1. Disease Information
1.1 Overview / definition (current understanding)
Testicular sex cord–stromal tumors (SCSTs) are a rare category of primary non-germ cell testicular neoplasms derived from sex cord elements and/or gonadal stromal elements. They are typically indolent with a tendency toward benign behavior but can metastasize, and metastatic cases often have poor response to chemotherapy. (colecchia2023newsinthe pages 2-4, kowalik2024sexcordstromaltumors pages 1-2)
A 2024 literature review summarizes this group as including androblastoma (Leydig cell tumor and Sertoli cell tumor), fibroma–thecoma group tumors, stromal tumors, and sex cord tumors (with WHO/EAU-based classification tables). (kowalik2024sexcordstromaltumors pages 1-2)
1.2 Key identifiers (ICD-10/ICD-11, MeSH, Orphanet, MONDO)
- WHO/IARC classification anchor: WHO Classification of Tumours of the Urinary System and Male Genital Tumours, 5th edition (published June 2022) is explicitly referenced as the current standard classification source. (colecchia2023newsinthe pages 1-2, colecchia2023newsinthe pages 4-5)
- ICD / MeSH / Orphanet / MONDO identifiers: Not retrievable from the current evidence set/tools invoked in this run (evidence gap).
1.3 Synonyms / alternative names
Commonly used names and umbrella terms in the retrieved sources include: - “Sex cord-stromal tumors of the testis” (review title/term) (kowalik2024sexcordstromaltumors pages 1-2) - “Sex-cord stromal tumours (SCSTs)” (WHO classification update article) (colecchia2023newsinthe pages 1-2) - “Gonadal stromal tumors” (used alongside SCSTs in review abstract) (kowalik2024sexcordstromaltumors pages 1-2) - Historical/variant terminology and reclassifications noted in WHO updates: - “Signet ring stromal tumour” (new entity) (colecchia2023newsinthe pages 1-2) - “Myoid gonadal stromal tumour” (new entity) (colecchia2023newsinthe pages 1-2) - “Sertoliform cystadenoma” moved into Sertoli cell tumors (WHO change) (colecchia2023newsinthe pages 1-2) - Mixed vs SCST-NOS definitions (WHO change): mixed SCSTs vs “SCST NOS reserved for SCSTs made up of undifferentiated/immature sex cord stromal cells” (colecchia2023newsinthe pages 2-4)
1.4 Source type (individual vs aggregated)
Evidence in this report comes from: - Aggregated disease-level resources/reviews (WHO classification summary; literature reviews) (colecchia2023newsinthe pages 1-2, kowalik2024sexcordstromaltumors pages 1-2) - Registry/real-world aggregated cohorts (National Cancer Database analysis) (zuniga2020acomparisonof pages 2-3, zuniga2020acomparisonof pages 3-5) - Individual patient reports (testicular adult granulosa cell tumor case with NGS) (deng2023adultgranulosacell pages 1-2) - Model organism studies (mouse Sertoli-cell TGFBR1 activation model) (fang2023sertolicellspecificactivation pages 1-2)
2. Etiology
2.1 Disease causal factors (mechanistic/genetic)
Most SCSTs are sporadic, but multiple lines of evidence implicate genetic drivers/syndromic associations and pathway dysregulation.
Key molecular/driver associations supported by retrieved evidence: - CTNNB1 / β-catenin (Sertoli-pattern tumors): A WHO classification update summarizes that a “large percentage” of Sertoli cell tumors show CTNNB1 mutation with diagnostic nuclear β-catenin staining. (colecchia2023newsinthe pages 1-2) - FOXL2 and granulosa cell tumors: A 2024 review notes adult-type granulosa cell tumor is associated “with a FOXL2 gene mutation.” (kowalik2024sexcordstromaltumors pages 2-3) - TGFβ pathway activation as a mechanistic driver in a mouse model: Sertoli-cell-specific activation of TGFBR1 leads to testicular granulosa-cell-tumor-like neoplasms and Sertoli-to-granulosa transdifferentiation (mechanistic evidence, model organism). (fang2023sertolicellspecificactivation pages 1-2)
Direct abstract quote (model organism mechanistic statement): - “Sertoli cell-specific activation of TGFBR1 led to the development of neoplasms resembling granulosa cell tumors…” (fang2023sertolicellspecificactivation pages 1-2)
2.2 Risk factors
- Precocious puberty (epidemiologic association): The 2024 review states: “boys with precocious puberty have an increased risk of developing sex cord-stromal tumors.” (kowalik2024sexcordstromaltumors pages 1-2)
- Syndromic predisposition: Large cell calcifying Sertoli cell tumor is described as associated with Carney complex and Peutz–Jeghers syndrome, and the WHO update notes the intratubular large cell hyalinising Sertoli cell neoplasia is only described in Peutz–Jeghers syndrome (syndromic context). (kowalik2024sexcordstromaltumors pages 2-3, colecchia2023newsinthe pages 2-4)
- Cryptorchidism: Unlike germ cell tumors, the review notes there is “no substantial correlation observed with undescended testes” for SCSTs overall; however, juvenile granulosa cell tumor is described as more common in children with cryptorchidism or karyotypic abnormalities. (kowalik2024sexcordstromaltumors pages 1-2, kowalik2024sexcordstromaltumors pages 2-3)
2.3 Protective factors
No protective factors were identified in the retrieved evidence set (evidence gap).
2.4 Gene–environment interactions
No specific gene–environment interaction evidence was identified in the retrieved evidence set (evidence gap).
3. Phenotypes
3.1 Core clinical presentation
- Many lesions are asymptomatic and discovered as a painless testicular mass; endocrine manifestations are particularly relevant for hormone-producing subtypes. (kowalik2024sexcordstromaltumors pages 2-3, kowalik2024sexcordstromaltumors pages 3-4)
3.2 Endocrine manifestations (notably Leydig cell tumor)
Leydig cell tumors can produce sex steroids and cause: - Gynecomastia (HP:0000788) - Decreased libido (HP:0000810) - Erectile dysfunction (HP:0100639) - Testicular atrophy (HP:0000029) These symptoms are attributed to production of estradiol/progesterone/testosterone in the review. (kowalik2024sexcordstromaltumors pages 2-3)
Pediatric manifestations include: - Precocious puberty (HP:0000826) (kowalik2024sexcordstromaltumors pages 2-3)
3.3 Granulosa cell tumor phenotypes
- Adult-type testicular granulosa cell tumors: the review reports gynecomastia in 50% of cases, and describes characteristic “coffee bean nuclei” histology. (kowalik2024sexcordstromaltumors pages 3-4)
- Juvenile granulosa cell tumors: usually occur in infants up to 6 months, often present as painless mass; AFP within normal range; benign behavior. (kowalik2024sexcordstromaltumors pages 2-3, kowalik2024sexcordstromaltumors pages 3-4)
3.4 Suggested HPO terms (non-exhaustive)
- Painless testicular mass: Testicular mass (HP:0100633)
- Gynecomastia (HP:0000788)
- Precocious puberty (HP:0000826)
- Testicular atrophy (HP:0000029)
- Erectile dysfunction (HP:0100639)
- Azoospermia (HP:0000027) — described as “exceptionally rare” for Leydig cell tumor (kowalik2024sexcordstromaltumors pages 2-3)
3.5 Quality-of-life impact
Direct QoL instruments (EQ-5D/SF-36/PROMIS) specific to testicular SCSTs were not identified in the retrieved evidence set (evidence gap). However, endocrine and sexual symptoms (gynecomastia, libido/ED) plausibly impact QoL. (kowalik2024sexcordstromaltumors pages 2-3)
4. Genetic / Molecular Information
4.1 Causal genes / recurrent alterations (somatic; evidence-supported)
- CTNNB1 (β-catenin pathway): frequent in Sertoli cell tumors; nuclear β-catenin can be used diagnostically. (colecchia2023newsinthe pages 1-2)
- FOXL2: adult-type granulosa cell tumor association. (kowalik2024sexcordstromaltumors pages 2-3)
4.2 Pathogenic variants (examples)
Testicular adult granulosa cell tumor case (NGS panel; 520 genes): - FOXL2 C134W - CDKN2A E87Gfs24 - TP53 S183 - TERT promoter c.-124C>T - H3F3A K28R Direct abstract quote: “A high-throughput sequencing… revealed FOXL2 C134W, CDKN2A… TP53… TERT… and H3F3A… mutations…” (deng2023adultgranulosacell pages 1-2)
Variant interpretation notes: The evidence set does not provide ACMG/AMP classifications, allele frequencies (gnomAD), or systematic somatic frequency estimates for these variants in testicular SCSTs (evidence gap).
4.3 Modifier genes / epigenetics
No direct modifier-gene or epigenetic profiling results for testicular SCSTs were retrieved in this run. (evidence gap)
4.4 Mechanistic chain (from model organism evidence)
In a genetically engineered mouse model, constitutive activation of TGFBR1 in Sertoli cells produced disorganized seminiferous tubules and tumor nodules; tumors expressed granulosa cell markers (FOXL2, FOXO1, INHA) and lineage tracing supported Sertoli-to-granulosa transdifferentiation. (fang2023sertolicellspecificactivation pages 1-2)
Suggested GO biological process terms (conceptual mapping to the model evidence): - TGF-beta receptor signaling pathway (GO:0007179) - Cell fate commitment / transdifferentiation (general concept; specific GO term selection would require ontology lookup beyond current evidence) - Regulation of spermatogenesis (GO:0007283)
Suggested Cell Ontology (CL) terms (conceptual): - Sertoli cell (CL:0000212) - Leydig cell (CL:0000174) - Granulosa cell (CL:0000501)
5. Environmental Information
No toxin/lifestyle/infectious drivers were identified in the retrieved evidence set for testicular SCSTs. (evidence gap)
6. Mechanism / Pathophysiology
6.1 Molecular pathways implicated (from retrieved evidence)
- Wnt/β-catenin pathway (CTNNB1) in Sertoli-pattern tumors (diagnostic and likely oncogenic role). (colecchia2023newsinthe pages 1-2)
- TGFβ signaling dysregulation as sufficient to drive granulosa-like testicular tumorigenesis in a mouse model via Sertoli cell reprogramming. (fang2023sertolicellspecificactivation pages 1-2)
6.2 Cellular processes
- Sertoli cell reprogramming/transdifferentiation toward granulosa-like fate during tumorigenesis (model organism). (fang2023sertolicellspecificactivation pages 1-2)
7. Anatomical Structures Affected
7.1 Primary organ
- Testis (UBERON:0000473; ontology ID suggested conceptually)
7.2 Tissue/cell level
- Neoplastic processes involve sex cord elements (Sertoli-like / granulosa-like) and stromal components including Leydig cells depending on subtype. (colecchia2023newsinthe pages 1-2, fang2023sertolicellspecificactivation pages 1-2)
7.3 Localization and laterality
- Leydig cell tumors are typically unilateral; bilateral reported ~3%. (kowalik2024sexcordstromaltumors pages 1-2)
- Multiple described entities are “unilateral” and “solitary” in reported series (e.g., signet ring stromal tumor “always benign and unilateral”). (kowalik2024sexcordstromaltumors pages 3-4)
8. Temporal Development
8.1 Onset
- SCSTs occur across age groups depending on subtype: Leydig tumors mainly adults 20–60 with pediatric cases; juvenile granulosa tumors typically infants ≤6 months; adult-type granulosa mean ~42 years (review). (kowalik2024sexcordstromaltumors pages 1-2, kowalik2024sexcordstromaltumors pages 3-4)
8.2 Progression
- Although “usually indolent,” SCSTs can metastasize; advanced disease has poor outcomes and poor response to chemotherapy. (colecchia2023newsinthe pages 2-4, zuniga2020acomparisonof pages 3-5)
- Adult-type granulosa cell tumor of the testis: described as having “potentiality for late recurrence and metastasis.” (deng2023adultgranulosacell pages 1-2)
9. Inheritance and Population
9.1 Epidemiology and demographics (recently emphasized with registry data)
- Overall rarity: SCSTs represent about 5% of all testicular tumors. (colecchia2023newsinthe pages 1-2)
- Subtypes: Leydig cell tumors are the most common SCST subtype (~75% of SCSTs), followed by Sertoli cell tumors. (colecchia2023newsinthe pages 1-2)
NCDB (2004–2013) registry study—population and stage distribution: - 42,192 testicular cancers: 280 SCSTs, 41,912 GCTs. (zuniga2020acomparisonof pages 2-3) - SCST median age 45 (IQR 34–59) vs GCT 34 (IQR 27–43). (zuniga2020acomparisonof pages 2-3) - Stage: SCSTs were mostly stage I (93% in NCDB comparison). (zuniga2020acomparisonof pages 2-3)
9.2 Inheritance patterns
The evidence set includes syndromic associations (Carney complex; Peutz–Jeghers), but does not provide structured inheritance penetrance/expressivity data for testicular SCSTs (evidence gap). (kowalik2024sexcordstromaltumors pages 2-3, colecchia2023newsinthe pages 2-4)
10. Diagnostics
10.1 Laboratory markers
- Classic testicular tumor markers (AFP, β-hCG, LDH) are often normal in SCSTs and in multiple specific subtypes (e.g., large cell calcifying Sertoli cell tumor; juvenile granulosa cell tumor). (kowalik2024sexcordstromaltumors pages 2-3, kowalik2024sexcordstromaltumors pages 3-4)
10.2 Imaging
- Leydig cell tumor: typically hypoechoic on ultrasound; MRI is described as “particularly significant” and improves preoperative diagnostic accuracy for Leydig tumors. (kowalik2024sexcordstromaltumors pages 2-3)
10.3 Histopathology and immunohistochemistry (IHC)
Key IHC markers used in practice across SCSTs (subtype dependent): - Inhibin / inhibin A (common across sex cord-stromal tumors; e.g., juvenile granulosa “positive reactivity for inhibin alpha like all sex cord-stromal tumors”) (kowalik2024sexcordstromaltumors pages 3-4) - SF1 and Melan-A profiles for Leydig (noted in review table summary) (kowalik2024sexcordstromaltumors pages 4-6) - Large cell calcifying Sertoli: alpha-inhibin (≈90%), pan-cytokeratin, EMA, S-100, desmin, vimentin, NSE, chromogranin; negative OCT4/CD10/CD99/Melan-A (kowalik2024sexcordstromaltumors pages 2-3) - PRKAR1A IHC can aid diagnosis for large cell calcifying Sertoli cell tumor. (colecchia2023newsinthe pages 4-5) - Nuclear β-catenin staining supports CTNNB1-mutant Sertoli-pattern tumors and is diagnostically useful. (colecchia2023newsinthe pages 1-2)
Direct quote (WHO update; classification definitions): - “SCST NOS is instead reserved for SCSTs made up of undifferentiated/immature sex cord stromal cells which cannot be subtyped precisely.” (colecchia2023newsinthe pages 2-4)
10.4 Differential diagnosis
- Juvenile granulosa cell tumor vs yolk sac tumor: differential emphasized; juvenile granulosa typically has normal AFP and inhibin positivity. (kowalik2024sexcordstromaltumors pages 3-4)
11. Outcome / Prognosis
11.1 Registry-level survival statistics (real-world evidence)
NCDB analysis (Zuniga et al., BMC Urology; publication date Apr 2020; URL in paper record): - Stage I SCST: 1-, 2-, 5-year OS 99%, 96%, 94%. (zuniga2020acomparisonof pages 3-5) - Stage II/III SCST: 1-, 2-, 5-year OS 60%, 44%, 25%; adjusted mortality vs GCTs HR 3.28 (95% CI 1.88–5.73). (zuniga2020acomparisonof pages 3-5) - Overall SCST vs GCT adjusted HR for all-cause mortality: 1.68 (95% CI 1.13–2.49). (zuniga2020acomparisonof pages 2-3)
11.2 Subtype-level survival (from 2024 review synthesis)
- Malignant Leydig cell tumor: 5-year survival ~91%. (kowalik2024sexcordstromaltumors pages 1-2)
- Malignant Sertoli cell tumor stage I: 5-year survival ~77%. (kowalik2024sexcordstromaltumors pages 2-3)
11.3 Individual-level outcomes
- Adult testicular granulosa cell tumor case: no recurrence/metastasis at 6 years after orchiectomy + adjuvant BEP. (deng2023adultgranulosacell pages 1-2)
12. Treatment
12.1 Surgical management (standard of care)
- Inguinal radical orchiectomy is described as “gold standard” for multiple SCST subtypes in the 2024 review, especially when malignancy is suspected. (kowalik2024sexcordstromaltumors pages 2-3)
- Testis-sparing surgery (TSS) is recommended/considered for peripheral/small lesions and in scenarios such as solitary testis; however, “observation… below 1 cm is currently not recommended” in the review. (kowalik2024sexcordstromaltumors pages 1-2)
12.2 Lymph node surgery
- For malignant Sertoli tumors stage I, the review recommends retroperitoneal lymph node dissection (RPLND) even for stage I disease. (kowalik2024sexcordstromaltumors pages 2-3)
12.3 Systemic therapy and radiosensitivity
- The review notes SCSTs are “considered insensitive to chemotherapy and radiotherapy,” with scattered use of BEP/EP and other agents in advanced settings; residual masses after chemotherapy should be surgically removed (limited evidence base). (kowalik2024sexcordstromaltumors pages 4-6)
12.4 Example real-world regimen use
- Testicular adult granulosa cell tumor case: received 4 cycles of BEP as adjuvant therapy due to follow-up constraints, with 6-year disease-free status. (deng2023adultgranulosacell pages 1-2)
12.5 Clinical trials / registries relevant to testicular SCSTs (real-world implementations)
High-value implementations for rare tumor evidence generation are registries and natural history protocols: - NCT01970696 (International Ovarian & Testicular Stromal Tumor Registry; 2011; recruiting): collects clinical/pathologic/family history and biospecimens; explicitly focuses on ovarian/testicular stromal tumors, with emphasis on DICER1 and miRNA analyses. (NCT01970696 chunk 1) - URL: https://clinicaltrials.gov/study/NCT01970696 (registry entry) - NCT01572467 (COG; “DICER1 Mutations and miRNA in Ovarian and Testicular Sex Cord Stromal Tumors of Childhood”; 2012; completed): archived tissues, DICER1/miRNA analyses with clinical correlation; includes testicular sex cord–stromal tumor subtypes. (NCT01572467 chunk 1) - URL: https://clinicaltrials.gov/study/NCT01572467 (registry entry) - NCT03382158 (International PPB/DICER1 Registry; 2016; recruiting): includes sex-cord stromal tumor eligibility language; focuses on incidence and outcomes among germline DICER1 carriers. (NCT03382158 chunk 2) - URL: https://clinicaltrials.gov/study/NCT03382158 (registry entry)
12.6 Suggested MAXO terms (conceptual mapping)
- Radical orchiectomy (MAXO term suggestion; requires MAXO lookup outside current evidence)
- Testis-sparing surgery / partial orchiectomy (MAXO suggestion)
- Retroperitoneal lymph node dissection (MAXO suggestion)
- Platinum-based combination chemotherapy (e.g., BEP) (MAXO suggestion)
13. Prevention
No primary prevention measures were identified in the retrieved evidence set. Secondary prevention via screening is not standardized; however, registries aim to inform risk stratification and screening in genetically predisposed patients (e.g., DICER1-related). (NCT01970696 chunk 1, NCT03382158 chunk 2)
14. Other Species / Natural Disease
No naturally occurring veterinary/other-species evidence for testicular SCSTs was retrieved in this run (evidence gap).
15. Model Organisms
A mechanistic mouse model supports a causative role for TGFβ signaling activation in testicular granulosa-like tumor formation: - Sertoli-cell-specific TGFBR1 activation (Amh-Cre) → disorganized seminiferous tubules, tumor nodules, granulosa-marker expression (FOXL2/FOXO1/INHA), Sertoli-to-granulosa transdifferentiation evidence (lineage tracing). (fang2023sertolicellspecificactivation pages 1-2)
Recent developments and latest research emphasis (2023–2024)
WHO classification updates (2022 WHO; summarized in 2023)
A 2023 editorial summarizing WHO 5th edition updates highlights the introduction of new entities (signet ring stromal tumour; myoid gonadal stromal tumour) and reclassification moves (e.g., sertoliform cystadenoma). (colecchia2023newsinthe pages 1-2)
2024 synthesis in clinical literature
A 2024 review consolidates real-world management patterns (orchiectomy vs TSS), endocrine presentations, and rare subtype statistics (e.g., calcifying Sertoli tumor case counts; adult granulosa case counts). (kowalik2024sexcordstromaltumors pages 1-2, kowalik2024sexcordstromaltumors pages 3-4)
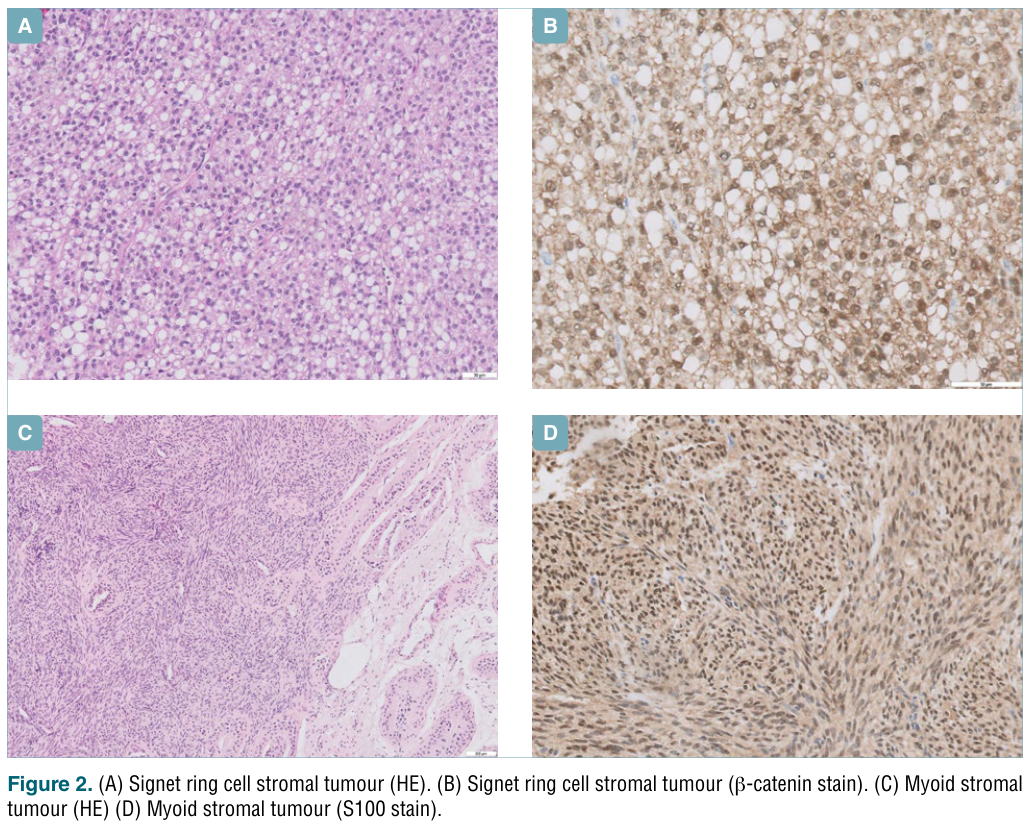
Visual evidence (classification/pathology figures)
- Representative micrographs of signet ring stromal tumour, myoid stromal tumour, and large cell calcifying Sertoli cell tumour with inhibin stain were extracted from the WHO classification update paper. (colecchia2023newsinthe media f299a589, colecchia2023newsinthe media 5201accc)
Summary Table of Major Subtypes
The following table consolidates subtype-level clinical, diagnostic, molecular, and outcome features from the retrieved sources.
Table (click to expand)
| Entity/subtype | Typical age | Frequency/rarity stats | Key clinical/endocrine features | Key diagnostic IHC markers | Key molecular/genetic associations | Typical management | Prognosis/outcome stats | Key sources (citation IDs) |
|---|---|---|---|---|---|---|---|---|
| Leydig cell tumor | Mostly adults 20–60 years; ~20% in children | ~1% of all testicular tumors; most common SCST; bilateral in ~3%; benign in ~80–90%, malignant in 10–20% | Adults: gynecomastia, testicular atrophy, decreased libido, erectile dysfunction, prostate atrophy; due to estradiol/progesterone/testosterone production. Children: precocious puberty, gynecomastia. Tumor markers usually normal; US typically hypoechoic; MRI useful | Reinke crystals on histology; table in review lists inhibin+, SF1+, MelanA+ for Leydig cell tumor | Sporadic FH mutation association reported with RCC; beta-catenin alterations reported in some Leydig tumors | Inguinal orchiectomy standard; testis-sparing surgery (TSS) for peripheral/small lesions; low sensitivity to chemo/radiotherapy | Malignant LCT 5-year survival ~91% | (kowalik2024sexcordstromaltumors pages 1-2, kowalik2024sexcordstromaltumors pages 2-3, kowalik2024sexcordstromaltumors pages 4-6, colecchia2023newsinthe pages 4-5) |
| Sertoli cell tumor (classic) | Not clearly specified in provided context; generally adult | <1% of all testicular tumors; second most common SCST after Leydig; usually benign and unilateral | Tumor markers usually normal; slight AFP elevation reported in some cases | WHO-recognized classic SCT; beta-catenin nuclear staining can be diagnostically useful in many Sertoli-pattern tumors | Large percentage show CTNNB1 mutation with nuclear β-catenin staining | Inguinal orchiectomy if malignancy suspected | Malignant stage I Sertoli tumor 5-year survival ~77%; RPLND recommended even for stage I malignant disease in cited review | (kowalik2024sexcordstromaltumors pages 2-3, colecchia2023newsinthe pages 1-2, colecchia2023newsinthe pages 4-5) |
| Large cell calcifying Sertoli cell tumor | Not clearly specified; can occur in syndromic settings | ~90 cases reported in literature; 16 malignant; ~17% may show malignancy/local invasion | Usually palpable hard painless testicular mass; often unilateral/single; may show skin involvement; US with calcifications and central vascularity; tumor markers may be normal | Alpha-inhibin positive in ~90%; also pan-cytokeratin, EMA, S100, desmin, vimentin, NSE, chromogranin positive; OCT4, CD10, CD99, Melan-A negative; PRKAR1A IHC may aid diagnosis | Associated with Carney complex; large cell calcifying SCT included among sporadic tumors and genetic syndromes; PRKAR1A diagnostically useful | Radical inguinal orchiectomy if suspected; RPLND if retroperitoneal nodes involved; TSS may be considered for superficial/peripheral/small/bilateral tumors given predominantly benign behavior | Predominantly benign; malignancy defined by adverse histologic criteria such as size >4 cm, vascular invasion, atypia, necrosis, increased mitoses | (kowalik2024sexcordstromaltumors pages 2-3, colecchia2023newsinthe pages 1-2, colecchia2023newsinthe pages 4-5) |
| Adult-type granulosa cell tumor | Average onset ~42 years; oldest reported 87 years | Extremely rare; 73 cases reported in review; usually large (10–14 cm) and unilateral | Gynecomastia in ~50%; often large masses with possible cystic components; microscopic “coffee-bean nuclei” | Inhibin A positive; in case report: inhibin+, vimentin+, CD117-, CD30-, CK/CK8-, EMA-, PLAP-, S100- | Associated with FOXL2 mutation; testicular frequency lower than ovarian counterpart; one sequenced case had FOXL2 C134W plus CDKN2A, TP53, TERT promoter, H3F3A mutations; recent work suggests testicular AGCTs differ molecularly from ovarian tumors | Inguinal orchiectomy is gold standard; TSS considered for atrophic/single testis; one case used adjuvant BEP after orchiectomy | Potential for late recurrence/metastasis; case report disease-free at 6 years after orchiectomy + BEP | (kowalik2024sexcordstromaltumors pages 3-4, deng2023adultgranulosacell pages 1-2, fang2023sertolicellspecificactivation pages 1-2) |
| Juvenile granulosa cell tumor | Primarily infants up to 6 months; rarely adults | Extremely rare | Usually painless testicular mass; often firm/cystic; associated with cryptorchidism or karyotypic abnormalities; AFP remains normal; lacks adult-type “coffee-bean nuclei” | Inhibin alpha positive like other SCSTs | Potential link to chromosomal abnormalities/aberrant gonadal development noted in review of testicular GCTs | TSS considered sufficient | No malignant cases reported in the cited literature; benign behavior | (kowalik2024sexcordstromaltumors pages 2-3, kowalik2024sexcordstromaltumors pages 3-4, fang2023sertolicellspecificactivation pages 1-2) |
| Signet ring stromal tumor | Not clearly specified in provided context | Exceptionally rare; testicular tumors usually 0.5–2.8 cm (average 0.9 cm) | Usually solitary, unilateral; no recurrences reported | Positive mainly for beta-keratin and vimentin; occasional CD99; resembles Sertoli tumor immunophenotypically; lacks Reinke crystals | Added as new WHO 5th edition entity; debate whether within Sertoli spectrum because of shared β-catenin profile | No official recommendations due to rarity; TSS appears appropriate | Reported as always benign in experts’ view; no malignant cases or recurrences reported | (kowalik2024sexcordstromaltumors pages 3-4, colecchia2023newsinthe pages 1-2, colecchia2023newsinthe pages 2-4) |
| Myoid gonadal stromal tumor | Adult men, around 40 years | Rare; usually ≤3 cm; largest reported 4.3 cm | Tumor markers usually normal; recent literature suggests benign behavior | Positive for FOXL2, S100, SF1, inhibin | New WHO 5th edition entity; listed separately because morphologically/IHC distinct from other sex-cord tumors | Not standardized; conservative/testis-sparing approach often favored for presumed benign lesions | Appears benign in available literature | (kowalik2024sexcordstromaltumors pages 3-4, kowalik2024sexcordstromaltumors pages 4-6, colecchia2023newsinthe pages 1-2) |
| SCST-NOS / mixed sex cord-stromal tumor | Not clearly specified in provided context | Rare; SCST-NOS reserved for undifferentiated/immature cells that cannot be precisely subtyped | Mixed tumors may present as gelatinous testicular masses; tumor markers usually normal; may show cystic/hemorrhagic areas; histology can include spindle, Sertoli, and granulosa-like elements | No single defining panel provided in context; diagnosis relies on mixed/undifferentiated morphology; SCST-NOS used when precise subtype not possible | WHO 2022 separates mixed SCSTs from SCST-NOS; mixed tumors contain variable sex-cord/stromal elements | Orchiectomy often performed because of diagnostic uncertainty; TSS may be considered if benign features suspected | SCSTs usually indolent overall, but metastases can occur even in morphologically typical tumors; advanced SCSTs have poor outcomes compared with GCTs | (colecchia2023newsinthe pages 2-4, kowalik2024sexcordstromaltumors pages 3-4, zuniga2020acomparisonof pages 3-5) |
Table: This table summarizes the major recognized subtypes of testicular sex cord-stromal tumors using only the provided context. It compares rarity, phenotype, diagnostic markers, molecular associations, management, and outcome data to support disease knowledge-base curation.
Key evidence gaps (for knowledge-base completion)
Within the tool-retrieved corpus for this run, the following could not be populated with primary sources: - MONDO/Orphanet/MeSH/ICD identifiers for the umbrella disease entity - Population incidence/prevalence per 100,000 specific to SCSTs (as opposed to the general testicular cancer incidence statement) - Systematic somatic mutation frequencies for FOXL2/CTNNB1/other genes across subtypes - QoL instrument data for testicular SCSTs specifically - Environmental/lifestyle protective factors and gene–environment interactions
These gaps are resolvable with targeted retrieval from ontologies (MONDO/MeSH/ICD) and additional subtype-specific genomic series (e.g., Modern Pathology/Histopathology cohorts) not accessible in the current evidence set.
References
-
(kowalik2024sexcordstromaltumors pages 1-2): Krzysztof Kowalik, Katarzyna Hetman, Krystian Kasperowicz, and Andrzej Modrzejewski. Sex cord-stromal tumors of the testis—a rare group of benign and malignant gonadal neoplasms. literature review. Oncology in Clinical Practice, 20:343-350, Oct 2024. URL: https://doi.org/10.5603/ocp.97184, doi:10.5603/ocp.97184. This article has 1 citations.
-
(colecchia2023newsinthe pages 1-2): Maurizio Colecchia, Felix Bremmer, and Giacomo Maria Pini. News in the classification of who 2022 testicular tumours. Pathologica, 115:3-7, Jan 2023. URL: https://doi.org/10.32074/1591-951x-825, doi:10.32074/1591-951x-825. This article has 6 citations.
-
(colecchia2023newsinthe pages 2-4): Maurizio Colecchia, Felix Bremmer, and Giacomo Maria Pini. News in the classification of who 2022 testicular tumours. Pathologica, 115:3-7, Jan 2023. URL: https://doi.org/10.32074/1591-951x-825, doi:10.32074/1591-951x-825. This article has 6 citations.
-
(colecchia2023newsinthe pages 4-5): Maurizio Colecchia, Felix Bremmer, and Giacomo Maria Pini. News in the classification of who 2022 testicular tumours. Pathologica, 115:3-7, Jan 2023. URL: https://doi.org/10.32074/1591-951x-825, doi:10.32074/1591-951x-825. This article has 6 citations.
-
(zuniga2020acomparisonof pages 2-3): Kyle B. Zuniga, Samuel L. Washington, Sima P. Porten, and Maxwell V. Meng. A comparison of stage-specific all-cause mortality between testicular sex cord stromal tumors and germ cell tumors: results from the national cancer database. BMC Urology, Apr 2020. URL: https://doi.org/10.1186/s12894-020-00609-2, doi:10.1186/s12894-020-00609-2. This article has 5 citations and is from a peer-reviewed journal.
-
(zuniga2020acomparisonof pages 3-5): Kyle B. Zuniga, Samuel L. Washington, Sima P. Porten, and Maxwell V. Meng. A comparison of stage-specific all-cause mortality between testicular sex cord stromal tumors and germ cell tumors: results from the national cancer database. BMC Urology, Apr 2020. URL: https://doi.org/10.1186/s12894-020-00609-2, doi:10.1186/s12894-020-00609-2. This article has 5 citations and is from a peer-reviewed journal.
-
(deng2023adultgranulosacell pages 1-2): Lili Deng, Jingjing Zeng, Jin Feng Qiu, Li Hua Yang, and Jie Ma. Adult granulosa cell tumor of the testis with malignant tendency: a case report with genetic analysis using high-throughput sequencing. Medicine, 102:e34523, Aug 2023. URL: https://doi.org/10.1097/md.0000000000034523, doi:10.1097/md.0000000000034523. This article has 1 citations and is from a peer-reviewed journal.
-
(fang2023sertolicellspecificactivation pages 1-2): Xin Fang, Linfeng Nie, Satwikreddy Putluri, Nan Ni, Laurent Bartholin, and Qinglei Li. Sertoli cell-specific activation of transforming growth factor beta receptor 1 leads to testicular granulosa cell tumor formation. Cells, 12:2717, Nov 2023. URL: https://doi.org/10.3390/cells12232717, doi:10.3390/cells12232717. This article has 5 citations.
-
(kowalik2024sexcordstromaltumors pages 2-3): Krzysztof Kowalik, Katarzyna Hetman, Krystian Kasperowicz, and Andrzej Modrzejewski. Sex cord-stromal tumors of the testis—a rare group of benign and malignant gonadal neoplasms. literature review. Oncology in Clinical Practice, 20:343-350, Oct 2024. URL: https://doi.org/10.5603/ocp.97184, doi:10.5603/ocp.97184. This article has 1 citations.
-
(kowalik2024sexcordstromaltumors pages 3-4): Krzysztof Kowalik, Katarzyna Hetman, Krystian Kasperowicz, and Andrzej Modrzejewski. Sex cord-stromal tumors of the testis—a rare group of benign and malignant gonadal neoplasms. literature review. Oncology in Clinical Practice, 20:343-350, Oct 2024. URL: https://doi.org/10.5603/ocp.97184, doi:10.5603/ocp.97184. This article has 1 citations.
-
(kowalik2024sexcordstromaltumors pages 4-6): Krzysztof Kowalik, Katarzyna Hetman, Krystian Kasperowicz, and Andrzej Modrzejewski. Sex cord-stromal tumors of the testis—a rare group of benign and malignant gonadal neoplasms. literature review. Oncology in Clinical Practice, 20:343-350, Oct 2024. URL: https://doi.org/10.5603/ocp.97184, doi:10.5603/ocp.97184. This article has 1 citations.
-
(NCT01970696 chunk 1): Kris Ann Schultz. International Ovarian & Testicular Stromal Tumor Registry. Children's Hospitals and Clinics of Minnesota. 2011. ClinicalTrials.gov Identifier: NCT01970696
-
(NCT01572467 chunk 1): Studying Genes in Samples From Younger Patients With Ovarian or Testicular Sex Cord Stromal Tumors. Children's Oncology Group. 2012. ClinicalTrials.gov Identifier: NCT01572467
-
(NCT03382158 chunk 2): International PPB/DICER1 Registry. Children's Hospitals and Clinics of Minnesota. 2016. ClinicalTrials.gov Identifier: NCT03382158
-
(colecchia2023newsinthe media f299a589): Maurizio Colecchia, Felix Bremmer, and Giacomo Maria Pini. News in the classification of who 2022 testicular tumours. Pathologica, 115:3-7, Jan 2023. URL: https://doi.org/10.32074/1591-951x-825, doi:10.32074/1591-951x-825. This article has 6 citations.
-
(colecchia2023newsinthe media 5201accc): Maurizio Colecchia, Felix Bremmer, and Giacomo Maria Pini. News in the classification of who 2022 testicular tumours. Pathologica, 115:3-7, Jan 2023. URL: https://doi.org/10.32074/1591-951x-825, doi:10.32074/1591-951x-825. This article has 6 citations.