1. Disease Information
1.1 Concise overview (current understanding)
Volumetric muscle loss (VML) is most commonly defined clinically as “the traumatic or surgical loss of skeletal muscle with resultant functional impairment.” (grogan2011volumetricmuscleloss pages 1-3, greising2019therapeuticapproachesfor pages 6-8). A key distinguishing feature is that VML represents tissue loss beyond typical skeletal muscle regenerative capacity, producing chronic functional deficits and disability (greising2019therapeuticapproachesfor pages 3-5, gahlawat2024tissueengineered3d pages 1-3).
Operational definitions vary across publications and settings: - A biomaterials paper describes VML as “a loss of over ~10% of muscle mass that results in functional impairment.” (Patel 2019; publication date Apr 2019; https://doi.org/10.1088/1748-605x/ab0b06) (patel2019alignednanofibersof pages 1-5). - A 2024 review cites a frequently used translational threshold: “When the loss of skeletal muscle exceeds 20%, the innate capacity for repair and regeneration is permanently compromised.” (Gahlawat 2024; publication date Jul 2024; https://doi.org/10.1007/s10439-024-03541-w) (gahlawat2024tissueengineered3d pages 1-3). - A ClinicalTrials.gov protocol (NCT04051242; 2020 posting) required both: structural deficit ≥20% of muscle-group mass and functional deficit ≥25% versus contralateral limb (NCT04051242 chunk 2).
1.2 Synonyms / alternative names
The dominant term in the retrieved literature is “volumetric muscle loss” / “VML.” Many sources also frame it as critical-sized skeletal muscle defect or critical VML versus subcritical defects that can regenerate (e.g., size-threshold models) (hymel2023identifyingdysregulatedimmune pages 1-2, chowdary2023macrophagemediatedpdgfactivation pages 1-3).
1.3 Data provenance
Most mechanistic knowledge is derived from aggregated preclinical models (murine/rat VML defects with defined sizes) and integrated -omics studies, with limited but important human cohort evidence for certain scaffold-based approaches (greising2019therapeuticapproachesfor pages 1-3, larouche2023spatiotemporalmappingof pages 1-3, dziki2016anacellularbiologic pages 1-2).
2. Etiology
2.1 Disease causal factors (primary causes)
VML arises from severe trauma (e.g., blast or crush injury) and/or surgical removal of skeletal muscle (e.g., resection after injury or oncologic surgery), producing large, abrupt loss of muscle tissue and architectural cues (gahlawat2024tissueengineered3d pages 1-3, grogan2011volumetricmuscleloss pages 1-3, greising2019therapeuticapproachesfor pages 3-5).
2.2 Risk factors
The key “risk factor” for VML is exposure to injury mechanisms that create large muscle voids (e.g., combat blast trauma, high-energy extremity injuries, complex open fractures with soft-tissue loss) (gahlawat2024tissueengineered3d pages 1-3, grogan2011volumetricmuscleloss pages 1-3).
- Military context: VML is described as disproportionately common among military personnel and estimated to comprise ~50% of combat-related injuries in one 2024 review synthesis (Gahlawat 2024; Jul 2024; https://doi.org/10.1007/s10439-024-03541-w) (gahlawat2024tissueengineered3d pages 1-3).
- Explosion-related extremity wounds: In OEF/OIF, extremity wounds were the majority of injuries, and “more than 75%” were due to explosions (Grogan & Hsu 2011; Feb 2011; https://doi.org/10.5435/00124635-201102001-00007) (grogan2011volumetricmuscleloss pages 1-3).
2.3 Protective factors / gene–environment interactions
No protective genetic variants or gene–environment interactions were identified in the retrieved VML-focused sources for this run. This aligns with VML being primarily a trauma phenotype rather than an inherited disease entity.
3. Phenotypes
3.1 Core phenotypes (symptoms/signs)
Commonly reported clinical and biological manifestations include: - Persistent muscle weakness / reduced force generation, chronic functional deficit (greising2019therapeuticapproachesfor pages 3-5, gahlawat2024tissueengineered3d pages 1-3). - Structural muscle void with replacement by fibrotic tissue / scar, impaired range of motion and task performance (dziki2016anacellularbiologic pages 1-2, larouche2023spatiotemporalmappingof pages 1-3). - Chronic inflammation and fibrosis, with regenerative failure (greising2019therapeuticapproachesfor pages 3-5, hymel2023identifyingdysregulatedimmune pages 1-2, larouche2023spatiotemporalmappingof pages 1-3).
3.2 Severity, progression, frequency
- Onset pattern: Typically acute at injury/surgery.
- Course: Often chronic deficits due to incomplete restoration of contractile tissue and persistent fibrosis (greising2019therapeuticapproachesfor pages 3-5, larouche2023spatiotemporalmappingof pages 1-3).
- Severity thresholding: Animal and translational literature uses size/percent-loss thresholds (e.g., >~10%, >20%, or millimeter-scale defects) to define subcritical vs critical, nonhealing VML (patel2019alignednanofibersof pages 1-5, gahlawat2024tissueengineered3d pages 1-3, chowdary2023macrophagemediatedpdgfactivation pages 1-3).
3.3 Quality of life impact
VML is framed as causing long-term disability and loss of function, with significant impact in civilian and military trauma populations (patel2019alignednanofibersof pages 1-5, grogan2011volumetricmuscleloss pages 1-3).
3.4 Suggested HPO terms (examples)
(Recommendations based on phenotype descriptions in retrieved sources) - Muscle weakness: HP:0001324 - Abnormal muscle morphology (muscle tissue loss/atrophy): HP:0003202 (Muscular atrophy) - Decreased joint range of motion: HP:0001376 - Fibrosis (muscle): may map to broader fibrosis phenotypes such as HP:0002206 (Pulmonary fibrosis is organ-specific; HPO fibrosis terms vary by tissue—use tissue-specific fibrosis term if available).
4. Genetic / Molecular Information
4.1 Causal genes / variants
VML is not primarily a Mendelian genetic disease; no causal genes/variants were identified in the retrieved sources.
4.2 Molecular mediators implicated (not inherited “causal genes”)
Recent mechanistic studies emphasize signaling axes that shape regenerative vs fibrotic outcomes: - TGF-β signaling / TGFBR2: spatial transcriptomics + scRNA-seq indicated a pro-fibrotic program; pharmacologic inhibition of TGFBR2 increased MuSC infiltration into the defect and reduced inflammatory/fibrotic transcripts, improving regeneration (Larouche 2023; Jun 2023; https://doi.org/10.1101/2022.06.03.494707) (larouche2023spatiotemporalmappingof pages 1-3). - PDGF vs TGF-β as regenerative vs fibrotic correlates: single-cell analysis across injury models found enhanced TGF-β signaling in fibrotic conditions and enhanced PDGF signaling in regenerative conditions, with macrophage subtypes (fibrotic-like vs regenerative-like) better predicting outcome than classic M1/M2 polarization (Chowdary 2023; Sep 2023; https://doi.org/10.1097/SLA.0000000000005704) (chowdary2023macrophagemediatedpdgfactivation pages 1-3). - IL-10 signaling / Treg axis: delayed local IL-10 delivery after VML repair improved torque and increased ST2 (Treg receptor) expression at repair site (Huynh 2023; Feb 2023; https://doi.org/10.1038/s41598-023-27981-x) (huynh2023localil10delivery pages 1-2).
5. Environmental Information
VML is primarily driven by external injury mechanisms (blast, crush, complex open fractures, surgical resection). No toxin/radiation/pollution-specific environmental etiologies were identified in the retrieved VML-focused sources.
6. Mechanism / Pathophysiology
6.1 High-level causal chain
Trigger: acute traumatic/surgical excision of skeletal muscle → loss of myofibers, satellite cells, and native ECM scaffolding → altered immune dynamics and impaired structural guidance for regeneration → persistent inflammation and macrophage–mesenchymal progenitor crosstalk → excess collagen deposition/fibrosis and reduced vascular/nerve integration → chronic weakness and functional impairment (greising2019therapeuticapproachesfor pages 3-5, larouche2023spatiotemporalmappingof pages 1-3, hymel2023identifyingdysregulatedimmune pages 1-2).
A 2019 systematic review summarizes key mechanisms for failure of regeneration after VML: loss of resident satellite cells, loss of native extracellular matrix organization cues, and dysregulated/prolonged pro-inflammatory programs promoting fibrous tissue accumulation (greising2019therapeuticapproachesfor pages 3-5).
6.2 Immune dysregulation and fibrosis (2023–2024 advances)
Macrophage–FAP/MDC circuit and spatial restriction - In murine + canine VML, spatial transcriptomics integrated with scRNA-seq showed the defect zone enriched for inflammatory and collagen genes (e.g., Ctss/S100a8/S100a9 and Col1a1/Col1a2), while myogenic developmental genes were localized to a transition zone; MuSCs were largely confined to transition zone rather than infiltrating the defect, consistent with spatially restricted regeneration (larouche2023spatiotemporalmappingof pages 1-3). - A 2023 Communications Biology study found critical VML (3 mm) displayed sustained M2-like and CD206hiLy6Chi hybrid macrophages with aberrant cytokine production that co-localized with fibroadipogenic progenitors (FAPs) in collagen deposition regions; multiple T-cell subpopulations were elevated and the immune response failed to resolve into a pro-regenerative microenvironment within the first week (hymel2023identifyingdysregulatedimmune pages 1-2).
Defect-size thresholds and immune programs - Cross-study scRNA-seq analysis across musculoskeletal injuries identified that smaller VML defects regenerate while larger defects fibrose (size thresholds reported as <2 mm regenerative vs >3 mm fibrotic in that analysis framework) (chowdary2023macrophagemediatedpdgfactivation pages 1-3).
Lipid mediator imbalance and pro-resolving therapeutics - A 2023 eLife study profiled lipid mediators and found degenerative VML showed increased pro-inflammatory eicosanoids (e.g., LTB4, PGE2, PGF2α) with insufficient increases in pro-resolving mediators; replenishing Maresin 1 reduced neutrophils/macrophages, attenuated fibrosis, increased MuSC activation, and improved force recovery (Castor-Macias 2023; Dec 2023; https://doi.org/10.7554/eLife.86437) (castormacias2023maresin1repletion pages 9-11, castormacias2023maresin1repletion pages 2-5).
Immunotherapy: IL-10 - In a rat VML model repaired with minced muscle, delayed local recombinant IL-10 dosing from 7–14 days post-injury improved contractile outcomes at 56 days (torque 82% of uninjured; 170% of PBS controls) and induced IL-10 signaling and lymphocyte pathway signatures at 14 days (huynh2023localil10delivery pages 1-2).
6.3 Suggested GO biological process terms (examples)
- Muscle tissue regeneration (GO:0055001)
- Skeletal muscle satellite cell activation / myoblast differentiation (e.g., myoblast differentiation GO:0045445)
- Inflammatory response (GO:0006954)
- Macrophage activation (GO:0042116)
- Extracellular matrix organization (GO:0030198)
- Collagen fibril organization / fibrosis-related processes (e.g., collagen fibril organization GO:0030199)
- Transforming growth factor beta receptor signaling pathway (GO:0007179)
- Platelet-derived growth factor receptor signaling pathway (GO:0048008)
6.4 Suggested Cell Ontology (CL) terms (examples)
- Skeletal muscle satellite cell / muscle stem cell (MuSC): skeletal muscle satellite cell (CL term; commonly used)
- Macrophage: macrophage (CL:0000235)
- Neutrophil: neutrophil (CL:0000775)
- T cell / regulatory T cell: T cell (CL:0000084), regulatory T cell (CL:0000815)
- Fibro-adipogenic progenitor / mesenchymal stromal progenitor: map to mesenchymal stromal cell / fibroblast progenitor terms depending on ontology availability
7. Anatomical Structures Affected
7.1 Organ/tissue
Primary tissue: skeletal muscle (e.g., extremity muscle compartments such as quadriceps, tibialis anterior, posterior compartment muscles) (hymel2023identifyingdysregulatedimmune pages 1-2, huynh2023localil10delivery pages 1-2).
7.2 Suggested UBERON terms (examples)
- Skeletal muscle tissue: UBERON:0001134
- Lower limb muscle / hindlimb muscle: appropriate limb-region UBERON terms depending on injury site
8. Temporal Development
8.1 Onset
Typically immediate/acute at the time of trauma or surgery (grogan2011volumetricmuscleloss pages 1-3).
8.2 Progression
- Early inflammatory phase that fails to resolve in critical VML, evolving into chronic fibrosis with persistent functional deficits (hymel2023identifyingdysregulatedimmune pages 1-2, larouche2023spatiotemporalmappingof pages 1-3).
9. Inheritance and Population
9.1 Epidemiology / burden (available quantitative statistics)
Quantitative population incidence/prevalence per 100,000 was not found in the retrieved sources for this run (and may be difficult to quantify due to underreporting and coding/billing limitations) (gahlawat2024tissueengineered3d pages 1-3).
However, burden statistics in authoritative reviews include: - ~50% of combat-related injuries in military populations (review synthesis) (gahlawat2024tissueengineered3d pages 1-3). - In OEF/OIF, extremity wounds were the majority of soldier injuries and >75% were due to explosions (grogan2011volumetricmuscleloss pages 1-3). - Type-III open tibia fractures (with severe bone and soft tissue injury context) were associated with a reported 65% incidence of permanent disability/medical retirement (gahlawat2024tissueengineered3d pages 1-3).
9.2 Genetics / inheritance
Not applicable as a primary disease mechanism.
10. Diagnostics
10.1 Clinical assessment and outcome measures
There is no standardized protocol for characterizing/quantifying VML; recommended clinical documentation includes photographs/video, range-of-motion measurements, manual muscle strength testing, and isokinetic muscle function testing (Grogan & Hsu 2011; Feb 2011; https://doi.org/10.5435/00124635-201102001-00007) (grogan2011volumetricmuscleloss pages 1-3).
10.2 Imaging and tissue assessment (human cohort/trials)
In the 13-patient cohort using ECM scaffolds, imaging (CT/MRI pre-op and ~7 months post-op) assessed volumetric loss and fatty infiltration; ultrasound-guided biopsies were sampled at ~6 and 26 weeks; electrodiagnostics were performed in 8/13 subjects (Dziki 2016; Jul 2016; https://doi.org/10.1038/npjregenmed.2016.8) (dziki2016anacellularbiologic pages 10-10).
10.3 Trial-based operational diagnostic thresholds
NCT04051242 used: structural deficit ≥20% muscle-group mass and functional deficit ≥25% vs contralateral limb (ClinicalTrials.gov; 2020; https://clinicaltrials.gov/study/NCT04051242) (NCT04051242 chunk 2).
11. Outcome / Prognosis
11.1 Functional prognosis
VML is associated with persistent functional deficits because ablated myofibers do not regenerate and fibrosis replaces contractile tissue in critical injuries (greising2019therapeuticapproachesfor pages 3-5, larouche2023spatiotemporalmappingof pages 1-3). Functional deficits may exceed those predicted by mass loss alone (gahlawat2024tissueengineered3d pages 1-3).
11.2 Human outcome data (ECM scaffold cohort)
Dziki et al. reported that by 6 months after ECM implantation with aggressive physical therapy, patients showed average improvements vs pre-operative performance of 37.3% in strength and 27.1% in range-of-motion tasks (both P<0.05) (Dziki 2016; Jul 2016; https://doi.org/10.1038/npjregenmed.2016.8; NCT01292876) (dziki2016anacellularbiologic pages 1-2).
11.3 Evidence caveats
A 2019 systematic review noted limited human evidence and reported case reports with minimal net strength deficit improvement after acellular biomaterial repair in two service members (72%→~68% deficit at 4 months; 89%→~87% deficit at ~6 months), emphasizing that some “functional gains” may not reflect true muscle regeneration (greising2019therapeuticapproachesfor pages 14-16).
12. Treatment
12.1 Current applications / real-world implementations (standard of care)
Clinical management frequently includes: - Soft-tissue reconstruction (clinical gold standard): functional free muscle transfer and/or fasciocutaneous flaps, with limitations including donor-site morbidity and incomplete functional restoration (gahlawat2024tissueengineered3d pages 1-3). - Orthotics/bracing (including advanced bracing designs; carbon fiber-based braces described in 2024 review) and physical therapy as supportive care, though not correcting underlying strength deficits in many cases (grogan2011volumetricmuscleloss pages 1-3, gahlawat2024tissueengineered3d pages 1-3).
12.2 Regenerative medicine / advanced therapeutics (current state)
Acellular ECM bioscaffolds (human evidence) - Dziki et al. (2016) described a 13-patient cohort receiving ECM bioscaffolds plus aggressive early physical therapy with improved strength and ROM at 6 months and evidence of vascularized/innervated islands of skeletal muscle (dziki2016anacellularbiologic pages 1-2).
Clinical trials - NCT01292876: registered for the 13-patient ECM cohort described by Dziki et al. (2016) (dziki2016anacellularbiologic pages 1-2). - NCT04051242: “Enhanced Bioscaffold for Volumetric Muscle Loss” testing XENMATRIX AB™; includes explicit structural/functional inclusion criteria; status terminated; record notes two participants received the graft (ClinicalTrials.gov; 2020; https://clinicaltrials.gov/study/NCT04051242) (NCT04051242 chunk 2).
Immunomodulatory / immuno-regenerative strategies (preclinical, 2023) - IL-10 therapy improved contractile torque to 82% of uninjured values (and 170% of PBS controls) in a rat VML model (Huynh 2023; Feb 2023; https://doi.org/10.1038/s41598-023-27981-x) (huynh2023localil10delivery pages 1-2). - Maresin 1 (DHA-derived pro-resolving mediator) reduced fibrosis and improved strength after degenerative VML in mice (Castor-Macias 2023; Dec 2023; https://doi.org/10.7554/eLife.86437) (castormacias2023maresin1repletion pages 9-11). - Anti-fibrotic pathway targeting: inhibition of TGFBR2 increased MuSC infiltration and reduced inflammatory/fibrotic signatures (Larouche 2023; Jun 2023; https://doi.org/10.1101/2022.06.03.494707) (larouche2023spatiotemporalmappingof pages 1-3).
Expert synthesis / meta-analysis (animal evidence) A systematic review/meta-analysis found that in animal models, treatments improved functional capacity versus untreated controls with pooled effect size Hedges’ g = 0.75 (95% CI 0.53–0.96; p<1e-7), but authors emphasized the ~16% average beneficial effect was small and current paradigms require maturation; network meta-analysis suggested acellular biomaterial + stem/progenitor cells as the most effective tested class (Greising 2019; Dec 2019; https://doi.org/10.1089/ten.teb.2019.0207) (greising2019therapeuticapproachesfor pages 1-3).
12.3 MAXO term suggestions (examples)
- Surgical tissue transfer / reconstruction (e.g., free functional muscle transfer): MAXO:0000004 (surgical procedure; use more specific MAXO if available)
- Physical therapy / rehabilitation: MAXO term for rehabilitation therapy (ontology-dependent)
- Orthotic device use/bracing: MAXO term for orthotic intervention
- Implantation of biological scaffold / biomaterial implant: MAXO term for implantation of medical device/biomaterial
- Cytokine therapy (IL-10): MAXO term for cytokine therapy
13. Prevention
Primary prevention is mainly trauma prevention (combat injury mitigation, occupational/vehicular safety). No specific biomedical prophylaxis is established in the retrieved VML-focused sources.
14. Other Species / Natural Disease
Not applicable as a naturally occurring transmissible disease; however, mechanistic and translational studies include canine VML models in addition to murine models, indicating cross-species conservation of immune–progenitor crosstalk with kinetic differences (larouche2023spatiotemporalmappingof pages 1-3).
15. Model Organisms
Commonly used experimental systems include: - Mouse models with standardized defect sizes (e.g., subcritical vs critical millimeter-scale injuries) enabling immune/omics comparisons (hymel2023identifyingdysregulatedimmune pages 1-2, chowdary2023macrophagemediatedpdgfactivation pages 1-3). - Rat tibialis anterior VML models used for minced muscle repair and cytokine delivery studies (huynh2023localil10delivery pages 1-2). - Canine models used in spatial transcriptomic analyses alongside mouse, supporting translational relevance (larouche2023spatiotemporalmappingof pages 1-3).
Key Quantitative Evidence Map (summary table)
The following table consolidates major quantitative thresholds, burden statistics, human clinical outcomes, and key mechanistic findings across the retrieved literature.
Table (click to expand)
| Topic | Key data/claim | Evidence type (human/animal/in vitro/trial protocol) | Source (first author, year) | PMID if known | URL | Citation context ID |
|---|---|---|---|---|---|---|
| Definition | VML is the traumatic or surgical loss of skeletal muscle resulting in functional impairment. | Human/clinical review | Grogan, 2011 | https://doi.org/10.5435/00124635-201102001-00007 | (grogan2011volumetricmuscleloss pages 1-3) | |
| Quantitative threshold | Loss of skeletal muscle exceeding 20% is cited as a threshold beyond which innate repair/regeneration is permanently compromised. | Review/synthesized clinical-preclinical | Gahlawat, 2024 | https://doi.org/10.1007/s10439-024-03541-w | (gahlawat2024tissueengineered3d pages 1-3) | |
| Alternative threshold | VML has also been described as loss of over ~10% of muscle mass causing functional impairment. | In vitro/review context | Patel, 2019 | https://doi.org/10.1088/1748-605x/ab0b06 | (patel2019alignednanofibersof pages 1-5) | |
| Trial enrollment definition | Human VML trial protocol required both a structural deficit ≥20% of the muscle group mass and a functional deficit ≥25% versus the contralateral limb. | Trial protocol | Rubin/NCT04051242, 2020 | https://clinicaltrials.gov/study/NCT04051242 | (NCT04051242 chunk 2) | |
| Epidemiology/burden | VML is disproportionately common in military populations, comprising ~50% of combat-related injuries. | Review | Gahlawat, 2024 | https://doi.org/10.1007/s10439-024-03541-w | (gahlawat2024tissueengineered3d pages 1-3) | |
| Extremity trauma burden | Extremity wounds are the majority of soldier injuries in OEF/OIF, and >75% are due to explosions. | Human clinical review | Grogan, 2011 | https://doi.org/10.5435/00124635-201102001-00007 | (grogan2011volumetricmuscleloss pages 1-3) | |
| Disability burden | Severe extremity injuries such as type-III open tibia fractures with major soft-tissue loss are associated with a 65% incidence of permanent disability/medical retirement. | Review | Gahlawat, 2024 | https://doi.org/10.1007/s10439-024-03541-w | (gahlawat2024tissueengineered3d pages 1-3) | |
| Human cohort outcomes | In a 13-patient ECM bioscaffold cohort, mean improvement at 6 months was 37.3% in strength and 27.1% in range-of-motion versus pre-op. | Human cohort | Dziki, 2016 | https://doi.org/10.1038/npjregenmed.2016.8 | (dziki2016anacellularbiologic pages 1-2) | |
| Human cohort baseline severity | In the same 13-patient cohort, mean estimated tissue deficit was ~66.2% (individual deficits ~25% to 90%). | Human cohort | Dziki, 2016 | https://doi.org/10.1038/npjregenmed.2016.8 | (dziki2016anacellularbiologic pages 1-2) | |
| Human evidence caveat | Case reports of quadriceps acellular biomaterial repair showed minimal net recovery: 72%→~68% deficit at 4 months in one patient and 89%→~87% deficit at ~6 months in another. | Human case reports/review | Greising, 2019 | https://doi.org/10.1089/ten.teb.2019.0207 | (greising2019therapeuticapproachesfor pages 14-16) | |
| Meta-analysis efficacy | Across 44 animal studies, pooled functional benefit of VML treatments was Hedges’ g 0.75 (95% CI 0.53–0.96; p<0.0000001), corresponding to ~16% average beneficial effect. | Animal systematic review/meta-analysis | Greising, 2019 | https://doi.org/10.1089/ten.teb.2019.0207 | (greising2019therapeuticapproachesfor pages 1-3) | |
| Best-performing treatment class | Network meta-analysis suggested acellular biomaterial combined with stem/progenitor cells was the most effective experimental strategy. | Animal systematic review/meta-analysis | Greising, 2019 | https://doi.org/10.1089/ten.teb.2019.0207 | (greising2019therapeuticapproachesfor pages 1-3) | |
| Critical vs subcritical injury | In murine quadriceps, 2 mm defects regenerated while 3 mm defects produced persistent fibrotic scarring and chronic inflammation through 4 weeks. | Animal primary study | Hymel, 2023 | https://doi.org/10.1038/s42003-023-04790-6 | (hymel2023identifyingdysregulatedimmune pages 1-2) | |
| Mechanism: immune dysregulation | Critical VML showed sustained M2-like and CD206hiLy6Chi hybrid macrophages co-localized with FAPs in collagen-rich regions, implicating macrophage–FAP crosstalk in fibrosis. | Animal primary study | Hymel, 2023 | https://doi.org/10.1038/s42003-023-04790-6 | (hymel2023identifyingdysregulatedimmune pages 1-2) | |
| Mechanism: spatial fibrosis program | Spatial transcriptomics/scRNA-seq showed macrophages concentrated in the defect zone, MDCs/FAPs in defect/transition zones, and MuSCs largely restricted to transition zones; TGFBR2 inhibition improved MuSC infiltration and reduced fibrosis. | Animal primary study/omics | Larouche, 2023 | https://doi.org/10.1101/2022.06.03.494707 | (larouche2023spatiotemporalmappingof pages 1-3) | |
| Mechanism: lipid mediators | Degenerative VML showed increased pro-inflammatory eicosanoids (e.g., LTB4, PGE2, PGF2α) with insufficient rise in pro-resolving mediators (e.g., MaR1, PD1, RvD6). | Animal primary study/metabolipidomics | Castor-Macias, 2023 | https://doi.org/10.7554/elife.86437 | (castormacias2023maresin1repletion pages 9-11, castormacias2023maresin1repletion pages 2-5) | |
| Immunotherapy result | Delayed local IL-10 delivery after minced-muscle repair improved contractile torque to 82% of uninjured values and 170% of PBS controls at 56 days. | Animal primary study | Huynh, 2023 | https://doi.org/10.1038/s41598-023-27981-x | (huynh2023localil10delivery pages 1-2) | |
| Pro-resolving mediator result | Maresin 1 repletion reduced neutrophils/macrophages, attenuated fibrosis, increased MuSC activation, and partially restored force after degenerative VML. | Animal primary study | Castor-Macias, 2023 | https://doi.org/10.7554/elife.86437 | (castormacias2023maresin1repletion pages 9-11, castormacias2023maresin1repletion pages 1-2) | |
| Standard of care | Current clinical management includes physical therapy/orthotics and soft-tissue reconstruction such as functional free muscle transfer; these approaches have donor-site morbidity and limited restoration of function. | Human clinical review | Grogan, 2011 | https://doi.org/10.5435/00124635-201102001-00007 | (grogan2011volumetricmuscleloss pages 1-3) |
Table: This table summarizes the most actionable quantitative definitions, burden statistics, human clinical results, and recent mechanistic findings for volumetric muscle loss. It is useful as a compact evidence map spanning disease characterization, translational thresholds, and therapeutic implications.
Visual Evidence (figures/tables)
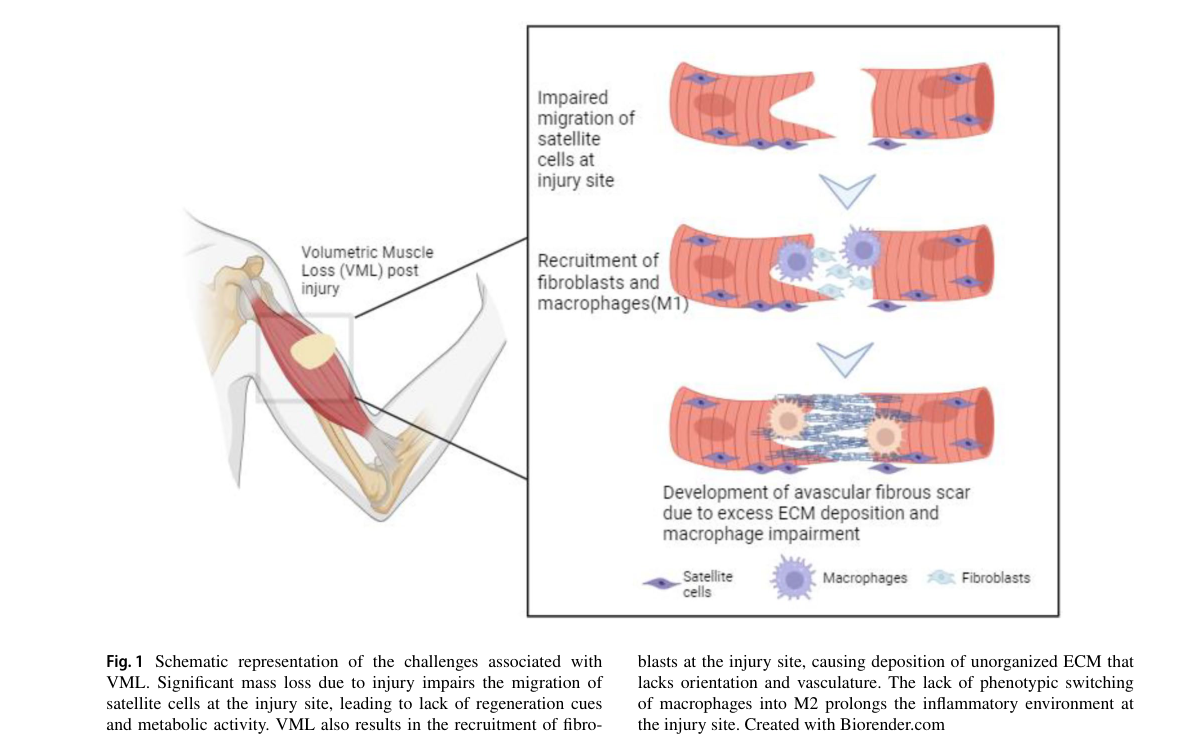
A 2024 review provides schematic summaries of (i) VML pathophysiology (immune infiltration → impaired satellite cell migration → avascular fibrous scar) and (ii) tissue engineering strategies (in situ / in vivo / in vitro TE), plus tables of biomaterials and growth factors used in TE constructs (gahlawat2024tissueengineered3d media 816f8097, gahlawat2024tissueengineered3d media 4d3d8f7b, gahlawat2024tissueengineered3d media a8bea718, gahlawat2024tissueengineered3d media 26d381a5).
Notes on evidence limitations for knowledge-base population
- Robust registry-style epidemiology (incidence/prevalence per 100,000) and standardized ICD/MeSH/MONDO identifiers were not available in retrieved sources using the tools in this run; the report therefore emphasizes well-supported operational definitions, burden statistics in military trauma, and translational thresholds used in trials and preclinical modeling.
References
-
(grogan2011volumetricmuscleloss pages 1-3): Brian F. Grogan and Joseph R. Hsu. Volumetric muscle loss. American Academy of Orthopaedic Surgeon, 19:S35–S37, Feb 2011. URL: https://doi.org/10.5435/00124635-201102001-00007, doi:10.5435/00124635-201102001-00007. This article has 475 citations.
-
(greising2019therapeuticapproachesfor pages 6-8): Sarah M. Greising, Benjamin T. Corona, Christopher McGann, Jeremy K. Frankum, and Gordon L. Warren. Therapeutic approaches for volumetric muscle loss injury: a systematic review and meta-analysis. Tissue engineering. Part B, Reviews, 25:510-525, Dec 2019. URL: https://doi.org/10.1089/ten.teb.2019.0207, doi:10.1089/ten.teb.2019.0207. This article has 130 citations.
-
(greising2019therapeuticapproachesfor pages 3-5): Sarah M. Greising, Benjamin T. Corona, Christopher McGann, Jeremy K. Frankum, and Gordon L. Warren. Therapeutic approaches for volumetric muscle loss injury: a systematic review and meta-analysis. Tissue engineering. Part B, Reviews, 25:510-525, Dec 2019. URL: https://doi.org/10.1089/ten.teb.2019.0207, doi:10.1089/ten.teb.2019.0207. This article has 130 citations.
-
(gahlawat2024tissueengineered3d pages 1-3): Sonal Gahlawat, Doga Oruc, Nikhil Paul, Mark Ragheb, Swati Patel, Oyinkansola Fasasi, Peeyush Sharma, David I. Shreiber, and Joseph W. Freeman. Tissue engineered 3d constructs for volumetric muscle loss. Annals of Biomedical Engineering, 52:2325-2347, Jul 2024. URL: https://doi.org/10.1007/s10439-024-03541-w, doi:10.1007/s10439-024-03541-w. This article has 30 citations and is from a domain leading peer-reviewed journal.
-
(patel2019alignednanofibersof pages 1-5): Krishna H Patel, Andrew J Dunn, Muhamed Talovic, Gabriel J Haas, Madison Marcinczyk, Hady Elmashhady, Emily Growney Kalaf, Scott A Sell, and Koyal Garg. Aligned nanofibers of decellularized muscle ecm support myogenic activity in primary satellite cells in vitro. Biomedical Materials, 14:035010, Apr 2019. URL: https://doi.org/10.1088/1748-605x/ab0b06, doi:10.1088/1748-605x/ab0b06. This article has 88 citations and is from a peer-reviewed journal.
-
(NCT04051242 chunk 2): J. Peter Rubin, MD. Enhanced Bioscaffold for Volumetric Muscle Loss. J. Peter Rubin, MD. 2020. ClinicalTrials.gov Identifier: NCT04051242
-
(hymel2023identifyingdysregulatedimmune pages 1-2): Lauren A. Hymel, Shannon E. Anderson, Thomas C. Turner, William Y. York, Hongmanlin Zhang, Adrian R. Liversage, Hong Seo Lim, Peng Qiu, Luke J. Mortensen, Young C. Jang, Nick J. Willett, and Edward A. Botchwey. Identifying dysregulated immune cell subsets following volumetric muscle loss with pseudo-time trajectories. Communications Biology, Jul 2023. URL: https://doi.org/10.1038/s42003-023-04790-6, doi:10.1038/s42003-023-04790-6. This article has 20 citations and is from a peer-reviewed journal.
-
(chowdary2023macrophagemediatedpdgfactivation pages 1-3): Ashish R. Chowdary, Tristan Maerz, Dominic Henn, Kurt D. Hankenson, Chase A. Pagani, Simone Marini, Katherine Gallagher, Carlos A. Aguilar, Robert J. Tower, and Benjamin Levi. Macrophage-mediated pdgf activation correlates with regenerative outcomes following musculoskeletal trauma. Annals of Surgery, 278:e349-e359, Sep 2023. URL: https://doi.org/10.1097/sla.0000000000005704, doi:10.1097/sla.0000000000005704. This article has 17 citations and is from a highest quality peer-reviewed journal.
-
(greising2019therapeuticapproachesfor pages 1-3): Sarah M. Greising, Benjamin T. Corona, Christopher McGann, Jeremy K. Frankum, and Gordon L. Warren. Therapeutic approaches for volumetric muscle loss injury: a systematic review and meta-analysis. Tissue engineering. Part B, Reviews, 25:510-525, Dec 2019. URL: https://doi.org/10.1089/ten.teb.2019.0207, doi:10.1089/ten.teb.2019.0207. This article has 130 citations.
-
(larouche2023spatiotemporalmappingof pages 1-3): Jacqueline A. Larouche, Emily C. Wallace, Bonnie D. Spence, Scott A. Johnson, Mangesh Kulkarni, Eric Buras, Bryan N. Brown, Stephen F. Badylak, and Carlos A. Aguilar. Spatiotemporal mapping of immune and stem cell dysregulation after volumetric muscle loss. JCI Insight, Jun 2023. URL: https://doi.org/10.1101/2022.06.03.494707, doi:10.1101/2022.06.03.494707. This article has 53 citations and is from a domain leading peer-reviewed journal.
-
(dziki2016anacellularbiologic pages 1-2): Jenna Dziki, Stephen Badylak, Mohammad Yabroudi, Brian Sicari, Fabrisia Ambrosio, Kristen Stearns, Neill Turner, Aaron Wyse, Michael L Boninger, Elke H P Brown, and J Peter Rubin. An acellular biologic scaffold treatment for volumetric muscle loss: results of a 13-patient cohort study. NPJ Regenerative Medicine, Jul 2016. URL: https://doi.org/10.1038/npjregenmed.2016.8, doi:10.1038/npjregenmed.2016.8. This article has 248 citations and is from a peer-reviewed journal.
-
(huynh2023localil10delivery pages 1-2): tai huynh, Cassandra Reed, Zain Blackwell, Payton Phelps, Luis C. Pinzon Herrera, Jorge Almodovar, David A. Zaharoff, and Jeffrey C Wolchok. Local il-10 delivery modulates the immune response and enhances repair of volumetric muscle loss muscle injury. Scientific Reports, Feb 2023. URL: https://doi.org/10.1038/s41598-023-27981-x, doi:10.1038/s41598-023-27981-x. This article has 43 citations and is from a peer-reviewed journal.
-
(castormacias2023maresin1repletion pages 9-11): Jesus A Castor-Macias, Jacqueline A Larouche, Emily C Wallace, Bonnie D Spence, Alec Eames, Pamela Duran, Benjamin A Yang, Paula M Fraczek, Carol A Davis, Susan V Brooks, Krishna Rao Maddipati, James F Markworth, and Carlos A Aguilar. Maresin 1 repletion improves muscle regeneration after volumetric muscle loss. eLife, Dec 2023. URL: https://doi.org/10.7554/elife.86437, doi:10.7554/elife.86437. This article has 22 citations and is from a domain leading peer-reviewed journal.
-
(castormacias2023maresin1repletion pages 2-5): Jesus A Castor-Macias, Jacqueline A Larouche, Emily C Wallace, Bonnie D Spence, Alec Eames, Pamela Duran, Benjamin A Yang, Paula M Fraczek, Carol A Davis, Susan V Brooks, Krishna Rao Maddipati, James F Markworth, and Carlos A Aguilar. Maresin 1 repletion improves muscle regeneration after volumetric muscle loss. eLife, Dec 2023. URL: https://doi.org/10.7554/elife.86437, doi:10.7554/elife.86437. This article has 22 citations and is from a domain leading peer-reviewed journal.
-
(dziki2016anacellularbiologic pages 10-10): Jenna Dziki, Stephen Badylak, Mohammad Yabroudi, Brian Sicari, Fabrisia Ambrosio, Kristen Stearns, Neill Turner, Aaron Wyse, Michael L Boninger, Elke H P Brown, and J Peter Rubin. An acellular biologic scaffold treatment for volumetric muscle loss: results of a 13-patient cohort study. NPJ Regenerative Medicine, Jul 2016. URL: https://doi.org/10.1038/npjregenmed.2016.8, doi:10.1038/npjregenmed.2016.8. This article has 248 citations and is from a peer-reviewed journal.
-
(greising2019therapeuticapproachesfor pages 14-16): Sarah M. Greising, Benjamin T. Corona, Christopher McGann, Jeremy K. Frankum, and Gordon L. Warren. Therapeutic approaches for volumetric muscle loss injury: a systematic review and meta-analysis. Tissue engineering. Part B, Reviews, 25:510-525, Dec 2019. URL: https://doi.org/10.1089/ten.teb.2019.0207, doi:10.1089/ten.teb.2019.0207. This article has 130 citations.
-
(castormacias2023maresin1repletion pages 1-2): Jesus A Castor-Macias, Jacqueline A Larouche, Emily C Wallace, Bonnie D Spence, Alec Eames, Pamela Duran, Benjamin A Yang, Paula M Fraczek, Carol A Davis, Susan V Brooks, Krishna Rao Maddipati, James F Markworth, and Carlos A Aguilar. Maresin 1 repletion improves muscle regeneration after volumetric muscle loss. eLife, Dec 2023. URL: https://doi.org/10.7554/elife.86437, doi:10.7554/elife.86437. This article has 22 citations and is from a domain leading peer-reviewed journal.
-
(gahlawat2024tissueengineered3d media 816f8097): Sonal Gahlawat, Doga Oruc, Nikhil Paul, Mark Ragheb, Swati Patel, Oyinkansola Fasasi, Peeyush Sharma, David I. Shreiber, and Joseph W. Freeman. Tissue engineered 3d constructs for volumetric muscle loss. Annals of Biomedical Engineering, 52:2325-2347, Jul 2024. URL: https://doi.org/10.1007/s10439-024-03541-w, doi:10.1007/s10439-024-03541-w. This article has 30 citations and is from a domain leading peer-reviewed journal.
-
(gahlawat2024tissueengineered3d media 4d3d8f7b): Sonal Gahlawat, Doga Oruc, Nikhil Paul, Mark Ragheb, Swati Patel, Oyinkansola Fasasi, Peeyush Sharma, David I. Shreiber, and Joseph W. Freeman. Tissue engineered 3d constructs for volumetric muscle loss. Annals of Biomedical Engineering, 52:2325-2347, Jul 2024. URL: https://doi.org/10.1007/s10439-024-03541-w, doi:10.1007/s10439-024-03541-w. This article has 30 citations and is from a domain leading peer-reviewed journal.
-
(gahlawat2024tissueengineered3d media a8bea718): Sonal Gahlawat, Doga Oruc, Nikhil Paul, Mark Ragheb, Swati Patel, Oyinkansola Fasasi, Peeyush Sharma, David I. Shreiber, and Joseph W. Freeman. Tissue engineered 3d constructs for volumetric muscle loss. Annals of Biomedical Engineering, 52:2325-2347, Jul 2024. URL: https://doi.org/10.1007/s10439-024-03541-w, doi:10.1007/s10439-024-03541-w. This article has 30 citations and is from a domain leading peer-reviewed journal.
-
(gahlawat2024tissueengineered3d media 26d381a5): Sonal Gahlawat, Doga Oruc, Nikhil Paul, Mark Ragheb, Swati Patel, Oyinkansola Fasasi, Peeyush Sharma, David I. Shreiber, and Joseph W. Freeman. Tissue engineered 3d constructs for volumetric muscle loss. Annals of Biomedical Engineering, 52:2325-2347, Jul 2024. URL: https://doi.org/10.1007/s10439-024-03541-w, doi:10.1007/s10439-024-03541-w. This article has 30 citations and is from a domain leading peer-reviewed journal.