Omphalocele
Omphalocele (exomphalos) is a congenital midline ventral abdominal wall defect at the base of the umbilical cord in which abdominal viscera herniate outside the abdomen, typically protected by a membranous sac composed of peritoneum, Wharton's jelly, and amnion. It arises from a developmental defect of ventral body wall formation, with persistence of the normal physiologic midgut herniation (which occurs at roughly 6-10 weeks' gestation and normally returns to the abdomen). Defects are commonly classified as small (no liver herniation) versus large/giant (liver herniation with viscero-abdominal disproportion). Omphalocele is etiologically heterogeneous: many cases are sporadic, but a substantial subset is associated with aneuploidy (trisomy 13, 18, 21), chromosomal rearrangements, and genetic syndromes (notably Beckwith-Wiedemann syndrome). Associated malformations - especially congenital heart defects - and chromosomal/syndromic diagnoses are the principal determinants of prognosis, rather than the abdominal wall defect alone.
Ask OpenScientist
Ask a research question about Omphalocele. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Mappings
Subtypes
5Pathophysiology
3Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Pathograph
Phenotypes
7Cardiovascular 3
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Digestive 1
Show evidence (1 reference)
Respiratory 2
Show evidence (1 reference)
Show evidence (1 reference)
Other 1
Show evidence (1 reference)
Genetic Associations
3Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Medical Actions
6Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Source YAML
click to showname: Omphalocele
creation_date: "2026-06-15T00:00:00Z"
description: >-
Omphalocele (exomphalos) is a congenital midline ventral abdominal wall defect
at the base of the umbilical cord in which abdominal viscera herniate outside
the abdomen, typically protected by a membranous sac composed of peritoneum,
Wharton's jelly, and amnion. It arises from a developmental defect of ventral
body wall formation, with persistence of the normal physiologic midgut
herniation (which occurs at roughly 6-10 weeks' gestation and normally returns
to the abdomen). Defects are commonly classified as small (no liver herniation)
versus large/giant (liver herniation with viscero-abdominal disproportion).
Omphalocele is etiologically heterogeneous: many cases are sporadic, but a
substantial subset is associated with aneuploidy (trisomy 13, 18, 21),
chromosomal rearrangements, and genetic syndromes (notably
Beckwith-Wiedemann syndrome). Associated malformations - especially congenital
heart defects - and chromosomal/syndromic diagnoses are the principal
determinants of prognosis, rather than the abdominal wall defect alone.
category: Congenital
disease_term:
preferred_term: Omphalocele
term:
id: MONDO:0019015
label: omphalocele
synonyms:
- Exomphalos
- Congenital omphalocele
- Exomphalos major
- Giant omphalocele
parents:
- Abdominal wall malformation
mappings:
mondo_mappings:
- term:
id: MONDO:0019015
label: omphalocele
mapping_predicate: skos:exactMatch
mapping_source: MONDO
mapping_justification: >-
MONDO:0019015 (omphalocele) is the disease term for this entry; it lists
Orphanet:660, NCIT:C98997, and ICD-10 Q79.2 cross-references.
has_subtypes:
- name: Isolated
display_name: Isolated (non-syndromic) omphalocele
description: >-
Omphalocele occurring without associated major malformations, chromosomal
abnormality, or recognized syndrome. Isolated cases have the most favorable
prognosis, with high survival in the absence of chromosomal defects.
- name: Syndromic
display_name: Syndromic / chromosomal omphalocele
description: >-
Omphalocele occurring as part of a recognized genetic syndrome or
chromosomal abnormality. Includes aneuploidies (trisomy 13, 18, 21) and
monogenic/imprinting syndromes. Carries substantially worse prognosis,
driven by the associated anomalies and chromosomal/syndromic diagnosis.
- name: BWS-associated
display_name: Beckwith-Wiedemann syndrome-associated omphalocele
description: >-
Omphalocele as a cardinal feature of Beckwith-Wiedemann syndrome, an
overgrowth/imprinting disorder of chromosome 11p15.5. Counseling and
follow-up differ because of the BWS tumor-predisposition and overgrowth
phenotype.
- name: Pentalogy of Cantrell
display_name: Pentalogy of Cantrell (thoraco-abdominal omphalocele)
description: >-
A rare midline defect complex combining a (supraumbilical) omphalocele with
defects of the lower sternum, anterior diaphragm, diaphragmatic pericardium,
and intracardiac anomalies. Reflects a defect of cephalic/anterior body-fold
closure.
- name: OEIS
display_name: OEIS complex (cloacal exstrophy)
description: >-
Omphalocele-Exstrophy of the cloaca-Imperforate anus-Spinal defects complex,
a caudal body-fold closure defect in which omphalocele co-occurs with
cloacal exstrophy, imperforate anus, and spinal/vertebral anomalies.
pathophysiology:
- name: Ventral Body Wall Closure Failure
description: >-
The primary developmental lesion in omphalocele is failure to complete
normal ventral body wall formation at the umbilical region. During normal
embryogenesis the lateral, cephalic, and caudal body folds migrate ventrally
and fuse at the umbilical ring; failure of this morphogenetic process leaves
a central defect through which abdominal viscera herniate into the base of
the umbilical cord, covered by a membranous (peritoneum/Wharton's
jelly/amnion) sac. This distinguishes omphalocele from gastroschisis (a
paraumbilical defect without a sac).
cell_types:
- preferred_term: Body wall mesenchymal cell
term:
id: CL:0000134
label: mesenchymal stem cell
- preferred_term: Body wall fibroblast
term:
id: CL:0000057
label: fibroblast
biological_processes:
- preferred_term: Embryonic body morphogenesis (ventral body wall closure)
term:
id: GO:0010172
label: embryonic body morphogenesis
modifier: ABNORMAL
- preferred_term: Mesenchymal cell migration (body-fold migration)
term:
id: GO:0090497
label: mesenchymal cell migration
modifier: DECREASED
- preferred_term: Umbilical cord morphogenesis
term:
id: GO:0036304
label: umbilical cord morphogenesis
modifier: ABNORMAL
evidence:
- reference: PMID:38021990
reference_title: "Enhancing Omphalocele Care: Navigating Complications and Innovative Treatment Approaches."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Omphalocele refers to the herniation of abdominal contents through a defect in the abdominal wall at the umbilicus with or without the presence of a sac."
explanation: >-
Review defining omphalocele as herniation of abdominal contents through a
ventral abdominal wall defect at the umbilicus, the anatomic consequence
of failed ventral body wall closure.
- reference: PMID:37726736
reference_title: "Ultrasonographic characteristics, genetic features, and maternal and fetal outcomes in fetuses with omphalocele in China: a single tertiary center study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Patients with omphalocele, a midline abdominal wall defect at the umbilical cord base, have a low survival rate."
explanation: >-
Confirms the midline umbilical-base location of the abdominal wall defect
that defines omphalocele.
downstream:
- target: Midgut Herniation and Viscero-Abdominal Disproportion
description: >-
Failure of ventral body wall closure leaves an open umbilical-ring defect
through which abdominal viscera herniate into the membrane-covered sac.
- name: Midgut Herniation and Viscero-Abdominal Disproportion
description: >-
Abdominal viscera - intestine and, in large/giant defects, the liver -
herniate through the body wall defect into the sac. In normal development a
physiologic midgut herniation occurs at ~6-10 weeks' gestation and returns
to the abdominal cavity; persistence/failure of this return contributes to
the pathologic herniation. The resulting reduction in intra-abdominal domain
produces viscero-abdominal disproportion, which both complicates surgical
reduction (risk of abdominal compartment syndrome) and, in giant defects,
constrains thoraco-abdominal development.
cell_types:
- preferred_term: Hepatocyte (herniated liver)
term:
id: CL:0000182
label: hepatocyte
biological_processes:
- preferred_term: Midgut development
term:
id: GO:0007494
label: midgut development
modifier: ABNORMAL
evidence:
- reference: PMID:38021990
reference_title: "Enhancing Omphalocele Care: Navigating Complications and Innovative Treatment Approaches."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "Omphalocele refers to the herniation of abdominal contents through a defect in the abdominal wall at the umbilicus with or without the presence of a sac."
explanation: >-
Supports herniation of abdominal contents (midgut, and in large defects
liver) through the umbilical defect; the abstract does not separately
quantify viscero-abdominal disproportion.
- reference: PMID:40150018
reference_title: "Omphalocele and Associated Anomalies: Exploring Pulmonary Development and Genetic Correlations-A Literature Review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "giant omphaloceles are frequently linked to lung hypoplasia, as reduced intra-abdominal space restricts fetal lung expansion"
explanation: >-
Supports that reduced intra-abdominal space (viscero-abdominal
disproportion) in giant omphalocele restricts fetal development.
downstream:
- target: Pulmonary Hypoplasia and Pulmonary Hypertension
description: >-
Viscero-abdominal disproportion in large/giant defects reduces the
intra-abdominal domain and constrains thoraco-abdominal development,
restricting fetal lung expansion and pulmonary vascular growth.
- name: Pulmonary Hypoplasia and Pulmonary Hypertension
description: >-
In large/giant omphalocele the reduced intra-abdominal domain and abnormal
thoraco-abdominal dynamics constrain fetal lung expansion, producing
pulmonary hypoplasia with impaired pulmonary vascular development. This
contributes to elevated pulmonary vascular resistance and pulmonary
hypertension, a major driver of neonatal respiratory morbidity and
mortality, and a key consideration when planning closure (avoiding
increases in intra-abdominal pressure that worsen ventilation).
cell_types:
- preferred_term: Pulmonary artery endothelial cell
term:
id: CL:1001568
label: pulmonary artery endothelial cell
- preferred_term: Pulmonary arterial smooth muscle cell
term:
id: CL:0002591
label: smooth muscle cell of the pulmonary artery
biological_processes:
- preferred_term: Lung development
term:
id: GO:0030324
label: lung development
modifier: DECREASED
- preferred_term: Pulmonary vasculature development
term:
id: GO:0001944
label: vasculature development
modifier: ABNORMAL
evidence:
- reference: PMID:40150018
reference_title: "Omphalocele and Associated Anomalies: Exploring Pulmonary Development and Genetic Correlations-A Literature Review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Among its most significant complications, pulmonary hypoplasia (PH) and pulmonary hypertension (PPH) have been shown to negatively impact neonatal prognosis. These conditions result from impaired pulmonary vascular development, leading to respiratory distress and hypoxemia."
explanation: >-
Directly supports pulmonary hypoplasia and pulmonary hypertension arising
from impaired pulmonary vascular development as major complications.
- reference: PMID:40150018
reference_title: "Omphalocele and Associated Anomalies: Exploring Pulmonary Development and Genetic Correlations-A Literature Review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "giant omphaloceles are frequently linked to lung hypoplasia, as reduced intra-abdominal space restricts fetal lung expansion, leading to structural lung abnormalities and increased pulmonary vascular resistance."
explanation: >-
Supports the mechanistic chain from reduced intra-abdominal space to lung
hypoplasia and increased pulmonary vascular resistance.
phenotypes:
- category: Physical
name: Omphalocele (ventral abdominal wall defect)
description: >-
Core defining phenotype: a midline abdominal wall defect at the umbilicus
with sac-covered herniation of abdominal viscera.
phenotype_term:
preferred_term: Omphalocele
term:
id: HP:0001539
label: Omphalocele
onset:
onset_category: CONGENITAL
evidence:
- reference: PMID:38021990
reference_title: "Enhancing Omphalocele Care: Navigating Complications and Innovative Treatment Approaches."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Omphalocele refers to the herniation of abdominal contents through a defect in the abdominal wall at the umbilicus with or without the presence of a sac."
explanation: Defines the core omphalocele phenotype.
- category: Physical
name: Congenital heart defects
description: >-
Cardiac anomalies are among the most frequent associated malformations in
omphalocele and are an important prognostic determinant. In one postnatal
cohort, cardiac anomalies were identified in 37.5% of omphalocele patients.
phenotype_term:
preferred_term: Abnormal heart morphology
term:
id: HP:0001627
label: Abnormal heart morphology
evidence:
- reference: PMID:37189937
reference_title: "Additional Anomalies in Children with Gastroschisis and Omphalocele: A Retrospective Cohort Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "in patients with omphalocele, cardiac anomalies were most identified (n = 15, 37.5%)"
explanation: >-
Supports congenital heart defects as the most common associated anomaly in
omphalocele, present in 37.5% of the cohort.
- category: Physical
name: Ventricular septal defect
description: >-
Ventricular septal defect was the single most common associated
malformation in the Swedish national omphalocele cohort.
phenotype_term:
preferred_term: Ventricular septal defect
term:
id: HP:0001629
label: Ventricular septal defect
evidence:
- reference: PMID:34392395
reference_title: "Omphalocele: national current birth prevalence and survival."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "About 62% of the cases had associated malformations and/or genetic disorders; most common was ventricular septal defect."
explanation: >-
Supports ventricular septal defect as the most common associated
malformation in a national cohort.
- category: Physical
name: Pulmonary hypoplasia
description: >-
Pulmonary hypoplasia is an important complication, especially in giant
omphalocele, and is linked to worse neonatal respiratory outcomes.
phenotype_term:
preferred_term: Pulmonary hypoplasia
term:
id: HP:0002089
label: Pulmonary hypoplasia
evidence:
- reference: PMID:40150018
reference_title: "Omphalocele and Associated Anomalies: Exploring Pulmonary Development and Genetic Correlations-A Literature Review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Among its most significant complications, pulmonary hypoplasia (PH) and pulmonary hypertension (PPH) have been shown to negatively impact neonatal prognosis."
explanation: Supports pulmonary hypoplasia as a significant complication.
- category: Physical
name: Pulmonary hypertension
description: >-
Pulmonary hypertension occurs in infants with giant omphalocele and
contributes to respiratory morbidity and mortality.
phenotype_term:
preferred_term: Pulmonary hypertension
term:
id: HP:0002092
label: Pulmonary arterial hypertension
evidence:
- reference: PMID:40150018
reference_title: "Omphalocele and Associated Anomalies: Exploring Pulmonary Development and Genetic Correlations-A Literature Review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Severe respiratory insufficiency, particularly due to pulmonary hypoplasia and pulmonary hypertension, significantly increases neonatal morbidity and mortality."
explanation: >-
Supports pulmonary hypertension as a contributor to neonatal morbidity and
mortality.
- category: Physical
name: Respiratory insufficiency
description: >-
Severe respiratory insufficiency is a major morbidity in giant omphalocele,
particularly with pulmonary hypoplasia/hypertension.
phenotype_term:
preferred_term: Respiratory insufficiency
term:
id: HP:0002093
label: Respiratory insufficiency
evidence:
- reference: PMID:40150018
reference_title: "Omphalocele and Associated Anomalies: Exploring Pulmonary Development and Genetic Correlations-A Literature Review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Severe respiratory insufficiency, particularly due to pulmonary hypoplasia and pulmonary hypertension, significantly increases neonatal morbidity and mortality."
explanation: Supports severe respiratory insufficiency as a major morbidity.
- category: Physical
name: Feeding difficulties
description: >-
Feeding difficulty is a recognized sequela, particularly in giant
omphalocele; management studies track time to full enteral feeds.
phenotype_term:
preferred_term: Feeding difficulties
term:
id: HP:0011968
label: Feeding difficulties
evidence:
- reference: PMID:38376641
reference_title: "A case series of successfully managing exomphalos major with awake graduated compression dressing and early enteral feeding."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The average time taken to reach full feeds was 1 week; only one patient required parenteral nutrition."
explanation: >-
A case series of exomphalos major tracks time to full feeds, reflecting
feeding difficulty as a clinically relevant sequela.
genetic:
- name: Chromosomal aneuploidy (trisomy 13, 18, 21)
inheritance:
- name: Chromosomal
features: >-
Omphalocele is frequently associated with chromosomal aneuploidy, most
commonly trisomy 13, trisomy 18, and trisomy 21. Across population cohorts,
the chromosomal-abnormality subgroup carries markedly elevated mortality;
in the Swedish national cohort about 62% of cases had associated
malformations and/or genetic disorders.
subtype: Syndromic
evidence:
- reference: PMID:34392395
reference_title: "Omphalocele: national current birth prevalence and survival."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "About 62% of the cases had associated malformations and/or genetic disorders; most common was ventricular septal defect."
explanation: >-
Supports the high proportion of omphalocele cases with associated genetic
disorders, including chromosomal abnormalities.
- name: Associated chromosomal abnormalities (population estimate)
inheritance:
- name: Chromosomal
features: >-
In a Finnish population-based study, chromosomal abnormalities were the most
common associated anomaly (9.3%), and 1-year survival was far lower for
neonates with chromosomal defects (17%) than for isolated cases (80%).
evidence:
- reference: PMID:32131131
reference_title: "Omphalocele in Finland from 1993 to 2014: Trends, Prevalence, Mortality, and Associated Malformations-A Population-Based Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "most commonly chromosomal abnormalities (9.3%), heart defects (6.3%), central nervous system anomalies (3.0%)"
explanation: >-
Supports chromosomal abnormalities as the most common associated anomaly
in a population-based omphalocele cohort.
- name: Monogenic variants in selected non-isolated cases
features: >-
When prenatal karyotype and chromosomal microarray are normal, whole exome
sequencing can identify monogenic variants in selected non-isolated cases. In
a Chinese prenatal cohort, WES of six karyotype/CMA-normal non-isolated cases
revealed one pathogenic and two suspected pathogenic variants.
subtype: Syndromic
evidence:
- reference: PMID:37726736
reference_title: "Ultrasonographic characteristics, genetic features, and maternal and fetal outcomes in fetuses with omphalocele in China: a single tertiary center study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Six nonisolated cases had normal CMA results and conventional karyotype tests, and further WES examination revealed one pathogenic variant and two suspected pathogenic variants."
explanation: >-
Supports a monogenic contribution detectable by WES in selected
non-isolated omphalocele cases with normal karyotype/CMA.
prevalence:
- population: Danish live births (1997-2021)
measure_type: BIRTH_PREVALENCE
prevalence_class: BAND_1_9_PER_100000
rate_per_100000: 9.8
percentage: "0.0098"
notes: >-
Danish nationwide live-birth register study: omphalocele birth prevalence of
0.98 per 10,000 infants (95% CI 0.83-1.15). Over half (53.7%) had one or more
major malformations and an additional 17.0% had a diagnosed syndrome.
evidence:
- reference: PMID:39576336
reference_title: "Omphalocele prevalence and co-occurring malformations: a nationwide register-based study of Danish live births in 1997-2021."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Among 1,498,685 live births, 147 infants with omphalocele were identified, yielding a combined and stable prevalence (per 10,000 infants) of 0.98 (95% CI 0.83-1.15). Over one-half (53.7%) presented with one or more major malformations, and an additional 17.0% were diagnosed with a syndrome."
explanation: >-
Provides nationwide live-birth prevalence and the proportion of cases with
co-occurring major malformations and syndromes.
- population: Finnish births (1993-2014, including terminations)
notes: >-
Finnish population-based register study including terminations: total
prevalence 4.71 per 10,000 births, birth prevalence 1.96 per 10,000, with
55% of pregnancies terminated.
evidence:
- reference: PMID:32131131
reference_title: "Omphalocele in Finland from 1993 to 2014: Trends, Prevalence, Mortality, and Associated Malformations-A Population-Based Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Birth prevalence in Finland was 1.96 per 10,000 births with no consistent trend over time. However, total prevalence was much higher (4.71/10,000) because more than half of these families chose option for the termination of pregnancy."
explanation: >-
Provides total and birth prevalence including terminations, and the high
termination rate.
progression:
- phase: Neonatal outcome (chromosome/anomaly dependent)
notes: >-
Omphalocele is congenital and frequently diagnosed prenatally by ultrasound.
Prognosis is driven primarily by associated anomalies and chromosomal/
syndromic diagnoses rather than the abdominal wall defect alone; in the
absence of chromosomal defects survival is reasonably good. In the Finnish
cohort, 1-year survival was 80% for isolated omphalocele versus 17% for
neonates with chromosomal defects.
evidence:
- reference: PMID:32131131
reference_title: "Omphalocele in Finland from 1993 to 2014: Trends, Prevalence, Mortality, and Associated Malformations-A Population-Based Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Total 1-year survival rates for isolated omphalocele, cases with multiple anomalies and neonates with chromosomal defects were 80, 88, and 17%, respectively."
explanation: >-
Quantifies the large survival difference between isolated and
chromosomally abnormal omphalocele.
- reference: PMID:32131131
reference_title: "Omphalocele in Finland from 1993 to 2014: Trends, Prevalence, Mortality, and Associated Malformations-A Population-Based Study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "In the absence of chromosomal defects, survival is reasonably good."
explanation: >-
Supports good survival when chromosomal defects are absent.
treatments:
- name: Primary surgical closure
description: >-
Definitive early operative reduction of herniated viscera and closure of the
abdominal wall defect. Best suited to small omphaloceles or cases without
major viscero-abdominal disproportion; urgent reduction can dangerously raise
intra-abdominal pressure and precipitate abdominal compartment syndrome.
treatment_term:
preferred_term: surgical procedure
term:
id: MAXO:0000004
label: surgical procedure
evidence:
- reference: PMID:40389219
reference_title: "European Paediatric Surgeons' Association Consensus Statement on the Management of Giant Omphalocele."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Giant omphalocele is appropriately defined as viscero-abdominal disproportion preventing primary closure."
explanation: >-
The EUPSA consensus defines giant omphalocele by viscero-abdominal
disproportion that precludes primary closure, indicating primary closure
is the approach for non-giant defects.
- name: Staged / traction-assisted closure
description: >-
Staged reduction (e.g., silo) or vertical traction-assisted staged closure
is used when primary closure is unsafe because of a large defect, liver
herniation, or marked viscero-abdominal disproportion. A prospective device
series achieved complete fascial closure in all 16 patients (10 giant
omphalocele, 6 gastroschisis) with no abdominal compartment syndrome.
treatment_term:
preferred_term: surgical procedure
term:
id: MAXO:0000004
label: surgical procedure
evidence:
- reference: PMID:38960901
reference_title: "Use of a new vertical traction device for early traction-assisted staged closure of congenital abdominal wall defects: a prospective series of 16 patients."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Complete fascial closure was achieved after a median time of 7 days (range 4-22) in GOC and 5 days (range 4-11) in GS."
explanation: >-
Supports traction-assisted staged closure achieving complete fascial
closure in giant omphalocele and gastroschisis.
- name: Conservative "paint and wait" management
description: >-
Non-operative topical epithelialization of the intact sac, recommended when
anatomical constraints or high surgical risk preclude primary closure
(especially giant omphalocele with liver exteriorization and/or pulmonary
hypoplasia/hypertension). Common painting agents include povidone-iodine and
silver sulfadiazine. Later definitive ventral hernia repair is often needed.
treatment_term:
preferred_term: topical pharmacotherapy
term:
id: MAXO:0001573
label: topical pharmacotherapy
evidence:
- reference: PMID:40389219
reference_title: "European Paediatric Surgeons' Association Consensus Statement on the Management of Giant Omphalocele."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "the \"paint and wait\" approach is recommended when anatomical constraints or high surgical risk preclude primary closure. Common painting agents include povidone-iodine and silver sulfadiazine"
explanation: >-
EUPSA consensus recommends paint-and-wait conservative topical management
when primary closure is precluded.
- name: Awake graduated compression dressing
description: >-
A bedside, awake gradual compression dressing technique for exomphalos major
that reduces sac contents without general anaesthetic or respiratory
compromise and permits simultaneous early enteral feeding.
treatment_term:
preferred_term: supportive care
term:
id: MAXO:0000950
label: supportive care
evidence:
- reference: PMID:38376641
reference_title: "A case series of successfully managing exomphalos major with awake graduated compression dressing and early enteral feeding."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "This case series describes a successful compression dressing technique that reduces sac content without the need for general anaesthetic or respiratory compromise, whereby simultaneous enteral feeding is tolerated."
explanation: >-
Supports awake graduated compression dressing as a conservative bedside
reduction strategy for exomphalos major.
- name: Prenatal diagnosis and genetic testing
description: >-
Prenatal ultrasound is the principal diagnostic modality and supports
classification into isolated versus non-isolated omphalocele, guiding genetic
testing (karyotype + chromosomal microarray, with WES escalation) and
counseling.
treatment_term:
preferred_term: prenatal examination
term:
id: MAXO:0000528
label: prenatal examination
evidence:
- reference: PMID:37726736
reference_title: "Ultrasonographic characteristics, genetic features, and maternal and fetal outcomes in fetuses with omphalocele in China: a single tertiary center study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Routine karyotyping with CMA testing should be provided for fetuses with omphalocele. WES is an option if karyotype and CMA tests are normal."
explanation: >-
Supports prenatal genetic testing workflow (karyotype + CMA, then WES) for
prenatally diagnosed omphalocele.
- name: Genetic counseling
description: >-
Genetic counseling addresses the high rate of associated chromosomal
abnormalities and syndromes (including Beckwith-Wiedemann syndrome) and their
prognostic and recurrence implications.
treatment_term:
preferred_term: Genetic Counseling
term:
id: NCIT:C15240
label: Genetic Counseling
evidence:
- reference: PMID:39576336
reference_title: "Omphalocele prevalence and co-occurring malformations: a nationwide register-based study of Danish live births in 1997-2021."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Over one-half (53.7%) presented with one or more major malformations, and an additional 17.0% were diagnosed with a syndrome."
explanation: >-
The high burden of co-occurring malformations and syndromes supports the
role of genetic counseling.
references:
- reference: PMID:32131131
title: "Omphalocele in Finland from 1993 to 2014: Trends, Prevalence, Mortality, and Associated Malformations-A Population-Based Study."
- reference: PMID:34392395
title: "Omphalocele: national current birth prevalence and survival."
- reference: PMID:37189937
title: "Additional Anomalies in Children with Gastroschisis and Omphalocele: A Retrospective Cohort Study."
- reference: PMID:37726736
title: "Ultrasonographic characteristics, genetic features, and maternal and fetal outcomes in fetuses with omphalocele in China: a single tertiary center study."
- reference: PMID:38021990
title: "Enhancing Omphalocele Care: Navigating Complications and Innovative Treatment Approaches."
- reference: PMID:38376641
title: "A case series of successfully managing exomphalos major with awake graduated compression dressing and early enteral feeding."
- reference: PMID:38960901
title: "Use of a new vertical traction device for early traction-assisted staged closure of congenital abdominal wall defects: a prospective series of 16 patients."
- reference: PMID:39576336
title: "Omphalocele prevalence and co-occurring malformations: a nationwide register-based study of Danish live births in 1997-2021."
- reference: PMID:40150018
title: "Omphalocele and Associated Anomalies: Exploring Pulmonary Development and Genetic Correlations-A Literature Review."
- reference: PMID:40389219
title: "European Paediatric Surgeons' Association Consensus Statement on the Management of Giant Omphalocele."
References & Deep Research
References
10Deep Research
11. Disease Information
1.1 What is omphalocele? (current definition)
Omphalocele is a congenital midline abdominal wall defect at the umbilicus/base of the umbilical cord in which abdominal viscera herniate outside the abdomen, typically covered by a membranous sac (often described as peritoneum/Wharton’s jelly/amnion layers). (malhotra2023enhancingomphalocelecare pages 1-3)
A population-based Danish register study similarly describes omphalocele (exomphalos) as herniation of abdominal contents through the umbilical insertion, often categorized clinically as small (no liver herniation) vs large (liver herniation). (laustenthomsen2024omphaloceleprevalenceand pages 1-2)
1.2 Synonyms and alternative names
- Exomphalos (common synonym in European literature and coding) (fogelstrom2021omphalocelenationalcurrent pages 1-2, fogelstrom2021omphalocelenationalcurrent pages 2-4)
- Giant omphalocele / exomphalos major (large defects with viscero-abdominal disproportion and/or liver herniation; definitions vary across studies) (malhotra2023enhancingomphalocelecare pages 3-5, pijpers2023additionalanomaliesin pages 2-4)
1.3 Evidence sources (aggregated vs individual)
The information summarized here is derived from: - Aggregated, disease-level resources: nationwide population-based registry cohorts (Denmark, Sweden, Finland) (laustenthomsen2024omphaloceleprevalenceand pages 1-2, fogelstrom2021omphalocelenationalcurrent pages 1-2, raitio2021omphaloceleinfinland pages 5-9) - Aggregated cohort studies: tertiary-center prenatal cohort (China) (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 4-6) - Clinical case series/implementation studies: staged closure traction device; compression-dressing management (ziegler2024useofa pages 5-7, widatella2024acaseseries pages 1-3)
2. Etiology
2.1 Primary causes (current understanding)
Omphalocele is generally regarded as a developmental/embryologic defect of ventral body wall formation; its etiology is often multifactorial, with a prominent contribution from genetic and chromosomal abnormalities and syndromic conditions. (malhotra2023enhancingomphalocelecare pages 1-3, laustenthomsen2024omphaloceleprevalenceand pages 1-2)
Direct abstract-supported definition-related embryology in the 2023 review notes that physiologic midgut herniation occurs at ~6–10 weeks’ gestation, and persistence/failure of normal return is part of the conceptual embryologic framework used clinically when distinguishing normal from pathologic herniation. (malhotra2023enhancingomphalocelecare pages 3-5)
2.2 Risk factors
Maternal and demographic associations are reported in review-level sources (with heterogeneous evidence quality). A 2023 narrative review lists potential risk factors including advanced maternal age, and exposures such as smoking, alcohol, aspirin, SSRIs, and certain nutritional factors (e.g., high-dose vitamin E; abnormal vitamin B12 production). These should be interpreted cautiously as they are not uniformly supported across high-quality population-based causal studies. (malhotra2023enhancingomphalocelecare pages 3-5)
For giant omphalocele, prognostic/risk correlates for adverse outcomes include chromosomal anomalies, congenital heart defects, CNS defects, lung hypoplasia, defect size, and birth weight, as summarized in the European Paediatric Surgeons’ Association (EUPSA) consensus statement synthesis. (saxena2025europeanpaediatricsurgeons pages 7-8)
2.3 Protective factors
No protective factors with strong direct evidence were identified in the retrieved corpus.
2.4 Gene–environment interactions
No specific, well-validated gene–environment interaction mechanisms were identified in the retrieved corpus.
3. Phenotypes (clinical manifestations)
3.1 Core phenotype
- Congenital abdominal wall defect at umbilicus with sac-covered herniation (HP:0001539 Omphalocele) (malhotra2023enhancingomphalocelecare pages 1-3)
3.2 Common associated phenotypes/conditions (with data)
Omphalocele is frequently non-isolated and associated with other malformations/syndromes: - In Denmark (live births 1997–2021), 53.7% had ≥1 major malformation and 17.0% had a syndrome diagnosis. (laustenthomsen2024omphaloceleprevalenceand pages 1-2) - In Sweden (1997–2016), 62% of live-born cases had associated malformations and/or genetic disorders; ventricular septal defect was the most common associated malformation. (fogelstrom2021omphalocelenationalcurrent pages 1-2, fogelstrom2021omphalocelenationalcurrent pages 2-4)
A detailed prenatal cohort from China (120 fetuses) reported high rates of associated abnormalities in non-isolated cases, with ultrasound categories including cardiovascular, skeletal, CNS, and facial anomalies; the most common ultrasound category in the cohort table was cardiovascular findings. (que2023ultrasonographiccharacteristicsgenetic pages 4-6)
3.3 Pulmonary complications (important for giant omphalocele)
A literature review emphasizes pulmonary hypoplasia and pulmonary hypertension as key complications that worsen neonatal prognosis, particularly in giant omphalocele where reduced intra-abdominal capacity may restrict fetal lung expansion. (namat2025omphaloceleandassociated pages 11-13)
3.4 HPO term suggestions
A phenotype-to-HPO mapping table is provided for knowledge-base ingestion.
| Clinical feature / phenotype | Phenotype type | Suggested HPO term(s) | Notes / frequency or context | Evidence source |
|---|---|---|---|---|
| Midline abdominal wall defect at umbilicus covered by sac (omphalocele/exomphalos) | Congenital structural anomaly | HP:0001539 Omphalocele | Core defining phenotype: herniation of abdominal contents through the umbilical insertion, typically sac-covered | (malhotra2023enhancingomphalocelecare pages 1-3, laustenthomsen2024omphaloceleprevalenceand pages 1-2) |
| Herniation of liver into sac | Congenital structural anomaly | HP:0012368 Herniation of the liver | Used clinically to distinguish larger/giant lesions; large lesions commonly involve liver herniation | (laustenthomsen2024omphaloceleprevalenceand pages 1-2, pijpers2023additionalanomaliesin pages 2-4) |
| Herniation of bowel/intestine into sac | Congenital structural anomaly | HP:0002240 Intestinal malrotation; HP:0033127 Abnormality of the intestine morphology | Bowel is commonly among herniated viscera; exact HPO for “bowel in sac” is not standard, so broader intestinal morphology terms may be needed in addition to HP:0001539 | (malhotra2023enhancingomphalocelecare pages 1-3, widatella2024acaseseries pages 1-3) |
| Pulmonary hypoplasia | Respiratory structural anomaly | HP:0002089 Pulmonary hypoplasia | Important complication, especially in giant omphalocele; linked to worse neonatal respiratory outcomes and mortality | (namat2025omphaloceleandassociated pages 11-13, malhotra2023enhancingomphalocelecare pages 3-5) |
| Pulmonary hypertension | Cardiopulmonary complication | HP:0002092 Pulmonary hypertension | Reported in infants with giant omphalocele and associated with respiratory morbidity | (namat2025omphaloceleandassociated pages 11-13, malhotra2023enhancingomphalocelecare pages 3-5) |
| Congenital heart defects (overall) | Congenital structural anomaly | HP:0001627 Abnormal heart morphology | Cardiac anomalies are among the most frequent associated anomalies in omphalocele; 37.5% in one postnatal cohort of omphalocele patients | (pijpers2023additionalanomaliesin pages 2-4, que2023ultrasonographiccharacteristicsgenetic pages 1-2) |
| Ventricular septal defect | Congenital structural anomaly | HP:0001629 Ventricular septal defect | Most common associated malformation in Swedish national cohort | (fogelstrom2021omphalocelenationalcurrent pages 1-2, fogelstrom2021omphalocelenationalcurrent pages 2-4) |
| Atrial septal defect | Congenital structural anomaly | HP:0001631 Atrial septal defect | Common associated cardiac lesion, reported after VSD in Swedish cohort | (fogelstrom2021omphalocelenationalcurrent pages 2-4) |
| Skeletal anomalies | Congenital structural anomaly | HP:0000924 Abnormality of the skeletal system | Prenatal cohort reported skeletal anomalies in 31.2% (38/120) of fetuses with omphalocele | (que2023ultrasonographiccharacteristicsgenetic pages 4-6, que2023ultrasonographiccharacteristicsgenetic pages 2-4) |
| Central nervous system anomalies | Congenital structural anomaly | HP:0000707 Abnormality of the nervous system | Prenatal cohort reported CNS malformations in 22.5% (27/120) | (que2023ultrasonographiccharacteristicsgenetic pages 4-6, que2023ultrasonographiccharacteristicsgenetic pages 2-4) |
| Feeding difficulties / delayed achievement of feeds | Functional / gastrointestinal phenotype | HP:0011968 Feeding difficulties in infancy | Feeding difficulty is a recognized sequela in giant omphalocele; management studies track time to full feeds | (saxena2025europeanpaediatricsurgeons pages 8-9, widatella2024acaseseries pages 1-3) |
| Respiratory insufficiency / respiratory distress | Clinical sign | HP:0002093 Respiratory insufficiency; HP:0002098 Respiratory distress | Severe respiratory insufficiency is a major morbidity in giant omphalocele, especially with pulmonary hypoplasia/hypertension | (namat2025omphaloceleandassociated pages 11-13, saxena2025europeanpaediatricsurgeons pages 8-9) |
| Gastroesophageal reflux disease (GERD) | Gastrointestinal symptom/disorder | HP:0002020 Gastroesophageal reflux | Reported as a later morbidity in giant omphalocele survivors | (malhotra2023enhancingomphalocelecare pages 3-5) |
| Neurodevelopmental delay | Neurodevelopmental phenotype | HP:0012758 Neurodevelopmental delay | Long-term neurodevelopmental issues are recognized in giant omphalocele survivors and in children with major associated anomalies | (saxena2025europeanpaediatricsurgeons pages 8-9, que2023ultrasonographiccharacteristicsgenetic pages 2-4) |
| Autism spectrum disorder | Behavioral / neurodevelopmental phenotype | HP:0000729 Autism | Evidence mainly from giant omphalocele survivor cohorts rather than all omphalocele cases | (saxena2025europeanpaediatricsurgeons pages 8-9) |
Table: This table maps major clinical features of omphalocele to suggested HPO terms and summarizes the supporting evidence. It is useful for populating phenotype annotations in a disease knowledge base, especially for distinguishing core defects from common associated cardiopulmonary and neurodevelopmental complications.
4. Genetic/Molecular Information
4.1 Chromosomal abnormalities and syndromic associations
Population cohorts show frequent co-occurrence with chromosomal diagnoses: - Sweden: trisomy 13 (n=8), trisomy 18 (n=4), trisomy 21 (n=4) among 207 liveborn cases (with markedly elevated mortality in the chromosomal-abnormality subgroup). (fogelstrom2021omphalocelenationalcurrent pages 2-4, fogelstrom2021omphalocelenationalcurrent pages 4-5) - China prenatal cohort (tested subset): trisomy 18 (3), trisomy 13 (1), and a chromosome 8–11 translocation (1) among those undergoing karyotype+CMA. (que2023ultrasonographiccharacteristicsgenetic pages 1-2)
4.2 Recommended prenatal genetic testing workflow
A stepwise strategy supported by cohort data and review synthesis is: 1) Karyotype + chromosomal microarray (CMA) as first-line testing in prenatal omphalocele. (que2023ultrasonographiccharacteristicsgenetic pages 1-2, namat2025omphaloceleandassociated pages 11-13) 2) WES if karyotype and CMA are normal, especially in non-isolated cases; the Chinese cohort found abnormal WES results in 3/6 selected cases with normal karyotype/CMA, including variants in COL2A1 and SCP2, and an SDHB finding (details in source). (que2023ultrasonographiccharacteristicsgenetic pages 4-6)
The prenatal genetic testing summary table is provided below.
| Test modality | When to use in prenatal omphalocele | Diagnostic yield / typical findings | Example abnormalities detected or targeted | Supporting sources |
|---|---|---|---|---|
| Conventional karyotype | Recommended routinely once fetal omphalocele is diagnosed prenatally, especially for non-isolated cases or when additional ultrasound abnormalities are present | Detects aneuploidy and large structural chromosome abnormalities; in one 2023 cohort, 35 patients underwent karyotype+CMA and 5/35 (14.3%) had chromosomal abnormalities; all abnormal karyotypes were in non-isolated cases | Trisomy 18 (3 cases), trisomy 13 (1 case), trisomy 21 is a recognized recurrent association, chromosome 8;11 translocation (1 case) (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 4-6, fogelstrom2021omphalocelenationalcurrent pages 2-4) | (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 4-6, fogelstrom2021omphalocelenationalcurrent pages 2-4) |
| Chromosomal microarray (CMA) | Recommended together with karyotype as first-line prenatal genetic testing for omphalocele; useful when ultrasound suggests associated anomalies and for clarifying submicroscopic CNVs | Adds genome-wide CNV detection beyond karyotype; in the Que et al. cohort, CMA was performed with karyotype in 35 cases and was normal in 6 selected non-isolated cases later escalated to WES; parental blood/pedigree analysis is recommended when CMA yields VUS | Can detect pathogenic/likely pathogenic CNVs not visible on karyotype; examples in the cohort were mainly normal CMA followed by WES escalation rather than specific recurrent CNVs reported in the excerpt (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 2-4, que2023ultrasonographiccharacteristicsgenetic pages 8-9) | (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 2-4, que2023ultrasonographiccharacteristicsgenetic pages 8-9) |
| QF-PCR | Rapid adjunct test when rapid confirmation of common aneuploidies is needed, particularly if trisomy is strongly suspected on ultrasound | Fast targeted confirmation rather than genome-wide discovery; highlighted as useful for rapid confirmation of trisomy 13 in review evidence | Trisomy 13, and by standard panel use also common autosomal trisomies such as T18/T21 when suspected (namat2025omphaloceleandassociated pages 11-13) | (namat2025omphaloceleandassociated pages 11-13) |
| Whole exome sequencing (WES) | Consider when karyotype and CMA are normal, especially in non-isolated omphalocele or persistent suspicion of syndromic/genetic disease | In Que et al., 6 non-isolated cases with normal karyotype/CMA underwent WES and 3/6 had abnormal findings (1 pathogenic, 2 suspected pathogenic); review evidence notes WES may increase diagnostic yield by ~8–10% after normal karyotype/CMA | COL2A1 c.2759C>A (p.Pro920His), SCP2 c.674+1G>C, SDHB c.725G>A (p.R242H); review also notes WES is an option after normal karyotype/CMA and may improve yield (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 4-6, que2023ultrasonographiccharacteristicsgenetic pages 2-4, que2023ultrasonographiccharacteristicsgenetic pages 8-9, namat2025omphaloceleandassociated pages 11-13) | (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 4-6, que2023ultrasonographiccharacteristicsgenetic pages 2-4, que2023ultrasonographiccharacteristicsgenetic pages 8-9, namat2025omphaloceleandassociated pages 11-13) |
| Stepwise prenatal testing strategy | Practical recommendation for current care pathways in prenatally diagnosed omphalocele | Start with karyotype + CMA because aneuploidy risk is elevated; escalate to WES if first-line testing is normal; if all are normal but phenotype remains suggestive, additional syndrome-specific testing may be needed | Common prenatal genetic associations include T13, T18, T21; structural rearrangements such as t(8;11); monogenic findings by WES may include COL2A1, SCP2, SDHB; if karyotype/CMA/WES are normal, additional testing may be required to evaluate disorders such as Beckwith-Wiedemann syndrome (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 8-9, namat2025omphaloceleandassociated pages 11-13) | (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 8-9, namat2025omphaloceleandassociated pages 11-13) |
Table: This table summarizes the main prenatal genetic testing modalities used for omphalocele, when each is recommended, and the kinds of abnormalities they can detect. It is useful for structuring a diagnostic workflow from aneuploidy testing through exome sequencing in isolated and non-isolated cases.
4.3 Mechanistic / pathway detail
The retrieved evidence primarily supports a developmental malformation framework with strong genetic/chromosomal contributions rather than a single molecular pathway model. Molecular pathway enrichment, epigenetic signatures, or omics profiling specific to omphalocele were not identified in the retrieved corpus.
5. Environmental Information
No specific infectious etiologies were identified. Environmental/lifestyle associations are discussed in review-level sources but without strong causal confirmation from the evidence retrieved here. (malhotra2023enhancingomphalocelecare pages 3-5)
6. Mechanism / Pathophysiology
6.1 Causal chain (high-level)
Primary developmental defect → failure to achieve normal abdominal domain/closure at umbilicus → herniation of viscera (often including liver in large/giant cases) → viscero-abdominal disproportion → perinatal cardiopulmonary vulnerability; repair decisions must avoid dangerous rises in intra-abdominal pressure that can precipitate abdominal compartment syndrome and multi-organ physiologic compromise. (namat2025omphaloceleandassociated pages 11-13)
6.2 Pulmonary hypoplasia and pulmonary hypertension
Pulmonary hypoplasia and pulmonary hypertension are emphasized as major contributors to neonatal morbidity/mortality in large/giant omphalocele, likely related to constrained fetal thoracoabdominal dynamics and pulmonary vascular development. (namat2025omphaloceleandassociated pages 11-13)
Suggested GO biological process terms (GO): - GO:0001944 vasculature development (re pulmonary vascular development) - GO:0030324 lung development - GO:0003015 heart process (hemodynamic consequences)
Suggested cell types (CL): - CL:0002062 pulmonary artery endothelial cell - CL:0002543 lung microvascular endothelial cell
(These ontology suggestions are based on mechanistic interpretation of the cited review’s pulmonary-development framing; direct single-cell evidence was not retrieved.) (namat2025omphaloceleandassociated pages 11-13)
7. Anatomical Structures Affected
7.1 Primary anatomy
- Anterior abdominal wall / umbilical region (primary defect site) (malhotra2023enhancingomphalocelecare pages 1-3, laustenthomsen2024omphaloceleprevalenceand pages 1-2)
- Herniated organs frequently include liver and bowel in larger defects (pijpers2023additionalanomaliesin pages 2-4, widatella2024acaseseries pages 1-3)
7.2 Systems commonly involved via associated anomalies
- Cardiovascular system (common co-occurring CHD such as VSD/ASD) (fogelstrom2021omphalocelenationalcurrent pages 1-2, fogelstrom2021omphalocelenationalcurrent pages 2-4)
- Central nervous system, skeletal system (notable frequencies in prenatal cohort) (que2023ultrasonographiccharacteristicsgenetic pages 4-6)
UBERON suggestions (non-exhaustive): - UBERON:0000945 stomach (if herniated) - UBERON:0002107 liver - UBERON:0000160 intestine - UBERON:0002398 abdominal wall
8. Temporal Development
8.1 Onset
- Congenital; frequently diagnosed prenatally by ultrasound. (malhotra2023enhancingomphalocelecare pages 1-3, que2023ultrasonographiccharacteristicsgenetic pages 1-2)
8.2 Course/progression
Immediate neonatal course depends strongly on: - Isolated vs non-isolated status (que2023ultrasonographiccharacteristicsgenetic pages 1-2) - Cardiopulmonary status (pulmonary hypoplasia/hypertension; CHD) (namat2025omphaloceleandassociated pages 11-13, saxena2025europeanpaediatricsurgeons pages 7-8)
9. Inheritance and Population
9.1 Epidemiology (recent population-based statistics)
Population-based estimates vary by ascertainment (live births only vs total including terminations). Key recent benchmarks include: - Denmark live births (1997–2021): 0.98 per 10,000 live births. (laustenthomsen2024omphaloceleprevalenceand pages 1-2) - Sweden live births (1997–2016): 1 per 10,000 live births; prenatal diagnosis frequently leads to termination. (fogelstrom2021omphalocelenationalcurrent pages 1-2, fogelstrom2021omphalocelenationalcurrent pages 2-4) - Finland total prevalence including terminations (1993–2014): 4.71 per 10,000 births, with birth prevalence 1.96/10,000 and live-birth prevalence 1.69/10,000; 55% terminations. (raitio2021omphaloceleinfinland pages 5-9)
A cross-study epidemiology and outcomes comparison table is embedded below.
| Study (country) | Years | Design | n (cases) | Prevalence (per 10,000 live births or total) | Termination rate | Associated anomalies % | Key anomalies | 1-year mortality/survival |
|---|---|---|---|---|---|---|---|---|
| Lausten-Thomsen 2024 (Denmark) | 1997–2021 | Nationwide register-based live-birth cohort | 147 liveborn infants with omphalocele among 1,498,685 live births | 0.98 per 10,000 live births (95% CI 0.83–1.15) | Not directly estimated in cohort; authors note European prenatal termination rates often exceed 50% | 53.7% had ≥1 major malformation; additional 17.0% had a diagnosed syndrome | Broad co-occurring defects affecting cardiac, renal, limb, and CNS systems; syndromic/chromosomal conditions noted | Not reported in extracted context (laustenthomsen2024omphaloceleprevalenceand pages 1-2) |
| Fogelström 2021 (Sweden) | 1997–2016 | Nationwide population-based cohort | 207 live-born cases; 449 prenatally diagnosed pregnancies | 1.0 per 10,000 live births | 59% of prenatally diagnosed pregnancies (263/449) | 62% had associated malformations and/or genetic disorders | Ventricular septal defect most common; ASD also frequent; trisomy 13 (n=8), trisomy 18 (n=4), trisomy 21 (n=4) reported | 13% mortality within 1 year; ~87% 1-year survival (fogelstrom2021omphalocelenationalcurrent pages 1-2, fogelstrom2021omphalocelenationalcurrent pages 2-4, fogelstrom2021omphalocelenationalcurrent pages 4-5) |
| Raitio 2021 (Finland) | 1993–2014 | Nationwide population-based register study | 600 total cases: 229 live births, 39 stillbirths, 332 terminations | Total prevalence 4.71 per 10,000 births; birth prevalence 1.96 per 10,000; live-birth prevalence 1.69 per 10,000 | 55% (332/600) | Among liveborns, 18% had multiple anomalies; chromosomal abnormalities 9.3% overall; isolated cases 77% of liveborns | Chromosomal abnormalities 9.3%; heart defects 6.3%; CNS anomalies 3.0%; GI and urogenital malformations 2.0% each; Beckwith-Wiedemann noted among syndromes | Overall infant mortality 22%; 1-year survival 80% isolated, 88% multiple anomalies, 17% chromosomal defects (raitio2021omphaloceleinfinland pages 5-9, raitioUnknownyearomphaloceleinfinland pages 1-5) |
| Que 2023 (China) | 2015–2022 | Single tertiary-center prenatal cohort | 120 fetuses with prenatal omphalocele; 112 followed | Not a population prevalence study | 71.4% of followed pregnancies (80/112) requested termination | 77.5% non-isolated (93/120); 22.5% isolated (27/120) | Cardiac anomalies common (17 fetuses); broader ultrasound findings included cardiovascular, skeletal, CNS, facial anomalies; chromosomal findings: trisomy 18 (n=3), trisomy 13 (n=1), translocation 8–11 (n=1); WES identified pathogenic/suspected pathogenic variants including COL2A1, SCP2, SDHB | Among 25 live births, 72% survived to 1 year (7/25 died in first year) (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 4-6, que2023ultrasonographiccharacteristicsgenetic pages 2-4) |
Table: This table summarizes recent and foundational cohort data on omphalocele prevalence, associated anomalies, termination rates, and 1-year outcomes across Denmark, Sweden, Finland, and a large prenatal cohort from China. It is useful for quickly comparing population-based burden and prognosis across settings.
9.2 Inheritance patterns
Omphalocele is best conceptualized as heterogeneous: - Many cases are sporadic, - A substantial subset relates to aneuploidy/chromosomal abnormalities and syndromic disorders, - Some non-isolated cases may be attributable to monogenic variants detected by WES in selected contexts. (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 4-6)
10. Diagnostics
10.1 Prenatal diagnosis
Prenatal ultrasound is a principal diagnostic modality; in the China cohort, prenatal ultrasound diagnosis supported classification into isolated vs non-isolated omphalocele and guided subsequent genetic testing and counseling. (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 4-6)
10.2 Postnatal evaluation for associated anomalies
Because associated anomalies are frequent and prognostically important, registry and cohort evidence supports comprehensive evaluation. For example, a postnatal cohort emphasized routine screening for additional anomalies; a center implemented routine cardiac ultrasound screening since 2018 in children with omphalocele. (pijpers2023additionalanomaliesin pages 2-4)
10.3 Genetic testing
Evidence supports routine karyotype + CMA and escalation to WES if first-line tests are normal, particularly in non-isolated cases. (que2023ultrasonographiccharacteristicsgenetic pages 1-2, namat2025omphaloceleandassociated pages 11-13)
11. Outcome / Prognosis
11.1 Key prognostic determinants
Across multiple sources, prognosis is driven primarily by associated anomalies and chromosomal/syndromic diagnoses, rather than the abdominal wall defect alone. (malhotra2023enhancingomphalocelecare pages 6-7, laustenthomsen2024omphaloceleprevalenceand pages 1-2)
11.2 Survival statistics
- Sweden (liveborn cohort): 13% mortality within 1 year; mortality in the chromosomal-abnormality subgroup was high (65%). (fogelstrom2021omphalocelenationalcurrent pages 2-4, fogelstrom2021omphalocelenationalcurrent pages 4-5)
- Finland (register including terminations): overall infant mortality 22%; 1-year survival 80% in isolated cases vs 17% in chromosomal defects. (raitio2021omphaloceleinfinland pages 5-9)
- China prenatal cohort: among 25 live births, 72% survived to 1 year (18/25). (que2023ultrasonographiccharacteristicsgenetic pages 1-2, que2023ultrasonographiccharacteristicsgenetic pages 4-6)
11.3 Morbidity and quality of life
Long-term morbidity includes cardiopulmonary complications, feeding problems, and neurodevelopmental sequelae particularly in giant omphalocele survivors, as synthesized in consensus/review sources. (saxena2025europeanpaediatricsurgeons pages 8-9, namat2025omphaloceleandassociated pages 11-13)
12. Treatment
12.1 Management goals
A major surgical principle is to achieve safe reduction/closure while avoiding pathologic increases in intra-abdominal pressure (abdominal compartment syndrome physiology). (namat2025omphaloceleandassociated pages 11-13)
12.2 Current applications and real-world implementations (2023–2024)
Recent clinical implementation studies highlight non-traditional strategies alongside standard primary/staged closure:
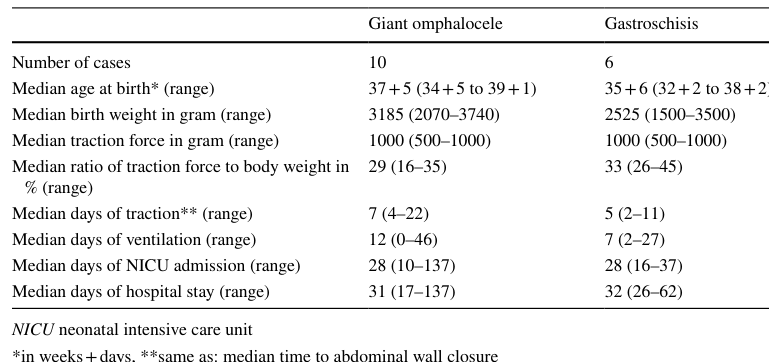
A) Traction-assisted staged closure (fasciotens®Pediatric) A multicenter prospective series (2022–2023 recruitment period) achieved complete fascial closure in 16/16 patients (10 giant omphalocele, 6 gastroschisis), with median closure times of 7 days (giant omphalocele) and 5 days (gastroschisis), and reported no SSI or abdominal compartment syndrome; no hernias were observed at median 12-month follow-up. (ziegler2024useofa pages 1-2, ziegler2024useofa pages 5-7)
A table image summarizing outcomes is available from the paper (Table 3). (ziegler2024useofa media f0a1df53)
B) Awake graduated compression dressings for exomphalos major A 2024 case series (n=4) started bedside compression dressings on days 1–3 of life, achieved full feeds in ~1 week on average, limited parenteral nutrition, and enabled delayed repairs without patch and without prolonged ventilation. (widatella2024acaseseries pages 1-3)
12.3 Treatment strategy summary (with MAXO suggestions)
A treatment table (knowledge-base ready) is embedded below.
| Strategy | Suggested MAXO term(s) | Indication / selection factors | Key outcomes / complications | Real-world implementation notes | Sources |
|---|---|---|---|---|---|
| Immediate primary closure | MAXO: surgical repair; primary closure of abdominal wall defect | Best suited to small omphaloceles or cases without major viscero-abdominal disproportion and without prohibitive cardiopulmonary risk; goal is definitive early closure while avoiding dangerous rise in intra-abdominal pressure | Preferred when feasible, but urgent reduction can precipitate abdominal compartment syndrome with reduced cardiac output, splanchnic hypoperfusion, lactic acidosis, renal failure, intestinal ischemia, and hypoventilation; prognosis strongly influenced by associated anomalies rather than closure alone | Standard neonatal surgical approach in many centers for smaller defects; in the Amsterdam cohort, primary closure was performed in 33/40 (82.5%) omphalocele patients overall, though this cohort included both minor and giant cases (malhotra2023enhancingomphalocelecare pages 6-7, pijpers2023additionalanomaliesin pages 2-4) | (malhotra2023enhancingomphalocelecare pages 6-7, pijpers2023additionalanomaliesin pages 2-4) |
| Staged reduction with silo / delayed primary closure | MAXO: staged surgical closure; silo placement; delayed primary closure | Used when primary closure is unsafe because of large defect, liver herniation, or marked viscero-abdominal disproportion; also used to reduce risk of cardiorespiratory compromise | EUPSA summary of giant omphalocele literature reported early closure strategies used patches more often (44% vs 17% for delayed), with mortality 8% for early closure overall versus delayed subgroups: simple 18%, composite 0%, patch 63%; intervention-related complications include infection, small-bowel obstruction, abdominal compartment syndrome, and rare vascular kinking of portal/hepatic vessels | Widely used conventional option; silastic/synthetic silo allows gradual bedside or OR reductions before fascial closure; literature is heterogeneous and outcomes depend heavily on defect severity and associated anomalies | (saxena2025europeanpaediatricsurgeons pages 7-8, saxena2025europeanpaediatricsurgeons pages 8-9, malhotra2023enhancingomphalocelecare pages 6-7) |
| Traction-assisted staged closure (fasciotens® Pediatric) | MAXO: traction-assisted closure; staged surgical closure | Consider for giant omphalocele when primary closure is not amenable but early neonatal fascial closure is desired; aims to enlarge abdominal domain and enable tension-less fascial approximation | Prospective multicenter series: 10 giant omphalocele + 6 gastroschisis; complete fascial closure in all; median time to closure 7 days for giant omphalocele (range 4–22); 2 traction-suture tear-outs and 1 skin dehiscence; no SSI, no abdominal compartment syndrome, and no ventral/umbilical hernia after median 12-month follow-up | Requires specialized device, fascial traction sutures/mesh anchoring, and NICU/surgical expertise; practical recommendations include direct fascial exposure and traction around ~30% body weight | (ziegler2024useofa pages 5-7, ziegler2024useofa pages 1-2, ziegler2024useofa pages 4-5, ziegler2024useofa pages 8-9) |
| Conservative delayed closure / “paint-and-wait” | MAXO: conservative management; topical medication administration; delayed closure | Recommended when anatomical constraints or high surgical risk preclude primary closure, especially giant omphalocele with liver exteriorization and/or pulmonary hypoplasia/pulmonary hypertension | EUPSA recommends paint-and-wait when primary closure is not feasible; common agents include povidone-iodine and silver sulfadiazine, with Manuka honey of emerging interest; consensus on dosing/duration remains unclear; avoids early compartment syndrome risk but requires prolonged epithelialization and later ventral hernia management | Standard non-operative pathway in many centers for severe giant omphaloceles; later definitive ventral hernia repair often needed; literature lacks standardized protocols | (namat2025omphaloceleandassociated pages 11-13, saxena2025europeanpaediatricsurgeons pages 7-8, saxena2025europeanpaediatricsurgeons pages 8-9, malhotra2023enhancingomphalocelecare pages 6-7) |
| Awake graduated compression dressing | MAXO: compression therapy; staged reduction; enteral feeding support | Alternative bedside strategy for exomphalos major when avoiding repeated general anesthesia/ventilation is desirable and sac integrity permits gradual reduction | Case series of 4 neonates: defects 5–7 cm; dressings started days 1–3; average time to full feeds 1 week; only 1 infant required parenteral nutrition; 3 underwent repair at 2–16 weeks, 1 at 1 year; none required patch repair or prolonged ventilation | Applied at bedside in neonatal ward while infants are awake; parents can be trained for dressing changes and some infants discharged home during compression period; facilitates simultaneous early enteral feeding | (widatella2024acaseseries pages 1-3, widatella2024acaseseries pages 5-6, widatella2024acaseseries pages 3-5) |
| Biological mesh for early closure | MAXO: surgical implantation of biological prosthesis; patch repair | Considered when early closure is pursued but native fascial closure is not yet possible; preferred over synthetic material in EUPSA guidance for early repair | EUPSA consensus states early closure favors biological meshes and suggests lower morbidity/mortality than synthetic materials; however, delayed patch closure had the highest mortality in pooled comparisons (63%), likely reflecting the sickest/severest defects | Choice depends on center experience, contamination risk, tissue availability, and defect severity; biologic material may integrate better than synthetic mesh | (saxena2025europeanpaediatricsurgeons pages 7-8, saxena2025europeanpaediatricsurgeons pages 8-9) |
| Component separation / native-tissue delayed closure | MAXO: component separation technique; delayed abdominal wall reconstruction | Used for delayed reconstruction after conservative management or staged reduction, particularly when native tissue closure is possible and patch avoidance is desired | EUPSA notes delayed closure appears most effective using native tissues; complications are generally intervention-related and long-term multidisciplinary follow-up is needed; may reduce need for permanent prosthetic material | Often part of later ventral hernia repair after paint-and-wait or delayed management; timing individualized based on growth, respiratory status, and abdominal domain | (saxena2025europeanpaediatricsurgeons pages 7-8, saxena2025europeanpaediatricsurgeons pages 8-9) |
Table: This table summarizes current management options for omphalocele, especially giant omphalocele, with indications, outcomes, complications, and suggested MAXO annotations. It highlights how treatment choice is driven mainly by defect size, viscero-abdominal disproportion, and cardiopulmonary risk.
13. Prevention
No specific primary prevention interventions with strong causal evidence were identified in the retrieved corpus. However, secondary prevention through prenatal detection is widely implemented and substantially influences observed live-birth prevalence because termination rates are high in many settings. (fogelstrom2021omphalocelenationalcurrent pages 1-2, raitio2021omphaloceleinfinland pages 5-9)
14. Other Species / Natural Disease
No veterinary/natural disease evidence was retrieved in the tool-accessible corpus.
15. Model Organisms
No model organism studies specific to omphalocele mechanisms were retrieved in the tool-accessible corpus.
Direct abstract quotes supporting key claims
-
Danish register prevalence and co-occurrence: “Among 1,498,685 live births, 147 infants with omphalocele were identified, yielding… prevalence… 0.98… Over one-half (53.7%) presented with one or more major malformations, and an additional 17.0% were diagnosed with a syndrome.” (Lausten‑Thomsen et al., 2024; https://doi.org/10.1007/s00383-024-05897-5) (laustenthomsen2024omphaloceleprevalenceand pages 1-2)
-
Chinese prenatal cohort outcomes & testing: “Routine karyotyping with CMA testing should be provided for fetuses with omphalocele. WES is an option if karyotype and CMA tests are normal… A 72% 1-year survival rate was observed from the successful 25 live births.” (Que et al., 2023; https://doi.org/10.1186/s12884-023-05999-3) (que2023ultrasonographiccharacteristicsgenetic pages 1-2)
-
Swedish coding and termination rate: “All cases of omphalocele were identified with the ICD-10 code Q79.2 (Omphalocele/Exomphalos)… The rate of termination of pregnancy was 59%.” (Fogelström et al., 2021; https://doi.org/10.1007/s00383-021-04978-z) (fogelstrom2021omphalocelenationalcurrent pages 1-2, fogelstrom2021omphalocelenationalcurrent pages 2-4)
-
Traction-assisted closure conclusion: “Traction-assisted staged closure… enabled an early tension-less fascial closure in GOC and GS in the newborn period.” (Ziegler et al., 2024; https://doi.org/10.1007/s00383-024-05745-6) (ziegler2024useofa pages 1-2)
Limitations of this report (evidence gaps)
- MONDO/Orphanet/MeSH/OMIM IDs were not accessible via the current tool evidence and should be appended from ontology databases.
- Evidence for environmental causes/protective factors, gene–environment interactions, multi-omics profiling, model organisms, and standardized global guidelines was limited in the retrieved corpus.
- The EUPSA consensus statement quantitative table data were extractable via text evidence but the article’s figures/tables were not accessible for image extraction in this run due to document retrieval limitations. (saxena2025europeanpaediatricsurgeons pages 7-8)
References
-
(fogelstrom2021omphalocelenationalcurrent pages 1-2): Anna Fogelström, Cecilia Caldeman, Jenny Oddsberg, Anna Löf Granström, and Carmen Mesas Burgos. Omphalocele: national current birth prevalence and survival. Pediatric Surgery International, 37:1515-1520, Aug 2021. URL: https://doi.org/10.1007/s00383-021-04978-z, doi:10.1007/s00383-021-04978-z. This article has 48 citations and is from a peer-reviewed journal.
-
(fogelstrom2021omphalocelenationalcurrent pages 2-4): Anna Fogelström, Cecilia Caldeman, Jenny Oddsberg, Anna Löf Granström, and Carmen Mesas Burgos. Omphalocele: national current birth prevalence and survival. Pediatric Surgery International, 37:1515-1520, Aug 2021. URL: https://doi.org/10.1007/s00383-021-04978-z, doi:10.1007/s00383-021-04978-z. This article has 48 citations and is from a peer-reviewed journal.
-
(malhotra2023enhancingomphalocelecare pages 1-3): Ritika Malhotra, Bhavana Malhotra, and Harshal Ramteke. Enhancing omphalocele care: navigating complications and innovative treatment approaches. Cureus, Oct 2023. URL: https://doi.org/10.7759/cureus.47638, doi:10.7759/cureus.47638. This article has 11 citations.
-
(laustenthomsen2024omphaloceleprevalenceand pages 1-2): Ulrik Lausten-Thomsen, Paula L. Hedley, Kristin M. Conway, Katrine M. Løfberg, Lars S. Johansen, Paul A. Romitti, and Michael Christiansen. Omphalocele prevalence and co-occurring malformations: a nationwide register-based study of danish live births in 1997–2021. Pediatric Surgery International, Nov 2024. URL: https://doi.org/10.1007/s00383-024-05897-5, doi:10.1007/s00383-024-05897-5. This article has 5 citations and is from a peer-reviewed journal.
-
(malhotra2023enhancingomphalocelecare pages 3-5): Ritika Malhotra, Bhavana Malhotra, and Harshal Ramteke. Enhancing omphalocele care: navigating complications and innovative treatment approaches. Cureus, Oct 2023. URL: https://doi.org/10.7759/cureus.47638, doi:10.7759/cureus.47638. This article has 11 citations.
-
(pijpers2023additionalanomaliesin pages 2-4): Adinda G. H. Pijpers, Cunera M. C. de Beaufort, Sanne C. Maat, Chantal J. M. Broers, Bart Straver, Ernest van Heurn, Ramon R. Gorter, and Joep P. M. Derikx. Additional anomalies in children with gastroschisis and omphalocele: a retrospective cohort study. Children, 10:688, Apr 2023. URL: https://doi.org/10.3390/children10040688, doi:10.3390/children10040688. This article has 11 citations.
-
(raitio2021omphaloceleinfinland pages 5-9): Arimatias Raitio, Asta Tauriainen, Johanna Syvänen, Teemu Kemppainen, Eliisa Löyttyniemi, Ulla Sankilampi, Kari Vanamo, Mika Gissler, Anna Hyvärinen, and Ilkka Helenius. Omphalocele in finland from 1993 to 2014: trends, prevalence, mortality, and associated malformations—a population-based study. European Journal of Pediatric Surgery, 31:172-176, Mar 2021. URL: https://doi.org/10.1055/s-0040-1703012, doi:10.1055/s-0040-1703012. This article has 37 citations and is from a peer-reviewed journal.
-
(que2023ultrasonographiccharacteristicsgenetic pages 1-2): Yanting Que, Meiying Cai, Fang Yang, Qingqiang Ji, Shuqi Zhang, Wenhui Huang, Yashi Gao, Bojing Zhou, Hailong Huang, Hua Cao, and Na Lin. Ultrasonographic characteristics, genetic features, and maternal and fetal outcomes in fetuses with omphalocele in china: a single tertiary center study. BMC Pregnancy and Childbirth, Sep 2023. URL: https://doi.org/10.1186/s12884-023-05999-3, doi:10.1186/s12884-023-05999-3. This article has 10 citations and is from a peer-reviewed journal.
-
(que2023ultrasonographiccharacteristicsgenetic pages 4-6): Yanting Que, Meiying Cai, Fang Yang, Qingqiang Ji, Shuqi Zhang, Wenhui Huang, Yashi Gao, Bojing Zhou, Hailong Huang, Hua Cao, and Na Lin. Ultrasonographic characteristics, genetic features, and maternal and fetal outcomes in fetuses with omphalocele in china: a single tertiary center study. BMC Pregnancy and Childbirth, Sep 2023. URL: https://doi.org/10.1186/s12884-023-05999-3, doi:10.1186/s12884-023-05999-3. This article has 10 citations and is from a peer-reviewed journal.
-
(ziegler2024useofa pages 5-7): Anna-Maria Ziegler, Daniel Svoboda, Britta Lüken-Darius, Andreas Heydweiller, Fritz Kahl, Sophie Christine Falk, Udo Rolle, and Till-Martin Theilen. Use of a new vertical traction device for early traction-assisted staged closure of congenital abdominal wall defects: a prospective series of 16 patients. Pediatric Surgery International, Jul 2024. URL: https://doi.org/10.1007/s00383-024-05745-6, doi:10.1007/s00383-024-05745-6. This article has 8 citations and is from a peer-reviewed journal.
-
(widatella2024acaseseries pages 1-3): Hussam Widatella, Sami Abd Elwahab, Zakya Penny, and Sri Thambipillai Paran. A case series of successfully managing exomphalos major with awake graduated compression dressing and early enteral feeding. Irish Journal of Medical Science, 193:1453-1459, Feb 2024. URL: https://doi.org/10.1007/s11845-024-03630-8, doi:10.1007/s11845-024-03630-8. This article has 2 citations and is from a peer-reviewed journal.
-
(saxena2025europeanpaediatricsurgeons pages 7-8): Amulya K. Saxena, Romilly K. Hayward, Annika Mutanen, Ayman Goneidy, Harmit Ghattaura, Ramon Gorter, Rene Weijnen, Richard Keijzer, and Tutku Soyer. European paediatric surgeons' association consensus statement on the management of giant omphalocele. European Journal of Pediatric Surgery, May 2025. URL: https://doi.org/10.1055/a-2590-5592, doi:10.1055/a-2590-5592. This article has 4 citations and is from a peer-reviewed journal.
-
(namat2025omphaloceleandassociated pages 11-13): Dina Al Namat, Romulus Adrian Roșca, Razan Al Namat, Elena Hanganu, Andrei Ivan, Delia Hînganu, Ancuța Lupu, and Marius Valeriu Hînganu. Omphalocele and associated anomalies: exploring pulmonary development and genetic correlations—a literature review. Diagnostics, 15:675, Mar 2025. URL: https://doi.org/10.3390/diagnostics15060675, doi:10.3390/diagnostics15060675. This article has 9 citations.
-
(que2023ultrasonographiccharacteristicsgenetic pages 2-4): Yanting Que, Meiying Cai, Fang Yang, Qingqiang Ji, Shuqi Zhang, Wenhui Huang, Yashi Gao, Bojing Zhou, Hailong Huang, Hua Cao, and Na Lin. Ultrasonographic characteristics, genetic features, and maternal and fetal outcomes in fetuses with omphalocele in china: a single tertiary center study. BMC Pregnancy and Childbirth, Sep 2023. URL: https://doi.org/10.1186/s12884-023-05999-3, doi:10.1186/s12884-023-05999-3. This article has 10 citations and is from a peer-reviewed journal.
-
(saxena2025europeanpaediatricsurgeons pages 8-9): Amulya K. Saxena, Romilly K. Hayward, Annika Mutanen, Ayman Goneidy, Harmit Ghattaura, Ramon Gorter, Rene Weijnen, Richard Keijzer, and Tutku Soyer. European paediatric surgeons' association consensus statement on the management of giant omphalocele. European Journal of Pediatric Surgery, May 2025. URL: https://doi.org/10.1055/a-2590-5592, doi:10.1055/a-2590-5592. This article has 4 citations and is from a peer-reviewed journal.
-
(fogelstrom2021omphalocelenationalcurrent pages 4-5): Anna Fogelström, Cecilia Caldeman, Jenny Oddsberg, Anna Löf Granström, and Carmen Mesas Burgos. Omphalocele: national current birth prevalence and survival. Pediatric Surgery International, 37:1515-1520, Aug 2021. URL: https://doi.org/10.1007/s00383-021-04978-z, doi:10.1007/s00383-021-04978-z. This article has 48 citations and is from a peer-reviewed journal.
-
(que2023ultrasonographiccharacteristicsgenetic pages 8-9): Yanting Que, Meiying Cai, Fang Yang, Qingqiang Ji, Shuqi Zhang, Wenhui Huang, Yashi Gao, Bojing Zhou, Hailong Huang, Hua Cao, and Na Lin. Ultrasonographic characteristics, genetic features, and maternal and fetal outcomes in fetuses with omphalocele in china: a single tertiary center study. BMC Pregnancy and Childbirth, Sep 2023. URL: https://doi.org/10.1186/s12884-023-05999-3, doi:10.1186/s12884-023-05999-3. This article has 10 citations and is from a peer-reviewed journal.
-
(raitioUnknownyearomphaloceleinfinland pages 1-5): A Raitio, A Tauriainen, J Syvänen, and T Kemppainen. Omphalocele in finland from 1993 to 2014: trends. Unknown journal, Unknown year.
-
(malhotra2023enhancingomphalocelecare pages 6-7): Ritika Malhotra, Bhavana Malhotra, and Harshal Ramteke. Enhancing omphalocele care: navigating complications and innovative treatment approaches. Cureus, Oct 2023. URL: https://doi.org/10.7759/cureus.47638, doi:10.7759/cureus.47638. This article has 11 citations.
-
(ziegler2024useofa pages 1-2): Anna-Maria Ziegler, Daniel Svoboda, Britta Lüken-Darius, Andreas Heydweiller, Fritz Kahl, Sophie Christine Falk, Udo Rolle, and Till-Martin Theilen. Use of a new vertical traction device for early traction-assisted staged closure of congenital abdominal wall defects: a prospective series of 16 patients. Pediatric Surgery International, Jul 2024. URL: https://doi.org/10.1007/s00383-024-05745-6, doi:10.1007/s00383-024-05745-6. This article has 8 citations and is from a peer-reviewed journal.
-
(ziegler2024useofa media f0a1df53): Anna-Maria Ziegler, Daniel Svoboda, Britta Lüken-Darius, Andreas Heydweiller, Fritz Kahl, Sophie Christine Falk, Udo Rolle, and Till-Martin Theilen. Use of a new vertical traction device for early traction-assisted staged closure of congenital abdominal wall defects: a prospective series of 16 patients. Pediatric Surgery International, Jul 2024. URL: https://doi.org/10.1007/s00383-024-05745-6, doi:10.1007/s00383-024-05745-6. This article has 8 citations and is from a peer-reviewed journal.
-
(ziegler2024useofa pages 4-5): Anna-Maria Ziegler, Daniel Svoboda, Britta Lüken-Darius, Andreas Heydweiller, Fritz Kahl, Sophie Christine Falk, Udo Rolle, and Till-Martin Theilen. Use of a new vertical traction device for early traction-assisted staged closure of congenital abdominal wall defects: a prospective series of 16 patients. Pediatric Surgery International, Jul 2024. URL: https://doi.org/10.1007/s00383-024-05745-6, doi:10.1007/s00383-024-05745-6. This article has 8 citations and is from a peer-reviewed journal.
-
(ziegler2024useofa pages 8-9): Anna-Maria Ziegler, Daniel Svoboda, Britta Lüken-Darius, Andreas Heydweiller, Fritz Kahl, Sophie Christine Falk, Udo Rolle, and Till-Martin Theilen. Use of a new vertical traction device for early traction-assisted staged closure of congenital abdominal wall defects: a prospective series of 16 patients. Pediatric Surgery International, Jul 2024. URL: https://doi.org/10.1007/s00383-024-05745-6, doi:10.1007/s00383-024-05745-6. This article has 8 citations and is from a peer-reviewed journal.
-
(widatella2024acaseseries pages 5-6): Hussam Widatella, Sami Abd Elwahab, Zakya Penny, and Sri Thambipillai Paran. A case series of successfully managing exomphalos major with awake graduated compression dressing and early enteral feeding. Irish Journal of Medical Science, 193:1453-1459, Feb 2024. URL: https://doi.org/10.1007/s11845-024-03630-8, doi:10.1007/s11845-024-03630-8. This article has 2 citations and is from a peer-reviewed journal.
-
(widatella2024acaseseries pages 3-5): Hussam Widatella, Sami Abd Elwahab, Zakya Penny, and Sri Thambipillai Paran. A case series of successfully managing exomphalos major with awake graduated compression dressing and early enteral feeding. Irish Journal of Medical Science, 193:1453-1459, Feb 2024. URL: https://doi.org/10.1007/s11845-024-03630-8, doi:10.1007/s11845-024-03630-8. This article has 2 citations and is from a peer-reviewed journal.