1. Disease Information
1.1 Definition / overview
Pituitary neuroendocrine tumors (PitNETs; historically “pituitary adenomas”) are common intracranial neoplasms; clinically relevant pituitary adenomas occur at an estimated prevalence of ~1 in 1000. (torresmoran2023hotspotsofsomatic pages 1-2)
In this context, GNAS-related pituitary adenomas most commonly refer to growth hormone (GH)-secreting somatotroph PitNETs (and often mammosomatotroph tumors with GH±prolactin co-secretion) that cause acromegaly and harbor somatic activating hotspot mutations in GNAS (also referred to historically as the gsp oncogene). (dillon2026clinicalcharacteristicsassociated pages 1-2, vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic pages 1-2)
Direct abstract support (review): Sousa et al. (2023) states: “The vast majority of pituitary tumours are pituitary adenomas, also recently referred to as pituitary neuroendocrine tumours (PitNET)… In addition, we discuss McCune-Albright syndrome… [where] causative GNAS mutations are postzygotic…” and contrasts this with “somatic GNAS mutations [that] contribute to sporadic acromegaly.” (torresmoran2023hotspotsofsomatic pages 1-2)
1.2 Key identifiers (and gaps)
- MONDO / OMIM / Orphanet / MeSH / ICD-10/11: A specific identifier for the exact phrase “GNAS-related pituitary adenoma 3” was not found in the retrieved evidence set.
- Best practical mapping using retrieved disease ontologies: Open Targets disease associations link GNAS to:
- “Pituitary Gland Adenoma” (EFO_1000478)
- “Growth Hormone-Producing Pituitary Gland Adenoma” (EFO_1000287)
- “Mixed Somatotroph-Lactotroph Pituitary Gland Adenoma” (EFO_1000383) supporting that this entity corresponds to GH-lineage PitNETs. (OpenTargets Search: pituitary adenoma,acromegaly-GNAS)
1.3 Synonyms / alternative names
- Pituitary adenoma (historical)
- Pituitary neuroendocrine tumor (PitNET) (current WHO-aligned terminology in much of recent literature) (torresmoran2023hotspotsofsomatic pages 1-2)
- Somatotroph PitNET / somatotropinoma / GH-secreting pituitary adenoma (rymuza2024highlevelof pages 1-2)
- Mammosomatotroph adenoma/PitNET (GH+PRL) (dillon2026clinicalcharacteristicsassociated pages 1-2)
- “gsp” oncogene-positive somatotroph tumor (historical term for GNAS-activating variants) (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8)
1.4 Evidence source type for disease information
The disease characterization here is derived from aggregated disease-level resources and cohort/review literature, not individual EHR-derived entities. (OpenTargets Search: pituitary adenoma,acromegaly-GNAS, dillon2026clinicalcharacteristicsassociated pages 1-2, vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic pages 1-2)
2. Etiology
2.1 Disease causal factors
Primary causal factor (molecular): Somatic gain-of-function GNAS variants (hotspots at residues R201 and Q227) cause constitutive Gsα activation, driving cAMP/PKA signaling in somatotroph-lineage pituitary cells and contributing to tumorigenesis and GH hypersecretion. (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic media 804a8a89, torresmoran2023hotspotsofsomatic media 493c647d)
2.2 Risk factors
- Genetic (somatic) risk factor: Presence of tumor somatic GNAS hotspot mutations in somatotroph PitNETs; cohort-level prevalence is commonly ~30–40% and varies by series. (balinisteanu2024unlockingthegenetic pages 9-11, vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, tang2024gnasmutationssuppress pages 1-2, rymuza2024highlevelof pages 1-2)
- Syndromic / mosaic genetic context: Postzygotic activating GNAS variants cause McCune–Albright syndrome (MAS), which can include GH excess and pituitary involvement; this is a related mechanism but distinct from most sporadic acromegaly-associated somatotroph tumors. (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic pages 1-2)
Environmental, infectious, and lifestyle risk factors: Not identified in the retrieved evidence set specific to GNAS-driven pituitary adenomas.
2.3 Protective factors
No robust genetic or environmental protective factors specific to this entity were identified in the retrieved evidence set.
2.4 Gene–environment interactions
No specific gene–environment interaction evidence was identified in the retrieved evidence set.
3. Phenotypes
3.1 Core clinical phenotype: GH excess / acromegaly
Somatotroph PitNETs cause acromegaly, classically characterized biochemically by elevated IGF-1 and failure of GH suppression after oral glucose tolerance testing (OGTT). (rymuza2024highlevelof pages 1-2)
HPO suggestions (common in acromegaly; map for knowledge base use): * Elevated insulin-like growth factor 1: HP:0033688 (suggested) * Elevated growth hormone: HP:0011745 (suggested) * Enlarged hands/feet: HP:0001197, HP:0001833 (suggested) * Prognathism: HP:0000303 (suggested) * Headache: HP:0002315 (suggested; pituitary mass effect) * Visual field defect (e.g., bitemporal hemianopia): HP:0000580 (suggested; mass effect)
(These HPO mappings are ontology suggestions; the retrieved evidence directly supports acromegaly/GH excess and tumor behavior rather than listing individual HPO-coded symptoms.) (dillon2026clinicalcharacteristicsassociated pages 1-2, rymuza2024highlevelof pages 1-2)
3.2 Tumor phenotype: size and invasion
Across studies, GNAS-mutant acromegaly tumors are frequently reported to be smaller and possibly less invasive than GNAS-wild-type tumors. (dillon2026clinicalcharacteristicsassociated pages 1-2, tang2024gnasmutationssuppress pages 1-2)
Recent cohort statistic: In a Chinese surgical cohort (n=97), patients with GNAS-mutant tumors had smaller maximum tumor diameters (mean 1.75 ± 0.83 cm vs 2.23 ± 0.89 cm, P=0.008). (balinisteanu2024unlockingthegenetic pages 9-11)
HPO suggestions (tumor invasion/mass effect): * Pituitary adenoma: HP:0007009 (suggested) * Visual field defect: HP:0000580 (suggested) * Headache: HP:0002315 (suggested)
3.3 Histopathology phenotype (tumor subtype associations)
Reviews and clinical series commonly associate GNAS-mutant tumors with densely granulated somatotroph histology and, in some series, mammosomatotroph classification. (balinisteanu2024unlockingthegenetic pages 9-11, dillon2026clinicalcharacteristicsassociated pages 1-2, balinisteanu2024unlockingthegenetic pages 3-4)
4. Genetic / Molecular Information
4.1 Causal gene
- GNAS (HGNC symbol: GNAS; “GNAS complex locus”) encodes Gsα, the α subunit of a stimulatory heterotrimeric G protein coupling GPCRs to adenylyl cyclase. (torresmoran2023hotspotsofsomatic pages 4-6, torresmoran2023hotspotsofsomatic media 493c647d)
4.2 Pathogenic variants (somatic hotspots)
- Hotspot residues: R201 and Q227 are recurrently mutated in PitNETs, especially somatotroph tumors. (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic media 804a8a89)
- Mechanistic consequence: Hotspot variants stabilize Gsα in an active state and inhibit its intrinsic GTPase activity, resulting in constitutive cAMP signaling. (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic media 804a8a89, torresmoran2023hotspotsofsomatic media 493c647d)
Variant examples (from review text): p.R201C, p.R201S are explicitly mentioned as hotspot examples in the PitNET hotspot review. (torresmoran2023hotspotsofsomatic pages 4-6)
Somatic vs germline: The driver context for most GNAS-related pituitary adenomas is somatic tumor mutation; MAS reflects postzygotic mosaic (not inherited) activating variants. (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic pages 1-2)
ACMG/AMP classification & population allele frequency: Not directly retrievable from the current evidence set (ClinVar/gnomAD were not queried within the tool outputs).
4.3 Modifier genes / additional genomic features
A 2024 multi-omics study of somatotroph PitNETs emphasized heterogeneous copy number alteration (CNA) patterns and described recurrent chromosome 11 loss with reduced MEN1 and AIP, and a highly aneuploid subgroup that was largely GNAS-wild-type. (rymuza2024highlevelof pages 1-2)
4.4 Epigenetic information
Not specifically extracted for GNAS-mutant tumors in the current evidence set; however, CNA-associated methylation/transcriptome differences were reported in somatotroph PitNETs at the cohort level. (rymuza2024highlevelof pages 1-2)
5. Environmental Information
No disease-specific environmental, lifestyle, or infectious contributors were identified in the retrieved evidence set for GNAS-driven pituitary adenomas.
6. Mechanism / Pathophysiology
6.1 Canonical pathway: GPCR–Gsα–adenylyl cyclase–cAMP–PKA
A recent hotspot-focused review outlines the normal Gsα cycle (GPCR-triggered GDP→GTP exchange, adenylyl cyclase activation, cAMP production, termination by intrinsic GTPase) and explains that GNAS hotspot variants disable termination, driving persistent signaling. (torresmoran2023hotspotsofsomatic pages 4-6, torresmoran2023hotspotsofsomatic media 493c647d)
Causal chain (mechanistic): 1. Somatic activating GNAS hotspot mutation in somatotroph-lineage pituitary cell (upstream trigger). (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic media 804a8a89) 2. Constitutive activation of adenylyl cyclase → increased cAMP → increased PKA activity and downstream transcriptional programs (e.g., via CREB). (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic media 493c647d) 3. Increased GH transcription and secretion and enhanced somatotroph proliferation → formation of GH-secreting PitNET. (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, torresmoran2023hotspotsofsomatic media 493c647d) 4. Systemic GH/IGF-1 excess → clinical acromegaly. (rymuza2024highlevelof pages 1-2)
Ontology suggestions (GO / pathways): * GO: cAMP-mediated signaling: GO:0019933 (suggested) * GO: adenylate cyclase-activating GPCR signaling: GO:0007189 (suggested) * GO: protein kinase A signaling: GO:0010737 (suggested) * GO: regulation of hormone secretion: GO:0046883 (suggested)
6.2 Invasion biology (recent 2024 development): MEG3–EMT–Wnt/β-catenin
A 2024 experimental study reported that GNAS-mutant GH pituitary adenomas show increased MEG3 (lncRNA) expression and that MEG3 suppresses invasion by inhibiting EMT and Wnt/β-catenin signaling; the authors conclude “GNAS mutations may suppress cell invasion… through the activation of the MEG3/Wnt/β-catenin signaling pathway.” (tang2024gnasmutationssuppress pages 1-2)
Direct abstract support (primary): Tang et al. (2024) states: “Approximately 30%–40% of growth hormone–secreting pituitary adenomas (GHPAs) harbor somatic activating mutations in GNAS…” and describes MEG3-associated suppression of invasion. (tang2024gnasmutationssuppress pages 1-2)
Ontology suggestions: * GO: epithelial to mesenchymal transition: GO:0001837 (suggested) * GO: Wnt signaling pathway: GO:0016055 (suggested)
6.3 Cell types involved (Cell Ontology suggestions)
- Pituitary somatotroph: CL:0002371 (suggested)
- Pituitary lactotroph: CL:0002370 (suggested; relevant to mammosomatotroph phenotype)
7. Anatomical Structures Affected
7.1 Organ/tissue
- Primary site: Anterior pituitary (adenohypophysis) (UBERON suggestion: UBERON:0000007 pituitary gland; adenohypophysis UBERON:0000005).
7.2 Secondary systemic involvement (via hormone excess)
Systemic morbidity is mediated largely by GH/IGF-1 excess (acromegaly), rather than metastatic spread (PitNETs are generally benign). (torresmoran2023hotspotsofsomatic pages 1-2)
8. Temporal Development
8.1 Onset and diagnostic delay
Acromegaly is described as an “insidious” disease in systematic review synthesis, consistent with delayed diagnosis. (dillon2026clinicalcharacteristicsassociated pages 1-2)
A recent cohort reported longer diagnosis delays in GNAS-mutant patients (median 72 vs 36 months) in one series. (balinisteanu2024unlockingthegenetic pages 9-11)
8.2 Course / progression
GNAS-mutant tumors are often described as smaller and less invasive, suggesting a comparatively less aggressive local course in many series, though prognostic utility remains insufficient for clinical decision-making. (dillon2026clinicalcharacteristicsassociated pages 1-2, tang2024gnasmutationssuppress pages 1-2)
9. Inheritance and Population
9.1 Epidemiology
- Clinically relevant pituitary adenomas overall: ~1/1000 prevalence (review). (torresmoran2023hotspotsofsomatic pages 1-2)
- GNAS mutation frequency in somatotroph (GH-secreting) PitNETs: commonly ~35–40% in reviews. (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8, tang2024gnasmutationssuppress pages 1-2, rymuza2024highlevelof pages 1-2)
9.2 Population demographics (recent cohort-level observations)
A systematic review found that while some studies report older age or male predominance among GNAS+ tumors, “most did not find this association,” indicating inconsistent demographic correlation. (dillon2026clinicalcharacteristicsassociated pages 1-2)
10. Diagnostics
10.1 Clinical / biochemical
- IGF-1 elevation and lack of GH suppression on OGTT are used in somatotroph PitNET characterization (study background/definition). (rymuza2024highlevelof pages 1-2)
10.2 Imaging
Pituitary MRI is used to assess tumor size and invasion; in the 2024 mechanistic study, invasiveness was operationalized by MRI-based Knosp grading. (tang2024gnasmutationssuppress pages 1-2)
10.3 Pathology
Somatotroph tumors are classified by granulation patterns (dense vs sparse) and lineage markers (e.g., PIT-1, GH). (rymuza2024highlevelof pages 1-2)
10.4 Molecular testing (real-world implementation)
Hotspot driver mutations “are easily detectable in clinical samples via Sanger or next-generation sequencing (NGS).” (torresmoran2023hotspotsofsomatic pages 1-2)
Implementation note: Routine clinical adoption of GNAS testing varies by center; the systematic review concludes that GNAS status cannot yet be used reliably to guide prognosis and treatment in acromegaly, implying limited decision-impact in current practice. (dillon2026clinicalcharacteristicsassociated pages 1-2)
11. Outcome / Prognosis
GNAS+ somatotroph tumors are more consistently associated with smaller size and possibly less invasiveness, but systematic review synthesis concludes that GNAS mutation status “cannot reliably inform prognosis and treatment… based on findings to date.” (dillon2026clinicalcharacteristicsassociated pages 1-2)
No overall survival statistics specific to GNAS-mutant somatotroph tumors were identified in the retrieved evidence set.
12. Treatment
12.1 Standard-of-care modalities (real-world)
- Transsphenoidal surgery is a mainstay (noted as treatment context in recent cohorts). (balinisteanu2024unlockingthegenetic pages 9-11, rymuza2024highlevelof pages 1-2)
- Somatostatin receptor ligands (SRLs) such as octreotide and lanreotide are used preoperatively and/or as medical therapy. (rymuza2024highlevelof pages 1-2)
12.2 Relationship of GNAS status to treatment response (expert synthesis)
- A systematic review reports greater acute GH suppression after octreotide is “frequently” observed, but long-term biochemical control with SRLs is not consistently associated with GNAS mutation status. (dillon2026clinicalcharacteristicsassociated pages 1-2)
- A management-focused review notes better response to somatostatin analogues has been reported in some studies, but results are “controversial” across cohorts. (vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8)
12.3 MAXO suggestions
- Transsphenoidal hypophysectomy / pituitary tumor resection: MAXO:0001088 (suggested)
- Somatostatin analog therapy: MAXO:0000574 (suggested)
- MRI of pituitary: MAXO:0000910 (suggested; if used for diagnostic action)
(These MAXO terms are suggestions; the retrieved evidence supports these interventions but does not provide MAXO annotations.) (dillon2026clinicalcharacteristicsassociated pages 1-2, rymuza2024highlevelof pages 1-2)
13. Prevention
No primary prevention strategies specific to GNAS-driven pituitary adenoma formation were identified in the retrieved evidence set. Secondary prevention in practice is generally earlier recognition of acromegaly and pituitary mass effects, but no guideline-level screening recommendations were retrieved here.
14. Other Species / Natural Disease
No naturally occurring veterinary analogs specific to GNAS-mutant pituitary adenomas were identified in the retrieved evidence set.
15. Model Organisms
A 2024 mechanistic study used: * GH3 pituitary cell line (rat somatotroph/lactotroph lineage model) with mutant GNAS expression (in vitro) and * a mouse xenograft model to test effects on tumor invasiveness (in vivo). (tang2024gnasmutationssuppress pages 1-2)
Model limitations (inferred from study design): GH3/xenograft systems model invasion biology but do not fully capture human pituitary microenvironment, endocrine feedback loops, or long-term treatment response heterogeneity. (tang2024gnasmutationssuppress pages 1-2)
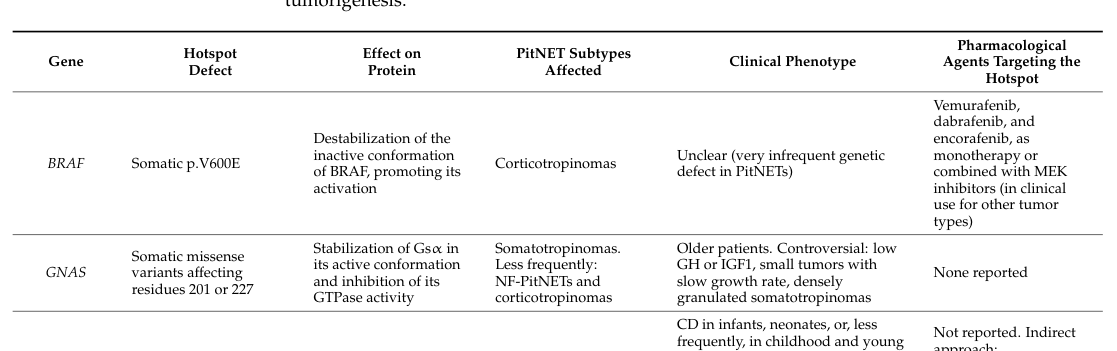
Visual evidence (figure/table)
A hotspot-variant review includes a table and pathway figure summarizing GNAS hotspots (R201, Q227) and the cAMP pathway in somatotroph cells, supporting the mechanistic chain and hotspot definition. (torresmoran2023hotspotsofsomatic media 804a8a89, torresmoran2023hotspotsofsomatic media 493c647d)
Notes on evidence coverage and gaps
- The specific label “GNAS-related pituitary adenoma 3” did not appear as a standardized entity name within the retrieved papers; therefore, this report uses genotype+phenotype mapping to GH-lineage PitNETs with somatic activating GNAS variants, supported by reviews, systematic synthesis, and disease-target ontology resources. (OpenTargets Search: pituitary adenoma,acromegaly-GNAS, dillon2026clinicalcharacteristicsassociated pages 1-2, vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8)
- Some requested elements (e.g., formal MONDO/ICD/MeSH identifiers for the exact label; ClinVar classifications; population allele frequencies from gnomAD; dedicated QoL instruments) were not available in the retrieved evidence set.
References
-
(OpenTargets Search: pituitary adenoma,acromegaly-GNAS): Open Targets Query (pituitary adenoma,acromegaly-GNAS, 5 results). Buniello, A. et al. (2025). Open Targets Platform: facilitating therapeutic hypotheses building in drug discovery. Nucleic Acids Research.
-
(dillon2026clinicalcharacteristicsassociated pages 1-2): Brendan R. Dillon, Margaret Ruddy, Emily C. McQuade, Shruti N. Shah, Alberta Twi-Yeboah, Benjamin A. Levinson, and Nidhi Agrawal. Clinical characteristics associated with somatic gnas mutations in acromegaly: a systematic review and institutional experience. Frontiers in Endocrinology, Jan 2026. URL: https://doi.org/10.3389/fendo.2026.1736208, doi:10.3389/fendo.2026.1736208. This article has 2 citations.
-
(vamvoukaki2023pituitarytumorigenesis—implicationsfor pages 6-8): Rodanthi Vamvoukaki, Maria Chrysoulaki, Grigoria Betsi, and Paraskevi Xekouki. Pituitary tumorigenesis—implications for management. Medicina, 59:812, Apr 2023. URL: https://doi.org/10.3390/medicina59040812, doi:10.3390/medicina59040812. This article has 15 citations.
-
(torresmoran2023hotspotsofsomatic pages 1-2): Mariana Torres-Morán, Alexa L. Franco-Álvarez, Rosa G. Rebollar-Vega, and Laura C. Hernández-Ramírez. Hotspots of somatic genetic variation in pituitary neuroendocrine tumors. Cancers, 15:5685, Dec 2023. URL: https://doi.org/10.3390/cancers15235685, doi:10.3390/cancers15235685. This article has 9 citations.
-
(torresmoran2023hotspotsofsomatic pages 4-6): Mariana Torres-Morán, Alexa L. Franco-Álvarez, Rosa G. Rebollar-Vega, and Laura C. Hernández-Ramírez. Hotspots of somatic genetic variation in pituitary neuroendocrine tumors. Cancers, 15:5685, Dec 2023. URL: https://doi.org/10.3390/cancers15235685, doi:10.3390/cancers15235685. This article has 9 citations.
-
(torresmoran2023hotspotsofsomatic media 804a8a89): Mariana Torres-Morán, Alexa L. Franco-Álvarez, Rosa G. Rebollar-Vega, and Laura C. Hernández-Ramírez. Hotspots of somatic genetic variation in pituitary neuroendocrine tumors. Cancers, 15:5685, Dec 2023. URL: https://doi.org/10.3390/cancers15235685, doi:10.3390/cancers15235685. This article has 9 citations.
-
(tang2024gnasmutationssuppress pages 1-2): Chao Tang, Chunyu Zhong, Junhao Zhu, Feng Yuan, Jin Yang, Yong Xu, and Chiyuan Ma. Gnas mutations suppress cell invasion by activating meg3 in growth hormone–secreting pituitary adenoma. Oncology Research, 32:1079-1091, May 2024. URL: https://doi.org/10.32604/or.2024.046007, doi:10.32604/or.2024.046007. This article has 5 citations and is from a peer-reviewed journal.
-
(rymuza2024highlevelof pages 1-2): Julia Rymuza, Paulina Kober, Maria Maksymowicz, Aleksandra Nyc, Beata J. Mossakowska, Renata Woroniecka, Natalia Maławska, Beata Grygalewicz, Szymon Baluszek, Grzegorz Zieliński, Jacek Kunicki, and Mateusz Bujko. High level of aneuploidy and recurrent loss of chromosome 11 as relevant features of somatotroph pituitary tumors. Journal of Translational Medicine, Nov 2024. URL: https://doi.org/10.1186/s12967-024-05736-0, doi:10.1186/s12967-024-05736-0. This article has 8 citations and is from a peer-reviewed journal.
-
(balinisteanu2024unlockingthegenetic pages 9-11): Ioana Balinisteanu, Lavinia Caba, Andreea Florea, Roxana Popescu, Laura Florea, Maria-Christina Ungureanu, Letitia Leustean, Eusebiu Vlad Gorduza, and Cristina Preda. Unlocking the genetic secrets of acromegaly: exploring the role of genetics in a rare disorder. Current Issues in Molecular Biology, 46:9093-9121, Aug 2024. URL: https://doi.org/10.3390/cimb46080538, doi:10.3390/cimb46080538. This article has 8 citations.
-
(balinisteanu2024unlockingthegenetic pages 3-4): Ioana Balinisteanu, Lavinia Caba, Andreea Florea, Roxana Popescu, Laura Florea, Maria-Christina Ungureanu, Letitia Leustean, Eusebiu Vlad Gorduza, and Cristina Preda. Unlocking the genetic secrets of acromegaly: exploring the role of genetics in a rare disorder. Current Issues in Molecular Biology, 46:9093-9121, Aug 2024. URL: https://doi.org/10.3390/cimb46080538, doi:10.3390/cimb46080538. This article has 8 citations.
-
(torresmoran2023hotspotsofsomatic media 493c647d): Mariana Torres-Morán, Alexa L. Franco-Álvarez, Rosa G. Rebollar-Vega, and Laura C. Hernández-Ramírez. Hotspots of somatic genetic variation in pituitary neuroendocrine tumors. Cancers, 15:5685, Dec 2023. URL: https://doi.org/10.3390/cancers15235685, doi:10.3390/cancers15235685. This article has 9 citations.