1. Disease Information
1.1 Concise overview
Solitary fibrous tumor (SFT) is a rare fibroblastic mesenchymal neoplasm that can arise in many anatomical sites and often behaves indolently but has an unpredictable propensity for local recurrence and distant metastasis (ren2024advancesinthe pages 1-2, janik2023diagnosticsandtreatment pages 1-2). A defining molecular hallmark is the NAB2::STAT6 gene fusion, and nuclear STAT6 immunohistochemistry (IHC) is widely used as a surrogate diagnostic marker (ren2024advancesinthe pages 1-2, ren2024advancesinthe pages 10-12, janik2023diagnosticsandtreatment pages 1-2).
Recent synthesis characterizes SFT as “a rare fibroblastic mesenchymal neoplasm” (Ren 2024, published Aug 2024) (https://doi.org/10.1007/s10555-024-10204-8) (ren2024advancesinthe pages 1-2).
1.2 Key identifiers (availability in retrieved sources)
- MONDO: MONDO:0016238 (OpenTargets) (OpenTargets Search: Solitary fibrous tumor)
- Other identifiers (ICD-10/ICD-11, MeSH, Orphanet, OMIM): Not extracted from the retrieved full-text evidence in this run; should be completed by direct lookup in ICD/MeSH/Orphanet/OMIM.
1.3 Synonyms / alternative names
- Hemangiopericytoma (HPC): legacy terminology; many CNS and soft tissue tumors formerly classified as HPC are now encompassed within SFT under WHO reclassifications (wu2024clinicaloutcomesof pages 1-2, piccinelli2024demographicandclinical pages 1-2).
1.4 Evidence sources (individual patient vs aggregated)
This report integrates: - Aggregated cohort/registry evidence (SEER analysis; CNS cohort studies; systematic reviews) (wu2024clinicaloutcomesof pages 1-2, piccinelli2024demographicandclinical pages 1-2, tolstrup2024riskfactorsfor pages 1-2). - Aggregated review evidence (molecular/clinical reviews) (ren2024advancesinthe pages 1-2, janik2023diagnosticsandtreatment pages 1-2). - Individual case-based molecular pathology (e.g., intraosseous/epithelioid variants) used mainly for diagnostic marker panels and molecular confirmation methods (argyris2024primaryintraosseoussolitary pages 1-2, zhao2024epithelioidsolitaryfibrous pages 1-2).
2. Etiology
2.1 Disease causal factors (molecular/genetic mechanism)
SFT is primarily driven by a somatic intrachromosomal rearrangement on chromosome 12q13 producing the NAB2–STAT6 fusion (ren2024advancesinthe pages 1-2, zhao2024epithelioidsolitaryfibrous pages 1-2). Mechanistically, the fusion alters transcriptional control: Ren 2024 states the fusion “transforms NAB2 into a transcriptional activator, activating early growth response 1 (EGR1)” (https://doi.org/10.1007/s10555-024-10204-8; Aug 2024) (ren2024advancesinthe pages 1-2).
2.2 Risk factors
Evidence in the retrieved corpus supports prognostic risk factors (risk of recurrence/metastasis) more than pre-disease exposures: - The 2024 systematic review found the most consistent recurrence predictors were high mitotic index, high Ki‑67, and necrosis (Tolstrup 2024; Jan 2024) (https://doi.org/10.3389/fsurg.2024.1332421) (tolstrup2024riskfactorsfor pages 1-2). - Molecular risk factors/biomarkers suggested to refine risk include TERT promoter mutations and TP53 alterations, with additional factors (APAF1 inactivation, etc.) variably reported (yao2024prognosticanalysisof pages 1-2, janik2023diagnosticsandtreatment pages 16-17, tolstrup2024riskfactorsfor pages 1-2).
Pre-disease environmental/lifestyle risks: not established in the retrieved sources; SFT is generally treated as a sporadic tumor entity.
2.3 Protective factors
No protective genetic/environmental factors were identified in the retrieved evidence.
2.4 Gene–environment interaction
No gene–environment interaction evidence was identified in the retrieved evidence.
3. Phenotypes
3.1 Clinical presentation (common patterns)
SFTs often present as slow-growing masses and can be asymptomatic depending on site (ren2024advancesinthe pages 1-2, janik2023diagnosticsandtreatment pages 1-2). Symptomatology is largely site-driven (compression, pain, neurologic deficits in CNS, etc.). In malignant pleural SFT, a majority in one cohort were symptomatic (62%) (ricciardi2023malignantsolitaryfibrous pages 1-2).
3.2 Histopathologic phenotype
Core morphologic phenotype includes spindle-to-ovoid cells with a prominent branching (“staghorn”) vasculature. For example, an intraosseous case review described “a haphazardly-arranged population of spindled-to-ovoid cells surrounding a prominent, branching and hyalinized vasculature” (Argyris 2024; Dec 2024) (https://doi.org/10.1007/s12105-024-01735-1) (argyris2024primaryintraosseoussolitary pages 1-2).
3.3 Suggested HPO terms (examples; frequency generally not quantified in retrieved evidence)
Because SFT manifestations are site-dependent, suggested HPO terms are necessarily generic: - Mass / tumor: HP:0002664 (Neoplasm) (suggested) - Localized pain: HP:0012531 (Pain) (suggested) - Compression symptoms (site-specific): e.g., HP:0002664 (Neoplasm) + organ-specific dysfunction terms (suggested)
Note: The retrieved evidence did not provide robust phenotype frequency tables beyond site distributions in malignant cohorts (piccinelli2024demographicandclinical pages 1-2).
4. Genetic / Molecular Information
4.1 Causal gene(s) and hallmark alteration
- NAB2::STAT6 gene fusion (driver/defining event) (ren2024advancesinthe pages 1-2, argyris2024primaryintraosseoussolitary pages 1-2, zhao2024epithelioidsolitaryfibrous pages 1-2).
- Common fusion variants reported as frequent include NAB2ex4–STAT6ex2 and NAB2ex6–STAT6ex16/ex17 (Ren 2024; Aug 2024) (ren2024advancesinthe pages 1-2).
4.2 Somatic vs germline
SFT is generally treated as nonhereditary/sporadic. An RNA-therapy SFT model paper explicitly states: “This nonhereditary cancer is the result of an environmental intrachromosomal gene fusion between NAB2 and STAT6 on chromosome 12” (Li 2023; Jun 2023) (https://doi.org/10.3390/cancers15123127) ().
4.3 Diagnostic molecular surrogates
STAT6 IHC is widely used as a surrogate for NAB2–STAT6 fusion. A key quantitative statement from Ren 2024 notes: “diffuse and robust nuclear expression of STAT6 through IHC was documented in 100% of cases, with concurrent gene fusion detection in 92% of cases through RT-PCR” (https://doi.org/10.1007/s10555-024-10204-8; Aug 2024) (ren2024advancesinthe pages 10-12).
4.4 Additional molecular alterations (progression/aggressiveness)
- In an extrameningeal cohort (n=111), TP53 and TERT promoter mutations were associated with progression in several patients (Yao 2024; Jan 2024) (https://doi.org/10.3389/fonc.2023.1272090) (yao2024prognosticanalysisof pages 1-2).
- The WHO-referenced clinical review highlights aggressive-associated findings such as TERT promoter mutations and TP53 immunopositivity with loss of APAF1 (janik2023diagnosticsandtreatment pages 16-17).
4.5 Epigenetic information
Not extracted from retrieved evidence in this run.
4.6 Suggested GO / CL terms (mechanism-linked; examples)
- GO:0006355 (Regulation of transcription, DNA-templated) — consistent with fusion-driven transcriptional reprogramming (suggested; supported mechanistically by EGR1 activation narrative) (ren2024advancesinthe pages 1-2).
- CL:0002554 (fibroblast) — consistent with fibroblastic/mesenchymal tumor lineage (suggested) (ren2024advancesinthe pages 1-2, janik2023diagnosticsandtreatment pages 1-2).
5. Environmental Information
No specific toxins, radiation, lifestyle exposures, or infectious agents were identified as causal or modifying factors in the retrieved evidence.
6. Mechanism / Pathophysiology
6.1 Causal chain (current understanding)
- Initiating lesion: intrachromosomal rearrangement on chromosome 12q13 → NAB2::STAT6 fusion (ren2024advancesinthe pages 1-2, zhao2024epithelioidsolitaryfibrous pages 1-2).
- Transcriptional reprogramming: fusion alters NAB2/STAT6 function; review states it “transforms NAB2 into a transcriptional activator” and activates EGR1 programs (ren2024advancesinthe pages 1-2).
- Cellular consequences: altered enhancer/promoter activity and gene-expression programs consistent with proliferative and pro-survival states; mechanistic model systems show the fusion can be studied via inducible expression systems and primary tumor chromatin profiling (hill2025nab2stat6drivesan pages 4-6, hill2025nab2stat6drivesan pages 1-3).
- Clinical manifestation: tumor formation with characteristic fibroblastic morphology and hypervascular “staghorn” vasculature; malignant transformation/progression correlates with proliferation/necrosis and additional molecular lesions (TP53/TERT/APAF1) (argyris2024primaryintraosseoussolitary pages 1-2, janik2023diagnosticsandtreatment pages 16-17, yao2024prognosticanalysisof pages 1-2).
6.2 Upstream vs downstream
- Upstream (driver/defining): NAB2::STAT6 fusion (ren2024advancesinthe pages 1-2, argyris2024primaryintraosseoussolitary pages 1-2).
- Downstream (progression modifiers): mitotic index, Ki-67, necrosis and secondary alterations (TERT promoter mutation, TP53 alteration, APAF1 loss) that correlate with recurrence/progression (tolstrup2024riskfactorsfor pages 1-2, yao2024prognosticanalysisof pages 1-2, janik2023diagnosticsandtreatment pages 16-17).
7. Anatomical Structures Affected
7.1 Organ-level distribution (malignant SFT registry evidence)
A large SEER analysis of 1,134 malignant SFT cases (2000–2019) reported primary sites: chest 28–29%, CNS 22–23%, head and neck 11%, pelvis 11%, extremities 10%, abdomen 10%, retroperitoneum 6% (Piccinelli 2024; Sep 2024) (https://doi.org/10.3390/cancers16193331) (piccinelli2024demographicandclinical pages 1-2, piccinelli2024demographicandclinical pages 2-4).
7.2 Suggested UBERON terms (examples)
- UBERON:0002048 (lung) / pleura-adjacent thoracic tissues (thoracic SFT common) (suggested; supported by pleural predominance in reviews and SEER distribution) (ren2024advancesinthe pages 1-2, piccinelli2024demographicandclinical pages 1-2)
- UBERON:0000955 (brain) / meninges (CNS SFT) (suggested; CNS cohorts) (wu2024clinicaloutcomesof pages 1-2)
- UBERON:0002385 (trunk) and region/site-specific structures depending on presentation (suggested)
8. Temporal Development
8.1 Onset
Typical diagnosis is in middle age to older adults; an extrameningeal review notes presentation often in the 50s–70s (janik2023diagnosticsandtreatment pages 1-2). SEER malignant cohort median age was 60 years (piccinelli2024demographicandclinical pages 2-4).
8.2 Progression and disease course
SFT may recur late; a systematic review reports recurrence estimates around 10–20% in many studies, with longer follow-up cohorts reporting >30% (Tolstrup 2024; Jan 2024) (tolstrup2024riskfactorsfor pages 2-3). CNS SFT demonstrates grade-dependent outcomes with median PFS/OS decreasing from grade 1 to grade 3 (wu2024clinicaloutcomesof pages 1-2).
9. Inheritance and Population
9.1 Epidemiology
- Rarity/incidence: one recent review reports 1–2 per million (Ren 2024; Aug 2024) (ren2024advancesinthe pages 1-2); another review reports ~0.061 per 100,000/year and SFTs representing <2% of soft tissue tumors/masses (Janik 2023; Dec 2023) (janik2023diagnosticsandtreatment pages 1-2).
9.2 Population demographics
- SEER malignant cohort: 49% male; 87% underwent surgery; stage distribution localized 42%, locally advanced 35%, metastatic 13% (piccinelli2024demographicandclinical pages 1-2).
9.3 Inheritance
No Mendelian inheritance pattern is supported; evidence emphasizes nonhereditary/sporadic nature ().
10. Diagnostics
10.1 Pathology and immunohistochemistry (IHC)
- Core IHC markers: STAT6 (nuclear) and CD34 (cytoplasmic) are emphasized as mainstays in extrameningeal SFT diagnosis (Janik 2023; Dec 2023) (janik2023diagnosticsandtreatment pages 1-2).
- STAT6 as fusion surrogate: “STAT6 IHC nuclear staining … has been validated as a valuable surrogate marker for detecting NAB2-STAT6 gene fusion” (Ren 2024; Aug 2024) (ren2024advancesinthe pages 10-12), with the quantitative concordance statement noted above (100% STAT6 nuclear IHC; 92% RT-PCR fusion detection) (ren2024advancesinthe pages 10-12).
- Diagnostic caveat: specificity is imperfect because STAT6 expression can occur in other sarcomas (Ren 2024) (ren2024advancesinthe pages 10-12).
10.2 Molecular confirmation options
Molecular confirmation and characterization may use RT-PCR, targeted RNA sequencing/NGS fusion panels, WGS/WES/RNA-seq, or FISH depending on specimen and clinical need (ren2024advancesinthe pages 10-12, argyris2024primaryintraosseoussolitary pages 1-2). A concrete implementation example is an intraosseous SFT case that used an RNA-based NGS fusion panel (Arriba software) plus a DNA NGS panel and FISH for other differential considerations (Argyris 2024; Dec 2024) (argyris2024primaryintraosseoussolitary pages 1-2).
10.3 Differential diagnosis (marker panels)
An epithelioid SFT series noted STAT6/CD34 positivity with negative keratins and other lineage markers, supporting broad differential exclusion in unusual morphologies (Zhao 2024; Oct 2024) (https://doi.org/10.1186/s13000-024-01564-4) (zhao2024epithelioidsolitaryfibrous pages 1-2).
10.4 Imaging
Imaging is important for localization/staging but not diagnostic alone; histologic confirmation is required (review-level statement) (ren2024advancesinthe pages 1-2).
11. Outcome / Prognosis
11.1 Prognostic models and key statistics
A compact quantitative summary of major outcome and prognostic evidence is provided in the table below.
Table (click to expand)
| Item | Key numbers/findings | Population/context | Source (URL; year) | Evidence citation id |
|---|---|---|---|---|
| Incidence / rarity | Incidence reported at ~0.061 per 100,000/year; also described as 1–2 per million people/year; SFTs account for <2% of soft tissue tumors/masses | General / extrameningeal SFT in reviews | Janik et al., Cancers (https://doi.org/10.3390/cancers15245854; 2023); Ren et al., Cancer Metastasis Rev. (https://doi.org/10.1007/s10555-024-10204-8; 2024) | (janik2023diagnosticsandtreatment pages 1-2, ren2024advancesinthe pages 1-2) |
| Recurrence / metastasis rates | Reviews cite 10–30% recurrence after resection; recurrence/metastasis rate broadly 10–40%; longer-follow-up cohorts may report recurrence >30% | Mixed non-CNS SFT cohorts, especially resected torso/extremity disease | Tolstrup et al., Front Surg (https://doi.org/10.3389/fsurg.2024.1332421; 2024); Zhang et al., Nat Commun (https://doi.org/10.1038/s41467-023-43249-4; 2023) | (tolstrup2024riskfactorsfor pages 1-2, tolstrup2024riskfactorsfor pages 2-3, yao2024prognosticanalysisof pages 1-2) |
| SEER malignant SFT cohort | n=1,134 malignant SFTs; sites: chest 28–29%, CNS 22–23%, head/neck 11%, pelvis 11%, extremities 10%, abdomen 10%, retroperitoneum 6%; stage: localized 42%, locally advanced 35%, metastatic 13%; surgery in 87% | SEER 2000–2019 malignant SFT population-based cohort | Piccinelli et al., Cancers (https://doi.org/10.3390/cancers16193331; 2024) | (piccinelli2024demographicandclinical pages 1-2, piccinelli2024demographicandclinical pages 2-4) |
| SEER prognostic factors | Higher cancer-specific mortality with locally advanced stage HR 1.6, metastatic stage HR 2.9, non-surgical management HR 3.6, tumor size 9–15.9 cm HR 1.6, ≥16 cm HR 1.9 | Multivariable competing-risks analysis in SEER malignant SFT cohort | Piccinelli et al., Cancers (https://doi.org/10.3390/cancers16193331; 2024) | (piccinelli2024demographicandclinical pages 1-2) |
| CNS WHO grade outcomes | Grade 1: median PFS 105 mo, OS 199 mo; Grade 2: PFS 77 mo, OS 145 mo; Grade 3: PFS 44 mo, OS 112 mo; cohort counts: grade 1 86, grade 2 35, grade 3 25 | Reclassified CNS SFT/HPC cohort, n=146, per WHO 2021 CNS classification | Wu et al., J Neurosurg (https://doi.org/10.3171/2023.4.JNS23147; 2024) | (wu2024clinicaloutcomesof pages 1-2) |
| CNS recurrence / mortality / treatment effect | Local recurrence in 61/146; deaths 31/146, of which 27/31 (87.1%) disease-related; subtotal resection worsened PFS (HR 4.648) and OS (HR 3.217); grade 3 worsened PFS (HR 5.814) and OS (HR 3.433) | Same CNS cohort | Wu et al., J Neurosurg (https://doi.org/10.3171/2023.4.JNS23147; 2024) | (wu2024clinicaloutcomesof pages 1-2) |
| Pleural malignant SFT outcomes | 5-year OS 81.2%, 5-year DFS 77.4%; recurrence in 9/34 (26.5%); median follow-up 111 months; median age 67 years | Single-center cohort of malignant pleural SFT, n=34 | Ricciardi et al., J Clin Med (https://doi.org/10.3390/jcm12030966; 2023) | (ricciardi2023malignantsolitaryfibrous pages 1-2) |
| Pleural malignant SFT prognostic factors | Worse OS: necrosis, nuclear atypia, tumor size >11.5 cm, relapse/progression; worse DFS: non-radical resection, larger size, necrosis, nuclear atypia, pleural pattern; Tapias score best predicted OS/DFS | Same malignant pleural SFT cohort | Ricciardi et al., J Clin Med (https://doi.org/10.3390/jcm12030966; 2023) | (ricciardi2023malignantsolitaryfibrous pages 1-2) |
| Recurrence risk factors across studies | Most consistent adverse factors: high mitotic index, necrosis, high Ki-67 index; additional variably associated factors: age, tumor size, sex, margins, location, pleomorphism, hypercellularity, dedifferentiation, CD34, TP53, APAF1, TERT promoter mutation, NAB2::STAT6 variant | 81 retrospective studies in systematic review of resected torso/extremity SFT | Tolstrup et al., Front Surg (https://doi.org/10.3389/fsurg.2024.1332421; 2024) | (tolstrup2024riskfactorsfor pages 2-3, tolstrup2024riskfactorsfor pages 1-2) |
| Modified Demicco model performance caveat | In 111 extrameningeal SFTs, progression still occurred in 3/74 low-risk and 7/21 intermediate-risk cases; TP53 alterations: progression in 3/5; TERT promoter mutations: progression in 3/4 followed cases | East China extrameningeal SFT series, n=111 | Yao et al., Front Oncol (https://doi.org/10.3389/fonc.2023.1272090; 2024) | (yao2024prognosticanalysisof pages 1-2) |
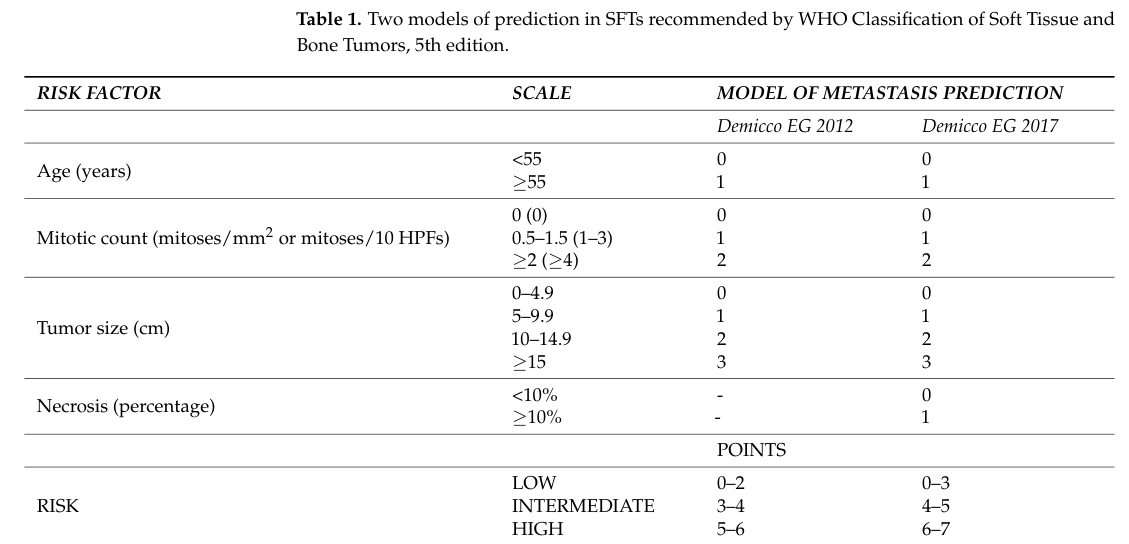
| Demicco risk model variables | WHO-recommended Demicco models use age, tumor size, mitotic count, and in the modified 4-variable model necrosis to assign low/intermediate/high metastatic risk | Risk stratification for extrameningeal SFT | Janik et al., Cancers (https://doi.org/10.3390/cancers15245854; 2023); image extract of Demicco table | (janik2023diagnosticsandtreatment pages 16-17, janik2023diagnosticsandtreatment media 2935871a) |
| WHO/CNS grading variables | CNS WHO grading uses mitotic activity and necrosis: grade 1 <2.5 mitoses/mm², grade 2 ≥2.5 mitoses/mm², grade 3 ≥2.5 mitoses/mm² plus necrosis | WHO 2021 CNS SFT framework | Wu et al., J Neurosurg (https://doi.org/10.3171/2023.4.JNS23147; 2024) | (wu2024clinicaloutcomesof pages 1-2) |
Table: This table compiles the main quantitative epidemiology, prognosis, and risk-model findings for solitary fibrous tumor from the gathered evidence. It is useful as a compact reference for incidence, recurrence, survival, and the variables used in current risk stratification systems.
11.2 Risk stratification (Demicco and others)
WHO-referenced models use age, tumor size, mitotic count, and (in a 4-variable modification) necrosis to stratify metastatic risk (janik2023diagnosticsandtreatment pages 16-17). The extracted table image below shows the Demicco scoring framework as presented in a 2023 review (janik2023diagnosticsandtreatment media 2935871a).
11.3 Evidence-based prognostic factors
The 2024 systematic review identified mitotic index, necrosis, and Ki‑67 as the most solid predictors of recurrence after resection across multiple retrospective studies (tolstrup2024riskfactorsfor pages 1-2). Large-registry evidence indicates stage, surgery, and tumor size independently predict cancer-specific mortality in malignant SFT (piccinelli2024demographicandclinical pages 1-2).
12. Treatment
12.1 Localized disease
- Surgery: Radical/en bloc resection with negative margins is the cornerstone of treatment (review consensus) (ren2024advancesinthe pages 10-12, janik2023diagnosticsandtreatment pages 1-2).
- Radiotherapy: In CNS SFT, gross-total resection prolongs PFS/OS; adjuvant radiotherapy appears beneficial after subtotal resection (Wu 2024; Jan 2024) (https://doi.org/10.3171/2023.4.JNS23147) (wu2024clinicaloutcomesof pages 1-2).
12.2 Advanced/metastatic disease (systemic therapy)
Evidence synthesized in recent reviews indicates: - Conventional chemotherapy has limited durable benefit; one review states conventional chemotherapy is “not associated with long-term positive effects” (Janik 2023; Dec 2023) (janik2023diagnosticsandtreatment pages 13-14). - Anti-angiogenic therapy (TKIs/VEGF-pathway inhibition) shows more consistent disease control and higher response rates by Choi criteria. Janik 2023 summarizes pazopanib as “the best first-line treatment” in the advanced setting with reported Choi partial responses and high disease-control rates, and reports activity for axitinib and sunitinib with median PFS on the order of months (janik2023diagnosticsandtreatment pages 13-14). - A broader systemic-therapy synthesis reports typical outcomes such as pazopanib median PFS ~5–6 months in aggressive SFT trials (with higher Choi response rates than RECIST) and sunitinib median PFS ~6–7 months in series; temozolomide+bevacizumab has reported median PFS ~9.7–10.8 months in retrospective analyses (martinbroto2021acomprehensivereview pages 15-16).
12.3 Clinical trials (real-world implementation)
ClinicalTrials.gov evidence in this run identified completed phase II studies specifically in SFT: - Axitinib in advanced SFT (NCT02261207; Phase II; completed; n=17) (). - Pazopanib in SFT (NCT02066285; Phase II; completed; n=96) ().
Note: The retrieved trial records provide trial existence/phase/enrollment; numerical efficacy endpoints were not extracted from the trial registry chunks in this run.
12.4 Suggested MAXO terms (examples)
- MAXO:0000601 (Surgical resection) (suggested; supported by standard-of-care) (janik2023diagnosticsandtreatment pages 1-2)
- MAXO:0000016 (Radiotherapy) (suggested; CNS adjuvant RT evidence) (wu2024clinicaloutcomesof pages 1-2)
- MAXO:0000750 (Targeted therapy) / antiangiogenic TKI therapy (suggested; multiple TKI evidence) (janik2023diagnosticsandtreatment pages 13-14)
13. Prevention
No established primary prevention strategies are supported in the retrieved evidence. Secondary prevention largely corresponds to surveillance/follow-up to detect late recurrence (review consensus) (janik2023diagnosticsandtreatment pages 1-2, tolstrup2024riskfactorsfor pages 1-2).
14. Other Species / Natural Disease
Robust evidence for naturally occurring SFT in non-human species was not identified in the retrieved, SFT-focused corpus for this run. (A separate veterinary sarcoma imaging/metastasis paper retrieved was not SFT-specific and is therefore not used to support SFT natural-history claims.)
15. Model Organisms / Experimental Models
Recent and emerging SFT research leverages engineered and patient-derived models: - CRISPR/SpCas9 engineered in vitro models harboring NAB2–STAT6, used to evaluate fusion-specific antisense oligonucleotides and CRISPR/CasRx approaches (Li 2023; Jun 2023) (https://doi.org/10.3390/cancers15123127) (). - Inducible fusion-expression cell models for chromatin/transcriptional studies and use of primary human tumor material for ChIP-seq-based mapping of fusion-associated binding (hill2025nab2stat6drivesan pages 4-6). - Patient-derived xenograft (mouse) models are reported in RNA/antisense oligonucleotide development literature (e.g., STAT6-targeting ASO studies) (Li 2024; Jun 2024) (https://doi.org/10.1016/j.omtn.2024.102154) ().
Visual Evidence: Demicco Risk Model Table
The following image extract shows a WHO-referenced Demicco risk stratification table (variables: age, tumor size, mitotic count, necrosis) as presented in a 2023 review. (janik2023diagnosticsandtreatment media 2935871a)
Notes on Evidence Gaps
- ICD/MeSH/Orphanet/OMIM identifiers, detailed phenotype frequencies, and epigenomic profiling summaries were not present in the retrieved evidence snippets and should be filled via targeted database queries.
- Some systemic therapy efficacy statistics cited here derive from review-level syntheses; for knowledge-base ingestion, confirm each numerical endpoint against the original trial/series publications referenced in those reviews.
References
-
(OpenTargets Search: Solitary fibrous tumor): Open Targets Query (Solitary fibrous tumor, 15 results). Buniello, A. et al. (2025). Open Targets Platform: facilitating therapeutic hypotheses building in drug discovery. Nucleic Acids Research.
-
(ren2024advancesinthe pages 1-2): Chongmin Ren, Gina Z D'Amato, Francis J Hornicek, Hao Tao, and Zhenfeng Duan. Advances in the molecular biology of the solitary fibrous tumor and potential impact on clinical applications. Cancer Metastasis Reviews, 43:1337-1352, Aug 2024. URL: https://doi.org/10.1007/s10555-024-10204-8, doi:10.1007/s10555-024-10204-8. This article has 21 citations.
-
(piccinelli2024demographicandclinical pages 1-2): Mattia Luca Piccinelli, Kyle Law, Reha-Baris Incesu, Stefano Tappero, Cristina Cano Garcia, Francesco Barletta, Simone Morra, Lukas Scheipner, Andrea Baudo, Zhe Tian, Stefano Luzzago, Francesco Alessandro Mistretta, Matteo Ferro, Fred Saad, Shahrokh F. Shariat, Luca Carmignani, Sascha Ahyai, Nicola Longo, Alberto Briganti, Felix K. H. Chun, Carlo Terrone, Derya Tilki, Ottavio de Cobelli, Gennaro Musi, and Pierre I. Karakiewicz. Demographic and clinical characteristics of malignant solitary fibrous tumors: a seer database analysis. Cancers, 16:3331, Sep 2024. URL: https://doi.org/10.3390/cancers16193331, doi:10.3390/cancers16193331. This article has 12 citations.
-
(janik2023diagnosticsandtreatment pages 1-2): Anna Maria Janik, Anna Terlecka, Mateusz J. Spałek, Kjetil Boye, Bartłomiej Szostakowski, Paulina Chmiel, Anna Szumera-Ciećkiewicz, Klaudia Bobak, Tomasz Świtaj, Piotr Rutkowski, and Anna M. Czarnecka. Diagnostics and treatment of extrameningeal solitary fibrous tumors. Cancers, 15:5854, Dec 2023. URL: https://doi.org/10.3390/cancers15245854, doi:10.3390/cancers15245854. This article has 21 citations.
-
(ren2024advancesinthe pages 10-12): Chongmin Ren, Gina Z D'Amato, Francis J Hornicek, Hao Tao, and Zhenfeng Duan. Advances in the molecular biology of the solitary fibrous tumor and potential impact on clinical applications. Cancer Metastasis Reviews, 43:1337-1352, Aug 2024. URL: https://doi.org/10.1007/s10555-024-10204-8, doi:10.1007/s10555-024-10204-8. This article has 21 citations.
-
(wu2024clinicaloutcomesof pages 1-2): Yingxi Wu, Tianzhi Zhao, Yaning Cai, Min Zheng, Yunze Zhang, Yan Qu, and Qing Cai. Clinical outcomes of solitary fibrous tumors and hemangiopericytomas and risk factors related to recurrence and survival based on the 2021 who classification of central nervous system tumors. Journal of Neurosurgery, 140(1):69-79, Jan 2024. URL: https://doi.org/10.3171/2023.4.jns23147, doi:10.3171/2023.4.jns23147. This article has 27 citations and is from a domain leading peer-reviewed journal.
-
(tolstrup2024riskfactorsfor pages 1-2): Johan Tolstrup, Anand Loya, Ninna Aggerholm-Pedersen, Louise Preisler, and Luit Penninga. Risk factors for recurrent disease after resection of solitary fibrous tumor: a systematic review. Frontiers in Surgery, Jan 2024. URL: https://doi.org/10.3389/fsurg.2024.1332421, doi:10.3389/fsurg.2024.1332421. This article has 21 citations.
-
(argyris2024primaryintraosseoussolitary pages 1-2): Prokopios P. Argyris, Kristie L. Wise, Kristin K. McNamara, Daniel M. Jones, and John R. Kalmar. Primary intraosseous solitary fibrous tumor of the mandible: report of a diagnostically challenging case with nab2::stat6 fusion and review of the literature. Head and neck pathology, 18 1:128, Dec 2024. URL: https://doi.org/10.1007/s12105-024-01735-1, doi:10.1007/s12105-024-01735-1. This article has 1 citations and is from a peer-reviewed journal.
-
(zhao2024epithelioidsolitaryfibrous pages 1-2): Lina Zhao, Jiajing Ma, Jiacai Ren, Jingping Yuan, Huihua He, Yabing Huang, and Honglin Yan. Epithelioid solitary fibrous tumors from cns and soft tissues: an unusual morphologic variant. Diagnostic Pathology, Oct 2024. URL: https://doi.org/10.1186/s13000-024-01564-4, doi:10.1186/s13000-024-01564-4. This article has 2 citations and is from a peer-reviewed journal.
-
(yao2024prognosticanalysisof pages 1-2): Chen-chen Yao, Jian Zhou, Xiao Li, Jun Yang, Gang Chen, Jia Wei, Qin-he Fan, and Qi-xing Gong. Prognostic analysis of extrameningeal solitary fibrous tumor using the modified demicco model: a clinicopathologic study of 111 chinese cases. Frontiers in Oncology, Jan 2024. URL: https://doi.org/10.3389/fonc.2023.1272090, doi:10.3389/fonc.2023.1272090. This article has 2 citations.
-
(janik2023diagnosticsandtreatment pages 16-17): Anna Maria Janik, Anna Terlecka, Mateusz J. Spałek, Kjetil Boye, Bartłomiej Szostakowski, Paulina Chmiel, Anna Szumera-Ciećkiewicz, Klaudia Bobak, Tomasz Świtaj, Piotr Rutkowski, and Anna M. Czarnecka. Diagnostics and treatment of extrameningeal solitary fibrous tumors. Cancers, 15:5854, Dec 2023. URL: https://doi.org/10.3390/cancers15245854, doi:10.3390/cancers15245854. This article has 21 citations.
-
(ricciardi2023malignantsolitaryfibrous pages 1-2): Sara Ricciardi, Delia Giovanniello, Luigi Carbone, Francesco Carleo, Marco Di Martino, Massimo Osvaldo Jaus, Sara Mantovani, Stefano Treggiari, Andrea Tornese, and Giuseppe Cardillo. Malignant solitary fibrous tumours of the pleura are not all the same: analysis of long-term outcomes and evaluation of risk stratification models in a large single-centre series. Journal of Clinical Medicine, 12:966, Jan 2023. URL: https://doi.org/10.3390/jcm12030966, doi:10.3390/jcm12030966. This article has 4 citations.
-
(hill2025nab2stat6drivesan pages 4-6): Connor M Hill, Alexandra Indeglia, Francis Picone, Maureen E Murphy, Cara Cipriano, Robert G Maki, and Alessandro Gardini. Nab2-stat6 drives an egr1-dependent neuroendocrine program in solitary fibrous tumors. Feb 2025. URL: https://doi.org/10.7554/elife.98072, doi:10.7554/elife.98072. This article has 7 citations.
-
(hill2025nab2stat6drivesan pages 1-3): Connor M Hill, Alexandra Indeglia, Francis Picone, Maureen E Murphy, Cara Cipriano, Robert G Maki, and Alessandro Gardini. Nab2-stat6 drives an egr1-dependent neuroendocrine program in solitary fibrous tumors. Feb 2025. URL: https://doi.org/10.7554/elife.98072, doi:10.7554/elife.98072. This article has 7 citations.
-
(piccinelli2024demographicandclinical pages 2-4): Mattia Luca Piccinelli, Kyle Law, Reha-Baris Incesu, Stefano Tappero, Cristina Cano Garcia, Francesco Barletta, Simone Morra, Lukas Scheipner, Andrea Baudo, Zhe Tian, Stefano Luzzago, Francesco Alessandro Mistretta, Matteo Ferro, Fred Saad, Shahrokh F. Shariat, Luca Carmignani, Sascha Ahyai, Nicola Longo, Alberto Briganti, Felix K. H. Chun, Carlo Terrone, Derya Tilki, Ottavio de Cobelli, Gennaro Musi, and Pierre I. Karakiewicz. Demographic and clinical characteristics of malignant solitary fibrous tumors: a seer database analysis. Cancers, 16:3331, Sep 2024. URL: https://doi.org/10.3390/cancers16193331, doi:10.3390/cancers16193331. This article has 12 citations.
-
(tolstrup2024riskfactorsfor pages 2-3): Johan Tolstrup, Anand Loya, Ninna Aggerholm-Pedersen, Louise Preisler, and Luit Penninga. Risk factors for recurrent disease after resection of solitary fibrous tumor: a systematic review. Frontiers in Surgery, Jan 2024. URL: https://doi.org/10.3389/fsurg.2024.1332421, doi:10.3389/fsurg.2024.1332421. This article has 21 citations.
-
(janik2023diagnosticsandtreatment media 2935871a): Anna Maria Janik, Anna Terlecka, Mateusz J. Spałek, Kjetil Boye, Bartłomiej Szostakowski, Paulina Chmiel, Anna Szumera-Ciećkiewicz, Klaudia Bobak, Tomasz Świtaj, Piotr Rutkowski, and Anna M. Czarnecka. Diagnostics and treatment of extrameningeal solitary fibrous tumors. Cancers, 15:5854, Dec 2023. URL: https://doi.org/10.3390/cancers15245854, doi:10.3390/cancers15245854. This article has 21 citations.
-
(janik2023diagnosticsandtreatment pages 13-14): Anna Maria Janik, Anna Terlecka, Mateusz J. Spałek, Kjetil Boye, Bartłomiej Szostakowski, Paulina Chmiel, Anna Szumera-Ciećkiewicz, Klaudia Bobak, Tomasz Świtaj, Piotr Rutkowski, and Anna M. Czarnecka. Diagnostics and treatment of extrameningeal solitary fibrous tumors. Cancers, 15:5854, Dec 2023. URL: https://doi.org/10.3390/cancers15245854, doi:10.3390/cancers15245854. This article has 21 citations.
-
(martinbroto2021acomprehensivereview pages 15-16): Javier Martin-Broto, Jose L. Mondaza-Hernandez, David S. Moura, and Nadia Hindi. A comprehensive review on solitary fibrous tumor: new insights for new horizons. Jun 2021. URL: https://doi.org/10.3390/cancers13122913, doi:10.3390/cancers13122913. This article has 87 citations.