1. Disease Information
1.1 Concise overview (current understanding)
Smith–Magenis syndrome is a complex neurodevelopmental disorder characterized by distinctive physical features, developmental delay/intellectual disability, and a characteristic behavioral phenotype that prominently includes sleep disturbance and self-injury. A recent clinical review describes SMS as “a complex genetic disorder characterized by distinctive physical features, developmental delay, cognitive impairment, and a typical behavioral phenotype” (Rinaldi et al., 2022; publication date 2022-02; URL https://doi.org/10.3390/genes13020335). (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2)
1.2 Key identifiers (from retrieved evidence)
- OMIM: #182290 (explicitly stated in Rinaldi et al., 2022). (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2)
- Orphanet (ORPHA), ICD-10/ICD-11, MeSH, MONDO: Not present in the retrieved text excerpts; not separately retrieved from those databases in this run. (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2, rinaldi2022smithmagenissyndrome—clinicalreview pages 2-4)
1.3 Synonyms / alternative names
Not comprehensively enumerated in the retrieved sources. In practice, “Smith–Magenis syndrome” and “SMS” are the dominant names used across clinical and research literature. (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2)
1.4 Evidence provenance
Most knowledge used here is from aggregated disease-level resources (clinical reviews, retrospective cohorts, patient registries, and ClinicalTrials.gov trial records), rather than EHR-derived single-patient records. (gouard2021smith‐magenissyndromeclinical pages 1-2, brennan2024speechlanguagehearing pages 1-2, NCT02231008 chunk 1)
2. Etiology
2.1 Disease causal factors
SMS is caused by RAI1 haploinsufficiency, most commonly via a 17p11.2 interstitial deletion and less commonly via pathogenic variants in RAI1.
Verbatim abstract-supported statement: Falco et al. (2017; publication date 2017-11; URL https://doi.org/10.2147/TACG.S128455) states: “SMS is caused by interstitial 17p11.2 deletions, encompassing multiple genes and including the retinoic acid-induced 1 gene (RAI1), or by mutations in RAI1 itself. About 10% of all the SMS patients, in fact, carry an RAI1 mutation responsible for the phenotype.” (falco2017rai1genemutations pages 1-2)
Rinaldi et al. (2022) similarly summarizes that SMS is caused by ~90% 17p11.2 deletions (including RAI1) and ~10% pathogenic RAI1 variants. (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2)
2.2 Risk factors
For a Mendelian genomic disorder such as SMS, “risk factors” are primarily genetic and relate to de novo mutational mechanisms generating recurrent CNVs at 17p11.2 (e.g., NAHR mediated by low-copy repeats). (poisson2015behavioraldisturbanceand pages 1-2, gouard2021smith‐magenissyndromeclinical pages 1-2)
2.3 Protective factors
No genetic or environmental protective factors were identified in the retrieved sources.
2.4 Gene–environment interactions
No specific GxE interactions were identified in the retrieved sources.
3. Phenotypes (with quantitative frequencies, onset, and HPO suggestions)
3.1 Key phenotype domains
SMS phenotypes span neurodevelopmental, behavioral/sleep, craniofacial, musculoskeletal, ENT/hearing, ophthalmologic, cardiovascular, gastrointestinal, and metabolic domains.
A large European retrospective cohort of 47 individuals with 17p11.2 deletions (Le Gouard/Gouard et al., 2021; publication date 2021-01; URL https://doi.org/10.1111/cge.13906) reported: ophthalmological problems 89%, scoliosis 43%, deafness 32%, obstipation/constipation 45%, epilepsy 2%, behavioral problems (temper tantrums/difficult behaviors) 84%, and night-time awakenings 86%. (gouard2021smith‐magenissyndromeclinical pages 1-2)
A 2024 international patient-registry analysis focused on speech/hearing (Brennan et al., 2024; publication date 2024-03; URL https://doi.org/10.1044/2023_JSLHR-23-00179) reported (n=82): hearing loss 35%, otitis media history 66%, and PE tube placement 62%. (brennan2024speechlanguagehearing pages 1-2)
3.2 Developmental timing (temporal development)
- Behavioral phenotype emergence: Gouard et al. (2021) notes characteristic behaviors emerging between 18–36 months; Falco et al. (2017) describes the neurobehavioral phenotype becoming recognizable “usually, from the second year of life.” (gouard2021smith‐magenissyndromeclinical pages 1-2, falco2017rai1genemutations pages 1-2)
- Speech milestones (registry): Brennan et al. (2024) reported mean age of first words 26 months (range 11–72), and that 79% began speaking words at/after 24 months and 92% combined words at/after 36 months. (brennan2024speechlanguagehearing pages 1-2, brennan2024speechlanguagehearing pages 4-6)
3.3 Quality of life / family impact
In the 47-person cohort, Gouard et al. (2021) reported a substantial social/family burden: “70% of parents had to adapt their working time,” supporting high caregiver impact. (gouard2021smith‐magenissyndromeclinical pages 1-2)
3.4 Suggested HPO terms (examples; not exhaustive)
Based on retrieved phenotypes: - Sleep disturbance / night awakenings: HP:0002360 (Sleep disturbance); HP:0002323 (Sleep fragmentation) - Self-injury / stereotypies: HP:0100716 (Self-injurious behavior); HP:0000733 (Stereotypy) - Intellectual disability / developmental delay: HP:0001249 (Intellectual disability); HP:0001263 (Global developmental delay) - Speech delay: HP:0000750 (Delayed speech and language development) - Hearing loss / otitis media: HP:0000365 (Hearing impairment); HP:0000388 (Otitis media) - Scoliosis: HP:0002650 (Scoliosis) - Constipation: HP:0002019 (Constipation) - Overweight/obesity: HP:0001513 (Obesity); HP:0004324 (Hyperphagia)
(Phenotype frequencies supporting these suggestions are documented in Gouard 2021 and Brennan 2024.) (gouard2021smith‐magenissyndromeclinical pages 1-2, brennan2024speechlanguagehearing pages 1-2)
4. Genetic / Molecular Information
4.1 Causal gene(s) and structural mechanism
- Key gene: RAI1 (retinoic acid-induced 1), a dosage-sensitive transcriptional regulator. (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2, falco2017rai1genemutations pages 1-2)
- Genetic classes:
- 17p11.2 deletion (majority of cases)
- Pathogenic sequence variants in RAI1 (minority)
4.2 Variant spectrum and chromosomal abnormalities
Gouard et al. (2021) reports that the 17p11.2 region contains multiple low-copy repeats, with a common NAHR-mediated deletion of ~3.7 Mb; ~30% can be atypical deletions (1.5–9 Mb), with a ~650 kb critical region including RAI1. (gouard2021smith‐magenissyndromeclinical pages 1-2)
4.3 Inheritance
SMS is generally autosomal dominant but usually de novo. - Gouard et al. (2021) notes recurrence risk from gonadal mosaicism <1%, rising to 3%–5% if a parent is mosaic. (gouard2021smith‐magenissyndromeclinical pages 1-2)
4.4 Modifier genes / epigenetics
No validated modifier genes or disease-specific epigenetic mechanisms were identified in the retrieved sources.
5. Environmental Information
No specific toxins, lifestyle, or infectious etiologies were identified as causal or triggering factors in the retrieved sources; SMS is primarily genetic. (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2, falco2017rai1genemutations pages 1-2)
6. Mechanism / Pathophysiology
6.1 Sleep/circadian mechanism (melatonin inversion)
A core mechanistic feature is circadian dysregulation with an inverted melatonin rhythm. - Poisson et al. (2015; publication date 2015-09; URL https://doi.org/10.1186/s13023-015-0330-x) describes sleep disturbance with “an inversion of the melatonin secretion cycle,” associated with excessive daytime sleepiness and nighttime agitation. (poisson2015behavioraldisturbanceand pages 1-2) - A mechanistic synthesis reports that the sleep phenotype “results in >90% of cases from an inverted circadian rhythm of melatonin,” observed in both RAI1 mutation and deletion cases, and measurable via urinary 6-sulfatoxymelatonin (aMT6s). (sciarrillo2018identificationofnovel pages 10-13)
Causal chain (simplified): RAI1 haploinsufficiency → altered regulation of circadian genes and melatonin timing → daytime sleepiness + nocturnal awakenings/agitation → downstream behavioral dysregulation and caregiver burden. (poisson2015behavioraldisturbanceand pages 1-2, sciarrillo2018identificationofnovel pages 10-13)
6.2 Obesity/hyperphagia mechanism (hypothalamic satiety circuitry)
Obesity and hyperphagic behaviors are common and often emerge later in childhood/adolescence. - Lazareva et al. (2024; publication date 2024-07; URL https://doi.org/10.1016/j.orcp.2024.07.001) notes that RAI1 haploinsufficiency affects feeding and satiety and that obesity in SMS is believed in part to involve proximal melanocortin (MC4R-related) pathway dysfunction. (lazareva2024investigationofsetmelanotide pages 1-3, lazareva2024investigationofsetmelanotide pages 3-4)
Causal chain (simplified): RAI1 haploinsufficiency → dysregulated hypothalamic satiety signaling (including reduced Pomc and reduced Bdnf expression in mouse models, as summarized) → hyperphagia/foraging behaviors → overweight/obesity and metabolic complications. (lazareva2024investigationofsetmelanotide pages 3-4)
6.3 Suggested GO biological process / cellular component terms (examples)
- GO:0007623 (circadian rhythm)
- GO:0042752 (regulation of circadian rhythm)
- GO:0002024 (regulation of heart rate) (for arrhythmia-related surveillance considerations summarized in reviews)
- GO:0007610 (behavior)
- GO:0008340 (determination of adult lifespan) not supported here; omitted.
Suggested cell types (Cell Ontology, examples): - CL:0000540 (neuron) - CL:0000700 (hypothalamic neuron)
Suggested anatomical structures (UBERON, examples): - UBERON:0000955 (brain) - UBERON:0001898 (hypothalamus) - UBERON:0002107 (liver) for metabolic sequelae (not directly quantified in retrieved texts)
7. Anatomical Structures Affected
Based on multi-system phenotype frequencies: - Nervous system/brain (neurodevelopmental disability, sleep/circadian dysregulation, behavioral phenotype). (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2, poisson2015behavioraldisturbanceand pages 1-2) - Ear/middle ear and auditory system (otitis media, hearing loss, PE tubes). (brennan2024speechlanguagehearing pages 1-2) - Eye (high prevalence of ophthalmologic problems in cohort). (gouard2021smith‐magenissyndromeclinical pages 1-2) - Spine/musculoskeletal system (scoliosis). (gouard2021smith‐magenissyndromeclinical pages 1-2) - Gastrointestinal tract (constipation/obstipation). (gouard2021smith‐magenissyndromeclinical pages 1-2) - Cardiovascular system (congenital heart defects in cohort). (gouard2021smith‐magenissyndromeclinical pages 1-2)
A visual cohort table summarizing multi-system features and frequencies is available from Gouard et al. (2021). (gouard2021smith‐magenissyndromeclinical media 051e48d8, gouard2021smith‐magenissyndromeclinical media ff7a4193, gouard2021smith‐magenissyndromeclinical media 1a70035f, gouard2021smith‐magenissyndromeclinical media 28a66c76)
8. Temporal Development
- Onset: Many features begin in infancy (hypotonia, feeding issues) with behavioral/sleep phenotype typically becoming recognizable in toddlerhood (“second year of life”). (falco2017rai1genemutations pages 1-2, gouard2021smith‐magenissyndromeclinical pages 1-2)
- Course: Lifelong neurodevelopmental disorder; sleep and behavioral problems often persist and require ongoing management. (poisson2015behavioraldisturbanceand pages 1-2, rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2)
9. Inheritance and Population
9.1 Epidemiology
Prevalence estimates repeatedly cited across sources range from ~1/15,000 to 1/25,000. (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2, falco2017rai1genemutations pages 1-2, gouard2021smith‐magenissyndromeclinical pages 1-2)
9.2 Inheritance, penetrance, expressivity
- Inheritance: autosomal dominant, most often de novo. (gouard2021smith‐magenissyndromeclinical pages 1-2, rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2)
- Penetrance/expressivity: quantitative penetrance estimates were not available in retrieved sources; expressivity is clearly variable (e.g., 10% normal IQ in one cohort), supporting variable expressivity. (gouard2021smith‐magenissyndromeclinical pages 1-2)
9.3 Demographics
Registry sample demographics reported predominantly White and US-based (which may reflect ascertainment and limits generalizability). (brennan2024speechlanguagehearing pages 3-4)
10. Diagnostics
10.1 Clinical recognition
Diagnosis can be delayed because early facial features may be subtle and behavioral features emerge later in childhood. (sciarrillo2018identificationofnovel pages 6-10)
10.2 Genetic testing (real-world implementation)
- First-line for suspected SMS typically includes chromosomal microarray/aCGH and/or targeted CNV assays (FISH, MLPA) for 17p11.2 deletion detection. (gouard2021smith‐magenissyndromeclinical pages 1-2, poisson2015behavioraldisturbanceand pages 1-2)
- If deletion testing is negative and suspicion remains, proceed to RAI1 sequence analysis. (poisson2015behavioraldisturbanceand pages 1-2)
10.3 Differential diagnosis
Differential diagnosis details were not comprehensively retrievable in the current document set (though reviews note overlap with other syndromic neurodevelopmental disorders). (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2)
11. Outcome / Prognosis
Quantitative survival/life expectancy statistics were not available in retrieved sources. Morbidity is substantial due to sleep disturbance, behavioral dysregulation, developmental disability, and multi-system medical issues (ENT, ophthalmologic, musculoskeletal, GI), with documented caregiver work impact. (gouard2021smith‐magenissyndromeclinical pages 1-2, poisson2015behavioraldisturbanceand pages 1-2)
12. Treatment
12.1 Sleep/circadian targeted approaches
A frequently discussed circadian-targeting strategy is morning beta-blocker plus evening melatonin. - Poisson et al. (2015) states sleep disturbances are linked to “an inversion of the melatonin secretion cycle” and that “the combined intake of beta-blockers in the morning and melatonin in the evening may radically alleviate the circadian rhythm problems.” (publication date 2015-09; URL https://doi.org/10.1186/s13023-015-0330-x) (poisson2015behavioraldisturbanceand pages 1-2) - A mechanistic synthesis summarizes small interventional evidence where acenbutolol suppressed daytime melatonin peaks and combined acenbutolol + controlled-release melatonin produced subjective improvement. (sciarrillo2018identificationofnovel pages 10-13)
MAXO suggestions (examples): - Melatonin supplementation: MAXO:0001039 (melatonin therapy) (term label may vary by version) - Beta-adrenergic antagonist therapy: MAXO:0000474 (beta-blocker therapy) - Light therapy: MAXO:0000560 (phototherapy/light therapy)
12.2 Targeted pharmacotherapy for obesity/hyperphagia (2024 development)
Setmelanotide (MC4R agonist) pilot trial: Lazareva et al. (2024; publication date 2024-07; URL https://doi.org/10.1016/j.orcp.2024.07.001) conducted an open-label pilot in SMS (n=12; 10 completed), reporting mean percent weight change −0.28% (P=0.66) and decreased self-reported hunger (p=0.011), concluding no significant weight reduction; adverse events were common (injection-site reactions, hyperpigmentation) without withdrawals/deaths attributed to AEs. (lazareva2024investigationofsetmelanotide pages 1-3)
MAXO suggestions (examples): - MC4R agonist therapy / anti-obesity pharmacotherapy: MAXO term depends on vocabulary version; annotate as anti-obesity pharmacotherapy and melanocortin pathway agonist treatment.
12.3 Clinical trials and real-world research infrastructure
Key ClinicalTrials.gov records retrieved include: - NCT02231008 (Vanda; tasimelteon vs placebo; double-blind randomized crossover; start Sep 2015, primary completion 2018-11-19, study completion Jan 2022; primary outcome improvement in sleep parameters over 9 weeks). No results were posted in the retrieved trial record excerpt. URL https://clinicaltrials.gov/study/NCT02231008 (NCT02231008 chunk 1) - NCT00506259 (NIH; light therapy + controlled-release melatonin; randomized crossover; completed; no posted results in retrieved excerpt). (NCT00506259 chunk 1) - NCT03154697 (Vanda; observational database of SMS and sleep disturbances; recruiting; last update posted 2024-03-20; URL https://clinicaltrials.gov/study/NCT03154697). (NCT03154697 chunk 1)
13. Prevention
Primary prevention is not generally applicable because most cases arise de novo; however, genetic counseling and prenatal diagnosis may be considered for families with a known pathogenic variant or mosaicism risk. Specific prevention guideline statements were not retrieved in the current corpus. (gouard2021smith‐magenissyndromeclinical pages 1-2)
14. Other Species / Natural Disease
No naturally occurring non-human SMS analogs were identified in the retrieved sources.
15. Model Organisms
Mouse models with Rai1 haploinsufficiency are used to study SMS-relevant obesity/hyperphagia mechanisms and hypothalamic satiety signaling disruptions, and to test candidate pathway interventions (e.g., BDNF signaling augmentation), as summarized in the context of human translational work. (lazareva2024investigationofsetmelanotide pages 3-4)
Recent developments and expert analysis (2023–2024 emphasis)
- 2024 registry-scale phenotyping: Brennan et al. (2024) provides updated, registry-based quantitative characterization of hearing/otopathology and communication milestones (n=82), supporting real-world care pathways including frequent PE tube placement and speech-language therapy. (brennan2024speechlanguagehearing pages 1-2)
- 2024 translational obesity pharmacotherapy test: Lazareva et al. (2024) tested MC4R agonism (setmelanotide) and found no significant weight loss, informing mechanistic interpretation that proximal MC4R dysfunction may not be the predominant driver of SMS obesity (despite some hunger improvement). (lazareva2024investigationofsetmelanotide pages 1-3)
- Ongoing industry-sponsored sleep trial infrastructure: Tasimelteon trial NCT02231008 is completed (2015–2022) but results were not available in the retrieved record excerpt, highlighting a key evidence gap for clinicians and knowledge-base builders relying on posted registry outcomes. (NCT02231008 chunk 1)
Evidence map (high-yield quantitative facts)
The following table compiles the most decision-relevant, quantitatively supported findings from the retrieved sources.
Table (click to expand)
| Domain | Specific finding | Evidence type | Primary source | PMID if known | URL | Citation ID |
|---|---|---|---|---|---|---|
| Identifiers | Smith–Magenis syndrome (SMS) is identified as OMIM #182290; defined as a complex genetic disorder with distinctive physical features, developmental delay, cognitive impairment, and a behavioral phenotype. | Review | Rinaldi 2022 Genes | https://doi.org/10.3390/genes13020335 | (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2) | |
| Genetics | SMS is caused in ~90% of cases by 17p11.2 deletions including RAI1, and in ~10% by pathogenic RAI1 variants; RAI1 is dosage-sensitive and acts as a transcriptional regulator. | Review | Rinaldi 2022 Genes | https://doi.org/10.3390/genes13020335 | (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2) | |
| Genetics | About 10% of SMS patients carry an RAI1 mutation; the recurrent ~3.7 Mb deletion is observed in about 70–80% of deleted patients. | Review | Falco 2017 Application of Clinical Genetics | https://doi.org/10.2147/TACG.S128455 | (falco2017rai1genemutations pages 1-2) | |
| Prevalence | Estimated prevalence/birth incidence is 1 in 15,000 to 1 in 25,000, with no sex predominance reported. | Review | Rinaldi 2022 Genes | https://doi.org/10.3390/genes13020335 | (rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2) | |
| Prevalence | Epidemiology estimates: prevalence 1/15,000 and birth incidence 1/25,000. | Review | Falco 2017 Application of Clinical Genetics | https://doi.org/10.2147/TACG.S128455 | (falco2017rai1genemutations pages 1-2) | |
| Genetics/Inheritance | Deletions or mutations are usually de novo; recurrence risk from parental gonadal mosaicism is <1%, rising to 3%–5% if a parent is mosaic for the deletion or an RAI1 variant. | Human cohort | Gouard 2021 Clinical Genetics | https://doi.org/10.1111/cge.13906 | (gouard2021smith‐magenissyndromeclinical pages 1-2) | |
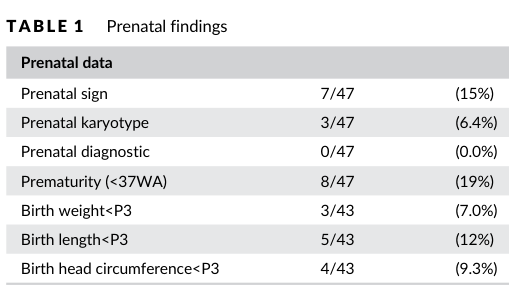
| Key phenotypes | In a 47-patient European cohort with 17p11.2 deletions: prenatal anomalies 15%, reduced fetal movements 50%, ophthalmologic problems 89%, scoliosis 43%, deafness 32%, obstipation 45%, epilepsy 2%, behavioral problems 84%, and night-time awakenings 86%. | Human cohort | Gouard 2021 Clinical Genetics | https://doi.org/10.1111/cge.13906 | (gouard2021smith‐magenissyndromeclinical pages 1-2) | |
| Key phenotypes | In the same cohort, among patients older than 10 years, >60% were overweight; heart defects included 6.5% tetralogy of Fallot and 6.5% pulmonary stenosis; all had learning difficulties, but 10% had IQ in the normal range. | Human cohort | Gouard 2021 Clinical Genetics | https://doi.org/10.1111/cge.13906 | (gouard2021smith‐magenissyndromeclinical pages 1-2) | |
| Temporal development | Clinical/behavioral phenotype often becomes recognizable between 18–36 months; maladaptive behaviors may start around 18 months, and the overall neurobehavioral phenotype is usually recognizable from the second year of life. | Human cohort/review | Gouard 2021 Clinical Genetics; Falco 2017 Application of Clinical Genetics | https://doi.org/10.1111/cge.13906 ; https://doi.org/10.2147/TACG.S128455 | (gouard2021smith‐magenissyndromeclinical pages 1-2, falco2017rai1genemutations pages 1-2) | |
| Registry findings | International SMS registry (n=82): 35% had hearing loss, 66% had otitis media history, and 62% had pressure-equalization (PE) tubes. | Registry | Brennan 2024 JSLHR | https://doi.org/10.1044/2023_JSLHR-23-00179 | (brennan2024speechlanguagehearing pages 1-2) | |
| Registry findings | In the same registry, 60% communicated using speech; 79% spoke first words at/after 24 months; 92% combined words at/after 36 months; 41% used sign language before speech. | Registry | Brennan 2024 JSLHR | https://doi.org/10.1044/2023_JSLHR-23-00179 | (brennan2024speechlanguagehearing pages 1-2) | |
| Registry findings | More detailed registry results: mean age at first PE tube placement 24 months (range 6–72), mean 3 tube sets (range 1–18), average age hearing loss first suspected 38 months (range 0–480), and mean age of first words 26 months (range 11–72). | Registry | Brennan 2024 JSLHR | https://doi.org/10.1044/2023_JSLHR-23-00179 | (brennan2024speechlanguagehearing pages 4-6) | |
| Registry findings | Age-group analyses showed significant associations between age group and hearing loss (p=.019), otitis media (p=.001), and PE tube history (p=.001). | Registry | Brennan 2024 JSLHR | https://doi.org/10.1044/2023_JSLHR-23-00179 | (brennan2024speechlanguagehearing pages 4-6) | |
| Sleep-circadian mechanism | Sleep disturbance is a hallmark with excessive daytime sleepiness and nighttime agitation, underpinned by inversion of the melatonin secretion cycle. | Review | Poisson 2015 Orphanet Journal of Rare Diseases | https://doi.org/10.1186/s13023-015-0330-x | (poisson2015behavioraldisturbanceand pages 1-2) | |
| Sleep-circadian mechanism | The sleep phenotype is reported to result in >90% of cases from an inverted circadian rhythm of melatonin; inversion was observed in both RAI1-mutated patients and those with the common SMS deletion. | Mechanistic review | Sciarrillo 2018 thesis/text | https://doi.org/10.13130/sciarrillo-maria_phd2018-02-19 | (sciarrillo2018identificationofnovel pages 10-13) | |
| Sleep-circadian mechanism | A 2024 study notes altered melatonin timing with an abnormal inverted circadian rhythm estimated in 95% of SMS individuals. | Human genomics study/reviewed background | Smieszek 2024 Egyptian Journal of Medical Human Genetics | https://doi.org/10.1186/s43042-024-00508-3 | (smieszek2024retinoicacidinduced1 pages 1-2) | |
| Treatments & trials | Combined morning beta-blocker and evening melatonin may “radically alleviate” circadian rhythm problems in SMS. | Review | Poisson 2015 Orphanet Journal of Rare Diseases | https://doi.org/10.1186/s13023-015-0330-x | (poisson2015behavioraldisturbanceand pages 1-2) | |
| Treatments & trials | A cited study reported oral β1-antagonist acenbutolol suppressed daytime melatonin peaks with subjective behavioral improvement; combined daytime acenbutolol + evening controlled-release melatonin also produced subjective behavioral improvement. | Human interventional evidence summarized in review | Sciarrillo 2018 thesis/text | https://doi.org/10.13130/sciarrillo-maria_phd2018-02-19 | (sciarrillo2018identificationofnovel pages 10-13) | |
| Treatments & trials | NCT02231008: completed Phase 2/3 double-blind randomized two-period crossover of tasimelteon vs placebo; 49 participants, start Sep 2015, primary completion 2018-11-19, study completion Jan 2022. Primary endpoint: improvement in sleep parameters over 9 weeks; results/statistics not posted in the retrieved record. | Clinical trial registry | ClinicalTrials.gov NCT02231008 | https://clinicaltrials.gov/study/NCT02231008 | (NCT02231008 chunk 1) | |
| Treatments & trials | NCT00506259: Phase 1 randomized crossover of bright light phototherapy and controlled-release melatonin in children with SMS; 23 enrolled; primary outcome was change in melatonin level, with secondary actigraphy/behavior outcomes; no numerical results available in the retrieved record. | Clinical trial registry | ClinicalTrials.gov NCT00506259 | https://clinicaltrials.gov/study/NCT00506259 | (NCT00506259 chunk 1) | |
| Treatments & trials | NCT00691574: pilot melatonin + bright-light study, non-randomized parallel design; actual enrollment 5, started 1998-09, completed 2009-05; terminated due to funding/extension issues, with no posted efficacy statistics in the retrieved record. | Clinical trial registry | ClinicalTrials.gov NCT00691574 | https://clinicaltrials.gov/study/NCT00691574 | (NCT00691574 chunk 1) | |
| Treatments & trials | NCT03492970: adult SMS melatonin characterization study, single-group, 10 adults, hourly plasma melatonin over 24 h plus ~2 weeks actimetry; completed 2019-03-30; no posted numerical results in the retrieved record. | Clinical trial registry | ClinicalTrials.gov NCT03492970 | https://clinicaltrials.gov/study/NCT03492970 | (NCT03492970 chunk 1) | |
| Obesity mechanism | SMS obesity is believed partly due to dysfunction of the proximal MC4R pathway; RAI1 haploinsufficiency affects feeding, satiety, and fat deposition. Most people with SMS have overweight/obesity, with 80% having BMI ≥85th percentile, and overeating/foraging often appears by adolescence. | Review + interventional study background | Lazareva 2024 Obesity Research & Clinical Practice | https://doi.org/10.1016/j.orcp.2024.07.001 | (lazareva2024investigationofsetmelanotide pages 1-3) | |
| Obesity mechanism | Mouse/mechanistic data summarized in Lazareva 2024: Rai1+/− mice show high circulating leptin and PYY, reduced hypothalamic satiety signaling, reduced Bdnf, and reduced Pomc expression, supporting upstream dysregulation of melanocortin satiety circuits. | Model/preclinical evidence summarized in human study | Lazareva 2024 Obesity Research & Clinical Practice; Javed 2022 Human Molecular Genetics | https://doi.org/10.1016/j.orcp.2024.07.001 ; https://doi.org/10.1093/hmg/ddab245 | (lazareva2024investigationofsetmelanotide pages 3-4, lazareva2024investigationofsetmelanotide pages 1-3) | |
| Treatments & trials | Open-label phase 2 setmelanotide pilot in SMS: 12 enrolled (ages 11–39), 10 completed; once-daily dosing titrated to 3 mg. Mean percent weight change was −0.28% (95% CI −2.1% to 1.5%; P=0.66), so no significant weight reduction. | Interventional trial | Lazareva 2024 Obesity Research & Clinical Practice | https://doi.org/10.1016/j.orcp.2024.07.001 | (lazareva2024investigationofsetmelanotide pages 1-3) | |
| Treatments & trials | In the same setmelanotide SMS pilot, self-reported hunger decreased (p=0.011); all participants had adverse events, most commonly injection-site reactions and skin hyperpigmentation, with no withdrawals or deaths due to adverse events. | Interventional trial | Lazareva 2024 Obesity Research & Clinical Practice | https://doi.org/10.1016/j.orcp.2024.07.001 | (lazareva2024investigationofsetmelanotide pages 1-3) | |
| Genetics/ASD overlap | In a 2024 WGS ASD cohort analysis, RAI1 rare missense variants were enriched in ASD (54/6080 ASD vs 6/2541 controls, p<0.002, OR 3.78), supporting overlap between SMS-related circadian phenotypes and ASD. | Human genomics study | Smieszek 2024 Egyptian Journal of Medical Human Genetics | https://doi.org/10.1186/s43042-024-00508-3 | (smieszek2024retinoicacidinduced1 pages 1-2) | |
| Diagnostics | Recommended testing summarized across cohort/review sources: peripheral blood FISH, CGH array/aCGH, and MLPA for 17p11.2 deletion detection; if negative despite clinical suspicion, proceed to RAI1 sequencing. | Review/human cohort | Poisson 2015 Orphanet Journal of Rare Diseases; Gouard 2021 Clinical Genetics | https://doi.org/10.1186/s13023-015-0330-x ; https://doi.org/10.1111/cge.13906 | (poisson2015behavioraldisturbanceand pages 1-2, gouard2021smith‐magenissyndromeclinical pages 1-2) |
Table: This table compiles the most decision-relevant, quantitatively supported findings on Smith–Magenis syndrome from the retrieved cohort studies, registry analyses, reviews, mechanistic summaries, and clinical trial records. It is useful as a high-yield evidence map for genetics, phenotypes, sleep-circadian biology, obesity, diagnostics, and treatment development.
Visual evidence (phenotype frequency tables)
Cropped table images from Gouard et al. (2021) summarizing prenatal findings and multi-system clinical characteristics/frequencies were retrieved. These can be used for manual extraction/verification of phenotype frequency details beyond the text excerpts. (gouard2021smith‐magenissyndromeclinical media 051e48d8, gouard2021smith‐magenissyndromeclinical media ff7a4193, gouard2021smith‐magenissyndromeclinical media 1a70035f, gouard2021smith‐magenissyndromeclinical media 28a66c76)
Key limitations of this report (data not retrieved in this run)
- ORPHA/ICD/MeSH/MONDO identifiers were not available in the retrieved excerpts and would require direct database lookups.
- PMIDs were not provided in the retrieved text snippets/metadata; therefore they could not be reliably attached here without additional database retrieval.
- Tasimelteon trial outcomes (NCT02231008) and several melatonin/light trials have no posted results in the retrieved ClinicalTrials.gov excerpts, limiting quantitative treatment-effect reporting.
- Detailed differential diagnosis, formal diagnostic criteria, and survival/life expectancy statistics were not present in the available sources.
References
-
(rinaldi2022smithmagenissyndrome—clinicalreview pages 1-2): Berardo Rinaldi, Roberta Villa, Alessandra Sironi, Livia Garavelli, Palma Finelli, and Maria Francesca Bedeschi. Smith-magenis syndrome—clinical review, biological background and related disorders. Genes, 13:335, Feb 2022. URL: https://doi.org/10.3390/genes13020335, doi:10.3390/genes13020335. This article has 78 citations.
-
(rinaldi2022smithmagenissyndrome—clinicalreview pages 2-4): Berardo Rinaldi, Roberta Villa, Alessandra Sironi, Livia Garavelli, Palma Finelli, and Maria Francesca Bedeschi. Smith-magenis syndrome—clinical review, biological background and related disorders. Genes, 13:335, Feb 2022. URL: https://doi.org/10.3390/genes13020335, doi:10.3390/genes13020335. This article has 78 citations.
-
(gouard2021smith‐magenissyndromeclinical pages 1-2): Nicolas Rive Le Gouard, Adeline Jacquinet, Lyse Ruaud, Hélène Deleersnyder, Faustine Ageorges, Jennifer Gallard, Didier Lacombe, Sylvie Odent, Myriam Mikaty, Sylvie Manouvrier‐Hanu, Jamal Ghoumid, David Geneviève, Natacha Lehman, Nicole Philip, Patrick Edery, Delphine Héron, Coralie Rastel, Sophie Chancenotte, Christel Thauvin‐Robinet, Laurence Faivre, Laurence Perrin, and Alain Verloes.
smith‐magenis syndrome: clinical and behavioral characteristics in a large retrospective cohort. Jan 2021. URL: https://doi.org/10.1111/cge.13906, doi:10.1111/cge.13906. This article has 37 citations and is from a peer-reviewed journal. -
(brennan2024speechlanguagehearing pages 1-2): Christine Brennan, Mara Louise Smith, Rachael R. Baiduc, and Liam O'Connor. Speech, language, hearing, and otopathology results from the international smith–magenis syndrome patient registry. Journal of Speech, Language, and Hearing Research, 67:917-938, Mar 2024. URL: https://doi.org/10.1044/2023_jslhr-23-00179, doi:10.1044/2023_jslhr-23-00179. This article has 4 citations and is from a highest quality peer-reviewed journal.
-
(NCT02231008 chunk 1): Evaluating the Effects of Tasimelteon vs Placebo on Sleep Disturbances in SMS. Vanda Pharmaceuticals. 2015. ClinicalTrials.gov Identifier: NCT02231008
-
(falco2017rai1genemutations pages 1-2): Mariateresa Falco, Sonia Amabile, and Fabio Acquaviva. Rai1 gene mutations: mechanisms of smith–magenis syndrome. The Application of Clinical Genetics, 10:85-94, Nov 2017. URL: https://doi.org/10.2147/tacg.s128455, doi:10.2147/tacg.s128455. This article has 86 citations.
-
(poisson2015behavioraldisturbanceand pages 1-2): Alice Poisson, Alain Nicolas, Pierre Cochat, Damien Sanlaville, Caroline Rigard, Hélène de Leersnyder, Patricia Franco, Vincent Des Portes, Patrick Edery, and Caroline Demily. Behavioral disturbance and treatment strategies in smith-magenis syndrome. Orphanet Journal of Rare Diseases, Sep 2015. URL: https://doi.org/10.1186/s13023-015-0330-x, doi:10.1186/s13023-015-0330-x. This article has 80 citations and is from a peer-reviewed journal.
-
(brennan2024speechlanguagehearing pages 4-6): Christine Brennan, Mara Louise Smith, Rachael R. Baiduc, and Liam O'Connor. Speech, language, hearing, and otopathology results from the international smith–magenis syndrome patient registry. Journal of Speech, Language, and Hearing Research, 67:917-938, Mar 2024. URL: https://doi.org/10.1044/2023_jslhr-23-00179, doi:10.1044/2023_jslhr-23-00179. This article has 4 citations and is from a highest quality peer-reviewed journal.
-
(sciarrillo2018identificationofnovel pages 10-13): MARIA SCIARRILLO. Identification of novel mechanisms for neurological conditions overlapping smith-magenis syndrome. Text, Feb 2018. URL: https://doi.org/10.13130/sciarrillo-maria_phd2018-02-19, doi:10.13130/sciarrillo-maria_phd2018-02-19. This article has 0 citations and is from a peer-reviewed journal.
-
(lazareva2024investigationofsetmelanotide pages 1-3): Julia Lazareva, Stephanie R. Sisley, Sheila M. Brady, Ann C.M. Smith, Sarah H. Elsea, Jeremy J. Pomeroy, Christian L. Roth, Jennifer E. Sprague, Martin Wabitsch, Jill Garrison, and Jack A. Yanovski. Investigation of setmelanotide, an mc4r agonist, for obesity in individuals with smith-magenis syndrome. Obesity research & clinical practice, 18:301-307, Jul 2024. URL: https://doi.org/10.1016/j.orcp.2024.07.001, doi:10.1016/j.orcp.2024.07.001. This article has 13 citations and is from a peer-reviewed journal.
-
(lazareva2024investigationofsetmelanotide pages 3-4): Julia Lazareva, Stephanie R. Sisley, Sheila M. Brady, Ann C.M. Smith, Sarah H. Elsea, Jeremy J. Pomeroy, Christian L. Roth, Jennifer E. Sprague, Martin Wabitsch, Jill Garrison, and Jack A. Yanovski. Investigation of setmelanotide, an mc4r agonist, for obesity in individuals with smith-magenis syndrome. Obesity research & clinical practice, 18:301-307, Jul 2024. URL: https://doi.org/10.1016/j.orcp.2024.07.001, doi:10.1016/j.orcp.2024.07.001. This article has 13 citations and is from a peer-reviewed journal.
-
(gouard2021smith‐magenissyndromeclinical media 051e48d8): Nicolas Rive Le Gouard, Adeline Jacquinet, Lyse Ruaud, Hélène Deleersnyder, Faustine Ageorges, Jennifer Gallard, Didier Lacombe, Sylvie Odent, Myriam Mikaty, Sylvie Manouvrier‐Hanu, Jamal Ghoumid, David Geneviève, Natacha Lehman, Nicole Philip, Patrick Edery, Delphine Héron, Coralie Rastel, Sophie Chancenotte, Christel Thauvin‐Robinet, Laurence Faivre, Laurence Perrin, and Alain Verloes.
smith‐magenis syndrome: clinical and behavioral characteristics in a large retrospective cohort. Jan 2021. URL: https://doi.org/10.1111/cge.13906, doi:10.1111/cge.13906. This article has 37 citations and is from a peer-reviewed journal. -
(gouard2021smith‐magenissyndromeclinical media ff7a4193): Nicolas Rive Le Gouard, Adeline Jacquinet, Lyse Ruaud, Hélène Deleersnyder, Faustine Ageorges, Jennifer Gallard, Didier Lacombe, Sylvie Odent, Myriam Mikaty, Sylvie Manouvrier‐Hanu, Jamal Ghoumid, David Geneviève, Natacha Lehman, Nicole Philip, Patrick Edery, Delphine Héron, Coralie Rastel, Sophie Chancenotte, Christel Thauvin‐Robinet, Laurence Faivre, Laurence Perrin, and Alain Verloes.
smith‐magenis syndrome: clinical and behavioral characteristics in a large retrospective cohort. Jan 2021. URL: https://doi.org/10.1111/cge.13906, doi:10.1111/cge.13906. This article has 37 citations and is from a peer-reviewed journal. -
(gouard2021smith‐magenissyndromeclinical media 1a70035f): Nicolas Rive Le Gouard, Adeline Jacquinet, Lyse Ruaud, Hélène Deleersnyder, Faustine Ageorges, Jennifer Gallard, Didier Lacombe, Sylvie Odent, Myriam Mikaty, Sylvie Manouvrier‐Hanu, Jamal Ghoumid, David Geneviève, Natacha Lehman, Nicole Philip, Patrick Edery, Delphine Héron, Coralie Rastel, Sophie Chancenotte, Christel Thauvin‐Robinet, Laurence Faivre, Laurence Perrin, and Alain Verloes.
smith‐magenis syndrome: clinical and behavioral characteristics in a large retrospective cohort. Jan 2021. URL: https://doi.org/10.1111/cge.13906, doi:10.1111/cge.13906. This article has 37 citations and is from a peer-reviewed journal. -
(gouard2021smith‐magenissyndromeclinical media 28a66c76): Nicolas Rive Le Gouard, Adeline Jacquinet, Lyse Ruaud, Hélène Deleersnyder, Faustine Ageorges, Jennifer Gallard, Didier Lacombe, Sylvie Odent, Myriam Mikaty, Sylvie Manouvrier‐Hanu, Jamal Ghoumid, David Geneviève, Natacha Lehman, Nicole Philip, Patrick Edery, Delphine Héron, Coralie Rastel, Sophie Chancenotte, Christel Thauvin‐Robinet, Laurence Faivre, Laurence Perrin, and Alain Verloes.
smith‐magenis syndrome: clinical and behavioral characteristics in a large retrospective cohort. Jan 2021. URL: https://doi.org/10.1111/cge.13906, doi:10.1111/cge.13906. This article has 37 citations and is from a peer-reviewed journal. -
(brennan2024speechlanguagehearing pages 3-4): Christine Brennan, Mara Louise Smith, Rachael R. Baiduc, and Liam O'Connor. Speech, language, hearing, and otopathology results from the international smith–magenis syndrome patient registry. Journal of Speech, Language, and Hearing Research, 67:917-938, Mar 2024. URL: https://doi.org/10.1044/2023_jslhr-23-00179, doi:10.1044/2023_jslhr-23-00179. This article has 4 citations and is from a highest quality peer-reviewed journal.
-
(sciarrillo2018identificationofnovel pages 6-10): MARIA SCIARRILLO. Identification of novel mechanisms for neurological conditions overlapping smith-magenis syndrome. Text, Feb 2018. URL: https://doi.org/10.13130/sciarrillo-maria_phd2018-02-19, doi:10.13130/sciarrillo-maria_phd2018-02-19. This article has 0 citations and is from a peer-reviewed journal.
-
(NCT00506259 chunk 1): Treatment Strategies for Children With Smith-Magenis Syndrome. National Human Genome Research Institute (NHGRI). 2007. ClinicalTrials.gov Identifier: NCT00506259
-
(NCT03154697 chunk 1): Development of Clinical Database of Individuals With Smith-Magenis Syndrome and Sleep Disturbances. Vanda Pharmaceuticals. 2016. ClinicalTrials.gov Identifier: NCT03154697
-
(smieszek2024retinoicacidinduced1 pages 1-2): Sandra Paulina Smieszek. Retinoic acid-induced 1 gene variants associated with smith–magenis syndrome circadian phenotypes enriched in autism spectrum disorder: whole-genome sequencing study. Egyptian Journal of Medical Human Genetics, May 2024. URL: https://doi.org/10.1186/s43042-024-00508-3, doi:10.1186/s43042-024-00508-3. This article has 0 citations and is from a peer-reviewed journal.
-
(NCT00691574 chunk 1): Melatonin Levels in Smith Magenis Syndrome (SMS). Oregon Health and Science University. 1998. ClinicalTrials.gov Identifier: NCT00691574
-
(NCT03492970 chunk 1): Melatonin in Adults With SMS. Hôpital le Vinatier. 2018. ClinicalTrials.gov Identifier: NCT03492970