1. Disease Information
1.1 Concise overview (current understanding)
Leigh syndrome is the most frequent pediatric manifestation of primary mitochondrial disease, typically presenting in infancy/early childhood with developmental delay or regression and progressive neurologic dysfunction; multisystem involvement (e.g., cardiac, hepatic, renal, GI) can occur. (lake2016leighsyndromeone pages 1-6, baldo2024acomprehensiveapproach pages 1-2)
Neuroimaging hallmark: bilateral symmetric basal ganglia and/or brainstem lesions, visible as focal T2 hyperintensities; MR spectroscopy can show elevated lactate. (lake2016leighsyndromeone pages 1-6, baldo2024acomprehensiveapproach pages 1-2, lim2022naturalhistoryof pages 2-3)
1.2 Synonyms / alternative names
- Subacute necrotizing encephalomyelopathy (classical terminology) (lake2016leighsyndromeone pages 1-6, mccormick2023expertpanelcuration pages 9-10)
- Leigh syndrome spectrum (LSS): nomenclature used to encompass classic Leigh plus “Leigh-like” phenotypes in modern clinical genetics and ClinGen curation. (baldo2024acomprehensiveapproach pages 1-2, mccormick2023expertpanelcuration pages 9-10)
1.3 Key identifiers
Evidence retrieved in this run supports disease-level identifiers primarily through literature and ClinGen-oriented curation, but did not contain explicit Orphanet, ICD-10/ICD-11, MeSH, or MONDO IDs in the accessible text snippets. Therefore, those specific codes cannot be asserted here from tool-retrieved evidence.
1.4 Evidence source type
The report integrates: - Aggregated disease-level resources and expert consensus (ClinGen curation; diagnostic review) (mccormick2023expertpanelcuration pages 9-10, baldo2024acomprehensiveapproach pages 1-2) - Cohort/natural history studies (human observational) (lim2022naturalhistoryof pages 2-3, stenton2022leighsyndromea pages 1-1) - Patient registry (patient-/caregiver-reported outcomes) (zilber2023leighsyndromeglobal pages 1-2, zilber2023leighsyndromeglobal pages 8-11, zilber2023leighsyndromeglobal pages 2-4, zilber2023leighsyndromeglobal pages 11-12) - Model organism mechanistic studies (e.g., Ndufs4−/− mouse) (lake2016leighsyndromeone pages 19-24, spencer2023volatileanaesthetictoxicity pages 1-2)
2. Etiology
2.1 Primary causal factors
Primary cause: inherited mitochondrial dysfunction leading to impaired ATP generation, commonly due to defects in oxidative phosphorylation (OXPHOS) and/or pyruvate dehydrogenase complex (PDHc). (lake2016leighsyndromeone pages 1-6)
2.2 Genetic risk factors (causal variants/genes)
LS/LSS is highly genetically heterogeneous, caused by pathogenic variants in both nuclear DNA (nDNA) and mitochondrial DNA (mtDNA) genes. A key diagnostic challenge is establishing gene–disease relationships across “>100 monogenic causes” spanning both genomes. (mccormick2023expertpanelcuration pages 9-10, lake2016leighsyndromeone pages 1-6)
ClinGen/Expert-panel evidence (2023): The ClinGen Mitochondrial Disease Gene Curation Expert Panel (Mito GCEP) curated 113 primary mitochondrial disease genes for LSS and evaluated 114 gene–disease relationships (GDRs), classified as 31 definitive (27%), 38 moderate (33%), 43 limited (38%), and 2 disputed (2%). Inheritance among curated genes was predominantly autosomal recessive (90), with fewer maternal (16), autosomal dominant (5), and X-linked (3). (mccormick2023expertpanelcuration pages 9-10, mccormick2023expertpanelcuration pages 4-5)
Commonly implicated genes/defects (examples): - Complex I deficiency (often most frequent OXPHOS defect in LS cohorts/reviews) and complex I gene involvement across both genomes (e.g., MT-ND genes; nuclear complex I genes). (lake2016leighsyndromeone pages 1-6, henke2024diseasemodelsof pages 2-5) - MT-ATP6 (complex V/ATP synthase) variants: frequently highlighted in LSS diagnostic reviews and cohorts, including m.8993T>G/C and m.9176T>C. (baldo2024acomprehensiveapproach pages 1-2, lim2022naturalhistoryof pages 2-3, baldo2024acomprehensiveapproach pages 2-4) - SURF1 (complex IV assembly factor) is repeatedly cited as a common nuclear cause in LSS frameworks. (baldo2024acomprehensiveapproach pages 1-2, stenton2022leighsyndromea pages 1-1) - PDHA1 (PDHc) appears among frequent genes in a large pediatric cohort. (stenton2022leighsyndromea pages 1-1)
2.3 Environmental risk factors / triggers
LS is Mendelian/mitochondrial in etiology; however, physiologic stressors can worsen clinical status. A 2023 preclinical study provides mechanistic evidence that volatile anesthetic exposure (isoflurane) can be toxic in a canonical LS model (Ndufs4−/−), producing hyperlactatemia, weight loss, and increased mortality in a disease-stage-dependent manner. (spencer2023volatileanaesthetictoxicity pages 1-2)
2.4 Protective factors
No validated protective variants or environmental protective factors were identified in the retrieved evidence.
2.5 Gene–environment interactions
Direct, human-proven gene–environment interaction datasets were not retrieved in this run. However, experimental evidence in Ndufs4−/− mice indicates a strong interaction between genetic mitochondrial disease state and volatile anesthetic exposure, and suggests a neuroimmune component modulating toxicity (attenuation with CSF1R inhibitor pexidartinib/PLX3397). (spencer2023volatileanaesthetictoxicity pages 1-2)
3. Phenotypes
3.1 Core phenotype spectrum (human)
Across cohorts and reviews, common clinical features include: - Developmental delay / developmental regression - Hypotonia, weakness - Ataxia, dystonia / movement disorders - Epilepsy/seizures - Feeding difficulties/poor feeding - Ophthalmologic manifestations (e.g., ophthalmoparesis/optic atrophy in classic descriptions) (lake2016leighsyndromeone pages 1-6, lim2022naturalhistoryof pages 2-3, henke2024diseasemodelsof pages 2-5)
Quantitative cohort examples - In a 209-patient cohort, common clinical/biochemical features included elevated serum lactate (144/195), global developmental delay (142/209), and developmental regression (103/209). (stenton2022leighsyndromea pages 1-1)
Registry-reported developmental impacts - In the global registry analysis, 68% of participant concerns were developmental delay/regression; 56% never achieved at least one milestone and 40% never walked. (zilber2023leighsyndromeglobal pages 11-12)
3.2 Phenotype characteristics and HPO suggestions
Below are practical phenotype-to-HPO mappings aligned with retrieved evidence.
Table (click to expand)
| Phenotype | Type | Typical onset/course (from retrieved evidence) | Suggested HPO term(s) |
|---|---|---|---|
| Developmental delay/regression | Neurodevelopmental | Often infancy/early childhood; median onset 9 months in one cohort | HP:0001263 (Global developmental delay); HP:0002376 (Developmental regression) (lim2022naturalhistoryof pages 2-3, stenton2022leighsyndromea pages 1-1) |
| Seizures/epilepsy | Neurologic | Common in LSS diagnostic discussions | HP:0001250 (Seizures); HP:0001270 (Epileptic encephalopathy) (baldo2024acomprehensiveapproach pages 1-2, henke2024diseasemodelsof pages 2-5) |
| Hypotonia/weakness | Neuromuscular | Frequent sign in reviews/models | HP:0001252 (Muscular hypotonia); HP:0001324 (Muscle weakness) (lake2016leighsyndromeone pages 1-6, henke2024diseasemodelsof pages 2-5) |
| Ataxia | Neurologic | Common in reviews | HP:0001251 (Ataxia) (lake2016leighsyndromeone pages 1-6) |
| Dystonia/movement disorder | Neurologic | Common; registry and cohorts emphasize motor impairment | HP:0001332 (Dystonia) (lake2016leighsyndromeone pages 1-6, zilber2023leighsyndromeglobal pages 8-11) |
| Lactic acidosis / elevated lactate | Laboratory abnormality | Frequent across cohorts; MRS lactate peak supportive | HP:0003128 (Lactic acidemia); HP:0002151 (Increased lactate) (baldo2024acomprehensiveapproach pages 1-2, lim2022naturalhistoryof pages 2-3) |
| Symmetric basal ganglia/brainstem lesions | Imaging finding | Core neuroradiologic hallmark | HP:0002136 (Bilateral basal ganglia lesions); HP:0012557 (Brainstem lesion) (conceptual mapping; supported by imaging descriptions) (lake2016leighsyndromeone pages 1-6, lim2022naturalhistoryof pages 2-3) |
3.3 Quality-of-life and caregiver burden (registry data; 2023–2025)
Abstract-quotable statements (2023 registry paper): - “Reported results include demographics, diagnostic information, symptom history, loss of milestones, disease management, healthcare utilization, quality of life, and caregiver burden for 116 participants.” (zilber2023leighsyndromeglobal pages 1-2) - “Results show a high disease burden, but a relatively short time to diagnosis.” (zilber2023leighsyndromeglobal pages 1-2) - Participants “in general, are described as having a good quality of life and caregivers are overall resilient, while also reporting a significant amount of stress.” (zilber2023leighsyndromeglobal pages 1-2)
Additional quantitative registry findings (selected): - International distribution: nearly 70% outside the US, 25 countries; heavy representation in Eastern Europe and North America in early analysis. (zilber2023leighsyndromeglobal pages 8-11, zilber2023leighsyndromeglobal pages 2-4) - Healthcare utilization example: in one 3-month window, ~74% reported 0 inpatient nights; among those with any inpatient stay, mean nights were ~12.5 (SD 12.3). (zilber2023leighsyndromeglobal pages 8-11)
4. Genetic/Molecular Information
4.1 Causal genes (selected, evidence-supported)
Disease-level statement: >75 genes were recognized in a high-citation review, with continued expansion to >100 genes in more recent frameworks; ClinGen curated 113 genes as a minimum set for LSS gene–disease validity. (lake2016leighsyndromeone pages 1-6, mccormick2023expertpanelcuration pages 9-10)
Examples (non-exhaustive): - mtDNA: MT-ATP6 (e.g., m.8993T>G/C; m.9176T>C), MT-ND genes (complex I subunits) (baldo2024acomprehensiveapproach pages 1-2, lim2022naturalhistoryof pages 2-3, henke2024diseasemodelsof pages 2-5) - nDNA: SURF1, PDHA1, nuclear complex I genes and assembly factors (stenton2022leighsyndromea pages 1-1, henke2024diseasemodelsof pages 2-5)
4.2 Pathogenic variant classes and functional consequences
Retrieved sources emphasize functional consequences primarily as energy generation failure due to: - OXPHOS complex dysfunction (complex I frequently; complex IV; complex V/ATP synthase) (lake2016leighsyndromeone pages 1-6, henke2024diseasemodelsof pages 2-5) - PDHc defects impairing entry of pyruvate into the TCA cycle (lake2016leighsyndromeone pages 1-6)
Variant load/heteroplasmy (mtDNA): One natural history cohort noted mtDNA pathogenic variants in ~22% and that MT-ATP6 variants were the most frequent mtDNA causes; mtDNA heteroplasmy is a key determinant of severity in mitochondrial disease biology, although detailed allele-frequency distributions in population databases were not retrievable here. (lim2022naturalhistoryof pages 2-3)
4.3 Modifier genes / epigenetics / chromosomal abnormalities
No robust modifier-gene or epigenetic-signature evidence was retrieved in this run. (Not available from the gathered context.)
5. Environmental Information
5.1 Environmental/lifestyle/infectious contributors
No infectious causes are implicated; LS is a genetic neurometabolic disorder. However, exposures that alter mitochondrial function can be clinically relevant.
Volatile anesthetics (environmental/iatrogenic exposure): Isoflurane exposure was toxic in Ndufs4−/− mice, inducing hyperlactatemia, weight loss, and mortality; toxicity depended on neurological disease status and was attenuated by microglia/macrophage depletion using CSF1R inhibitor pexidartinib. (spencer2023volatileanaesthetictoxicity pages 1-2)
6. Mechanism / Pathophysiology
6.1 Causal chain (gene → cellular → tissue → clinical)
Upstream trigger: pathogenic variants in mtDNA or nDNA affecting mitochondrial energy generation (OXPHOS/PDHc). (lake2016leighsyndromeone pages 1-6)
Cellular consequence: reduced ATP production with compensatory glycolysis and altered redox state; biochemical accumulation of lactate/pyruvate is common. (baldo2024acomprehensiveapproach pages 1-2, henke2024diseasemodelsof pages 2-5)
Tissue vulnerability: CNS regions with high energy demand (basal ganglia/brainstem/cerebellum) develop bilateral necrotizing lesions → neurodevelopmental regression, movement disorders, seizures, respiratory failure. (lake2016leighsyndromeone pages 1-6, lim2022naturalhistoryof pages 2-3)
6.2 Molecular pathways and cellular processes (evidence-supported)
- OXPHOS / electron transport chain dysfunction (complex I, IV, V prominent in examples). (lake2016leighsyndromeone pages 1-6, henke2024diseasemodelsof pages 2-5)
- mTOR signaling: a high-citation review summarizes that rapamycin improved lifespan and neurodegeneration in the Ndufs4−/− LS model, supporting nutrient-sensing dysregulation as a contributory mechanism and a potential therapeutic axis. (lake2016leighsyndromeone pages 19-24)
- Neuroimmune involvement: anesthetic toxicity in Ndufs4−/− mice was attenuated by CSF1R inhibitor pexidartinib, implicating microglia/macrophages. (spencer2023volatileanaesthetictoxicity pages 1-2)
6.3 Suggested ontology terms
GO Biological Process (examples): - GO:0006119 oxidative phosphorylation - GO:0006099 tricarboxylic acid cycle (as downstream of PDHc) - GO:0010906 regulation of glucose metabolic process (reflecting glycolytic shift)
GO Cellular Component: - GO:0005739 mitochondrion - GO:0005743 mitochondrial inner membrane - GO:0005753 mitochondrial proton-transporting ATP synthase complex
Cell Ontology (CL) likely involved: - CL:0000540 neuron - CL:0000129 microglial cell (supported by CSF1R inhibitor result in model) (spencer2023volatileanaesthetictoxicity pages 1-2)
7. Anatomical Structures Affected
7.1 Organ/system level
- Central nervous system is primary: basal ganglia and brainstem involvement are defining. (lake2016leighsyndromeone pages 1-6, baldo2024acomprehensiveapproach pages 1-2)
- Multisystem involvement can include muscle, eye, and heart (noted generally in reviews; detailed organ-frequency breakdown not consistently available across retrieved human cohorts in this run). (lake2016leighsyndromeone pages 1-6)
7.2 Localization (UBERON suggestions)
- UBERON:0002421 basal ganglion
- UBERON:0002298 brainstem
- UBERON:0002037 cerebellum
7.3 MRI lesion distribution (quantitative cohort)
In one pediatric natural-history cohort, the commonest MRI findings were symmetrical putaminal signal abnormality (57.1%), globus pallidus (41.3%), and caudate (39.7%). (lim2022naturalhistoryof pages 2-3)
8. Temporal Development
8.1 Onset
- Typical onset is before age 2 years, with median onset 9 months in one natural history cohort. (lake2016leighsyndromeone pages 1-6, lim2022naturalhistoryof pages 2-3)
8.2 Progression/course
- Course is often progressive and may be rapid in severe early-onset forms; prognosis is strongly genotype- and onset-age-dependent. (lake2016leighsyndromeone pages 1-6, stenton2022leighsyndromea pages 1-1)
9. Inheritance and Population
9.1 Epidemiology (statistics)
- A widely cited prevalence estimate is ~1 per 40,000 live births. (lake2016leighsyndromeone pages 1-6, baldo2024acomprehensiveapproach pages 1-2, lim2022naturalhistorystudy pages 50-53)
- Founder effects can produce much higher incidence in particular populations (e.g., LRPPRC in Saguenay–Lac-Saint-Jean; SUCLA2 in Faroe Islands) per compiled prevalence notes. (lim2022naturalhistorystudy pages 50-53)
9.2 Inheritance patterns
- Mixed: autosomal recessive, maternal (mtDNA), X-linked—supported by expert-panel curated distribution and classic review descriptions. (lake2016leighsyndromeone pages 1-6, mccormick2023expertpanelcuration pages 9-10)
10. Diagnostics
10.1 Core clinical + imaging criteria
Modern LSS diagnostic approaches emphasize: - Compatible neurologic presentation (developmental delay/regression, epilepsy, movement disorder, etc.) - Neuroradiology: bilateral symmetric basal ganglia/brainstem lesions (T2 hyperintensities; CT hypodensities) - Biochemical support (lactate/pyruvate abnormalities) - Genetic confirmation increasingly required/central (baldo2024acomprehensiveapproach pages 1-2, baldo2024acomprehensiveapproach pages 2-4)
10.2 Biochemical and laboratory tests
Commonly used markers include: - Elevated lactate (serum and/or CSF) (lim2022naturalhistoryof pages 2-3) - Lactate/pyruvate ratio: L/P >20 highlighted as more specific in one diagnostic review (baldo2024acomprehensiveapproach pages 1-2) - Plasma amino acids (e.g., alanine elevation reflecting glycolytic shift) and urine organic acids/acylcarnitines as parallel first-tier studies to identify treatable etiologies faster. (baldo2024acomprehensiveapproach pages 1-2, baldo2024acomprehensiveapproach pages 2-4)
10.3 Genetic testing strategy
- A diagnostic review proposes a pipeline adding rapid biochemical screening (amino acids, acylcarnitine, urinary organic acids) in parallel with genetic testing; in their cohort, this approach “characterized 80%” and enabled “specific intervention in 10% of confirmed cases.” (baldo2024acomprehensiveapproach pages 1-2)
- Large cohorts show high genetic diagnostic yield (e.g., 82% in one natural-history cohort). (lim2022naturalhistoryof pages 2-3)
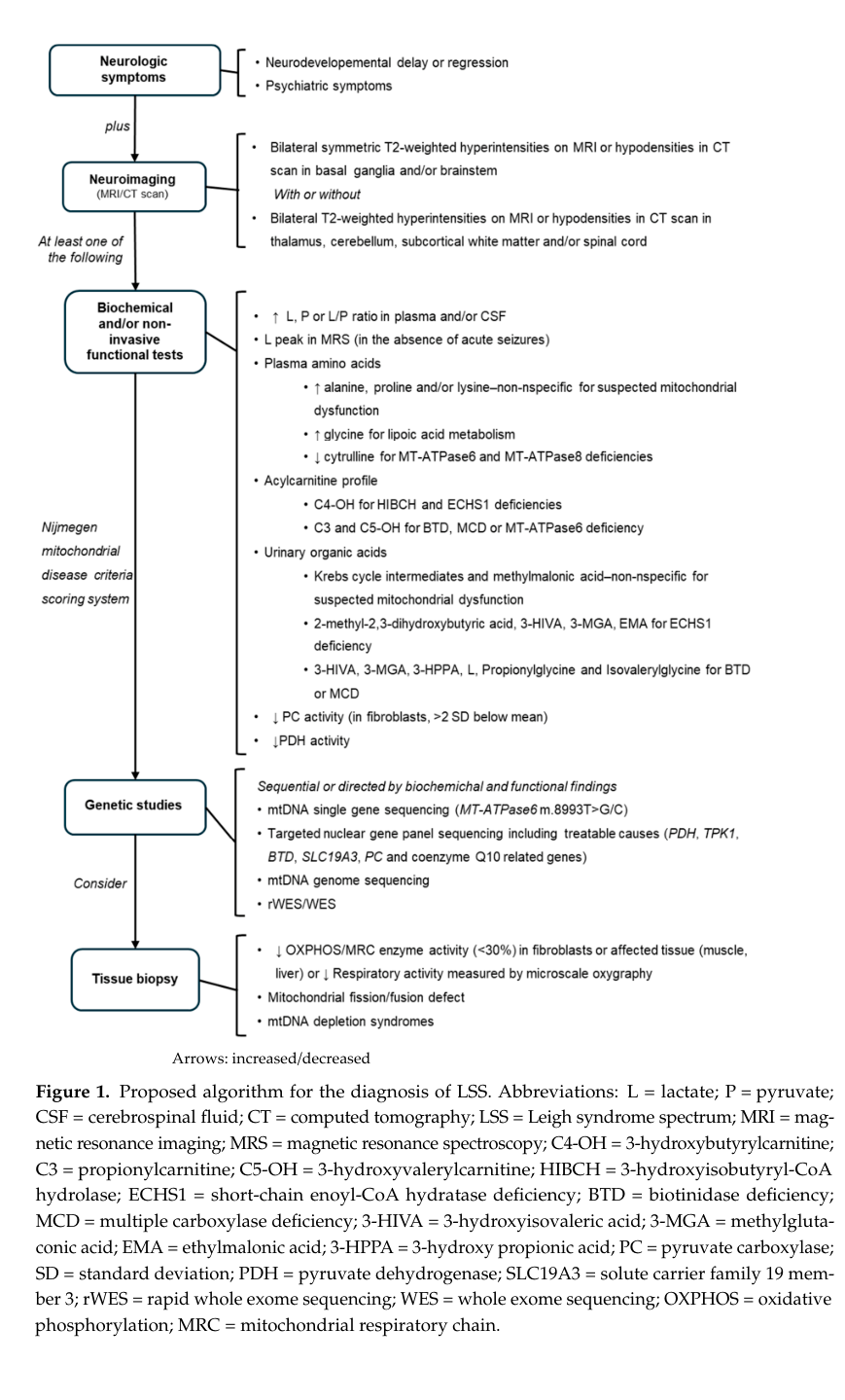
10.4 Visual evidence: diagnostic workflow
A diagnostic algorithm (flowchart) summarizing imaging criteria, biochemical screening, and genetic studies for LSS is presented in the Baldo et al. 2024 paper (Figure 1). (baldo2024acomprehensiveapproach media 389448a6)
11. Outcome/Prognosis
11.1 Survival and mortality (recent cohort statistics)
- Japanese cohort (n=166): 24.1% deceased at follow-up; “Nearly 90% of deaths occurred by age 6.” Earlier onset (<6 months) predicted higher mortality; all neonatal-onset were deceased or bedridden. (lim2022naturalhistoryof pages 2-3)
- Beijing cohort (n=209): genotype-specific outcomes; poorest outcomes (≤50% 3-year survival) included MT-ND5, MT-ATP6 m.8993T>C/m.9176T>C, SURF1, ALDH5A1, while treatable causes (ECHS1, SLC19A3) had 100% 3-year survival. (stenton2022leighsyndromea pages 1-1)
11.2 Prognostic factors
- Age at onset is consistently prognostic (early onset worse). (lim2022naturalhistoryof pages 2-3)
- Genotype is prognostic with strong defect-specific patterns. (stenton2022leighsyndromea pages 1-1)
12. Treatment
12.1 Standard of care (current real-world implementation)
There is no broadly curative therapy; management is typically supportive and multidisciplinary (neurology, metabolic genetics, nutrition, PT/OT/SLP) plus targeted interventions for treatable genetic subtypes when identified. Reviews and cohort data indicate widespread use of vitamin/cofactor supplementation in practice, though a natural history study observed no clear effect on overall course during follow-up. (lake2016leighsyndromeone pages 19-24, lim2022naturalhistoryof pages 2-3)
12.2 Genotype-targeted / treatable causes
Treatable etiologies highlighted in diagnostic reviews include: - SLC19A3 (biotin–thiamine-responsive basal ganglia disease; a Leigh(-like) mimic/overlap) - Valine pathway disorders (e.g., ECHS1, HIBCH) (baldo2024acomprehensiveapproach pages 2-4)
12.3 Recent developments (prioritizing 2023–2024)
Gene curation and trial readiness (2023): ClinGen Mito GCEP provided a curated gene list and refined phenotype criteria intended to streamline diagnosis and enable inclusive clinical trials. (mccormick2023expertpanelcuration pages 9-10)
Global patient registry (2023): registry infrastructure aims to support natural history understanding and facilitate clinical trial recruitment with global reach (nearly 70% outside US). (zilber2023leighsyndromeglobal pages 1-2, zilber2023leighsyndromeglobal pages 8-11)
Anesthesia safety signal (2023): volatile anesthetic toxicity shown in the Ndufs4−/− model suggests disease-stage dependence and potential neuroimmune modulation—important for perioperative risk management research. (spencer2023volatileanaesthetictoxicity pages 1-2)
12.4 Pharmacotherapy/experimental trials (ClinicalTrials.gov)
EPI-743 (vatiquinone) in Leigh syndrome (NCT01721733): Phase 2B randomized, placebo-controlled, double-blind trial in children (6–17 years), n=35, primary endpoint change in NPMDS over 6 months; completed (study completion 2015-05-31). (NCT01721733 chunk 1)
12.5 MAXO suggestions (treatments/actions)
- Supportive mitochondrial disease management: MAXO terms not directly retrievable here; suggested mappings include supportive care, nutritional support, feeding tube placement, physical therapy/rehabilitation (consistent with registry “devices” and interventions). (zilber2023leighsyndromeglobal pages 8-11)
- Genotype-guided vitamin therapy: thiamine/biotin supplementation for SLC19A3-related treatable disease. (baldo2024acomprehensiveapproach pages 2-4)
13. Prevention
13.1 Primary prevention
No population-level prevention exists for most LS causes. Prevention is primarily via genetic counseling, reproductive options, and avoidance of known iatrogenic stressors when possible.
13.2 Secondary/tertiary prevention
- Earlier diagnosis via streamlined biochemical + genetic pipelines can enable prompt treatment for treatable mimics/overlaps and improve supportive management planning. (baldo2024acomprehensiveapproach pages 1-2, baldo2024acomprehensiveapproach pages 2-4)
- Registry efforts aim to improve early recognition and trial readiness. (zilber2023leighsyndromeglobal pages 1-2)
14. Other Species / Natural Disease
Direct evidence for naturally occurring Leigh syndrome in non-human species was not retrieved in this run. (Not available from the gathered context.)
15. Model Organisms
15.1 Model landscape (2024 review)
A 2024 review summarizes LS disease models “from yeast to organoids,” including yeast biochemical models, invertebrates (Drosophila, C. elegans), zebrafish, mammalian models, and patient-derived iPSCs/organoids; it states that mutations in “more than 100 genes” can cause LS and emphasizes model selection based on the research question. (henke2024diseasemodelsof pages 2-5)
15.2 Widely used mammalian model: Ndufs4−/− mouse
- Highlighted as a gold-standard model recapitulating LSS features in ClinGen scoring guidance and used extensively in mechanistic and therapy studies. (mccormick2023expertpanelcuration pages 9-10, lake2016leighsyndromeone pages 19-24)
- Used to study volatile anesthetic toxicity (isoflurane) and neuroimmune modulation via CSF1R inhibition. (spencer2023volatileanaesthetictoxicity pages 1-2)
Embedded Summary Artifact
The following table consolidates key nomenclature and headline epidemiology/prognosis facts from the retrieved evidence:
Table (click to expand)
| Item type | Value | Notes | Source (with PMID if available) | URL | Publication date |
|---|---|---|---|---|---|
| Identifier | Leigh syndrome (OMIM 256000) | Baldo & Vilarinho review explicitly states “Leigh Syndrome (OMIM 256000)”; classic synonym is subacute necrotizing encephalomyelopathy (lake2016leighsyndromeone pages 1-6, zilber2023leighsyndromeglobal pages 2-4) | Baldo MS, Vilarinho L. Orphanet J Rare Dis. 2020; PMID not provided in gathered context | https://doi.org/10.1186/s13023-020-1297-9 | 2020-01 |
| Synonym | Subacute necrotizing encephalomyelopathy | Classical neuropathologic designation used for LS/LSS in reviews and ClinGen-oriented literature (lake2016leighsyndromeone pages 1-6, mccormick2023expertpanelcuration pages 9-10) | Lake NJ et al. Ann Neurol. 2016; PMID not provided in gathered context | https://doi.org/10.1002/ana.24551 | 2016-02 |
| Synonym | Leigh syndrome spectrum (LSS) | Newer umbrella term encompassing classical Leigh syndrome and Leigh-like phenotypes; used in recent diagnostic and ClinGen frameworks (baldo2024acomprehensiveapproach pages 1-2, mccormick2023expertpanelcuration pages 9-10) | Baldo MS et al. Diagnostics. 2024; PMID not provided in gathered context | https://doi.org/10.3390/diagnostics14192133 | 2024-09 |
| Identifier/Nomenclature | ClinGen Mito GCEP curated 113 primary mitochondrial disease genes for LSS | Expert-panel framework to standardize LSS definition and gene–disease relationships; 114 GDRs assessed (31 definitive, 38 moderate, 43 limited, 2 disputed) (mccormick2023expertpanelcuration pages 9-10, mccormick2023expertpanelcuration pages 4-5) | McCormick E et al. Ann Neurol. 2023; PMID not provided in gathered context | https://doi.org/10.1002/ana.26716 | 2023-08 |
| Epidemiology | Prevalence/birth prevalence ~1 per 40,000 live births | Repeated across authoritative reviews and recent diagnostic review as the standard headline prevalence estimate (lake2016leighsyndromeone pages 1-6, baldo2024acomprehensiveapproach pages 1-2, lim2022naturalhistorystudy pages 50-53) | Lake NJ et al. Ann Neurol. 2016; PMID not provided in gathered context | https://doi.org/10.1002/ana.24551 | 2016-02 |
| Epidemiology | Higher-prevalence founder populations reported | Examples include LRPPRC in Saguenay–Lac-Saint-Jean (~1:2000) and SUCLA2 in the Faroe Islands (~1:1700) (lim2022naturalhistorystudy pages 50-53) | Lim AZ. Natural history thesis/report, 2022; PMID not provided in gathered context | Not available in gathered context | 2022 |
| Epidemiology | Most common pediatric manifestation of primary mitochondrial disease | Leigh syndrome/LSS is consistently described as the most frequent pediatric mitochondrial neurodegenerative disorder (baldo2024acomprehensiveapproach pages 1-2, mccormick2023expertpanelcuration pages 9-10) | Baldo MS et al. Diagnostics. 2024; PMID not provided in gathered context | https://doi.org/10.3390/diagnostics14192133 | 2024-09 |
| Prognosis | Typical onset before age 2 years | Onset generally by age 2 years; median age at onset 9 months in one natural-history cohort (lake2016leighsyndromeone pages 1-6, lim2022naturalhistoryof pages 2-3) | Lim AZ et al. Ann Neurol. 2022; PMID not provided in gathered context | https://doi.org/10.1002/ana.26260 | 2022-11 |
| Prognosis | Often rapidly progressive | Authoritative review notes progression is often rapid, with classic severe pediatric course (lake2016leighsyndromeone pages 1-6) | Lake NJ et al. Ann Neurol. 2016; PMID not provided in gathered context | https://doi.org/10.1002/ana.24551 | 2016-02 |
| Prognosis | Typical historical outcome: death by ~3 years in severe early-onset disease | Review summarizes classic expectation of death by age 3; more recent cohorts show genotype-specific variability and some longer survival (lake2016leighsyndromeone pages 1-6, stenton2022leighsyndromea pages 1-1) | Lake NJ et al. Ann Neurol. 2016; PMID not provided in gathered context | https://doi.org/10.1002/ana.24551 | 2016-02 |
| Prognosis | Nearly 90% of deaths occurred by age 6 in a Japanese cohort | In 166 patients, early onset (<6 months) strongly worsened mortality; all neonatal-onset patients were deceased or bedridden (lim2022naturalhistoryof pages 2-3) | Ogawa E et al. J Inherit Metab Dis. 2020; PMID not provided in gathered context | https://doi.org/10.1002/jimd.12218 | 2020-02 |
| Prognosis | Genotype-specific 3-year survival differs substantially | Poorest outcomes (≤50% 3-year survival) reported for MT-ND5, MT-ATP6 m.8993T>C/m.9176T>C, SURF1, ALDH5A1; treatable causes such as ECHS1 and SLC19A3 had 100% 3-year survival in the Beijing cohort (stenton2022leighsyndromea pages 1-1) | Stenton SL et al. Ann Neurol. 2022; PMID not provided in gathered context | https://doi.org/10.1002/ana.26313 | 2022-03 |
| Prognosis | Registry snapshot suggests substantial burden but some resilience | Global registry (n=116) found high disease burden, relatively short time to diagnosis, generally good reported QoL, and caregivers reporting significant stress; ~70% lived outside the US (zilber2023leighsyndromeglobal pages 1-2, zilber2023leighsyndromeglobal pages 8-11, zilber2023leighsyndromeglobal pages 2-4) | Zilber S et al. Orphanet J Rare Dis. 2023; PMID not provided in gathered context | https://doi.org/10.1186/s13023-023-02886-0 | 2023-09 |
Table: This table summarizes core nomenclature, identifiers, and headline epidemiology/prognosis facts for Leigh syndrome/Leigh syndrome spectrum using only gathered evidence. It is useful as a compact reference for disease knowledge base population.
References (URLs and publication dates from retrieved sources)
- Lake NJ et al. Annals of Neurology (2016-02). “Leigh syndrome: One disorder, more than 75 monogenic causes.” https://doi.org/10.1002/ana.24551 (lake2016leighsyndromeone pages 1-6, lake2016leighsyndromeone pages 19-24)
- McCormick E et al. Annals of Neurology (2023-08). “Expert panel curation of 113 primary mitochondrial disease genes for the Leigh syndrome spectrum.” https://doi.org/10.1002/ana.26716 (mccormick2023expertpanelcuration pages 9-10, mccormick2023expertpanelcuration pages 4-5)
- Baldo MS et al. Diagnostics (2024-09). “A Comprehensive Approach to the Diagnosis of Leigh Syndrome Spectrum.” https://doi.org/10.3390/diagnostics14192133 (baldo2024acomprehensiveapproach pages 1-2, baldo2024acomprehensiveapproach pages 2-4, baldo2024acomprehensiveapproach media 389448a6)
- Lim AZ et al. Annals of Neurology (2022-11). “Natural History of Leigh Syndrome: A Study of Disease Burden and Progression.” https://doi.org/10.1002/ana.26260 (lim2022naturalhistoryof pages 2-3)
- Stenton SL et al. Annals of Neurology (2022-03). “Leigh Syndrome: A Study of 209 Patients at the Beijing Children’s Hospital.” https://doi.org/10.1002/ana.26313 (stenton2022leighsyndromea pages 1-1)
- Zilber S et al. Orphanet Journal of Rare Diseases (2023-09). “Leigh syndrome global patient registry: uniting patients and researchers worldwide.” https://doi.org/10.1186/s13023-023-02886-0 (zilber2023leighsyndromeglobal pages 1-2, zilber2023leighsyndromeglobal pages 8-11, zilber2023leighsyndromeglobal pages 2-4, zilber2023leighsyndromeglobal pages 11-12)
- Spencer KA et al. British Journal of Anaesthesia (2023-11). “Volatile anaesthetic toxicity in the genetic mitochondrial disease Leigh syndrome.” https://doi.org/10.1016/j.bja.2023.08.009 (spencer2023volatileanaesthetictoxicity pages 1-2)
- ClinicalTrials.gov: NCT01721733 (EPI-743/vatiquinone). First posted 2012; completed 2015. https://clinicaltrials.gov/study/NCT01721733 (NCT01721733 chunk 1)
References
-
(lake2016leighsyndromeone pages 1-6): Nicole J. Lake, Alison G. Compton, Shamima Rahman, and David R. Thorburn. Leigh syndrome: one disorder, more than 75 monogenic causes. Annals of Neurology, 79:190-203, Feb 2016. URL: https://doi.org/10.1002/ana.24551, doi:10.1002/ana.24551. This article has 646 citations and is from a highest quality peer-reviewed journal.
-
(baldo2024acomprehensiveapproach pages 1-2): Manuela Schubert Baldo, Luísa Azevedo, Margarida Paiva Coelho, Esmeralda Martins, and Laura Vilarinho. A comprehensive approach to the diagnosis of leigh syndrome spectrum. Diagnostics, 14:2133, Sep 2024. URL: https://doi.org/10.3390/diagnostics14192133, doi:10.3390/diagnostics14192133. This article has 3 citations.
-
(mccormick2023expertpanelcuration pages 9-10): E. McCormick, Kierstin N. Keller, Julie Taylor, A. Coffey, Lishuang Shen, D. Krotoski, B. Harding, C. Alves, A. Ardissone, Renkui Bai, I.P. de Barcelos, E. Bertini, Krista K. Bluske, J. Christodoulou, Amanda R. Clause, W. Copeland, G. Diaz, D. Diodato, M. Dulik, G. Enns, A. Feigenbaum, C. Fratter, D. Ghezzi, A. Goldstein, A. Gropman, R. Haas, A. Karaa, M. Koenig, B. Monteleone, S. Parikh, B. P. Dueñas, Revathi Rajkumar, Ann Saada, R. Saneto, K. Sergeant, J. Shoffner, Conrad Smith, C. Stanley, Isabelle Thiffault, D. Thorburn, M. Walker, D. Wallace, L. Wong, Xiaowu Gai, Marni J. Falk, Z. Zolkipli-Cunningham, and S. Rahman. Expert panel curation of 113 primary mitochondrial disease genes for the leigh syndrome spectrum. Annals of Neurology, 94:696-712, Aug 2023. URL: https://doi.org/10.1002/ana.26716, doi:10.1002/ana.26716. This article has 61 citations and is from a highest quality peer-reviewed journal.
-
(lim2022naturalhistoryof pages 2-3): Albert Z. Lim, Yi Shiau Ng, Alasdair Blain, Cecilia Jiminez‐Moreno, Charlotte L. Alston, Victoria Nesbitt, Louise Simmons, Saikat Santra, Evangeline Wassmer, Emma L. Blakely, Doug M. Turnbull, Robert W. Taylor, Gráinne S. Gorman, and Robert McFarland. Natural history of leigh syndrome: a study of disease burden and progression. Annals of Neurology, 91:117-130, Nov 2022. URL: https://doi.org/10.1002/ana.26260, doi:10.1002/ana.26260. This article has 50 citations and is from a highest quality peer-reviewed journal.
-
(stenton2022leighsyndromea pages 1-1): Sarah L. Stenton, Ying Zou, Hua Cheng, Zhimei Liu, Junling Wang, Danmin Shen, Hong Jin, Changhong Ding, Xiaolu Tang, Suzhen Sun, Hong Han, Yanli Ma, Weihua Zhang, Ruifeng Jin, Hua Wang, Dan Sun, Jun Lan Lv, Holger Prokisch, and Fang Fang. Leigh syndrome: a study of 209 patients at the beijing children's hospital. Mar 2022. URL: https://doi.org/10.1002/ana.26313, doi:10.1002/ana.26313. This article has 44 citations and is from a highest quality peer-reviewed journal.
-
(zilber2023leighsyndromeglobal pages 1-2): Sophia Zilber, Kasey Woleben, Simon C. Johnson, Carolina Fischinger Moura de Souza, Danielle Boyce, Kevin Freiert, Courtney Boggs, Souad Messahel, Melinda J. Burnworth, Titilola M. Afolabi, and Saima Kayani. Leigh syndrome global patient registry: uniting patients and researchers worldwide. Orphanet Journal of Rare Diseases, Sep 2023. URL: https://doi.org/10.1186/s13023-023-02886-0, doi:10.1186/s13023-023-02886-0. This article has 19 citations and is from a peer-reviewed journal.
-
(zilber2023leighsyndromeglobal pages 8-11): Sophia Zilber, Kasey Woleben, Simon C. Johnson, Carolina Fischinger Moura de Souza, Danielle Boyce, Kevin Freiert, Courtney Boggs, Souad Messahel, Melinda J. Burnworth, Titilola M. Afolabi, and Saima Kayani. Leigh syndrome global patient registry: uniting patients and researchers worldwide. Orphanet Journal of Rare Diseases, Sep 2023. URL: https://doi.org/10.1186/s13023-023-02886-0, doi:10.1186/s13023-023-02886-0. This article has 19 citations and is from a peer-reviewed journal.
-
(zilber2023leighsyndromeglobal pages 2-4): Sophia Zilber, Kasey Woleben, Simon C. Johnson, Carolina Fischinger Moura de Souza, Danielle Boyce, Kevin Freiert, Courtney Boggs, Souad Messahel, Melinda J. Burnworth, Titilola M. Afolabi, and Saima Kayani. Leigh syndrome global patient registry: uniting patients and researchers worldwide. Orphanet Journal of Rare Diseases, Sep 2023. URL: https://doi.org/10.1186/s13023-023-02886-0, doi:10.1186/s13023-023-02886-0. This article has 19 citations and is from a peer-reviewed journal.
-
(zilber2023leighsyndromeglobal pages 11-12): Sophia Zilber, Kasey Woleben, Simon C. Johnson, Carolina Fischinger Moura de Souza, Danielle Boyce, Kevin Freiert, Courtney Boggs, Souad Messahel, Melinda J. Burnworth, Titilola M. Afolabi, and Saima Kayani. Leigh syndrome global patient registry: uniting patients and researchers worldwide. Orphanet Journal of Rare Diseases, Sep 2023. URL: https://doi.org/10.1186/s13023-023-02886-0, doi:10.1186/s13023-023-02886-0. This article has 19 citations and is from a peer-reviewed journal.
-
(lake2016leighsyndromeone pages 19-24): Nicole J. Lake, Alison G. Compton, Shamima Rahman, and David R. Thorburn. Leigh syndrome: one disorder, more than 75 monogenic causes. Annals of Neurology, 79:190-203, Feb 2016. URL: https://doi.org/10.1002/ana.24551, doi:10.1002/ana.24551. This article has 646 citations and is from a highest quality peer-reviewed journal.
-
(spencer2023volatileanaesthetictoxicity pages 1-2): Kira A. Spencer, Michael Mulholland, John Snell, Miranda Howe, Katerina James, Allison R. Hanaford, Philip G. Morgan, Margaret Sedensky, and Simon C. Johnson. Volatile anaesthetic toxicity in the genetic mitochondrial disease leigh syndrome. British Journal of Anaesthesia, 131:832-846, Nov 2023. URL: https://doi.org/10.1016/j.bja.2023.08.009, doi:10.1016/j.bja.2023.08.009. This article has 14 citations and is from a highest quality peer-reviewed journal.
-
(mccormick2023expertpanelcuration pages 4-5): E. McCormick, Kierstin N. Keller, Julie Taylor, A. Coffey, Lishuang Shen, D. Krotoski, B. Harding, C. Alves, A. Ardissone, Renkui Bai, I.P. de Barcelos, E. Bertini, Krista K. Bluske, J. Christodoulou, Amanda R. Clause, W. Copeland, G. Diaz, D. Diodato, M. Dulik, G. Enns, A. Feigenbaum, C. Fratter, D. Ghezzi, A. Goldstein, A. Gropman, R. Haas, A. Karaa, M. Koenig, B. Monteleone, S. Parikh, B. P. Dueñas, Revathi Rajkumar, Ann Saada, R. Saneto, K. Sergeant, J. Shoffner, Conrad Smith, C. Stanley, Isabelle Thiffault, D. Thorburn, M. Walker, D. Wallace, L. Wong, Xiaowu Gai, Marni J. Falk, Z. Zolkipli-Cunningham, and S. Rahman. Expert panel curation of 113 primary mitochondrial disease genes for the leigh syndrome spectrum. Annals of Neurology, 94:696-712, Aug 2023. URL: https://doi.org/10.1002/ana.26716, doi:10.1002/ana.26716. This article has 61 citations and is from a highest quality peer-reviewed journal.
-
(henke2024diseasemodelsof pages 2-5): Marie‐Thérèse Henke, Alessandro Prigione, and Markus Schuelke. Disease models of leigh syndrome: from yeast to organoids. Journal of Inherited Metabolic Disease, 47:1292-1321, Oct 2024. URL: https://doi.org/10.1002/jimd.12804, doi:10.1002/jimd.12804. This article has 15 citations and is from a peer-reviewed journal.
-
(baldo2024acomprehensiveapproach pages 2-4): Manuela Schubert Baldo, Luísa Azevedo, Margarida Paiva Coelho, Esmeralda Martins, and Laura Vilarinho. A comprehensive approach to the diagnosis of leigh syndrome spectrum. Diagnostics, 14:2133, Sep 2024. URL: https://doi.org/10.3390/diagnostics14192133, doi:10.3390/diagnostics14192133. This article has 3 citations.
-
(lim2022naturalhistorystudy pages 50-53): AZ Lim. Natural history study of childhood-onset mitochondrial disorders by using outcome measure assessments. Unknown journal, 2022.
-
(baldo2024acomprehensiveapproach media 389448a6): Manuela Schubert Baldo, Luísa Azevedo, Margarida Paiva Coelho, Esmeralda Martins, and Laura Vilarinho. A comprehensive approach to the diagnosis of leigh syndrome spectrum. Diagnostics, 14:2133, Sep 2024. URL: https://doi.org/10.3390/diagnostics14192133, doi:10.3390/diagnostics14192133. This article has 3 citations.
-
(NCT01721733 chunk 1): Safety and Efficacy Study of EPI-743 in Children With Leigh Syndrome. PTC Therapeutics. 2012. ClinicalTrials.gov Identifier: NCT01721733