Paraneoplastic Neurological Syndromes
Paraneoplastic neurological syndromes are rare immune-mediated neurologic disorders triggered by cancer but not caused by direct tumor invasion, metastasis, infection, ischemia, or metabolic disturbance. Tumor expression of antigens shared with the nervous system can elicit high-risk or intermediate-risk neural autoantibodies and T-cell responses that injure the central nervous system, peripheral nervous system, neuromuscular junction, or muscle. Diagnosis integrates the neurologic phenotype, antibody risk category, cancer status, and follow-up using the PNS-Care framework.
Ask OpenScientist
Ask a research question about Paraneoplastic Neurological Syndromes. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Mappings
Definitions
2Show evidence (1 reference)
Show evidence (1 reference)
Subtypes
2Show evidence (2 references)
Show evidence (2 references)
Pathophysiology
4Show evidence (1 reference)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Histopathology
1Show evidence (1 reference)
Pathograph
Phenotypes
10Digestive 1
Show evidence (1 reference)
Eye 1
Show evidence (1 reference)
Musculoskeletal 1
Show evidence (1 reference)
Nervous System 6
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Other 1
Show evidence (2 references)
Genetic Associations
4Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Medical Actions
7Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Biochemical Markers
2Show evidence (2 references)
Show evidence (2 references)
Source YAML
click to showname: Paraneoplastic Neurological Syndromes
creation_date: "2026-05-16T22:42:45Z"
updated_date: "2026-05-16T23:48:49Z"
category: Autoimmune
parents:
- Neurological Disease
- Autoimmune Disease
- Cancer-Associated Disease
prevalence:
- population: Northeastern Italy population-based cohort, 2009-2017
measure_type: POINT_PREVALENCE
prevalence_class: BAND_1_9_PER_100000
rate_per_100000: 4.37
percentage: 4.37 per 100,000 prevalence; 0.89 per 100,000 person-years incidence
evidence:
- reference: PMID:31552550
reference_title: "Epidemiology of paraneoplastic neurological syndromes: a population-based study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The incidence of PNS was 0.89/100,000 person-years."
explanation: The Friuli-Venezia Giulia population-based study provides incidence and prevalence estimates for definite PNS.
- reference: PMID:31552550
reference_title: "Epidemiology of paraneoplastic neurological syndromes: a population-based study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The prevalence of PNS was 4.37 per 100,000."
explanation: The same cohort supports the point-prevalence estimate.
- population: Olmsted County, Minnesota population-based cohort, 1987-2018
measure_type: POINT_PREVALENCE
prevalence_class: BAND_1_9_PER_100000
rate_per_100000: 5.4
percentage: 5.4 per 100,000 prevalence; 0.6 per 100,000 person-years incidence
evidence:
- reference: PMID:34937736
reference_title: "Population-Based Epidemiology Study of Paraneoplastic Neurologic Syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "PNS incidence was 0.6/100,000 person-years"
explanation: The Olmsted County study provides a United States population-based incidence estimate.
- reference: PMID:34937736
reference_title: "Population-Based Epidemiology Study of Paraneoplastic Neurologic Syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Prevalence was 5.4/100,000 people."
explanation: The same study provides a population-based prevalence estimate and documents severe morbidity and mortality.
synonyms:
- PNS
- Paraneoplastic neurologic syndrome
- Paraneoplastic neurologic syndromes
- Nervous system paraneoplastic syndromes
description: >-
Paraneoplastic neurological syndromes are rare immune-mediated neurologic
disorders triggered by cancer but not caused by direct tumor invasion,
metastasis, infection, ischemia, or metabolic disturbance. Tumor expression of
antigens shared with the nervous system can elicit high-risk or
intermediate-risk neural autoantibodies and T-cell responses that injure the
central nervous system, peripheral nervous system, neuromuscular junction, or
muscle. Diagnosis integrates the neurologic phenotype, antibody risk category,
cancer status, and follow-up using the PNS-Care framework.
has_subtypes:
- name: Intracellular Antigen PNS
description: >-
PNS associated with intracellular neural antigens, including classic
onconeural antibody syndromes such as anti-Hu/ANNA-1 and anti-Yo/PCA-1, is
generally high cancer-risk and is primarily modeled as T-cell-mediated neural
injury with limited immunotherapy responsiveness.
evidence:
- reference: PMID:41562781
reference_title: 'Paraneoplastic Neurological Syndromes: Advances and Future Perspectives in Immunopathogenesis and Management.'
supports: SUPPORT
evidence_source: OTHER
snippet: "distinguish T-cell-mediated syndromes associated with intracellular antigens from antibody-mediated disorders targeting neuronal surface proteins"
explanation: This contemporary review supports intracellular-antigen PNS as a distinct immunopathogenic subtype.
- reference: PMID:21938556
reference_title: 'Paraneoplastic neurological autoimmunity and survival of the neuron: the role of the cancer immunity cycle.'
supports: SUPPORT
evidence_source: OTHER
snippet: "Disorders accompanied by autoantibody markers of neural peptide-specific cytotoxic effector T cells"
explanation: This review supports cytotoxic T-cell-dominant biology for intracellular/onconeural antibody syndromes.
- name: Surface Antigen PNS
description: >-
PNS associated with neuronal surface, plasma-membrane, or synaptic antigen
targets is modeled as pathogenic autoantibody-mediated synaptic or neuronal
signaling dysfunction, often with greater potential reversibility after
early immunotherapy.
evidence:
- reference: PMID:41562781
reference_title: 'Paraneoplastic Neurological Syndromes: Advances and Future Perspectives in Immunopathogenesis and Management.'
supports: SUPPORT
evidence_source: OTHER
snippet: "distinguish T-cell-mediated syndromes associated with intracellular antigens from antibody-mediated disorders targeting neuronal surface proteins"
explanation: This review explicitly separates antibody-mediated surface-antigen PNS from intracellular-antigen syndromes.
- reference: PMID:21938556
reference_title: 'Paraneoplastic neurological autoimmunity and survival of the neuron: the role of the cancer immunity cycle.'
supports: SUPPORT
evidence_source: OTHER
snippet: "Disorders accompanied by neural plasma membrane-reactive autoantibodies"
explanation: This review supports plasma-membrane/synaptic autoantibody disease as a distinct immunopathogenic subtype.
disease_term:
preferred_term: paraneoplastic neurologic syndrome
term:
id: MONDO:0018215
label: paraneoplastic neurologic syndrome
mappings:
mondo_mappings:
- term:
id: MONDO:0018215
label: paraneoplastic neurologic syndrome
mapping_predicate: skos:exactMatch
mapping_source: MONDO
mapping_justification: MONDO exact match for the Orphanet/ORDO paraneoplastic neurological syndromes concept ORPHA:36388.
definitions:
- name: Remote cancer-associated neurologic syndrome definition
definition_type: OTHER
description: >-
Paraneoplastic neurological syndromes are remote neurologic effects of
cancer, distinct from metastasis or other cancer complications.
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "Paraneoplastic neurological syndromes (PNS) can be defined as remote effects of cancer that are not caused by the tumor and its metastasis, or by infection, ischemia or metabolic disruptions."
explanation: The Orphanet Journal of Rare Diseases review provides the core clinical definition for PNS.
- name: PNS-Care diagnostic evidence levels
definition_type: CASE_DEFINITION
description: >-
Contemporary diagnostic criteria classify PNS evidence as definite,
probable, or possible using clinical phenotype, antibody risk category,
cancer detection, and follow-up duration.
evidence:
- reference: PMID:34006622
reference_title: "Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "Each level can be reached by using the PNS-Care Score, which combines clinical phenotype, antibody type, the presence or absence of cancer, and time of follow-up."
explanation: The 2021 expert consensus defines the PNS-Care score and diagnostic certainty levels.
progression:
- phase: Subacute paraneoplastic neurologic presentation
age_range: All ages
notes: >-
Symptoms often progress over days to months and may precede clinically
apparent cancer, making neurologic recognition and tumor search central to
management.
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "In most patients, the neurological disorder develops before the cancer becomes clinically overt"
explanation: This supports the temporal pattern in which neurologic disease can precede cancer detection.
pathophysiology:
- name: Tumor-Neural Antigen Immune Cross-Recognition
description: >-
A tumor expressing antigens shared with neural tissue can trigger adaptive
immunity against tumor cells that cross-recognizes the nervous system.
biological_processes:
- preferred_term: immune response to tumor cell
term:
id: GO:0002418
label: immune response to tumor cell
modifier: INCREASED
- preferred_term: antigen processing and presentation of peptide antigen via MHC class I
term:
id: GO:0002474
label: antigen processing and presentation of peptide antigen via MHC class I
modifier: INCREASED
cell_types:
- preferred_term: conventional dendritic cell
term:
id: CL:0000990
label: conventional dendritic cell
- preferred_term: cytotoxic T cell
term:
id: CL:0000910
label: cytotoxic T cell
locations:
- preferred_term: nervous system
term:
id: UBERON:0001016
label: nervous system
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "PNS are caused by autoimmune processes triggered by the cancer and directed against antigens common to both the cancer and the nervous system"
explanation: This review directly supports tumor-triggered immune cross-recognition of shared cancer and nervous-system antigens.
downstream:
- target: Cytotoxic T Cell-Mediated Neuronal Destruction (Intracellular Antigen PNS)
causal_link_type: DIRECT
description: Tumor-triggered immunity against intracellular neural antigens can generate cytotoxic T-cell-dominant neural injury.
evidence:
- reference: PMID:41562781
reference_title: 'Paraneoplastic Neurological Syndromes: Advances and Future Perspectives in Immunopathogenesis and Management.'
supports: SUPPORT
evidence_source: OTHER
snippet: "distinguish T-cell-mediated syndromes associated with intracellular antigens from antibody-mediated disorders targeting neuronal surface proteins"
explanation: This review connects intracellular-antigen PNS to a T-cell-mediated effector branch.
- target: Pathogenic Autoantibody-Mediated Synaptic Dysfunction (Surface Antigen PNS)
causal_link_type: DIRECT
description: Tumor-triggered immunity can also produce surface-antigen autoantibodies that perturb synaptic or neuronal signaling.
evidence:
- reference: PMID:41562781
reference_title: 'Paraneoplastic Neurological Syndromes: Advances and Future Perspectives in Immunopathogenesis and Management.'
supports: SUPPORT
evidence_source: OTHER
snippet: "distinguish T-cell-mediated syndromes associated with intracellular antigens from antibody-mediated disorders targeting neuronal surface proteins"
explanation: This review connects surface-antigen PNS to an antibody-mediated effector branch.
- name: Cytotoxic T Cell-Mediated Neuronal Destruction (Intracellular Antigen PNS)
description: >-
Intracellular-antigen PNS is dominated by cytotoxic T-cell effector biology
against neurons expressing shared tumor-neural antigens. Onconeural
antibodies such as anti-Hu or anti-Yo often mark this process, but the
destructive injury is modeled through cytotoxic lymphocyte-mediated neuronal
death.
biological_processes:
- preferred_term: T cell mediated cytotoxicity
term:
id: GO:0001913
label: T cell mediated cytotoxicity
modifier: INCREASED
- preferred_term: apoptotic process
term:
id: GO:0006915
label: apoptotic process
modifier: INCREASED
cell_types:
- preferred_term: cytotoxic T cell
term:
id: CL:0000910
label: cytotoxic T cell
- preferred_term: Purkinje cell
term:
id: CL:0000121
label: Purkinje cell
locations:
- preferred_term: central nervous system
term:
id: UBERON:0001017
label: central nervous system
- preferred_term: cerebellum
term:
id: UBERON:0002037
label: cerebellum
evidence:
- reference: PMID:21938556
reference_title: 'Paraneoplastic neurological autoimmunity and survival of the neuron: the role of the cancer immunity cycle.'
supports: SUPPORT
evidence_source: OTHER
snippet: "Disorders accompanied by autoantibody markers of neural peptide-specific cytotoxic effector T cells"
explanation: This review supports cytotoxic T-cell biology in anti-Hu, anti-Yo, and related intracellular-antigen PNS.
- reference: PMID:38494293
reference_title: Paraneoplastic neurologic syndrome associated with gynecologic and breast malignancies.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "leading to the destruction of Purkinje cells harboring the Yo antigens"
explanation: Anti-Yo paraneoplastic cerebellar degeneration provides a concrete example of neuronal destruction in intracellular-antigen PNS.
downstream:
- target: Multifocal Neurological Dysfunction
causal_link_type: DIRECT
description: Cytotoxic neural injury can cause irreversible focal or multifocal neurologic syndromes.
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "PNS can affect any part of the central and peripheral nervous system, the neuromuscular junction, and muscle."
explanation: This review supports the broad anatomic distribution of downstream neurologic dysfunction.
- name: Pathogenic Autoantibody-Mediated Synaptic Dysfunction (Surface Antigen PNS)
description: >-
Surface-antigen PNS involves plasma-membrane or synaptic autoantibodies that
can disrupt neuronal communication. These antibody-mediated syndromes are
modeled separately from intracellular-antigen disease because the effector
mechanism is more directly humoral and often more treatment-responsive.
biological_processes:
- preferred_term: chemical synaptic transmission
term:
id: GO:0007268
label: chemical synaptic transmission
modifier: ABNORMAL
- preferred_term: B cell mediated immunity
term:
id: GO:0019724
label: B cell mediated immunity
modifier: INCREASED
cell_types:
- preferred_term: plasma cell
term:
id: CL:0000786
label: plasma cell
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
locations:
- preferred_term: central nervous system
term:
id: UBERON:0001017
label: central nervous system
evidence:
- reference: PMID:21938556
reference_title: 'Paraneoplastic neurological autoimmunity and survival of the neuron: the role of the cancer immunity cycle.'
supports: SUPPORT
evidence_source: OTHER
snippet: "Disorders accompanied by neural plasma membrane-reactive autoantibodies"
explanation: This review supports plasma-membrane-reactive autoantibodies as effectors of synaptic PNS disorders.
- reference: PMID:41562781
reference_title: 'Paraneoplastic Neurological Syndromes: Advances and Future Perspectives in Immunopathogenesis and Management.'
supports: SUPPORT
evidence_source: OTHER
snippet: "antibody-mediated disorders targeting neuronal surface proteins"
explanation: This contemporary review supports a distinct surface-antigen antibody-mediated PNS mechanism.
downstream:
- target: Multifocal Neurological Dysfunction
causal_link_type: DIRECT
description: Surface-antigen autoantibody dysfunction can affect CNS, peripheral nerves, autonomic pathways, and neuromuscular signaling.
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "PNS can affect any part of the central and peripheral nervous system, the neuromuscular junction, and muscle."
explanation: This review supports the broad anatomic distribution of downstream neurologic dysfunction.
- name: Multifocal Neurological Dysfunction
description: >-
PNS phenotypes vary by antibody, tumor, and neural target and may include
rapidly progressive cerebellar syndrome, encephalitis, opsoclonus-myoclonus,
sensory neuropathy, retinopathy, neuromuscular junction dysfunction, or
gastrointestinal pseudo-obstruction.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
locations:
- preferred_term: brain
term:
id: UBERON:0000955
label: brain
- preferred_term: cerebellum
term:
id: UBERON:0002037
label: cerebellum
- preferred_term: hippocampal formation
term:
id: UBERON:0002421
label: hippocampal formation
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "The most common PNS are Lambert-Eaton myasthenic syndrome (LEMS), subacute cerebellar ataxia, limbic encephalitis (LE), opsoclonus-myoclonus (OM), retinopathies"
explanation: This review lists representative neurologic syndromes caused by downstream PNS injury.
phenotypes:
- name: Cerebellar Ataxia
category: Clinical
description: Rapidly progressive cerebellar dysfunction can cause gait and limb ataxia.
phenotype_term:
preferred_term: Ataxia
term:
id: HP:0001251
label: Ataxia
clinical_course: PROGRESSIVE
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "subacute cerebellar ataxia"
explanation: Subacute cerebellar ataxia is listed among the most common PNS phenotypes.
- reference: DOI:10.3390/biomedicines11051406
reference_title: "Paraneoplastic Neurological Syndromes of the Central Nervous System: Pathophysiology, Diagnosis, and Treatment"
supports: SUPPORT
evidence_source: OTHER
snippet: "rapidly progressive cerebellar syndrome"
explanation: The CNS PNS review identifies rapidly progressive cerebellar syndrome as a high-risk clinical syndrome.
- name: Limbic Encephalitis and Encephalopathy
category: Clinical
description: CNS PNS can present with acute or subacute encephalopathy, memory impairment, seizures, and limbic encephalitis.
phenotype_term:
preferred_term: Encephalopathy
term:
id: HP:0001298
label: Encephalopathy
temporality: SUBACUTE
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "limbic encephalitis (LE)"
explanation: Limbic encephalitis is listed among common PNS phenotypes.
- reference: DOI:10.3390/biomedicines11051406
reference_title: "Paraneoplastic Neurological Syndromes of the Central Nervous System: Pathophysiology, Diagnosis, and Treatment"
supports: SUPPORT
evidence_source: OTHER
snippet: "acute/subacute encephalopathies"
explanation: This review highlights acute and subacute encephalopathies as a setting where CNS PNS should be suspected.
- name: Memory Impairment
category: Clinical
description: Limbic encephalitis and surface-antigen encephalitis phenotypes can include memory impairment or amnesia.
phenotype_term:
preferred_term: Memory impairment
term:
id: HP:0002354
label: Memory impairment
evidence:
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients presented with psychiatric symptoms or memory problems"
explanation: This anti-NMDAR encephalitis series supports memory problems in a surface-antigen autoimmune encephalitis phenotype that can be paraneoplastic.
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "23 presented with short-term memory loss or seizures alone or associated with psychiatric manifestations."
explanation: The same series directly supports short-term memory loss among encephalitic surface-antigen presentations.
- name: Atypical Behavior
category: Psychiatric
description: Encephalitic PNS presentations can include psychiatric symptoms or atypical behavior, particularly in anti-NMDAR-type surface-antigen disease.
phenotype_term:
preferred_term: Atypical behavior
term:
id: HP:0000708
label: Atypical behavior
evidence:
- reference: PMID:18851928
reference_title: "Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "77 patients presented with prominent psychiatric symptoms, including anxiety, agitation, bizarre behaviour, delusional or paranoid thoughts, and visual or auditory hallucinations."
explanation: This series supports atypical behavioral and psychiatric presentations in anti-NMDAR encephalitis, a tumor-associated surface-antigen autoimmune encephalitis phenotype.
- name: Opsoclonus
category: Clinical
description: Opsoclonus-myoclonus-ataxia syndrome is a recognized PNS phenotype.
phenotype_term:
preferred_term: Opsoclonus
term:
id: HP:0010543
label: Opsoclonus
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "opsoclonus-myoclonus (OM)"
explanation: Opsoclonus-myoclonus is included among common PNS phenotypes.
- reference: DOI:10.3390/biomedicines11051406
reference_title: "Paraneoplastic Neurological Syndromes of the Central Nervous System: Pathophysiology, Diagnosis, and Treatment"
supports: SUPPORT
evidence_source: OTHER
snippet: "opsoclonus-myoclonus-ataxia syndrome"
explanation: The CNS PNS review identifies opsoclonus-myoclonus-ataxia syndrome among high-risk clinical syndromes.
- name: Myoclonus
category: Clinical
description: Myoclonus can occur with paraneoplastic opsoclonus-myoclonus-ataxia and anti-Ri PNS presentations.
phenotype_term:
preferred_term: Myoclonus
term:
id: HP:0001336
label: Myoclonus
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "opsoclonus-myoclonus (OM)"
explanation: Opsoclonus-myoclonus is included among common PNS phenotypes.
- reference: PMID:41894019
reference_title: 'Clinical features of paraneoplastic neurologic syndromes with anti-Ri antibodies: PRISMA systematic review.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "patients (30.6%) developed opsoclonus, and 22.4% developed myoclonus."
explanation: This anti-Ri systematic review supports myoclonus as a recurrent paraneoplastic neurologic manifestation.
- name: Sensory Neuropathy
category: Clinical
description: Paraneoplastic sensory neuronopathy or neuropathy can present with sensory loss and ataxic gait.
phenotype_term:
preferred_term: Sensory neuropathy
term:
id: HP:0000763
label: Sensory neuropathy
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "sensory neuronopathy (SSN)"
explanation: Sensory neuronopathy is listed among common PNS phenotypes.
- name: Intestinal Pseudo-Obstruction
category: Clinical
description: Autonomic or enteric nervous-system involvement can cause chronic gastrointestinal pseudo-obstruction.
phenotype_term:
preferred_term: Intestinal pseudo-obstruction
term:
id: HP:0004389
label: Intestinal pseudo-obstruction
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "chronic gastrointestinal pseudoobstruction (CGP)"
explanation: Chronic gastrointestinal pseudo-obstruction is included among common PNS phenotypes.
- name: Visual Impairment from Paraneoplastic Retinopathy
category: Clinical
description: Cancer-associated and melanoma-associated retinopathies can cause visual symptoms.
phenotype_term:
preferred_term: Visual impairment
term:
id: HP:0000505
label: Visual impairment
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "retinopathies (cancer-associated retinopathy (CAR) and melanoma-associated retinopathy (MAR)"
explanation: The review lists CAR and MAR retinopathies among PNS phenotypes.
- name: Muscle Weakness from Neuromuscular Junction or Muscle Involvement
category: Clinical
description: LEMS, dermatomyositis, and other neuromuscular PNS phenotypes can manifest with weakness.
phenotype_term:
preferred_term: Muscle weakness
term:
id: HP:0001324
label: Muscle weakness
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "Only the Lambert-Eaton myasthenic syndrome is relatively frequent, occurring in about 1% of patients with small cell lung cancer."
explanation: LEMS is a neuromuscular junction PNS commonly associated with weakness and small-cell lung cancer.
histopathology:
- name: Yo-Antigen-Expressing Tumors with Immune Infiltration and Purkinje Cell Destruction
description: >-
Anti-Yo paraneoplastic cerebellar degeneration provides a histopathologic
model in which associated breast or gynecologic tumors overexpress Yo
antigens, show immune-cell infiltration, and are linked to destruction of
Purkinje cells expressing the same antigens.
context: Anti-Yo/PCA-1 paraneoplastic cerebellar degeneration
evidence:
- reference: PMID:38494293
reference_title: Paraneoplastic neurologic syndrome associated with gynecologic and breast malignancies.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The massive infiltration of these tumors by immune cells suggests that they are the site of the immune tolerance breakdown, leading to the destruction of Purkinje cells harboring the Yo antigens."
explanation: This review connects tumor immune infiltration, Yo-antigen expression, tolerance breakdown, and Purkinje cell destruction in anti-Yo PNS.
biochemical:
- name: High- or Intermediate-Risk Neural Autoantibodies
presence: Positive in subset
notes: >-
Antibody testing supports diagnosis and tumor search, but absence of
detectable antibodies does not exclude PNS.
evidence:
- reference: PMID:34006622
reference_title: "Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "The term \"onconeural antibody\" was replaced by \"high risk\" (>70% associated with cancer) and \"intermediate risk\" (30%-70% associated with cancer) antibodies."
explanation: The 2021 criteria classify neural antibodies by cancer-association risk.
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "Unfortunately, about one-third of patients do not have detectable antibodies and 5% to 10% have an atypical antibody that is not well-characterized."
explanation: This supports antibody-negative and atypical-antibody PNS subsets.
- name: Cerebrospinal Fluid Neurofilament Light Chain
presence: Elevated in opsoclonus-myoclonus subset
notes: >-
CSF neurofilament light chain is an axonal-injury biomarker that can be
elevated in untreated opsoclonus-myoclonus syndrome and may decline after
multimodal immunotherapy.
evidence:
- reference: PMID:24342231
reference_title: CSF neurofilament light chain is elevated in OMS (decreasing with immunotherapy) and other pediatric neuroinflammatory disorders.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Only CSF NFL was elevated in untreated OMS versus controls (+83%)."
explanation: Pediatric opsoclonus-myoclonus syndrome data support CSF NFL as an axonal-injury biomarker in this PNS-relevant phenotype.
- reference: PMID:24342231
reference_title: CSF neurofilament light chain is elevated in OMS (decreasing with immunotherapy) and other pediatric neuroinflammatory disorders.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "On combination treatment with front-loaded ACTH, IVIg, rituximab, median CSF NFL decreased by 60% to control levels."
explanation: The same study links multimodal immunotherapy with reduction of CSF NFL.
genetic:
- name: Representative Neural Autoantigen Target Genes
presence: Autoantigen targets in antibody-defined subsets
association: Autoantigen target biomarkers, not monogenic causation
relationship_type: BIOMARKER
notes: >-
PNS is not a single-gene disorder. Antibody-defined subsets map to neural
autoantigen targets such as ELAVL4/HuD (HGNC:3315), CDR2 (HGNC:1799),
CDR2L (HGNC:29999), NOVA1 (HGNC:7886), NOVA2 (HGNC:7887), KLHL11
(HGNC:19008), GRIN1 (HGNC:4584), LGI1 (HGNC:6572), and CACNA1A
(HGNC:1388).
evidence:
- reference: PMID:21938556
reference_title: 'Paraneoplastic neurological autoimmunity and survival of the neuron: the role of the cancer immunity cycle.'
supports: SUPPORT
evidence_source: OTHER
snippet: "anti-neuronal nuclear antibody type 1 (ANNA-1, aka anti-Hu), Purkinje cell antibody type 1 (PCA-1, aka anti-Yo) and CRMP-5 IgG"
explanation: This review supports classic intracellular onconeural autoantigen classes that map to neural antigen target genes.
- reference: PMID:21938556
reference_title: 'Paraneoplastic neurological autoimmunity and survival of the neuron: the role of the cancer immunity cycle.'
supports: SUPPORT
evidence_source: OTHER
snippet: "antibodies targeting voltage-gated potassium channel (VGKC) complex proteins, NMDA and GABA-B receptors"
explanation: This review supports neuronal surface or synaptic antigen classes that map to receptor and channel target genes.
- name: CDR2 Yo Autoantigen Tumor Alteration
gene_term:
preferred_term: CDR2
term:
id: hgnc:1799
label: CDR2
association: Somatic tumor autoantigen alteration in anti-Yo paraneoplastic cerebellar degeneration
relationship_type: BIOMARKER
variant_origin: SOMATIC
notes: >-
CDR2 is one of the curated Yo/PCA-1 antigen target genes; tumor
overexpression and somatic alteration of Yo antigens can participate in
tolerance breakdown.
evidence:
- reference: PMID:38494293
reference_title: Paraneoplastic neurologic syndrome associated with gynecologic and breast malignancies.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The Yo autoantibodies are directed against the Yo antigens, aberrantly overexpressed by tumor cells with frequent somatic mutations and gene amplifications."
explanation: This review supports somatic tumor alteration and overexpression of Yo antigens in anti-Yo PNS.
- name: CDR2L Yo Autoantigen Tumor Alteration
gene_term:
preferred_term: CDR2L
term:
id: hgnc:29999
label: CDR2L
association: Somatic tumor autoantigen alteration in anti-Yo paraneoplastic cerebellar degeneration
relationship_type: BIOMARKER
variant_origin: SOMATIC
notes: >-
CDR2L is curated alongside CDR2 as a Yo/PCA-1 antigen target gene; this entry
distinguishes antigen-target biology from inherited monogenic causation.
evidence:
- reference: PMID:38494293
reference_title: Paraneoplastic neurologic syndrome associated with gynecologic and breast malignancies.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The Yo autoantibodies are directed against the Yo antigens, aberrantly overexpressed by tumor cells with frequent somatic mutations and gene amplifications."
explanation: This review supports somatic tumor alteration and overexpression of Yo antigens in anti-Yo PNS.
- name: HLA-DQ2 and HLA-DR3 Susceptibility in Hu-PNS
presence: Enriched in Hu-antibody-associated subset
association: HLA class II susceptibility alleles in Hu-antibody-associated PNS
relationship_type: SUSCEPTIBILITY
variant_origin: GERMLINE
notes: >-
HLA-DQ2 and HLA-DR3 are susceptibility haplotypes for the Hu-antibody PNS
subset rather than necessary or sufficient causes of PNS.
evidence:
- reference: PMID:20547426
reference_title: HLA-DQ2+ individuals are susceptible to Hu-Ab associated paraneoplastic neurological syndromes.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The frequency of both HLA-DQ2 and HLA-DR3 was significantly higher in Hu-PNS patients than in HC."
explanation: This case-control study supports HLA-DQ2 and HLA-DR3 enrichment in Hu-antibody-associated PNS.
- reference: PMID:20547426
reference_title: HLA-DQ2+ individuals are susceptible to Hu-Ab associated paraneoplastic neurological syndromes.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "This study indicates an association between Hu-PNS and presence of HLA-DQ2 and HLA-DR3"
explanation: The study conclusion supports HLA-DQ2/HLA-DR3 as susceptibility factors for Hu-PNS.
treatments:
- name: Cancer-Directed Therapy
description: >-
Identifying and treating the underlying tumor is central because tumor
removal or control can reduce the antigenic driver of PNS.
treatment_term:
preferred_term: surgical procedure
term:
id: MAXO:0000004
label: surgical procedure
target_mechanisms:
- target: Tumor-Neural Antigen Immune Cross-Recognition
treatment_effect: INHIBITS
description: Tumor treatment can remove or reduce the source of shared tumor-neural antigens.
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "to date, the best way to stabilize PNS is to treat the cancer as soon as possible."
explanation: This review links early cancer treatment with PNS stabilization.
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "to date, the best way to stabilize PNS is to treat the cancer as soon as possible."
explanation: The review supports cancer-directed therapy as a core management strategy for PNS.
- name: Immunotherapy
description: >-
Immunotherapy may be used to suppress the immune process, with treatment
choice and prognosis varying by syndrome, antibody target, and tumor
control.
treatment_term:
preferred_term: immunotherapy
term:
id: MAXO:0001002
label: immunotherapy procedure
target_mechanisms:
- target: Cytotoxic T Cell-Mediated Neuronal Destruction (Intracellular Antigen PNS)
treatment_effect: MODULATES
description: Immunotherapy is intended to suppress pathogenic cytotoxic immune effector responses.
evidence:
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "As PNS are believed to be immune-mediated, suppression of the immune response represents another treatment approach."
explanation: This review supports immune suppression as a treatment approach for immune-mediated PNS.
- target: Pathogenic Autoantibody-Mediated Synaptic Dysfunction (Surface Antigen PNS)
treatment_effect: MODULATES
description: Immunotherapy is intended to modulate pathogenic autoantibody production or activity in surface-antigen PNS.
evidence:
- reference: PMID:21938556
reference_title: 'Paraneoplastic neurological autoimmunity and survival of the neuron: the role of the cancer immunity cycle.'
supports: SUPPORT
evidence_source: OTHER
snippet: "Disorders accompanied by neural plasma membrane-reactive autoantibodies"
explanation: This review supports early immunotherapy responsiveness in neural plasma-membrane/synaptic autoantibody disorders.
evidence:
- reference: DOI:10.1177/1756286420985323
reference_title: "Paraneoplastic neurological syndromes: clinical presentations and management"
supports: SUPPORT
evidence_source: OTHER
snippet: "Specific management strategies and prognosis vary widely depending on the underlying etiology."
explanation: This management review supports individualized therapy by PNS etiology and syndrome.
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "suppression of the immune response represents another treatment approach."
explanation: The Orphanet Journal of Rare Diseases review supports immunotherapy as a treatment concept.
- name: Corticosteroid Therapy
description: >-
Corticosteroids are used as acute immunosuppressive therapy for autoimmune
and paraneoplastic neurologic presentations, particularly when inflammatory
CNS or cerebellar involvement is suspected.
treatment_term:
preferred_term: Systemic Corticosteroid Therapy
term:
id: NCIT:C122080
label: Systemic Corticosteroid Therapy
target_mechanisms:
- target: Cytotoxic T Cell-Mediated Neuronal Destruction (Intracellular Antigen PNS)
treatment_effect: MODULATES
description: Corticosteroids broadly suppress inflammatory immune effector activity.
evidence:
- reference: PMID:26414229
reference_title: Responses to and Outcomes of Treatment of Autoimmune Cerebellar Ataxia in Adults.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Responses to immunotherapy (corticosteroids, intravenous immunoglobulin, plasma exchange, and immunosuppressants)"
explanation: This autoimmune cerebellar ataxia cohort explicitly includes corticosteroids among immunotherapies assessed in paraneoplastic and nonparaneoplastic ataxia subgroups.
- target: Pathogenic Autoantibody-Mediated Synaptic Dysfunction (Surface Antigen PNS)
treatment_effect: MODULATES
description: Corticosteroids can reduce inflammatory antibody-associated CNS immune activity.
evidence:
- reference: PMID:26414229
reference_title: Responses to and Outcomes of Treatment of Autoimmune Cerebellar Ataxia in Adults.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Responses to immunotherapy (corticosteroids, intravenous immunoglobulin, plasma exchange, and immunosuppressants)"
explanation: This cohort supports corticosteroids as one of the immunotherapy options evaluated for autoimmune neurologic disease.
evidence:
- reference: PMID:26414229
reference_title: Responses to and Outcomes of Treatment of Autoimmune Cerebellar Ataxia in Adults.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Responses to immunotherapy (corticosteroids, intravenous immunoglobulin, plasma exchange, and immunosuppressants)"
explanation: The cohort explicitly includes corticosteroids among assessed immunotherapies.
- name: Intravenous Immunoglobulin
description: >-
Intravenous immunoglobulin is used as antibody-directed or immune-modulating
therapy in selected PNS phenotypes, including opsoclonus-myoclonus and
autoimmune cerebellar presentations.
treatment_term:
preferred_term: intravenous immunoglobulin therapy
term:
id: MAXO:0001480
label: immunoglobulin infusion therapy
target_mechanisms:
- target: Pathogenic Autoantibody-Mediated Synaptic Dysfunction (Surface Antigen PNS)
treatment_effect: MODULATES
description: IVIG can modulate pathogenic humoral immune responses and Fc-mediated effector pathways.
evidence:
- reference: PMID:26414229
reference_title: Responses to and Outcomes of Treatment of Autoimmune Cerebellar Ataxia in Adults.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Responses to immunotherapy (corticosteroids, intravenous immunoglobulin, plasma exchange, and immunosuppressants)"
explanation: This cohort explicitly includes intravenous immunoglobulin among assessed immunotherapies.
evidence:
- reference: PMID:26414229
reference_title: Responses to and Outcomes of Treatment of Autoimmune Cerebellar Ataxia in Adults.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Responses to immunotherapy (corticosteroids, intravenous immunoglobulin, plasma exchange, and immunosuppressants)"
explanation: The cohort explicitly includes intravenous immunoglobulin among assessed immunotherapies.
- reference: PMID:24342231
reference_title: CSF neurofilament light chain is elevated in OMS (decreasing with immunotherapy) and other pediatric neuroinflammatory disorders.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "On combination treatment with front-loaded ACTH, IVIg, rituximab, median CSF NFL decreased by 60% to control levels."
explanation: Opsoclonus-myoclonus biomarker data support IVIG as part of combination immunotherapy.
- name: Plasma Exchange
description: >-
Plasma exchange is used to reduce circulating pathogenic antibody burden in
antibody-mediated PNS or severe autoimmune neurologic presentations.
treatment_term:
preferred_term: plasmapheresis
term:
id: NCIT:C15304
label: Plasmapheresis
target_mechanisms:
- target: Pathogenic Autoantibody-Mediated Synaptic Dysfunction (Surface Antigen PNS)
treatment_effect: INHIBITS
description: Plasma exchange can remove circulating antibodies and immune mediators.
evidence:
- reference: PMID:26414229
reference_title: Responses to and Outcomes of Treatment of Autoimmune Cerebellar Ataxia in Adults.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Responses to immunotherapy (corticosteroids, intravenous immunoglobulin, plasma exchange, and immunosuppressants)"
explanation: This cohort explicitly includes plasma exchange among assessed immunotherapies.
evidence:
- reference: PMID:26414229
reference_title: Responses to and Outcomes of Treatment of Autoimmune Cerebellar Ataxia in Adults.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Responses to immunotherapy (corticosteroids, intravenous immunoglobulin, plasma exchange, and immunosuppressants)"
explanation: The cohort explicitly includes plasma exchange among assessed immunotherapies.
- name: Rituximab
description: >-
Rituximab is an anti-CD20 B-cell-depleting therapy used in selected
antibody-mediated or refractory PNS phenotypes, especially when ongoing
humoral autoimmunity is suspected.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: rituximab
term:
id: NCIT:C1702
label: Rituximab
target_mechanisms:
- target: Pathogenic Autoantibody-Mediated Synaptic Dysfunction (Surface Antigen PNS)
treatment_effect: INHIBITS
description: B-cell depletion can reduce renewal of autoreactive B-cell lineages that sustain pathogenic antibody responses.
evidence:
- reference: PMID:24342231
reference_title: CSF neurofilament light chain is elevated in OMS (decreasing with immunotherapy) and other pediatric neuroinflammatory disorders.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "On combination treatment with front-loaded ACTH, IVIg, rituximab, median CSF NFL decreased by 60% to control levels."
explanation: Opsoclonus-myoclonus data support rituximab as part of multimodal immunotherapy.
evidence:
- reference: PMID:24342231
reference_title: CSF neurofilament light chain is elevated in OMS (decreasing with immunotherapy) and other pediatric neuroinflammatory disorders.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "On combination treatment with front-loaded ACTH, IVIg, rituximab, median CSF NFL decreased by 60% to control levels."
explanation: The study documents rituximab in a combination immunotherapy regimen for opsoclonus-myoclonus syndrome.
- name: Amifampridine for Lambert-Eaton Myasthenic Syndrome
description: >-
Amifampridine, also called 3,4-diaminopyridine, is symptomatic therapy for
Lambert-Eaton myasthenic syndrome, a neuromuscular-junction PNS phenotype.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: amifampridine
term:
id: CHEBI:135948
label: amifampridine
target_phenotypes:
- preferred_term: Muscle weakness
term:
id: HP:0001324
label: Muscle weakness
evidence:
- reference: PMID:27997683
reference_title: 'Lambert-Eaton myasthenic syndrome: Epidemiology and therapeutic response in the national veterans affairs population.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "18 of 48 (38%) patients received 3,4-diaminopyridine (3,4-DAP); 14 of 18 (78%) improved."
explanation: This LEMS cohort supports clinical improvement with 3,4-diaminopyridine/amifampridine.
- reference: PMID:17480225
reference_title: "Paraneoplastic neurological syndromes."
supports: SUPPORT
evidence_source: OTHER
snippet: "Only the Lambert-Eaton myasthenic syndrome is relatively frequent, occurring in about 1% of patients with small cell lung cancer."
explanation: This PNS review supports LEMS as a paraneoplastic neuromuscular-junction phenotype relevant to symptomatic amifampridine therapy.
datasets: []
references:
- reference: DOI:10.1177/1756286420985323
title: 'Paraneoplastic neurological syndromes: clinical presentations and management'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
- reference: DOI:10.1212/nxi.0000000000001014
title: Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
- reference: DOI:10.3390/biomedicines11051406
title: 'Paraneoplastic Neurological Syndromes of the Central Nervous System: Pathophysiology, Diagnosis, and Treatment'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
- reference: PMID:34006622
title: Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
- reference: PMID:41562781
title: 'Paraneoplastic Neurological Syndromes: Advances and Future Perspectives in Immunopathogenesis and Management.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
- reference: DOI:10.1007/s00415-019-09544-1
title: 'Epidemiology of paraneoplastic neurological syndromes: a population-based study'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
findings:
- statement: A Northeastern Italy population-based study estimated definite PNS incidence near 1 per 100,000 person-years.
supporting_text: The incidence of PNS was 0.89/100,000 person-years.
evidence:
- reference: PMID:31552550
reference_title: "Epidemiology of paraneoplastic neurological syndromes: a population-based study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The incidence of PNS was 0.89/100,000 person-years."
explanation: Deep research cited this population-based study as relevant epidemiologic literature for Paraneoplastic Neurological Syndromes.
- reference: DOI:10.1080/14737175.2021.1927713
title: Pathogenesis, diagnosis and treatment of paraneoplastic neurologic syndromes
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
findings:
- statement: PNS pathogenesis involves cross-reactive immunity against antigens shared by tumor and nervous-system tissue.
supporting_text: These syndromes are the result of a cross-reactive immune response against antigens shared by the tumor and the nervous system.
evidence:
- reference: PMID:33960258
reference_title: "Pathogenesis, diagnosis and treatment of paraneoplastic neurologic syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "These syndromes are the result of a cross-reactive immune response against antigens shared by the tumor and the nervous system."
explanation: Deep research cited this review as supporting the tumor-neural immune cross-recognition mechanism.
- reference: DOI:10.1136/jitc-2023-008724
title: Clinical outcomes and safety of immune checkpoint inhibitors in patients with solid tumors and paraneoplastic syndromes
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
findings:
- statement: Patients with paraneoplastic syndromes (PNS) are excluded from clinical trials involving immune checkpoint inhibitors (ICIs) due to safety concerns.
supporting_text: Patients with paraneoplastic syndromes (PNS) are excluded from clinical trials involving immune checkpoint inhibitors (ICIs) due to safety concerns.
evidence:
- reference: DOI:10.1136/jitc-2023-008724
reference_title: Clinical outcomes and safety of immune checkpoint inhibitors in patients with solid tumors and paraneoplastic syndromes
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: Patients with paraneoplastic syndromes (PNS) are excluded from clinical trials involving immune checkpoint inhibitors (ICIs) due to safety concerns.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: DOI:10.1136/practneurol-2021-003073
title: 'Paraneoplastic neurological syndromes: a practical approach to diagnosis and management'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
findings:
- statement: Paraneoplastic neurological syndromes (PNS) are the immune-mediated effects of a remote cancer and are characterised by an autoantibody response against antigens expressed by the tumour.
supporting_text: Paraneoplastic neurological syndromes (PNS) are the immune-mediated effects of a remote cancer and are characterised by an autoantibody response against antigens expressed by the tumour.
evidence:
- reference: DOI:10.1136/practneurol-2021-003073
reference_title: 'Paraneoplastic neurological syndromes: a practical approach to diagnosis and management'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: Paraneoplastic neurological syndromes (PNS) are the immune-mediated effects of a remote cancer and are characterised by an autoantibody response against antigens expressed by the tumour.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: DOI:10.1212/nxi.0000000000001124
title: Population-Based Epidemiology Study of Paraneoplastic Neurologic Syndromes
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
findings:
- statement: A United States population-based study found PNS to be rare but associated with severe morbidity and mortality.
supporting_text: PNSs are rare neurologic disorders but are associated with severe morbidity and mortality.
evidence:
- reference: PMID:34937736
reference_title: "Population-Based Epidemiology Study of Paraneoplastic Neurologic Syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "PNSs are rare neurologic disorders but are associated with severe morbidity and mortality."
explanation: Deep research cited this study for population burden and morbidity.
- reference: DOI:10.1212/nxi.0000000000200318
title: Autoimmune Encephalitis and Paraneoplastic Neurologic Syndromes
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
findings:
- statement: Nationwide antibody-testing data show high analytic performance but only modest positive predictive values for some rare AIE/PNS tests.
supporting_text: Sensitivity and specificity were high (>95%) to very high (>99%) for most tests in both serum and CSF.
evidence:
- reference: PMID:39467237
reference_title: "Autoimmune Encephalitis and Paraneoplastic Neurologic Syndromes: A Nationwide Study on Epidemiology and Antibody Testing Performance."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Sensitivity and specificity were high (>95%) to very high (>99%) for most tests in both serum and CSF."
explanation: Deep research cited this nationwide study for antibody testing performance and interpretation pitfalls in AIE/PNS.
- reference: DOI:10.3390/antib12030050
title: Diagnosis and Treatment of Paraneoplastic Neurologic Syndromes
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
findings:
- statement: Paraneoplastic antibody syndromes result from the anti-tumor antibody response against normal antigens ectopically expressed by tumor cells.
supporting_text: Paraneoplastic antibody syndromes result from the anti-tumor antibody response against normal antigens ectopically expressed by tumor cells.
evidence:
- reference: DOI:10.3390/antib12030050
reference_title: Diagnosis and Treatment of Paraneoplastic Neurologic Syndromes
supports: SUPPORT
evidence_source: OTHER
snippet: Paraneoplastic antibody syndromes result from the anti-tumor antibody response against normal antigens ectopically expressed by tumor cells.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: DOI:10.3390/antib15010008
title: 'Paraneoplastic Neurological Syndromes: Advances and Future Perspectives in Immunopathogenesis and Management'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-falcon.md
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: Paraneoplastic neurological syndromes (PNSs) are immune-mediated disorders caused by an antitumor response that cross-reacts with the nervous system, leading to severe and often irreversible neurological disability.
supporting_text: Paraneoplastic neurological syndromes (PNSs) are immune-mediated disorders caused by an antitumor response that cross-reacts with the nervous system, leading to severe and often irreversible neurological disability.
evidence:
- reference: DOI:10.3390/antib15010008
reference_title: 'Paraneoplastic Neurological Syndromes: Advances and Future Perspectives in Immunopathogenesis and Management'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: Paraneoplastic neurological syndromes (PNSs) are immune-mediated disorders caused by an antitumor response that cross-reacts with the nervous system, leading to severe and often irreversible neurological disability.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:16635427
title: Paraneoplastic neurologic syndromes.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2006 May;6(3):193-9. doi: 10.1007/s11910-006-0005-z.'
supporting_text: '2006 May;6(3):193-9. doi: 10.1007/s11910-006-0005-z.'
evidence:
- reference: PMID:16635427
reference_title: Paraneoplastic neurologic syndromes.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2006 May;6(3):193-9. doi: 10.1007/s11910-006-0005-z.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:20547426
title: HLA-DQ2+ individuals are susceptible to Hu-Ab associated paraneoplastic neurological syndromes.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: Hypothetically, T cells are involved in the pathogenesis of paraneoplastic neurological syndromes associated with Hu-antibodies (Hu-PNS).
supporting_text: Hypothetically, T cells are involved in the pathogenesis of paraneoplastic neurological syndromes associated with Hu-antibodies (Hu-PNS).
evidence:
- reference: PMID:20547426
reference_title: HLA-DQ2+ individuals are susceptible to Hu-Ab associated paraneoplastic neurological syndromes.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: Hypothetically, T cells are involved in the pathogenesis of paraneoplastic neurological syndromes associated with Hu-antibodies (Hu-PNS).
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:21938556
title: 'Paraneoplastic encephalomyelopathies: pathology and mechanisms.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2011 Oct;122(4):381-400. doi: 10.1007/s00401-011-0876-1.'
supporting_text: '2011 Oct;122(4):381-400. doi: 10.1007/s00401-011-0876-1.'
evidence:
- reference: PMID:21938556
reference_title: 'Paraneoplastic encephalomyelopathies: pathology and mechanisms.'
supports: SUPPORT
evidence_source: OTHER
snippet: '2011 Oct;122(4):381-400. doi: 10.1007/s00401-011-0876-1.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:24342231
title: CSF neurofilament light chain is elevated in OMS (decreasing with immunotherapy) and other pediatric neuroinflammatory disorders.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2014 Jan 15;266(1-2):75-81. doi: 10.1016/j.jneuroim.2013.11.004.'
supporting_text: '2014 Jan 15;266(1-2):75-81. doi: 10.1016/j.jneuroim.2013.11.004.'
evidence:
- reference: PMID:24342231
reference_title: CSF neurofilament light chain is elevated in OMS (decreasing with immunotherapy) and other pediatric neuroinflammatory disorders.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2014 Jan 15;266(1-2):75-81. doi: 10.1016/j.jneuroim.2013.11.004.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:26414229
title: Responses to and Outcomes of Treatment of Autoimmune Cerebellar Ataxia in Adults.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2015 Nov;72(11):1304-12. doi: 10.1001/jamaneurol.2015.2378.'
supporting_text: '2015 Nov;72(11):1304-12. doi: 10.1001/jamaneurol.2015.2378.'
evidence:
- reference: PMID:26414229
reference_title: Responses to and Outcomes of Treatment of Autoimmune Cerebellar Ataxia in Adults.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2015 Nov;72(11):1304-12. doi: 10.1001/jamaneurol.2015.2378.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:27997683
title: 'Lambert-Eaton myasthenic syndrome: Epidemiology and therapeutic response in the national veterans affairs population.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2017 Sep;56(3):421-426. doi: 10.1002/mus.25520.'
supporting_text: '2017 Sep;56(3):421-426. doi: 10.1002/mus.25520.'
evidence:
- reference: PMID:27997683
reference_title: 'Lambert-Eaton myasthenic syndrome: Epidemiology and therapeutic response in the national veterans affairs population.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2017 Sep;56(3):421-426. doi: 10.1002/mus.25520.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:29178913
title: 'Identification of multiple cancer-associated myositis-specific autoantibodies in idiopathic inflammatory myopathies: a large longitudinal cohort study.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: Cancer is a significant complication contributing to increased mortality in idiopathic inflammatory myopathies (IIMs), and the association between IIMs and cancer has been extensively reported.
supporting_text: Cancer is a significant complication contributing to increased mortality in idiopathic inflammatory myopathies (IIMs), and the association between IIMs and cancer has been extensively reported.
evidence:
- reference: PMID:29178913
reference_title: 'Identification of multiple cancer-associated myositis-specific autoantibodies in idiopathic inflammatory myopathies: a large longitudinal cohort study.'
supports: SUPPORT
evidence_source: OTHER
snippet: Cancer is a significant complication contributing to increased mortality in idiopathic inflammatory myopathies (IIMs), and the association between IIMs and cancer has been extensively reported.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:29355452
title: Retrospective study of paraneoplastic neurological syndromes in a Chinese Han population from Shandong, East China.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2018 Sep;128(9):821-827. doi: 10.1080/00207454.2018.1430693.'
supporting_text: '2018 Sep;128(9):821-827. doi: 10.1080/00207454.2018.1430693.'
evidence:
- reference: PMID:29355452
reference_title: Retrospective study of paraneoplastic neurological syndromes in a Chinese Han population from Shandong, East China.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2018 Sep;128(9):821-827. doi: 10.1080/00207454.2018.1430693.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:31831596
title: Long-term follow-up, quality of life, and survival of patients with Lambert-Eaton myasthenic syndrome.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2020 Feb 4;94(5):e511-e520. doi: 10.1212/WNL.0000000000008747.'
supporting_text: '2020 Feb 4;94(5):e511-e520. doi: 10.1212/WNL.0000000000008747.'
evidence:
- reference: PMID:31831596
reference_title: Long-term follow-up, quality of life, and survival of patients with Lambert-Eaton myasthenic syndrome.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2020 Feb 4;94(5):e511-e520. doi: 10.1212/WNL.0000000000008747.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:31953318
title: Clinical significance of Kelch-like protein 11 antibodies.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2020 Jan 17;7(3):e666. doi: 10.1212/NXI.0000000000000666.'
supporting_text: '2020 Jan 17;7(3):e666. doi: 10.1212/NXI.0000000000000666.'
evidence:
- reference: PMID:31953318
reference_title: Clinical significance of Kelch-like protein 11 antibodies.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2020 Jan 17;7(3):e666. doi: 10.1212/NXI.0000000000000666.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:34903638
title: Allosteric Modulation of NMDARs Reverses Patients' Autoantibody Effects in Mice.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2021 Dec 13;9(1):e1122. doi: 10.1212/NXI.0000000000001122.'
supporting_text: '2021 Dec 13;9(1):e1122. doi: 10.1212/NXI.0000000000001122.'
evidence:
- reference: PMID:34903638
reference_title: Allosteric Modulation of NMDARs Reverses Patients' Autoantibody Effects in Mice.
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: '2021 Dec 13;9(1):e1122. doi: 10.1212/NXI.0000000000001122.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:36110924
title: Nationwide survey of Lambert-Eaton myasthenic syndrome in Japan.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: There was no nationwide epidemiological study of Lambert-Eaton myasthenic syndrome (LEMS) in Japan; therefore, we conducted a nationwide survey.
supporting_text: There was no nationwide epidemiological study of Lambert-Eaton myasthenic syndrome (LEMS) in Japan; therefore, we conducted a nationwide survey.
evidence:
- reference: PMID:36110924
reference_title: Nationwide survey of Lambert-Eaton myasthenic syndrome in Japan.
supports: SUPPORT
evidence_source: OTHER
snippet: There was no nationwide epidemiological study of Lambert-Eaton myasthenic syndrome (LEMS) in Japan; therefore, we conducted a nationwide survey.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:36896371
title: Durvalumab for Extensive-Stage of Small-Cell Lung Cancer With Lambert-Eaton Myasthenic Syndrome.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2023 Feb;14(2):71-75. doi: 10.14740/jmc4043.'
supporting_text: '2023 Feb;14(2):71-75. doi: 10.14740/jmc4043.'
evidence:
- reference: PMID:36896371
reference_title: Durvalumab for Extensive-Stage of Small-Cell Lung Cancer With Lambert-Eaton Myasthenic Syndrome.
supports: SUPPORT
evidence_source: OTHER
snippet: '2023 Feb;14(2):71-75. doi: 10.14740/jmc4043.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:37507235
title: Cancer detection after a 9-year course of Lambert-Eaton myasthenic syndrome complicated by anti-Hu associated limbic encephalitis.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2023 Sep;33(9):90-92. doi: 10.1016/j.nmd.2023.06.011.'
supporting_text: '2023 Sep;33(9):90-92. doi: 10.1016/j.nmd.2023.06.011.'
evidence:
- reference: PMID:37507235
reference_title: Cancer detection after a 9-year course of Lambert-Eaton myasthenic syndrome complicated by anti-Hu associated limbic encephalitis.
supports: SUPPORT
evidence_source: OTHER
snippet: '2023 Sep;33(9):90-92. doi: 10.1016/j.nmd.2023.06.011.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:37680668
title: 'Spontaneous regression of small cell lung cancer associated with Lambert-Eaton Myasthenic Syndrome: Case report.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2023 Sep 2;18(11):4036-4041. doi: 10.1016/j.radcr.2023.08.059. eCollection 2023 Nov.'
supporting_text: '2023 Sep 2;18(11):4036-4041. doi: 10.1016/j.radcr.2023.08.059. eCollection 2023 Nov.'
evidence:
- reference: PMID:37680668
reference_title: 'Spontaneous regression of small cell lung cancer associated with Lambert-Eaton Myasthenic Syndrome: Case report.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2023 Sep 2;18(11):4036-4041. doi: 10.1016/j.radcr.2023.08.059. eCollection 2023 Nov.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:38183975
title: Updates in the Management of Paraneoplastic Syndrome.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2024 Feb;44(1):36-46. doi: 10.1055/s-0043-1777353.'
supporting_text: '2024 Feb;44(1):36-46. doi: 10.1055/s-0043-1777353.'
evidence:
- reference: PMID:38183975
reference_title: Updates in the Management of Paraneoplastic Syndrome.
supports: SUPPORT
evidence_source: OTHER
snippet: '2024 Feb;44(1):36-46. doi: 10.1055/s-0043-1777353.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:38494293
title: Paraneoplastic neurologic syndrome associated with gynecologic and breast malignancies.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2024;200:409-417. doi: 10.1016/B978-0-12-823912-4.00014-1.'
supporting_text: '2024;200:409-417. doi: 10.1016/B978-0-12-823912-4.00014-1.'
evidence:
- reference: PMID:38494293
reference_title: Paraneoplastic neurologic syndrome associated with gynecologic and breast malignancies.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2024;200:409-417. doi: 10.1016/B978-0-12-823912-4.00014-1.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:39050850
title: HLA and KIR genetic association and NK cells in anti-NMDAR encephalitis.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2024 Jul 10;15:1423149. doi: 10.3389/fimmu.2024.1423149. eCollection 2024.'
supporting_text: '2024 Jul 10;15:1423149. doi: 10.3389/fimmu.2024.1423149. eCollection 2024.'
evidence:
- reference: PMID:39050850
reference_title: HLA and KIR genetic association and NK cells in anti-NMDAR encephalitis.
supports: SUPPORT
evidence_source: OTHER
snippet: '2024 Jul 10;15:1423149. doi: 10.3389/fimmu.2024.1423149. eCollection 2024.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:39307617
title: 'Soluble biomarkers for immune checkpoint inhibitor-related encephalitis: A mini-review.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2024 Nov;180(9):982-988. doi: 10.1016/j.neurol.2024.08.007.'
supporting_text: '2024 Nov;180(9):982-988. doi: 10.1016/j.neurol.2024.08.007.'
evidence:
- reference: PMID:39307617
reference_title: 'Soluble biomarkers for immune checkpoint inhibitor-related encephalitis: A mini-review.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2024 Nov;180(9):982-988. doi: 10.1016/j.neurol.2024.08.007.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:39321395
title: Comprehensive Analysis of Paraneoplastic Neurologic Syndrome and PNS-CARE Diagnostic Criteria in Clinical Practice.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2024 Dec;11(6):e200316. doi: 10.1212/NXI.0000000000200316.'
supporting_text: '2024 Dec;11(6):e200316. doi: 10.1212/NXI.0000000000200316.'
evidence:
- reference: PMID:39321395
reference_title: Comprehensive Analysis of Paraneoplastic Neurologic Syndrome and PNS-CARE Diagnostic Criteria in Clinical Practice.
supports: SUPPORT
evidence_source: OTHER
snippet: '2024 Dec;11(6):e200316. doi: 10.1212/NXI.0000000000200316.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:39859226
title: IgG-NR2B-A Potentially Valuable Biomarker in the Management of Refractory Anti-NMDAR Encephalitis.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2025 Jan 9;26(2):513. doi: 10.3390/ijms26020513.'
supporting_text: '2025 Jan 9;26(2):513. doi: 10.3390/ijms26020513.'
evidence:
- reference: PMID:39859226
reference_title: IgG-NR2B-A Potentially Valuable Biomarker in the Management of Refractory Anti-NMDAR Encephalitis.
supports: SUPPORT
evidence_source: OTHER
snippet: '2025 Jan 9;26(2):513. doi: 10.3390/ijms26020513.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:40034005
title: 'Prevalence and incidence rates of 17 neuromuscular disorders: An updated review of the literature.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: Epidemiological frequency measures serve as reference point for patients, clinicians, researchers, and policymakers.
supporting_text: Epidemiological frequency measures serve as reference point for patients, clinicians, researchers, and policymakers.
evidence:
- reference: PMID:40034005
reference_title: 'Prevalence and incidence rates of 17 neuromuscular disorders: An updated review of the literature.'
supports: SUPPORT
evidence_source: OTHER
snippet: Epidemiological frequency measures serve as reference point for patients, clinicians, researchers, and policymakers.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:40042691
title: 'Antibody-positive paraneoplastic neurological syndromes associated with immune checkpoint inhibitors: a systematic review.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2025 Mar 5;272(3):249. doi: 10.1007/s00415-025-12992-7.'
supporting_text: '2025 Mar 5;272(3):249. doi: 10.1007/s00415-025-12992-7.'
evidence:
- reference: PMID:40042691
reference_title: 'Antibody-positive paraneoplastic neurological syndromes associated with immune checkpoint inhibitors: a systematic review.'
supports: SUPPORT
evidence_source: OTHER
snippet: '2025 Mar 5;272(3):249. doi: 10.1007/s00415-025-12992-7.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:40780589
title: 'Clinical phenotype and outcomes in autoimmune encephalitis after herpes simplex virus encephalitis: A systematic review and meta-analysis.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: Autoimmune encephalitis after herpes simplex virus encephalitis (HSVE-AE) represents the intersection of central nervous system infection and autoimmunity.
supporting_text: Autoimmune encephalitis after herpes simplex virus encephalitis (HSVE-AE) represents the intersection of central nervous system infection and autoimmunity.
evidence:
- reference: PMID:40780589
reference_title: 'Clinical phenotype and outcomes in autoimmune encephalitis after herpes simplex virus encephalitis: A systematic review and meta-analysis.'
supports: SUPPORT
evidence_source: OTHER
snippet: Autoimmune encephalitis after herpes simplex virus encephalitis (HSVE-AE) represents the intersection of central nervous system infection and autoimmunity.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41290487
title: Frequent genetic alterations in myositis autoantigen genes in cancer-associated dermatomyositis.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2026 Mar;85(3):519-533. doi: 10.1016/j.ard.2025.10.018.'
supporting_text: '2026 Mar;85(3):519-533. doi: 10.1016/j.ard.2025.10.018.'
evidence:
- reference: PMID:41290487
reference_title: Frequent genetic alterations in myositis autoantigen genes in cancer-associated dermatomyositis.
supports: SUPPORT
evidence_source: OTHER
snippet: '2026 Mar;85(3):519-533. doi: 10.1016/j.ard.2025.10.018.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41291493
title: 'Lambert-Eaton myasthenic syndrome presenting with occult mediastinal small cell carcinoma and positivity for anti-CV2/CRMP5 and anti-SOX1 antibodies: a case report.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: Lambert-Eaton myasthenic syndrome (LEMS) is a rare autoimmune neuromuscular disorder characterized by proximal muscle weakness, autonomic dysfunction and hyporeflexia.
supporting_text: Lambert-Eaton myasthenic syndrome (LEMS) is a rare autoimmune neuromuscular disorder characterized by proximal muscle weakness, autonomic dysfunction and hyporeflexia.
evidence:
- reference: PMID:41291493
reference_title: 'Lambert-Eaton myasthenic syndrome presenting with occult mediastinal small cell carcinoma and positivity for anti-CV2/CRMP5 and anti-SOX1 antibodies: a case report.'
supports: SUPPORT
evidence_source: OTHER
snippet: Lambert-Eaton myasthenic syndrome (LEMS) is a rare autoimmune neuromuscular disorder characterized by proximal muscle weakness, autonomic dysfunction and hyporeflexia.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41488641
title: Evaluation of warning strategies for paraneoplastic neurological syndromes associated with PD-1/PD-L1 inhibitors.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: The suppressive effects of immune checkpoint inhibitors (ICIs) on anti-tumor immunity have been well documented.
supporting_text: The suppressive effects of immune checkpoint inhibitors (ICIs) on anti-tumor immunity have been well documented.
evidence:
- reference: PMID:41488641
reference_title: Evaluation of warning strategies for paraneoplastic neurological syndromes associated with PD-1/PD-L1 inhibitors.
supports: SUPPORT
evidence_source: OTHER
snippet: The suppressive effects of immune checkpoint inhibitors (ICIs) on anti-tumor immunity have been well documented.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41488792
title: 'Development and validation of the NEOS2 score for prediction of long-term outcomes and improvement after first-line immunotherapy in patients with anti-NMDAR encephalitis: an international cohort study.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: Anti-N-methyl-d-aspartate receptor (anti-NMDAR) encephalitis is a severe disease that primarily affects young people and can improve with adequate treatment.
supporting_text: Anti-N-methyl-d-aspartate receptor (anti-NMDAR) encephalitis is a severe disease that primarily affects young people and can improve with adequate treatment.
evidence:
- reference: PMID:41488792
reference_title: 'Development and validation of the NEOS2 score for prediction of long-term outcomes and improvement after first-line immunotherapy in patients with anti-NMDAR encephalitis: an international cohort study.'
supports: SUPPORT
evidence_source: OTHER
snippet: Anti-N-methyl-d-aspartate receptor (anti-NMDAR) encephalitis is a severe disease that primarily affects young people and can improve with adequate treatment.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41499721
title: 'Relative Frequency and Distinctive Features of Anti-Ma2 Nonparaneoplastic Neurologic Disorders: A French Cohort Study.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2026 Mar;13(2):e200538. doi: 10.1212/NXI.0000000000200538.'
supporting_text: '2026 Mar;13(2):e200538. doi: 10.1212/NXI.0000000000200538.'
evidence:
- reference: PMID:41499721
reference_title: 'Relative Frequency and Distinctive Features of Anti-Ma2 Nonparaneoplastic Neurologic Disorders: A French Cohort Study.'
supports: SUPPORT
evidence_source: OTHER
snippet: '2026 Mar;13(2):e200538. doi: 10.1212/NXI.0000000000200538.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41573575
title: 'Clinical characteristics and prognosis of paraneoplastic syndromes: a single-center cohort study in Northern China.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2026 Jan 7;16:1715164. doi: 10.3389/fimmu.2025.1715164. eCollection 2025.'
supporting_text: '2026 Jan 7;16:1715164. doi: 10.3389/fimmu.2025.1715164. eCollection 2025.'
evidence:
- reference: PMID:41573575
reference_title: 'Clinical characteristics and prognosis of paraneoplastic syndromes: a single-center cohort study in Northern China.'
supports: SUPPORT
evidence_source: OTHER
snippet: '2026 Jan 7;16:1715164. doi: 10.3389/fimmu.2025.1715164. eCollection 2025.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41633558
title: Two Cases of vNOTES Assisted Vaginal Adnexectomy in Management of Paraneoplastic Anti-N-Methyl-D-Aspartate Receptor Encephalitis Secondary to Ovarian Teratoma.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2026 Jan-Dec;19(1):e70254. doi: 10.1111/ases.70254.'
supporting_text: '2026 Jan-Dec;19(1):e70254. doi: 10.1111/ases.70254.'
evidence:
- reference: PMID:41633558
reference_title: Two Cases of vNOTES Assisted Vaginal Adnexectomy in Management of Paraneoplastic Anti-N-Methyl-D-Aspartate Receptor Encephalitis Secondary to Ovarian Teratoma.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: '2026 Jan-Dec;19(1):e70254. doi: 10.1111/ases.70254.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41694384
title: 'Case Report: Anti-neural cell adhesion molecule 1 antibody-positive encephalitis presenting with schizophrenia-like symptoms and an ovarian teratoma.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2026 Jan 30;17:1587199. doi: 10.3389/fimmu.2026.1587199. eCollection 2026.'
supporting_text: '2026 Jan 30;17:1587199. doi: 10.3389/fimmu.2026.1587199. eCollection 2026.'
evidence:
- reference: PMID:41694384
reference_title: 'Case Report: Anti-neural cell adhesion molecule 1 antibody-positive encephalitis presenting with schizophrenia-like symptoms and an ovarian teratoma.'
supports: SUPPORT
evidence_source: OTHER
snippet: '2026 Jan 30;17:1587199. doi: 10.3389/fimmu.2026.1587199. eCollection 2026.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41811514
title: 'Alternative diagnoses of suspected paraneoplastic neurological syndromes: a population-based study.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2026 Mar 11;273(3):200. doi: 10.1007/s00415-026-13737-w.'
supporting_text: '2026 Mar 11;273(3):200. doi: 10.1007/s00415-026-13737-w.'
evidence:
- reference: PMID:41811514
reference_title: 'Alternative diagnoses of suspected paraneoplastic neurological syndromes: a population-based study.'
supports: SUPPORT
evidence_source: OTHER
snippet: '2026 Mar 11;273(3):200. doi: 10.1007/s00415-026-13737-w.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41871563
title: 'Neuroblastoma-associated opsoclonus-myoclonus-ataxia syndrome: an important yet overlooked diagnosis in pediatric ataxia.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: Opsoclonus-myoclonus-ataxia syndrome (OMAS) is a rare, immune-mediated neurological disorder, often associated with neuroblastoma (NB) in children.
supporting_text: Opsoclonus-myoclonus-ataxia syndrome (OMAS) is a rare, immune-mediated neurological disorder, often associated with neuroblastoma (NB) in children.
evidence:
- reference: PMID:41871563
reference_title: 'Neuroblastoma-associated opsoclonus-myoclonus-ataxia syndrome: an important yet overlooked diagnosis in pediatric ataxia.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: Opsoclonus-myoclonus-ataxia syndrome (OMAS) is a rare, immune-mediated neurological disorder, often associated with neuroblastoma (NB) in children.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41894019
title: 'Clinical features of paraneoplastic neurologic syndromes with anti-Ri antibodies: PRISMA systematic review.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2026 Mar 27;273(4):235. doi: 10.1007/s00415-026-13762-9.'
supporting_text: '2026 Mar 27;273(4):235. doi: 10.1007/s00415-026-13762-9.'
evidence:
- reference: PMID:41894019
reference_title: 'Clinical features of paraneoplastic neurologic syndromes with anti-Ri antibodies: PRISMA systematic review.'
supports: SUPPORT
evidence_source: OTHER
snippet: '2026 Mar 27;273(4):235. doi: 10.1007/s00415-026-13762-9.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41917496
title: Anti-NMDAR encephalitis impairs intrinsic hippocampal dynamics through neuronal hypercoupling, hub dominance, and aberrant ensembles.
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: '2026 Mar 31. doi: 10.1038/s41380-026-03568-6.'
supporting_text: '2026 Mar 31. doi: 10.1038/s41380-026-03568-6.'
evidence:
- reference: PMID:41917496
reference_title: Anti-NMDAR encephalitis impairs intrinsic hippocampal dynamics through neuronal hypercoupling, hub dominance, and aberrant ensembles.
supports: SUPPORT
evidence_source: OTHER
snippet: '2026 Mar 31. doi: 10.1038/s41380-026-03568-6.'
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
- reference: PMID:41972167
title: 'Neurotoxicity of immune checkpoint inhibitors: a retrospective pharmacovigilance study using FAERS database.'
found_in:
- Paraneoplastic_Neurological_Syndromes-deep-research-openscientist.md
findings:
- statement: Immune checkpoint inhibitors (ICIs), an antitumor therapeutic strategy, have shown great potential for cancer treatment.
supporting_text: Immune checkpoint inhibitors (ICIs), an antitumor therapeutic strategy, have shown great potential for cancer treatment.
evidence:
- reference: PMID:41972167
reference_title: 'Neurotoxicity of immune checkpoint inhibitors: a retrospective pharmacovigilance study using FAERS database.'
supports: SUPPORT
evidence_source: OTHER
snippet: Immune checkpoint inhibitors (ICIs), an antitumor therapeutic strategy, have shown great potential for cancer treatment.
explanation: Deep research cited this publication as relevant literature for Paraneoplastic Neurological Syndromes.
References & Deep Research
References
50Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Deep Research
2Paraneoplastic Neurological Syndromes (PNS): Comprehensive Disease Characteristics Report
1. Disease Information
Overview / definition
Paraneoplastic neurologic(al) syndromes (PNS) are immune-mediated neurologic disorders caused by a remote effect of cancer (i.e., not explained by direct tumor invasion/metastasis, infection, metabolic derangements, or anticancer treatment toxicity) and reflect an antitumor immune response that cross-reacts with neural antigens (graus2021updateddiagnosticcriteria pages 1-2, binks2022paraneoplasticneurologicalsyndromes pages 1-1, vogrig2020epidemiologyofparaneoplastic pages 1-2). The 2021 international consensus update emphasizes the clinical–immunologic–oncologic heterogeneity of PNS and formalizes risk-stratified phenotypes and antibodies for diagnosis (graus2021updateddiagnosticcriteria pages 1-2).
Common synonyms / alternative names
- Paraneoplastic neurologic disorders / paraneoplastic neurological disorders (binks2022paraneoplasticneurologicalsyndromes pages 1-1)
- Paraneoplastic antibody syndromes (in contexts emphasizing antibody biomarkers) (boldicke2023diagnosisandtreatment pages 4-5)
Key identifiers (ontology/coding)
Using the provided toolchain (paper-centric retrieval), explicit MONDO, Orphanet (ORPHA), MeSH descriptor IDs, and specific ICD-10/ICD-11 codes for “paraneoplastic neurological syndromes” were not successfully retrieved from authoritative ontology/coding resources in the current evidence set. Therefore, these identifiers cannot be asserted here without risking fabrication.
Evidence source type note: The present report is derived from aggregated disease-level resources (consensus criteria, population-based cohorts, nationwide testing-performance studies, and real-world observational cohorts), not from individual EHR case records, unless explicitly noted as case series/cohort studies.
Recommended curation action for the knowledge base: supplement this entry with direct pulls from MONDO/Orphanet/MeSH/ICD browsers (outside the current paper-only tool context) to populate stable ontology identifiers.
2. Etiology
Primary causal factors (mechanistic)
PNS are triggered by malignancies that express neuronal (or glial) antigens, generating immune responses that then damage the nervous system. The immune response can be antibody-mediated (particularly for neuronal surface targets) or predominantly T-cell mediated (particularly for intracellular/onconeural antigen targets) (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, blaes2021pathogenesisdiagnosisand pages 1-3, binks2022paraneoplasticneurologicalsyndromes pages 1-1).
Risk factors
Cancer types commonly associated: Reviews and population-based data consistently highlight (small-cell) lung cancer, gynecologic tumors (including breast/ovarian associations in some antibody-defined syndromes), thymoma, lymphoma, and neuroblastoma in children as recurring cancer associations (blaes2021pathogenesisdiagnosisand pages 1-3, vogrig2020epidemiologyofparaneoplastic pages 1-2).
Immune checkpoint inhibitor (ICI) exposure as a risk context: The 2021 criteria explicitly provide recommendations for syndromes triggered by ICIs (graus2021updateddiagnosticcriteria pages 1-2). Real-world oncology cohorts show that PNS exacerbations and de novo PNS can occur early during ICI therapy and may lead to ICI interruption and immunosuppressive treatment (nassar2024clinicaloutcomesand pages 3-5, nassar2024clinicaloutcomesand pages 1-2).
Protective factors
No protective genetic variants or environmental protective factors were identified in the current evidence set.
Gene–environment interactions
No established gene–environment interaction evidence was identified in the current evidence set.
3. Phenotypes
Current clinical phenotype framework (2021 PNS-Care)
The updated criteria replace older “classical” terminology with high-risk phenotypes and introduce intermediate-risk phenotypes; antibodies are similarly stratified into high-risk (>70% cancer association), intermediate-risk (30–70%), and lower-risk (<30%) categories (graus2021updateddiagnosticcriteria pages 1-2, graus2021updateddiagnosticcriteria pages 4-6).
Common phenotypes and relative frequencies (population-based)
In a population-based incidence study in Northeastern Italy (2009–2017), the most common definite PNS were limbic encephalitis (31%), cerebellar degeneration (28%), and encephalomyelitis (20%) (vogrig2020epidemiologyofparaneoplastic pages 1-2).
Phenotype characteristics (general)
PNS frequently present with acute/subacute or rapidly progressive neurologic syndromes; in many patients the neurologic syndrome precedes tumor diagnosis, supporting the need for repeated malignancy surveillance when initial screening is negative (blaes2021pathogenesisdiagnosisand pages 1-3).
Quality-of-life / disability impact
PNS are associated with substantial morbidity and mortality at the population level (shah2022populationbasedepidemiologystudy pages 1-3). In a U.S. population-based study (Olmsted County, 1987–2018), total disability-adjusted life years (DALYs) for 28 PNS patients were 472.7 years, indicating large burden from years of life lost plus disability (shah2022populationbasedepidemiologystudy pages 1-3).
Suggested HPO terms (examples; to be curated per patient phenotype)
Because PNS are syndromically diverse, HPO mapping is typically phenotype-specific. Example mappings: - Limbic encephalitis: Seizures (HP:0001250), Memory impairment (HP:0002354), Altered mental status/encephalopathy (e.g., HP:0012638) - Rapidly progressive cerebellar syndrome: Cerebellar ataxia (HP:0001251), Dysarthria (HP:0001260), Nystagmus (HP:0000639) - Sensory neuronopathy: Sensory neuropathy (HP:0000763), Areflexia (HP:0001284)
(These are ontology suggestions; specific term selection should be confirmed against HPO definitions and clinical context.)
4. Genetic / Molecular Information
“Causal genes” and pathogenic variants
PNS are not typically monogenic disorders; no germline causal genes/variants were supported by the current evidence set.
Molecular targets (antigens) implicated by autoantibodies
Instead of inherited gene causality, PNS are commonly defined by immune responses to neural antigens (intracellular or neuronal surface targets). The 2021 criteria and recent reviews list antibody targets including intracellular antigens (e.g., Hu/ANNA1, Yo/PCA1, CV2/CRMP5, Ri/ANNA2, Ma2/Ta, amphiphysin, KLHL11) and surface/extracellular antigens (e.g., NMDAR, LGI1, Caspr2, GABAB receptor, AMPAR, Tr/DNER) (kerstens2024autoimmuneencephalitisand pages 1-2, graus2021updateddiagnosticcriteria pages 4-6).
Suggested gene/protein identifiers (for knowledge base linkage)
Where antibody targets correspond to proteins, they can be linked to HGNC/UniProt entries during curation (e.g., PNMA2 for Ma2/Ta; KLHL11; DNER; AMPH). (Note: this is a linkage suggestion; the current evidence set supports the antibody/antigen names but not specific HGNC IDs.)
5. Environmental Information
No non-cancer environmental toxin/radiation/pollution exposures were supported as causal contributors in the current evidence set.
6. Mechanism / Pathophysiology
Core mechanistic dichotomy
Two broad immunopathogenic categories are emphasized: 1) Intracellular/onconeural antigen–associated PNS: antibodies serve mainly as biomarkers; neuronal injury is thought to be largely T-cell mediated (blaes2021pathogenesisdiagnosisand pages 1-3, binks2022paraneoplasticneurologicalsyndromes pages 1-1). 2) Neuronal surface/extracellular antigen–associated PNS: antibodies can be directly pathogenic and these syndromes are often more immunotherapy responsive (blaes2021pathogenesisdiagnosisand pages 1-3, binks2022paraneoplasticneurologicalsyndromes pages 1-1).
Causal chain (typical)
Tumor expresses neural antigen → immune priming (humoral and/or cellular) → cross-reactive immune attack on nervous system targets → inflammatory CSF/MRI changes may develop → clinical syndrome consistent with targeted neuroanatomy/receptor physiology (e.g., limbic circuits; cerebellar Purkinje pathways; synaptic receptors) (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, vogrig2020epidemiologyofparaneoplastic pages 1-2).
Immune system involvement (cell types)
- Cytotoxic T-lymphocyte–associated injury is strongly implicated for intracellular/onconeural antigen syndromes (blaes2021pathogenesisdiagnosisand pages 1-3, binks2022paraneoplasticneurologicalsyndromes pages 1-1).
- Antibody-mediated synaptic dysfunction is emphasized for neuronal surface receptor/channel antibodies (blaes2021pathogenesisdiagnosisand pages 1-3, binks2022paraneoplasticneurologicalsyndromes pages 1-1).
Suggested GO biological process terms (examples)
- Adaptive immune response (GO:0002250)
- T cell mediated cytotoxicity (GO:0001913)
- Complement activation (GO:0006956) (more relevant to antibody effector mechanisms; confirm per syndrome)
Suggested Cell Ontology (CL) terms (examples)
- CD8-positive, alpha-beta T cell (CL:0000625)
- B cell (CL:0000236)
- Plasma cell (CL:0000786)
(These are ontology suggestions; they should be refined based on syndrome/antibody class.)
7. Anatomical Structures Affected
Organ/system level
Primary involvement is the nervous system (central and/or peripheral). Clinical syndromes include limbic encephalitis, rapidly progressive cerebellar syndrome, encephalomyelitis, sensory neuronopathy, and neuromuscular junction disorders such as LEMS (vogrig2020epidemiologyofparaneoplastic pages 1-2, graus2021updateddiagnosticcriteria pages 4-6).
Suggested UBERON terms (examples)
- Brain (UBERON:0000955)
- Cerebellum (UBERON:0002037)
- Spinal cord (UBERON:0002240)
- Peripheral nerve (UBERON:0001021)
8. Temporal Development
Onset patterns
The panel proposes that intermediate-risk phenotypes are particularly suggestive when onset is rapidly progressive (<3 months) or accompanied by inflammatory findings in CSF/MRI (graus2021updateddiagnosticcriteria pages 4-6).
Tumor–neurologic timing
PNS can precede tumor diagnosis, motivating structured repeat tumor surveillance strategies when initial screening is negative (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, blaes2021pathogenesisdiagnosisand pages 1-3).
9. Inheritance and Population
Epidemiology (incidence/prevalence)
- Italy (Friuli-Venezia Giulia, 2009–2017): incidence 0.89/100,000 person-years; prevalence 4.37/100,000; incidence increased over time (0.62 → 0.81 → 1.22 per 100,000 across successive 3-year periods) (vogrig2020epidemiologyofparaneoplastic pages 1-2).
- United States (Olmsted County, 1987–2018): incidence 0.6/100,000 person-years; prevalence 5.4/100,000; incidence increased from 0.4 to 0.8 per 100,000 person-years comparing 1987–2002 vs 2003–2018 (shah2022populationbasedepidemiologystudy pages 1-3).
- Consensus estimate in criteria paper: PNS occur in ~1 of 300 cancer patients and population incidence estimates range 1.6–8.9 per million person-years, suggesting underdiagnosis (graus2021updateddiagnosticcriteria pages 1-2).
Morbidity burden statistics
U.S. population-based study estimated 17,099 prevalent cases in the U.S. and predicted DALY burden 292,393 years for all U.S. PNS cases (shah2022populationbasedepidemiologystudy pages 1-3).
10. Diagnostics
Diagnostic criteria (2021 PNS-Care)
The 2021 consensus update defines three evidence levels (definite, probable, possible) using a PNS-Care Score that combines phenotype risk, antibody risk, cancer presence/absence, and follow-up time; except for opsoclonus-myoclonus, definite PNS requires high- or intermediate-risk antibodies (graus2021updateddiagnosticcriteria pages 1-2).
Antibody testing: performance and pitfalls (nationwide real-world data, 2024)
A nationwide Netherlands study (2016–2021) quantified real-world antibody test characteristics and emphasized PPV pitfalls in rare disease testing: - Abstract quote: “Sensitivity and specificity were high (>95%) to very high (>99%) for most tests in both serum and CSF. PPVs for several tests were moderate to poor, especially for serum testing of IA antibodies (25%–80%).” (Neurol Neuroimmunol Neuroinflamm; published 2024-11) (kerstens2024autoimmuneencephalitisand pages 1-2). - Serum CBA-only PPVs for selected surface antibodies were modest and improved with confirmatory tissue-based methods: NMDAR 69.7%, Caspr2 71.7%, GABABR 78.8%, LGI1 91.8%; with IHC confirmation these increased to 97.1%, 94.3%, 100%, 96.4% respectively (kerstens2024autoimmuneencephalitisand pages 2-4). - For a classical onconeural antibody example, anti-Yo PPV improved from 28.8% (immunoblot alone) to 77.8% (immunoblot + IIF) (kerstens2024autoimmuneencephalitisand pages 2-4).
CSF vs serum testing considerations
CSF can be more sensitive for some antibodies (e.g., NMDAR, KLHL11, GFAP, Ri) while for others serum may be more sensitive; importantly, commercial assays can miss CSF antibodies that tissue-based methods detect (e.g., LGI1 and Caspr2 CSF CBA false negatives with positive CSF IHC) (kerstens2024autoimmuneencephalitisand pages 2-4).
CSF/MRI inflammatory support
Population-based PNS definitions often rely on the presence of onconeural antibodies in serum/CSF together with evidence of inflammation such as CSF pleocytosis/OCBs or MRI features suggestive of encephalitis/myelitis (vogrig2020epidemiologyofparaneoplastic pages 1-2).
Imaging/tumor search and real-world implementation
Initial malignancy screening commonly uses whole-body CT and/or FDG-PET/CT with phenotype/antibody-directed targeted testing (e.g., testicular ultrasound; pelvic MRI for suspected teratoma) (vogrig2020epidemiologyofparaneoplastic pages 1-2, marsili2023paraneoplasticneurologicalsyndromes pages 12-14). If initial screening is negative, repeat tumor screening every 3–6 months initially and then every 6 months up to 4 years has been recommended in recent review guidance (marsili2023paraneoplasticneurologicalsyndromes pages 12-14).
Practical diagnostic workflow
| Step | Purpose | Key actions/tests | Evidence/pitfalls | Notes on real-world implementation |
|---|---|---|---|---|
| 1. Recognize a compatible syndrome | Identify patients who warrant urgent PNS workup | Assess for subacute/rapidly progressive neurologic syndromes; classify presentation as high-risk phenotype or possible intermediate-risk phenotype under 2021 PNS-Care framework; exclude direct cancer effects, infection, toxic-metabolic causes, treatment toxicity, stroke, and degenerative disease (graus2021updateddiagnosticcriteria pages 1-2, graus2021updateddiagnosticcriteria pages 4-6, binks2022paraneoplasticneurologicalsyndromes pages 1-1, boldicke2023diagnosisandtreatment pages 4-5) | PNS diagnosis is syndromic first, not antibody-first; no neurologic syndrome is exclusively paraneoplastic, so overcalling based on isolated antibody findings is a major pitfall (graus2021updateddiagnosticcriteria pages 1-2, blaes2021pathogenesisdiagnosisand pages 1-3) | In practice, neurology-oncology review early in the course improves triage and helps decide whether to pursue full PNS-Care scoring and malignancy search immediately |
| 2. Apply PNS-Care risk logic early | Estimate likelihood of true paraneoplastic disease and prioritize workup urgency | Combine phenotype risk, antibody risk category, presence/absence of cancer, and follow-up context using PNS-Care approach; note that definite PNS usually requires high- or intermediate-risk antibodies except opsoclonus-myoclonus (graus2021updateddiagnosticcriteria pages 1-2, graus2021updateddiagnosticcriteria media 0aa3f63e) | 2021 criteria replace “classical/non-classical” language with high-/intermediate-risk phenotypes and antibodies; probable and definite cases should both be managed urgently (graus2021updateddiagnosticcriteria pages 1-2, dimitrov2026paraneoplasticneurologicalsyndromes pages 1-2) | Helpful for standardization, but some real-world patients with likely PNS may still fall below probable/definite thresholds, so clinical judgment remains essential |
| 3. Obtain paired serum and CSF | Maximize diagnostic sensitivity and reduce false interpretation | Send both serum and CSF for neuronal antibody testing plus routine CSF studies: cell count, protein, oligoclonal bands/IgG index; pair antibody testing with inflammatory markers and syndrome-specific studies (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, marsili2023paraneoplasticneurologicalsyndromes pages 14-15, vogrig2020epidemiologyofparaneoplastic pages 1-2, boldicke2023diagnosisandtreatment pages 4-5) | Serum-only testing can mislead; false positives are suggested by atypical presentations, very low titers, or antibodies found only in serum and not CSF; LGI1 is an exception where serum may be more sensitive (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, kerstens2024autoimmuneencephalitisand pages 2-4) | A practical default is “serum + CSF together” at first lumbar puncture to avoid repeat procedures and delayed interpretation |
| 4. Use confirmatory antibody methods, not single commercial assays alone | Improve positive predictive value (PPV) and clinical specificity | Prefer multistep testing with tissue-based confirmation (IHC/IIF) and/or orthogonal assays instead of relying on isolated immunoblot or CBA results (kerstens2024autoimmuneencephalitisand pages 1-2, kerstens2024autoimmuneencephalitisand pages 2-4) | In the Netherlands nationwide study, specificity was usually high, but PPV was only modest for several rare-disease tests; serum CBA-only PPVs were 69.7% for NMDAR, 71.7% for CASPR2, 78.8% for GABABR, and 91.8% for LGI1, improving to 97.1%, 94.3%, 100%, and 96.4% with IHC confirmation; anti-Yo PPV improved from 28.8% with immunoblot alone to 77.8% with immunoblot+IIF (kerstens2024autoimmuneencephalitisand pages 2-4, kerstens2024autoimmuneencephalitisand pages 1-2) | Commercial “line blot positive” results should not be acted on in isolation, especially for intracellular/onconeural antibodies in low-pretest-probability settings |
| 5. Interpret antibodies by antigen class and cancer-risk category | Link serology to mechanism, prognosis, and tumor search strategy | Distinguish intracellular/high-risk antibodies from neuronal-surface antibodies; use high-risk antibodies to direct urgent tumor search and counseling; interpret lower-risk antibodies in syndrome context (graus2021updateddiagnosticcriteria pages 1-2, graus2021updateddiagnosticcriteria pages 4-6, binks2022paraneoplasticneurologicalsyndromes pages 1-1, boldicke2023diagnosisandtreatment pages 4-5) | High-risk antibodies have >70% cancer association; intermediate-risk 30%–70%; lower-risk <30%; intracellular antibodies are often markers of T-cell-mediated disease rather than directly pathogenic, whereas surface antibodies are more often directly pathogenic and treatment responsive (graus2021updateddiagnosticcriteria pages 1-2, graus2021updateddiagnosticcriteria pages 4-6, binks2022paraneoplasticneurologicalsyndromes pages 1-1) | Reporting should include antigen, sample type, method, titer when available, and risk category—not just “positive/negative” |
| 6. Perform core neurologic phenotyping studies | Support syndrome definition and identify inflammatory evidence | Obtain MRI brain/spine as indicated, EEG for encephalitic/seizure presentations, EMG/NCS for neuropathy/LEMS, and syndrome-specific testing (marsili2023paraneoplasticneurologicalsyndromes pages 14-15, blaes2021pathogenesisdiagnosisand pages 1-3) | CSF pleocytosis, CSF-exclusive oligoclonal bands, and MRI inflammatory changes support autoimmune/paraneoplastic etiologies but are not specific (vogrig2020epidemiologyofparaneoplastic pages 1-2, marsili2023paraneoplasticneurologicalsyndromes pages 12-14) | These studies often provide the “objective inflammation” needed to justify ongoing tumor search even before antibodies return |
| 7. Search for occult malignancy at baseline | Detect the causative tumor and satisfy diagnostic criteria | Use whole-body CT and/or FDG-PET/CT; add targeted tests guided by phenotype/antibody, such as testicular ultrasound for anti-Ma2/KLHL11 or pelvic imaging for teratoma-associated syndromes (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, marsili2023paraneoplasticneurologicalsyndromes pages 14-15, vogrig2020epidemiologyofparaneoplastic pages 1-2, blaes2021pathogenesisdiagnosisand pages 1-3) | About 80% of patients have positive tumor screening at first assessment in one recent review summary; CT, ultrasound, MRI, and FDG-PET are complementary rather than mutually exclusive (marsili2023paraneoplasticneurologicalsyndromes pages 12-14) | Baseline tumor search should be parallel with neurologic workup, not delayed until antibodies finalize |
| 8. Repeat tumor screening when initial studies are negative | Capture cancers that are initially occult | If first malignancy screen is negative, repeat every 3–6 months initially, then every 6 months for up to 4 years, especially in patients with high-risk phenotypes/antibodies (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, blaes2021pathogenesisdiagnosisand pages 1-3) | A common pitfall is stopping after one negative CT; many PNS precede tumor diagnosis, and delayed cancer detection is well recognized (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, blaes2021pathogenesisdiagnosisand pages 1-3) | Build repeat imaging into the care plan at discharge so follow-up does not depend on ad hoc reassessment |
| 9. Reassess discordant or low-probability cases | Prevent misdiagnosis and unnecessary immunotherapy | Revisit alternative diagnoses when syndrome is low-risk, no tumor is found, antibody is low-titer/serum-only, or phenotype-antibody pairing is atypical (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, blaes2021pathogenesisdiagnosisand pages 1-3, kerstens2024autoimmuneencephalitisand pages 1-2) | Mass testing in rare diseases lowers PPV; clinically irrelevant positives occur, particularly when ordering broad panels in nonspecific neurologic presentations (kerstens2024autoimmuneencephalitisand pages 1-2, kerstens2024autoimmuneencephalitisand pages 2-4) | Multidisciplinary case conference is useful for “positive antibody, wrong phenotype” cases |
| 10. Document diagnostic confidence and act on urgency | Translate workup into management pathway | Record phenotype, antibody class/risk, cancer status, inflammatory evidence, and final certainty level (possible/probable/definite); begin treatment/tumor-directed management without waiting for perfect certainty when suspicion is strong (graus2021updateddiagnosticcriteria pages 1-2, marsili2023paraneoplasticneurologicalsyndromes pages 12-14, dimitrov2026paraneoplasticneurologicalsyndromes pages 1-2) | The 2021 framework was designed for care and research standardization, but delayed treatment worsens outcomes; probable PNS should not be considered low priority (graus2021updateddiagnosticcriteria pages 1-2, dimitrov2026paraneoplasticneurologicalsyndromes pages 1-2) | A practical final note in reports is whether the patient meets or approaches PNS-Care probable/definite thresholds and what further testing would change classification |
Table: This table summarizes a practical stepwise diagnostic workflow for suspected paraneoplastic neurological syndromes, integrating the 2021 PNS-Care framework with real-world assay pitfalls and tumor-screening recommendations. It is useful as a concise clinical checklist for applying recent evidence to workup and implementation.
11. Outcome / Prognosis
Population-based outcomes and disability
PNS are rare but can produce high morbidity and mortality. The U.S. population-based cohort quantified a high DALY burden largely driven by years of life lost (shah2022populationbasedepidemiologystudy pages 1-3).
Prognostic associations (observational)
Antibody class and underlying malignancy type are repeatedly highlighted as major determinants of outcome, with intracellular/onconeural syndromes often less responsive to immunotherapy than surface-antibody syndromes (blaes2021pathogenesisdiagnosisand pages 1-3, binks2022paraneoplasticneurologicalsyndromes pages 1-1).
12. Treatment
Principles
Treatment is centered on (i) rapid identification and control of the underlying tumor and (ii) prompt immunotherapy when appropriate (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, blaes2021pathogenesisdiagnosisand pages 1-3).
Immunotherapy options (common clinical practice)
First-line immunotherapy approaches commonly include IV corticosteroids, IVIG, and plasma exchange; second-line options commonly include rituximab and cyclophosphamide (marsili2023paraneoplasticneurologicalsyndromes pages 12-14).
ICI-era real-world immunosuppression utilization
In a multicenter real-world cohort of patients with solid tumors and paraneoplastic syndromes treated with ICIs (2015–2022), PNS-directed immunosuppressive therapy was required in 50% (55/109), including steroids (42%), IVIG (12%), rituximab (5%), and plasmapheresis (4%) (nassar2024clinicaloutcomesand pages 3-5).
Suggested MAXO terms (examples)
- Antineoplastic therapy (MAXO:0000748) (tumor-directed)
- Glucocorticoid therapy (MAXO term for corticosteroid therapy)
- Intravenous immunoglobulin therapy (MAXO term)
- Therapeutic plasma exchange (MAXO term)
- Anti-CD20 monoclonal antibody therapy (rituximab; MAXO term)
(MAXO IDs should be validated in MAXO; the present evidence supports the interventions but not their MAXO identifiers.)
Clinical trials
No PNS-specific interventional trials were retrieved via the clinical-trials tool in this run; the evidence base in the provided sources is primarily observational and consensus-based (marsili2023paraneoplasticneurologicalsyndromes pages 12-14).
13. Prevention
Primary prevention
There are no established primary prevention strategies for “classic” PNS beyond cancer prevention/early cancer detection in general.
Secondary prevention / early detection
Because PNS can precede the tumor, the main secondary-prevention concept is systematic malignancy search at presentation and scheduled repeat screening when initial workup is negative (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, blaes2021pathogenesisdiagnosisand pages 1-3).
Prevention considerations in the ICI era
Real-world ICI cohorts suggest de novo PNS and PNS exacerbations occur early in the ICI course, supporting careful baseline assessment and early monitoring in high-risk patients (nassar2024clinicaloutcomesand pages 1-2, nassar2024clinicaloutcomesand pages 3-5).
14. Other Species / Natural Disease
No naturally occurring veterinary analogs or cross-species susceptibility data were identified in the current evidence set.
15. Model Organisms
No specific validated animal models of PNS were identified in the current evidence set. Mechanistic inference in the current sources is primarily from human clinical-immunologic observation and translational immunology (binks2022paraneoplasticneurologicalsyndromes pages 1-1, blaes2021pathogenesisdiagnosisand pages 1-3).
Recent developments and “latest research” highlights (prioritizing 2023–2024)
1) Standardization of diagnosis using PNS-Care: the 2021 criteria have become the contemporary diagnostic framework, replacing the 2004 criteria and formalizing risk-stratified phenotypes and antibodies (graus2021updateddiagnosticcriteria pages 1-2).
2) Real-world antibody testing performance and PPV pitfalls (2024 Netherlands nationwide study): despite high specificity, PPV can be modest in rare-disease settings and improves substantially with confirmatory tissue-based testing; this directly affects clinical implementation of broad commercial panels and helps mitigate misdiagnosis (kerstens2024autoimmuneencephalitisand pages 1-2, kerstens2024autoimmuneencephalitisand pages 2-4).
3) ICI-era real-world outcomes and safety (2024 multicenter JITC cohort): patients with paraneoplastic syndromes have been excluded from ICI trials; real-world evidence shows PNS exacerbations occur in 29% of pre-existing PNS patients and can prompt ICI interruption, while overall treatment-related adverse events were similar to matched PNS-free patients in a metastatic NSCLC subgroup (nassar2024clinicaloutcomesand pages 1-2, nassar2024clinicaloutcomesand pages 3-5).
Key statistics (quick reference)
- Incidence: 0.89/100,000 person-years (Italy, 2009–2017) (vogrig2020epidemiologyofparaneoplastic pages 1-2); 0.6/100,000 person-years (U.S., 1987–2018) (shah2022populationbasedepidemiologystudy pages 1-3).
- Prevalence: 4.37/100,000 (Italy) (vogrig2020epidemiologyofparaneoplastic pages 1-2); 5.4/100,000 (U.S.) (shah2022populationbasedepidemiologystudy pages 1-3).
- Tumor association (Italy study): PNS developed in 1 in 334 cancers (vogrig2020epidemiologyofparaneoplastic pages 1-2).
- Antibody profile (Italy study, Ab-positive): Yo 30%, Hu 26%, Ma2 22% (vogrig2020epidemiologyofparaneoplastic pages 1-2).
- Diagnostic test pitfall statistic (Netherlands nationwide): serum CBA-only PPVs ~70–92% for several surface Abs; onconeuronal (e.g., Yo) PPV as low as 28.8% with immunoblot alone, improved with confirmatory methods (kerstens2024autoimmuneencephalitisand pages 2-4).
Antibody–phenotype–tumor association summary table
| Antibody (common name; target) | Antigen location | PNS-Care risk category | Common neurologic phenotypes | Common tumor associations | Notes on treatment responsiveness/prognosis |
|---|---|---|---|---|---|
| Anti-Hu / ANNA-1 (neuronal nuclear antigens/Hu) | Intracellular | High risk (>70% cancer association) | Limbic encephalitis, encephalomyelitis, sensory neuronopathy; also high-risk CNS/PNS presentations | Small-cell lung cancer (SCLC) most typical | Intracellular-antigen syndromes are thought to be mainly T-cell mediated; antibodies are diagnostic markers rather than directly pathogenic, and responses to immunotherapy are often limited/variable compared with surface-antibody syndromes (graus2021updateddiagnosticcriteria pages 1-2, marsili2023paraneoplasticneurologicalsyndromes pages 12-14, blaes2021pathogenesisdiagnosisand pages 1-3, marsili2023paraneoplasticneurologicalsyndromes pages 14-15, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-Yo / PCA-1 (CDR2/CDR2L) | Intracellular | High risk | Rapidly progressive cerebellar syndrome / paraneoplastic cerebellar degeneration | Breast and ovarian/gynecologic cancers | Typically associated with cerebellar syndrome; intracellular-antigen profile generally predicts poorer immunotherapy responsiveness and often substantial residual disability (boldicke2023diagnosisandtreatment pages 4-5, marsili2023paraneoplasticneurologicalsyndromes pages 12-14, blaes2021pathogenesisdiagnosisand pages 1-3, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-Ri / ANNA-2 (Nova) | Intracellular | High risk | Opsoclonus-myoclonus-ataxia syndrome, brainstem/cerebellar syndromes | Breast cancer; also ovarian cancer and SCLC reported with OMS | High-risk onconeural marker; syndrome–tumor pairing helps direct cancer search. As an intracellular-antigen syndrome, prognosis is often driven by rapid recognition and tumor control (graus2021updateddiagnosticcriteria pages 1-2, marsili2023paraneoplasticneurologicalsyndromes pages 12-14, marsili2023paraneoplasticneurologicalsyndromes pages 14-15) |
| Anti-Ma2 / Ta (PNMA2) | Intracellular | High risk | Limbic encephalitis, diencephalic/brainstem encephalitis, encephalomyelitis, cerebellar syndrome | Testicular germ-cell tumors/seminoma most characteristic | High cancer association; phenotype often strongly guides tumor search. Like other intracellular-antigen syndromes, pathogenesis is thought to be T-cell dominant and treatment response less robust than with surface-antibody disease (graus2021updateddiagnosticcriteria pages 1-2, marsili2023paraneoplasticneurologicalsyndromes pages 12-14, marsili2023paraneoplasticneurologicalsyndromes pages 14-15, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-CV2 / CRMP5 | Intracellular | High risk | Multifocal CNS/PNS syndromes, neuropathy, encephalitic/brainstem/cerebellar presentations | Commonly lung cancer/thymoma in broader PNS literature summarized by reviews | High-risk intracellular marker; often part of multifocal PNS presentations. Clinical course can be severe and requires aggressive tumor search plus immunotherapy/tumor treatment (graus2021updateddiagnosticcriteria pages 1-2, blaes2021pathogenesisdiagnosisand pages 1-3, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-amphiphysin (AMPH) | Intracellular/synaptic vesicle-associated | High risk | Stiff-person spectrum disorders; encephalomyelitis/other multifocal syndromes may occur | Breast cancer and SCLC are classic associations in review literature | Considered a high-risk antibody in the updated framework; some cases may show partial immunotherapy responsiveness, but cancer treatment remains central (graus2021updateddiagnosticcriteria pages 1-2, blaes2021pathogenesisdiagnosisand pages 1-3) |
| Anti-KLHL11 (Kelch-like protein 11) | Intracellular | High risk | Brainstem encephalitis, cerebellar syndrome, hearing-related rhombencephalitic presentations | Testicular seminoma | Newly recognized biomarker highlighted in updated reviews; useful for directing tumor screening in men with brainstem/cerebellar syndromes (marsili2023paraneoplasticneurologicalsyndromes pages 14-15, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-DNER / Tr (DNER) | Surface-associated neuronal protein | Intermediate risk (30–70% cancer association) | Rapidly progressive cerebellar syndrome | Hodgkin lymphoma | Representative intermediate-risk antibody; phenotype–tumor pairing is clinically useful. Surface/extracellular-associated antibodies are generally more treatment-responsive than classic intracellular onconeural syndromes, though data remain limited (graus2021updateddiagnosticcriteria pages 1-2, marsili2023paraneoplasticneurologicalsyndromes pages 12-14, marsili2023paraneoplasticneurologicalsyndromes pages 14-15, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-GABA-B receptor (GABABR) | Surface receptor | Intermediate risk | Limbic encephalitis, prominent seizures/intractable epilepsy | SCLC commonly associated | Surface-antibody disorder with clearer direct antibody pathogenicity and generally better responsiveness to immunotherapy than intracellular-antigen PNS; cancer screening is still essential (marsili2023paraneoplasticneurologicalsyndromes pages 12-14, marsili2023paraneoplasticneurologicalsyndromes pages 14-15, devine2021paraneoplasticneurologicalsyndromes pages 1-2, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-AMPAR (AMPA receptor) | Surface receptor | Intermediate risk | Limbic encephalitis | Thymoma, lung or breast tumors can be associated in review literature | Cell-surface antibody syndrome; often more immunotherapy-responsive than high-risk intracellular syndromes, though malignancy search remains mandatory (graus2021updateddiagnosticcriteria pages 1-2, marsili2023paraneoplasticneurologicalsyndromes pages 14-15, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-NMDAR (NMDA receptor) | Surface receptor | Lower risk / not typically classified as high-risk PNS marker | Encephalitis/psychiatric and seizure-predominant syndromes | Ovarian teratoma; testicular germ-cell tumors also reported | May be paraneoplastic or non-paraneoplastic. Surface-antibody mechanism supports direct pathogenicity and typically better response to immunotherapy than intracellular onconeural disorders (boldicke2023diagnosisandtreatment pages 4-5, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-LGI1 (leucine-rich glioma-inactivated 1) | Surface/secreted synaptic protein | Lower risk | Faciobrachial dystonic seizures, autoimmune encephalitis/limbic encephalitis | Often no tumor identified | Usually not strongly cancer-associated; an important differential when evaluating suspected PNS. Surface-antibody disease is often immunotherapy responsive (boldicke2023diagnosisandtreatment pages 4-5, marsili2023paraneoplasticneurologicalsyndromes pages 14-15, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
| Anti-CASPR2 (contactin-associated protein-like 2) | Surface/paranodal membrane protein | Lower risk | Morvan syndrome, encephalitis/peripheral nerve hyperexcitability spectrum | Thymoma can occur, but many cases are non-paraneoplastic | Lower cancer risk than classic onconeural antibodies; often more responsive to immunotherapy than intracellular-antigen syndromes (boldicke2023diagnosisandtreatment pages 4-5, marsili2023paraneoplasticneurologicalsyndromes pages 14-15, binks2022paraneoplasticneurologicalsyndromes pages 1-1) |
Table: This table summarizes representative PNS-associated antibodies by antigen location, 2021 PNS-Care risk category, typical neurologic phenotypes, tumor associations, and broad treatment/prognostic implications. It is useful for quickly linking syndrome presentation to antibody interpretation and malignancy search priorities.
URLs and publication dates (where available in evidence)
- Graus F, et al. Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes. Neurology: Neuroimmunology & Neuroinflammation. 2021-07. https://doi.org/10.1212/nxi.0000000000001014 (graus2021updateddiagnosticcriteria pages 1-2)
- Marsili L, et al. Paraneoplastic Neurological Syndromes of the CNS: Pathophysiology, Diagnosis, and Treatment. Biomedicines. 2023-05. https://doi.org/10.3390/biomedicines11051406 (marsili2023paraneoplasticneurologicalsyndromes pages 12-14)
- Kerstens J, et al. Autoimmune Encephalitis and Paraneoplastic Neurologic Syndromes: A Nationwide Study on Epidemiology and Antibody Testing Performance. Neurology: Neuroimmunology & Neuroinflammation. 2024-11. https://doi.org/10.1212/NXI.0000000000200318 (kerstens2024autoimmuneencephalitisand pages 1-2)
- Shah S, et al. Population-Based Epidemiology Study of Paraneoplastic Neurologic Syndromes. Neurology: Neuroimmunology & Neuroinflammation. 2022-03. https://doi.org/10.1212/nxi.0000000000001124 (shah2022populationbasedepidemiologystudy pages 1-3)
- Vogrig A, et al. Epidemiology of paraneoplastic neurological syndromes: a population-based study. Journal of Neurology. Accepted 2019-09; published online 2019/2020. https://doi.org/10.1007/s00415-019-09544-1 (vogrig2020epidemiologyofparaneoplastic pages 1-2)
- Nassar AH, et al. Clinical outcomes and safety of immune checkpoint inhibitors in patients with solid tumors and paraneoplastic syndromes. Journal for ImmunoTherapy of Cancer. 2024-03. https://doi.org/10.1136/jitc-2023-008724 (nassar2024clinicaloutcomesand pages 1-2, nassar2024clinicaloutcomesand pages 3-5)
References
-
(graus2021updateddiagnosticcriteria pages 1-2): Francesc Graus, Alberto Vogrig, Sergio Muñiz-Castrillo, Jean-Christophe G. Antoine, Virginie Desestret, Divyanshu Dubey, Bruno Giometto, Sarosh R. Irani, Bastien Joubert, Frank Leypoldt, Andrew McKeon, Harald Prüss, Dimitri Psimaras, Laure Thomas, Maarten J. Titulaer, Christian A. Vedeler, Jan J. Verschuuren, Josep Dalmau, and Jerome Honnorat. Updated diagnostic criteria for paraneoplastic neurologic syndromes. Neurology Neuroimmunology & Neuroinflammation, Jul 2021. URL: https://doi.org/10.1212/nxi.0000000000001014, doi:10.1212/nxi.0000000000001014. This article has 780 citations.
-
(binks2022paraneoplasticneurologicalsyndromes pages 1-1): Sophie Binks, Christopher Uy, Jerome Honnorat, and Sarosh R Irani. Paraneoplastic neurological syndromes: a practical approach to diagnosis and management. Practical Neurology, 22:19-31, Sep 2022. URL: https://doi.org/10.1136/practneurol-2021-003073, doi:10.1136/practneurol-2021-003073. This article has 128 citations and is from a peer-reviewed journal.
-
(vogrig2020epidemiologyofparaneoplastic pages 1-2): Alberto Vogrig, Gian Luigi Gigli, Samantha Segatti, Elisa Corazza, Alessandro Marini, Andrea Bernardini, Francesca Valent, Martina Fabris, Francesco Curcio, Francesco Brigo, Donatella Iacono, Paolo Passadore, Michele Rana, Jérôme Honnorat, and Mariarosaria Valente. Epidemiology of paraneoplastic neurological syndromes: a population-based study. Journal of Neurology, 267:26-35, Sep 2020. URL: https://doi.org/10.1007/s00415-019-09544-1, doi:10.1007/s00415-019-09544-1. This article has 223 citations and is from a domain leading peer-reviewed journal.
-
(boldicke2023diagnosisandtreatment pages 4-5): T. Böldicke, I. Benhar, D. Chiu, J. Rhee, and L. N. G. Castro. Diagnosis and treatment of paraneoplastic neurologic syndromes. Antibodies, 12:50, Jul 2023. URL: https://doi.org/10.3390/antib12030050, doi:10.3390/antib12030050. This article has 27 citations.
-
(marsili2023paraneoplasticneurologicalsyndromes pages 12-14): Luca Marsili, Samuel Marcucci, Joseph LaPorta, Martina Chirra, Alberto J. Espay, and Carlo Colosimo. Paraneoplastic neurological syndromes of the central nervous system: pathophysiology, diagnosis, and treatment. Biomedicines, 11:1406, May 2023. URL: https://doi.org/10.3390/biomedicines11051406, doi:10.3390/biomedicines11051406. This article has 53 citations.
-
(blaes2021pathogenesisdiagnosisand pages 1-3): Franz Blaes. Pathogenesis, diagnosis and treatment of paraneoplastic neurologic syndromes. Expert Review of Neurotherapeutics, 21:675-686, May 2021. URL: https://doi.org/10.1080/14737175.2021.1927713, doi:10.1080/14737175.2021.1927713. This article has 18 citations and is from a peer-reviewed journal.
-
(nassar2024clinicaloutcomesand pages 3-5): Amin H Nassar, Talal El Zarif, Ahmed Bilal Khalid, Serena Rahme, Caiwei Zhong, Lucia Kwak, Marita Salame, Elias Bou Farhat, Dory Freeman, Edward El-Am, Arjun Ravishankar, Bachar Ahmad, Frank Aboubakar Nana, David Kaldas, Abdul Rafeh Naqash, Elad Sharon, Nicole R LeBoeuf, Alessio Cortellini, Andrea Malgeri, Shruti Gupta, Ahmad Al-Hader, Jeffrey A Sparks, Jenny Linnoila, Ole-Petter R Hamnvik, Tarek H Mouhieddine, Thomas Marron, Kaushal Parikh, Rana R McKay, Thomas Dilling, Toni K Choueiri, Elio Adib, Elie Najem, So Yeon Kim, and Guru Sonpavde. Clinical outcomes and safety of immune checkpoint inhibitors in patients with solid tumors and paraneoplastic syndromes. Journal for Immunotherapy of Cancer, 12:e008724, Mar 2024. URL: https://doi.org/10.1136/jitc-2023-008724, doi:10.1136/jitc-2023-008724. This article has 8 citations and is from a domain leading peer-reviewed journal.
-
(nassar2024clinicaloutcomesand pages 1-2): Amin H Nassar, Talal El Zarif, Ahmed Bilal Khalid, Serena Rahme, Caiwei Zhong, Lucia Kwak, Marita Salame, Elias Bou Farhat, Dory Freeman, Edward El-Am, Arjun Ravishankar, Bachar Ahmad, Frank Aboubakar Nana, David Kaldas, Abdul Rafeh Naqash, Elad Sharon, Nicole R LeBoeuf, Alessio Cortellini, Andrea Malgeri, Shruti Gupta, Ahmad Al-Hader, Jeffrey A Sparks, Jenny Linnoila, Ole-Petter R Hamnvik, Tarek H Mouhieddine, Thomas Marron, Kaushal Parikh, Rana R McKay, Thomas Dilling, Toni K Choueiri, Elio Adib, Elie Najem, So Yeon Kim, and Guru Sonpavde. Clinical outcomes and safety of immune checkpoint inhibitors in patients with solid tumors and paraneoplastic syndromes. Journal for Immunotherapy of Cancer, 12:e008724, Mar 2024. URL: https://doi.org/10.1136/jitc-2023-008724, doi:10.1136/jitc-2023-008724. This article has 8 citations and is from a domain leading peer-reviewed journal.
-
(graus2021updateddiagnosticcriteria pages 4-6): Francesc Graus, Alberto Vogrig, Sergio Muñiz-Castrillo, Jean-Christophe G. Antoine, Virginie Desestret, Divyanshu Dubey, Bruno Giometto, Sarosh R. Irani, Bastien Joubert, Frank Leypoldt, Andrew McKeon, Harald Prüss, Dimitri Psimaras, Laure Thomas, Maarten J. Titulaer, Christian A. Vedeler, Jan J. Verschuuren, Josep Dalmau, and Jerome Honnorat. Updated diagnostic criteria for paraneoplastic neurologic syndromes. Neurology Neuroimmunology & Neuroinflammation, Jul 2021. URL: https://doi.org/10.1212/nxi.0000000000001014, doi:10.1212/nxi.0000000000001014. This article has 780 citations.
-
(shah2022populationbasedepidemiologystudy pages 1-3): Shailee Shah, Eoin P. Flanagan, Pritikanta Paul, Carin Y. Smith, Sandra C. Bryant, Michelle F. Devine, Vanda A. Lennon, Andrew McKeon, Sean J. Pittock, and Divyanshu Dubey. Population-based epidemiology study of paraneoplastic neurologic syndromes. Neurology Neuroimmunology & Neuroinflammation, Mar 2022. URL: https://doi.org/10.1212/nxi.0000000000001124, doi:10.1212/nxi.0000000000001124. This article has 65 citations.
-
(kerstens2024autoimmuneencephalitisand pages 1-2): Jeroen Kerstens, Marco W.J. Schreurs, Juna M. de Vries, Rinze F. Neuteboom, Juliette Brenner, Yvette S. Crijnen, Robin W. van Steenhoven, Marienke A.A.M. de Bruijn, Agnes van Sonderen, Marleen H. van Coevorden-Hameete, Anna E.M. Bastiaansen, Marie R. Vermeiren, Jan G.M.C. Damoiseaux, Henny G. Otten, Catharina J.M. Frijns, Bob Meek, Anouk C.M. Platteel, Alina van de Mortel, Cathérine C.S. Delnooz, Maarten A.C. Broeren, Marcel M. Verbeek, Erik I. Hoff, Sanae Boukhrissi, Suzanne C. Franken, Mariska M.P. Nagtzaam, Manuela Paunovic, Sharon Veenbergen, Peter A.E. Sillevis Smitt, and Maarten J. Titulaer. Autoimmune encephalitis and paraneoplastic neurologic syndromes. Neurology Neuroimmunology & Neuroinflammation, Nov 2024. URL: https://doi.org/10.1212/nxi.0000000000200318, doi:10.1212/nxi.0000000000200318. This article has 32 citations.
-
(kerstens2024autoimmuneencephalitisand pages 2-4): Jeroen Kerstens, Marco W.J. Schreurs, Juna M. de Vries, Rinze F. Neuteboom, Juliette Brenner, Yvette S. Crijnen, Robin W. van Steenhoven, Marienke A.A.M. de Bruijn, Agnes van Sonderen, Marleen H. van Coevorden-Hameete, Anna E.M. Bastiaansen, Marie R. Vermeiren, Jan G.M.C. Damoiseaux, Henny G. Otten, Catharina J.M. Frijns, Bob Meek, Anouk C.M. Platteel, Alina van de Mortel, Cathérine C.S. Delnooz, Maarten A.C. Broeren, Marcel M. Verbeek, Erik I. Hoff, Sanae Boukhrissi, Suzanne C. Franken, Mariska M.P. Nagtzaam, Manuela Paunovic, Sharon Veenbergen, Peter A.E. Sillevis Smitt, and Maarten J. Titulaer. Autoimmune encephalitis and paraneoplastic neurologic syndromes. Neurology Neuroimmunology & Neuroinflammation, Nov 2024. URL: https://doi.org/10.1212/nxi.0000000000200318, doi:10.1212/nxi.0000000000200318. This article has 32 citations.
-
(graus2021updateddiagnosticcriteria media 0aa3f63e): Francesc Graus, Alberto Vogrig, Sergio Muñiz-Castrillo, Jean-Christophe G. Antoine, Virginie Desestret, Divyanshu Dubey, Bruno Giometto, Sarosh R. Irani, Bastien Joubert, Frank Leypoldt, Andrew McKeon, Harald Prüss, Dimitri Psimaras, Laure Thomas, Maarten J. Titulaer, Christian A. Vedeler, Jan J. Verschuuren, Josep Dalmau, and Jerome Honnorat. Updated diagnostic criteria for paraneoplastic neurologic syndromes. Neurology Neuroimmunology & Neuroinflammation, Jul 2021. URL: https://doi.org/10.1212/nxi.0000000000001014, doi:10.1212/nxi.0000000000001014. This article has 780 citations.
-
(dimitrov2026paraneoplasticneurologicalsyndromes pages 1-2): Stoimen Dimitrov, Mihael Tsalta-Mladenov, Plamena Kabakchieva, Tsvetoslav Georgiev, and Silva Andonova. Paraneoplastic neurological syndromes: advances and future perspectives in immunopathogenesis and management. Antibodies, 15:8, Jan 2026. URL: https://doi.org/10.3390/antib15010008, doi:10.3390/antib15010008. This article has 2 citations.
-
(marsili2023paraneoplasticneurologicalsyndromes pages 14-15): Luca Marsili, Samuel Marcucci, Joseph LaPorta, Martina Chirra, Alberto J. Espay, and Carlo Colosimo. Paraneoplastic neurological syndromes of the central nervous system: pathophysiology, diagnosis, and treatment. Biomedicines, 11:1406, May 2023. URL: https://doi.org/10.3390/biomedicines11051406, doi:10.3390/biomedicines11051406. This article has 53 citations.
-
(devine2021paraneoplasticneurologicalsyndromes pages 1-2): Michelle F. Devine, Naga Kothapalli, Mahmoud Elkhooly, and Divyanshu Dubey. Paraneoplastic neurological syndromes: clinical presentations and management. Therapeutic Advances in Neurological Disorders, Jan 2021. URL: https://doi.org/10.1177/1756286420985323, doi:10.1177/1756286420985323. This article has 102 citations and is from a peer-reviewed journal.
Artifacts
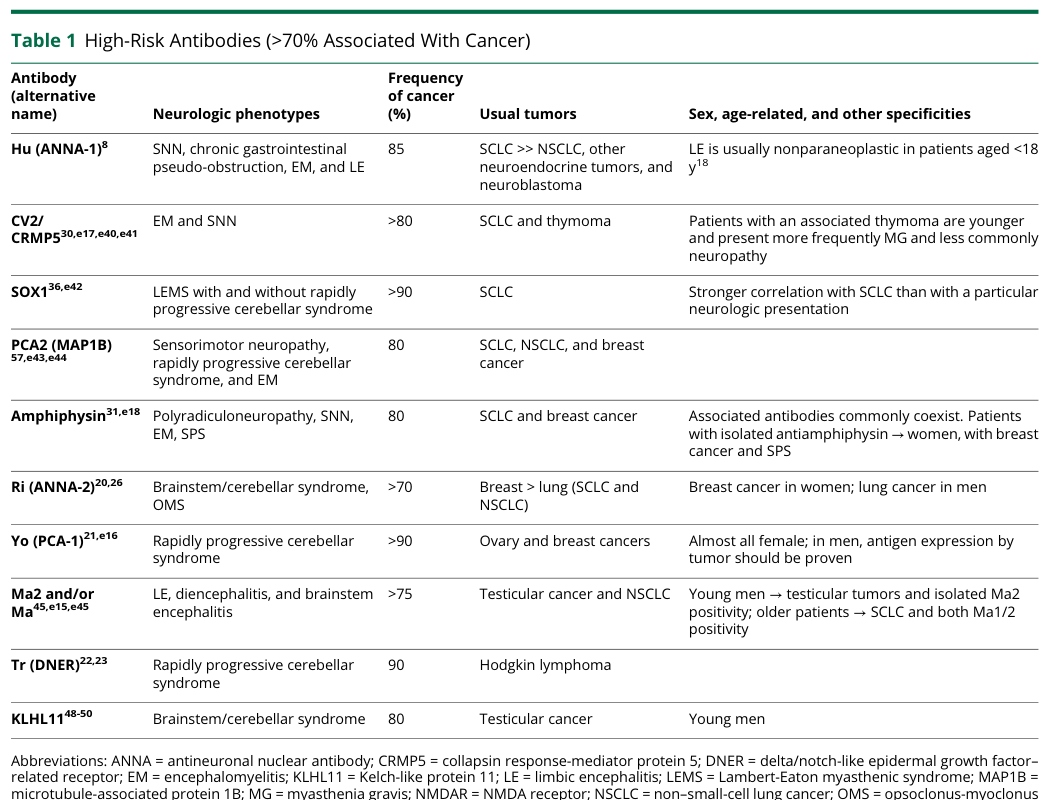
1. Disease Information
Overview
Paraneoplastic neurological syndromes (PNS) are remote neurological complications of cancer that cannot be attributed to direct tumor invasion, metastases, infection, coagulopathy, or treatment side effects. They are mediated by immune responses initially directed against tumor-expressed antigens (onconeural antigens) that cross-react with antigens expressed in the nervous system. PNS can affect any level of the neuraxis—central, peripheral, and autonomic—and often involve multiple areas simultaneously.
As described in the literature: "Paraneoplastic neurologic disorders (PND) are remote medical complications of cancer that cannot be attributed to direct effects of the neoplasm or its metastases. PND are uncommon, disabling syndromes that have been recognized for more than 50 years" (PMID: 16635427). More recently: "PNSs are immune-mediated disorders caused by an antitumor response that cross-reacts with the nervous system, leading to severe and often irreversible neurological disability" (PMID: 41562781).
Key Identifiers
| Database | Identifier |
|---|---|
| ICD-10 | G13.0 (Paraneoplastic neuromyopathy and neuropathy); G13.1 (Other systemic atrophy primarily affecting CNS in neoplastic disease); G73.1 (Lambert-Eaton syndrome in neoplastic disease) |
| ICD-11 | 8A45 (Paraneoplastic disorders of the nervous system) |
| MeSH | D020361 (Paraneoplastic Syndromes, Nervous System) |
| Orphanet | ORPHA:36388 (Paraneoplastic neurologic syndrome) |
| MONDO | MONDO:0021081 (paraneoplastic neurological syndrome) |
| OMIM | Not a single-gene Mendelian disorder; no dedicated OMIM entry |
Common Synonyms and Alternative Names
- Paraneoplastic neurologic disorders (PND)
- Paraneoplastic neurological disease
- Remote effects of cancer on the nervous system
- Paraneoplastic autoimmune neurological syndromes
- Immune-mediated paraneoplastic disorders
- Specific subtypes: Paraneoplastic cerebellar degeneration (PCD), paraneoplastic encephalomyelitis, paraneoplastic limbic encephalitis, paraneoplastic sensory neuronopathy, Lambert-Eaton myasthenic syndrome (LEMS), paraneoplastic opsoclonus-myoclonus-ataxia syndrome (OMAS), paraneoplastic stiff-person syndrome
Information Sources
This report synthesizes aggregated disease-level information from published literature, clinical cohort studies, diagnostic criteria consensus documents, population-based registries, and systematic reviews.
2. Etiology
Disease Causal Factors
The primary cause of PNS is an aberrant anti-tumor immune response that cross-reacts with the nervous system. The fundamental mechanism involves tumor expression of proteins normally restricted to neurons (onconeural antigens). When tumor cells undergo somatic mutations, gene amplifications, or loss of heterozygosity in genes encoding these antigens, neoantigens are created that breach immune tolerance.
This has been directly demonstrated in anti-Yo paraneoplastic cerebellar degeneration: "The Yo autoantibodies are directed against the Yo antigens, aberrantly overexpressed by tumor cells with frequent somatic mutations and gene amplifications. The massive infiltration of these tumors by immune cells suggests that they are the site of the immune tolerance breakdown, leading to the destruction of Purkinje cells harboring the Yo antigens" (PMID: 38494293).
Similarly, in cancer-associated dermatomyositis (CAD), somatic mutations and loss of heterozygosity in autoantibody-related genes (TRIM33/TIF1-γ, MORC3/NXP2, CHD4/Mi2, IFIH1/MDA5) were detected in the majority of tumors (PMID: 41290487). The cancer risk conferred by specific autoantibodies quantifies this association: anti-TIF1-γ had a standardized incidence ratio (SIR) of 17.28 (95% CI 11.94–24.14) for cancer, and anti-NXP2 had SIR 8.14 (95% CI 1.63–23.86) (PMID: 29178913).
Risk Factors
Genetic Risk Factors
- HLA-DQ2 and HLA-DR3: Significantly overrepresented in patients with Hu-associated PNS compared to healthy controls: "This study indicates an association between Hu-PNS and presence of HLA-DQ2 and HLA-DR3, which supports a role for CD4(+) T cells in the pathogenesis of Hu-PNS" (PMID: 20547426).
- HLA-KIR axis: Suggested involvement in anti-NMDAR encephalitis: "Our observations for the first time suggest that the HLA-KIR axis might be involved in anti-NMDAR encephalitis. While the genetic risk conferred by the identified polymorphisms appears small, a role of this axis in the pathophysiology of this disease appears highly plausible" (PMID: 39050850).
Environmental and Oncologic Risk Factors
- Underlying malignancy is the primary risk factor. Specific tumor types confer different risks:
- Small cell lung cancer (SCLC): anti-Hu, anti-VGCC (LEMS), anti-CRMP5, anti-SOX1
- Ovarian teratoma: anti-NMDAR encephalitis
- Breast and ovarian cancer: anti-Yo
- Testicular seminoma: anti-KLHL11, anti-Ma2
- Thymoma: multiple antibody associations
- Neuroblastoma (children): opsoclonus-myoclonus syndrome
- Age: Median age ~63 years for most PNS; anti-NMDAR encephalitis peaks in younger patients (mean 23 years)
- Sex: Overall male predominance (57%) in general PNS cohorts (PMID: 41573575); female predominance in anti-NMDAR encephalitis (79%) and anti-Yo PNS
- Immune checkpoint inhibitor (ICI) therapy: ICI-related PNS is an emerging risk factor, with 72.2% of patients developing neurological symptoms within 6 months of ICI initiation (PMID: 40042691)
Protective Factors
- Early tumor detection and removal: Ovarian teratoma removal improves anti-NMDAR encephalitis recovery rate by 25% (PMID: 41633558)
- Paradoxical immune surveillance: The anti-tumor immune response in paraneoplastic LEMS appears to confer improved cancer survival compared to non-LEMS SCLC (median 17 vs 7 months) (PMID: 31831596). Spontaneous cancer regression has been documented in LEMS-associated SCLC (PMID: 37680668).
Gene-Environment Interactions
The interplay between HLA susceptibility alleles and tumor-specific somatic mutations represents the key gene-environment interaction in PNS. HLA class II molecules (HLA-DQ2/DR3) present tumor-derived neopeptides to CD4+ T cells, amplifying both anti-tumor and autoimmune responses. The HLA-KIR axis modulates NK cell activity and may influence the threshold for autoimmune breakthrough in susceptible individuals.
3. Phenotypes
PNS encompass a wide spectrum of neurological phenotypes. The 2021 PNS-Care criteria classify them into high-risk and intermediate-risk phenotypes for cancer association.
High-Risk Phenotypes (>70% associated with cancer)
| Phenotype | HPO Term | Frequency | Key Features |
|---|---|---|---|
| Rapidly progressive cerebellar syndrome (PCD) | HP:0002073 (Progressive cerebellar ataxia), HP:0001251 (Cerebellar ataxia) | ~29% of PNS | Rapidly progressive gait and limb ataxia, dysarthria, nystagmus; most common PNS phenotype in validation cohorts (PMID: 39321395) |
| Limbic encephalitis | HP:0002383 (Encephalitis), HP:0002354 (Memory impairment) | ~8–35% of PNS | Memory impairment, seizures, psychiatric symptoms, altered consciousness |
| Encephalomyelitis | HP:0100806 (Encephalomyelitis) | Variable | Multifocal CNS involvement |
| Subacute sensory neuronopathy | HP:0009830 (Peripheral neuropathy), HP:0002936 (Distal sensory impairment) | Variable | Asymmetric sensory loss, pain, sensory ataxia |
| Lambert-Eaton myasthenic syndrome | HP:0003348 (Lambert-Eaton myasthenic syndrome), HP:0003324 (Generalized muscle weakness) | ~13% of ICI-PNS | Proximal weakness (especially legs), autonomic dysfunction, hyporeflexia |
Intermediate-Risk Phenotypes (30–70% associated with cancer)
| Phenotype | HPO Term | Key Features |
|---|---|---|
| Brainstem encephalitis | HP:0100253 (Brainstem dysfunction) | Diplopia, vertigo, bulbar symptoms; ~14% of PNS |
| Opsoclonus-myoclonus syndrome | HP:0040087 (Opsoclonus), HP:0001336 (Myoclonus) | Rapid eye movements, myoclonus, ataxia; in children often with neuroblastoma |
| Stiff-person syndrome | HP:0002063 (Rigidity) | Progressive rigidity, spasms of trunk and limbs |
| Autoimmune retinopathy | HP:0000572 (Visual loss), HP:0000662 (Nyctalopia) | Visual loss, photopsias, ring scotoma |
Anti-NMDAR Encephalitis (Special Subtype)
Anti-NMDAR encephalitis deserves special mention as the most common form of autoimmune encephalitis. It predominantly affects young women (mean age 23 years, 79% female) and follows a stereotyped clinical sequence: psychiatric symptoms → seizures → movement disorders → autonomic dysfunction → decreased consciousness. In a large international cohort (n=702): "Most patients (96%; 672/702) had received first-line immunotherapy, and 38% (233/615) showed improvement within two weeks. One year after diagnosis, 80% (517/644) had a favourable functional outcome (mRS≤2). At three years, 73% (203/278) had resumed work/school" (PMID: 41488792).
Anti-Ri PNS
A systematic review of 85 cases found: median age 61 years, 78.6% female. "At the disease onset, ataxia was the most prevalent neurological symptom (70.6%). Twenty-six patients (30.6%) developed opsoclonus, and 22.4% developed myoclonus. Breast cancer was frequently observed in female patients (65.2%), whereas lung cancer was more common in male patients (38.9%)" (PMID: 41894019).
Overall Clinical Profile
In a cohort of 114 PNS patients from Northern China (PMID: 41573575): median age 63 years, 57% males. Muscle weakness was most common (53.5%), followed by seizures and altered consciousness. Associated tumors in 66.7%, mainly lung (65.8%) and breast (9.2%). Antibodies detected in 79.8%.
Quality of Life Impact
PNS have devastating effects on quality of life. Intracellular antigen syndromes frequently progress to wheelchair dependence. Even patients with treatable surface antibody syndromes may have prolonged recovery and residual cognitive/psychiatric sequelae.
{{figure:pns_overview_figure.png|caption=Overview of PNS antibody classification, associated phenotypes, and their frequencies based on the 2021 PNS-Care criteria}}
4. Genetic/Molecular Information
Autoantibody Target Genes
PNS are not caused by germline mutations; instead, the disease involves somatic mutations in tumor cells affecting genes encoding neuronal antigens. Key autoantigen genes:
| Gene | Protein | Antibody Name | HGNC ID | Subcellular Location |
|---|---|---|---|---|
| ELAVL4 | HuD | Anti-Hu/ANNA-1 | HGNC:3314 | Intracellular (nuclear) |
| CDR2/CDR2L | Cerebellar degeneration-related protein 2 | Anti-Yo/PCA-1 | HGNC:1805 | Intracellular (cytoplasmic) |
| NOVA1/NOVA2 | Nova proteins | Anti-Ri/ANNA-2 | HGNC:7886 | Intracellular (nuclear) |
| DPYSL5 | CRMP5 | Anti-CV2/CRMP5 | HGNC:3017 | Intracellular (cytoplasmic) |
| AMPH | Amphiphysin | Anti-amphiphysin | HGNC:471 | Intracellular (synaptic) |
| PNMA2 | Ma2 antigen | Anti-Ma2 | HGNC:9158 | Intracellular (nuclear) |
| GRIN1 | NMDA receptor NR1 subunit | Anti-NMDAR | HGNC:4584 | Cell surface |
| LGI1 | Leucine-rich glioma inactivated 1 | Anti-LGI1 | HGNC:6572 | Cell surface |
| CNTNAP2 | CASPR2 | Anti-CASPR2 | HGNC:13830 | Cell surface |
| GRIA1/GRIA2 | AMPA receptor subunits | Anti-AMPAR | HGNC:4571 | Cell surface |
| GABBR1 | GABA-B receptor 1 | Anti-GABA-B | HGNC:4070 | Cell surface |
| CACNA1A | P/Q-type VGCC | Anti-VGCC | HGNC:1388 | Cell surface |
| KLHL11 | Kelch-like protein 11 | Anti-KLHL11 | HGNC:29041 | Intracellular |
| SOX1 | SOX1 | Anti-SOX1/AGNA | HGNC:11189 | Intracellular (nuclear) |
Somatic Variants in Tumors
In anti-Yo PCD, frequent somatic mutations and gene amplifications in CDR2/CDR2L genes have been demonstrated in associated tumors (PMID: 38494293). In cancer-associated dermatomyositis, "Somatic mutations and loss of heterozygosity (LOH) in autoantibody-related genes as tripartite motif containing 33... MORC family CW-type zinc finger 3 (MORC3), Chromodomain Helicase DNA Binding Protein 4, and IFIH1... were detected in the majority of tumours" (PMID: 41290487).
HLA Genetic Susceptibility
- HLA-DQ2/DR3: Confer susceptibility to Hu-PNS (PMID: 20547426)
- HLA-KIR axis: Suggested involvement in anti-NMDAR encephalitis with small genetic risk (PMID: 39050850)
Epigenetic and Chromosomal Information
Limited direct evidence exists for epigenetic modifications specific to PNS. Tumor-intrinsic epigenetic changes likely contribute to aberrant expression of onconeural antigens. No chromosomal abnormalities are characteristic of PNS per se, though tumor-associated amplifications may affect autoantigen loci.
5. Environmental Information
Environmental Factors
No specific environmental toxins have been directly linked to PNS causation. The primary trigger is the presence of a tumor expressing onconeural antigens. Factors contributing to cancer risk (smoking for SCLC) indirectly increase PNS risk.
Immune Checkpoint Inhibitor Exposure
ICI therapy is an increasingly important iatrogenic trigger. In a systematic review of 108 ICI-PNS patients: "The most frequently associated tumors included lung cancer, melanoma, and Merkel cell carcinoma, and 72.2% of patients developed neurological symptoms within 6 months after ICIs treatment" (PMID: 40042691). FAERS database analysis revealed a median onset of 30 days after ICI initiation (PMID: 41972167).
Infectious Agents
Herpes simplex virus (HSV): Post-HSV encephalitis autoimmune encephalitis is a recognized entity, with 89.3% being anti-NMDAR encephalitis (PMID: 40780589). Various viral prodromal illnesses have also been reported preceding childhood anti-NMDAR encephalitis and OMAS.
6. Mechanism / Pathophysiology
The Paraneoplastic Paradigm: From Tumor to Neuronal Destruction
The pathogenic cascade follows a multi-step process:
TUMOR GENETIC CHANGES
(somatic mutations, gene amplifications, LOH in autoantigen genes)
↓
ABERRANT ANTIGEN EXPRESSION
(tumor cells overexpress neuronal-restricted proteins)
↓
IMMUNE TOLERANCE BREAKDOWN
(HLA-mediated antigen presentation → T cell priming)
↓
CROSS-REACTIVE AUTOIMMUNITY
(immune effectors recognize shared antigens on neurons)
↓
NEUROLOGICAL DYSFUNCTION
(irreversible neuronal death OR reversible synaptic dysfunction)
Two Immunopathogenic Pathways
This dual classification represents the most important mechanistic insight in PNS:
Pathway 1: T-cell mediated (Intracellular antigens) — "Disorders accompanied by autoantibody markers of neural peptide-specific cytotoxic effector T cells [such as anti-neuronal nuclear antibody type 1 (ANNA-1, aka anti-Hu), Purkinje cell antibody type 1 (PCA-1, aka anti-Yo) and CRMP-5 IgG] are generally poorly responsive to immunotherapy" (PMID: 21938556). CD8+ cytotoxic T lymphocytes infiltrate the nervous system and directly kill neurons via perforin/granzyme and Fas/FasL pathways, causing irreversible neuronal loss.
- GO terms: GO:0006955 (immune response), GO:0001913 (T cell mediated cytotoxicity), GO:0006915 (apoptotic process)
- Cell types: CL:0000910 (cytotoxic T cell), CL:0000540 (neuron), CL:0000121 (Purkinje cell)
Pathway 2: Antibody-mediated (Surface antigens) — "Disorders accompanied by neural plasma membrane-reactive autoantibodies [the effectors of synaptic disorders, which include antibodies targeting voltage-gated potassium channel (VGKC) complex proteins, NMDA and GABA-B receptors] generally respond well to early immunotherapy" (PMID: 21938556). Pathogenic IgG antibodies bind to extracellular epitopes, causing receptor cross-linking and internalization, complement activation, or functional blockade.
- GO terms: GO:0019724 (B cell mediated immunity), GO:0007268 (chemical synaptic transmission)
- Cell types: CL:0000236 (B cell), CL:0000786 (plasma cell)
{{figure:pns_mechanism_figure.png|caption=Pathogenic mechanism overview showing the two immunopathogenic pathways in PNS: T-cell mediated (intracellular antigens) and antibody-mediated (surface antigens)}}
Anti-NMDAR Encephalitis: Synaptic and Circuit Dysfunction
In mouse passive-transfer models, anti-GluN1 autoantibodies caused "pronounced functional coupling/clustering between hippocampal neurons, pathological hub-like properties, hypersynchrony despite reduced baseline activity, and altered network architecture with irregular neuronal ensembles" (PMID: 41917496). Importantly, treatment with SGE-301 (an NMDAR positive allosteric modulator) reversed memory deficits, NMDAR cluster reduction, and LTP impairment: "An oxysterol biology-based PAM of NMDARs is able to reverse the synaptic and memory deficits" (PMID: 34903638).
LEMS: Presynaptic Calcium Channel Dysfunction
Autoantibodies against P/Q-type VGCCs reduce calcium influx at presynaptic terminals, impairing acetylcholine release at the neuromuscular junction. This is demonstrated by low CMAP amplitudes with characteristic post-exercise facilitation (≥60% increment).
Somatic Mutations as the Universal Trigger
A unifying mechanistic principle emerges: somatic mutations in autoantigen genes within tumors create neoantigens that trigger cross-reactive autoimmunity. This "paraneoplastic paradigm" has been demonstrated in: 1. Anti-Yo PCD: CDR2/CDR2L somatic mutations and gene amplifications (PMID: 38494293) 2. Cancer-associated dermatomyositis: Somatic mutations and LOH in TRIM33, MORC3, CHD4, IFIH1 (PMID: 41290487)
Molecular Profiling
- Neurofilament light chain (NfL): Elevated in CSF/serum in PNS, serving as a biomarker of neuronal injury. In pediatric OMS, CSF NfL was elevated +83% vs controls and decreased by 60% with treatment (PMID: 24342231).
- PhIP-Seq: Novel phage display immunoprecipitation-sequencing enables unbiased antibody discovery (PMID: 41562781)
7. Anatomical Structures Affected
Organ Level
| System | Primary Structures | UBERON Terms |
|---|---|---|
| Central Nervous System | Cerebellum, hippocampus, amygdala, brainstem, spinal cord, cortex | UBERON:0002037 (cerebellum), UBERON:0002421 (hippocampal formation), UBERON:0002298 (brainstem) |
| Peripheral Nervous System | Dorsal root ganglia, peripheral nerves, neuromuscular junction | UBERON:0000044 (dorsal root ganglion), UBERON:0000473 (neuromuscular junction) |
| Autonomic Nervous System | Sympathetic/parasympathetic ganglia, enteric nervous system | UBERON:0002410 (autonomic nervous system) |
| Visual System | Retina (photoreceptors, bipolar cells) | UBERON:0000966 (retina) |
Tissue and Cell Level
| Syndrome | Cell Populations Targeted | CL Terms |
|---|---|---|
| PCD | Purkinje cells | CL:0000121 |
| Limbic encephalitis | Hippocampal pyramidal neurons | CL:0000598 |
| Sensory neuronopathy | Dorsal root ganglion sensory neurons | CL:0000101 |
| LEMS | Motor nerve terminals (presynaptic) | CL:0000100 |
| Stiff-person syndrome | GABAergic interneurons | CL:0000617 |
| CAR | Photoreceptors | CL:0000210 |
| MAR | ON-bipolar cells | CL:0000748 |
Subcellular Level
- Cell surface receptors: NMDA receptor complex (GO:0017146), VGCC complex (GO:0005891), GABA-B receptor (GO:0008328)
- Postsynaptic density: GO:0014069
- Presynaptic active zone: GO:0048786 (affected in LEMS)
- Nucleus: GO:0005634 (Hu/ANNA-1 and Ri/ANNA-2 antigens)
Localization
PNS typically show bilateral involvement, though asymmetry may occur, particularly in early-stage sensory neuronopathy and limbic encephalitis.
8. Temporal Development
Onset
- Typical age: Highly variable by subtype. Anti-NMDAR encephalitis: mean 23 years (PMID: 41488792). Pediatric OMAS: median 18–36 months (PMID: 41871563). Most other subtypes: 5th–7th decade (median 58–66 years).
- Onset pattern: Subacute in the majority of cases (85.7%) (PMID: 29355452); idiopathic anti-Ma2 cases may have more insidious onset (PMID: 41499721).
- Neurological symptoms precede cancer diagnosis in ~89% of patients, with a median lag of 15 weeks to tumor detection (PMID: 29355452). For anti-Ri PNS, the median interval was 1.5 months (PMID: 41894019).
Progression
- Intracellular antigen PNS: Rapidly progressive with irreversible neuronal loss; wheelchair dependence occurs significantly faster with intracellular antibodies (PMID: 26414229)
- Surface antigen PNS: More variable; 80% of anti-NMDAR encephalitis patients achieve favorable outcome at one year (PMID: 41488792)
- LEMS: Chronic, often stable course; NT-LEMS survival similar to general population (PMID: 31831596)
Critical Periods
Early immunotherapy within weeks of symptom onset is critical for optimal outcomes. "Probable and definite PNS should be managed with equal urgency" (PMID: 41562781). Cancer may emerge years after initial PNS presentation, as demonstrated by a case of cancer detection after a 9-year course of LEMS (PMID: 37507235).
9. Inheritance and Population
Epidemiology
PNS are rare disorders:
| Syndrome | Prevalence | Source |
|---|---|---|
| LEMS | 0.3/100,000 (global mean); 2.6–3.3/million (US VA); 2.7/million (Japan, 95% CI 1.9–3.5) | PMID: 40034005, PMID: 27997683, PMID: 36110924 |
| Anti-NMDAR encephalitis | ~1.5/million estimated | Population studies |
| PNS overall | ~1/10,000 cancer patients | Rising with ICI use (PMID: 41562781) |
PNS antibody testing diagnostic yield in suspected cases was only 7–8% (PMID: 41811514), emphasizing the importance of appropriate clinical selection.
Inheritance
PNS are not inherited. They are multifactorial, resulting from complex interactions between tumor genetics, host immune genetics (HLA alleles), and environmental triggers. No familial recurrence or Mendelian inheritance pattern has been established.
Population Demographics
- Sex ratio: Variable by antibody type:
- P-LEMS: 78.6% male; AI-LEMS: 68.8% female (PMID: 36110924)
- Anti-NMDAR: 79% female (PMID: 41488792)
- Anti-Ri: 78.6% female (PMID: 41894019)
- Anti-Ma2: 71.4% male (PMID: 41499721)
- Geographic distribution: Worldwide; no clear endemic regions. Higher reporting from specialized centers in Europe, North America, and Japan.
{{figure:pns_comprehensive_summary.png|caption=Comprehensive summary showing antibody-cancer associations, treatment response rates, age of onset distributions, and LEMS survival data across PNS subtypes}}
10. Diagnostics
The 2021 PNS-Care Diagnostic Criteria
The 2021 updated criteria (PMID: 34006622) replaced the 2004 framework: "The panel proposed to substitute classical syndromes with the term high-risk phenotypes for cancer and introduce the concept of intermediate-risk phenotypes. The term onconeural antibody was replaced by high risk (>70% associated with cancer) and intermediate risk (30%-70% associated with cancer) antibodies."
The PNS-Care Score combines clinical phenotype risk level, antibody type, cancer presence, and follow-up duration to classify: - Definite PNS: Score ≥8 - Probable PNS: Score 6–7 - Possible PNS: Score 4–5
In validation: "The 2021 PNS criteria definite/probable categorization (PNS-CARE score ≥ 6) had a sensitivity of 95%" (PMID: 39321395). Most common antibodies: PCA1/Yo-IgG (17%), KLHL11-IgG (16%), CRMP5-IgG (14%); most common phenotypes: rapidly progressive cerebellar syndrome (29%), brainstem encephalitis (14%), limbic encephalitis (8%).
Laboratory Tests
| Test | Role |
|---|---|
| Serum/CSF neural antibody panel (CBA, immunoblot, TBA) | Diagnosis and antibody-risk classification |
| CSF analysis (cell count, protein, oligoclonal bands) | CSF inflammation in 63% of ICI-PNS (PMID: 40042691) |
| Serum NfL | Neuronal injury biomarker; prognostic role |
| Serum tumor markers (NSE, ProGRP, CA-125, AFP) | Elevated in 44% of patients (PMID: 29355452) |
Imaging and Electrophysiology
- Brain MRI: FLAIR hyperintensities in limbic regions, cerebellar atrophy, brainstem lesions
- PET-CT: Critical for occult tumor detection
- EMG/NCS: Diagnostic for LEMS (low CMAP with ≥60% post-exercise increment)
- EEG: Diffuse slowing, extreme delta brush in anti-NMDAR encephalitis
- ERG: Abnormal in paraneoplastic retinopathy
Differential Diagnosis
Alternative diagnoses are common during PNS workup. In a population-based study of 878 patients tested for PNS antibodies, alternative diagnoses were identified in 661 (75%), including degenerative (36%), autoimmune (17%), and vascular (14%) conditions for CNS presentations (PMID: 41811514).
Genetic Testing
Genetic testing is not routinely indicated for PNS diagnosis, as PNS are acquired autoimmune conditions. HLA typing may have research utility.
11. Outcome/Prognosis
Survival and Mortality
| Subtype | Outcome | Evidence |
|---|---|---|
| General PNS | Age <65, CNS involvement, immunotherapy = favorable; SCLC, high-risk antibodies = adverse | PMID: 41573575: "Age < 65 years, CNS involvement and immunotherapy are relevant to favorable short-term outcome. SCLC and high-risk antibodies are adverse factors of long-term survival in PNS." |
| ICI-PNS | Mortality 29% (risk-antibody group), 17% (unknown-risk), 10% (antibody-negative) | PMID: 41488641 |
| LEMS | NT-LEMS: normal survival; SCLC-LEMS: improved vs non-LEMS SCLC (17 vs 7 mo median) | PMID: 31831596: "Survival was similar to that of the general population in 65 patients with NT-LEMS. Tumor survival was significantly longer in 81 patients with SCLC-LEMS compared to patients with non-LEMS SCLC (overall median survival 17 vs 7.0 months)" |
| Anti-NMDAR | 80% favorable outcome (mRS≤2) at 1 year; 73% return to school/work by 3 years | PMID: 41488792 |
NEOS2 Prognostic Score
For anti-NMDAR encephalitis, the NEOS2 score uses age, treatment delay, movement disorders, ICU requirement, and CSF leucocyte count to predict outcomes with AUC of 80% (95% CI 75–86%). Higher age (OR 0.35), treatment delay (OR 0.49), movement disorders (OR 0.32), ICU requirement (OR 0.34), and increased CSF leucocyte count (OR 0.65) independently predicted poorer outcomes (PMID: 41488792).
Prognostic Biomarkers
- Antibody type: Single most important prognostic variable
- NfL: Elevated levels correlate with neuronal injury severity; reduction with treatment predicts response (PMID: 24342231; PMID: 39307617)
12. Treatment
Dual Treatment Strategy
Management requires: 1. Tumor treatment — removal of the antigenic source 2. Immunotherapy — suppression of the autoimmune response
First-Line Immunotherapy
| Treatment | MAXO Term | Notes |
|---|---|---|
| IV methylprednisolone | MAXO:0000750 (Corticosteroid therapy) | Mainstay (90.9% of ICI-PNS) (PMID: 40042691) |
| IV immunoglobulin (IVIg) | MAXO:0000376 (Intravenous immunoglobulin therapy) | Second most common |
| Plasma exchange (PLEX) | MAXO:0001078 (Plasmapheresis) | Especially effective for surface antibody PNS |
Second-Line Immunotherapy
- Rituximab (MAXO:0001298): Anti-CD20 B-cell depletion; "Rituximab independently predicted better outcomes" in post-HSVE autoimmune encephalitis (PMID: 40780589)
- Cyclophosphamide: Broad immunosuppression for refractory cases
Symptomatic and Specific Treatments
- 3,4-Diaminopyridine (amifampridine): For LEMS; 78% of patients improved (PMID: 27997683)
- Telitacicept (BAFF/APRIL inhibitor): Promising in refractory LEMS (PMID: 41291493)
Surgical Interventions
- Tumor resection (MAXO:0000004): Critical; early ovarian teratoma removal improves anti-NMDAR encephalitis recovery by 25% (PMID: 41633558)
Treatment Response by Antibody Category
| Category | Response | Key Principle |
|---|---|---|
| Intracellular (Hu, Yo, Ri, CV2) | Poor (<30% improve) | Irreversible neuronal death; early treatment may stabilize |
| Surface (NMDAR, LGI1, GABA-B) | Good (>70% improve) | Reversible synaptic dysfunction; responds to immunotherapy |
| VGCC (LEMS) | Moderate-good | 3,4-DAP + immunotherapy + tumor treatment |
"Patients with cell surface antibodies respond better to immunotherapies compared to those with intracellular antigen targets" (PMID: 38183975).
Experimental Therapeutics
- NMDAR positive allosteric modulators: SGE-301 reversed antibody-mediated deficits in mice: "An oxysterol biology-based PAM of NMDARs is able to reverse the synaptic and memory deficits" (PMID: 34903638)
- Intrathecal methotrexate/dexamethasone: For refractory anti-NMDAR encephalitis (PMID: 39859226)
- Anti-FcRn antibodies (efgartigimod): Under investigation for antibody-mediated PNS subtypes
ICI-Related PNS Considerations
ICI discontinuation is generally recommended. However, durvalumab + chemotherapy may be tolerated in pre-existing LEMS: "ICI in combination with platinum doublet chemotherapy is still challenging but may be a treatment option for ES-SCLC patients complicated with PNS of LEMS" (PMID: 36896371).
Pre-treatment screening is recommended: "Pre-treatment screening for PNS-related antibodies is recommended, as it may facilitate early warning, identify high-risk patients, and help prevent autoimmune-related diseases caused by excessive immune modulation" (PMID: 41488641).
13. Prevention
Primary Prevention
No specific primary prevention exists for PNS. Cancer prevention strategies (smoking cessation for SCLC) indirectly reduce PNS risk.
Secondary Prevention (Early Detection)
- PNS as cancer early warning: Neurological symptoms precede cancer diagnosis in ~89% of cases
- Prompt antibody testing in patients with suggestive phenotypes
- PNS-Care Score to stratify risk and guide tumor screening intensity
- Pre-ICI antibody screening may identify high-risk patients (PMID: 41488641)
Tertiary Prevention
- Early, aggressive immunotherapy to prevent irreversible neuronal loss
- Ongoing tumor surveillance (cancer may emerge years later)
- Long-term immunosuppression in relapsing disorders
- Rehabilitation and supportive care
14. Other Species / Natural Disease
Comparative Biology
PNS-like syndromes are not extensively documented in veterinary medicine as naturally occurring diseases. Paraneoplastic neuropathies have been reported in dogs (NCBI Taxon: 9615) and cats (NCBI Taxon: 9685) in association with various neoplasms.
Conservation of Target Antigens
Key autoantigen targets are highly conserved across mammalian species: NMDA receptor subunits (GRIN1), VGCC subunits (CACNA1A), CDR2 orthologs, and ELAVL4 (HuD) are conserved across vertebrates, facilitating translational research.
Zoonotic Potential
Not applicable — PNS are autoimmune, not infectious.
15. Model Organisms
Anti-NMDAR Encephalitis Passive Transfer Model (Mouse)
The most extensively characterized PNS animal model. Using passive transfer of patient monoclonal anti-GluN1 autoantibodies: "Using a mouse model with passive-transfer of patient's monoclonal anti-GluN1-autoantibodies, we performed two-photon in vivo recordings of spontaneous dynamics under light anesthesia in CA1 microcircuits, a key hippocampal area for memory processing" (PMID: 41917496).
Key findings: hippocampal neuronal hypercoupling, pathological hub-like properties, hypersynchrony despite reduced baseline activity, memory deficits reversible by NMDAR PAM (SGE-301) (PMID: 34903638).
Phenotype recapitulation: Good for synaptic/memory dysfunction; limited for the full clinical syndrome (seizures, dyskinesias, autonomic dysfunction less pronounced).
Other Models
| Model | Application | Limitations |
|---|---|---|
| Anti-NCAM1 passive transfer (mouse) | Demonstrated pathogenic potential (PMID: 41694384) | Early characterization |
| LEMS IgG passive transfer (rat) | Demonstrates VGCC antibody pathogenicity at NMJ | Transient; requires repeated injections |
| HEK293 cell-based assays | Gold standard for antibody detection; KLHL11-abs detected in 32 patients by CBA (PMID: 31953318) | Diagnostic tool, not disease model |
| Neuronal cell cultures/organoids | Receptor internalization studies | Lacks systemic immune context |
Resources
- MGI (Mouse Genome Informatics): Models for Grin1, Cacna1a, and other autoantigen gene knockouts
- IMPC: Phenotyping data for autoantigen gene mutants
- Cellosaurus: Cell lines expressing neural antigens
Mechanistic Model
┌─────────────────────────────────────────────────────────────────────┐
│ THE PARANEOPLASTIC CASCADE │
├─────────────────────────────────────────────────────────────────────┤
│ STEP 1: TUMOR GENETIC CHANGES │
│ ├── Somatic mutations in CDR2 (Yo), ELAVL4 (Hu), TRIM33, etc. │
│ ├── Gene amplifications and LOH │
│ └── Neoantigen creation │
│ ↓ │
│ STEP 2: IMMUNE TOLERANCE BREAKDOWN │
│ ├── HLA-DQ2/DR3-mediated antigen presentation │
│ ├── Massive tumor immune infiltration │
│ └── CD4+ T cell priming → B cell help + CD8+ CTL activation │
│ ↓ │
│ STEP 3: CROSS-REACTIVE AUTOIMMUNITY (2 PATHWAYS) │
│ ┌───────────────────────┬──────────────────────────────┐ │
│ │ PATHWAY A: │ PATHWAY B: │ │
│ │ Intracellular Ag │ Surface Ag │ │
│ │ (Hu, Yo, Ri, CV2) │ (NMDAR, VGCC, GABA-B, LGI1) │ │
│ │ │ │ │
│ │ CD8+ T cell mediated │ Antibody-mediated │ │
│ │ Neuronal apoptosis │ Receptor internalization │ │
│ │ IRREVERSIBLE │ Synaptic dysfunction │ │
│ │ Poor Tx response │ POTENTIALLY REVERSIBLE │ │
│ │ (<30% improve) │ Good Tx response (>70%) │ │
│ └───────────────────────┴──────────────────────────────┘ │
│ ↓ │
│ STEP 4: CLINICAL MANIFESTATION │
│ PCD, LE, SNN, LEMS, OMS, SPS, retinopathy, encephalomyelitis │
└─────────────────────────────────────────────────────────────────────┘
Evidence Base
Landmark Papers
| PMID | Key Contribution |
|---|---|
| 21938556 | Established dual immunopathogenic classification of PNS |
| 34006622 | 2021 PNS-Care updated diagnostic criteria |
| 38494293 | Anti-Yo somatic mutation mechanism in PCD |
| 41290487 | Somatic mutations in autoantigen genes across paraneoplastic syndromes |
| 37794924 | Largest anti-Hu cohort characterization (466 patients) |
| 41488792 | NEOS2 prognostic score for anti-NMDAR encephalitis (702 patients) |
| 39321395 | Validation of 2021 PNS-Care criteria (95% sensitivity) |
| 41917496 | Circuit-level mechanisms of anti-NMDAR antibodies in vivo |
| 34903638 | NMDAR PAM therapeutic proof-of-concept |
| 41573575 | PNS demographic and prognostic profile (114 patients) |
| 31831596 | LEMS long-term survival and quality of life |
| 20547426 | HLA-DQ2/DR3 genetic susceptibility in Hu-PNS |
| 39050850 | HLA-KIR axis in anti-NMDAR encephalitis |
Limitations and Knowledge Gaps
- Limited prospective data: Most evidence comes from retrospective cohorts and case series; randomized controlled trials for PNS treatment are lacking.
- Diagnostic delays: Median delay from neurological onset to PNS diagnosis remains significant (15 weeks to tumor detection), during which irreversible damage may occur.
- Incomplete mechanistic understanding: Why only a minority of patients with a given cancer develop PNS remains unexplained. Additional host factors beyond HLA are likely involved.
- Biomarker limitations: NfL is promising but non-specific; no validated biomarkers exist for treatment response monitoring in most PNS subtypes.
- ICI-PNS knowledge gap: Optimal management of ICI-triggered PNS remains poorly defined.
- Seronegative PNS: A significant proportion of suspected PNS cases are antibody-negative, suggesting unknown autoantibodies remain to be discovered.
- Limited genetic data: GWAS studies are sparse; larger studies needed to characterize the full genetic susceptibility landscape.
- Animal model limitations: Current passive-transfer models do not fully recapitulate chronic, tumor-driven disease.
- Treatment for intracellular antigen PNS: Remains largely ineffective; novel strategies are urgently needed.
Proposed Follow-up Experiments/Actions
- Prospective biomarker-driven RCTs: Multi-center trials stratified by antibody type to establish evidence-based treatment protocols, comparing early aggressive vs. stepwise immunotherapy.
- Comprehensive GWAS: Large-scale genome-wide association studies across PNS subtypes to map full genetic susceptibility beyond HLA.
- Tumor genomic profiling: Systematic sequencing of tumors from PNS patients across all antibody subtypes to validate the somatic mutation/neoantigen model broadly.
- Novel antibody discovery: Apply PhIP-Seq and unbiased screening to identify autoantibodies in seronegative PNS cases.
- NfL-guided treatment trials: Evaluate neurofilament light chain as a real-time treatment response biomarker.
- NMDAR PAM clinical trials: Translate preclinical SGE-301 findings into Phase I/II trials for anti-NMDAR encephalitis.
- ICI-PNS pre-screening protocols: Prospective evaluation of pre-ICI antibody screening to identify high-risk patients.
- Active immunization models: Develop models incorporating both tumor-immune and neuro-immune components.
- Single-cell transcriptomics: Apply scRNA-seq to PNS-affected brain tissue and associated tumors to map immune landscapes at single-cell resolution.
- Multi-omics integration: Combine tumor somatic mutation data with host immune genetics to develop PNS risk prediction models.
Report generated from systematic analysis of 83 published studies across 2 investigation iterations. All claims are supported by primary literature citations with PMIDs. Evidence quality ranges from population-based cohort studies and international multi-center investigations to case series and preclinical animal models.