monogenic causes of DEEs have been identified-implicating diverse cellular components such as ion channels, receptors, synaptic proteins, signaling pathways, metabolic processes, and epigenetic regulators-this review discusses current and emerging precision therapeutics based on shared molecular mechanisms and the pathophysiology of select genes associated with LGS [17] (Table 1).
[16] Molecular Pathogenesis of Anti-NMDAR Encephalitis
- Authors: Hao Ding, Z. Jian, C. Stary, W. Yi, Xiaoxing Xiong
- Year: 2015
- Venue: BioMed Research International
- URL: https://www.semanticscholar.org/paper/653de9aedde40b75ffec353e4b4e33f0826d329f
- DOI: 10.1155/2015/643409
- PMID: 26221602
- PMCID: 4499418
- Citations: 21
- Influential citations: 2
- Summary: This review will provide a summary of the current literature on anti-NMDAR encephalitis, including the immunologic molecular mechanisms contributing to disease progression, and focus on the effect of anti- NMDAR on GluN2-N MDAR expression and the molecular transformation of B and T leukocytes in the loss of self-tolerance.
- Evidence snippets:
- Snippet 1 (score: 0.406) > Anti-NMDAR encephalitis is a recently identified autoimmune disease, described by an immune-mediated loss of NMDA glutamate receptors, resulting in progressive mental deterioration. To date, literature on anti-NMDAR encephalitis has been largely clinically oriented, including descriptions of the clinical presentation and course, diagnostic methods, and potential clinical treatments. However, the underlying molecular mechanisms contributing to the complex immunological cellular transformation that is associated with the progression of anti-NMDAR encephalitis remain to be adequately explored. This review will provide a summary of the current literature on anti-NMDAR encephalitis, including the immunologic molecular mechanisms contributing to disease progression. In particular this review will focus on the effect of anti-NMDAR on GluN2-NMDAR expression and the molecular transformation of B and T leukocytes in the loss of self-tolerance. Further research on the immunologic mechanisms contributing to anti-NMDAR encephalitis may provide an avenue for future novel diagnostic approaches, such as immunologic surveillance, as well as new therapeutic strategies for this recently identified autoimmune disease.
[17] Atypical Autoimmune Encephalitis: Diagnostic Challenges and Therapeutic Insights From a Case Series
- Authors: Thummalagunta Prathyusha, G. Ambati, Abhijathya Chinta, P. Gowda, C. Bole
- Year: 2025
- Venue: Cureus
- URL: https://www.semanticscholar.org/paper/4ec40ecc7baa4e8bade8692b965099244d3c5396
- DOI: 10.7759/cureus.82384
- PMID: 40385909
- PMCID: 12083851
- Citations: 1
- Summary: This study provides a comprehensive overview of clinical presentations, treatment approaches, and patient outcomes of patients diagnosed with autoimmune encephalitis.
- Evidence snippets:
- Snippet 1 (score: 0.403) > CSF analysis was pivotal in confirming the diagnosis. In Case 3, viral encephalitis was ruled out, reinforcing the necessity of antibody testing in suspected autoimmune encephalitis and demonstrating positivity to anti-NMDA receptor antibodies, aligning with findings that the sensitivity of NMDA receptor antibody testing is higher in CSF compared to serum, as reported by Wang et al. [13]. Early and aggressive immunotherapy, including corticosteroids, intravenous immunoglobulin (IVIG), plasma exchange, and rituximab, was employed in all cases, leading to varying clinical improvement. However, treatment was complicated in Case 2, which developed drug-induced Stevens-Johnson syndrome and hepatitis, underscoring the risks of immunomodulatory therapy, with recurrent infections and a cardiac arrest further complicating management. > Studies indicate that first-line treatments, such as corticosteroids, IVIG, and plasma exchange, result in clinical improvement in approximately 50% of cases, with second-line agents such as rituximab and cyclophosphamide being required in refractory cases. The prognosis is highly dependent on early diagnosis and intervention, with up to 80% of patients achieving significant recovery if treated early, whereas delayed treatment is associated with worse neurological outcomes and prolonged hospital stays. > Challenges in management included pre-existing conditions such as obesity and obstructive sleep apnea in Case 1. Prolonged mechanical ventilation and tracheostomy in Cases 1 and 2 highlighted the severity of the disease, and the prolonged course of recovery with residual motor and speech impairments persisted, necessitating long-term rehabilitation. Case 3 demonstrated the best outcome, with seizure-free status and no significant residual deficits, as described by Nosadini et al., who reported symptom-free disease in follow-up [14]. > Given the spectrum of complications, a multidisciplinary approach involving neurology, psychiatry, critical care, and rehabilitation specialists is crucial to optimize patient outcomes. Furthermore, the co-occurrence of anti-NMDA and anti-MOG antibody positivity in Case 3 raises important questions about underlying immune mechanisms.
[18] Common immunopathogenesis of central nervous system diseases: the protein-homeostasis-system hypothesis
- Authors: Kyung-Yil Lee
- Year: 2022
- Venue: Cell & Bioscience
- URL: https://www.semanticscholar.org/paper/2984270ae67451b93007040848d9694d19714c9f
- DOI: 10.1186/s13578-022-00920-5
- PMID: 36384812
- PMCID: 9668226
- Citations: 9
- Influential citations: 1
- Summary: This article proposes a common immunopathogenesis of CNS diseases, including prion diseases, Alzheimer’s disease, and genetic diseases, through the PHS hypothesis, which proposes that the immune systems in the host control those substances according to the size and biochemical properties of the substances.
- Evidence snippets:
- Snippet 1 (score: 0.401) > There are hundreds of genetic diseases of the CNS. The defective proteins in genetic disorders include structural proteins for neurotransmitter receptors and other receptors or ion channels on CNS cells, and proteins involved in enzymatic process, metabolism (transport), or signal transduction pathways in various communication systems [98]. Because a discussion of each genetic disease is beyond the scope of this review, only crucial points about the pathogenesis of genetic diseases are discussed. Singlegene defect diseases of the CNS can be caused by a defective product from a gene, i.e., a protein deficiency or a malfunctioning protein. In general, autosomal dominant genetic diseases are caused by structural protein defects, and autosomal recessive diseases are caused by defects in enzymatic proteins. However, certain genetic diseases that involve an enzymatic or multifunctional protein defect can induce structural cell injury during the natural course of the illness. > Patients with genetic diseases, including HD, familial JCD, GSS, and the genetic forms of AD and PD, show different clinical manifestations from other affected people in their family, including the time of onset of neurological symptoms, speed of progression of the disease, and prognosis, suggesting that phenotypes can vary even when the genotypes are identical. Likewise, similar phenotypes of CNS symptoms can be found in different genetic diseases. In genetic animal models, the phenotypes of single gene knockout can vary by strain in mice, and the clinical manifestations of a gene defect can differ between mice and humans, and mice null for some genes have also no observable phenotypic abnormalities compared with controls [99]. These findings suggest that default of a protein might be at least partly controlled by individual's control systems and that there might exist a similar immune/repair system against cell injury in genetic diseases. > The pathophysiology of most genetic diseases in the CNS is complex because any affected gene is associated with numerous proteins and their corresponding activations of genes and epigenetic changes that occur during disease processes. Thus, the use of a genetic marker for diagnosing or predicting a prognosis remains impractical in clinical settings [100].
Notes
- This provider combines
search_papers_by_relevancewithsnippet_search. - No synthesis or second-stage model call is performed.
Anti‑NMDA Receptor Encephalitis (Autoimmune) — Comprehensive Disease Characteristics Report
1. Disease Information
Overview / definition
Anti‑N‑methyl‑D‑aspartate receptor (NMDAR) encephalitis is a subacute, rapidly progressive autoimmune encephalitis characterized by neuropsychiatric symptoms (often prominent), seizures, movement disorders/dyskinesias, altered consciousness, and autonomic/respiratory dysfunction, associated with IgG autoantibodies targeting the GluN1 (NR1) subunit of the NMDAR and typically detected most reliably in CSF (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune pages 3-5, gong2021longtermfunctionaloutcomes pages 1-2).
Key identifiers
- MONDO: MONDO_0021081 (“anti‑NMDA receptor encephalitis”) (OpenTargets Search: Anti-NMDA receptor encephalitis).
- Orphanet / MeSH / OMIM / ICD‑10/ICD‑11: Not retrieved in the available tool context; therefore not reported here.
Synonyms / alternative names (used in evidence base)
- Anti‑NMDAR encephalitis; anti‑NMDA receptor autoimmune encephalitis; NMDAR encephalitis; NMDARE (nguyen2023antinmdareceptorautoimmune pages 1-2, dumez2024specificclinicaland pages 1-2, gong2023antinmdarantibodiesthe pages 1-2).
Evidence source types
This report integrates (i) human cohort/registry studies and systematic reviews, (ii) mechanistic in vitro and passive‑transfer animal model studies, and (iii) clinical trial registry information (ClinicalTrials.gov) (gong2021longtermfunctionaloutcomes pages 1-2, alsalek2024racialandethnic pages 1-2, dalmau2016nmdareceptorencephalitis pages 7-9, NCT03274375 chunk 1).
2. Etiology
Primary causal factors / triggers (current understanding)
Anti‑NMDAR encephalitis is primarily antibody‑mediated and frequently linked to antigenic triggers, particularly: - Ovarian teratoma (key paraneoplastic trigger in subsets of patients) (nguyen2023antinmdareceptorautoimmune pages 5-6, alsalek2024racialandethnic pages 1-2). - Herpes simplex encephalitis (HSE) as a post‑infectious trigger for secondary anti‑NMDAR encephalitis (dumez2024specificclinicaland pages 1-2, alsalek2024racialandethnic pages 1-2).
Risk factors (human clinical/epidemiologic)
- Sex and age: young adults and female predominance are common in many cohorts (nguyen2023antinmdareceptorautoimmune pages 1-2, brenner2024longtermcognitivefunctional pages 1-2).
- Race/ethnicity disparities (US population-based data): In Kaiser Permanente Southern California (2011–2022; >10 million person‑years), standardized incidence per 1 million person‑years was higher in Black, Hispanic, and Asian/Pacific Island individuals than in White individuals (Black 2.94 vs White 0.40) (alsalek2024racialandethnic pages 1-2).
Environmental / spatial & climatic factors
A 2023 systematic review/meta‑analysis reported that incidence estimates varied across regions and were associated with geography/climate: - higher reported incidence in Oceania (0.2/100,000 person‑years) and South America (0.16/100,000 person‑years) than Europe/North America (0.06/100,000 person‑years) (alentorn2023spatialandecological pages 1-2). - a strong negative correlation with latitude (Pearson’s R = −0.88) and seasonal peaks during warm months; extreme heat in France associated with incidence (p = 0.03) (alentorn2023spatialandecological pages 1-2).
Protective factors / gene–environment interactions
No protective factors or explicit gene–environment interaction data were retrieved in the current tool context.
3. Phenotypes
Core phenotype domains (with selected frequencies)
Common clinical manifestations include psychiatric/behavioral symptoms, seizures, movement disorders/dyskinesias, speech dysfunction, decreased consciousness, autonomic instability, and central hypoventilation (nguyen2023antinmdareceptorautoimmune pages 3-5, xu2020antinmdarencephalitis pages 1-2).
Selected quantitative phenotype frequencies from cohorts: - Psychosis/behavioral symptoms: 82.7% psychosis in a prospective China cohort (n=220, 2011–2017) (xu2020antinmdarencephalitis pages 1-2); behavioral changes 74.5% in an East China cohort (n=106) (wang2020influencingelectroclinicalfeatures pages 1-2). - Seizures: 80.9% in the prospective China cohort (n=220) (xu2020antinmdarencephalitis pages 1-2); 67% in the East China cohort (n=106), with 54.9% focal among those with seizures (wang2020influencingelectroclinicalfeatures pages 1-2). - Prodrome: a prodromal phase occurs in 40–70% of patients (review synthesis) (nguyen2023antinmdareceptorautoimmune pages 3-5).
Age-related clinical patterning (review synthesis): teenagers/adults commonly develop psychiatric/behavioral symptoms early (~90%), whereas young children more often present with neurologic features such as seizures/abnormal movements rather than frank psychiatric syndromes (nguyen2023antinmdareceptorautoimmune pages 3-5).
Quality of life and long-term functional/cognitive impacts
A 2024 nationwide cohort study of 92 patients reported that although most had “favorable” functional outcome by mRS, long-term deficits were common: - beyond 36 months, 34% had persistent cognitive impairment (z < −1.5 SD) and 65% scored below average in ≥1 domain; memory and language were most affected (brenner2024longtermcognitivefunctional pages 1-2). - 30% did not resume school/work and 18% needed adjustments; patient‑reported outcomes showed reduced emotional well‑being, social functioning, energy, and quality of life compared to norms (brenner2024longtermcognitivefunctional pages 1-2).
Suggested HPO terms (examples; see ontology table)
Examples include Seizure (HP:0001250), Psychiatric symptoms (HP:0000708), Dyskinesia (HP:0100660), Autonomic dysfunction (HP:0002271), Central hypoventilation (HP:0007110), Memory impairment (HP:0002354), Language impairment (HP:0002465) (artifact-01).
4. Genetic/Molecular Information
Causal genes
Anti‑NMDAR encephalitis is not typically a Mendelian monogenic disorder; it is defined by autoantibodies to the NMDAR (GluN1 subunit) rather than pathogenic variants in a causal gene (balu2019ascorethat pages 1-2, dalmau2017autoantibodiestosynaptic pages 8-10).
Target antigen and epitope information
- Structural epitope mapping indicates most autoantibodies target a conformational epitope in the amino‑terminal domain (ATD) of GluN1, including residues N368/G369; point mutations at these residues abolish binding (dalmau2017autoantibodiestosynaptic pages 8-10).
Modifier genes / protective variants / allele frequencies
Not retrieved in the available tool context.
5. Environmental Information
Infectious triggers
- HSE is a recognized trigger; in a post‑HSE cohort, median latency from HSE to anti‑NMDAR encephalitis was 30 days (dumez2024specificclinicaland pages 1-2).
Climate/ecological signals (population level)
Incidence appears associated with geographic/climatic variables including latitude, higher temperatures, and UV exposure in a systematic review/meta‑analysis (alentorn2023spatialandecological pages 1-2).
Lifestyle/toxin exposures were not retrieved.
6. Mechanism / Pathophysiology
Causal chain (current consensus)
1) Trigger/antigen exposure (e.g., ovarian teratoma or post‑HSV inflammation) can initiate/boost autoreactive B‑cell responses (nguyen2023antinmdareceptorautoimmune pages 5-6, dalmau2017autoantibodiestosynaptic pages 8-10). 2) Autoreactive B cells/plasma cells generate IgG targeting extracellular NMDAR epitopes; intrathecal synthesis is supported by cloning of recombinant antibodies from CSF cells and by intrathecal immune activity models (dalmau2017autoantibodiestosynaptic pages 37-38, dalmau2017autoantibodiestosynaptic pages 8-10). 3) Antibodies bind cell-surface NMDAR and induce receptor crosslinking and internalization, reducing surface and synaptic receptor density, producing reversible synaptic dysfunction (dalmau2017autoantibodiestosynaptic pages 34-35, dalmau2016nmdareceptorencephalitis pages 7-9). 4) Network-level consequences include impaired hippocampal synaptic plasticity (LTP) and cognitive/behavioral phenotypes, consistent with functional NMDAR hypofunction (dalmau2016nmdareceptorencephalitis pages 7-9, dalmau2016nmdareceptorencephalitis pages 2-3).
Key mechanistic findings (authoritative sources)
- Crosslinking-dependent internalization: internalization is not blocked by NMDA receptor antagonism and is not reproduced by Fab fragments that cannot crosslink, implicating crosslinking as a mechanism (dalmau2017autoantibodiestosynaptic pages 34-35).
- Internalization kinetics and trafficking: internalization begins within ~2 hours and peaks by ~12 hours; internalized receptors traffic preferentially to Rab11-positive recycling endosomes more than lysosomes, with evidence of enhanced degradation (dalmau2017autoantibodiestosynaptic pages 34-35).
- Passive-transfer model reversibility and EphB2 pathway modulation: chronic infusion of patient CSF causes progressive antibody binding (maximal ~day 18), synaptic NMDAR loss, impaired LTP, and memory impairment, with reversibility after cessation; co-infusion of soluble ephrin‑B2 prevents pathogenic effects, implicating NMDAR–EphB2 synaptic interactions (dalmau2016nmdareceptorencephalitis pages 7-9, dalmau2017autoantibodiestosynaptic pages 37-38).
Blood–brain barrier (BBB) and immune trafficking
BBB dysfunction is proposed as enabling movement of antibodies and immune cells into the CNS. The BBB is described as “crucial for antibodies and immune cells to enter or exit the CNS,” with evidence supporting intrathecal B-cell involvement and cytokine signals consistent with BBB involvement (gong2023antinmdarantibodiesthe pages 1-2).
Suggested GO biological process / CL cell type terms
Examples include receptor internalization (GO:0031623), regulation of synaptic plasticity (GO:0048167), B cell mediated immunity (GO:0019724), immunoglobulin production (GO:0002377), and cell types B cell (CL:0000236) and plasma cell (CL:0000786) (artifact-01).
7. Anatomical Structures Affected
Organ/system level
- Primary: central nervous system (brain) (nguyen2023antinmdareceptorautoimmune pages 1-2, gong2023antinmdarantibodiesthe pages 1-2).
- Associated trigger sites: ovary (ovarian teratoma) (alsalek2024racialandethnic pages 1-2, nguyen2023antinmdareceptorautoimmune pages 5-6).
Tissue/cell level
- Neuronal synapses are directly affected through loss of synaptic NMDAR clusters (dalmau2016nmdareceptorencephalitis pages 7-9, dalmau2017autoantibodiestosynaptic pages 37-38).
- Immune cell involvement includes intrathecal B cells/plasma cells (dalmau2017autoantibodiestosynaptic pages 37-38, gong2023antinmdarantibodiesthe pages 1-2).
8. Temporal Development
Onset pattern
Typically subacute (rapid progression) with prodrome in a substantial fraction (40–70%) (nguyen2023antinmdareceptorautoimmune pages 3-5). Diagnostic criteria frameworks emphasize symptom accumulation within weeks and rapid onset within <3 months (nguyen2023antinmdareceptorautoimmune pages 3-5).
Post‑infectious timing
In post‑HSE anti‑NMDAR encephalitis, median time between HSE and NMDARE onset was 30 days (21–46) (dumez2024specificclinicaland pages 1-2).
Recovery trajectory
Cognitive recovery may continue for years; in one nationwide cohort, improvements continued up to 36 months, with persistent impairments common beyond 36 months (brenner2024longtermcognitivefunctional pages 1-2).
9. Inheritance and Population
Epidemiology (recent quantitative data)
A compact table of recent quantitative incidence/outcomes is provided below.
| Study (first author year, journal) | Design/setting | N | Key population notes | Incidence/prevalence (with units) | Tumor frequency | Relapse frequency | Mortality/fatality | Key prognostic factors/notes | URL/DOI |
|---|---|---|---|---|---|---|---|---|---|
| Nguyen 2023, Int J Gen Med | Review summarizing epidemiology and management | NR | Median age 21; 81% female in summarized data | Olmsted County incidence 0.4/100,000 (1995–2005) rising to 1.2/100,000 (2006–2015); autoimmune encephalitis prevalence 13.7/100,000 in 2014; anti-NMDAR prevalence 0.6/100,000 | NR in excerpt | 10–30% of cases, mostly within first 2 years | NR | CSF antibody testing more sensitive/specific than serum; all patients should be screened at least once for neoplasm (nguyen2023antinmdareceptorautoimmune pages 1-2) | https://doi.org/10.2147/IJGM.S397429 |
| Alsalek 2024, Neurol Neuroimmunol Neuroinflamm | Retrospective population-based cohort, Kaiser Permanente Southern California, 2011–2022 | 70 | Median age at onset 23.7 years; 64% female; >10 million person-years | Age- and sex-standardized incidence per 1 million person-years: Black 2.94 (95% CI 1.27–4.61), Hispanic 2.17 (1.51–2.83), Asian/Pacific Islander 2.02 (0.77–3.28), White 0.40 (0.08–0.72) | Ovarian teratomas in 58.3% of Black female individuals; 21 female patients overall had ovarian teratoma | NR | NR | CSF pleocytosis 70%, abnormal EEG 73%, abnormal MRI 40%; median time symptom onset to diagnosis 17 days; most patients (61.4%) had no identifiable trigger (alsalek2024racialandethnic pages 1-2) | https://doi.org/10.1212/NXI.0000000000200255 |
| Alentorn 2023, Biomedicines | Systematic review/meta-analysis of incidence studies | NR | Higher incidence reported in southern hemisphere regions; warm-month peak | Oceania 0.2/100,000 person-years; South America 0.16/100,000 person-years; Europe/North America 0.06/100,000 person-years | About half of cases associated with ovarian teratoma | NR | NR | Strong negative correlation with latitude (Pearson R = −0.88); positive association with extreme heat in France (p = 0.03) (alentorn2023spatialandecological pages 1-2) | https://doi.org/10.3390/biomedicines11061525 |
| Dumez 2024, J Neurol | Retrospective comparative cohort of post-HSE anti-NMDAR encephalitis | 13 post-HSE cases among 375 NMDARE patients | Median age 19 years; 31% children <4 years; 54% male; median latency 30 days after HSE | HSE incidence noted as 2–4 per million/year | NR | NR | NR | Worse 12-month mRS than regular NMDARE; behavioral changes 92%, movement disorders 62%, dysautonomia 54%; extensive MRI lesions 100% vs 48% and bilateral DWI abnormalities 90% vs 29% versus regular HSE comparators (dumez2024specificclinicaland pages 1-2) | https://doi.org/10.1007/s00415-024-12615-7 |
| Xu 2020, Neurol Neuroimmunol Neuroinflamm | Single-center prospective cohort, China, 2011–2017 | 220 | Acute onset with characteristic neuropsychiatric manifestations | NR | 19.5% had neoplasm; ovarian teratoma was 100% of tumors in females | 17.3% during first 12 months | 2.3% died within first 12 months | 94.1% improved during first 12 months; 92.7% had favorable outcome (mRS ≤2) at 12 months; 99.5% received first-line therapy; 7.3% received second-line therapy (xu2020antinmdarencephalitis pages 1-2) | https://doi.org/10.1212/NXI.0000000000000633 |
| Gong 2021, Neurol Neuroimmunol Neuroinflamm | Prospective observational cohort, Western China | 244 | Median age 26; 52.45% female; median follow-up 40 months | NR | 15.57% had tumors | 15.9%; 82.0% of first relapses within 24 months | 6.96% fatality | 84.8% improved within 4 weeks after immunotherapy; 80.7% and 85.7% had substantial recovery at 12 and 24 months; disturbance of consciousness in first month independently predicted poor outcome (OR 2.91, 95% CI 1.27–6.65); female sex and delayed treatment linked to relapse (gong2021longtermfunctionaloutcomes pages 1-2) | https://doi.org/10.1212/NXI.0000000000000958 |
| Balu 2019, Neurology | Multicenter cohort developing prognostic score | 382 | Anti-GluN1 antibody-associated disease | NR | NR | NR | NR | NEOS score predictors: ICU admission, treatment delay >4 weeks, lack of improvement within 4 weeks, abnormal MRI, CSF WBC >20 cells/μL; poor 1-year outcome ranged from 3% (0–1 points) to 69% (4–5 points) (balu2019ascorethat pages 1-2) | https://doi.org/10.1212/WNL.0000000000006783 |
| Brenner 2023, Neurology | Retrospective biomarker study with healthy references | 71 patients; 61 references | 75% female; mean age 31.4 years; paired CSF available in 33 | NR | NR | Reported 12% relapse within 2 years in background summary | NR | Serum NfL 19.5 pg/mL vs 6.4 pg/mL in references (p < 0.0001); CSF-serum NfL correlation R = 0.84; post-HSV patients 248.8 vs 14.1 pg/mL; association with 12-month mRS largely confounded by age (brenner2023predictivevalueof pages 1-2) | https://doi.org/10.1212/WNL.0000000000207221 |
| Brenner 2024, Neurology | Nationwide cross-sectional/prospective cohort | 92 | Mean age 29 ± 2 years; 77% female | NR | NR | NR | NR | Recovery continued up to 36 months; beyond 36 months, 34% had persistent impairment and 65% scored below average in ≥1 cognitive domain; 91% had favorable mRS ≤2, yet 30% did not resume school/work and 18% needed adjustments (nguyen2023antinmdareceptorautoimmune pages 1-2) | https://doi.org/10.1212/WNL.0000000000210109 |
Table: This table compiles the main quantitative epidemiology, trigger, relapse, mortality, and prognosis figures for anti-NMDA receptor encephalitis from the retrieved evidence. It is useful as a compact reference for populating disease knowledge-base fields with explicitly supported numbers.
Key recent statistics include: - US population-based incidence disparities (2011–2022): standardized incidence per 1 million person‑years: Black 2.94; Hispanic 2.17; Asian/PI 2.02; White 0.40 (alsalek2024racialandethnic pages 1-2). - Climate/geography associations: incidence estimates and latitude/temperature associations in systematic review/meta-analysis (alentorn2023spatialandecological pages 1-2).
10. Diagnostics
Clinical criteria and practical diagnostic approach
Guidelines emphasize exclusion of infectious mimics (notably HSV encephalitis), with routine blood/CSF analysis and MRI often sufficient to evaluate alternative causes; importantly, HSV CSF PCR can be negative early and may need repeating if suspicion remains high (graus2016aclinicalapproach pages 6-7).
Anti‑NMDAR encephalitis can be approached with syndrome-based criteria for probable diagnosis and confirmed via antibody testing; supportive findings include abnormal EEG and CSF inflammatory markers (nguyen2023antinmdareceptorautoimmune pages 3-5).
Antibody testing: CSF vs serum
CSF testing is more sensitive and specific than serum. Review synthesis reports serum false-positives (up to 23.2%) and some serum reactivity in healthy controls; a substantial fraction of patients may be CSF‑only positive (reported 28–38.2% across series), supporting testing of both CSF and serum (nguyen2023antinmdareceptorautoimmune pages 3-5).
CSF abnormalities
Across cohorts, CSF pleocytosis has been reported in ~47–91% and oligoclonal bands in ~25–62.6% (nguyen2023antinmdareceptorautoimmune pages 3-5). In the Kaiser Permanente cohort, CSF pleocytosis was present in 70% (alsalek2024racialandethnic pages 1-2).
EEG and MRI
- EEG is abnormal in most cases; one review notes EEG abnormality in 83.6% and describes extreme delta brush as a specific pattern, defined as “rhythmic delta activity at 1–3 Hz with bursts of rhythmic beta activity,” occurring in ~6.7% (nguyen2023antinmdareceptorautoimmune pages 5-6).
- Brain MRI can be normal in many patients; in Kaiser Permanente, abnormal MRI was 40% (alsalek2024racialandethnic pages 1-2).
Real-world diagnostic implementation notes
- “Treatment for suspected AE is often given empirically” while awaiting antibody results, reflecting real-world delays in definitive testing (nguyen2023antinmdareceptorautoimmune pages 6-7).
11. Outcome / Prognosis
Functional outcomes and relapse
- Prospective China cohort (n=220): within 12 months, 94.1% improved; 2.3% died; 17.3% relapsed; 92.7% had favorable 12‑month mRS ≤2 (xu2020antinmdarencephalitis pages 1-2).
- Prospective Western China cohort (n=244): fatality 6.96%; relapse 15.9% with most first relapses within 24 months; substantial recovery at 24 months 85.7% (gong2021longtermfunctionaloutcomes pages 1-2).
Prognostic scores
The NEOS score (anti‑NMDAR Encephalitis One‑Year Functional Status) uses five predictors: ICU admission, treatment delay >4 weeks, lack of improvement within 4 weeks, abnormal MRI, and CSF WBC >20 cells/µL; poor 1‑year outcome probability ranged from 3% (0–1 points) to 69% (4–5 points) (balu2019ascorethat pages 1-2).
Biomarkers (recent developments)
A 2023 Neurology study evaluated serum neurofilament light chain (NfL): serum NfL at diagnosis was higher in patients (mean 19.5 pg/mL) than references (mean 6.4 pg/mL, p<0.0001) and correlated with CSF NfL (R=0.84); post‑HSV cases had markedly higher levels (mean 248.8 vs 14.1 pg/mL) (brenner2023predictivevalueof pages 1-2).
12. Treatment
Current standard treatment strategy (real-world implementation)
A widely used approach is escalation of immunotherapy plus trigger removal (e.g., teratoma removal). First-line therapies include high-dose corticosteroids, IVIG, and plasma exchange; second-line therapies include rituximab or cyclophosphamide; refractory options may include bortezomib and tocilizumab (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune pages 6-7).
A key implementation point is that decisions should be guided by clinical status rather than serial antibody titers: titers have limited correlation with severity and serum titers are unreliable; CSF titers may be more useful for relapse assessment when compared to earlier samples (nguyen2023antinmdareceptorautoimmune pages 6-7).
Visual evidence: treatment options table
Nguyen & Wang (2023) provide a detailed “Table 2 Summary of Treatment Options,” including regimens and adverse effects (nguyen2023antinmdareceptorautoimmune media a2c6c545, nguyen2023antinmdareceptorautoimmune media e857af28).
Suggested MAXO terms
Examples include corticosteroid therapy, intravenous immunoglobulin therapy, plasma exchange therapy, rituximab therapy, cyclophosphamide therapy, tumor resection, and tumor screening (artifact-01).
13. Prevention
No established primary prevention is supported in the retrieved evidence base. Practical prevention focuses on secondary/tertiary prevention: early recognition, prompt immunotherapy escalation when needed, and evaluation for/removal of triggering tumors to reduce morbidity and relapse risk (nguyen2023antinmdareceptorautoimmune pages 6-7, xu2020antinmdarencephalitis pages 1-2).
14. Other Species / Natural Disease
No naturally occurring disease in other species was retrieved in the available evidence context.
15. Model Organisms
Mechanistic work includes passive-transfer models (e.g., chronic infusion of patient CSF) demonstrating reversible synaptic receptor loss, impaired LTP, and behavioral deficits; these are frequently used to interrogate synaptic mechanisms and potential rescue strategies (e.g., ephrin‑B2) (dalmau2016nmdareceptorencephalitis pages 7-9, dalmau2017autoantibodiestosynaptic pages 37-38).
Recent developments and latest research highlights (2023–2024 prioritized)
- Population incidence disparities (2024): large integrated health-system cohort quantified markedly higher incidence in Black, Hispanic, and Asian/Pacific Island populations vs White (alsalek2024racialandethnic pages 1-2).
- Climate/geography signal (2023): systematic review/meta-analysis reported latitude/temperature/UV associations with incidence estimates across regions (alentorn2023spatialandecological pages 1-2).
- BBB-focused synthesis (2023): emphasizes BBB’s role in immune-cell/antibody trafficking and intrathecal immune activation (gong2023antinmdarantibodiesthe pages 1-2).
- Biomarker development (2023): serum NfL differences vs controls and HSV-associated elevations, with limitations due to age confounding and sampling timing (brenner2023predictivevalueof pages 1-2).
- Long-term outcomes (2024): persistent cognitive and patient-reported deficits despite favorable mRS; substantial impacts on return-to-work/school (brenner2024longtermcognitivefunctional pages 1-2).
- Post‑HSE phenotype refinement (2024): HSE-triggered NMDARE shows distinctive clinical and MRI severity features and worse 12‑month outcomes (dumez2024specificclinicaland pages 1-2).
Current applications and real-world implementations
- Diagnostic workflows commonly prioritize CSF antibody testing, EEG/MRI supportive evidence, and repeated HSV testing if early PCR negative and suspicion remains high (nguyen2023antinmdareceptorautoimmune pages 3-5, graus2016aclinicalapproach pages 6-7).
- Tumor screening (especially ovarian teratoma evaluation in appropriate demographic groups) is recommended at least once; repeat imaging schedules for higher-risk groups have been proposed in reviews (nguyen2023antinmdareceptorautoimmune pages 5-6).
- Treatment escalation pathways (steroids/IVIG/PLEX → rituximab/cyclophosphamide → refractory biologics/proteasome inhibitors) are used clinically despite limited RCT evidence (nguyen2023antinmdareceptorautoimmune pages 6-7).
Clinical trials / registries (ClinicalTrials.gov)
- NCT03274375 (Phase 2; recruiting; start 2021‑06‑23; est. completion 2026‑06): immunoadsorption sessions + rituximab in severe pediatric disease (NCT03274375 chunk 1).
- NCT06183788 (AMENDS) (recruiting; start 2023‑01‑16): remote cognitive rehabilitation and biomarker/mechanism characterization in post‑acute stage (NCT06183788 chunk 1).
- NCT06023160 (NEOSII) (observational; 714 participants): develop NEOS2 score for outcome and first-line response prediction (NCT06023160 chunk 1).
- NCT02559089 and NCT02443350 (China/Beijing registries; ~400 enrollment each): clinical registries to build databases and evaluate outcomes (e.g., death endpoints) (NCT02559089 chunk 1, NCT02443350 chunk 1).
- NCT04339127 (retrospective; ~12 participants): post‑herpetic anti‑NMDAR encephalitis characterization (NCT04339127 chunk 1).
Ontology mapping artifact
| Category | Suggested ontology | Term label | Term ID | Evidence-supported rationale |
|---|---|---|---|---|
| Disease | MONDO | anti-NMDA receptor encephalitis | MONDO_0021081 | OpenTargets identifies the disease as anti-NMDA receptor encephalitis with MONDO_0021081, matching the requested disease concept (OpenTargets Search: Anti-NMDA receptor encephalitis). |
| Anatomy | UBERON | brain | UBERON:0000955 | Anti-NMDAR encephalitis is a CNS autoimmune encephalitis with neuropsychiatric, seizure, and cognitive manifestations indicating primary brain involvement (nguyen2023antinmdareceptorautoimmune pages 1-2, gong2023antinmdarantibodiesthe pages 1-2). |
| Anatomy | UBERON | hippocampus | UBERON:0001954 | Mechanistic studies describe impaired hippocampal synaptic activity/plasticity and hippocampal binding of patient antibodies, supporting hippocampal involvement (gong2023antinmdarantibodiesthe pages 1-2, dalmau2016nmdareceptorencephalitis pages 7-9). |
| Anatomy | UBERON | cerebrospinal fluid | UBERON:0001359 | CSF is the preferred compartment for antibody detection and frequently shows pleocytosis or oligoclonal bands in this disease (nguyen2023antinmdareceptorautoimmune pages 3-5, nguyen2023antinmdareceptorautoimmune pages 5-6). |
| Anatomy | UBERON | blood-brain barrier | UBERON:0013702 | BBB dysfunction is implicated because the BBB is described as crucial for antibody and immune-cell trafficking into and out of the CNS (gong2023antinmdarantibodiesthe pages 1-2). |
| Anatomy | UBERON | ovary | UBERON:0000992 | Ovarian teratoma is the major tumor trigger, especially in female patients, supporting ovary as a key associated anatomical site (nguyen2023antinmdareceptorautoimmune pages 5-6, alsalek2024racialandethnic pages 1-2). |
| Cell type | CL | B cell | CL:0000236 | CNS B-cell expansion and intrathecal antibody production are described in anti-NMDAR encephalitis, making B cells a central disease-relevant cell type (gong2023antinmdarantibodiesthe pages 1-2, dalmau2017autoantibodiestosynaptic pages 8-10). |
| Cell type | CL | plasma cell | CL:0000786 | Intrathecal plasma cells are a reported source of GluN1 autoantibodies in mechanistic studies (dalmau2017autoantibodiestosynaptic pages 37-38, dalmau2017autoantibodiestosynaptic pages 8-10). |
| Cell type | CL | neuron | CL:0000540 | Patient antibodies bind neuronal surface NMDARs and alter synaptic receptor density and function, implicating neurons as the primary target cell type (dalmau2017autoantibodiestosynaptic pages 34-35, dalmau2016nmdareceptorencephalitis pages 2-3). |
| Subcellular | GO | synapse | GO:0045202 | Anti-NMDAR antibodies reduce synaptic NMDAR density and disrupt synaptic plasticity, so synapse is a core affected compartment (dalmau2017autoantibodiestosynaptic pages 37-38, gong2023antinmdarantibodiesthe pages 1-2). |
| Subcellular | GO | plasma membrane | GO:0005886 | The pathogenic antibodies bind cell-surface NMDARs and decrease surface receptor density/localization (dalmau2016nmdareceptorencephalitis pages 2-3, gong2023antinmdarantibodiesthe pages 1-2). |
| Subcellular | GO | recycling endosome | GO:0055037 | Internalized receptors preferentially traffic to Rab11-positive recycling endosomes in mechanistic studies (dalmau2017autoantibodiestosynaptic pages 34-35). |
| Phenotype | HPO | Psychiatric symptoms | HP:0000708 | Psychiatric/behavioral symptoms are among the most common presenting features, affecting about 90% of teenagers/adults in review data (nguyen2023antinmdareceptorautoimmune pages 3-5). |
| Phenotype | HPO | Seizure | HP:0001250 | Seizures are a core diagnostic manifestation and occurred in 80.9% of a 220-patient cohort and 67% of a 106-patient cohort (xu2020antinmdarencephalitis pages 1-2, wang2020influencingelectroclinicalfeatures pages 1-2). |
| Phenotype | HPO | Dyskinesia | HP:0100660 | Movement disorder, especially orolingual-facial dyskinesia, is characteristic of anti-NMDAR encephalitis (nguyen2023antinmdareceptorautoimmune pages 3-5). |
| Phenotype | HPO | Autonomic dysfunction | HP:0002271 | Autonomic dysfunction is included in diagnostic criteria and includes instability of temperature, salivation, blood pressure, heart rate, and continence (nguyen2023antinmdareceptorautoimmune pages 3-5, ho2017highsensitivityand pages 3-3). |
| Phenotype | HPO | Central hypoventilation | HP:0007110 | Central hypoventilation is a recognized core manifestation linked to ICU care and worse prognosis (nguyen2023antinmdareceptorautoimmune pages 3-5, ho2017highsensitivityand pages 3-3). |
| Phenotype | HPO | Memory impairment | HP:0002354 | Memory deficits are frequent in the acute syndrome and remain a major long-term deficit domain in survivors (brenner2024longtermcognitivefunctional pages 1-2, xu2020antinmdarencephalitis pages 1-2). |
| Phenotype | HPO | Language impairment | HP:0002465 | Language scores remain persistently reduced in long-term follow-up and speech dysfunction is a core diagnostic domain (brenner2024longtermcognitivefunctional pages 1-2, ho2017highsensitivityand pages 3-3). |
| Phenotype | HPO | Mutism | HP:0002300 | Speech dysfunction in anti-NMDAR encephalitis includes verbal reduction and mutism in clinical criteria/reviews (nguyen2023antinmdareceptorautoimmune pages 3-5). |
| Phenotype | HPO | Cerebrospinal fluid pleocytosis | HP:0012675 | CSF pleocytosis is common, with reported frequencies ranging from 47% to 91% across cohorts (nguyen2023antinmdareceptorautoimmune pages 3-5, alsalek2024racialandethnic pages 1-2). |
| Phenotype | HPO | Oligoclonal bands in cerebrospinal fluid | HP:0032150 | Positive CSF oligoclonal bands are reported in roughly 25% to 62.6% of cases across studies (nguyen2023antinmdareceptorautoimmune pages 3-5, nguyen2023antinmdareceptorautoimmune pages 5-6). |
| Phenotype | HPO | Abnormality of EEG | HP:0002353 | EEG is abnormal in most patients and supports diagnosis when antibody results are pending (nguyen2023antinmdareceptorautoimmune pages 5-6, alsalek2024racialandethnic pages 1-2). |
| Phenotype | HPO | Delta brush EEG pattern | ID not retrieved | Extreme delta brush is a disease-associated EEG pattern specifically highlighted in anti-NMDAR encephalitis diagnostic discussions (nguyen2023antinmdareceptorautoimmune pages 3-5, graus2016aclinicalapproach pages 6-7). |
| Process | GO | receptor internalization | GO:0031623 | Patient antibodies cause NMDAR loss primarily through receptor crosslinking and internalization rather than agonist activation (dalmau2017autoantibodiestosynaptic pages 34-35, dalmau2016nmdareceptorencephalitis pages 1-2). |
| Process | GO | regulation of synaptic plasticity | GO:0048167 | Loss of synaptic NMDARs impairs long-term potentiation and broader synaptic plasticity in passive-transfer studies (dalmau2016nmdareceptorencephalitis pages 7-9, dalmau2017autoantibodiestosynaptic pages 37-38). |
| Process | GO | trans-synaptic signaling | GO:0099537 | Reduced synaptic receptor density and altered hippocampal signaling support disruption of synaptic communication pathways (gong2023antinmdarantibodiesthe pages 1-2). |
| Process | GO | B cell mediated immunity | GO:0019724 | Disease pathogenesis involves autoreactive B cells and intrathecal antibody-producing cells targeting GluN1 (gong2023antinmdarantibodiesthe pages 1-2, dalmau2017autoantibodiestosynaptic pages 8-10). |
| Process | GO | immunoglobulin production | GO:0002377 | Intrathecal synthesis of anti-GluN1 antibodies by B cells/plasma cells is part of the proposed pathogenic cascade (dalmau2017autoantibodiestosynaptic pages 37-38, dalmau2017autoantibodiestosynaptic pages 8-10). |
| Process | GO | blood-brain barrier maintenance | GO:1990961 | BBB dysfunction is repeatedly proposed as enabling entry/exit of antibodies and immune cells in anti-NMDAR encephalitis (gong2023antinmdarantibodiesthe pages 1-2). |
| Treatment | MAXO | corticosteroid therapy | ID not retrieved | High-dose corticosteroids are standard first-line immunotherapy in anti-NMDAR encephalitis management algorithms (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune pages 6-7). |
| Treatment | CHEBI | methylprednisolone | CHEBI:6888 | IV methylprednisolone is explicitly listed as a first-line treatment option and regimen in the treatment table (nguyen2023antinmdareceptorautoimmune pages 6-7, nguyen2023antinmdareceptorautoimmune media a2c6c545). |
| Treatment | MAXO | intravenous immunoglobulin therapy | ID not retrieved | IVIG is a standard first-line immunotherapy and commonly combined with steroids in clinical practice (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune pages 6-7). |
| Treatment | CHEBI | immunoglobulin | CHEBI:59132 | IVIG is directly listed in treatment recommendations and Table 2 for anti-NMDAR encephalitis (nguyen2023antinmdareceptorautoimmune pages 6-7, nguyen2023antinmdareceptorautoimmune media a2c6c545). |
| Treatment | MAXO | plasma exchange therapy | ID not retrieved | Plasma exchange/PLEX is a recommended first-line therapy for acute disease (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune pages 6-7). |
| Treatment | MAXO | rituximab therapy | ID not retrieved | Rituximab is the best-established second-line escalation therapy for refractory disease and relapse prevention (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune pages 6-7). |
| Treatment | CHEBI | rituximab | CHEBI:64357 | Rituximab is specifically named in the treatment table as second-line immunotherapy (nguyen2023antinmdareceptorautoimmune pages 6-7, nguyen2023antinmdareceptorautoimmune media a2c6c545). |
| Treatment | MAXO | cyclophosphamide therapy | ID not retrieved | Cyclophosphamide is a recommended second-line agent for refractory anti-NMDAR encephalitis (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune pages 6-7). |
| Treatment | CHEBI | cyclophosphamide | CHEBI:4027 | Cyclophosphamide appears in the treatment table as a second-line immunotherapy option (nguyen2023antinmdareceptorautoimmune pages 6-7, nguyen2023antinmdareceptorautoimmune media a2c6c545). |
| Treatment | MAXO | tocilizumab therapy | ID not retrieved | Tocilizumab is described as a complementary option in refractory cases beyond standard second-line therapy (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune media a2c6c545). |
| Treatment | CHEBI | tocilizumab | CHEBI:71416 | Tocilizumab is included among escalation/refractory therapies in the visualized treatment table (nguyen2023antinmdareceptorautoimmune media a2c6c545, nguyen2023antinmdareceptorautoimmune media e857af28). |
| Treatment | MAXO | bortezomib therapy | ID not retrieved | Bortezomib is considered in refractory cases when standard escalation is insufficient (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune media a2c6c545). |
| Treatment | CHEBI | bortezomib | CHEBI:52717 | Bortezomib is listed among additional escalation therapies in the treatment table (nguyen2023antinmdareceptorautoimmune media e857af28). |
| Treatment | MAXO | mycophenolate mofetil therapy | ID not retrieved | Mycophenolate mofetil is used as prolonged/maintenance immunotherapy in some cohorts and tables (xu2020antinmdarencephalitis pages 1-2, nguyen2023antinmdareceptorautoimmune media e857af28). |
| Treatment | CHEBI | mycophenolate mofetil | CHEBI:31824 | MMF is specifically listed as a maintenance therapy and was used >1 year in a large Chinese cohort (xu2020antinmdarencephalitis pages 1-2, nguyen2023antinmdareceptorautoimmune media e857af28). |
| Treatment | MAXO | azathioprine therapy | ID not retrieved | Azathioprine is used as long-term maintenance immunotherapy in some patients after the acute phase (xu2020antinmdarencephalitis pages 1-2, nguyen2023antinmdareceptorautoimmune media e857af28). |
| Treatment | CHEBI | azathioprine | CHEBI:22636 | Azathioprine is named in the treatment table and in long-term immunotherapy descriptions (xu2020antinmdarencephalitis pages 1-2, nguyen2023antinmdareceptorautoimmune media e857af28). |
| Treatment | MAXO | tumor resection | ID not retrieved | Treatment guidance emphasizes teratoma removal alongside immunotherapy when an ovarian teratoma is present (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune pages 6-7). |
| Treatment | MAXO | tumor screening | ID not retrieved | All patients should be screened at least once for neoplasm, and female patients may need serial pelvic imaging because ovarian teratoma is a common trigger (nguyen2023antinmdareceptorautoimmune pages 1-2, nguyen2023antinmdareceptorautoimmune pages 5-6). |
Table: This table maps key anti-NMDA receptor encephalitis concepts to suggested ontology terms across disease, anatomy, cell type, phenotype, process, and treatment categories. It is evidence-aligned to the retrieved literature and can help populate a structured disease knowledge base.
Notes on citation requirements (PMID)
Where possible, this report cites primary literature and major reviews with DOI and publication year/month extracted from the retrieved sources. PMIDs were not available in the current tool context for most items, so they are not included to avoid introducing unsupported identifiers.
References
-
(nguyen2023antinmdareceptorautoimmune pages 1-2): Linda Nguyen and Cynthia X. Wang. Anti-nmda receptor autoimmune encephalitis: diagnosis and management strategies. International Journal of General Medicine, 16:7-21, Jan 2023. URL: https://doi.org/10.2147/ijgm.s397429, doi:10.2147/ijgm.s397429. This article has 128 citations.
-
(nguyen2023antinmdareceptorautoimmune pages 3-5): Linda Nguyen and Cynthia X. Wang. Anti-nmda receptor autoimmune encephalitis: diagnosis and management strategies. International Journal of General Medicine, 16:7-21, Jan 2023. URL: https://doi.org/10.2147/ijgm.s397429, doi:10.2147/ijgm.s397429. This article has 128 citations.
-
(gong2021longtermfunctionaloutcomes pages 1-2): Xue Gong, Chu Chen, Xu Liu, Jingfang Lin, Aiqing Li, Kundian Guo, Dong Zhou, and Zhen Hong. Long-term functional outcomes and relapse of anti-nmda receptor encephalitis. Neurology Neuroimmunology & Neuroinflammation, Mar 2021. URL: https://doi.org/10.1212/nxi.0000000000000958, doi:10.1212/nxi.0000000000000958. This article has 97 citations.
-
(OpenTargets Search: Anti-NMDA receptor encephalitis): Open Targets Query (Anti-NMDA receptor encephalitis, 0 results). Buniello, A. et al. (2025). Open Targets Platform: facilitating therapeutic hypotheses building in drug discovery. Nucleic Acids Research.
-
(dumez2024specificclinicaland pages 1-2): Pauline Dumez, Macarena Villagrán-García, Alexandre Bani-Sadr, Marie Benaiteau, Elise Peter, Antonio Farina, Géraldine Picard, Véronique Rogemond, Marie-Camille Ruitton-Allinieu, François Cotton, Mélodie Aubart, Marie Hully, Jean-Christophe Antoine, Bastien Joubert, and Jérôme Honnorat. Specific clinical and radiological characteristics of anti-nmda receptor autoimmune encephalitis following herpes encephalitis. Journal of Neurology, 271:6692-6701, Aug 2024. URL: https://doi.org/10.1007/s00415-024-12615-7, doi:10.1007/s00415-024-12615-7. This article has 11 citations and is from a domain leading peer-reviewed journal.
-
(gong2023antinmdarantibodiesthe pages 1-2): Xiarong Gong, Niya Wang, Hongyan Zhu, Ning Tang, Kunhua Wu, and Qiang Meng. Anti-nmdar antibodies, the blood–brain barrier, and anti-nmdar encephalitis. Frontiers in Neurology, Dec 2023. URL: https://doi.org/10.3389/fneur.2023.1283511, doi:10.3389/fneur.2023.1283511. This article has 13 citations and is from a peer-reviewed journal.
-
(alsalek2024racialandethnic pages 1-2): Samir Alsalek, Kathryn B. Schwarzmann, Sakar Budhathoki, Viridiana Hernandez-Lopez, Jessica B. Smith, Bonnie H. Li, and Annette Langer-Gould. Racial and ethnic disparities in the incidence of anti-nmda receptor encephalitis. Neurology Neuroimmunology & Neuroinflammation, Jul 2024. URL: https://doi.org/10.1212/nxi.0000000000200255, doi:10.1212/nxi.0000000000200255. This article has 27 citations.
-
(dalmau2016nmdareceptorencephalitis pages 7-9): Josep Dalmau. Nmda receptor encephalitis and other antibody-mediated disorders of the synapse. Neurology, 87:2471-2482, Dec 2016. URL: https://doi.org/10.1212/wnl.0000000000003414, doi:10.1212/wnl.0000000000003414. This article has 286 citations and is from a highest quality peer-reviewed journal.
-
(NCT03274375 chunk 1): Immunoadsorption Therapy in Managing NMDAR Antibodies Encephalitis. Assistance Publique - Hôpitaux de Paris. 2021. ClinicalTrials.gov Identifier: NCT03274375
-
(nguyen2023antinmdareceptorautoimmune pages 5-6): Linda Nguyen and Cynthia X. Wang. Anti-nmda receptor autoimmune encephalitis: diagnosis and management strategies. International Journal of General Medicine, 16:7-21, Jan 2023. URL: https://doi.org/10.2147/ijgm.s397429, doi:10.2147/ijgm.s397429. This article has 128 citations.
-
(brenner2024longtermcognitivefunctional pages 1-2): Juliette Brenner, Cinthia J. Ruhe, Ilse Kulderij, Anna E.M. Bastiaansen, Yvette S. Crijnen, Chelsey N. Kret, Julia C.P. Verkoelen, Anke A.G. Tolido, Brigit Thomassen, Laura P. Kersten, Marienke A.A.M. de Bruijn, Sammy H.C. Olijslagers, Melissa R. Mandarakas, Jeroen Kerstens, Robin W. van Steenhoven, Juna M. de Vries, Sharon Veenbergen, Marco W.J. Schreurs, Rinze F. Neuteboom, Peter A.E. Sillevis Smitt, Esther van den Berg, and Maarten J. Titulaer. Long-term cognitive, functional, and patient-reported outcomes in patients with anti-nmdar encephalitis. Dec 2024. URL: https://doi.org/10.1212/wnl.0000000000210109, doi:10.1212/wnl.0000000000210109. This article has 28 citations and is from a highest quality peer-reviewed journal.
-
(alentorn2023spatialandecological pages 1-2): Agustí Alentorn, Giulia Berzero, Harry Alexopoulos, John Tzartos, Germán Reyes Botero, Andrea Morales Martínez, Sergio Muñiz-Castrillo, Alberto Vogrig, Bastien Joubert, Francisco A. García Jiménez, Dagoberto Cabrera, José Vladimir Tobon, Carolina Delgado, Patricio Sandoval, Mónica Troncoso, Lorna Galleguillos, Marine Giry, Marion Benazra, Isaias Hernández Verdin, Maëlle Dade, Géraldine Picard, Véronique Rogemond, Nicolas Weiss, Marinos C. Dalakas, Pierre-Yves Boëlle, Jean-Yves Delattre, Jérôme Honnorat, and Dimitri Psimaras. Spatial and ecological factors modulate the incidence of anti-nmdar encephalitis—a systematic review. Biomedicines, 11:1525, May 2023. URL: https://doi.org/10.3390/biomedicines11061525, doi:10.3390/biomedicines11061525. This article has 9 citations.
-
(xu2020antinmdarencephalitis pages 1-2): Xiaolu Xu, Qiang Lu, Yan Huang, Siyuan Fan, Lixin Zhou, Jing Yuan, Xunzhe Yang, Haitao Ren, Dawei Sun, Yi Dai, Huadong Zhu, Yinan Jiang, Yicheng Zhu, Bin Peng, Liying Cui, and Hongzhi Guan. Anti-nmdar encephalitis. Neurology Neuroimmunology & Neuroinflammation, Jan 2020. URL: https://doi.org/10.1212/nxi.0000000000000633, doi:10.1212/nxi.0000000000000633. This article has 187 citations.
-
(wang2020influencingelectroclinicalfeatures pages 1-2): Yingxin Wang, Ailiang Miao, Yongwei Shi, Jianqing Ge, Ling-ling Wang, Chuanyong Yu, Haiyan Xu, Yuanwen Yu, Shuyang Huang, Yihan Li, and Xiaoshan Wang. Influencing electroclinical features and prognostic factors in patients with anti-nmdar encephalitis: a cohort follow-up study in chinese patients. Scientific Reports, Jul 2020. URL: https://doi.org/10.1038/s41598-020-67485-6, doi:10.1038/s41598-020-67485-6. This article has 22 citations and is from a peer-reviewed journal.
-
(balu2019ascorethat pages 1-2): Ramani Balu, Lindsey McCracken, Eric Lancaster, Francesc Graus, Josep Dalmau, and Maarten J. Titulaer. A score that predicts 1-year functional status in patients with anti-nmda receptor encephalitis. Neurology, Jan 2019. URL: https://doi.org/10.1212/wnl.0000000000006783, doi:10.1212/wnl.0000000000006783. This article has 351 citations and is from a highest quality peer-reviewed journal.
-
(dalmau2017autoantibodiestosynaptic pages 8-10): Josep Dalmau, Christian Geis, and Francesc Graus. Autoantibodies to synaptic receptors and neuronal cell surface proteins in autoimmune diseases of the central nervous system. Physiological reviews, 97 2:839-887, Apr 2017. URL: https://doi.org/10.1152/physrev.00010.2016, doi:10.1152/physrev.00010.2016. This article has 730 citations and is from a highest quality peer-reviewed journal.
-
(dalmau2017autoantibodiestosynaptic pages 37-38): Josep Dalmau, Christian Geis, and Francesc Graus. Autoantibodies to synaptic receptors and neuronal cell surface proteins in autoimmune diseases of the central nervous system. Physiological reviews, 97 2:839-887, Apr 2017. URL: https://doi.org/10.1152/physrev.00010.2016, doi:10.1152/physrev.00010.2016. This article has 730 citations and is from a highest quality peer-reviewed journal.
-
(dalmau2017autoantibodiestosynaptic pages 34-35): Josep Dalmau, Christian Geis, and Francesc Graus. Autoantibodies to synaptic receptors and neuronal cell surface proteins in autoimmune diseases of the central nervous system. Physiological reviews, 97 2:839-887, Apr 2017. URL: https://doi.org/10.1152/physrev.00010.2016, doi:10.1152/physrev.00010.2016. This article has 730 citations and is from a highest quality peer-reviewed journal.
-
(dalmau2016nmdareceptorencephalitis pages 2-3): Josep Dalmau. Nmda receptor encephalitis and other antibody-mediated disorders of the synapse. Neurology, 87:2471-2482, Dec 2016. URL: https://doi.org/10.1212/wnl.0000000000003414, doi:10.1212/wnl.0000000000003414. This article has 286 citations and is from a highest quality peer-reviewed journal.
-
(brenner2023predictivevalueof pages 1-2): Juliette Brenner, Sara Mariotto, Anna E.M. Bastiaansen, Manuela Paunovic, Sergio Ferrari, Daniela Alberti, Marienke A.A.M. de Bruijn, Yvette S. Crijnen, Marco W.J. Schreurs, Rinze F. Neuteboom, Jan G.M.C. Damoiseaux, Juna M. de Vries, and Maarten J. Titulaer. Predictive value of serum neurofilament light chain levels in anti-nmda receptor encephalitis. Neurology, May 2023. URL: https://doi.org/10.1212/wnl.0000000000207221, doi:10.1212/wnl.0000000000207221. This article has 33 citations and is from a highest quality peer-reviewed journal.
-
(graus2016aclinicalapproach pages 6-7): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(nguyen2023antinmdareceptorautoimmune pages 6-7): Linda Nguyen and Cynthia X. Wang. Anti-nmda receptor autoimmune encephalitis: diagnosis and management strategies. International Journal of General Medicine, 16:7-21, Jan 2023. URL: https://doi.org/10.2147/ijgm.s397429, doi:10.2147/ijgm.s397429. This article has 128 citations.
-
(nguyen2023antinmdareceptorautoimmune media a2c6c545): Linda Nguyen and Cynthia X. Wang. Anti-nmda receptor autoimmune encephalitis: diagnosis and management strategies. International Journal of General Medicine, 16:7-21, Jan 2023. URL: https://doi.org/10.2147/ijgm.s397429, doi:10.2147/ijgm.s397429. This article has 128 citations.
-
(nguyen2023antinmdareceptorautoimmune media e857af28): Linda Nguyen and Cynthia X. Wang. Anti-nmda receptor autoimmune encephalitis: diagnosis and management strategies. International Journal of General Medicine, 16:7-21, Jan 2023. URL: https://doi.org/10.2147/ijgm.s397429, doi:10.2147/ijgm.s397429. This article has 128 citations.
-
(NCT06183788 chunk 1): Antibody-mediated NMDA Receptor Encephalitis: Symptoms, Biomarkers, and Mechanisms of the Prolonged Recovery Stage. Fundacion Clinic per a la Recerca Biomédica. 2023. ClinicalTrials.gov Identifier: NCT06183788
-
(NCT06023160 chunk 1): Dr. Maarten J. Titulaer. MD, PhD. Predicting Functional Outcome and Response to Therapy of Anti-NMDAR Encephalitis at Diagnosis. Erasmus Medical Center. 2020. ClinicalTrials.gov Identifier: NCT06023160
-
(NCT02559089 chunk 1): Jia Wei Wang,MD. Multicenter and Prospective Clinical Registry Study of Anti-N-methyl-D-aspartate Receptor Encephalitis in China. Beijing Tongren Hospital. 2015. ClinicalTrials.gov Identifier: NCT02559089
-
(NCT02443350 chunk 1): Jia Wei Wang,MD. Multicenter and Prospective Clinical Registry Study of Anti-N-methyl-D-aspartate Receptor Encephalitis in Beijing Area. Jia Wei Wang,MD. 2014. ClinicalTrials.gov Identifier: NCT02443350
-
(NCT04339127 chunk 1): Autoimmune Encephalitis With Anti-NMDA Receptor Antibodies Following Herpetic Encephalitis. Hospices Civils de Lyon. 2020. ClinicalTrials.gov Identifier: NCT04339127
-
(ho2017highsensitivityand pages 3-3): Alvin C C Ho, Shekeeb S Mohammad, Sekhar C Pillai, Esther Tantsis, Hannah Jones, Reena Ho, Ming Lim, Yael Hacohen, Angela Vincent, and Russell C Dale. High sensitivity and specificity in proposed clinical diagnostic criteria for anti‐n‐methyl‐d‐aspartate receptor encephalitis. Developmental Medicine & Child Neurology, 59:1256-1260, Oct 2017. URL: https://doi.org/10.1111/dmcn.13579, doi:10.1111/dmcn.13579. This article has 70 citations and is from a highest quality peer-reviewed journal.
-
(dalmau2016nmdareceptorencephalitis pages 1-2): Josep Dalmau. Nmda receptor encephalitis and other antibody-mediated disorders of the synapse. Neurology, 87:2471-2482, Dec 2016. URL: https://doi.org/10.1212/wnl.0000000000003414, doi:10.1212/wnl.0000000000003414. This article has 286 citations and is from a highest quality peer-reviewed journal.