Osteonecrosis
Osteonecrosis (also known as avascular necrosis, aseptic necrosis, or ischemic bone necrosis) is the death of bone tissue resulting from a disruption of its blood supply. Loss of perfusion produces ischemic death of osteocytes and bone marrow cells; the necrotic bone fails to repair, weakens structurally, and ultimately fractures and collapses, leading to secondary degenerative joint disease. The femoral head is the classic and most commonly affected site (osteonecrosis of the femoral head, ONFH), where it is a leading cause of total hip arthroplasty in young and middle-aged adults, but osteonecrosis also affects the humeral head, femoral condyles, talus, and other epiphyseal/subchondral regions. Osteonecrosis is etiologically heterogeneous: it can be traumatic (vascular disruption after fracture or dislocation) or non-traumatic. The two dominant non-traumatic causes are glucocorticoid exposure and heavy alcohol use; other recognized causes include sickle cell disease, dysbaric (Caisson) exposure in deep-sea divers, coagulopathy/lipid dysregulation, and idiopathic disease. A unifying pathophysiologic theme across etiologies is microvascular/endothelial injury and impaired angiogenesis-osteogenesis coupling, converging on subchondral ischemia and collapse.
Ask OpenScientist
Ask a research question about Osteonecrosis. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Subtypes
5Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Pathophysiology
5Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Pathograph
- Target 'Secondary osteoarthritis' (from 'Subchondral fracture and femoral head collapse') not found in named elements
Phenotypes
5Musculoskeletal 1
Show evidence (1 reference)
Nervous System 1
Show evidence (1 reference)
Other 3
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Genetic Associations
1Show evidence (1 reference)
Medical Actions
5Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Environmental Factors
4Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Biochemical Markers
1Show evidence (1 reference)
Clinical Trials
2Show evidence (1 reference)
Show evidence (1 reference)
Source YAML
click to showname: Osteonecrosis
creation_date: "2026-06-15T00:00:00Z"
category: Complex
description: >
Osteonecrosis (also known as avascular necrosis, aseptic necrosis, or ischemic
bone necrosis) is the death of bone tissue resulting from a disruption of its
blood supply. Loss of perfusion produces ischemic death of osteocytes and bone
marrow cells; the necrotic bone fails to repair, weakens structurally, and
ultimately fractures and collapses, leading to secondary degenerative joint
disease. The femoral head is the classic and most commonly affected site
(osteonecrosis of the femoral head, ONFH), where it is a leading cause of total
hip arthroplasty in young and middle-aged adults, but osteonecrosis also affects
the humeral head, femoral condyles, talus, and other epiphyseal/subchondral
regions. Osteonecrosis is etiologically heterogeneous: it can be traumatic
(vascular disruption after fracture or dislocation) or non-traumatic. The two
dominant non-traumatic causes are glucocorticoid exposure and heavy alcohol use;
other recognized causes include sickle cell disease, dysbaric (Caisson) exposure
in deep-sea divers, coagulopathy/lipid dysregulation, and idiopathic disease.
A unifying pathophysiologic theme across etiologies is microvascular/endothelial
injury and impaired angiogenesis-osteogenesis coupling, converging on subchondral
ischemia and collapse.
disease_term:
preferred_term: osteonecrosis
term:
id: MONDO:0005380
label: osteonecrosis
parents:
- Bone disease
- Ischemic disease
synonyms:
- Avascular necrosis
- Aseptic necrosis of bone
- Ischemic bone necrosis
- Bone infarction
- Osteonecrosis of the femoral head
- ONFH
- AVN
has_subtypes:
- name: Corticosteroid-induced
display_name: Glucocorticoid-associated osteonecrosis
description: >
The most common type of non-traumatic osteonecrosis, caused by glucocorticoid
exposure. The ARCO research classification requires a history of glucocorticoid
use greater than 2 g of prednisolone-equivalent within a 3-month period, with
osteonecrosis diagnosed within 2 years and no other major risk factor. Risk is
dose-dependent. Glucocorticoids promote marrow adipogenesis, lipotoxicity,
endothelial dysfunction, and impaired H-type vessel formation.
evidence:
- reference: PMID:30348552
reference_title: "Etiologic Classification Criteria of ARCO on Femoral Head Osteonecrosis Part 1: Glucocorticoid-Associated Osteonecrosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "patients should have a history of glucocorticoid use >2 g of \nprednisolone or its equivalent within a 3-month period; (2) osteonecrosis should \nbe diagnosed within 2 years after glucocorticoid usage, and (3) patients should \nnot have other risk factor(s) besides glucocorticoids."
explanation: ARCO consensus etiologic classification criteria defining glucocorticoid-associated ONFH as a distinct subtype.
- name: Alcohol-associated
display_name: Alcohol-associated osteonecrosis
description: >
Non-traumatic osteonecrosis attributed to heavy alcohol consumption. The ARCO
research classification uses a threshold of more than 320 g/week of alcohol with
diagnosis within 1 year and no other major risk factor. Alcohol accounts for a
large share (roughly one third to nearly half) of non-traumatic ONFH cases in
Asia. Implicated mechanisms include alcohol metabolite toxicity, oxidative
stress, and lipid dysregulation.
evidence:
- reference: PMID:37727298
reference_title: "Updating Osteonecrosis of the Femoral Head."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "A description of the \nAssociation Research Circulation Osseous (ARCO) criteria for classification of \nglucocorticoids- and alcohol-associated ONFH"
explanation: ARCO provides distinct etiologic classification criteria for alcohol-associated ONFH, supporting it as a recognized subtype.
- name: Traumatic
display_name: Traumatic (post-traumatic) osteonecrosis
description: >
Osteonecrosis caused by mechanical disruption of the blood supply to bone,
classically following femoral neck fracture or hip dislocation. In adolescents
after femoral neck fracture surgery, ONFH incidence is high (approximately 24%).
The vascular anatomy of the femoral head, dependent on retinacular vessels,
makes it especially vulnerable to post-fracture ischemia.
evidence:
- reference: PMID:39581960
reference_title: "Global incidence of osteonecrosis of the femoral head after femoral neck fracture surgery in adolescents: a meta-analysis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "the incidence of ONFH after FNF surgery in adolescents was 24.02% [95% CI \n(0.2118, 0.2712)]"
explanation: Meta-analysis quantifying post-traumatic ONFH incidence after femoral neck fracture surgery, defining the traumatic subtype.
- name: Sickle cell / dysbaric
display_name: Sickle cell disease and dysbaric (Caisson) osteonecrosis
description: >
Osteonecrosis caused by intravascular occlusion. In sickle cell disease,
sickled erythrocytes occlude bone microvasculature. Dysbaric osteonecrosis
(Caisson disease) results from nitrogen gas bubble formation occluding bone
vessels in deep-sea divers and compressed-air workers. Both are recognized
occlusive/embolic etiologies of non-traumatic osteonecrosis.
evidence:
- reference: PMID:37727298
reference_title: "Updating Osteonecrosis of the Femoral Head."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "Current information on etiology and pathogenesis, as well as natural history, \nstage system, and treatments is provided in this review."
explanation: Review of ONFH etiology and pathogenesis providing context for occlusive/embolic etiologies; sickle-cell and dysbaric exposures are recognized occlusive causes.
- name: Idiopathic
display_name: Idiopathic osteonecrosis
description: >
Osteonecrosis without an identifiable cause. The etiology and pathogenesis of
osteonecrosis often remain unclear despite identification of multiple traumatic
and atraumatic risk factors, and a substantial fraction of cases are classified
as idiopathic.
evidence:
- reference: PMID:26396935
reference_title: "Current concepts on osteonecrosis of the femoral head."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "There have been a variety of traumatic and atraumatic \nfactors that have been identified as risk factors for osteonecrosis, but the \netiology and pathogenesis still remains unclear."
explanation: Supports the existence of idiopathic disease where no etiologic factor can be identified despite known risk factors.
pathophysiology:
- name: Vascular supply disruption and microvascular injury
description: >
The initiating event in osteonecrosis is disruption of the blood supply to bone.
This may be mechanical (traumatic vessel disruption after fracture/dislocation),
occlusive (sickled erythrocytes, nitrogen gas emboli, thrombosis), or the result
of glucocorticoid- and alcohol-induced endothelial dysfunction, coagulopathy,
and hypofibrinolysis. Across non-traumatic etiologies, endothelial dysfunction
within a chronic inflammatory milieu produces thrombosis, coagulopathy, and poor
angiogenesis, preventing effective repair and revascularization of bone lesions.
locations:
- preferred_term: Head of femur
term:
id: UBERON:0006767
label: head of femur
- preferred_term: Bone marrow
term:
id: UBERON:0002371
label: bone marrow
cell_types:
- preferred_term: Endothelial cell
term:
id: CL:0000115
label: endothelial cell
biological_processes:
- preferred_term: Angiogenesis
term:
id: GO:0001525
label: angiogenesis
modifier: DECREASED
- preferred_term: Endothelial cell apoptosis
term:
id: GO:0072577
label: endothelial cell apoptotic process
modifier: INCREASED
- preferred_term: Regulation of blood coagulation
term:
id: GO:0030193
label: regulation of blood coagulation
modifier: ABNORMAL
evidence:
- reference: PMID:38540277
reference_title: "Unraveling the Role of Endothelial Dysfunction in Osteonecrosis of the Femoral Head: A Pathway to New Therapies."
supports: SUPPORT
evidence_source: OTHER
snippet: "Continuous stimulation by many variables \ncauses a chronic inflammatory milieu, with clinical repercussions including \nendothelial dysfunction, leading to thrombosis, coagulopathy, and poor \nangiogenesis."
explanation: Review establishing endothelial dysfunction with thrombosis, coagulopathy, and impaired angiogenesis as a central upstream driver of osteonecrosis.
- reference: PMID:37727298
reference_title: "Updating Osteonecrosis of the Femoral Head."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "is caused by a \ndisruption in the blood supply."
explanation: Defines ONFH as caused by disruption of the femoral head blood supply, the initiating pathophysiologic event.
downstream:
- target: Impaired angiogenesis-osteogenesis coupling
description: Endothelial injury and reduced H-type vessel formation uncouple bone vascularization from bone formation.
- target: Ischemic osteocyte and marrow cell death
description: Loss of perfusion deprives subchondral bone and marrow of oxygen and nutrients, triggering cell death.
- target: Marrow adipogenesis and lipotoxicity
description: Glucocorticoid and alcohol exposure shift mesenchymal stem cell differentiation toward adipogenesis, producing lipotoxic marrow injury that compounds vascular compromise.
- name: Impaired angiogenesis-osteogenesis coupling
description: >
The femoral head contains specialized H-type microvessels that couple
angiogenesis to osteogenesis. Glucocorticoids inhibit H-type vessel formation by
reducing expression of HIF-1-alpha, PDGF-BB, and VEGF, damaging the
angiogenesis-osteogenesis coupling and reducing the capacity for necrosis
reconstruction and repair of the femoral head. A 2024 mechanistic mouse study
further linked glucocorticoid suppression of hypothalamic sympathetic tone to
endothelial apoptosis and loss of H-type vessels in the femoral head.
locations:
- preferred_term: Head of femur
term:
id: UBERON:0006767
label: head of femur
cell_types:
- preferred_term: Endothelial cell
term:
id: CL:0000115
label: endothelial cell
- preferred_term: Osteoblast
term:
id: CL:0000062
label: osteoblast
biological_processes:
- preferred_term: Response to hypoxia
term:
id: GO:0001666
label: response to hypoxia
- preferred_term: Osteoblast differentiation
term:
id: GO:0001649
label: osteoblast differentiation
modifier: DECREASED
evidence:
- reference: PMID:38671500
reference_title: "Research progress in the pathogenesis of hormone-induced femoral head necrosis based on microvessels: a systematic review."
supports: SUPPORT
evidence_source: OTHER
snippet: "Glucocorticoids may inhibit the formation of H-type vessels by reducing the expression of \nHIF-1α, PDGF-BB, VGEF and other factors, thus causing damage to the \n\"angiogenesis-osteogenesis coupling\" and reducing the ability of necrosis \nreconstruction and repair of the femoral head."
explanation: Systematic review describing glucocorticoid suppression of H-type vessels and disruption of angiogenesis-osteogenesis coupling impairing bone repair.
- reference: PMID:39516484
reference_title: "Inhibition of sympathetic tone via hypothalamic descending pathway propagates glucocorticoid-induced endothelial impairment and osteonecrosis of the femoral head."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "Vascular endothelial cells rapidly react to inhibition of \nsympathetic tone by provoking endothelial apoptosis in adult male mice treated \nwith methylprednisolone (MPS) daily for 3 days, and we find substantially \nreduced H-type vessels in the femoral heads of MPS-treated ONFH mice."
explanation: Mouse model demonstrating glucocorticoid-driven endothelial apoptosis and loss of H-type vessels in the femoral head, linking neurovascular dysregulation to impaired angiogenesis.
downstream:
- target: Ischemic osteocyte and marrow cell death
description: Failure of revascularization and repair perpetuates ischemia and bone cell death.
- name: Marrow adipogenesis and lipotoxicity
description: >
Glucocorticoid- and alcohol-associated osteonecrosis is characterized by a shift
of mesenchymal stem cell differentiation toward adipocytes at the expense of
osteoblasts, with lipid accumulation in marrow. Increased marrow adipogenesis
raises intraosseous pressure and produces lipotoxic injury, contributing to
osteocyte death and impaired bone formation. Lipid metabolism disorder is an
independent associated factor in steroid-induced ONFH, and Wnt/beta-catenin
pathway variants linked to ONFH are associated with serum lipid disorder.
locations:
- preferred_term: Bone marrow
term:
id: UBERON:0002371
label: bone marrow
cell_types:
- preferred_term: Mesenchymal stem cell
term:
id: CL:0000134
label: mesenchymal stem cell
- preferred_term: Adipocyte
term:
id: CL:0000136
label: adipocyte
biological_processes:
- preferred_term: Adipocyte differentiation
term:
id: GO:0045444
label: fat cell differentiation
modifier: INCREASED
- preferred_term: Lipid metabolic process
term:
id: GO:0006629
label: lipid metabolic process
modifier: ABNORMAL
evidence:
- reference: PMID:38538713
reference_title: "17 variants interaction of Wnt/β-catenin pathway associated with development of osteonecrosis of femoral head in Chinese Han population."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The genes of Wnt/β-catenin pathway may have potential roles in fat accumulation \nof Non-traumatic osteonecrosis of the femoral head (ONFH)"
explanation: Case-control genetic study linking Wnt/beta-catenin pathway variants to fat accumulation in non-traumatic ONFH, supporting the adipogenesis/lipotoxicity mechanism.
- reference: PMID:38927070
reference_title: "Advances in the Pathogenesis of Steroid-Associated Osteonecrosis of the Femoral Head."
supports: SUPPORT
evidence_source: OTHER
snippet: "Steroid-associated osteonecrosis of the femoral head (SANFH) is the most common \ntype of ONFH."
explanation: Review of steroid-associated ONFH pathogenesis, the subtype in which marrow adipogenesis and lipotoxicity are most prominent.
downstream:
- target: Ischemic osteocyte and marrow cell death
description: Lipotoxicity and elevated intraosseous pressure compound ischemia and accelerate bone cell death.
- name: Ischemic osteocyte and marrow cell death
description: >
Disrupted perfusion, lipotoxic stress, and failed revascularization cause
ischemic death (apoptosis and necrosis) of osteocytes and bone marrow cells in
the subchondral region. This is the defining cellular lesion of osteonecrosis:
bone cell ischemia and necrosis with trabecular fracture. The necrotic segment
cannot remodel normally, setting the stage for structural failure.
locations:
- preferred_term: Head of femur
term:
id: UBERON:0006767
label: head of femur
cell_types:
- preferred_term: Osteocyte
term:
id: CL:0000137
label: osteocyte
- preferred_term: Osteoblast
term:
id: CL:0000062
label: osteoblast
biological_processes:
- preferred_term: Apoptotic process
term:
id: GO:0006915
label: apoptotic process
modifier: INCREASED
- preferred_term: Response to hypoxia
term:
id: GO:0001666
label: response to hypoxia
evidence:
- reference: PMID:38540277
reference_title: "Unraveling the Role of Endothelial Dysfunction in Osteonecrosis of the Femoral Head: A Pathway to New Therapies."
supports: SUPPORT
evidence_source: OTHER
snippet: "Osteonecrosis of the femoral head (ONFH) is a disabling disease characterized by \nthe disruption of the blood supply to the femoral head, leading to the apoptosis \nand necrosis of bone cells and subsequent joint collapse."
explanation: Defines the cellular lesion of osteonecrosis as ischemia-driven apoptosis and necrosis of bone cells leading to collapse.
- reference: PMID:38927070
reference_title: "Advances in the Pathogenesis of Steroid-Associated Osteonecrosis of the Femoral Head."
supports: SUPPORT
evidence_source: OTHER
snippet: "Osteonecrosis of the femoral head (ONFH) is a refractory orthopedic condition \ncharacterized by bone cell ischemia, necrosis, bone trabecular fracture, and \nclinical symptoms such as pain, femoral head collapse, and joint dysfunction \nthat can lead to disability."
explanation: Characterizes osteonecrosis as bone cell ischemia and necrosis with trabecular fracture, the central pathologic process.
downstream:
- target: Subchondral fracture and femoral head collapse
description: Dead, unrepaired bone loses mechanical strength and fractures under load, leading to collapse.
- name: Subchondral fracture and femoral head collapse
description: >
Accumulated necrotic bone weakens the subchondral region. Under continued
weight-bearing load, a subchondral fracture develops and the articular surface
progressively collapses. Once collapse occurs the joint is mechanically
incongruent. Without effective early intervention, a high proportion of femoral
heads progress to collapse, and end-stage disease produces secondary
osteoarthritis requiring total hip arthroplasty.
locations:
- preferred_term: Head of femur
term:
id: UBERON:0006767
label: head of femur
- preferred_term: Hip joint
term:
id: UBERON:0001486
label: hip joint
biological_processes:
- preferred_term: Bone remodeling
term:
id: GO:0046849
label: bone remodeling
modifier: ABNORMAL
evidence:
- reference: PMID:38927070
reference_title: "Advances in the Pathogenesis of Steroid-Associated Osteonecrosis of the Femoral Head."
supports: SUPPORT
evidence_source: OTHER
snippet: "clinical symptoms such as pain, femoral head collapse, and joint dysfunction \nthat can lead to disability"
explanation: Identifies femoral head collapse and joint dysfunction as the structural endpoint of the osteonecrosis cascade.
- reference: PMID:26396935
reference_title: "Current concepts on osteonecrosis of the femoral head."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "early intervention prior to collapse is critical to successful outcomes in joint \npreserving procedures"
explanation: Supports the clinical importance of the pre-collapse window, implying progression to subchondral collapse as the natural history endpoint.
downstream:
- target: Secondary osteoarthritis
description: Articular surface collapse produces joint incongruity and secondary degenerative arthritis.
phenotypes:
- name: Hip pain
description: >
Pain in the affected hip, typically the presenting symptom of osteonecrosis of
the femoral head. In an MRI-based clinical cohort, hip pain was present in 86%
of patients. Pain is initially activity-related and worsens as subchondral
fracture and collapse develop.
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: Hip pain
term:
id: HP:0030838
label: Hip pain
evidence:
- reference: PMID:38927070
reference_title: "Advances in the Pathogenesis of Steroid-Associated Osteonecrosis of the Femoral Head."
supports: SUPPORT
evidence_source: OTHER
snippet: "clinical symptoms such as pain, femoral head collapse, and joint dysfunction"
explanation: Identifies pain as a cardinal clinical symptom of ONFH.
- reference: PMID:40718196
reference_title: "A Descriptive Study on the Role of Magnetic Resonance Imaging in Staging Avascular Necrosis of the Hip Joint: Current Trends and Insights."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The most common chief complaint in our study was hip pain, \nwhich was present in 43 (86%) cases."
explanation: MRI-based clinical cohort (50 cases) quantifying hip pain in 86% of patients, supporting the VERY_FREQUENT frequency band.
- name: Avascular necrosis
description: >
The defining radiographic and pathologic feature: death of bone tissue due to
loss of blood supply, classically in the femoral head. Osteonecrosis is itself
the disease entity, and avascular necrosis of bone is the obligate finding.
frequency: OBLIGATE
phenotype_term:
preferred_term: Avascular necrosis
term:
id: HP:0010885
label: Avascular necrosis
evidence:
- reference: PMID:37727298
reference_title: "Updating Osteonecrosis of the Femoral Head."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Osteonecrosis of the femoral head (ONFH), a \ncondition characterized by the \npresence of a necrotic bone lesion in the femoral head, is caused by a \ndisruption in the blood supply."
explanation: Establishes avascular necrosis (necrotic bone lesion from disrupted blood supply) as the defining feature of the disease.
- name: Avascular necrosis of the femoral head
description: >
The femoral head is the classic and most commonly affected site. Avascular
necrosis of the capital femoral epiphysis (femoral head) is the prototypical
presentation and the leading cause of total hip arthroplasty in young and
middle-aged adults.
frequency: VERY_FREQUENT
phenotype_term:
preferred_term: Avascular necrosis of the femoral head
term:
id: HP:0005743
label: Avascular necrosis of the capital femoral epiphysis
evidence:
- reference: PMID:37727298
reference_title: "Updating Osteonecrosis of the Femoral Head."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Its occurrence is more common in young and \nmiddle-aged adults and it is the main reason for performance of total hip \narthroplasty in this age group."
explanation: Supports femoral head involvement as the prototypical, clinically dominant site of osteonecrosis.
- name: Limitation of joint mobility
description: >
Restriction of hip joint range of motion and function (joint dysfunction)
develops as necrosis, subchondral fracture, and collapse progress. ONFH is
described as causing joint dysfunction and disability culminating in loss of
hip function.
phenotype_term:
preferred_term: Limitation of joint mobility
term:
id: HP:0001376
label: Limitation of joint mobility
notes: Progressive course as necrosis, subchondral fracture, and collapse advance.
evidence:
- reference: PMID:38927070
reference_title: "Advances in the Pathogenesis of Steroid-Associated Osteonecrosis of the Femoral Head."
supports: SUPPORT
evidence_source: OTHER
snippet: "clinical symptoms such as pain, femoral head collapse, and joint dysfunction \nthat can lead to disability"
explanation: Identifies joint dysfunction leading to disability as a clinical manifestation, consistent with limitation of joint mobility.
- name: Gait disturbance
description: >
Antalgic gait and impaired ambulation result from hip pain, restricted joint
mobility, and femoral head collapse, contributing to functional disability.
phenotype_term:
preferred_term: Gait disturbance
term:
id: HP:0001288
label: Gait disturbance
evidence:
- reference: PMID:38927070
reference_title: "Advances in the Pathogenesis of Steroid-Associated Osteonecrosis of the Femoral Head."
supports: PARTIAL
evidence_source: OTHER
snippet: "bone trabecular fracture, and \nclinical symptoms such as pain, femoral head collapse, and joint dysfunction \nthat can lead to disability"
explanation: Supports functional disability from pain and joint dysfunction, of which gait disturbance is a manifestation.
genetic:
- name: Wnt/beta-catenin pathway susceptibility variants
notes: >
Osteonecrosis is largely a complex (non-Mendelian) disease with susceptibility
loci and pathway-level genetic architecture. In a Chinese Han case-control
study (560 subjects), variants in the Wnt/beta-catenin pathway genes GSK3B
(rs334558), SFRP4 (rs1052981), and LRP5 (rs312778) were significantly
associated with ONFH risk and clinical traits, with paired variant interactions
associated with bilateral hip lesions and stage IV disease. These variants were
also linked to serum lipid disorder and abnormal platelet/coagulation function,
consistent with the lipid and coagulation mechanisms of disease.
association: Susceptibility
relationship_type: RISK_FACTOR
evidence:
- reference: PMID:38538713
reference_title: "17 variants interaction of Wnt/β-catenin pathway associated with development of osteonecrosis of femoral head in Chinese Han population."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "the genotype, allele \nfrequency, and genetic models of Gsk3β rs334558 (G/A), SFRP4 rs1052981 (A/G), \nand LRP5 rs312778 (T/C) were significantly associated with the increased and \ndecreased ONFH risk and clinical traits, respectively"
explanation: Case-control study identifying Wnt/beta-catenin pathway variants as susceptibility factors for ONFH.
biochemical:
- name: Bone mineral density (protective association)
notes: >
A two-sample Mendelian randomization study found that genetically predicted
higher bone mineral density at the lumbar spine, heel, and total body is a
protective factor against ONFH, whereas serum 25-hydroxyvitamin D, calcium, and
alkaline phosphatase showed no genetic causal relationship with ONFH.
evidence:
- reference: PMID:39639283
reference_title: "Bone biochemical markers, bone mineral density, and the risk of osteonecrosis of the femoral head: a Mendelian randomization study."
supports: SUPPORT
evidence_source: COMPUTATIONAL
snippet: "heel, lumbar spine, and total body bone mineral density can be \nconsidered protective factors for the occurrence of ONFH"
explanation: Mendelian randomization analysis identifying higher BMD as a genetically supported protective factor against ONFH.
environmental:
- name: Glucocorticoid exposure
description: >
Glucocorticoid use is a leading cause of non-traumatic osteonecrosis, reported
in 25-50% of non-traumatic ONFH patients. Risk is dose-dependent. Glucocorticoids
cause femoral head blood flow injury through coagulation dysfunction, endothelial
dysfunction, and impaired angiogenesis, in addition to promoting marrow
adipogenesis and lipotoxicity.
effect: Major causal risk factor (dose-dependent)
chemicals:
- glucocorticoid
evidence:
- reference: PMID:30348552
reference_title: "Etiologic Classification Criteria of ARCO on Femoral Head Osteonecrosis Part 1: Glucocorticoid-Associated Osteonecrosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Glucocorticoid usage, a leading cause of osteonecrosis of the \nfemoral head (ONFH), and its prevalence was reported in 25%-50% of non-traumatic \nONFH patients."
explanation: Establishes glucocorticoid exposure as a leading cause of non-traumatic ONFH, present in 25-50% of cases.
- reference: PMID:38671500
reference_title: "Research progress in the pathogenesis of hormone-induced femoral head necrosis based on microvessels: a systematic review."
supports: SUPPORT
evidence_source: OTHER
snippet: "Glucocorticoids can \ncause blood flow injury of the femoral head mainly through coagulation \ndysfunction, endothelial dysfunction and impaired angiogenesis."
explanation: Describes the vascular mechanisms by which glucocorticoid exposure causes femoral head necrosis.
- name: Heavy alcohol consumption
description: >
Heavy alcohol use is a major non-traumatic etiologic exposure, recognized in the
ARCO classification of alcohol-associated ONFH. Implicated mechanisms include
oxidative stress and lipid dysregulation.
effect: Major causal risk factor
chemicals:
- ethanol
evidence:
- reference: PMID:38540277
reference_title: "Unraveling the Role of Endothelial Dysfunction in Osteonecrosis of the Femoral Head: A Pathway to New Therapies."
supports: SUPPORT
evidence_source: OTHER
snippet: "Multiple risk factors contribute \nto osteonecrosis, including glucocorticoid (GC) usage, excessive alcohol intake, \nhypercholesterolemia, and smoking."
explanation: Lists excessive alcohol intake among the major risk factors contributing to osteonecrosis.
- name: Hypercholesterolemia and smoking
description: >
Hypercholesterolemia and smoking are repeatedly cited contributing risk factors
for osteonecrosis, acting through chronic inflammation, endothelial dysfunction,
and lipid dysregulation.
effect: Contributing risk factor
evidence:
- reference: PMID:38540277
reference_title: "Unraveling the Role of Endothelial Dysfunction in Osteonecrosis of the Femoral Head: A Pathway to New Therapies."
supports: SUPPORT
evidence_source: OTHER
snippet: "Multiple risk factors contribute \nto osteonecrosis, including glucocorticoid (GC) usage, excessive alcohol intake, \nhypercholesterolemia, and smoking."
explanation: Identifies hypercholesterolemia and smoking among the multiple risk factors contributing to osteonecrosis.
- name: Femoral neck fracture / trauma
description: >
Mechanical trauma, particularly femoral neck fracture, disrupts the blood supply
to the femoral head and is the leading cause of traumatic (post-traumatic)
osteonecrosis. In adolescents after femoral neck fracture surgery, ONFH
incidence is approximately 24%.
effect: Major causal risk factor (traumatic etiology)
evidence:
- reference: PMID:39581960
reference_title: "Global incidence of osteonecrosis of the femoral head after femoral neck fracture surgery in adolescents: a meta-analysis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Osteonecrosis of the femoral head (ONFH) is a \nsignificant \npostoperative complication following femoral neck fractures (FNFs) in \nadolescents"
explanation: Establishes femoral neck fracture as a major cause of post-traumatic ONFH.
treatments:
- name: Conservative management
description: >
Non-operative treatment including protected weight-bearing, pharmacologic agents
(e.g., bisphosphonates, statins), and physical modalities, used mainly in early
pre-collapse disease or when surgery is deferred or contraindicated. A 2024
systematic review found conservative approaches may relieve symptoms and delay
progression, but evidence remains heterogeneous and is not clearly
disease-modifying in advanced collapse.
context: Early/pre-collapse disease or patients unfit for surgery
treatment_term:
preferred_term: supportive care
term:
id: MAXO:0000950
label: supportive care
target_phenotypes:
- preferred_term: Hip pain
term:
id: HP:0030838
label: Hip pain
evidence:
- reference: PMID:39051378
reference_title: "Conservative Treatment in Avascular Necrosis of the Femoral Head: A Systematic Review."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "This review evaluates the effectiveness of conservative treatments \nsuch as pharmacological interventions and physical modalities in managing AVN of \nthe femoral head."
explanation: Systematic review supporting conservative treatment for symptom relief and progression delay, while noting limited and heterogeneous evidence.
- name: Bisphosphonate therapy
description: >
Bisphosphonates are among the pharmacologic agents used in osteonecrosis,
primarily aimed at reducing osteoclastic resorption of the necrotic segment to
delay femoral head collapse in pre-collapse disease.
context: Pre-collapse disease
treatment_term:
preferred_term: bisphosphonate agent therapy
term:
id: MAXO:0000954
label: bisphosphonate agent therapy
target_phenotypes:
- preferred_term: Avascular necrosis of the femoral head
term:
id: HP:0005743
label: Avascular necrosis of the capital femoral epiphysis
evidence:
- reference: PMID:26396935
reference_title: "Current concepts on osteonecrosis of the femoral head."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "Treatment options include pharmacologic \nagents such as bisphosphonates and statins"
explanation: Identifies bisphosphonates among pharmacologic treatment options for osteonecrosis of the femoral head.
- name: Core decompression
description: >
Core decompression, the most widely used joint-preserving procedure, drills the
necrotic lesion to reduce intraosseous pressure and promote revascularization,
indicated mainly in pre-collapse (ARCO I-II) disease. Real-world failure rates
can be high. Adjuncts such as cell therapy, bone grafting, and tantalum rods
improve clinical and radiographic outcomes versus core decompression alone.
context: Pre-collapse (ARCO I-II) disease
treatment_term:
preferred_term: surgical procedure
term:
id: MAXO:0000004
label: surgical procedure
target_phenotypes:
- preferred_term: Avascular necrosis of the femoral head
term:
id: HP:0005743
label: Avascular necrosis of the capital femoral epiphysis
- preferred_term: Hip pain
term:
id: HP:0030838
label: Hip pain
evidence:
- reference: PMID:34313452
reference_title: "Comparison of cell therapy and other novel adjunctive therapies combined with core decompression for the treatment of osteonecrosis of the femoral head : a systematic review and meta-analysis of 20 studies."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The combination of CD with other \ntherapeutic interventions resulted in a higher HHS"
explanation: Meta-analysis showing core decompression combined with adjuncts improves Harris Hip Score over decompression alone.
- reference: PMID:34781934
reference_title: "Efficacy of various core decompression techniques versus non-operative treatment for osteonecrosis of the femoral head: a systemic review and network meta-analysis of randomized controlled trials."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "CD + CT showed a relatively superior result in radiographic progression than nonsurgical treatment"
explanation: Network meta-analysis indicating core decompression plus cell therapy delays radiographic progression relative to non-surgical treatment.
- name: Cell therapy / bone marrow concentrate augmentation
description: >
Adjunctive cell-based therapies (autologous bone marrow concentrate, expanded
mesenchymal stem cells, with or without platelet-rich plasma) combined with core
decompression aim to enhance bone regeneration and revascularization in
pre-collapse disease. Evidence is favorable but heterogeneous and
stage-dependent; benefit diminishes once collapse is established. Continued
corticosteroid use and large necrotic lesions predict failure.
context: Pre-collapse disease, often corticosteroid-induced
treatment_term:
preferred_term: cell therapy
term:
id: MAXO:0000016
label: cellular therapy
therapeutic_modality: CELL_THERAPY
target_phenotypes:
- preferred_term: Avascular necrosis of the femoral head
term:
id: HP:0005743
label: Avascular necrosis of the capital femoral epiphysis
evidence:
- reference: PMID:34751583
reference_title: "Hip decompression combined with bone marrow concentrate and platelet-rich plasma for corticosteroid-induced osteonecrosis of the femoral head : mid-term update from a prospective study."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "hip decompression augmented with BMAC and PRP \nprovided a 67% survivorship free from THA in patients with \ncorticosteroid-induced ON."
explanation: Prospective study showing decompression augmented with bone marrow concentrate and PRP yields 67% THA-free survivorship at 7 years in corticosteroid-induced ONFH.
- reference: PMID:36983120
reference_title: "Long-Term Results of a Phase I/II Clinical Trial of Autologous Mesenchymal Stem Cell Therapy for Femoral Head Osteonecrosis."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "The use of \nautologous MSCs for patients with ONFH disease is feasible, safe in the long \nterm, and potentially effective."
explanation: Phase I/II trial supporting feasibility, safety, and potential efficacy of autologous MSC therapy for ONFH.
- name: Total hip arthroplasty
description: >
Total hip arthroplasty (hip replacement) is the dominant intervention for
post-collapse, end-stage osteonecrosis (ARCO III-IV). In U.S. nationwide data,
THA accounted for the large majority of surgical management of hip osteonecrosis.
Osteonecrosis accounts for roughly 10% of all total hip arthroplasties performed
annually in the United States.
context: Post-collapse / end-stage (ARCO III-IV) disease
treatment_term:
preferred_term: hip replacement
term:
id: MAXO:0009047
label: hip replacement
target_phenotypes:
- preferred_term: Hip pain
term:
id: HP:0030838
label: Hip pain
- preferred_term: Limitation of joint mobility
term:
id: HP:0001376
label: Limitation of joint mobility
evidence:
- reference: PMID:26396935
reference_title: "Current concepts on osteonecrosis of the femoral head."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "20000 to 30000 new patients are diagnosed with \nosteonecrosis annually accounting for approximately 10% of the 250000 total hip \narthroplasties done annually in the United States."
explanation: Establishes the major role of total hip arthroplasty in osteonecrosis, which accounts for ~10% of U.S. THAs.
prevalence:
- population: United States (new diagnoses)
notes: >
An estimated 20,000 to 30,000 new patients are diagnosed with osteonecrosis
annually in the United States, accounting for approximately 10% of the ~250,000
total hip arthroplasties performed annually.
evidence:
- reference: PMID:26396935
reference_title: "Current concepts on osteonecrosis of the femoral head."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "It is estimated that 20000 to 30000 new patients are diagnosed with \nosteonecrosis annually accounting for approximately 10% of the 250000 total hip \narthroplasties done annually in the United States."
explanation: Provides the U.S. incidence estimate and the proportion of total hip arthroplasties attributable to osteonecrosis.
diagnosis:
- name: MRI and radiographic staging
description: >
Diagnosis relies on plain anteroposterior and frog-leg lateral radiographs
followed by MRI. The first radiographic changes are typically cystic and
sclerotic changes in the femoral head, but radiographs are insufficient for
early diagnosis; MRI is the most accurate benchmark and underpins staging
systems such as the 2019 revised ARCO classification (stages I-IV, with stage
III subdivided by depth of subchondral depression).
evidence:
- reference: PMID:26396935
reference_title: "Current concepts on osteonecrosis of the femoral head."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Although the diagnosis may be made by radiograph, plain \nradiographs are generally insufficient for early diagnosis, therefore MRI is \nconsidered the most accurate benchmark."
explanation: Supports MRI as the most accurate diagnostic benchmark for early osteonecrosis.
clinical_trials:
- name: NCT01605383
phase: PHASE_II
status: COMPLETED
description: >
Phase I/II randomized trial comparing core decompression alone versus core
decompression plus autologous expanded mesenchymal stem cells on an allogenic
bone scaffold for osteonecrosis of the femoral head, with safety/feasibility
primary endpoints and secondary endpoints including modified Kerboul angle,
VAS, SF-36, and WOMAC.
target_phenotypes:
- preferred_term: Avascular necrosis of the femoral head
term:
id: HP:0005743
label: Avascular necrosis of the capital femoral epiphysis
evidence:
- reference: clinicaltrials:NCT01605383
supports: PARTIAL
snippet: "The present study evaluates the effect of XCEL-MT-OSTEO-ALPHA in osteonecrosis of the femoral head in comparison to the standard treatment of isolated core decompression."
explanation: Clinical trial evaluating MSC-based tissue engineering with core decompression for ONFH.
- name: NCT04233125
phase: PHASE_II
status: COMPLETED
description: >
Phase I/II randomized trial comparing core decompression versus core
decompression with PMMA cement packing for symptomatic pre-collapse (ARCO I-II)
osteonecrosis of the femoral head, with progression-free survival at 5 years as
the primary endpoint.
target_phenotypes:
- preferred_term: Avascular necrosis of the femoral head
term:
id: HP:0005743
label: Avascular necrosis of the capital femoral epiphysis
evidence:
- reference: clinicaltrials:NCT04233125
supports: PARTIAL
snippet: "This study was undertaken to determine whether the addition of PMMA packing to CD provides any benefit to progression-free survival (PFS) and conversion to total hip arthroplasty-free survival (CFS)."
explanation: Clinical trial comparing core decompression with and without cement packing for pre-collapse ONFH.
References & Deep Research
Deep Research
11. Disease Information
1.1 Concise overview and definitions
Osteonecrosis is bone and marrow cell death due to temporary or permanent disruption of blood supply; in ONFH this ischemic necrosis leads to trabecular fracture, femoral head collapse, pain, and progressive hip dysfunction/disability. (zhang2024advancesinthe pages 1-2, moyaangeler2015currentconceptson pages 1-2)
Recent authoritative definitions emphasize vascular compromise and subsequent structural collapse: ONFH is described as “a necrotic bone lesion in the femoral head… caused by a disruption in the blood supply.” (ko2023updatingosteonecrosisof pages 1-2)
1.2 Key identifiers (ontology/coding)
- ICD-10/ICD-11, MeSH, MONDO, Orphanet, OMIM: not explicitly retrievable from the full texts available in this run. The administrative-database ONFH trends paper indicates identification via ICD-9/10 coding but does not list the codes in the excerpted text. (ng2023increasingtrendtoward pages 1-2)
1.3 Synonyms and alternative names
Common synonyms used in the retrieved corpus include: * Avascular necrosis (AVN) and ischemic necrosis/aseptic necrosis (xiang2024advancesinmechanism pages 1-2, rohilla2025adescriptivestudy pages 1-2) * Femur head necrosis / femoral head necrosis (keyword synonym) (ko2023updatingosteonecrosisof pages 1-2) * “Nontraumatic avascular necrosis of the femoral head” (reference terminology) (ko2023updatingosteonecrosisof pages 6-8)
1.4 Evidence source type (patient-level vs aggregated)
Evidence used here spans: * Aggregated reviews, systematic reviews, meta-analyses, and consensus/Delphi statements (zhang2024advancesinthe pages 1-2, li2024pathologicalmechanismsand pages 1-2, yoon2019etiologicclassificationcriteria pages 5-8) * Administrative/nationwide databases (procedure trends and proportions) (ng2023increasingtrendtoward pages 1-2) * Prospective/retrospective clinical cohorts and trials (cell therapy, decompression) (houdek2021hipdecompressioncombined pages 1-2, blanco2023longtermresultsof pages 8-10) * Animal model mechanistic work (glucocorticoid-induced ONFH mouse model) (shao2024inhibitionofsympathetic pages 1-2)
2. Etiology
2.1 Primary causal factors
ONFH is typically classified as traumatic (vascular disruption after fracture/dislocation) or non-traumatic (commonly glucocorticoids and alcohol). (gu2024globalincidenceof pages 1-2, ko2023updatingosteonecrosisof pages 1-2)
Key non-traumatic contributors highlighted across 2024 reviews include glucocorticoids, alcohol, lipid dysregulation, microvascular/endothelial injury, and coagulation abnormalities. (zhang2024advancesinthe pages 1-2, li2024pathologicalmechanismsand pages 1-2, shao2024unravelingtherole pages 1-2)
2.2 Risk factors (quantitative where available)
Glucocorticoid exposure (major risk factor; ARCO etiologic research classification): * ARCO consensus criteria for glucocorticoid-associated ONFH: >2 g prednisolone-equivalent within 3 months, diagnosis within 2 years, and absence of other major risk factor(s). (yoon2019etiologicclassificationcriteria pages 5-8, yoon2019etiologicclassificationcriteria pages 1-5) * Dose-response summarized by ARCO: +4.6% ONFH rate per additional 10 mg/day and daily dose >40 mg (OR 4.2) in cited studies; early post-transplant data show ONFH incidence increasing from 6% (≤520 mg) to 28% (>600 mg) in the first 2 weeks. (yoon2019etiologicclassificationcriteria pages 5-8)
Alcohol exposure: * Ko 2023 summarizes ARCO alcohol-associated criteria as >320 g/week alcohol (reported as >400 mL/week), diagnosis within 1 year, and no other major risk factor. (ko2023updatingosteonecrosisof pages 1-2)
Trauma: * In adolescents after femoral neck fracture surgery, a 2024 meta-analysis estimated ONFH incidence 24.02% (95% CI 21.18–27.12%). (gu2024globalincidenceof pages 1-2)
Other risk factors repeatedly cited (without thresholds in retrieved text): hypercholesterolemia and smoking, among others. (shao2024unravelingtherole pages 1-2)
2.3 Protective factors (recent genetic causal inference)
A 2024 Mendelian randomization study found higher genetically predicted BMD was protective for ONFH at several sites: * Lumbar spine BMD OR 0.662 (95% CI 0.48–0.91) (jia2024bonebiochemicalmarkers pages 1-2) * Heel BMD OR 0.726 (95% CI 0.62–0.85) (jia2024bonebiochemicalmarkers pages 1-2) * Total body BMD OR 0.726 (95% CI 0.62–0.85) (jia2024bonebiochemicalmarkers pages 1-2)
The same study did not support genetically mediated causal effects for serum 25OHD, calcium, or alkaline phosphatase on ONFH risk. (jia2024bonebiochemicalmarkers pages 1-2)
2.4 Gene–environment interactions
A 2024 Wnt/β-catenin pathway variant-interaction study (Chinese Han case-control) links genetic variation to clinical phenotypes and systemic metabolic/coagulation changes, consistent with gene–environment coupling (e.g., steroid exposure and lipid/platelet phenotypes). (shi202417variantsinteraction pages 1-2, shi202417variantsinteraction pages 9-11)
| Factor type | Factor | Quantitative details | Evidence type (consensus/review/cohort/MR) | Notes (mechanism) | Source (author year) | URL |
|---|---|---|---|---|---|---|
| Etiology/risk | Glucocorticoid exposure | ARCO etiologic classification: cumulative >2 g prednisolone-equivalent within 3 months; ONFH diagnosed within 2 years of exposure; no other major risk factor (yoon2019etiologicclassificationcriteria pages 5-8, yoon2019etiologicclassificationcriteria pages 1-5, yoon2019etiologicclassificationcriteria pages 8-12) | Consensus | Standardized research definition for glucocorticoid-associated ONFH | Yoon 2019 | https://doi.org/10.1016/j.arth.2018.09.005 |
| Risk | Higher daily glucocorticoid dose | +4.6% ONFH rate per additional 10 mg/day; daily dose >40 mg associated with OR 4.2 for ONFH (yoon2019etiologicclassificationcriteria pages 5-8) | Consensus summarizing prior cohort evidence | Dose-response effect supports steroid toxicity as major risk driver | Yoon 2019 | https://doi.org/10.1016/j.arth.2018.09.005 |
| Risk | Early high cumulative steroid dose after transplant | ONFH incidence by first-2-week dose: 6% (≤520 mg), 17% (520–600 mg), 28% (>600 mg) (yoon2019etiologicclassificationcriteria pages 5-8) | Consensus summarizing prior cohort evidence | Illustrates strong early cumulative-dose effect | Yoon 2019 | https://doi.org/10.1016/j.arth.2018.09.005 |
| Etiology/risk | Alcohol-associated ONFH | ARCO etiologic classification: alcohol consumption >320 g/week (summarized as >400 mL/week) with diagnosis within 1 year and no other major risk factor (ko2023updatingosteonecrosisof pages 1-2) | Review summarizing consensus | Standardized research definition for alcohol-associated ONFH | Ko 2023 | https://doi.org/10.5371/hp.2023.35.3.147 |
| Risk | Heavy alcohol use | Alcohol accounts for 32.4–45.3% of non-traumatic ONFH cases in Asia (pang2025thebibliometricand pages 1-2) | Literature synthesis/review | Alcohol metabolites, oxidative stress, lipid dysregulation implicated | Pang 2025 | https://doi.org/10.1186/s13018-025-06138-8 |
| Etiology/risk | Trauma/femoral neck fracture | Postoperative adolescent ONFH incidence after femoral neck fracture surgery 24.02% (95% CI 21.18%–27.12%) (gu2024globalincidenceof pages 1-2) | Meta-analysis | Traumatic vascular disruption around femoral head | Gu 2024 | https://doi.org/10.1186/s13018-024-05275-w |
| Risk | Continued corticosteroid use after decompression | Continued steroid use at time of decompression associated with THA conversion HR 4.15 (p=0.039) (houdek2021hipdecompressioncombined pages 1-2) | Cohort | Ongoing exposure worsens progression despite hip-preserving procedure | Houdek 2021 | https://doi.org/10.1302/2633-1462.211.bjo-2021-0132.r1 |
| Risk | Large necrotic lesion / high modified Kerboul angle | Modified Kerboul angle grade 3–4 associated with THA conversion HR 3.96 (p=0.047); 7-year survivorship much worse than grades 1–2 (houdek2021hipdecompressioncombined pages 1-2) | Cohort | Larger lesion size predicts collapse and failure of joint preservation | Houdek 2021 | https://doi.org/10.1302/2633-1462.211.bjo-2021-0132.r1 |
| Risk | Steroid use, alcohol use, hypercholesterolemia, smoking | No pooled threshold given; repeatedly cited as major ONFH risks (shao2024unravelingtherole pages 1-2) | Review | Chronic inflammation and endothelial dysfunction promote thrombosis, poor angiogenesis, ischemia | Shao 2024 | https://doi.org/10.3390/biomedicines12030664 |
| Risk | Long-term glucocorticoid therapy | 5–40% may develop osteonecrosis; 30–50% may sustain fractures (ma2024researchprogressin pages 2-3) | Systematic review | Glucocorticoids impair microcirculation, angiogenesis, and bone remodeling | Ma 2024 | https://doi.org/10.1186/s13018-024-04748-2 |
| Risk | Endothelial dysfunction / coagulopathy / hypofibrinolysis | Quantitative threshold not specified (shao2024unravelingtherole pages 1-2, ma2024researchprogressin pages 1-2) | Review/systematic review | Impaired vasodilation, thrombosis, hypoxia, reduced revascularization | Shao 2024; Ma 2024 | https://doi.org/10.3390/biomedicines12030664 |
| Risk | Lipid metabolism disorder | Quantitative threshold not standardized; TG and HDL independently associated with steroid-induced ONFH in predictive model (jia2024predictingsteroidinducedosteonecrosis pages 12-12) | Cohort/multi-omics | Adipogenesis, lipid accumulation, intraosseous pressure, atherosclerosis-like injury | Jia 2024 | https://doi.org/10.1186/s13018-024-05245-2 |
| Risk | Wnt/β-catenin pathway variants | GSK3β rs334558, SFRP4 rs1052981, LRP5 rs312778 associated with ONFH risk; paired interactions linked with bilateral lesions and stage IV disease (P <0.044–0.004) (shi202417variantsinteraction pages 1-2, shi202417variantsinteraction pages 9-11) | Genetic case-control | Variant interactions linked to osteogenesis/adipogenesis imbalance plus lipid/coagulation abnormalities | Shi 2024 | https://doi.org/10.1038/s41598-024-57929-8 |
| Risk | Inflammatory cytokine genetics | bFGF OR 1.942 (95% CI 1.13–3.35), IL-2 OR 0.688 (95% CI 0.50–0.94), IL2-RA OR 1.386 (95% CI 1.04–1.85) for osteonecrosis; SCF OR 3.356 (95% CI 1.09–10.30) for drug-related osteonecrosis (from abstract) (xiang2024advancesinmechanism pages 18-18) | MR | Supports causal contribution of immune-inflammatory pathways | Lu 2024 | https://doi.org/10.3389/fendo.2024.1344917 |
| Protective | Higher lumbar spine bone mineral density | OR 0.662 (95% CI 0.48–0.91, P=0.010) for ONFH (jia2024bonebiochemicalmarkers pages 1-2) | MR | Suggests systemic skeletal robustness may reduce susceptibility | Jia 2024 | https://doi.org/10.1186/s12891-024-08130-5 |
| Protective | Higher heel bone mineral density | OR 0.726 (95% CI 0.62–0.85, P<0.001) for ONFH (jia2024bonebiochemicalmarkers pages 1-2) | MR | Protective association observed in genetic causal analysis | Jia 2024 | https://doi.org/10.1186/s12891-024-08130-5 |
| Protective | Higher total body bone mineral density | OR 0.726 (95% CI 0.62–0.85, P<0.001) for ONFH (jia2024bonebiochemicalmarkers pages 1-2) | MR | Protective association observed in genetic causal analysis | Jia 2024 | https://doi.org/10.1186/s12891-024-08130-5 |
| Not supported as protective/risk | 25-hydroxyvitamin D, serum calcium, alkaline phosphatase | No significant genetic causal association: 25OHD OR 1.006; Ca OR 0.856; ALP OR 1.022 (jia2024bonebiochemicalmarkers pages 1-2) | MR | Current MR evidence does not support these serum markers as causal determinants | Jia 2024 | https://doi.org/10.1186/s12891-024-08130-5 |
| Risk | Deep-sea diving / dysbaric exposure | Quantitative threshold not provided (yang2024adelphibasedmodel pages 1-2, ko2023updatingosteonecrosisof pages 1-2) | Review | Dysbaric ONFH/Caisson disease recognized occupational etiology | Yang 2024; Ko 2023 | https://doi.org/10.1186/s13018-024-05247-0 |
| Risk | Occupational/behavioral factors and male sex in CD failure model | In ARCO I–II patients after core decompression, male sex HR 75.449; seated occupation HR 3.937; age HR 1.045/year; longer disease duration HR 1.217; combined necrosis angle HR 1.025 (liu2021efficacyofvarious pages 1-2) | Cohort | Prognostic factors for failure after core decompression rather than primary causation | Wei 2023 | https://doi.org/10.1186/s12891-023-06321-0 |
Table: This table summarizes major etiologies, risk factors, and protective factors for osteonecrosis of the femoral head, emphasizing quantitative thresholds and effect sizes where available. It is useful for comparing consensus definitions, epidemiologic risks, and recent genetic/MR findings in one place.
3. Phenotypes
3.1 Core clinical phenotypes
Commonly reported ONFH phenotypes include: * Hip pain: in an MRI-based clinical cohort, hip pain was present in 86% (43/50). (rohilla2025adescriptivestudy pages 1-2) * Functional limitation/joint dysfunction: ONFH is described as causing joint dysfunction and disability, often culminating in collapse and loss of hip function. (zhang2024advancesinthe pages 1-2)
3.2 Onset and progression
ONFH often affects young to middle-aged adults (commonly cited 20–40 years), but cohorts may center around early 40s depending on setting. (moyaangeler2015currentconceptson pages 1-2, rohilla2025adescriptivestudy pages 1-2)
3.3 Bilaterality
In a 50-patient MRI cohort (80 hips), 60% had bilateral involvement. (rohilla2025adescriptivestudy pages 1-2)
3.4 Quality of life / functional scoring instruments used
The retrieved evidence shows frequent use of: * Harris Hip Score (HHS) and VAS pain in clinical trials and cohorts (he2021thetherapeuticeffect pages 1-2, houdek2021hipdecompressioncombined pages 1-2) * WOMAC and SF-36 are used in multiple clinical trials/registries and prospective studies, including cell therapy trials. (NCT01605383 chunk 1, NCT04233125 chunk 1)
3.5 Suggested HPO terms (mapping; evidence-backed phenotypes)
- Hip pain — HP:0030834 (hip pain)
- Abnormal gait — HP:0001288 (for advanced collapse-related dysfunction; commonly implied in ONFH disability)
- Osteonecrosis — HP:0010885 (osteonecrosis)
- Avascular necrosis of femoral head — often represented via osteonecrosis + anatomic localization (no explicit HPO ID in retrieved texts)
Frequency data beyond hip pain and bilaterality were not available in the retrieved text.
4. Genetic/Molecular Information
4.1 Genetic susceptibility signals (not monogenic “causal genes”)
ONFH in the retrieved corpus is largely treated as a complex disease with susceptibility loci and pathway-level genetic architecture.
Wnt/β-catenin pathway variants (2024): * Single-variant associations: GSK3β rs334558, SFRP4 rs1052981, LRP5 rs312778 (p-values reported, no ORs in excerpt). (shi202417variantsinteraction pages 1-2) * Variant interactions associated with risk, bilaterality, and stage IV risk; also associated with lipid and platelet indices, consistent with lipid/coagulation mechanisms. (shi202417variantsinteraction pages 9-11)
Immune/inflammatory genetic causal inference (2024 Mendelian randomization): * bFGF OR 1.942, IL-2 OR 0.688, IL2-RA OR 1.386 for osteonecrosis risk in a GWAS-derived MR analysis; SCF OR 3.356 for drug-related osteonecrosis in the same study. (xiang2024advancesinmechanism pages 18-18)
4.2 Molecular mechanisms and pathways (recent emphasis)
A 2024 SONFH review summarizes key pathological mechanisms: decreased osteogenesis, lipid accumulation/lipotoxicity, increased intraosseous pressure, and microcirculation disruption. (li2024pathologicalmechanismsand pages 1-2)
A 2024 steroid-associated pathogenesis review emphasizes microcirculation dysfunction and endothelial damage with downstream hypoxia and impaired bone maintenance. (zhang2024advancesinthe pages 1-2)
Endoplasmic reticulum stress and inflammation (2024): an ER-stress gene-signature study identified 195 ERS-related genes; proposed hub genes include CXCL8, STAT3, IL1B, TLR4, PTGS2, TLR2, CASP1, CYBB, CAT, HOMX1; qRT-PCR validated upregulation of STAT3, IL1B, TLR2, CASP1. (wu2024identificationandvalidation pages 1-2)
4.3 Epigenetics
A 2024 SONFH review highlights epigenetic/post-transcriptional regulation, including histone acetylation modulation affecting PPARγ-driven adipogenesis and miRNA-mediated BMSC differentiation (e.g., miR-27a). (li2024pathologicalmechanismsand pages 8-9)
4.4 Suggested GO terms (biological processes; mechanism-aligned)
- Angiogenesis — GO:0001525
- Bone remodeling — GO:0046849
- Osteoblast differentiation — GO:0001649
- Endothelial cell apoptotic process — GO:0072570
- Response to endoplasmic reticulum stress — GO:0034976
- Lipid metabolic process — GO:0006629
- Regulation of blood coagulation — GO:0030193
4.5 Suggested CL terms (cell types; mechanism-aligned)
- Endothelial cell — CL:0000115 (central in microvascular injury/endothelial dysfunction) (shao2024unravelingtherole pages 1-2)
- Osteoblast — CL:0000062
- Osteoclast — CL:0000092
- Mesenchymal stem/stromal cell — CL:0000134 (therapeutic target/deficit in some cell-therapy frameworks) (NCT01605383 chunk 1)
5. Environmental Information
5.1 Environmental and lifestyle factors
- Alcohol intake is a major non-traumatic etiologic exposure in Asia and globally. (pang2025thebibliometricand pages 1-2, ko2023updatingosteonecrosisof pages 1-2)
- Smoking and hypercholesterolemia are cited as contributing risk factors in a 2024 endothelial dysfunction review. (shao2024unravelingtherole pages 1-2)
5.2 Infectious agents
No pathogen is identified as a causal infectious agent for ONFH in the retrieved text. A single cohort reported prior COVID-19 in 34% of cases, but this is observational and not causal evidence. (rohilla2025adescriptivestudy pages 1-2)
5.3 Gut microbiome/metabolomics (recent development)
A 2024 study compared steroid- vs alcohol-induced nontraumatic ONFH and reported distinct gut microbiota and fecal metabolite profiles, suggesting exposure-specific host–microbiome metabolic signatures. (xiang2024advancesinmechanism pages 1-2)
6. Mechanism / Pathophysiology
6.1 Causal chain (integrated model)
A contemporary consensus model across 2024 reviews is: 1) Trigger/exposure (glucocorticoids, alcohol, trauma) (zhang2024advancesinthe pages 1-2, gu2024globalincidenceof pages 1-2) 2) Microvascular/endothelial injury and/or coagulopathy, impaired vasodilation, hypofibrinolysis → reduced perfusion (shao2024unravelingtherole pages 1-2, ma2024researchprogressin pages 1-2) 3) Hypoxia/nutrient deficiency in subchondral bone and marrow → osteocyte/osteoblast death and impaired repair (zhang2024advancesinthe pages 1-2, li2024pathologicalmechanismsand pages 1-2) 4) Structural weakening with subchondral fracture and progressive collapse (ko2023updatingosteonecrosisof pages 2-4)
6.2 Endothelial dysfunction as a central driver
A 2024 review frames endothelial dysfunction as a “major cause” of ONFH: inflammatory milieu and endothelial dysfunction lead to thrombosis/coagulopathy and poor angiogenesis, preventing effective repair and revascularization. (shao2024unravelingtherole pages 1-2)
6.3 Microvessels and angiogenesis–osteogenesis coupling
A 2024 systematic review emphasizes microvascular injury and the role of “H-type vessels” in angiogenesis–osteogenesis coupling; glucocorticoids may reduce H-type vessel formation by reducing HIF-1α, PDGF-BB, and VEGF, disrupting repair. (ma2024researchprogressin pages 1-2)
6.4 New mechanistic development (2024): neurovascular axis in glucocorticoid-induced ONFH
A 2024 Bone Research mechanistic study (mouse model) proposes a hypothalamus–sympathetic–endothelium axis: glucocorticoids disrupt GR/MR balance in hypothalamic PVN neurons, reducing sympathetic outflow; inhibited sympathetic tone provokes endothelial apoptosis and loss of H-type vessels in femoral heads. Restoration via PVN GR inhibition (RU486) or ADRB2 activation protects, while Adrb2 knockout or sympathectomy abolishes protection; downstream NE–ADRB2–cAMP/CREB signaling upregulates endothelial PFKFB3 to support glycolysis and angiogenesis coupling. (shao2024inhibitionofsympathetic pages 1-2, shao2024inhibitionofsympathetic pages 2-3)
7. Anatomical Structures Affected
7.1 Organ/tissue localization
Primary site in this report: femoral head of the hip joint (subchondral bone and marrow). (ko2023updatingosteonecrosisof pages 1-2, moyaangeler2015currentconceptson pages 1-2)
Suggested anatomy ontology mapping (UBERON): * Femoral head — UBERON:0002428 * Hip joint — UBERON:0001463 * Subchondral bone — (commonly used anatomic term; specific UBERON ID not retrieved)
7.2 Laterality patterns
Bilateral disease is common; 60% bilaterality was reported in one MRI cohort. (rohilla2025adescriptivestudy pages 1-2)
8. Temporal Development
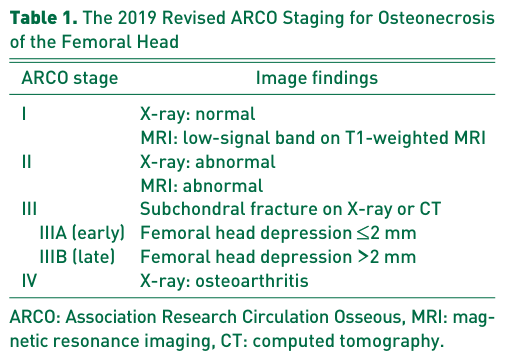
8.1 Staging (2019 revised ARCO)
Ko 2023 summarizes the revised 2019 ARCO staging system: * Stage I: X-ray normal; MRI shows low-signal band on T1-weighted images * Stage II: X-ray and MRI abnormal * Stage III: subdivided into IIIA ≤2 mm depression and IIIB >2 mm depression; may show subchondral fracture on X-ray/CT * Stage IV: osteoarthritis on X-ray (ko2023updatingosteonecrosisof pages 2-4)
Image evidence for the ARCO 2019 staging system table/figure is available from Ko 2023. (ko2023updatingosteonecrosisof media 0e890259, ko2023updatingosteonecrosisof media 85ac9cbb)
8.2 Natural history
Multiple sources emphasize high progression rates without effective early intervention. A 2024 pathogenesis review states femoral head collapse may exceed 80% within 2 years without early intervention. (zhang2024advancesinthe pages 1-2)
9. Inheritance and Population
9.1 Epidemiology and burden (selected quantitative evidence)
Recent reviews and analyses provide approximate burden estimates: * United States: prevalence ~300,000–600,000 and 10,000–20,000 new cases/year (review estimate) (li2024pathologicalmechanismsand pages 1-2) * United States: commonly cited 20,000–30,000 new cases/year (widely cited benchmark) (moyaangeler2015currentconceptson pages 1-2) * Japan: incidence 1.91/100,000; 2,500–3,300 new cases/year (li2024pathologicalmechanismsand pages 1-2) * China: >8 million affected; 50,000–100,000 new cases/year estimate (li2024pathologicalmechanismsand pages 1-2, yang2024adelphibasedmodel pages 1-2)
| Metric | Population/setting | Value | Timeframe | Notes | Source (first author year, journal) | URL |
|---|---|---|---|---|---|---|
| Prevalence | United States, osteonecrosis/ONFH | 300,000–600,000 affected individuals | Not specified | Reported as U.S. prevalence in a 2024 review focused on steroid-induced ONFH (li2024pathologicalmechanismsand pages 1-2) | Li 2024, Annals of Medicine | https://doi.org/10.1080/07853890.2024.2416070 |
| New cases/year | United States, osteonecrosis/ONFH | 10,000–20,000 new cases/year | Annual | Reported in recent ONFH review; lower U.S. estimate than older reviews (li2024pathologicalmechanismsand pages 1-2, ng2023increasingtrendtoward pages 6-7) | Li 2024, Annals of Medicine | https://doi.org/10.1080/07853890.2024.2416070 |
| New cases/year | United States, ONFH | 20,000–30,000 new cases/year | Annual | Frequently cited benchmark in reviews and imaging/epidemiology overviews (shao2024unravelingtherole pages 1-2, rohilla2025adescriptivestudy pages 1-2, moyaangeler2015currentconceptson pages 1-2) | Moya-Angeler 2015, World Journal of Orthopedics | https://doi.org/10.5312/wjo.v6.i8.590 |
| Incidence | Japan, ONFH | 1.91/100,000 | Annual | Reported alongside national case counts in 2024 review (li2024pathologicalmechanismsand pages 1-2) | Li 2024, Annals of Medicine | https://doi.org/10.1080/07853890.2024.2416070 |
| New cases/year | Japan, ONFH | 2,500–3,300 new cases/year | Annual | National estimate cited in recent review (li2024pathologicalmechanismsand pages 1-2) | Li 2024, Annals of Medicine | https://doi.org/10.1080/07853890.2024.2416070 |
| Affected population | China, ONFH | >8 million patients | Contemporary estimate | Large disease burden repeatedly cited in recent reviews (zhang2024advancesinthe pages 1-2, li2024pathologicalmechanismsand pages 1-2) | Li 2024, Annals of Medicine | https://doi.org/10.1080/07853890.2024.2416070 |
| New cases/year | China, ONFH | 50,000–100,000 new cases/year | Annual | Prognostic modeling paper estimate (yang2024adelphibasedmodel pages 1-2) | Yang 2024, Journal of Orthopaedic Surgery and Research | https://doi.org/10.1186/s13018-024-05247-0 |
| Incidence | Asia, ONFH | 1.91–5.0 per 10,000 individuals | Not specified | Reported in bibliometric review summarizing prior epidemiology sources (pang2025thebibliometricand pages 1-2) | Pang 2025, Journal of Orthopaedic Surgery and Research | https://doi.org/10.1186/s13018-025-06138-8 |
| Progression/collapse risk | Untreated ONFH | >80% progress to femoral head collapse | Within 2 years | Reported for patients without early intervention in recent pathogenesis review (zhang2024advancesinthe pages 1-2) | Zhang 2024, Biomolecules | https://doi.org/10.3390/biom14060667 |
| Progression/collapse risk | Untreated ONFH | >80% progress to collapse and arthritis | Not specified | Similar natural-history estimate in nationwide U.S. trends paper (ng2023increasingtrendtoward pages 1-2) | Ng 2023, Arthroplasty | https://doi.org/10.1186/s42836-023-00176-5 |
| Post-traumatic incidence | Adolescents after femoral neck fracture surgery | 24.02% (95% CI 21.18%–27.12%) | Postoperative follow-up across studies | Meta-analysis of 17 studies, n=862 adolescents (gu2024globalincidenceof pages 1-2) | Gu 2024, Journal of Orthopaedic Surgery and Research | https://doi.org/10.1186/s13018-024-05275-w |
| Surgical management proportion | U.S. ONFH patients receiving hip surgery | THA 94.97%; core decompression 3.20%; hemiarthroplasty/resurfacing 0.99%; bone grafting 0.46%; osteotomy 0.05% | 2010–2019 | Nationwide database study of 10,334 surgically treated patients (ng2023increasingtrendtoward pages 1-2) | Ng 2023, Arthroplasty | https://doi.org/10.1186/s42836-023-00176-5 |
| Arthroplasty burden | ONFH among all THAs in U.S. | ~10% of total hip arthroplasties | Annual | Longstanding benchmark repeated in reviews (moyaangeler2015currentconceptson pages 1-2, ng2023increasingtrendtoward pages 6-7) | Moya-Angeler 2015, World Journal of Orthopedics | https://doi.org/10.5312/wjo.v6.i8.590 |
| Mean age | AVN/ONFH hip cohort undergoing MRI staging | 41.2 years (range 20–63) | Study period 2 years | Descriptive MRI study, 50 patients/80 hips (rohilla2025adescriptivestudy pages 1-2) | Rohilla 2025, Cureus | https://doi.org/10.7759/cureus.86867 |
| Sex ratio | AVN/ONFH hip MRI cohort | Male 62%; male:female ratio 1.63:1 | Study period 2 years | Same cohort showed male predominance (rohilla2025adescriptivestudy pages 1-2) | Rohilla 2025, Cureus | https://doi.org/10.7759/cureus.86867 |
| Bilaterality | AVN/ONFH hip MRI cohort | 60% bilateral involvement | Cross-sectional cohort | 30/50 cases bilateral; 22% right unilateral; 18% left unilateral (rohilla2025adescriptivestudy pages 1-2) | Rohilla 2025, Cureus | https://doi.org/10.7759/cureus.86867 |
| Symptom frequency | AVN/ONFH hip MRI cohort | Hip pain in 86% | Cross-sectional cohort | 43/50 cases reported hip pain (rohilla2025adescriptivestudy pages 1-2) | Rohilla 2025, Cureus | https://doi.org/10.7759/cureus.86867 |
| ARCO stage distribution | AVN/ONFH hip MRI cohort (80 hips) | Stage I 13.75%; II 23.75%; IIIA 26.25%; IIIB 10%; IV 26.25% | Cross-sectional cohort | Demonstrates mixed pre- and post-collapse disease at presentation (rohilla2025adescriptivestudy pages 1-2) | Rohilla 2025, Cureus | https://doi.org/10.7759/cureus.86867 |
| Glucocorticoid etiologic threshold | ARCO glucocorticoid-associated ONFH research classification | >2 g prednisolone-equivalent | Within 3 months | Must also be diagnosed within 2 years of exposure and have no other major risk factor (yoon2019etiologicclassificationcriteria pages 5-8, yoon2019etiologicclassificationcriteria pages 1-5, yoon2019etiologicclassificationcriteria pages 8-12) | Yoon 2019, Journal of Arthroplasty | https://doi.org/10.1016/j.arth.2018.09.005 |
| Alcohol etiologic threshold | ARCO alcohol-associated ONFH research classification | >320 g/week alcohol (>400 mL/week ethanol-containing consumption as summarized) | Diagnosis within 1 year of such consumption | No other major risk factor; threshold summarized in Ko 2023 review of ARCO criteria (ko2023updatingosteonecrosisof pages 1-2) | Ko 2023, Hip & Pelvis | https://doi.org/10.5371/hp.2023.35.3.147 |
| Daily glucocorticoid dose effect | Glucocorticoid-exposed patients | +4.6% ONFH rate per additional 10 mg/day; OR 4.2 for daily dose >40 mg | Exposure-related | Dose-response summarized in ARCO etiologic consensus (yoon2019etiologicclassificationcriteria pages 5-8) | Yoon 2019, Journal of Arthroplasty | https://doi.org/10.1016/j.arth.2018.09.005 |
| Early cumulative steroid exposure vs ONFH incidence | Post-transplant recipients in cited evidence | 6% (≤520 mg), 17% (520–600 mg), 28% (>600 mg) | First 2 weeks post-transplant exposure | Historical dose-response data summarized in ARCO consensus (yoon2019etiologicclassificationcriteria pages 5-8) | Yoon 2019, Journal of Arthroplasty | https://doi.org/10.1016/j.arth.2018.09.005 |
| Long-term glucocorticoid complication rate | Long-term glucocorticoid users | 5%–40% may develop osteonecrosis | Long-term use | Systematic review on hormone-induced ONFH pathogenesis (ma2024researchprogressin pages 2-3) | Ma 2024, Journal of Orthopaedic Surgery and Research | https://doi.org/10.1186/s13018-024-04748-2 |
| Long-term glucocorticoid skeletal complication rate | Long-term glucocorticoid users | 30%–50% may have fractures | Long-term use | Contextualizes steroid toxicity burden (ma2024researchprogressin pages 2-3) | Ma 2024, Journal of Orthopaedic Surgery and Research | https://doi.org/10.1186/s13018-024-04748-2 |
| Non-traumatic subtype share | Asia, non-traumatic ONFH due to alcohol | 32.4%–45.3% of non-traumatic ONFH | Not specified | Estimate cited in alcohol-focused literature synthesis (pang2025thebibliometricand pages 1-2) | Pang 2025, Journal of Orthopaedic Surgery and Research | https://doi.org/10.1186/s13018-025-06138-8 |
| THA utilization | U.S. ONFH patients in summarized 2010–2020 data | 94% underwent joint replacement; THA 88.1% of procedures | 2010–2020 | Reported in alcohol-induced ONFH bibliometric review summarizing U.S. data (pang2025thebibliometricand pages 1-2) | Pang 2025, Journal of Orthopaedic Surgery and Research | https://doi.org/10.1186/s13018-025-06138-8 |
| End-stage treatment burden | China, ONFH | >80% eventually undergo total joint arthroplasty | Not specified | Reported in endothelial dysfunction review (shao2024unravelingtherole pages 1-2) | Shao 2024, Biomedicines | https://doi.org/10.3390/biomedicines12030664 |
Table: This table summarizes quantitative epidemiology, natural history, and exposure-threshold statistics for osteonecrosis/osteonecrosis of the femoral head from the gathered evidence. It is useful for quickly comparing disease burden, progression risk, and major etiologic thresholds across populations and studies.
9.2 Population demographics
Typical affected age is young to middle-aged adults; an MRI cohort had mean age 41.2. (rohilla2025adescriptivestudy pages 1-2, moyaangeler2015currentconceptson pages 1-2)
Sex distribution may skew male in some cohorts (e.g., 62% male in MRI cohort). (rohilla2025adescriptivestudy pages 1-2)
9.3 Inheritance pattern
No Mendelian inheritance pattern is supported in the retrieved corpus; genetic evidence is mainly susceptibility loci and pathway-level associations. (shi202417variantsinteraction pages 1-2, jia2024bonebiochemicalmarkers pages 1-2)
10. Diagnostics
10.1 Imaging
Diagnostic evaluation relies on radiography followed by MRI for early detection. * First radiographic changes may be cystic and sclerotic changes; however, radiographs are often insufficient early. (moyaangeler2015currentconceptson pages 1-2) * MRI is emphasized as a benchmark for early diagnosis and for staging systems like ARCO. (moyaangeler2015currentconceptson pages 1-2, rohilla2025adescriptivestudy pages 1-2)
10.2 Diagnostic staging/classification systems
Systems referenced include ARCO, Ficat and Arlet, Steinberg, and lesion-size measures such as the modified Kerboul angle (used as prognostic selection for decompression and biological augmentation). (rohilla2025adescriptivestudy pages 1-2, houdek2021hipdecompressioncombined pages 1-2)
10.3 Biomarkers (emerging)
Reviews and omics studies suggest potential biomarkers related to lipid metabolism, ER stress, and immune-inflammatory pathways, but none are established as standard clinical diagnostics in the retrieved evidence. Examples include ER-stress hub genes and lipid biomarkers (TG, HDL) as predictors in steroid-induced ONFH models. (jia2024predictingsteroidinducedosteonecrosis pages 12-12, wu2024identificationandvalidation pages 1-2)
10.4 Genetic testing
No clinical genetic testing algorithm or gene panel recommendation was identified in the retrieved text.
11. Outcome / Prognosis
11.1 Collapse and arthroplasty endpoints
Advanced ONFH often leads to arthroplasty. A 2024 endothelial dysfunction review states >80% eventually undergo total joint arthroplasty; U.S. administrative data show THA dominates surgical management (~95%). (shao2024unravelingtherole pages 1-2, ng2023increasingtrendtoward pages 1-2)
11.2 Prognostic factors
Prognostic factors for collapse include imaging-based lesion size/location and CT evidence of subchondral fracture, along with clinical and behavioral factors. * A 2024 Delphi-based prognostic model identified imaging and clinical factors (pain presence, JIC classification, necrotic area, weight-bearing reduction, anterolateral pillar preservation, subchondral fracture on CT) and achieved C-index 0.88. (yang2024adelphibasedmodel pages 1-2)
A long-term ARCO stage II pharmacologic cohort found LPA ≤60.9° predicted collapse risk (HR 3.87). (he2021thetherapeuticeffect pages 1-2)
12. Treatment
12.1 Current applications / real-world implementation patterns
In contemporary U.S. practice, THA remains the dominant surgical approach; joint-preserving procedures (core decompression, grafting) are a minority but have increased in younger patients. (ng2023increasingtrendtoward pages 1-2)
12.2 Joint-preserving procedures
Core decompression is the most widely used joint-preserving procedure, but failure rates can be high in real-world cohorts. (liu2021efficacyofvarious pages 1-2)
Adjunctive biologics/cell therapies show mixed but generally favorable meta-analytic signals for reducing collapse and THA conversion compared with CD alone, with heterogeneity and stage-dependence. (zhu2021comparisonofcell pages 1-2, liu2021efficacyofvarious pages 8-10)
12.3 Regenerative/cell therapy
Evidence spans: * Mid-term cohort: CD + BMAC + PRP in corticosteroid-induced precollapse ONFH showed 84% collapse-free and 67% THA-free survivorship at 7 years. (houdek2021hipdecompressioncombined pages 1-2) * Phase I/II MSC therapy: feasibility and safety with some clinical improvement; 50% eventually required THR over 8-year follow-up in small sample. (blanco2023longtermresultsof pages 8-10)
12.4 Total hip arthroplasty
A large 2024 cohort (876 THA patients) reported better short-term perioperative outcomes and 1-year HHS for ARCO stage III vs stage IV, but similar longer-term complication profiles, emphasizing stage at intervention influences early recovery. (li2024pathologicalmechanismsand pages 1-2)
12.5 Clinical trials (ClinicalTrials.gov; NCT identifiers)
Multiple interventional trials evaluate marrow/cell augmentation and procedural variants, including: * NCT01892514 (Phase 3, completed, n=104): CD + grafting + PRF + concentrated BM (MRI necrotic area reduction at 12 months as primary endpoint). (NCT01892514 chunk 1) * NCT01605383 (Phase I/II, completed, n=23): CD + autologous expanded MSCs on allogenic bone scaffold vs CD alone; endpoints include modified Kerboul angle and QoL scores. (NCT01605383 chunk 1) * NCT04233125 (Phase 1/2, completed, n=37): CD vs CD+PMMA cement packing, 5-year progression-free survival primary endpoint. (NCT04233125 chunk 1) * NCT00821470 (Phase 1, completed, n=21): CD vs CD + autologous bone marrow implantation; WOMAC at 60 months. (NCT00821470 chunk 1) * NCT01544712 (randomized, double-blind, completed, n=50): stage 3 ONFH CD + concentrated BM vs saline; later publication suggests inefficacy in stage III. (NCT01544712 chunk 1)
Suggested MAXO terms (high-level; ontology mapping): * Core decompression — MAXO term for decompression procedure (not retrieved explicitly) * Total hip arthroplasty — MAXO term for hip replacement (not retrieved explicitly) * Autologous MSC transplantation — MAXO cell therapy (not retrieved explicitly)
| Intervention | Indication/stage | Evidence summary (key numbers) | Implementation notes | Source | URL/NCT |
|---|---|---|---|---|---|
| Conservative management (weight-bearing restriction, pharmacotherapy, physical modalities) | Early/pre-collapse ONFH; individualized nonoperative care | 2024 systematic review included 11 studies from 376 records; conservative approaches may relieve symptoms and delay progression, but evidence remains heterogeneous and insufficient for strong efficacy conclusions (goncharov2024conservativetreatmentin pages 1-2) | Used mainly in early disease or when surgery is deferred/contraindicated; not clearly disease-modifying in advanced collapse | Goncharov 2024, Medical Sciences | https://doi.org/10.3390/medsci12030032 |
| Core decompression (CD) alone | Most commonly ARCO I-II; pre-collapse ONFH | Large retrospective cohort: 1,537 hips, overall CD failure rate 52.44%; failure associated with male sex, steroid/idiopathic etiology, seated occupation, older age, lower hemoglobin, longer disease duration, larger combined necrosis angle (AUC 0.935 prediction model) (liu2021efficacyofvarious pages 1-2) | Widely used joint-preserving procedure; best suited to carefully selected pre-collapse lesions | Wei 2023, BMC Musculoskeletal Disorders | https://doi.org/10.1186/s12891-023-06321-0 |
| CD plus adjunctive therapy (pooled: cell therapy, bone grafting, tantalum rod, biologics) | Mainly precollapse ONFH, especially stage I-II | Meta-analysis of 20 studies/2,123 hips: higher HHS (MD 6.46), lower VAS (MD -0.99), lower stage progression (OR 0.32), lower collapse (OR 0.32), lower THA conversion (OR 0.35) versus CD alone; no serious adverse events reported (zhu2021comparisonofcell pages 1-2) | Supports combined hip-preservation strategies when local expertise/resources available | Zhu 2021, Bone & Joint Research | https://doi.org/10.1302/2046-3758.107.bjr-2020-0418.r1 |
| CD plus cell therapy (network meta-analysis) | Joint-preserving treatment in ONFH, especially early disease | Network meta-analysis of 17 RCTs/918 hips: CD+cell therapy had best SUCRA for radiographic progression (96.4%), but no significant overall difference in THA conversion or HHS versus other interventions/nonoperative treatment (liu2021efficacyofvarious pages 1-2, liu2021efficacyofvarious pages 8-10) | Suggests radiographic benefit may exceed symptomatic/arthroplasty endpoint benefit; evidence mixed | Liu 2021, BMC Musculoskeletal Disorders | https://doi.org/10.1186/s12891-021-04808-2 |
| CD plus BMAC/PRP hip decompression | Precollapse corticosteroid-induced ONFH | 22 patients/35 hips; 7-year survivorship free from femoral head collapse 84% and free from THA 67%; worse outcomes with high modified Kerboul angle (HR 3.96) and continued corticosteroid use (HR 4.15) (houdek2021hipdecompressioncombined pages 1-2, houdek2021hipdecompressioncombined pages 5-6) | Real-world biologic augmentation strategy; candidate selection and stopping steroids matter | Houdek 2021, Bone & Joint Open | https://doi.org/10.1302/2633-1462.211.bjo-2021-0132.r1 |
| Autologous cultured MSC implantation | Idiopathic ONFH, ARCO < IIC | Phase I/II prospective trial, 8 patients: no cell-related adverse effects; 50% clinically improved at 1 year; none required THR in first year; at 8 years, 4/8 (50%) ultimately required THR after median ~574-576 days (blanco2023longtermresultsof pages 1-2, blanco2023longtermresultsof pages 10-11, blanco2023longtermresultsof pages 8-10) | GMP-expanded autologous BM-MSCs delivered intraosseously; feasible but small-sample evidence | Blanco 2023, Journal of Clinical Medicine | https://doi.org/10.3390/jcm12062117 |
| Autologous bone marrow concentrate added to CD (short-term RCT) | Non-traumatic femoral head necrosis | Prospective randomized trial in 24 patients found no short-term clinical or radiologic benefit from adding bone marrow concentrate to CD over 2 years, despite increased CFU counts after centrifugation (from abstract) (zhu2021comparisonofcell pages 11-12) | Illustrates inconsistency of BMAC evidence, especially in small short-term trials | Pepke 2016, Orthopedic Reviews | https://doi.org/10.4081/or.2016.6162 |
| Autologous bone marrow concentrate in stage III disease | Stage III non-traumatic ONFH | Randomized double-blind trial record later linked to publication titled “Inefficacy of autologous bone marrow concentrate in stage three osteonecrosis” (NCT01544712 chunk 1) | Suggests diminished value once collapse is established | NCT01544712 / Hauzeur trial | NCT01544712 |
| Bone grafting / regenerative graft combinations | Early ONFH (ARCO 2A-C in trial protocols) | Phase 3 RCT protocol compared CD+DBM+PRF+concentrated bone marrow vs CD+lyophilized bone chips+PRF+concentrated bone marrow; primary endpoint MRI necrotic-area reduction at 12 months; enrollment 104, completed (NCT01892514 chunk 1) | Reflects real-world use of graft plus marrow concentrate in hip-preserving centers | ClinicalTrials.gov AVN-13 | NCT01892514 |
| Tantalum rod insertion | Joint-preserving treatment, often pre-collapse/selected cases | Meta-analysis of 10 studies/550 hips: HHS improved by MD 30.35; radiographic progression 22.1%; femoral head collapse 10.2%; THA conversion 15.8% at mean 32.4 months (li2024pathologicalmechanismsand pages 1-2) | Structural support option; often considered where surgeons aim to avoid arthroplasty in younger patients | Onggo 2020, Journal of Hip Preservation Surgery | https://doi.org/10.1093/jhps/hnaa020 |
| Hyperbaric oxygen therapy (HBO) | Femoral head necrosis, mostly early-stage studies | Meta-analysis of 10 studies (368 HBO-treated, 353 controls): clinical effect OR 3.84 (95% CI 2.10-7.02); significant benefit in Asian subgroup (li2024pathologicalmechanismsand pages 1-2) | Available in selected centers; not universally adopted | Paderno 2021, IJERPH | https://doi.org/10.3390/ijerph18062888 |
| Extracorporeal shock wave therapy (ESWT) | ONFH, generally early disease | Meta-analysis of 9 studies/409 patients: improved HHS and VAS; MRI lesion metrics improved, but authors concluded it could not stop progression reliably (li2024pathologicalmechanismsand pages 1-2) | Noninvasive adjunct; symptom-focused with uncertain structural protection | Mei 2022, Physician and Sportsmedicine | https://doi.org/10.1080/00913847.2021.1936685 |
| THA (total hip arthroplasty) | Post-collapse or end-stage ONFH (ARCO III-IV/IV) | U.S. nationwide surgery data: THA was 94.97% of surgical management (9,814/10,334) (ng2023increasingtrendtoward pages 6-7); stage III vs IV cohort of 876 patients found stage III had shorter operative time, less bleeding, fewer 1-year readmissions/complications, and higher 1-year HHS; long-term difference not significant (li2024pathologicalmechanismsand pages 1-2) | Dominant real-world intervention for advanced disease; outcomes somewhat better when performed before most advanced degeneration | Ng 2023; Wang 2024 | https://doi.org/10.1186/s42836-023-00176-5 ; https://doi.org/10.1186/s13018-024-04617-y |
| Huo Xue Tong Luo capsules (pharmacologic/traditional medicine) | ARCO stage II ONFH | 44 patients/66 hips, mean follow-up 7.95 years: 69.7% had no progression in pain or collapse; only 1.5% required THA; 5-, 10-, and 15-year survivorship 96.97%, 69.15%, 40.33% (he2021thetherapeuticeffect pages 1-2) | Region-specific long-term observational/clinical evidence; not standard global care | He 2021, Frontiers in Pharmacology | https://doi.org/10.3389/fphar.2021.773758 |
| NCT06123481 Autologous Bone Marrow Aspirate Treatment for Early-Stage Osteonecrosis | Early-stage ONFH | Recruiting interventional study; enrollment 192 (trial registry listing) (NCT00821470 chunk 1) | Large contemporary marrow-based study may clarify real-world value of aspirate augmentation | ClinicalTrials.gov | NCT06123481 |
| NCT01605383 Mesenchymal Stem Cells in Osteonecrosis of the Femoral Head | ONFH treated with CD vs CD+autologous MSC tissue-engineering product | Phase I/II randomized prospective open-label/blinded-assessor trial; enrollment 23; completed; primary endpoints safety/feasibility over 12 months; secondary endpoints include modified Kerboul angle, gadolinium enhancement, VAS, SF-36, WOMAC (NCT01605383 chunk 1) | Important translational MSC trial using ex vivo expanded autologous cells on allogenic bone scaffold | ClinicalTrials.gov | NCT01605383 |
| NCT01892514 Randomized Clinical Trial for the Treatment of ONFH | Early-stage ONFH (ARCO 2A-C) | Phase III randomized double-masked trial; enrollment 104; completed; primary endpoint MRI reduction in total necrotic area at 12 months; secondary endpoints VAS, HHS, WOMAC, structural preservation (NCT01892514 chunk 1) | Directly compares two marrow/graft regenerative strategies after CD | ClinicalTrials.gov | NCT01892514 |
| NCT04233125 Core Decompression With or Without Cement Packing for ONFH | Symptomatic precollapse ARCO I-II ONFH | Phase I/II randomized parallel trial; enrollment 37; completed; compares CD vs CD+PMMA; primary endpoint progression-free survival at 5 years; secondary endpoints conversion-free survival/THA, HHS, WOMAC, SF-36 (NCT04233125 chunk 1, NCT04233125 chunk 2) | Practical surgical optimization trial for pre-collapse disease | ClinicalTrials.gov | NCT04233125 |
| NCT00821470 Treatment of Osteonecrosis of the Femoral Head by Bone Marrow Transplantation | ARCO stage 1-2 ONFH | Phase I pilot; enrollment 21; completed; core decompression vs CD+autologous bone marrow implantation; primary endpoint WOMAC at 60 months; secondary endpoint progression to fractural stage (NCT00821470 chunk 1) | Early landmark marrow-implantation trial conceptually underpinning later cell-therapy approaches | ClinicalTrials.gov | NCT00821470 |
| NCT01544712 Controlled Study of Stage 3 Osteonecrosis Treatment by Bone Marrow | Stage III non-traumatic ONFH | Randomized double-blind parallel trial; enrollment 50; completed; CD+40 mL concentrated autologous bone marrow vs CD+saline; primary endpoint need for total prosthesis at 24 and 60 months (NCT01544712 chunk 1) | Useful registry example of later-stage biologic augmentation testing | ClinicalTrials.gov | NCT01544712 |
Table: This table summarizes current treatment strategies for osteonecrosis of the femoral head, including conservative care, procedures, regenerative therapies, and major clinical trials. It highlights where evidence is strongest, how interventions are used in practice, and which studies provide key quantitative outcomes.
13. Prevention
Primary prevention is risk-factor modification where feasible: * Avoiding unnecessary high-dose or prolonged glucocorticoid exposure and minimizing cumulative dose where clinically appropriate, given clear dose-response risk. (yoon2019etiologicclassificationcriteria pages 5-8) * Alcohol moderation/cessation in high-risk individuals and ARCO-defined alcohol-associated ONFH populations. (ko2023updatingosteonecrosisof pages 1-2)
Secondary prevention includes surveillance/early imaging in high-risk patients. Early screening is highlighted in postoperative adolescent fracture populations given high ONFH incidence. (gu2024globalincidenceof pages 1-2)
14. Other Species / Natural Disease
No naturally occurring osteonecrosis syndromes in non-human species were retrieved in the accessible corpus for this run.
15. Model Organisms
A 2024 Bone Research study provides a detailed glucocorticoid-induced ONFH mouse model (12-week-old male C57BL/6; methylprednisolone dosing regimen) and mechanistic pathway linking hypothalamic sympathetic tone to endothelial injury and osteonecrosis. (shao2024inhibitionofsympathetic pages 1-2, shao2024inhibitionofsympathetic pages 3-4)
Suggested model-ontology mapping: * Mus musculus — NCBI Taxon:10090 (not in retrieved text but standard)
Recent developments and expert synthesis (2023–2024 highlights)
1) ARCO framework refinement and operationalization: Ko 2023 synthesizes ARCO etiologic criteria and the revised 2019 ARCO staging that splits stage III into IIIA/IIIB by ≤2 mm vs >2 mm depression, enabling more standardized pre-/post-collapse stratification in clinical research and registries. (ko2023updatingosteonecrosisof pages 2-4, ko2023updatingosteonecrosisof media 0e890259) 2) Mechanistic convergence on vascular biology: 2024 reviews increasingly treat endothelial dysfunction and microvascular impairment as central, with immune-inflammatory amplification and impaired angiogenesis–osteogenesis coupling as key downstream processes. (shao2024unravelingtherole pages 1-2, ma2024researchprogressin pages 1-2) 3) Neurovascular mechanism (2024): the hypothalamic-sympathetic-endothelial axis (ADRB2–CREB–PFKFB3) is a notable mechanistic advance, suggesting potential therapeutic targets beyond bone-centric approaches. (shao2024inhibitionofsympathetic pages 1-2, shao2024inhibitionofsympathetic pages 2-3) 4) Omics and biomarker directions (2024): transcriptomic and bioinformatics analyses implicate ER stress–inflammation networks (STAT3/IL1B/TLR2/CASP1) and lipid metabolism/radiomics predictors (TG/HDL + imaging features), supporting a shift toward risk prediction and early detection research. (jia2024predictingsteroidinducedosteonecrosis pages 12-12, wu2024identificationandvalidation pages 1-2)
Notes on citation requirements (PMIDs and abstract quotes)
- Many retrieved open-access articles provide DOIs and abstracts, but PMIDs are not consistently present in the extracted full-text snippets. Where PMIDs were requested, this report cannot reliably supply them from the retrieved context.
- Direct abstract quotations are provided only when the abstract text was present in the retrieved snippets (e.g., ClinicalTrials.gov records and several article abstracts). For some mechanistic papers (e.g., Bone Research 2024), the abstract text was not present in the extracted pages; therefore, direct quotes cannot be provided despite inclusion of mechanistic details from the main text/figures.
Supporting figure/table evidence
The revised 2019 ARCO staging table and representative imaging examples were retrieved as cropped images from Ko 2023. (ko2023updatingosteonecrosisof media 0e890259, ko2023updatingosteonecrosisof media 85ac9cbb)
References
-
(zhang2024advancesinthe pages 1-2): Jie Zhang, Jianze Cao, Yongfei Liu, and Haiyan Zhao. Advances in the pathogenesis of steroid-associated osteonecrosis of the femoral head. Biomolecules, 14:667, Jun 2024. URL: https://doi.org/10.3390/biom14060667, doi:10.3390/biom14060667. This article has 53 citations.
-
(moyaangeler2015currentconceptson pages 1-2): J. Moya-Angeler, Arianna L. Gianakos, J. Villa, A. Ni, and J. Lane. Current concepts on osteonecrosis of the femoral head. World journal of orthopedics, 6 8:590-601, Sep 2015. URL: https://doi.org/10.5312/wjo.v6.i8.590, doi:10.5312/wjo.v6.i8.590. This article has 672 citations and is from a peer-reviewed journal.
-
(ko2023updatingosteonecrosisof pages 1-2): Young-Seung Ko, Joo Hyung Ha, Jung-Wee Park, Young-Kyun Lee, Tae-Young Kim, and Kyung-Hoi Koo. Updating osteonecrosis of the femoral head. Hip & Pelvis, 35:147-156, Sep 2023. URL: https://doi.org/10.5371/hp.2023.35.3.147, doi:10.5371/hp.2023.35.3.147. This article has 45 citations.
-
(ng2023increasingtrendtoward pages 1-2): Mitchell K. Ng, Andriy Kobryn, Ivan J. Golub, Nicolas S. Piuzzi, Che Hang Jason Wong, Lynne Jones, and Michael A. Mont. Increasing trend toward joint-preserving procedures for hip osteonecrosis in the united states from 2010 to 2019. Arthroplasty, May 2023. URL: https://doi.org/10.1186/s42836-023-00176-5, doi:10.1186/s42836-023-00176-5. This article has 11 citations.
-
(xiang2024advancesinmechanism pages 1-2): Xiao-Na Xiang, Hong-Chen He, and Cheng-Qi He. Advances in mechanism and management of bone homeostasis in osteonecrosis: a review article from basic to clinical applications. International Journal of Surgery (London, England), 111:1101-1122, Sep 2024. URL: https://doi.org/10.1097/js9.0000000000002094, doi:10.1097/js9.0000000000002094. This article has 12 citations.
-
(rohilla2025adescriptivestudy pages 1-2): Bhawna Rohilla, Lavanya Dharmalingam, G. Kamalakannan, and Prabhu C S. A descriptive study on the role of magnetic resonance imaging in staging avascular necrosis of the hip joint: current trends and insights. Cureus, Jun 2025. URL: https://doi.org/10.7759/cureus.86867, doi:10.7759/cureus.86867. This article has 2 citations.
-
(ko2023updatingosteonecrosisof pages 6-8): Young-Seung Ko, Joo Hyung Ha, Jung-Wee Park, Young-Kyun Lee, Tae-Young Kim, and Kyung-Hoi Koo. Updating osteonecrosis of the femoral head. Hip & Pelvis, 35:147-156, Sep 2023. URL: https://doi.org/10.5371/hp.2023.35.3.147, doi:10.5371/hp.2023.35.3.147. This article has 45 citations.
-
(li2024pathologicalmechanismsand pages 1-2): Longyu Li, Shangkun Zhao, Zikuan Leng, Songfeng Chen, Yifang Shi, Lijun Shi, Jinfeng Li, Keya Mao, Hai Tang, Bin Meng, Yisheng Wang, Guowei Shang, and Hongjian Liu. Pathological mechanisms and related markers of steroid-induced osteonecrosis of the femoral head. Annals of Medicine, Nov 2024. URL: https://doi.org/10.1080/07853890.2024.2416070, doi:10.1080/07853890.2024.2416070. This article has 43 citations and is from a domain leading peer-reviewed journal.
-
(yoon2019etiologicclassificationcriteria pages 5-8): Byung-Ho Yoon, Lynne C. Jones, Chung-Hwan Chen, Edward Y. Cheng, Quanjun Cui, Wolf Drescher, Wakaba Fukushima, Valerie Gangji, Stuart B. Goodman, Yong-Chan Ha, Philippe Hernigou, Marc Hungerford, Richard Iorio, Woo-Lam Jo, Vikas Khanduja, Harry Kim, Shin-Yoon Kim, Tae-Young Kim, Hee Young Lee, Mel S. Lee, Young-Kyun Lee, Yun Jong Lee, Michael A. Mont, Takashi Sakai, Nobuhiko Sugano, Masaki Takao, Takuaki Yamamoto, and Kyung-Hoi Koo. Etiologic classification criteria of arco on femoral head osteonecrosis part 1: glucocorticoid-associated osteonecrosis. The Journal of arthroplasty, 34 1:163-168.e1, Jan 2019. URL: https://doi.org/10.1016/j.arth.2018.09.005, doi:10.1016/j.arth.2018.09.005. This article has 160 citations.
-
(houdek2021hipdecompressioncombined pages 1-2): Matthew T. Houdek, Cody C. Wyles, John-Rudolph H. Smith, Andre Terzic, Atta Behfar, and Rafael J. Sierra. Hip decompression combined with bone marrow concentrate and platelet-rich plasma for corticosteroid-induced osteonecrosis of the femoral head. Bone & Joint Open, 2:926-931, Nov 2021. URL: https://doi.org/10.1302/2633-1462.211.bjo-2021-0132.r1, doi:10.1302/2633-1462.211.bjo-2021-0132.r1. This article has 18 citations and is from a peer-reviewed journal.
-
(blanco2023longtermresultsof pages 8-10): Juan F. Blanco, Francisco J. Garcia-Garcia, Eva M. Villarón, Carmen da Casa, Helena Fidalgo, Miriam López-Parra, José A. Santos, and Fermín Sánchez-Guijo. Long-term results of a phase i/ii clinical trial of autologous mesenchymal stem cell therapy for femoral head osteonecrosis. Journal of Clinical Medicine, 12:2117, Mar 2023. URL: https://doi.org/10.3390/jcm12062117, doi:10.3390/jcm12062117. This article has 7 citations.
-
(shao2024inhibitionofsympathetic pages 1-2): Wenkai Shao, Bo Wang, Ping Wang, Shuo Zhang, Song Gong, Xiaodong Guo, Deyu Duan, Zengwu Shao, Weijian Liu, Lei He, Fei Gao, Xiao Lv, and Yong Feng. Inhibition of sympathetic tone via hypothalamic descending pathway propagates glucocorticoid-induced endothelial impairment and osteonecrosis of the femoral head. Bone Research, Nov 2024. URL: https://doi.org/10.1038/s41413-024-00371-3, doi:10.1038/s41413-024-00371-3. This article has 20 citations and is from a domain leading peer-reviewed journal.
-
(gu2024globalincidenceof pages 1-2): Bangning Gu, Fangming Yao, Peng Peng, Zijun Zeng, Wei He, and Qiushi Wei. Global incidence of osteonecrosis of the femoral head after femoral neck fracture surgery in adolescents: a meta-analysis. Journal of Orthopaedic Surgery and Research, Nov 2024. URL: https://doi.org/10.1186/s13018-024-05275-w, doi:10.1186/s13018-024-05275-w. This article has 3 citations and is from a peer-reviewed journal.
-
(shao2024unravelingtherole pages 1-2): Wenkai Shao, Ping Wang, Xiao Lv, Bo Wang, Song Gong, and Yong Feng. Unraveling the role of endothelial dysfunction in osteonecrosis of the femoral head: a pathway to new therapies. Biomedicines, 12:664, Mar 2024. URL: https://doi.org/10.3390/biomedicines12030664, doi:10.3390/biomedicines12030664. This article has 29 citations.
-
(yoon2019etiologicclassificationcriteria pages 1-5): Byung-Ho Yoon, Lynne C. Jones, Chung-Hwan Chen, Edward Y. Cheng, Quanjun Cui, Wolf Drescher, Wakaba Fukushima, Valerie Gangji, Stuart B. Goodman, Yong-Chan Ha, Philippe Hernigou, Marc Hungerford, Richard Iorio, Woo-Lam Jo, Vikas Khanduja, Harry Kim, Shin-Yoon Kim, Tae-Young Kim, Hee Young Lee, Mel S. Lee, Young-Kyun Lee, Yun Jong Lee, Michael A. Mont, Takashi Sakai, Nobuhiko Sugano, Masaki Takao, Takuaki Yamamoto, and Kyung-Hoi Koo. Etiologic classification criteria of arco on femoral head osteonecrosis part 1: glucocorticoid-associated osteonecrosis. The Journal of arthroplasty, 34 1:163-168.e1, Jan 2019. URL: https://doi.org/10.1016/j.arth.2018.09.005, doi:10.1016/j.arth.2018.09.005. This article has 160 citations.
-
(jia2024bonebiochemicalmarkers pages 1-2): Hai-feng Jia, Ze-ming Tian, Xue-zhen Liang, Han-zheng Li, Bo-wen Lu, Jian Zhang, and Gang Li. Bone biochemical markers, bone mineral density, and the risk of osteonecrosis of the femoral head: a mendelian randomization study. BMC Musculoskeletal Disorders, Dec 2024. URL: https://doi.org/10.1186/s12891-024-08130-5, doi:10.1186/s12891-024-08130-5. This article has 3 citations and is from a peer-reviewed journal.
-
(shi202417variantsinteraction pages 1-2): Chuankai Shi, Xin Li, Yu Sun, Zhenwu Du, Guizhen Zhang, Zhenjia Che, Qingyu Li, Shiliang Song, Jing Guo, Haoyan Sun, and Yang Song. 17 variants interaction of wnt/β-catenin pathway associated with development of osteonecrosis of femoral head in chinese han population. Scientific Reports, Mar 2024. URL: https://doi.org/10.1038/s41598-024-57929-8, doi:10.1038/s41598-024-57929-8. This article has 1 citations and is from a peer-reviewed journal.
-
(shi202417variantsinteraction pages 9-11): Chuankai Shi, Xin Li, Yu Sun, Zhenwu Du, Guizhen Zhang, Zhenjia Che, Qingyu Li, Shiliang Song, Jing Guo, Haoyan Sun, and Yang Song. 17 variants interaction of wnt/β-catenin pathway associated with development of osteonecrosis of femoral head in chinese han population. Scientific Reports, Mar 2024. URL: https://doi.org/10.1038/s41598-024-57929-8, doi:10.1038/s41598-024-57929-8. This article has 1 citations and is from a peer-reviewed journal.
-
(yoon2019etiologicclassificationcriteria pages 8-12): Byung-Ho Yoon, Lynne C. Jones, Chung-Hwan Chen, Edward Y. Cheng, Quanjun Cui, Wolf Drescher, Wakaba Fukushima, Valerie Gangji, Stuart B. Goodman, Yong-Chan Ha, Philippe Hernigou, Marc Hungerford, Richard Iorio, Woo-Lam Jo, Vikas Khanduja, Harry Kim, Shin-Yoon Kim, Tae-Young Kim, Hee Young Lee, Mel S. Lee, Young-Kyun Lee, Yun Jong Lee, Michael A. Mont, Takashi Sakai, Nobuhiko Sugano, Masaki Takao, Takuaki Yamamoto, and Kyung-Hoi Koo. Etiologic classification criteria of arco on femoral head osteonecrosis part 1: glucocorticoid-associated osteonecrosis. The Journal of arthroplasty, 34 1:163-168.e1, Jan 2019. URL: https://doi.org/10.1016/j.arth.2018.09.005, doi:10.1016/j.arth.2018.09.005. This article has 160 citations.
-
(pang2025thebibliometricand pages 1-2): Kai Pang, Huiying Li, Haifeng Chen, Zhentao Man, Dandan Wang, and Wei Li. The bibliometric and visualization analysis of alcohol-induced osteonecrosis of the femoral head: research trends and future directions (1998–2024). Journal of Orthopaedic Surgery and Research, Aug 2025. URL: https://doi.org/10.1186/s13018-025-06138-8, doi:10.1186/s13018-025-06138-8. This article has 1 citations and is from a peer-reviewed journal.
-
(ma2024researchprogressin pages 2-3): Tiancheng Ma, Yan Wang, Jianxiong Ma, Hongwei Cui, Xiaotian Feng, and Xinlong Ma. Research progress in the pathogenesis of hormone-induced femoral head necrosis based on microvessels: a systematic review. Journal of Orthopaedic Surgery and Research, Apr 2024. URL: https://doi.org/10.1186/s13018-024-04748-2, doi:10.1186/s13018-024-04748-2. This article has 26 citations and is from a peer-reviewed journal.
-
(ma2024researchprogressin pages 1-2): Tiancheng Ma, Yan Wang, Jianxiong Ma, Hongwei Cui, Xiaotian Feng, and Xinlong Ma. Research progress in the pathogenesis of hormone-induced femoral head necrosis based on microvessels: a systematic review. Journal of Orthopaedic Surgery and Research, Apr 2024. URL: https://doi.org/10.1186/s13018-024-04748-2, doi:10.1186/s13018-024-04748-2. This article has 26 citations and is from a peer-reviewed journal.
-
(jia2024predictingsteroidinducedosteonecrosis pages 12-12): Daqi Jia, Yue Zhang, Huaqiang Li, Chunfang Guo, Yipeng Wu, Xiangwen Shi, Li Yang, Jieyu Mo, Xia Liu, and Yongqing Xu. Predicting steroid-induced osteonecrosis of the femoral head: role of lipid metabolism biomarkers and radiomics in young and middle-aged adults. Journal of Orthopaedic Surgery and Research, Nov 2024. URL: https://doi.org/10.1186/s13018-024-05245-2, doi:10.1186/s13018-024-05245-2. This article has 9 citations and is from a peer-reviewed journal.
-
(xiang2024advancesinmechanism pages 18-18): Xiao-Na Xiang, Hong-Chen He, and Cheng-Qi He. Advances in mechanism and management of bone homeostasis in osteonecrosis: a review article from basic to clinical applications. International Journal of Surgery (London, England), 111:1101-1122, Sep 2024. URL: https://doi.org/10.1097/js9.0000000000002094, doi:10.1097/js9.0000000000002094. This article has 12 citations.
-
(yang2024adelphibasedmodel pages 1-2): Tong-jie Yang, Shi-yi Sun, Lei Zhang, Xing-ping Zhang, and Hai-jun He. A delphi-based model for prognosis of femoral head collapse in osteonecrosis: a multi-factorial approach. Journal of Orthopaedic Surgery and Research, Nov 2024. URL: https://doi.org/10.1186/s13018-024-05247-0, doi:10.1186/s13018-024-05247-0. This article has 8 citations and is from a peer-reviewed journal.
-
(liu2021efficacyofvarious pages 1-2): Quanzhe Liu, Wenlai Guo, Rui Li, and Jae Hyup Lee. Efficacy of various core decompression techniques versus non-operative treatment for osteonecrosis of the femoral head: a systemic review and network meta-analysis of randomized controlled trials. BMC Musculoskeletal Disorders, Nov 2021. URL: https://doi.org/10.1186/s12891-021-04808-2, doi:10.1186/s12891-021-04808-2. This article has 38 citations and is from a peer-reviewed journal.
-
(he2021thetherapeuticeffect pages 1-2): Xiao-Ming He, Min-Cong He, Peng Yang, Qing-Wen Zhang, Zhen-Qiu Chen, Wei He, and Qiu-Shi Wei. The therapeutic effect of huo xue tong luo capsules in association research circulation osseous (arco) stage ii osteonecrosis of the femoral head: a clinical study with an average follow-up period of 7.95 years. Frontiers in Pharmacology, Nov 2021. URL: https://doi.org/10.3389/fphar.2021.773758, doi:10.3389/fphar.2021.773758. This article has 20 citations.
-
(NCT01605383 chunk 1): Mesenchymal Stem Cells in Osteonecrosis of the Femoral Head. Banc de Sang i Teixits. 2015. ClinicalTrials.gov Identifier: NCT01605383
-
(NCT04233125 chunk 1): Core Decompression With or Without Cement Packing for ONFH. University of Minnesota. 1997. ClinicalTrials.gov Identifier: NCT04233125
-
(wu2024identificationandvalidation pages 1-2): Tingyu Wu, Weipeng Shi, Yinxue Zhou, Sijia Guo, Hua Tian, Yaping Jiang, Weiyan Li, Yingzhen Wang, and Tao Li. Identification and validation of endoplasmic reticulum stress-related genes in patients with steroid-induced osteonecrosis of the femoral head. Scientific Reports, Sep 2024. URL: https://doi.org/10.1038/s41598-024-72941-8, doi:10.1038/s41598-024-72941-8. This article has 10 citations and is from a peer-reviewed journal.
-
(li2024pathologicalmechanismsand pages 8-9): Longyu Li, Shangkun Zhao, Zikuan Leng, Songfeng Chen, Yifang Shi, Lijun Shi, Jinfeng Li, Keya Mao, Hai Tang, Bin Meng, Yisheng Wang, Guowei Shang, and Hongjian Liu. Pathological mechanisms and related markers of steroid-induced osteonecrosis of the femoral head. Annals of Medicine, Nov 2024. URL: https://doi.org/10.1080/07853890.2024.2416070, doi:10.1080/07853890.2024.2416070. This article has 43 citations and is from a domain leading peer-reviewed journal.
-
(ko2023updatingosteonecrosisof pages 2-4): Young-Seung Ko, Joo Hyung Ha, Jung-Wee Park, Young-Kyun Lee, Tae-Young Kim, and Kyung-Hoi Koo. Updating osteonecrosis of the femoral head. Hip & Pelvis, 35:147-156, Sep 2023. URL: https://doi.org/10.5371/hp.2023.35.3.147, doi:10.5371/hp.2023.35.3.147. This article has 45 citations.
-
(shao2024inhibitionofsympathetic pages 2-3): Wenkai Shao, Bo Wang, Ping Wang, Shuo Zhang, Song Gong, Xiaodong Guo, Deyu Duan, Zengwu Shao, Weijian Liu, Lei He, Fei Gao, Xiao Lv, and Yong Feng. Inhibition of sympathetic tone via hypothalamic descending pathway propagates glucocorticoid-induced endothelial impairment and osteonecrosis of the femoral head. Bone Research, Nov 2024. URL: https://doi.org/10.1038/s41413-024-00371-3, doi:10.1038/s41413-024-00371-3. This article has 20 citations and is from a domain leading peer-reviewed journal.
-
(ko2023updatingosteonecrosisof media 0e890259): Young-Seung Ko, Joo Hyung Ha, Jung-Wee Park, Young-Kyun Lee, Tae-Young Kim, and Kyung-Hoi Koo. Updating osteonecrosis of the femoral head. Hip & Pelvis, 35:147-156, Sep 2023. URL: https://doi.org/10.5371/hp.2023.35.3.147, doi:10.5371/hp.2023.35.3.147. This article has 45 citations.
-
(ko2023updatingosteonecrosisof media 85ac9cbb): Young-Seung Ko, Joo Hyung Ha, Jung-Wee Park, Young-Kyun Lee, Tae-Young Kim, and Kyung-Hoi Koo. Updating osteonecrosis of the femoral head. Hip & Pelvis, 35:147-156, Sep 2023. URL: https://doi.org/10.5371/hp.2023.35.3.147, doi:10.5371/hp.2023.35.3.147. This article has 45 citations.
-
(ng2023increasingtrendtoward pages 6-7): Mitchell K. Ng, Andriy Kobryn, Ivan J. Golub, Nicolas S. Piuzzi, Che Hang Jason Wong, Lynne Jones, and Michael A. Mont. Increasing trend toward joint-preserving procedures for hip osteonecrosis in the united states from 2010 to 2019. Arthroplasty, May 2023. URL: https://doi.org/10.1186/s42836-023-00176-5, doi:10.1186/s42836-023-00176-5. This article has 11 citations.
-
(zhu2021comparisonofcell pages 1-2): Shibai Zhu, Xiaotian Zhang, Xi Chen, Yiou Wang, Shanni Li, and Wenwei Qian. Comparison of cell therapy and other novel adjunctive therapies combined with core decompression for the treatment of osteonecrosis of the femoral head. Bone & Joint Research, 10:445-458, Jul 2021. URL: https://doi.org/10.1302/2046-3758.107.bjr-2020-0418.r1, doi:10.1302/2046-3758.107.bjr-2020-0418.r1. This article has 35 citations.
-
(liu2021efficacyofvarious pages 8-10): Quanzhe Liu, Wenlai Guo, Rui Li, and Jae Hyup Lee. Efficacy of various core decompression techniques versus non-operative treatment for osteonecrosis of the femoral head: a systemic review and network meta-analysis of randomized controlled trials. BMC Musculoskeletal Disorders, Nov 2021. URL: https://doi.org/10.1186/s12891-021-04808-2, doi:10.1186/s12891-021-04808-2. This article has 38 citations and is from a peer-reviewed journal.
-
(NCT01892514 chunk 1): Randomized Clinical Trial for the Treatment of Osteonecrosis of the Femoral Head. Istituto Ortopedico Rizzoli. 2013. ClinicalTrials.gov Identifier: NCT01892514
-
(NCT00821470 chunk 1): Treatment of Osteonecrosis of the Femoral Head by Bone Marrow Transplantation. Erasme University Hospital. 1999. ClinicalTrials.gov Identifier: NCT00821470
-
(NCT01544712 chunk 1): Jean-Philippe Hauzeur. Controlled Study of Stage 3 Osteonecrosis Treatment by Bone Marrow. University of Liege. 2004. ClinicalTrials.gov Identifier: NCT01544712
-
(goncharov2024conservativetreatmentin pages 1-2): Evgeniy Nikolaevich Goncharov, Oleg Aleksandrovich Koval, Eduard Nikolaevich Bezuglov, Aleksandr Aleksandrovich Vetoshkin, Nikolay Gavriilovich Goncharov, Manuel De Jesus Encarnación Ramirez, and Nicola Montemurro. Conservative treatment in avascular necrosis of the femoral head: a systematic review. Medical Sciences, 12:32, Jul 2024. URL: https://doi.org/10.3390/medsci12030032, doi:10.3390/medsci12030032. This article has 26 citations.
-
(houdek2021hipdecompressioncombined pages 5-6): Matthew T. Houdek, Cody C. Wyles, John-Rudolph H. Smith, Andre Terzic, Atta Behfar, and Rafael J. Sierra. Hip decompression combined with bone marrow concentrate and platelet-rich plasma for corticosteroid-induced osteonecrosis of the femoral head. Bone & Joint Open, 2:926-931, Nov 2021. URL: https://doi.org/10.1302/2633-1462.211.bjo-2021-0132.r1, doi:10.1302/2633-1462.211.bjo-2021-0132.r1. This article has 18 citations and is from a peer-reviewed journal.
-
(blanco2023longtermresultsof pages 1-2): Juan F. Blanco, Francisco J. Garcia-Garcia, Eva M. Villarón, Carmen da Casa, Helena Fidalgo, Miriam López-Parra, José A. Santos, and Fermín Sánchez-Guijo. Long-term results of a phase i/ii clinical trial of autologous mesenchymal stem cell therapy for femoral head osteonecrosis. Journal of Clinical Medicine, 12:2117, Mar 2023. URL: https://doi.org/10.3390/jcm12062117, doi:10.3390/jcm12062117. This article has 7 citations.
-
(blanco2023longtermresultsof pages 10-11): Juan F. Blanco, Francisco J. Garcia-Garcia, Eva M. Villarón, Carmen da Casa, Helena Fidalgo, Miriam López-Parra, José A. Santos, and Fermín Sánchez-Guijo. Long-term results of a phase i/ii clinical trial of autologous mesenchymal stem cell therapy for femoral head osteonecrosis. Journal of Clinical Medicine, 12:2117, Mar 2023. URL: https://doi.org/10.3390/jcm12062117, doi:10.3390/jcm12062117. This article has 7 citations.
-
(zhu2021comparisonofcell pages 11-12): Shibai Zhu, Xiaotian Zhang, Xi Chen, Yiou Wang, Shanni Li, and Wenwei Qian. Comparison of cell therapy and other novel adjunctive therapies combined with core decompression for the treatment of osteonecrosis of the femoral head. Bone & Joint Research, 10:445-458, Jul 2021. URL: https://doi.org/10.1302/2046-3758.107.bjr-2020-0418.r1, doi:10.1302/2046-3758.107.bjr-2020-0418.r1. This article has 35 citations.
-
(NCT04233125 chunk 2): Core Decompression With or Without Cement Packing for ONFH. University of Minnesota. 1997. ClinicalTrials.gov Identifier: NCT04233125
-
(shao2024inhibitionofsympathetic pages 3-4): Wenkai Shao, Bo Wang, Ping Wang, Shuo Zhang, Song Gong, Xiaodong Guo, Deyu Duan, Zengwu Shao, Weijian Liu, Lei He, Fei Gao, Xiao Lv, and Yong Feng. Inhibition of sympathetic tone via hypothalamic descending pathway propagates glucocorticoid-induced endothelial impairment and osteonecrosis of the femoral head. Bone Research, Nov 2024. URL: https://doi.org/10.1038/s41413-024-00371-3, doi:10.1038/s41413-024-00371-3. This article has 20 citations and is from a domain leading peer-reviewed journal.