1. Disease Information
1.1 Overview / definition (current understanding)
“Sarcoma of cervix uteri” is best treated as an umbrella disease concept covering multiple histologic and increasingly molecularly defined malignant mesenchymal tumors that arise primarily in the uterine cervix (rather than spreading from other sites). Contemporary reports emphasize that cervical sarcomas are very rare and their management often relies on small series/case reports and extrapolation from uterine/soft-tissue sarcoma practice (altmann2024fertilitysparingstrategyin pages 1-3, ghirardi2019roleofsurgery pages 9-10).
1.2 Common synonyms / alternative names
- Cervical sarcoma
- Primary sarcoma of the cervix uteri (altmann2024fertilitysparingstrategyin pages 1-3)
- Subtype-specific names are frequently used in practice (e.g., cervical embryonal rhabdomyosarcoma, cervical leiomyosarcoma, NTRK-rearranged spindle cell sarcoma, extraosseous Ewing sarcoma of cervix, COL1A1–PDGFB fusion uterine/cervical sarcoma) (yu2024clinicopathologiccharacteristicstreatment pages 1-2, szalai2024ntrkrearrangedspindlecell pages 1-3, xiao2024primaryewing’ssarcoma pages 1-2, lu2023casereporta pages 6-7).
1.3 Data provenance
Most cervix-sarcoma knowledge is derived from aggregated disease-level resources (guidelines for uterine sarcoma) plus individual case reports/series for cervix-specific entities (raycoquard2024esgoeuracangcigguidelinesfor pages 2-3, yu2024clinicopathologiccharacteristicstreatment pages 1-2, xiao2024primaryewing’ssarcoma pages 1-2).
2. Etiology
2.1 Disease causal factors
Cervical sarcomas are heterogeneous and include: - Fusion-driven sarcomas (e.g., NTRK fusions, COL1A1–PDGFB) (szalai2024ntrkrearrangedspindlecell pages 1-3, lu2023casereporta pages 6-7) - Oncogenic translocation-driven small round cell tumors (e.g., EWSR1–FLI1 in Ewing sarcoma) (xiao2024primaryewing’ssarcoma pages 1-2) - Predisposition-associated tumors (e.g., DICER1-associated cervical sarcoma, and literature linking DICER1 with cervical embryonal rhabdomyosarcoma) (altmann2024fertilitysparingstrategyin pages 1-3, yu2024clinicopathologiccharacteristicstreatment pages 1-2)
2.2 Risk factors
Evidence is limited for cervix-sarcoma-specific environmental risks. However, mechanistic “risk factors” in the sense of tumor-initiating genomic events are well described: - NTRK rearrangement defining an emerging subset of uterine/cervical sarcomas (szalai2024ntrkrearrangedspindlecell pages 1-3) - COL1A1–PDGFB fusion activating PDGFB/PDGFR signaling (lu2023casereporta pages 1-2) - DICER1 mutation in a reported cervical sarcoma case and a proposed DICER1-sarcoma entity (altmann2024fertilitysparingstrategyin pages 1-3)
2.3 Protective factors / GxE
No cervix-sarcoma-specific protective factors or gene–environment interactions were identified in the retrieved corpus.
3. Phenotypes (clinical presentation)
3.1 Common presenting phenotypes (with suggested HPO terms)
Cervical sarcomas frequently present with bleeding and/or a cervical mass/polypoid lesion across subtypes: - Irregular vaginal bleeding (HPO: Abnormal uterine bleeding HP:0100602; Postcoital bleeding HP:0030828) is common in DICER1-associated cervical sarcoma and other subtypes (altmann2024fertilitysparingstrategyin pages 1-3, xiao2024primaryewing’ssarcoma pages 1-2). - Vaginal tissue prolapse / polypoid mass (HPO: Pelvic organ prolapse HP:0000139 as a proxy; Vaginal mass HP:0030448 as a proxy) is prominent in cervical rhabdomyosarcoma series (yu2024clinicopathologiccharacteristicstreatment pages 1-2). - Abdominal/pelvic pain (HPO: Abdominal pain HP:0002027) and urinary frequency (HPO: HP:0000018) were reported in cervical rhabdomyosarcoma series (yu2024clinicopathologiccharacteristicstreatment pages 1-2).
3.2 Age of onset / severity / progression
- Cervical rhabdomyosarcoma clustered in adolescents/young women in a 12-patient institutional series (15–50 years; median 17) (yu2024clinicopathologiccharacteristicstreatment pages 1-2).
- DICER1-associated cervical sarcoma was reported in an 18-year-old (altmann2024fertilitysparingstrategyin pages 1-3).
- NTRK-rearranged cervix sarcomas often occur in premenopausal/perimenopausal women (example age 43 in a NUMA1::NTRK1 case) (szalai2024ntrkrearrangedspindlecell pages 1-3).
3.3 Quality of life impact
Direct QoL measures were not retrieved. Indirectly, heavy bleeding, prolapse/mass effect, radical surgery, and multi-agent chemotherapy imply substantial functional and reproductive impact (yu2024clinicopathologiccharacteristicstreatment pages 1-2, altmann2024fertilitysparingstrategyin pages 1-3).
4. Genetic / Molecular Information
4.1 Key actionable or defining alterations (recent 2023–2024 emphasis)
A) NTRK-rearranged spindle cell sarcoma/neoplasm of uterine cervix
- Defined by NTRK gene rearrangements leading to constitutive Trk activation (szalai2024ntrkrearrangedspindlecell pages 1-3).
- A 2024 cervix case reported a novel NUMA1::NTRK1 fusion detected by NGS; the fusion protein is “predicted to cause constant activation” of the NTRK1 kinase domain (szalai2024ntrkrearrangedspindlecell pages 1-3).
- Diagnostic theme: strong/diffuse pan-TRK and CD34 positivity (szalai2024ntrkrearrangedspindlecell pages 1-3, feng2025ntrkrearrangedspindlecell pages 1-2).
B) COL1A1–PDGFB fusion uterine/cervical sarcoma
- COL1A1–PDGFB fusion produces an oncogenic chimeric transcript activating PDGFB/PDGFR signaling (lu2023casereporta pages 1-2).
- The report stresses that “early precise diagnosis may allow patients to benefit from the targeted therapy imatinib” (PDGFR inhibitor activity) (lu2023casereporta pages 1-2).
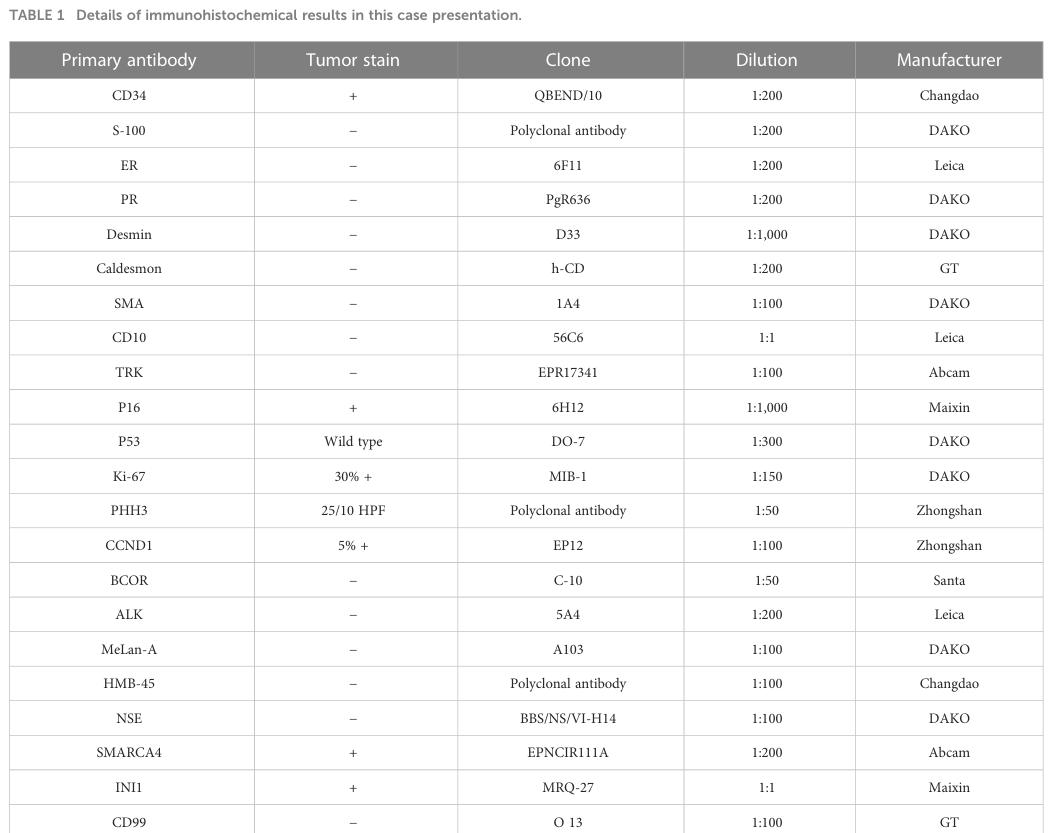
- Table evidence on immunophenotype and compiled cases is available in the retrieved table images (lu2023casereporta media bf56b6c0, lu2023casereporta media 92e7e479).
C) Extraosseous Ewing sarcoma of cervix
- Hallmark: EWSR1–FLI1 fusion; the review notes the EWS/FLI fusion occurs in ~85% of ESFT with ~15% other EWS–ETS fusions (xiao2024primaryewing’ssarcoma pages 1-2).
D) DICER1-associated cervical sarcoma
- A 2024 fertility-sparing case report describes a DICER1 mutation-associated sarcoma of the cervix and notes literature “hints towards a distinct DICER-1 sarcoma entity” (altmann2024fertilitysparingstrategyin pages 1-3).
4.2 Variant types / somatic vs germline
- NTRK rearrangements and EWSR1 rearrangements are reported as tumor (somatic) fusions identified by FISH/NGS/RNA sequencing (szalai2024ntrkrearrangedspindlecell pages 1-3, xiao2024primaryewing’ssarcoma pages 1-2).
- DICER1 alterations may be germline or somatic depending on context; in the retrieved cervix-sarcoma case, a DICER1 mutation was reported but the excerpt does not establish germline vs somatic status (altmann2024fertilitysparingstrategyin pages 1-3).
4.3 Epigenetics / modifier genes
Not specifically reported for cervix sarcoma in the retrieved evidence.
5. Environmental Information
No cervix-sarcoma-specific environmental, lifestyle, or infectious causal agents were identified in the retrieved corpus.
6. Mechanism / Pathophysiology
Cervical sarcomas reflect distinct oncogenic mechanisms by subtype:
6.1 Fusion-kinase driven signaling (upstream driver)
- NTRK fusions: NTRK rearrangement is the defining lesion, leading to Trk receptor overexpression/activation and potential sensitivity to selective TRK inhibitors (szalai2024ntrkrearrangedspindlecell pages 1-3, feng2025ntrkrearrangedspindlecell pages 1-2).
- Suggested GO biological process terms: protein tyrosine kinase signaling pathway (GO:0007169); cell proliferation (GO:0008283).
-
Suggested CL cell types (contextual): mesenchymal cell (CL:0000134); fibroblast (CL:0000057) (approximate, given fibrosarcoma-like morphology) (szalai2024ntrkrearrangedspindlecell pages 1-3).
-
COL1A1–PDGFB: fusion activates PDGFB signaling; conceptually upstream driver is ligand-driven PDGFR pathway activation (lu2023casereporta pages 1-2).
- Suggested GO terms: platelet-derived growth factor receptor signaling pathway (GO:0048008); positive regulation of cell migration (GO:0030335).
6.2 Transcriptional-program driven oncogenesis
- EWSR1–FLI1 fusion acts as a driver in Ewing sarcoma; diagnosis depends on demonstrating EWSR1 disruption and the EWSR1–FLI1 fusion (xiao2024primaryewing’ssarcoma pages 1-2).
6.3 miRNA processing pathway disruption
- DICER1-associated sarcoma: DICER1 mutation is consistent with disrupted miRNA biogenesis; the case report points to a potentially distinct DICER1-sarcoma entity (altmann2024fertilitysparingstrategyin pages 1-3).
7. Anatomical Structures Affected
7.1 Primary anatomic site
- Uterine cervix (UBERON:0000002 uterus; UBERON:0000003 cervix uteri—verify exact UBERON ID for cervix uteri in implementation). Primary tumors may extend into vagina or uterine cavity depending on subtype and growth pattern (lu2023casereporta pages 1-2, yu2024clinicopathologiccharacteristicstreatment pages 1-2).
7.2 Tissue/cell level
- Predominantly stromal/mesenchymal tissue of the cervix; subtype-dependent differentiation (smooth muscle in leiomyosarcoma; skeletal muscle differentiation in rhabdomyosarcoma; fibrosarcoma-like spindle cell tumors in NTRK-rearranged neoplasms) (ghirardi2019roleofsurgery pages 9-10, yu2024clinicopathologiccharacteristicstreatment pages 1-2, szalai2024ntrkrearrangedspindlecell pages 1-3).
8. Temporal Development
8.1 Onset and course
- Often subacute presentation with bleeding/mass.
- Course ranges from relatively favorable outcomes in some series (e.g., cervical RMS series) to aggressive recurrence in fusion-driven spindle cell sarcoma cases (yu2024clinicopathologiccharacteristicstreatment pages 1-2, szalai2024ntrkrearrangedspindlecell pages 1-3).
9. Inheritance and Population
9.1 Epidemiology (key statistics)
- A 2024 cervical DICER1-associated sarcoma report states: “Primary sarcomas of the cervix are very rare” and estimates they account for ~1.3% of cervical tumors (altmann2024fertilitysparingstrategyin pages 1-3).
- A 2024 institutional cervical rhabdomyosarcoma series states: “Only 0.5% of primary RMSs are located in the cervix” (yu2024clinicopathologiccharacteristicstreatment pages 1-2).
- For uterine sarcomas overall, GEIS guidelines cite incidence 0.36–0.64 per 100,000 (perezfidalgo2023uterinesarcomasclinical pages 1-1) and a uterine sarcoma guideline cites ~1.5–3 per 100,000 (denschlag2022sarcomaofthe pages 3-4). These values are not cervix-specific but contextualize rarity.
9.2 Population demographics
- Cervical RMS: ages 15–50, median 17 in one 12-case series (yu2024clinicopathologiccharacteristicstreatment pages 1-2).
- NTRK-rearranged cervix sarcoma: example patient age 43 in a 2024 case report (szalai2024ntrkrearrangedspindlecell pages 1-3).
10. Diagnostics
10.1 Core diagnostic workflow (cross-cutting principles)
Guidelines for uterine sarcoma emphasize diagnostic uncertainty and recommend imaging plus careful pathology, often requiring resection specimen for definitive diagnosis: - Pelvic ultrasound and MRI are recommended as first-line imaging approaches in uterine sarcoma diagnostic pathways (perezfidalgo2023uterinesarcomasclinical pages 1-1, perezfidalgo2023uterinesarcomasclinical pages 1-3). - Biopsy may have low sensitivity, and diagnosis is often established after surgical specimen analysis (perezfidalgo2023uterinesarcomasclinical pages 1-1, perezfidalgo2023uterinesarcomasclinical pages 1-3).
10.2 Histopathology + immunohistochemistry + molecular confirmation
Modern cervical sarcoma diagnosis increasingly requires molecular confirmation: - COL1A1–PDGFB fusion cervix/uterine sarcoma report: “confirmatory FISH or gene sequencing is mandatory in cases that are hard to identify” (lu2023casereporta pages 6-7). The retrieved tables summarize IHC and molecular detection across cases (lu2023casereporta media bf56b6c0, lu2023casereporta media 92e7e479). - NTRK-rearranged cervix spindle cell sarcoma: strong pan-TRK IHC and NGS-defined fusion; authors highlight importance of accurate diagnosis given targeted options (szalai2024ntrkrearrangedspindlecell pages 1-3). - Ewing sarcoma cervix: IHC (CD99, NKX2.2, FLI1), FISH for EWSR1 disruption, and NGS for EWSR1–FLI1 are central (xiao2024primaryewing’ssarcoma pages 1-2).
10.3 Suggested biomarkers / markers (examples)
- NTRK rearranged: pan-TRK positive, CD34 positive (szalai2024ntrkrearrangedspindlecell pages 1-3, feng2025ntrkrearrangedspindlecell pages 1-2).
- Ewing: CD99, NKX2.2, FLI1 positive; EWSR1 rearrangement/fusion (xiao2024primaryewing’ssarcoma pages 1-2).
- DICER1-associated sarcoma case: Ki-67 90% reported; IHC profile described (altmann2024fertilitysparingstrategyin pages 1-3).
10.4 Differential diagnosis
- Cervical leiomyosarcoma review notes reliance on sarcoma criteria (size, infiltrative margins, mitoses, atypia) and emphasizes smooth muscle marker profiling for differential diagnosis (ghirardi2019roleofsurgery pages 9-10).
11. Outcome / Prognosis
11.1 Reported outcomes (recent series/cases)
- Cervical rhabdomyosarcoma (12-case series): among 11 with follow-up, 10 were tumor-free (90.9%); median survival 91 months; fertility-sparing subgroup had 1/4 pregnancy (25%) (yu2024clinicopathologiccharacteristicstreatment pages 1-2).
- Ewing sarcoma cervix (case): disease-free at 1 year after surgery + adjuvant chemotherapy (xiao2024primaryewing’ssarcoma pages 1-2).
- NTRK-rearranged cervix spindle cell sarcoma (case): early recurrence with progression after adriamycin and radiotherapy reported in one case (szalai2024ntrkrearrangedspindlecell pages 1-3).
11.2 Prognostic factors (high-level)
- Tumor subtype and grade are critical; uterine sarcoma guidelines emphasize histologic grade as influential on behavior and prognosis (perezfidalgo2023uterinesarcomasclinical pages 1-1).
12. Treatment
12.1 Current applications / real-world implementation
Because of rarity, treatment is largely multimodal and individualized, ideally in specialized centers.
Cross-cutting expert/guideline principles
ESGO/EURACAN/GCIG uterine sarcoma guidelines emphasize: - Centralization of care and multidisciplinary tumor boards - Use of molecular tests (FISH, DNA sequencing, RNA sequencing) with histology/IHC to refine classification and identify therapeutic targets - Encouragement of clinical trial enrollment and prospective registries (raycoquard2024esgoeuracangcigguidelinesfor pages 2-3).
Surgical management
- Cervical leiomyosarcoma review: “complete surgical excision with negative margins is considered to be the primary treatment” and lymphadenectomy has limited role due to low lymphatic spread (ghirardi2019roleofsurgery pages 9-10).
- Cervical RMS series: radical or conservative resection (fertility-sparing) plus chemotherapy; age and reproductive intent are central (yu2024clinicopathologiccharacteristicstreatment pages 1-2).
Chemotherapy / radiotherapy
- Ewing sarcoma cervix case used hysterectomy-based surgery with multi-agent chemotherapy; radiotherapy is part of multimodal paradigms (xiao2024primaryewing’ssarcoma pages 1-2).
- NTRK-rearranged cervix sarcoma case progressed after adriamycin and radiotherapy, highlighting the need for targeted options when actionable fusions are present (szalai2024ntrkrearrangedspindlecell pages 1-3).
Targeted therapy
- TRK inhibitors (precision oncology): NTRK-rearranged uterine/cervical sarcomas are emphasized as therapeutically important because NTRK fusion “is indicative of treatment response with a selective small-molecule inhibitor of the Trk kinases” (szalai2024ntrkrearrangedspindlecell pages 1-3).
- Imatinib (PDGFR pathway): COL1A1–PDGFB fusion uterine sarcoma report notes imatinib use with a radiographic response (22.4 cm to 6.5 cm) before progression at 14 months in an imatinib-treated case from the literature (lu2023casereporta pages 6-7).
12.2 MAXO term suggestions (examples)
- Surgical resection / hysterectomy: MAXO:0000610 (surgical procedure—placeholder; verify exact MAXO mapping)
- Chemotherapy: MAXO:0000058
- Radiotherapy: MAXO:0000127
- Targeted therapy (TRK inhibitor / imatinib): MAXO:0000747 (pharmacotherapy/targeted therapy—verify)
13. Prevention
No cervix-sarcoma-specific primary prevention strategies were identified. Secondary prevention is not established due to rarity; early evaluation of symptomatic bleeding/masses and avoidance of morcellation in suspected sarcoma contexts are relevant general principles (perezfidalgo2023uterinesarcomasclinical pages 1-3, lu2023casereporta pages 6-7).
14. Other Species / Natural Disease
No evidence retrieved.
15. Model Organisms
No disease-specific animal models were retrieved in the current corpus.
Summary Table (cross-subtype comparison)
The table below summarizes key subtypes, molecular features, diagnostics, and outcomes captured in the retrieved evidence.
Table (click to expand)
| Entity / subtype | Typical presentation | Key molecular alteration(s) | Key diagnostic tests / IHC | Typical management approaches | Key quantitative / epidemiologic / prognostic data |
|---|---|---|---|---|---|
| Cervical rhabdomyosarcoma (mostly embryonal; rare pleomorphic) | Often adolescents/young women; vaginal bleeding, vaginal tissue prolapse, abdominal pain/urinary frequency; can mimic a cervical polyp (yu2024clinicopathologiccharacteristicstreatment pages 1-2) | DICER1 association reported in cervical ERMS; pathogenic DICER1 variation noted in literature/case reports (altmann2024fertilitysparingstrategyin pages 1-3) | MRI/CT/B-ultrasound used but nonspecific; RMS-marker IHC supportive of diagnosis (yu2024clinicopathologiccharacteristicstreatment pages 1-2) | Radical surgery or fertility-sparing conservative resection plus chemotherapy; management should be age- and fertility-tailored (yu2024clinicopathologiccharacteristicstreatment pages 1-2) | “Only 0.5% of primary RMSs are located in the cervix”; 12-case series age 15–50 years, median 17; 10/11 followed patients tumor-free (90.9%); median survival 91 months; 1/4 fertility-sparing patients conceived (25%) (yu2024clinicopathologiccharacteristicstreatment pages 1-2) |
| DICER1-associated cervical sarcoma | Irregular vaginal bleeding; exophytic cervical tumor in an 18-year-old (altmann2024fertilitysparingstrategyin pages 1-3) | DICER1 mutation; proposed distinct DICER1 sarcoma entity (altmann2024fertilitysparingstrategyin pages 1-3) | Histology with high mitotic activity; IHC: CD56+, calponin+, p53 wildtype, weak panCK <5%; CD34-, S100-, SMA-, desmin-, MyoD1-, caldesmon-, ER-, PR- (altmann2024fertilitysparingstrategyin pages 1-3) | Fertility preservation discussion, oocyte cryopreservation, local resection, doxorubicin + ifosfamide; radiation avoided to preserve fertility in reported case (altmann2024fertilitysparingstrategyin pages 1-3) | Primary cervical sarcomas estimated at ~1.3% of cervical tumors; carcinosarcoma ~50%, leiomyosarcoma/adenosarcoma next, remaining ~9% heterogeneous group; reported tumor 8.5 × 7 × 2.5 cm, Ki-67 90%, up to 15 mitoses/HPF; patient tumor-free at last follow-up (altmann2024fertilitysparingstrategyin pages 1-3) |
| Extraosseous Ewing sarcoma of the cervix | Vaginal bleeding with cervical mass; usually small round blue cell tumor presentation (xiao2024primaryewing’ssarcoma pages 1-2) | EWSR1–FLI1 fusion in most ES; case confirmed EWSR1–FLI1; EWS/FLI occurs in ~85% and other EWS–ETS fusions in ~15% of ESFT (xiao2024primaryewing’ssarcoma pages 1-2) | H&E small round blue cells; IHC positive CD99, NKX2.2, FLI1; FISH showing EWSR1 disruption; NGS confirming fusion; MRI and FDG-PET used (xiao2024primaryewing’ssarcoma pages 1-2) | Multimodal treatment: hysterectomy-based surgery plus adjuvant/induction chemotherapy, sometimes radiotherapy following ES paradigms (xiao2024primaryewing’ssarcoma pages 1-2) | ES is mostly osseous, with “only about 20% occurring outside the bone”; reported cervical tumor 2.5 × 2.1 × 1.8 cm; disease-free at 1 year in case report (xiao2024primaryewing’ssarcoma pages 1-2) |
| NTRK-rearranged spindle cell sarcoma / neoplasm of uterine cervix | Often pre/perimenopausal women with abnormal bleeding/menorrhagia or cervical polypoid mass; fibrosarcoma-like spindle cell tumor with cervical predilection (szalai2024ntrkrearrangedspindlecell pages 1-3, feng2025ntrkrearrangedspindlecell pages 1-2) | Recurrent NTRK fusions including TPM3::NTRK1, TFG-NTRK3, NUMA1::NTRK1; NTRK rearrangement drives constitutive Trk activation (szalai2024ntrkrearrangedspindlecell pages 1-3, feng2025ntrkrearrangedspindlecell pages 1-2) | Pan-TRK and CD34 usually diffuse positive; S100 may be negative in some cases; FISH and RNA/targeted NGS are emphasized as confirmatory tests (szalai2024ntrkrearrangedspindlecell pages 1-3, feng2025ntrkrearrangedspindlecell pages 1-2, lu2023casereporta pages 6-7) | Surgery is the initial treatment of choice; TRK inhibitors are important targeted options for recurrent/metastatic disease, and selective Trk inhibitors are specifically highlighted (szalai2024ntrkrearrangedspindlecell pages 1-3, feng2025ntrkrearrangedspindlecell pages 1-2) | Literature estimates vary: “less than 50” uterine NTRK-rearranged sarcomas described in one 2024 report; another review summarized 61 female-genital-tract cases (54 cervix, 7 corpus), mean age 39 years, mean tumor size 7.0 cm; NTRK1-fused tumors may present earlier and have more favorable outcomes (szalai2024ntrkrearrangedspindlecell pages 1-3, feng2025ntrkrearrangedspindlecell pages 1-2) |
| COL1A1–PDGFB fusion uterine sarcoma at cervix | Vaginal bleeding with cervical/vaginal mass; reported in older women including postmenopausal patients (lu2023casereporta pages 1-2) | COL1A1–PDGFB fusion activating PDGFB/PDGFRB signaling (lu2023casereporta pages 1-2) | RNA sequencing/NGS or FISH required for confirmation; IHC often CD34 positive, while TRK/S100/myogenic markers/hormone receptors often negative; differential includes leiomyoma, LMS, HGESS (lu2023casereporta pages 6-7, lu2023casereporta pages 1-2) | Surgery is standard in localized disease; early precise diagnosis may allow benefit from imatinib (lu2023casereporta pages 1-2, lu2023casereporta pages 6-7) | Only five prior uterine cases plus the reported additional case; reported ages 43–82 years (average 56.7, median 53.5); one imatinib-treated patient’s intra-abdominal mass shrank from 22.4 to 6.5 cm before progression at 14 months (lu2023casereporta pages 6-7) |
| Cervical leiomyosarcoma | Usually abnormal vaginal bleeding, often perimenopausal; rare cervical smooth muscle sarcoma (ghirardi2019roleofsurgery pages 9-10) | No single defining alteration summarized in retrieved cervix-specific evidence; generally considered part of complex uterine LMS biology (ghirardi2019roleofsurgery pages 9-10) | Pathology criteria suggested include ≥5 cm, infiltrative margins, ≥5 mitoses/10 HPF, and moderate–severe atypia; smooth muscle marker expression helps in differential diagnosis (ghirardi2019roleofsurgery pages 9-10, lu2023casereporta pages 6-7) | Complete surgical excision with negative margins is primary treatment; approaches in reports range from radical hysterectomy to trachelectomy/wide local excision; role of lymphadenectomy limited/uncertain (ghirardi2019roleofsurgery pages 9-10) | Described as “exceedingly rare”; lymphatic spread is low; prognosis favored by complete excision but overall optimal management remains uncertain because of rarity (ghirardi2019roleofsurgery pages 9-10) |
| Cervical adenosarcoma | Rare Müllerian adenosarcoma, sometimes asymptomatic or incidentally detected; may coexist with other cervical pathology (denschlag2022sarcomaofthe pages 3-4) | No specific recurrent cervical molecular alteration captured in retrieved recent evidence; uterine adenosarcoma classified as epithelial-mesenchymal tumor (denschlag2022sarcomaofthe pages 3-4) | Histopathology and IHC confirm diagnosis; awareness is important because preoperative CT/curettage and frozen section may miss malignancy (denschlag2022sarcomaofthe pages 3-4) | Hysterectomy ± bilateral adnexectomy in reported case; surgery remains main approach in early-stage disease (denschlag2022sarcomaofthe pages 3-4) | Rarely arises in cervix; case report emphasizes that diffuse growth in uterine cavity/cervical canal without symptoms is “even rarer”; patient recovered well after surgery with follow-up (denschlag2022sarcomaofthe pages 3-4) |
Table: This table summarizes the main cervical sarcoma subtypes identified in the retrieved evidence, focusing on presentation, molecular features, diagnostics, management, and quantitative findings. It is useful as a compact reference for comparing these rare entities and their actionable biomarkers.
Key Figures/Tables (visual evidence)
- Immunohistochemistry and compiled clinicopathologic/molecular findings tables for COL1A1–PDGFB fusion uterine/cervical sarcoma were retrieved from Lu et al., 2023 (Frontiers in Oncology) (lu2023casereporta media bf56b6c0, lu2023casereporta media 92e7e479).
Evidence gaps and limitations (important for knowledge base population)
- Ontology identifiers (MONDO/MeSH/ICD/Orphanet/OMIM) for the umbrella term “sarcoma of cervix uteri” were not captured in the accessible retrieved texts using the available tools; downstream curation should map this concept to the preferred ontology term(s) and consider whether the KB entry should be an umbrella class vs subtype-specific entities.
- Many cervix-sarcoma claims necessarily rely on case reports/series. Guidelines referenced are primarily uterine sarcoma guidelines and may not be cervix-specific (raycoquard2024esgoeuracangcigguidelinesfor pages 2-3, perezfidalgo2023uterinesarcomasclinical pages 1-1).
- Robust incidence, prevalence, and survival estimates for “cervical sarcoma” as a single category remain limited; subtype-specific registries and multi-institutional datasets are needed.
Key Source URLs (with publication dates)
- Lu et al. Mar 2023. Frontiers in Oncology: COL1A1–PDGFB fusion uterine sarcoma at cervix. https://doi.org/10.3389/fonc.2023.1108586 (lu2023casereporta pages 1-2)
- Xiao et al. May 2024. J Cancer Research and Clinical Oncology: Primary Ewing’s sarcoma of uterine cervix. https://doi.org/10.1007/s00432-024-05698-2 (xiao2024primaryewing’ssarcoma pages 1-2)
- Yu et al. Dec 2024. Ginekologia Polska: Cervical rhabdomyosarcoma case series. https://doi.org/10.5603/gpl.96919 (yu2024clinicopathologiccharacteristicstreatment pages 1-2)
- Szalai et al. Dec 2024. Virchows Archiv: NUMA1::NTRK1 cervical spindle cell sarcoma. https://doi.org/10.1007/s00428-023-03724-1 (szalai2024ntrkrearrangedspindlecell pages 1-3)
- Altmann et al. Jul 2024. Archives of Gynecology and Obstetrics: DICER1-associated cervical sarcoma fertility-sparing strategy. https://doi.org/10.1007/s00404-024-07588-x (altmann2024fertilitysparingstrategyin pages 1-3)
- Ray-Coquard et al. Oct 2024. International Journal of Gynecological Cancer: ESGO/EURACAN/GCIG uterine sarcoma guideline. https://doi.org/10.1136/ijgc-2024-005823 (raycoquard2024esgoeuracangcigguidelinesfor pages 2-3)
- Pérez-Fidalgo et al. Jan 2023. Therapeutic Advances in Medical Oncology: GEIS uterine sarcoma guidelines. https://doi.org/10.1177/17588359231157645 (perezfidalgo2023uterinesarcomasclinical pages 1-1)
References
-
(altmann2024fertilitysparingstrategyin pages 1-3): J. Altmann, K. Kubiak, J. Sehouli, and E. Roser. Fertility-sparing strategy in a rare case of highly malignant dicer-1-associated sarcoma of the cervix. Archives of Gynecology and Obstetrics, 310:2617-2621, Jul 2024. URL: https://doi.org/10.1007/s00404-024-07588-x, doi:10.1007/s00404-024-07588-x. This article has 0 citations and is from a peer-reviewed journal.
-
(ghirardi2019roleofsurgery pages 9-10): Valentina Ghirardi, Nicolò Bizzarri, Francesco Guida, Carmine Vascone, Barbara Costantini, Giovanni Scambia, and Anna Fagotti. Role of surgery in gynaecological sarcomas. Oncotarget, 10:2561-2575, Apr 2019. URL: https://doi.org/10.18632/oncotarget.26803, doi:10.18632/oncotarget.26803. This article has 34 citations.
-
(yu2024clinicopathologiccharacteristicstreatment pages 1-2): Xiuzhang Yu, Mingrong Qie, Liyan Huang, and Minmin Hou. Clinicopathologic characteristics, treatment, prognosis and pregnancy outcomes in rhabdomyosarcoma of the uterine cervix: a case series. Ginekologia polska, Dec 2024. URL: https://doi.org/10.5603/gpl.96919, doi:10.5603/gpl.96919. This article has 2 citations and is from a peer-reviewed journal.
-
(szalai2024ntrkrearrangedspindlecell pages 1-3): Luca Szalai, Ildikó Vereczkey, Marianna Szemes, András Rókusz, Erzsébet Csernák, Erika Tóth, and Zsombor Melegh. Ntrk-rearranged spindle cell sarcoma of the uterine cervix with a novel numa1::ntrk1 fusion. Virchows Archiv, 484:527-531, Dec 2024. URL: https://doi.org/10.1007/s00428-023-03724-1, doi:10.1007/s00428-023-03724-1. This article has 11 citations and is from a peer-reviewed journal.
-
(xiao2024primaryewing’ssarcoma pages 1-2): Yuhang Xiao, Yong Zhi, Guang-xu Cao, Heling Ma, Jinli Gao, and Fang Li. Primary ewing’s sarcoma of the uterine cervix: a case report and review of the literature. Journal of Cancer Research and Clinical Oncology, May 2024. URL: https://doi.org/10.1007/s00432-024-05698-2, doi:10.1007/s00432-024-05698-2. This article has 9 citations and is from a peer-reviewed journal.
-
(lu2023casereporta pages 6-7): Linghui Lu, Shunni Wang, Haoran Shen, Feiran Zhang, Fenghua Ma, Yue Shi, and Yan Ning. Case report: a case of col1a1–pdgfb fusion uterine sarcoma at cervix and insights into the clinical management of rare uterine sarcoma. Frontiers in Oncology, Mar 2023. URL: https://doi.org/10.3389/fonc.2023.1108586, doi:10.3389/fonc.2023.1108586. This article has 14 citations.
-
(raycoquard2024esgoeuracangcigguidelinesfor pages 2-3): Isabelle Ray-Coquard, Paolo Giovanni Casali, Sabrina Croce, Fiona M Fennessy, Daniela Fischerova, Robin Jones, Roberta Sanfilippo, Ignacio Zapardiel, Frédéric Amant, Jean-Yves Blay, Javier Martἰn-Broto, Antonio Casado, Sarah Chiang, Angelo Paolo Dei Tos, Rick Haas, Martee L Hensley, Peter Hohenberger, Jae-Weon Kim, Se Ik Kim, Mehmet Mutlu Meydanli, Patricia Pautier, Albiruni R Abdul Razak, Jalid Sehouli, Winan van Houdt, François Planchamp, and Michael Friedlander. Esgo/euracan/gcig guidelines for the management of patients with uterine sarcomas. Oct 2024. URL: https://doi.org/10.1136/ijgc-2024-005823, doi:10.1136/ijgc-2024-005823. This article has 57 citations and is from a peer-reviewed journal.
-
(lu2023casereporta pages 1-2): Linghui Lu, Shunni Wang, Haoran Shen, Feiran Zhang, Fenghua Ma, Yue Shi, and Yan Ning. Case report: a case of col1a1–pdgfb fusion uterine sarcoma at cervix and insights into the clinical management of rare uterine sarcoma. Frontiers in Oncology, Mar 2023. URL: https://doi.org/10.3389/fonc.2023.1108586, doi:10.3389/fonc.2023.1108586. This article has 14 citations.
-
(feng2025ntrkrearrangedspindlecell pages 1-2): Lulu Feng, Lei Li, Yan-mei He, and Wei Jiang. Ntrk-rearranged spindle cell neoplasm of the female genital tract: case report and literature review. Frontiers in Oncology, Aug 2025. URL: https://doi.org/10.3389/fonc.2025.1525722, doi:10.3389/fonc.2025.1525722. This article has 1 citations.
-
(lu2023casereporta media bf56b6c0): Linghui Lu, Shunni Wang, Haoran Shen, Feiran Zhang, Fenghua Ma, Yue Shi, and Yan Ning. Case report: a case of col1a1–pdgfb fusion uterine sarcoma at cervix and insights into the clinical management of rare uterine sarcoma. Frontiers in Oncology, Mar 2023. URL: https://doi.org/10.3389/fonc.2023.1108586, doi:10.3389/fonc.2023.1108586. This article has 14 citations.
-
(lu2023casereporta media 92e7e479): Linghui Lu, Shunni Wang, Haoran Shen, Feiran Zhang, Fenghua Ma, Yue Shi, and Yan Ning. Case report: a case of col1a1–pdgfb fusion uterine sarcoma at cervix and insights into the clinical management of rare uterine sarcoma. Frontiers in Oncology, Mar 2023. URL: https://doi.org/10.3389/fonc.2023.1108586, doi:10.3389/fonc.2023.1108586. This article has 14 citations.
-
(perezfidalgo2023uterinesarcomasclinical pages 1-1): Jose Alejandro Pérez-Fidalgo, Eugenia Ortega, Jordi Ponce, Andres Redondo, Isabel Sevilla, Claudia Valverde, Josep Isern Verdum, Enrique de Alava, Mar Galera López, Gloria Marquina, and Ana Sebio. Uterine sarcomas: clinical practice guidelines for diagnosis, treatment, and follow-up, by spanish group for research on sarcomas (geis). Therapeutic Advances in Medical Oncology, Jan 2023. URL: https://doi.org/10.1177/17588359231157645, doi:10.1177/17588359231157645. This article has 65 citations and is from a peer-reviewed journal.
-
(denschlag2022sarcomaofthe pages 3-4): Dominik Denschlag, Sven Ackermann, Marco Johannes Battista, Wolfgang Cremer, Gerlinde Egerer, Matthias Fehr, Markus Follmann, Heidemarie Haase, Philipp Harter, Simone Hettmer, Lars-Christian Horn, Ingolf Juhasz-Boess, Karin Kast, Günter Köhler, Thomas Kröncke, Katja Lindel, Peter Mallmann, Regine Meyer-Steinacker, Alexander Mustea, Edgar Petru, Peter Reichardt, Dietmar Schmidt, Hans-Georg Strauss, Falk Thiel, Uwe Andreas Ulrich, Thomas Vogl, Dirk Vordermark, Markus Wallwiener, Paul Gass, and Matthias W. Beckmann. Sarcoma of the uterus. guideline of the dggg, oeggg and sggg (s2k-level, awmf registry no. 015/074, april 2021). Geburtshilfe und Frauenheilkunde, 82:1337-1367, Dec 2022. URL: https://doi.org/10.1055/a-1897-5124, doi:10.1055/a-1897-5124. This article has 34 citations and is from a peer-reviewed journal.
-
(perezfidalgo2023uterinesarcomasclinical pages 1-3): Jose Alejandro Pérez-Fidalgo, Eugenia Ortega, Jordi Ponce, Andres Redondo, Isabel Sevilla, Claudia Valverde, Josep Isern Verdum, Enrique de Alava, Mar Galera López, Gloria Marquina, and Ana Sebio. Uterine sarcomas: clinical practice guidelines for diagnosis, treatment, and follow-up, by spanish group for research on sarcomas (geis). Therapeutic Advances in Medical Oncology, Jan 2023. URL: https://doi.org/10.1177/17588359231157645, doi:10.1177/17588359231157645. This article has 65 citations and is from a peer-reviewed journal.