Multiple Epiphyseal Dysplasia
Multiple epiphyseal dysplasia (MED) is a clinically and genetically heterogeneous skeletal dysplasia characterized by abnormal development and delayed, irregular ossification of multiple epiphyses. It typically presents in early childhood with joint pain (especially of the hips and knees), joint stiffness, fatigue, and waddling gait, and progresses to early-onset osteoarthritis of the large weight-bearing joints with variable, usually mild, short stature. MED is caused by pathogenic variants in genes encoding cartilage extracellular matrix proteins and a sulfate transporter. Autosomal dominant forms result from heterozygous variants in COMP (the most common and generally most severe subtype), MATN3, COL9A1, COL9A2, and COL9A3; an autosomal recessive form (rMED, MED-4) is caused by biallelic SLC26A2 variants. Dominant ECM-gene mutations act through mutant protein misfolding and retention in the chondrocyte endoplasmic reticulum with ER stress and abnormal cartilage matrix, whereas SLC26A2 deficiency impairs chondrocyte sulfate uptake, leading to undersulfated proteoglycans and disturbed chondrocyte differentiation.
Ask OpenScientist
Ask a research question about Multiple Epiphyseal Dysplasia. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Inheritance
2Show evidence (1 reference)
Show evidence (1 reference)
Subtypes
7Show evidence (1 reference)
Pathophysiology
4Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Pathograph
Phenotypes
14Limbs 2
Show evidence (1 reference)
Show evidence (1 reference)
Musculoskeletal 3
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Nervous System 1
Show evidence (1 reference)
Constitutional 1
Show evidence (2 references)
Growth 1
Show evidence (2 references)
Other 6
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Genetic Associations
7Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Medical Actions
5Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Source YAML
click to showname: Multiple Epiphyseal Dysplasia
creation_date: "2026-06-05T12:00:00Z"
category: Mendelian
description: >
Multiple epiphyseal dysplasia (MED) is a clinically and genetically
heterogeneous skeletal dysplasia characterized by abnormal development and
delayed, irregular ossification of multiple epiphyses. It typically presents
in early childhood with joint pain (especially of the hips and knees), joint
stiffness, fatigue, and waddling gait, and progresses to early-onset
osteoarthritis of the large weight-bearing joints with variable, usually mild,
short stature. MED is caused by pathogenic variants in genes encoding
cartilage extracellular matrix proteins and a sulfate transporter. Autosomal
dominant forms result from heterozygous variants in COMP (the most common and
generally most severe subtype), MATN3, COL9A1, COL9A2, and COL9A3; an
autosomal recessive form (rMED, MED-4) is caused by biallelic SLC26A2 variants.
Dominant ECM-gene mutations act through mutant protein misfolding and retention
in the chondrocyte endoplasmic reticulum with ER stress and abnormal cartilage
matrix, whereas SLC26A2 deficiency impairs chondrocyte sulfate uptake, leading
to undersulfated proteoglycans and disturbed chondrocyte differentiation.
notes: >
Health-related quality of life: the physical domain of HRQoL deteriorates at a
young age in MED. On the Short Form-36, the physical component summary score is
significantly lower than in the general population and tends to worsen with
age, and MED patients with osteoarthritis have a particularly low physical
component score (PMID:34909512). MED should be kept distinct from
spondyloepiphyseal dysplasia (SED), which is epiphyseal plus vertebral and
often involves ocular problems; MED is epiphyseal-predominant.
disease_term:
preferred_term: Multiple Epiphyseal Dysplasia
term:
id: MONDO:0016648
label: multiple epiphyseal dysplasia
parents:
- Skeletal Dysplasia
references:
- reference: PMID:20301302
title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
tags:
- GeneReviews
- reference: PMID:20301483
title: "SLC26A2-Related Multiple Epiphyseal Dysplasia."
tags:
- GeneReviews
has_subtypes:
- name: EDM1
display_name: MED type 1 (COMP-related, EDM1)
subtype_term:
preferred_term: Multiple epiphyseal dysplasia type 1
term:
id: MONDO:0007561
label: multiple epiphyseal dysplasia type 1
description: >
Autosomal dominant MED caused by heterozygous variants in COMP (cartilage
oligomeric matrix protein). The most common MED subtype, accounting for
roughly half of autosomal dominant MED, and generally the most severe, with
prominent involvement of the capital femoral epiphyses and irregular
acetabula and the greatest need for orthopedic surgery.
- name: EDM2
display_name: MED type 2 (COL9A2-related)
subtype_term:
preferred_term: Multiple epiphyseal dysplasia type 2
term:
id: MONDO:0010844
label: epiphyseal dysplasia, multiple, 2
description: >
Autosomal dominant MED caused by heterozygous variants in COL9A2 (collagen
type IX alpha 2 chain). Part of the collagen IX-related MED spectrum, which
tends to show relatively prominent knee involvement and may be associated
with osteochondritis dissecans and myopathy in some families.
- name: EDM3
display_name: MED type 3 (COL9A3-related)
subtype_term:
preferred_term: Multiple epiphyseal dysplasia type 3
term:
id: MONDO:0010964
label: epiphyseal dysplasia, multiple, 3
description: >
Autosomal dominant MED caused by heterozygous variants in COL9A3 (collagen
type IX alpha 3 chain), part of the collagen IX-related MED spectrum.
- name: EDM5
display_name: MED type 5 (MATN3-related)
subtype_term:
preferred_term: Multiple epiphyseal dysplasia type 5
term:
id: MONDO:0011765
label: multiple epiphyseal dysplasia type 5
description: >
Autosomal dominant MED caused by heterozygous variants in MATN3 (matrilin 3),
an established dominant MED gene associated with flattened epiphyses.
- name: EDM6
display_name: MED type 6 (COL9A1-related)
subtype_term:
preferred_term: Multiple epiphyseal dysplasia type 6
term:
id: MONDO:0013591
label: epiphyseal dysplasia, multiple, 6
description: >
Autosomal dominant MED caused by heterozygous variants in COL9A1 (collagen
type IX alpha 1 chain), part of the collagen IX-related MED spectrum.
- name: rMED
display_name: MED type 4 / recessive MED (SLC26A2-related, MED-4)
subtype_term:
preferred_term: Multiple epiphyseal dysplasia type 4
term:
id: MONDO:0009189
label: multiple epiphyseal dysplasia type 4
description: >
Autosomal recessive MED caused by biallelic variants in SLC26A2 (the
diastrophic dysplasia sulfate transporter, DTDST). Characterized by joint
pain, malformations of hands, feet and knees, scoliosis, and a relatively
characteristic double-layered/bipartite patella. Approximately half of
affected individuals have an abnormal finding at birth such as clubfoot.
- name: EDM7
display_name: MED type 7 (CANT1-related, MED-7)
subtype_term:
preferred_term: Multiple epiphyseal dysplasia type 7
term:
id: MONDO:0054680
label: epiphyseal dysplasia, multiple, 7
description: >
Autosomal recessive MED caused by biallelic variants in CANT1 (calcium
activated nucleotidase 1). CANT1 is the same gene mutated in Desbuquois
dysplasia, and MED type 7 represents a milder end of the CANT1-related
phenotypic spectrum that can present as isolated multiple epiphyseal
dysplasia without the classic Desbuquois features. No CANT1-positive family
was identified in the Daşar 2025 cohort, but CANT1 is an established gene in
the MED nosology.
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Multiple epiphyseal dysplasias are caused by variants in the genes
encoding important cartilage extracellular matrix proteins, enzymes, and
transporter proteins, including COMP, MATN3, COL9A1, COL9A2, COL9A3,
CANT1, and SLC26A2.
explanation: >-
Lists CANT1 among the established multiple epiphyseal dysplasia genes in
the disease nosology.
inheritance:
- name: Autosomal Dominant
description: >
MED caused by variants in COMP, MATN3, COL9A1, COL9A2, or COL9A3 is inherited
in an autosomal dominant manner; many affected individuals have an affected
parent, and each child of an affected individual has a 50% chance of
inheriting the variant.
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
By definition, autosomal dominant MED is inherited in an autosomal
dominant manner.
explanation: >-
GeneReviews establishes autosomal dominant inheritance for COMP/MATN3/COL9-
related MED.
- name: Autosomal Recessive
description: >
SLC26A2-related MED (rMED, MED-4) is inherited in an autosomal recessive
manner, with biallelic SLC26A2 variants required to cause disease.
evidence:
- reference: PMID:20301483
reference_title: "SLC26A2-Related Multiple Epiphyseal Dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
SLC26A2-MED is inherited in an autosomal recessive manner.
explanation: >-
GeneReviews establishes autosomal recessive inheritance for SLC26A2-related
MED.
prevalence:
- population: General population
notes: >-
MED is described as one of the more common skeletal dysplasias; it is
relatively common among the epiphyseal dysplasias, though precise
registry-derived prevalence figures are limited.
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Multiple epiphyseal dysplasias are relatively common skeletal disorders
explanation: >-
Single-center 20-year cohort describes MED as a relatively common skeletal
disorder.
progression:
- phase: Early Childhood Onset
age_range: Early childhood
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Autosomal dominant multiple epiphyseal dysplasia (MED) presents in early
childhood, usually with pain in the hips and/or knees after exercise.
explanation: >-
GeneReviews documents early-childhood onset of joint pain in autosomal
dominant MED.
- phase: Progressive Joint Degeneration and Early Osteoarthritis
age_range: Adolescence to adulthood
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Pain and joint deformity progress, resulting in early-onset
osteoarthritis, particularly of the large weight-bearing joints.
explanation: >-
GeneReviews documents progression to early-onset osteoarthritis of large
weight-bearing joints.
- reference: PMID:37904148
reference_title: "The favorable outcome of Bernese periacetabular osteotomy for the hip osteoarthritis in multiple epiphyseal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Patients with MED develop secondary hip osteoarthritis as early as the
third to the fourth decade.
explanation: >-
Surgical series documents secondary hip osteoarthritis emerging in early
adulthood.
pathophysiology:
- name: Mutant Cartilage Matrix Protein Misfolding and ER Retention
description: >
In autosomal dominant MED, mutant cartilage extracellular matrix proteins
(COMP, type IX collagen, matrilin-3) misfold and are retained within the
rough endoplasmic reticulum of chondrocytes, where they co-retain other ECM
proteins. This triggers endoplasmic reticulum stress and the unfolded
protein response, producing abnormal cartilage matrix. COMP-MED is the most
common and severe subtype, whereas collagen IX-related MED alters ECM
composition with relatively prominent knee involvement.
genes:
- preferred_term: COMP
term:
id: hgnc:2227
label: COMP
- preferred_term: MATN3
term:
id: hgnc:6909
label: MATN3
- preferred_term: COL9A1
term:
id: hgnc:2217
label: COL9A1
- preferred_term: COL9A2
term:
id: hgnc:2218
label: COL9A2
- preferred_term: COL9A3
term:
id: hgnc:2219
label: COL9A3
cell_types:
- preferred_term: Chondrocyte
term:
id: CL:0000138
label: chondrocyte
biological_processes:
- preferred_term: Protein Folding
term:
id: GO:0006457
label: protein folding
modifier: ABNORMAL
- preferred_term: Response to Endoplasmic Reticulum Stress
term:
id: GO:0034976
label: response to endoplasmic reticulum stress
modifier: INCREASED
- preferred_term: Extracellular Matrix Organization
term:
id: GO:0030198
label: extracellular matrix organization
modifier: ABNORMAL
downstream:
- target: Abnormal Epiphyseal Cartilage and Endochondral Ossification
causal_link_type: DIRECT
description: >-
Abnormal cartilage matrix from retained/misassembled ECM proteins disrupts
epiphyseal growth and ossification.
evidence:
- reference: PMID:39596690
reference_title: "Multiple Osteochondritis Dissecans as Main Manifestation of Multiple Epiphyseal Dysplasia Caused by a Novel Cartilage Oligomeric Matrix Protein Pathogenic Variant: A Clinical Report."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
MED, caused by mutations in the Cartilage Oligomeric Matrix Protein (COMP)
gene, is the most common form of the disease.
explanation: >-
Establishes COMP as the most common cause of MED, the central gene in the
dominant ECM-protein mechanism.
- reference: PMID:39596690
reference_title: "Multiple Osteochondritis Dissecans as Main Manifestation of Multiple Epiphyseal Dysplasia Caused by a Novel Cartilage Oligomeric Matrix Protein Pathogenic Variant: A Clinical Report."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
COMP-MED usually shows significant involvement of the capital femoral
epiphyses and irregular acetabulum; instead, COL9A1-, COL9A2-, and
COL9A3-MED appear to have more severe knee involvement than hips
explanation: >-
Documents the gene-specific anatomical patterns distinguishing COMP-MED
from collagen IX-related MED.
- name: SLC26A2 Sulfate Transport Defect and Disturbed Chondrocyte Homeostasis
description: >
In recessive MED (MED-4), biallelic SLC26A2 variants reduce sulfate uptake
into chondrocytes, producing undersulfated cartilage proteoglycans and
disturbed chondrocyte homeostasis. Mutant SLC26A2 protein shows reduced
expression and abnormal subcellular localization, and chondrocyte
differentiation markers are altered (decreased MMP13, COL10A1, and RUNX2;
increased aggrecan), favoring proliferation while inhibiting differentiation.
genes:
- preferred_term: SLC26A2
term:
id: hgnc:10994
label: SLC26A2
molecular_functions:
- preferred_term: sulfate transmembrane transporter activity
term:
id: GO:0015116
label: sulfate transmembrane transporter activity
cell_types:
- preferred_term: Chondrocyte
term:
id: CL:0000138
label: chondrocyte
biological_processes:
- preferred_term: Sulfate Transmembrane Transport
term:
id: GO:1902358
label: sulfate transmembrane transport
modifier: DECREASED
- preferred_term: Chondrocyte Differentiation
term:
id: GO:0002062
label: chondrocyte differentiation
modifier: ABNORMAL
downstream:
- target: Abnormal Epiphyseal Cartilage and Endochondral Ossification
causal_link_type: DIRECT
description: >-
Undersulfated proteoglycans and disturbed chondrocyte differentiation
impair epiphyseal cartilage and ossification.
evidence:
- reference: PMID:38956600
reference_title: "Biallelic variants in SLC26A2 cause multiple epiphyseal dysplasia-4 by disturbing chondrocyte homeostasis."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: >-
Overall, our data demonstrate that the variants p.Val341del and
p.Ile421Thr in SLC26A2 cause MED-4 and that these two variants promote
chondrocyte proliferation while inhibiting chondrocyte differentiation.
explanation: >-
Functional study in primary human chondrocytes links SLC26A2 variants to
disturbed chondrocyte differentiation in MED-4.
- reference: PMID:38956600
reference_title: "Biallelic variants in SLC26A2 cause multiple epiphyseal dysplasia-4 by disturbing chondrocyte homeostasis."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: >-
Expression levels of matrix metallopeptidase 13 (MMP13), α-1 chain of type
X collagen (COL10A1), and Runt-related transcription factor 2 (RUNX2) were
significantly decreased in the variant group. However, aggrecan (ACAN)
expression was higher in the variant group than the WT group.
explanation: >-
Documents the specific shift in chondrocyte differentiation markers caused
by SLC26A2 variants.
- name: Abnormal Epiphyseal Cartilage and Endochondral Ossification
description: >
Both the dominant ECM-protein and recessive sulfate-transport mechanisms
converge on abnormal epiphyseal cartilage with delayed and irregular
ossification of multiple epiphyses, producing the small, flat, irregular
epiphyses that are the radiographic hallmark of MED, predominantly in the
hips and knees, and driving progressive joint degeneration.
cell_types:
- preferred_term: Chondrocyte
term:
id: CL:0000138
label: chondrocyte
biological_processes:
- preferred_term: Cartilage Development
term:
id: GO:0051216
label: cartilage development
modifier: ABNORMAL
downstream:
- target: Premature Osteoarthritis
causal_link_type: DIRECT
description: >-
Abnormal epiphyseal cartilage and joint incongruity drive early-onset
degenerative joint disease in weight-bearing joints.
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Radiographs are characterized by flat, small, and irregularly shaped
epiphyses, especially in the hips and knees.
explanation: >-
Documents the abnormal epiphyseal cartilage/ossification phenotype central
to MED.
- name: Premature Osteoarthritis
description: >
Joint incongruity and abnormal cartilage from epiphyseal dysplasia lead to
early-onset osteoarthritis of large weight-bearing joints, often requiring
joint-preserving osteotomy or joint replacement at a relatively young age.
cell_types:
- preferred_term: Chondrocyte
term:
id: CL:0000138
label: chondrocyte
biological_processes:
- preferred_term: Cartilage Development
term:
id: GO:0051216
label: cartilage development
modifier: ABNORMAL
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Pain and joint deformity progress, resulting in early-onset
osteoarthritis, particularly of the large weight-bearing joints.
explanation: >-
GeneReviews documents premature osteoarthritis as the downstream
consequence of epiphyseal dysplasia.
genetic:
- name: COMP Pathogenic Variants
subtype: EDM1
gene_term:
preferred_term: COMP
term:
id: hgnc:2227
label: COMP
association: Causative
notes: >
Heterozygous COMP variants cause autosomal dominant MED type 1 (EDM1) and
are the most common cause of MED, accounting for roughly half of autosomal
dominant cases. COMP-MED is generally the most severe subtype.
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
COMP (13/25 patients, 52%; 7/12
families, 58.3%)
explanation: >-
COMP was the most frequent causative gene in this genetically resolved MED
cohort.
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Patients with COMP variants exhibited a more severe phenotype, consistent
with the literature.
explanation: >-
Documents that COMP-MED is the more severe MED subtype.
- name: MATN3 Pathogenic Variants
subtype: EDM5
gene_term:
preferred_term: MATN3
term:
id: hgnc:6909
label: MATN3
association: Causative
notes: >
Heterozygous MATN3 variants cause autosomal dominant MED type 5 (EDM5).
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
MATN3 (5/25 patients, 20%; 2/12 families, 16.6%)
explanation: >-
MATN3 was the second most frequent causative gene in this MED cohort.
- name: COL9A1 Pathogenic Variants
subtype: EDM6
gene_term:
preferred_term: COL9A1
term:
id: hgnc:2217
label: COL9A1
association: Causative
notes: >
Heterozygous COL9A1 variants cause autosomal dominant MED type 6 (EDM6),
part of the collagen IX-related MED spectrum.
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
a heterozygous pathogenic variant in COL9A1, COL9A2, COL9A3, COMP, or
MATN3 identified by molecular genetic testing.
explanation: >-
GeneReviews lists COL9A1 among the autosomal dominant MED genes.
- name: COL9A2 Pathogenic Variants
subtype: EDM2
gene_term:
preferred_term: COL9A2
term:
id: hgnc:2218
label: COL9A2
association: Causative
notes: >
Heterozygous COL9A2 variants cause autosomal dominant MED type 2 (EDM2),
part of the collagen IX-related MED spectrum, which may be associated with
osteochondritis dissecans.
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
COL9A2 (2/25 patients, 8%; 1/12
families 8.3%)
explanation: >-
COL9A2 was identified as a causative gene in this MED cohort.
- name: COL9A3 Pathogenic Variants
subtype: EDM3
gene_term:
preferred_term: COL9A3
term:
id: hgnc:2219
label: COL9A3
association: Causative
notes: >
Heterozygous COL9A3 variants cause autosomal dominant MED type 3 (EDM3),
part of the collagen IX-related MED spectrum.
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
a heterozygous pathogenic variant in COL9A1, COL9A2, COL9A3, COMP, or
MATN3 identified by molecular genetic testing.
explanation: >-
GeneReviews lists COL9A3 among the autosomal dominant MED genes.
- name: SLC26A2 Biallelic Pathogenic Variants
subtype: rMED
gene_term:
preferred_term: SLC26A2
term:
id: hgnc:10994
label: SLC26A2
association: Causative
notes: >
Biallelic SLC26A2 (DTDST) variants cause autosomal recessive MED (rMED,
MED-4). SLC26A2 is part of an allelic spectrum that also includes
diastrophic dysplasia, atelosteogenesis type 2, and achondrogenesis 1B; the
recurrent p.Arg279Trp (R279W) variant is commonly associated with rMED.
evidence:
- reference: PMID:38956600
reference_title: "Biallelic variants in SLC26A2 cause multiple epiphyseal dysplasia-4 by disturbing chondrocyte homeostasis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
MED-4 is caused by homozygous or compound heterozygous pathogenic variants
in the SLC26A2 gene.
explanation: >-
Establishes biallelic SLC26A2 variants as the cause of recessive MED-4.
- reference: PMID:36660027
reference_title: "SLC26A2/DTDST Spectrum: A Cohort of 12 Patients Associated with a Comprehensive Review of the Genotype-Phenotype Correlation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Outside of Finland, rMED is the most prevalent phenotype, usually
associated with R279W in hmz.
explanation: >-
Documents the genotype-phenotype correlation of the recurrent R279W variant
with rMED.
- name: CANT1 Biallelic Pathogenic Variants
subtype: EDM7
gene_term:
preferred_term: CANT1
term:
id: hgnc:19721
label: CANT1
association: Causative
notes: >
Biallelic CANT1 (calcium activated nucleotidase 1) variants cause autosomal
recessive MED type 7 (EDM7). CANT1 is allelic with Desbuquois dysplasia, and
MED-7 represents a milder phenotype within the CANT1 spectrum that can lack
the classic Desbuquois features. No CANT1-positive family was identified in
the Daşar 2025 cohort, but CANT1 remains an established gene in the MED
nosology.
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Multiple epiphyseal dysplasias are caused by variants in the genes
encoding important cartilage extracellular matrix proteins, enzymes, and
transporter proteins, including COMP, MATN3, COL9A1, COL9A2, COL9A3,
CANT1, and SLC26A2.
explanation: >-
Lists CANT1 among the established causative genes for multiple epiphyseal
dysplasia.
phenotypes:
- category: Skeletal
name: Multiple Epiphyseal Dysplasia
frequency: OBLIGATE
description: >
Abnormal development with delayed, irregular ossification of multiple
epiphyses is the defining feature, with flat, small, irregular epiphyses
most prominent in the hips and knees.
phenotype_term:
preferred_term: Multiple epiphyseal dysplasia
term:
id: HP:0002654
label: Multiple epiphyseal dysplasia
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Radiographs are characterized by flat, small, and irregularly shaped
epiphyses, especially in the hips and knees.
explanation: >-
The defining radiographic epiphyseal abnormality of MED.
- category: Skeletal
name: Joint Pain
frequency: FREQUENT
description: >
Joint pain, especially of the hips and knees and often after exercise, is the
most frequent presenting complaint in MED.
phenotype_term:
preferred_term: Arthralgia
term:
id: HP:0002829
label: Arthralgia
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
(17/25, 68%) experienced joint pain
explanation: >-
Joint pain was present in 68% of patients in this MED cohort.
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Autosomal dominant multiple epiphyseal dysplasia (MED) presents in early
childhood, usually with pain in the hips and/or knees after exercise.
explanation: >-
GeneReviews documents hip/knee joint pain as the typical presenting feature.
- category: Skeletal
name: Joint Stiffness
description: >
Joint stiffness is an early clinical manifestation, occurring in childhood
along with joint pain and evolving into degenerative joint disease.
phenotype_term:
preferred_term: Joint stiffness
term:
id: HP:0001387
label: Joint stiffness
evidence:
- reference: PMID:39596690
reference_title: "Multiple Osteochondritis Dissecans as Main Manifestation of Multiple Epiphyseal Dysplasia Caused by a Novel Cartilage Oligomeric Matrix Protein Pathogenic Variant: A Clinical Report."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
the first clinical manifestations still occur in childhood with joint pain
and stiffness that evolve into degenerative joint disease.
explanation: >-
Documents joint stiffness as an early childhood manifestation of MED.
- category: Skeletal
name: Waddling Gait
description: >
A waddling gait may be present, reflecting hip and lower-limb involvement,
and difficulty walking is a common reason for referral.
phenotype_term:
preferred_term: Waddling gait
term:
id: HP:0002515
label: Waddling gait
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Waddling gait may be present.
explanation: >-
GeneReviews documents waddling gait in autosomal dominant MED.
- category: Skeletal
name: Short Stature
frequency: FREQUENT
description: >
Short stature is variable and usually mild; adult height is either in the
lower range of normal or mildly shortened, with limbs relatively short
compared to the trunk.
phenotype_term:
preferred_term: Short stature
term:
id: HP:0004322
label: Short stature
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Nine patients (9/25, 36%) had short stature
explanation: >-
Short stature was present in 36% of patients in this MED cohort.
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Adult height is either in the lower range of normal or mildly shortened.
explanation: >-
GeneReviews documents mild/variable short stature in MED.
- category: Skeletal
name: Premature Osteoarthritis
frequency: FREQUENT
description: >
Early-onset osteoarthritis of the large weight-bearing joints, particularly
the hips, develops as a progressive complication, sometimes by the third to
fourth decade.
phenotype_term:
preferred_term: Premature osteoarthritis
term:
id: HP:0003088
label: Premature osteoarthritis
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Pain and joint deformity progress, resulting in early-onset
osteoarthritis, particularly of the large weight-bearing joints.
explanation: >-
GeneReviews documents early-onset osteoarthritis of weight-bearing joints.
- reference: PMID:37904148
reference_title: "The favorable outcome of Bernese periacetabular osteotomy for the hip osteoarthritis in multiple epiphyseal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Patients with MED develop secondary hip osteoarthritis as early as the
third to the fourth decade.
explanation: >-
Documents premature secondary hip osteoarthritis in MED.
- category: Skeletal
name: Flattened Epiphysis
description: >
Flat epiphyses are a characteristic radiographic finding in MED.
phenotype_term:
preferred_term: Flattened epiphysis
term:
id: HP:0003071
label: Flattened epiphysis
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Radiographs are characterized by flat, small, and irregularly shaped
epiphyses, especially in the hips and knees.
explanation: >-
Flat epiphyses are documented as a radiographic hallmark of MED.
- category: Skeletal
name: Fragmented, Irregular Epiphyses
description: >
Irregularly shaped, fragmented epiphyses are a core radiographic feature,
especially at the hips and knees.
phenotype_term:
preferred_term: Fragmented, irregular epiphyses
term:
id: HP:0005063
label: Fragmented, irregular epiphyses
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Radiographs are characterized by flat, small, and irregularly shaped
epiphyses, especially in the hips and knees.
explanation: >-
Irregularly shaped epiphyses are documented as a radiographic hallmark of
MED.
- category: Skeletal
name: Genu Valgum
description: >
Valgus knee deformity (genu valgum) is among the limb deformities for which
affected individuals are monitored, alongside genu varum.
phenotype_term:
preferred_term: Genu valgum
term:
id: HP:0002857
label: Genu valgum
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Evaluation by an orthopedic surgeon for chronic pain and/or limb
deformities (genu varum, genu valgum).
explanation: >-
GeneReviews documents genu valgum among MED limb deformities under
surveillance.
- category: Skeletal
name: Osteochondritis Dissecans
description: >
Osteochondritis dissecans is an uncommon but recognized manifestation,
reported in COL9A2-related MED families and, in an expanding phenotype, as a
main manifestation of COMP-related MED.
phenotype_term:
preferred_term: Osteochondritis dissecans
term:
id: HP:0010886
label: Osteochondritis dissecans
evidence:
- reference: PMID:39596690
reference_title: "Multiple Osteochondritis Dissecans as Main Manifestation of Multiple Epiphyseal Dysplasia Caused by a Novel Cartilage Oligomeric Matrix Protein Pathogenic Variant: A Clinical Report."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
multiple OCD can also be present in COMP-related MED as well as in
COL9A2-related MED.
explanation: >-
Documents osteochondritis dissecans in both COMP- and COL9A2-related MED.
- category: Skeletal
name: Bipartite Patella
subtype: rMED
description: >
A double-layered or bipartite patella is a relatively characteristic finding
in SLC26A2-related (recessive) MED.
phenotype_term:
preferred_term: Bipartite patella
term:
id: HP:0010498
label: Bipartite patella
evidence:
- reference: PMID:36660027
reference_title: "SLC26A2/DTDST Spectrum: A Cohort of 12 Patients Associated with a Comprehensive Review of the Genotype-Phenotype Correlation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Pathogenic variants in the SLC26A2/DTDST gene cause the following spectrum
of phenotypes: achondrogenesis 1B (ACG1B), atelosteogenesis 2 (AO2),
diastrophic dysplasia (DTD), and recessive-multiple epiphyseal dysplasia
(rMED)
explanation: >-
Establishes rMED as part of the SLC26A2 spectrum in which a double-layered
patella is characteristic.
- category: Skeletal
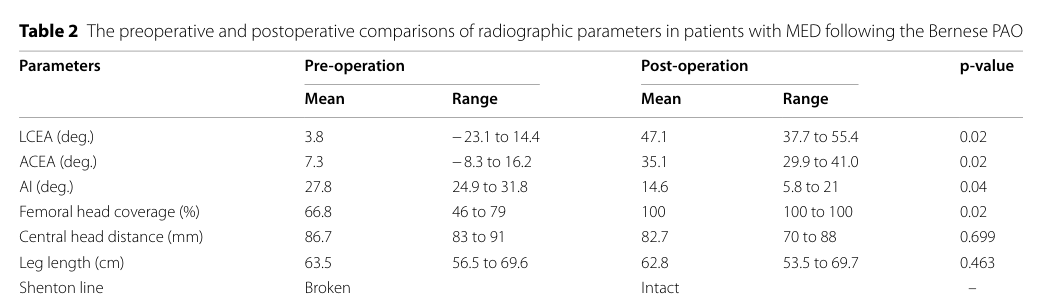
name: Acetabular Dysplasia
description: >
Acetabular dysplasia with deficient femoral head coverage is a recognized hip
manifestation of MED that contributes to hip pain and predisposes to secondary
hip osteoarthritis; it can be corrected by acetabular reshaping with
periacetabular osteotomy.
phenotype_term:
preferred_term: Acetabular dysplasia
term:
id: HP:0008807
label: Acetabular dysplasia
evidence:
- reference: PMID:37904148
reference_title: "The favorable outcome of Bernese periacetabular osteotomy for the hip osteoarthritis in multiple epiphyseal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The Bernese periacetabular osteotomy (PAO) is a joint-preserving surgery to
reshape acetabulum and extend femoral head coverage.
explanation: >-
MED hips show deficient femoral head coverage (acetabular dysplasia)
addressed by acetabular reshaping; the PAO series reports correction of a
markedly low preoperative lateral center-edge angle.
- category: Skeletal
name: Scoliosis
subtype: rMED
description: >
Scoliosis is part of the clinical picture of SLC26A2-related MED, alongside
hand, foot, and knee malformations.
phenotype_term:
preferred_term: Scoliosis
term:
id: HP:0002650
label: Scoliosis
evidence:
- reference: PMID:20301483
reference_title: "SLC26A2-Related Multiple Epiphyseal Dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
SLC26A2-related multiple epiphyseal dysplasia (SLC26A2-MED) is
characterized by joint pain (usually in the hips or knees); malformations
of hands, feet, and knees; and scoliosis.
explanation: >-
GeneReviews documents scoliosis as a feature of SLC26A2-related MED.
- category: Skeletal
name: Clubfoot
subtype: rMED
description: >
About half of individuals with SLC26A2-related MED have an abnormal finding
at birth such as clubfoot.
phenotype_term:
preferred_term: Clubfoot
term:
id: HP:0001762
label: Talipes equinovarus
evidence:
- reference: PMID:20301483
reference_title: "SLC26A2-Related Multiple Epiphyseal Dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Approximately 50% of affected individuals have an abnormal finding at
birth, including clubfoot, clinodactyly, or (rarely) cystic ear swelling.
explanation: >-
GeneReviews documents clubfoot as a congenital finding in roughly half of
SLC26A2-related MED cases.
diagnosis:
- name: Clinical and Radiographic Recognition
description: >-
MED should be considered in children with joint pain, difficulty walking,
waddling gait, joint deformities, or myopathy-like findings, especially when
radiographs show flat, small, and irregularly shaped epiphyses in the hips
and knees. A comprehensive skeletal survey helps identify the multi-joint
epiphyseal pattern needed to distinguish MED from isolated hip disease.
diagnosis_term:
preferred_term: clinical imaging procedure
term:
id: MAXO:0000005
label: clinical imaging procedure
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Multiple epiphyseal dysplasias are relatively common skeletal disorders,
and diagnosing children can often be challenging due to various presenting
complaints, including joint pain, short stature, waddling gait, joint
deformities, and myopathy findings.
explanation: >-
The recent pediatric cohort defines the clinical presentations that should
prompt diagnostic consideration of MED.
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Radiographs are characterized by flat, small, and irregularly shaped
epiphyses, especially in the hips and knees.
explanation: >-
Identifies the core radiographic pattern used to recognize MED.
- name: Molecular Confirmation and Subtype Assignment
description: >-
Molecular testing confirms MED and assigns subtype: heterozygous variants in
COMP, MATN3, COL9A1, COL9A2, or COL9A3 support autosomal dominant MED, while
biallelic SLC26A2 variants support recessive MED. Broader sequencing is
appropriate when presentation is atypical or targeted testing is negative.
diagnosis_term:
preferred_term: molecular genetic testing
term:
id: MAXO:0000533
label: molecular genetic testing
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The diagnosis of autosomal dominant MED is established in a proband with
typical clinical and radiographic findings and/or a heterozygous
pathogenic variant in COL9A1, COL9A2, COL9A3, COMP, or MATN3 identified by
molecular genetic testing.
explanation: >-
GeneReviews gives the diagnostic rule for the autosomal dominant MED genes.
- reference: PMID:20301483
reference_title: "SLC26A2-Related Multiple Epiphyseal Dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Diagnosis of SLC26A2-MED is based on detection of biallelic variants in
SLC26A2 by molecular genetic testing in an individual with compatible
clinical and radiographic findings.
explanation: >-
GeneReviews gives the molecular diagnostic rule for recessive
SLC26A2-related MED.
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
A comprehensive skeletal survey and genetic tests are essential for the
accurate diagnosis and management of this condition.
explanation: >-
The pediatric cohort supports pairing skeletal survey findings with
genetic testing for accurate diagnosis and management.
- name: Perthes-Like Presentation Differential
description: >-
MED can be overlooked when hip pain and radiographs resemble Perthes
disease. Multi-site epiphyseal involvement and molecular testing help
separate MED from isolated Perthes-like hip disease and guide counseling
for the assigned MED subtype.
diagnosis_term:
preferred_term: clinical imaging procedure
term:
id: MAXO:0000005
label: clinical imaging procedure
evidence:
- reference: PMID:40392407
reference_title: "Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
This condition should be considered when evaluating patients who
experience joint pain and have radiographic findings suggestive of Perthes
disease.
explanation: >-
The cohort explicitly warns that MED should be considered in patients with
joint pain and Perthes-like radiographic findings.
treatments:
- name: Analgesics and Anti-Inflammatory Medication
description: >
Pain control combines analgesics with physiotherapy. Nonsteroidal
anti-inflammatory drugs are used cautiously, particularly for chronic joint
pain and osteoarthritis-related symptoms.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: nonsteroidal anti-inflammatory drug
term:
id: NCIT:C257
label: Nonsteroidal Antiinflammatory Drug
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
For pain control, a combination of analgesics and physiotherapy including
hydrotherapy
explanation: >-
GeneReviews recommends analgesics for pain control in MED.
- reference: PMID:20301483
reference_title: "SLC26A2-Related Multiple Epiphyseal Dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
cautious use of analgesic medications such as nonsteroidal
anti-inflammatory drugs
explanation: >-
GeneReviews recommends cautious use of NSAIDs in SLC26A2-related MED.
- name: Physiotherapy
description: >
Physiotherapy, including hydrotherapy, is used for pain control, muscular
strengthening, and maintaining joint mobility, and may help delay joint
contractures.
treatment_term:
preferred_term: physical therapy
term:
id: MAXO:0000011
label: physical therapy
evidence:
- reference: PMID:20301483
reference_title: "SLC26A2-Related Multiple Epiphyseal Dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Physiotherapy for muscular strengthening and maintaining mobility
explanation: >-
GeneReviews recommends physiotherapy for muscular strengthening and
mobility in MED.
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
For pain control, a combination of analgesics and physiotherapy including
hydrotherapy
explanation: >-
GeneReviews recommends physiotherapy including hydrotherapy for pain
control in MED.
- name: Orthopedic Surgery
description: >
Orthopedic procedures include realignment and/or acetabular osteotomy to
limit joint destruction and delay osteoarthritis, and total joint
arthroplasty for end-stage degenerative hip changes causing uncontrollable
pain or dysfunction. Joint-preserving Bernese periacetabular osteotomy has
shown favorable short-term radiographic and functional outcomes for hip
disease in MED.
treatment_term:
preferred_term: orthopedic surgical procedure
term:
id: NCIT:C16186
label: Orthopedic Surgical Procedure
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
consideration of realignment osteotomy and/or acetabular osteotomy to
limit joint destruction and development of osteoarthritis. Consider total
joint arthroplasty if the degenerative hip changes cause uncontrollable
pain/dysfunction.
explanation: >-
GeneReviews documents realignment/acetabular osteotomy and arthroplasty in
MED management.
- reference: PMID:37904148
reference_title: "The favorable outcome of Bernese periacetabular osteotomy for the hip osteoarthritis in multiple epiphyseal dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Bernese PAO is a feasible treatment for hip disorders in MED patients. It
reshapes acetabular and femoral morphology efficiently.
explanation: >-
Surgical series supports periacetabular osteotomy as a joint-preserving
treatment for MED hip disease.
- name: Genetic Counseling
description: >
Genetic counseling addresses inheritance (autosomal dominant or recessive
depending on the gene), recurrence risk, and the availability of carrier,
prenatal, and preimplantation genetic testing once the family variant is
known.
treatment_term:
preferred_term: Genetic Counseling
term:
id: NCIT:C15240
label: Genetic Counseling
evidence:
- reference: PMID:20301483
reference_title: "SLC26A2-Related Multiple Epiphyseal Dysplasia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Once the SLC26A2 pathogenic variants have been identified in an affected
family member, carrier testing for at-risk relatives and
prenatal/preimplantation genetic testing are possible.
explanation: >-
GeneReviews documents the role of genetic counseling and family-based
testing in SLC26A2-related MED.
- name: Activity Modification and Weight Management
description: >
Conservative supportive care includes avoiding obesity and avoiding exercise
that causes repetitive strain on affected weight-bearing joints, in order to
reduce mechanical load and slow progression of secondary osteoarthritis.
treatment_term:
preferred_term: physical activity avoidance recommendation
term:
id: MAXO:0000049
label: physical activity avoidance recommendation
evidence:
- reference: PMID:20301302
reference_title: "Multiple Epiphyseal Dysplasia, Autosomal Dominant."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Agents/circumstances to avoid: Obesity; exercise causing repetitive strain
on affected joints.
explanation: >-
GeneReviews recommends avoiding obesity and joint-straining exercise as
conservative management in autosomal dominant MED.
datasets: []
References & Deep Research
References
2Deep Research
1Question: You are an expert researcher providing comprehensive, well-cited information.
Provide detailed information focusing on: 1. Key concepts and definitions with current understanding 2. Recent developments and latest research (prioritize 2023-2024 sources) 3. Current applications and real-world implementations 4. Expert opinions and analysis from authoritative sources 5. Relevant statistics and data from recent studies
Format as a comprehensive research report with proper citations. Include URLs and publication dates where available. Always prioritize recent, authoritative sources and provide specific citations for all major claims.
Disease Characteristics Research Template
Target Disease
- Disease Name: Multiple Epiphyseal Dysplasia
- MONDO ID: (if available)
- Category: Mendelian
Research Objectives
Please provide a comprehensive research report on Multiple Epiphyseal Dysplasia covering all of the disease characteristics listed below. This report will be used to populate a disease knowledge base entry. Be thorough and cite primary literature (PMID preferred) for all claims.
For each section, suggested databases/resources are listed. These are the first places you should search for information on each topic.
1. Disease Information
Search first: OMIM, Orphanet, ICD-10/ICD-11, MeSH, PubMed
- What is the disease? Provide a concise overview.
- What are the key identifiers? (OMIM, Orphanet, ICD-10/ICD-11, MeSH, Mondo)
- What are the common synonyms and alternative names?
- Is the information derived from individual patients (e.g., EHR) or aggregated disease-level resources?
2. Etiology
- Disease Causal Factors: What are the primary causes? (genetic, environmental, infectious, mechanistic)
- Risk Factors:
Search first: PubMed, Cochrane Library, UpToDate, clinical guidelines, ClinVar, ClinGen, GWAS Catalog, PheGenI, CTD, CDC, WHO, epidemiological databases
- Genetic risk factors (causal variants, susceptibility loci, modifier genes)
- Environmental risk factors (toxins, lifestyle, occupational exposures, age, sex, family history)
- Protective Factors:
Search first: PubMed, Cochrane Library, clinical trial databases, GWAS Catalog, gnomAD, WHO, CDC, nutrition databases
- Genetic protective factors (protective variants, modifier alleles)
- Environmental protective factors (diet, lifestyle, exposures that reduce risk)
- Gene-Environment Interactions: How do genetic and environmental factors interact to influence disease?
Search first: CTD, PubMed, PheGenI, GxE databases
3. Phenotypes
Search first: HPO (Human Phenotype Ontology), OMIM, Orphanet, PubMed, clinicaltrials.gov, MedDRA, SNOMED CT, DECIPHER, LOINC
For each phenotype, provide: - Phenotype type: symptoms, clinical signs, physical manifestations, behavioral changes, or laboratory abnormalities
For symptoms/signs: HPO, OMIM, Orphanet, PubMed For behavioral changes: HPO, DSM, RDoC (Research Domain Criteria), PubMed For laboratory abnormalities: LOINC, SNOMED CT, LabTests Online, PubMed - Phenotype characteristics: Search first: OMIM, Orphanet, HPO, PubMed - Age of symptom onset (neonatal, childhood, adult-onset, late-onset) - Symptom severity (mild, moderate, severe, variable) - Symptom progression (stable, progressive, episodic, fluctuating) - Frequency among affected individuals (percentage or qualitative) - Quality of life impact: Effects on daily functioning and well-being (per-phenotype when possible) Search first: EQ-5D database, SF-36, WHO QOL databases, PubMed - Suggest HPO (Human Phenotype Ontology) terms for each phenotype
4. Genetic/Molecular Information
- Causal Genes: Gene mutations or chromosomal abnormalities responsible for disease (gene symbols, OMIM IDs)
Search first: OMIM, ClinVar, HGMD, Ensembl, NCBI Gene
- Pathogenic Variants:
- Affected genes (gene symbols, HGNC IDs) > Search first: OMIM, NCBI Gene, Ensembl, HGNC, UniProt, GeneCards
- Variant classification (pathogenic, likely pathogenic, VUS per ACMG/AMP guidelines) > Search first: ClinVar, ClinGen, ACMG/AMP guidelines, VarSome
- Variant type/class (missense, frameshift, nonsense, splice-site, structural)
- Allele frequency in population databases > Search first: gnomAD, 1000 Genomes, ExAC, TOPMed, dbSNP
- Somatic vs germline origin > Search first: COSMIC (somatic), ClinVar, ICGC, TCGA
- Functional consequences (loss of function, gain of function, dominant negative)
- Modifier Genes: Genes that modify disease severity or expression
- Epigenetic Information: DNA methylation, histone modifications, chromatin changes affecting disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Chromosomal Abnormalities: Large-scale genetic changes (aneuploidy, translocations, inversions)
Search first: DECIPHER, ClinVar, ECARUCA, UCSC Genome Browser
5. Environmental Information
- Environmental Factors: Non-genetic contributing factors (toxins, radiation, pollution, occupational exposure)
Search first: CTD (Comparative Toxicogenomics Database), TOXNET, PubMed, EPA databases
- Lifestyle Factors: Behavioral factors (smoking, diet, exercise, alcohol consumption)
Search first: CDC databases, WHO, PubMed, NHANES
- Infectious Agents: If applicable, pathogens causing or triggering disease (bacteria, viruses, fungi, parasites)
Search first: NCBI Taxonomy, ViPR, BV-BRC, MicrobeDB, GIDEON
6. Mechanism / Pathophysiology
- Molecular Pathways: Specific signaling cascades or biochemical pathways involved (Wnt, MAPK, mTOR, PI3K-AKT, etc.)
Search first: KEGG, Reactome, WikiPathways, PathBank, BioCyc
- Cellular Processes: Cell-level mechanisms (apoptosis, autophagy, cell cycle dysregulation, inflammation, etc.)
Search first: Gene Ontology (GO), Reactome, KEGG, PubMed
- Protein Dysfunction: How protein structure or function is altered (misfolding, aggregation, loss of function, gain of function)
Search first: UniProt, PDB (Protein Data Bank), InterPro, Pfam, AlphaFold
- Metabolic Changes: Alterations in metabolic processes (energy metabolism, lipid metabolism, amino acid metabolism)
Search first: KEGG, BioCyc, HMDB (Human Metabolome Database), BRENDA
- Immune System Involvement: Role of immune response (autoimmunity, immunodeficiency, chronic inflammation)
Search first: ImmPort, Immunome Database, IEDB, Gene Ontology
- Tissue Damage Mechanisms: How tissues/ are injured (oxidative stress, ischemia, fibrosis, necrosis)
Search first: PubMed, Gene Ontology, Reactome
- Biochemical Abnormalities: Specific molecular defects (enzyme deficiencies, receptor dysfunction, ion channel defects)
Search first: BRENDA, UniProt, KEGG, OMIM, PubMed
- Epigenetic Changes: DNA methylation, histone modifications affecting gene expression in disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Molecular Profiling (if available):
- Transcriptomics/gene expression changes > Search first: GEO (Gene Expression Omnibus), ArrayExpress, GTEx, Human Cell Atlas, SRA
- Proteomics findings > Search first: PRIDE, ProteomeXchange, Human Protein Atlas, STRING, BioGRID
- Metabolomics signatures > Search first: MetaboLights, Metabolomics Workbench, HMDB, METLIN
- Lipidomics alterations > Search first: LIPID MAPS, SwissLipids, LipidHome, Metabolomics Workbench
- Genomic structural features > Search first: UCSC Genome Browser, Ensembl, NCBI, dbVar, DGV
- Advanced Technologies (if applicable):
- Single-cell analysis findings (cell-type specific mechanisms, cellular heterogeneity) > Search first: Human Cell Atlas, Single Cell Portal, GEO, CELLxGENE
- Spatial transcriptomics findings > Search first: GEO, Spatial Research, Vizgen, 10x Genomics data
- Multi-omics integration results > Search first: TCGA, ICGC, cBioPortal, LinkedOmics, PubMed
- Functional genomics screens (CRISPR, RNAi) > Search first: DepMap, GenomeRNAi, PubMed, BioGRID ORCS
For each mechanism, describe: - The causal chain from initial trigger to clinical manifestation - Which mechanisms are upstream vs downstream - What cell types and biological processes are involved - Suggest GO terms for biological processes and CL terms for cell types
7. Anatomical Structures Affected
- Organ Level:
- Primary organs directly affected
- Secondary organ involvement (complications, secondary effects)
- Body systems involved (cardiovascular, nervous, digestive, respiratory, endocrine, etc.)
Search first: Uberon, FMA (Foundational Model of Anatomy), OMIM, HPO, ICD-11, MeSH, SNOMED CT
- Tissue and Cell Level:
- Specific tissue types affected (epithelial, connective, muscle, nervous)
- Specific cell populations targeted (with Cell Ontology terms)
Search first: Uberon, Human Protein Atlas, Cell Ontology, Human Cell Atlas, CellMarker, PanglaoDB
- Subcellular Level:
- Cellular compartments involved (mitochondria, nucleus, ER, lysosomes) (with GO Cellular Component terms)
Search first: Gene Ontology (Cellular Component), UniProt, Human Protein Atlas
- Localization:
- Specific anatomical sites (with UBERON terms) > Search first: FMA, Uberon, NeuroNames (for brain), SNOMED CT
- Lateralization (unilateral, bilateral, asymmetric) > Search first: HPO, clinical literature, imaging databases
8. Temporal Development
- Onset:
- Typical age of onset (congenital, pediatric, adult, geriatric)
- Onset pattern (acute, subacute, chronic, insidious)
Search first: OMIM, Orphanet, HPO, PubMed
- Progression:
- Disease stages (early, intermediate, advanced, end-stage) > Search first: Cancer Staging Manual (AJCC), WHO classifications, PubMed
- Progression rate (rapid, slow, variable)
- Disease course pattern (episodic, relapsing-remitting, progressive, stable)
- Disease duration (self-limited, chronic lifelong)
Search first: Disease registries, longitudinal cohort databases, natural history studies, PubMed, Orphanet, OMIM
- Patterns:
- Remission patterns (spontaneous, treatment-induced) > Search first: Clinical trial databases, disease registries, PubMed
- Critical periods (time windows of vulnerability or opportunity for intervention) > Search first: PubMed, developmental biology databases, clinical guidelines
9. Inheritance and Population
- Epidemiology:
- Prevalence (cases per 100,000 at given time)
- Incidence (new cases per 100,000 per year)
Search first: Orphanet, CDC, WHO, GBD (Global Burden of Disease), national registries, SEER, disease registries
- For Genetic Etiology:
- Inheritance pattern (AD, AR, X-linked, mitochondrial, multifactorial, polygenic) > Search first: OMIM, Orphanet, ClinVar, GTR (Genetic Testing Registry)
- Penetrance (complete, incomplete, age-dependent) > Search first: ClinVar, OMIM, PubMed, ClinGen
- Expressivity (variable, consistent) > Search first: OMIM, ClinVar, PubMed
- Genetic anticipation (increasing severity in successive generations) > Search first: OMIM, PubMed (especially for repeat expansion disorders)
- Germline mosaicism > Search first: ClinVar, OMIM, genetic counseling literature, PubMed
- Founder effects (population-specific mutations) > Search first: gnomAD, population genetics databases, PubMed
- Consanguinity role > Search first: OMIM, population studies, genetic counseling resources
- Carrier frequency > Search first: gnomAD, carrier screening databases, GeneReviews, GTR
- Population Demographics:
- Affected populations (ethnic or demographic groups with higher prevalence) > Search first: gnomAD, 1000 Genomes, PAGE Study, PubMed, population registries
- Geographic distribution (endemic areas, regional variation) > Search first: WHO, CDC, GBD, Orphanet, geographic epidemiology databases
- Geographic distribution of specific variants
- Sex ratio (male:female) > Search first: Disease registries, OMIM, PubMed, epidemiological databases
- Age distribution of affected individuals > Search first: CDC, disease registries, SEER, Orphanet
10. Diagnostics
- Clinical Tests:
- Laboratory tests (blood, urine, tissue chemistry, specific enzyme assays) > Search first: LOINC, LabTests Online, PubMed
- Biomarkers (proteins, metabolites, genetic markers, circulating biomarkers) > Search first: FDA Biomarker List, BEST (Biomarkers, EndpointS, and other Tools), PubMed
- Imaging studies (X-ray, CT, MRI, PET, ultrasound) > Search first: RadLex, DICOM, Radiopaedia, imaging databases
- Functional tests (pulmonary function, cardiac stress tests) > Search first: LOINC, clinical guidelines, PubMed
- Electrophysiology (EEG, EMG, ECG, nerve conduction studies) > Search first: LOINC, clinical neurophysiology databases, PubMed
- Biopsy findings (histopathology, immunohistochemistry) > Search first: SNOMED CT, College of American Pathologists resources, PubMed
- Pathology findings (microscopic examination) > Search first: SNOMED CT, Digital Pathology databases, PubMed
- Genetic Testing:
Search first: GTR (Genetic Testing Registry), GeneReviews, ClinGen
- Overview of recommended genetic testing approach
- Whole genome sequencing (WGS) utility > Search first: GTR, ClinVar, GEL (Genomics England), gnomAD
- Whole exome sequencing (WES) utility > Search first: GTR, ClinVar, OMIM, GeneMatcher
- Gene panels (which panels, which genes) > Search first: GTR, ClinVar, laboratory-specific databases
- Single gene testing > Search first: GTR, ClinVar, OMIM, GeneReviews
- Chromosomal microarray (CMA) > Search first: DECIPHER, ClinVar, dbVar, ECARUCA
- Karyotyping > Search first: Chromosome Abnormality Database, ClinVar, cytogenetics resources
- FISH > Search first: ClinVar, cytogenetics databases, PubMed
- Mitochondrial DNA testing > Search first: MITOMAP, MSeqDR, ClinVar, GTR
- Repeat expansion testing > Search first: GTR, ClinVar, repeat expansion databases, PubMed
- Omics-Based Diagnostics (if applicable):
- RNA sequencing / transcriptomics > Search first: GEO, ArrayExpress, GTEx, RNA-seq databases
- Proteomics > Search first: PRIDE, ProteomeXchange, FDA Biomarker database
- Metabolomics > Search first: MetaboLights, Metabolomics Workbench, HMDB
- Epigenomics > Search first: GEO, ENCODE, Roadmap Epigenomics, MethBase
- Liquid biopsy > Search first: COSMIC, ClinVar, liquid biopsy databases, PubMed
- Clinical Criteria:
- Standardized diagnostic criteria (DSM, ICD, society guidelines) > Search first: DSM-5, ICD-11, clinical society guidelines, UpToDate
- Differential diagnosis (other conditions to rule out, with distinguishing features) > Search first: DynaMed, UpToDate, clinical decision support systems
- Screening:
- Screening methods for asymptomatic individuals (newborn screening, carrier screening, cascade screening) > Search first: ACMG recommendations, CDC newborn screening, GTR
11. Outcome/Prognosis
- Survival and Mortality:
- Survival rate (5-year, 10-year, overall) > Search first: SEER, cancer registries, disease-specific registries, PubMed
- Life expectancy (with and without treatment if applicable) > Search first: Orphanet, disease registries, actuarial databases, PubMed
- Mortality rate > Search first: CDC, WHO, GBD, national mortality databases
- Disease-specific mortality (deaths directly attributable to disease) > Search first: Disease registries, CDC Wonder, GBD, PubMed
- Morbidity and Function:
- Morbidity (disease-related disability and health impacts) > Search first: GBD, WHO, disability databases, PubMed
- Disability outcomes (long-term functional impairments) > Search first: ICF (International Classification of Functioning), disability registries
- Quality of life measures (EQ-5D, SF-36, PROMIS, disease-specific tools) > Search first: EQ-5D database, SF-36, PROMIS, PubMed
- Disease Course:
- Complications (secondary problems: infections, organ failure, etc.) > Search first: ICD codes, disease registries, clinical databases, PubMed
- Recovery potential (likelihood and extent of recovery, with vs without treatment) > Search first: Natural history studies, rehabilitation databases, PubMed
- Prediction:
- Prognostic factors (age, disease severity, biomarkers, treatment response) > Search first: Prognostic models databases, clinical calculators, PubMed
- Prognostic biomarkers (molecular markers predicting disease course) > Search first: FDA Biomarker database, PubMed, cancer prognostic databases
12. Treatment
- Pharmacotherapy:
- Pharmacological treatments (drug names, drug classes, mechanisms of action) > Search first: DrugBank, RxNorm, ATC classification, DailyMed, FDA databases
- Pharmacogenomics (how genetic variants affect drug metabolism, efficacy, toxicity) > Search first: PharmGKB, CPIC (Clinical Pharmacogenetics), FDA Table of PGx Biomarkers
- Advanced Therapeutics:
- Gene therapy (viral vectors, CRISPR, gene replacement, gene editing) > Search first: ClinicalTrials.gov, FDA gene therapy database, ASGCT resources
- Cell therapy (stem cell transplant, CAR-T, cellular therapeutics) > Search first: ClinicalTrials.gov, FDA cell therapy database, FACT standards
- RNA-based therapies (ASOs, siRNA, mRNA therapies) > Search first: ClinicalTrials.gov, FDA approvals, PubMed
- Targeted therapies (treatments directed at specific molecular targets) > Search first: My Cancer Genome, OncoKB, ClinicalTrials.gov, FDA approvals
- Immunotherapies (checkpoint inhibitors, monoclonal antibodies) > Search first: Cancer Immunotherapy Database, FDA approvals, ClinicalTrials.gov
- Surgical and Interventional:
- Surgical interventions (types of surgery, timing, outcomes) > Search first: CPT codes, surgical registries, clinical guidelines, PubMed
- Supportive and Rehabilitative:
- Supportive care (symptom management, pain control, nutrition) > Search first: Clinical guidelines, Cochrane Library, PubMed
- Rehabilitation (physical therapy, occupational therapy, speech therapy) > Search first: Rehabilitation medicine databases, clinical guidelines, PubMed
- Experimental:
- Experimental treatments in clinical trials (with NCT identifiers if available) > Search first: ClinicalTrials.gov, EU Clinical Trials Register, WHO ICTRP
- Treatment Outcomes:
- Treatment response rates > Search first: Clinical trial databases, FDA reviews, systematic reviews, PubMed
- Side effects and adverse events > Search first: FDA Adverse Event Reporting System (FAERS), MedWatch, PubMed
- Treatment Strategy:
- Treatment algorithms (clinical pathways, decision trees) > Search first: Clinical practice guidelines, NCCN Guidelines, UpToDate
- Combination therapies > Search first: ClinicalTrials.gov, treatment guidelines, PubMed
- Personalized medicine approaches (genotype-guided treatment) > Search first: My Cancer Genome, CIViC, PharmGKB, precision medicine databases
For each treatment, suggest MAXO (Medical Action Ontology) terms where applicable.
13. Prevention
- Prevention Levels:
- Primary prevention (preventing disease occurrence: vaccination, risk factor modification) > Search first: CDC, WHO, USPSTF recommendations, Cochrane Library
- Secondary prevention (early detection and treatment: screening programs, early intervention) > Search first: USPSTF, CDC screening guidelines, WHO
- Tertiary prevention (preventing complications in those with disease) > Search first: Clinical guidelines, disease management protocols, PubMed
- Immunization: Vaccine strategies (if applicable)
Search first: CDC vaccine schedules, WHO immunization, FDA vaccine database
- Screening and Early Detection:
- Screening programs (population-based: newborn screening, cancer screening) > Search first: CDC screening programs, USPSTF, cancer screening databases
- Genetic screening (carrier screening, preimplantation genetic diagnosis, prenatal testing) > Search first: ACMG recommendations, ACOG guidelines, GTR
- Risk stratification (identifying high-risk individuals for targeted prevention) > Search first: Risk prediction models, clinical calculators, PubMed
- Behavioral Interventions: Lifestyle modifications to reduce risk
Search first: CDC, WHO, behavioral intervention databases, Cochrane Library
- Counseling: Genetic counseling (risk assessment, family planning guidance)
Search first: NSGC resources, ACMG guidelines, GeneReviews
- Public Health:
- Public health interventions (sanitation, vector control, health education) > Search first: CDC, WHO, public health databases, PubMed
- Environmental interventions (reducing environmental risk factors) > Search first: EPA databases, WHO environmental health, PubMed
- Prophylaxis: Preventive medications or procedures
Search first: Clinical guidelines, FDA approvals, PubMed
14. Other Species / Natural Disease
- Taxonomy: Species affected (with NCBI Taxon identifiers)
Search first: NCBI Taxonomy
- Breed: Specific breeds affected (with VBO identifiers if applicable)
Search first: VBO (Vertebrate Breed Ontology)
- Gene: Orthologous genes in other species (with NCBI Gene IDs)
Search first: NCBI Gene
- Natural Disease:
- Naturally occurring disease in other species (companion animals, wildlife) > Search first: OMIA (Online Mendelian Inheritance in Animals), VetCompass, PubMed
- Veterinary relevance and importance in animal health > Search first: OMIA, veterinary databases, PubMed
- Comparative Biology:
- Comparative pathology (similarities and differences across species) > Search first: OMIA, comparative pathology databases, PubMed
- Evolutionary conservation of disease mechanisms > Search first: HomoloGene, OrthoMCL, Alliance of Genome Resources
- Transmission (if applicable):
- Zoonotic potential > Search first: CDC zoonotic diseases, WHO zoonoses, GIDEON
- Cross-species susceptibility > Search first: NCBI Taxonomy, veterinary databases, PubMed
15. Model Organisms
- Model Types:
- Model organism type (mammalian, invertebrate, cellular, in vitro) > Search first: Alliance of Genome Resources, model organism databases
- Specific model systems (mouse, rat, zebrafish, Drosophila, C. elegans, yeast, cell lines, organoids, iPSCs) > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, SGD, ATCC, Cellosaurus
- Induced models (drug treatment, surgical intervention, environmental manipulation) > Search first: MGI, model organism databases, PubMed
- Genetic Models:
- Types available (knockout, knock-in, transgenic, conditional, humanized) > Search first: MGI, IMPC, KOMP, EuMMCR, IMSR
- Model Characteristics:
- Phenotype recapitulation (how well model reproduces human disease features) > Search first: Model organism databases, comparative studies, PubMed
- Model limitations (aspects of human disease not captured) > Search first: Model organism databases, PubMed, review articles
- Applications:
- Research applications (what aspects of disease can be studied) > Search first: Model organism databases, PubMed
- Resources:
- Model databases > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, IMSR, EMMA, MMRRC
Citation Requirements
- Cite primary literature (PMID preferred) for all mechanistic and clinical claims
- Prioritize recent reviews and landmark papers
- Include direct quotes from abstracts where possible to support key statements
- Distinguish evidence source types: human clinical, model organism, in vitro, computational
Output Format
Structure your response as a comprehensive narrative organized by the sections above. For each section, provide: - Factual content with specific details (numbers, percentages, gene names, variant nomenclature) - Ontology term suggestions (HPO, GO, CL, UBERON, CHEBI, MAXO, MONDO) where applicable - Evidence citations with PMIDs - Direct quotes from abstracts to support key claims - Clear indication when information is not available or not applicable for this disease
This report will be used to populate a disease knowledge base entry with: - Pathophysiology descriptions with causal chains - Gene/protein annotations (HGNC, GO terms) - Phenotype associations (HP terms) with frequencies - Cell type involvement (CL terms) - Anatomical locations (UBERON terms) - Chemical entities (CHEBI terms) - Treatment annotations (MAXO terms) - Evidence items with PMIDs and exact abstract quotes - Epidemiology, prognosis, diagnostic, and prevention information - Animal model descriptions with phenotype recapitulation details
Multiple Epiphyseal Dysplasia (MED) — Comprehensive Disease Characteristics Report
Executive summary
Multiple epiphyseal dysplasia (MED) is a genetically heterogeneous skeletal dysplasia characterized by abnormal development and ossification of multiple epiphyses, typically presenting in childhood with joint pain, gait disturbance, and variable short stature, and progressing to early-onset osteoarthritis (OA) of large weight-bearing joints. The best-supported causal genes in the retrieved evidence are COMP, MATN3, COL9A1, COL9A2, COL9A3 (usually autosomal dominant) and SLC26A2 and CANT1 (autosomal recessive), with COMP-related MED representing the most common subtype in a recent longitudinal single-center cohort. Recent 2023–2024 work adds (i) mechanistic functional data for SLC26A2 MED-4 in human primary chondrocytes and (ii) expansion of COMP-MED phenotype to include multiple osteochondritis dissecans (OCD) in a 2024 case report. (dasar2025recognizingmultipleepiphyseal pages 1-2, li2024biallelicvariantsin pages 1-2, mazzotti2024multipleosteochondritisdissecans pages 7-8)
Evidence limitations relevant to knowledge-base curation: within the retrieved corpus, curated identifiers (MONDO, Orphanet ORPHAcode, MeSH, ICD-10/11) and PMID-specific citation metadata were not directly available; consequently, this report provides DOI/URLs and publication dates where available and explicitly flags gaps. (dasar2025recognizingmultipleepiphyseal pages 1-2, unger2023nosologyofgenetic pages 6-8)
1. Disease information
1.1 Overview / definition (current understanding)
MED is described as a clinically and genetically heterogeneous skeletal disorder affecting epiphyseal development, typically manifesting in early childhood with joint pain and stiffness, walking difficulty/waddling gait, deformities, and later degenerative joint disease/early OA; radiographs show delayed epiphyseal ossification with flat/small/irregular epiphyses, particularly in hips and knees. (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 2-4)
1.2 Key identifiers (available from retrieved evidence)
- MED-4 (SLC26A2-related): MIM 226900 (autosomal recessive). (li2024biallelicvariantsin pages 1-2, dasar2025recognizingmultipleepiphyseal pages 1-2)
- MED-7 (CANT1-related): OMIM 617719 (autosomal recessive). (dasar2025recognizingmultipleepiphyseal pages 1-2)
- Nosology context: the 2023 revision of the Nosology of Genetic Skeletal Disorders uses dyadic (gene-linked) naming and reports expansion to 771 disorders and 552 genes (useful for differential diagnosis and NGS interpretation). (unger2023nosologyofgenetic pages 6-8)
Not retrievable from the provided texts: MONDO ID, Orphanet ORPHAcode, ICD-10/ICD-11 codes, and MeSH ID for MED.
1.3 Synonyms / alternative names (from retrieved evidence)
- “Multiple epiphyseal dysplasias” (plural usage for the genetically heterogeneous group). (dasar2025recognizingmultipleepiphyseal pages 1-2)
- “EDM1” used for COMP-related disease in the COMP spectrum (noted in the context of COMP-related skeletal diseases). (dikova2024multipleepiphysealdysplasia pages 5-10)
1.4 Evidence source type
The current report relies primarily on: * Human clinical cohort data (single-center, 20-year experience). (dasar2025recognizingmultipleepiphyseal pages 1-2) * Human case reports expanding phenotype. (mazzotti2024multipleosteochondritisdissecans pages 7-8) * Human in vitro functional studies (primary chondrocytes) for SLC26A2 MED-4. (li2024biallelicvariantsin pages 1-2) * Guideline/consensus documents for skeletal dysplasia spinal/craniofacial management (not MED-specific but applicable). (white2020bestpracticeguidelines pages 2-4, savarirayan2021bestpracticeguidelines pages 1-2)
2. Etiology
2.1 Disease causal factors
MED in the retrieved literature is overwhelmingly described as genetic (Mendelian), caused by pathogenic variants in genes encoding cartilage extracellular matrix proteins and a sulfate transporter. (dasar2025recognizingmultipleepiphyseal pages 1-2, li2024biallelicvariantsin pages 1-2)
2.2 Risk factors
- Genetic: variants in MED genes (COMP, MATN3, COL9A1/2/3, SLC26A2, CANT1). (dasar2025recognizingmultipleepiphyseal pages 1-2, li2024biallelicvariantsin pages 1-2)
- Environmental / infectious: no specific environmental or infectious etiologic triggers were identified in retrieved MED sources.
2.3 Protective factors
No validated protective genetic or environmental factors were identified in the retrieved evidence.
2.4 Gene–environment interactions
No specific gene–environment interactions were identified in retrieved evidence.
3. Phenotypes
A phenotype-to-HPO mapping table is provided below.
| Feature | Suggested HPO term | Notes (age of onset / progression) | Frequency (if known) | Citations |
|---|---|---|---|---|
| Joint pain / arthralgia | Arthralgia (HP:0002829) | Often first recognized in early childhood; progressive and associated with later degenerative joint disease/early osteoarthritis | 17/25 (68%) in Daşar 2025 cohort | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 2-4) |
| Short stature / mildly reduced adult height | Short stature (HP:0004322) | Frequently mild or absent at birth; may become apparent in childhood; adult height often near-normal or mildly reduced | 9/25 (36%) in Daşar 2025 cohort | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 5-7, dasar2025recognizingmultipleepiphyseal pages 2-4) |
| Walking difficulty / abnormal gait | Abnormality of gait (HP:0001288) | Early-childhood presentation; often linked to hip/knee pain, deformity, or myopathy-like findings; may progress with joint degeneration | Not quantified in retrieved cohort text | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 5-7, dasar2025recognizingmultipleepiphyseal pages 2-4) |
| Waddling gait | Waddling gait (HP:0002515) | Reported in childhood and adolescence; reflects proximal lower-limb weakness/deformity and hip disease | Not quantified in retrieved cohort text | (dikova2024multipleepiphysealdysplasia pages 1-5, dasar2025recognizingmultipleepiphyseal pages 1-2) |
| Myopathy-like features / muscle weakness | Proximal muscle weakness (HP:0003701) | May be an early presenting complaint and can mimic neuromuscular disease; contributes to diagnostic delay | Not quantified in retrieved cohort text | (dasar2025recognizingmultipleepiphyseal pages 5-7, dasar2025recognizingmultipleepiphyseal pages 2-4) |
| Hypotonia | Hypotonia (HP:0001252) | Can be present in infancy/early childhood; associated with delayed walking and joint laxity in some cases | Not quantified in retrieved cohort text | (dikova2024multipleepiphysealdysplasia pages 5-10) |
| Epiphyseal irregularity / generalized epiphyseal dysplasia | Irregular epiphyses (HP:0003090) | Core radiographic hallmark; detected in childhood; involves hips and knees prominently and persists/progresses with growth | Not quantified in retrieved cohort text | (dasar2025recognizingmultipleepiphyseal pages 1-2, dikova2024multipleepiphysealdysplasia pages 1-5, dasar2025recognizingmultipleepiphyseal pages 4-5) |
| Flattened epiphyses | Flattened epiphysis (HP:0003100) | Seen on childhood radiographs; small, flat, irregular epiphyses are classic MED findings | Not quantified in retrieved cohort text | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 4-5) |
| Delayed epiphyseal/carpal ossification | Delayed ossification of epiphyses (HP:0003093) | Childhood radiographic feature; may include delayed carpal ossification and altered bone age | Not quantified in retrieved cohort text | (dikova2024multipleepiphysealdysplasia pages 1-5, dikova2024multipleepiphysealdysplasia pages 5-10, dasar2025recognizingmultipleepiphyseal pages 2-4, dasar2025recognizingmultipleepiphyseal pages 1-2) |
| Acetabular dysplasia | Acetabular dysplasia (HP:0003272) | Common hip manifestation; contributes to pain, gait abnormality, and later hip osteoarthritis; may prompt corrective osteotomy | Not quantified in retrieved cohort text | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 5-7) |
| Coxa vara | Coxa vara (HP:0002812) | Can be recognized in childhood; contributes to gait disturbance and hip dysfunction; may progress | Not quantified in retrieved cohort text | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 5-7, dasar2025recognizingmultipleepiphyseal pages 2-4) |
| Genu valgum | Genu valgum (HP:0002857) | Childhood lower-limb deformity; may require guided growth or osteotomy | Present in surgical subgroup; exact cohort-wide frequency not reported | (dasar2025recognizingmultipleepiphyseal pages 2-4, dasar2025recognizingmultipleepiphyseal pages 5-7) |
| Genu varum | Genu varum (HP:0002974) | Childhood deformity; may coexist with other lower-limb malalignment and progress with growth | Not quantified in retrieved cohort text | (dasar2025recognizingmultipleepiphyseal pages 5-7, dasar2025recognizingmultipleepiphyseal pages 1-2) |
| Early-onset osteoarthritis / degenerative joint disease | Osteoarthritis (HP:0002758) | Progressive complication, often emerging in adolescence or early adulthood and affecting large weight-bearing joints; may lead to arthroplasty | Not quantified in Daşar cohort; MED patients can require joint replacement relatively young | (dasar2025recognizingmultipleepiphyseal pages 1-2, mazzotti2024multipleosteochondritisdissecans pages 7-8, matsushita2021healthrelatedqualityof pages 1-2) |
| Orthopedic surgery requirement | Arthroplasty / corrective osteotomy-related phenotype annotation not directly represented by one HPO term; consider Abnormality of the musculoskeletal system (HP:0033127) plus procedure ontology outside HPO | Marker of severity; reflects progressive deformity/osteoarthritis requiring intervention | 7/25 (28%) in Daşar 2025 cohort | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 2-4) |
| Double-layered / bipartite patella | Bipartite patella (HP:0006485) | Relatively characteristic of SLC26A2-related MED; detected radiographically, often in childhood | ~60% of SLC26A2-related MED in one source | (li2024biallelicvariantsin pages 1-2, dasar2025recognizingmultipleepiphyseal pages 5-7, dasar2025recognizingmultipleepiphyseal pages 4-5) |
| Glacier sign / glacier crevice sign | Radiographic sign; no exact HPO term identified in retrieved evidence, suggested parent term Abnormality of the knee joint (HP:0002815) | Knee imaging sign reported in MED cohorts, particularly useful diagnostically in childhood | Not quantified in retrieved cohort text | (dasar2025recognizingmultipleepiphyseal pages 5-7, dasar2025recognizingmultipleepiphyseal pages 2-4, dasar2025recognizingmultipleepiphyseal pages 4-5) |
| Osteochondritis dissecans | Osteochondritis dissecans (HP:0002759) | Not a classic universal MED feature; reported as a major/expanding manifestation in some COMP- and COL9A2-related cases; may present in adolescence/young adulthood | Rare; no cohort frequency in retrieved MED cohort | (mazzotti2024multipleosteochondritisdissecans pages 7-8, mazzotti2024multipleosteochondritisdissecans pages 5-7) |
| Male sex in reported cohort | Phenotypic sex not an HPO disease feature | Cohort descriptor rather than phenotype; included for knowledge-base completeness | 16/25 (64%) male in Daşar 2025 cohort | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 2-4) |
Table: This table maps major clinical and radiographic features of multiple epiphyseal dysplasia to suggested HPO terms, with onset/progression notes and available cohort frequencies. It is useful for disease knowledge-base curation and phenotype annotation.
3.1 Core clinical phenotype (human)
In a 20-year single-center cohort (27 clinically diagnosed; 25 genetically resolved), key presenting features included joint pain, difficulty walking, variable short stature, and need for orthopedic surgery in a subset. Quantitative cohort data: short stature 9/25 (36%), joint pain 17/25 (68%), and orthopedic surgery 7/25 (28%); the age at genetic diagnosis ranged from 4 to 50 years (median 10), consistent with diagnostic delay and variable expressivity. (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 2-4)
3.2 Radiographic phenotype and named signs
Radiographic hallmarks across sources include delayed ossification and irregular/flattened epiphyses; multiple sources highlight hip and knee prominence. Additional named signs include double-layered/bipartite patella (particularly emphasized for SLC26A2-associated disease) and “glacier”/“glacier crevice” and “harlequin hat” knee signs in a pediatric cohort. (li2024biallelicvariantsin pages 1-2, dasar2025recognizingmultipleepiphyseal pages 2-4, dasar2025recognizingmultipleepiphyseal pages 4-5)
3.3 Quality of life impact
Adult MED/SED cohorts using SF-36 show the physical component summary (PCS) is significantly reduced compared with population norms and tends to worsen with age; in MED, osteoarthritis is associated with lower physical HRQoL. (matsushita2021healthrelatedqualityof pages 1-2, matsushita2021healthrelatedqualityof pages 3-6)
4. Genetic / molecular information
A gene/subtype summary table is provided below.
| MED subtype / label | Gene | Inheritance | Key notes / phenotype pointers | Citations |
|---|---|---|---|---|
| MED type 1 (OMIM 132400); COMP-MED / EDM1 | COMP | AD | Most common MED subtype; reported as up to half of MED cases. In the 2025 cohort, 13/25 patients (52%) and 7/12 families (58.3%) had COMP variants. COMP-associated disease tended to be more severe and accounted for most orthopedic surgeries; radiographically often shows small round epiphyses and dysplastic acetabula. Dikova 2024 also states pathogenic COMP variants account for ~50% of AD MED; de novo COMP variants occur. | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 5-7, dikova2024multipleepiphysealdysplasia pages 5-10) |
| MED type 5 (OMIM 607078) | MATN3 | AD | Established dominant MED gene. In the 2025 cohort, 5/25 patients (20%) and 2/12 families (16.6%) had MATN3 variants. Radiographically associated with flattened epiphyses in the cohort discussion. | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 5-7) |
| MED type 6 (OMIM 614135) | COL9A1 | AD | Listed among dominant MED genes in recent cohort/mechanistic summaries; part of collagen IX–related MED spectrum. Specific cohort frequency not reported in the retrieved evidence. | (dasar2025recognizingmultipleepiphyseal pages 1-2, li2024biallelicvariantsin pages 1-2) |
| MED type 2 (OMIM 600204) | COL9A2 | AD | Listed among dominant MED genes. In the 2025 cohort, 2/25 patients (8%) and 1/12 families (8.3%) had COL9A2 variants. One inherited intronic splice-region variant was noted; COL9A2-related disease may show relatively prominent knee involvement in prior literature. | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 5-7) |
| MED type 3 (OMIM 600969) | COL9A3 | AD | Listed among dominant MED genes in recent sources; no cohort frequency provided in the retrieved evidence. | (dasar2025recognizingmultipleepiphyseal pages 1-2, li2024biallelicvariantsin pages 1-2) |
| MED type 4 / MED-4 (MIM 226900); recessive MED; DTDST-related | SLC26A2 (alias DTDST) | AR | Recessive MED caused by biallelic SLC26A2 variants. In the 2025 cohort, 5/25 patients (20%) and 2/12 families (16.6%) had SLC26A2 variants. Phenotype pointers include double-layered/bipartite patella (reported as relatively specific; ~60% in one source) and glacier sign. Severity across the SLC26A2 spectrum relates partly to residual sulfate-transporter activity, though correlation is not absolute. | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 5-7, li2024biallelicvariantsin pages 1-2, silveira2022slc26a2dtdstspectruma pages 3-4) |
| MED type 7 (OMIM 617719) | CANT1 | AR | Recently described recessive MED subtype due to biallelic CANT1 variants. Cohort source notes MED type 7 may occur without classic Desbuquois features. Frequency not reported in the retrieved MED cohort because no CANT1-positive family was identified there. | (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 2-4) |
| Historical gene list in older reviews/case reports | DTDST | AR | DTDST is an older alias for SLC26A2, not a separate gene. Older MED literature/case reports may list causal genes as COMP, DTDST, MATN3, COL9A1, COL9A2, and COL9A3. | (dikova2024multipleepiphysealdysplasia pages 5-10, li2024biallelicvariantsin pages 9-10) |
Table: This table summarizes the main genes currently implicated in multiple epiphyseal dysplasia, their inheritance patterns, and distinguishing phenotype clues. It also highlights cohort frequencies from Daşar 2025 and the reported ~50% contribution of COMP variants to autosomal dominant MED from Dikova 2024.
4.1 Genetic architecture and inheritance
Across retrieved sources, MED is caused by variants in at least seven genes with both autosomal dominant (COMP, MATN3, COL9A1/2/3) and autosomal recessive (SLC26A2, CANT1) inheritance. (dasar2025recognizingmultipleepiphyseal pages 1-2, li2024biallelicvariantsin pages 1-2)
4.2 Quantitative gene contribution (single-center cohort)
In the 2025 cohort of genetically resolved cases (n=25), gene distribution was: COMP 13/25 (52%), MATN3 5/25 (20%), SLC26A2 5/25 (20%), COL9A2 2/25 (8%); COMP cases were clinically more severe and represented most surgeries (5 of 7 operated patients). (dasar2025recognizingmultipleepiphyseal pages 1-2)
4.3 Pathogenic variant examples (2023–2024)
- SLC26A2 MED-4 family: compound heterozygous c.1020_1022delTGT (p.Val341del) and c.1262T>C (p.Ile421Thr); functional consequences described in primary chondrocytes (see Mechanism). (li2024biallelicvariantsin pages 1-2)
- COMP-MED cases (2024): heterozygous c.1417_1419dupGAC (p.Asp473dup) and c.1754C>G (p.Thr585Arg) described with ClinVar/gnomAD/ACMG-based classification; de novo occurrence reported for p.Thr585Arg. (dikova2024multipleepiphysealdysplasia pages 5-10)
- COMP-MED phenotype expansion (2024): heterozygous c.1586C>A p.(Thr529Asn) associated with multiple OCD as main manifestation in a family (case report). (mazzotti2024multipleosteochondritisdissecans pages 5-7, mazzotti2024multipleosteochondritisdissecans pages 7-8)
4.4 Modifier genes, epigenetics, chromosomal abnormalities
The pediatric cohort notes phenotypic variability may involve intronic variants and modifier genes, but no specific modifier loci or epigenetic signatures were provided in retrieved evidence. (dasar2025recognizingmultipleepiphyseal pages 10-11)
5. Environmental information
No MED-specific environmental toxins, lifestyle etiologic factors, or infectious triggers were supported by retrieved MED evidence. Lifestyle and weight/activity modification appear in management as tertiary prevention of complications rather than primary causal factors. (dikova2024multipleepiphysealdysplasia pages 5-10)
6. Mechanism / pathophysiology
6.1 Mechanistic heterogeneity across genes
MED mechanisms differ by causal gene class (ECM proteins vs transporter), but converge on altered cartilage growth plate homeostasis and joint degeneration.
6.1.1 COMP-related MED
A COMP-MED mechanism summarized in a 2024 case report: mutant COMP misfolding leads to retention in the chondrocyte rough endoplasmic reticulum (rER) with co-retention of ECM proteins (e.g., type IX collagen, aggrecan), producing ER stress and downstream cartilage pathology. The same report contrasts COL9A2-related MED as altering ECM composition without ER stress, supporting gene-specific mechanisms. (mazzotti2024multipleosteochondritisdissecans pages 7-8)
Potential therapeutic concept: the report discusses targeting autophagy to reduce retained protein burden as a mechanistically motivated strategy (not yet demonstrated as clinical therapy in retrieved evidence). (mazzotti2024multipleosteochondritisdissecans pages 7-8)
6.1.2 SLC26A2-related MED-4
SLC26A2 encodes a sulfate transporter; MED-4 reflects disrupted sulfate-dependent cartilage matrix biology. In a 2024 Orphanet Journal of Rare Diseases study, mutant SLC26A2 proteins showed reduced expression and abnormal subcellular localization in primary human chondrocytes, with altered gene expression consistent with disturbed chondrocyte differentiation: ↓MMP13, ↓COL10A1, ↓RUNX2; ↑ACAN, interpreted as promoting proliferation while inhibiting differentiation. (li2024biallelicvariantsin pages 1-2)
Animal model support: a cited Slc26a2−/− mouse model of severe SLC26A2-related dysplasias shows FGFR3 overactivation and impaired extracellular deposition of collagen II and IX with defective cartilage formation. (li2024biallelicvariantsin pages 1-2)
6.2 Suggested ontology terms (mechanism-level)
- GO Biological Process (suggestions): “endoplasmic reticulum stress response,” “protein folding,” “extracellular matrix organization,” “chondrocyte differentiation,” “proteoglycan biosynthetic process,” “collagen fibril organization.” (Mechanistic basis: COMP ER stress and ECM co-retention; SLC26A2 chondrocyte differentiation markers.) (mazzotti2024multipleosteochondritisdissecans pages 7-8, li2024biallelicvariantsin pages 1-2)
- Cell Ontology (CL) (suggestions): chondrocyte (CL:0000138) as primary affected cell type in mechanistic studies. (li2024biallelicvariantsin pages 1-2)
7. Anatomical structures affected
7.1 Organ/system level
Primary involvement is the musculoskeletal system, especially hips and knees (weight-bearing joints). (dasar2025recognizingmultipleepiphyseal pages 1-2)
7.2 Tissue/cell level
Primary tissue: hyaline cartilage / growth plate cartilage; primary cell: chondrocytes. (li2024biallelicvariantsin pages 1-2, mazzotti2024multipleosteochondritisdissecans pages 7-8)
7.3 Suggested anatomical ontology terms
- UBERON (suggestions): “epiphysis,” “hip joint,” “knee joint,” “articular cartilage,” “growth plate.” (Supported by repeated hip/knee epiphyseal emphasis.) (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 2-4)
8. Temporal development
8.1 Onset
MED is commonly normal at birth with early-childhood onset of symptoms (pain, gait difficulty), though diagnosis may be delayed (median age at genetic diagnosis 10 years; range 4–50 years). (dasar2025recognizingmultipleepiphyseal pages 5-7, dasar2025recognizingmultipleepiphyseal pages 2-4)
8.2 Progression
Course is typically progressive, with increasing joint deformity and early OA; some individuals require arthroplasty or joint-preserving osteotomies. (dasar2025recognizingmultipleepiphyseal pages 1-2, matsushita2021healthrelatedqualityof pages 1-2)
9. Inheritance and population
9.1 Epidemiology
A pediatric cohort summary states MED prevalence is >1/10,000, but no registry-derived incidence or country-specific prevalence was retrieved. (dasar2025recognizingmultipleepiphyseal pages 5-7)
9.2 Inheritance
Both autosomal dominant and autosomal recessive forms occur, depending on gene (see Artifact-00). De novo autosomal dominant variants occur (COMP examples). (dasar2025recognizingmultipleepiphyseal pages 1-2, dikova2024multipleepiphysealdysplasia pages 5-10)
9.3 Penetrance/expressivity
Formal penetrance estimates were not retrieved. Evidence supports variable expressivity (broad age at diagnosis; variable need for surgery; subtype severity differences with COMP tending more severe). (dasar2025recognizingmultipleepiphyseal pages 1-2, dasar2025recognizingmultipleepiphyseal pages 2-4)
10. Diagnostics
10.1 Clinical + imaging approach
A practical workflow from the pediatric cohort emphasizes: * Consider MED in children with joint pain, walking difficulty, or myopathy-like findings even without obvious disproportionate short stature. (dasar2025recognizingmultipleepiphyseal pages 2-4) * Perform a comprehensive skeletal survey with radiographs (hands/feet/hips/knees/ankles) to identify delayed ossification, irregular/flattened epiphyses, and characteristic knee/hip signs (“glacier crevice,” “harlequin hat,” and double-layered patella/glacier sign in the cohort tables). (dasar2025recognizingmultipleepiphyseal pages 2-4, dasar2025recognizingmultipleepiphyseal pages 4-5)
10.2 Differential diagnosis
Differentials explicitly noted include Legg–Calvé–Perthes disease, spondyloepiphyseal dysplasia (COL2A-related), congenital hypothyroidism, mucopolysaccharidoses (e.g., IV/VI; urinary GAG testing), and pseudoachondroplasia. (dikova2024multipleepiphysealdysplasia pages 5-10)
10.3 Genetic testing
Real-world implementations across cohort/case report evidence include: * Targeted sequencing of known MED genes (often COMP first) with Sanger confirmation and parental segregation; proceed to WES when targeted testing is negative or phenotype is atypical. (dasar2025recognizingmultipleepiphyseal pages 2-4, dasar2025recognizingmultipleepiphyseal pages 5-7) * Use of broad skeletal dysplasia NGS panels (e.g., 442-gene panel) with ACMG interpretation and Sanger confirmation in complex cases. (mazzotti2024multipleosteochondritisdissecans pages 5-7)
11. Outcome / prognosis
MED is associated with premature osteoarthritis and may cause substantial functional limitation. Adult SF-36 data indicate early deterioration in physical HRQoL with PCS reduction compared with population norms, worsening with age; osteoarthritis is associated with lower PCS in MED patients. (matsushita2021healthrelatedqualityof pages 1-2, matsushita2021healthrelatedqualityof pages 3-6)
Mortality effects and life expectancy were not quantified in the retrieved evidence.
12. Treatment
A management/treatment summary with MAXO suggestions is provided below.
| Intervention / management | Indication / goal | Evidence / outcomes (quantitative when available) | Notes / implementation details | Suggested MAXO term(s) | Citations |
|---|---|---|---|---|---|
| NSAIDs / anti-inflammatory medication | Symptom relief for joint pain and stiffness; reduce pain from early degenerative joint disease | Supportive care is standard in case reports/reviews; quantitative MED-specific response rates were not reported in the retrieved evidence. Dikova 2024 explicitly lists anti-inflammatory drugs as part of management. | Used as part of conservative management alongside rehabilitation and lifestyle measures; appropriate for chronic pain flares and osteoarthritis-related symptoms rather than disease modification. | anti-inflammatory drug administration; pain management | (dikova2024multipleepiphysealdysplasia pages 5-10, white2020bestpracticeguidelines pages 5-7) |
| Physiotherapy / rehabilitation | Maintain mobility, muscle strength, gait function, and joint range of motion | Recommended in conservative management; no MED-specific effect sizes were reported in the retrieved sources. | Often combined with pain management, posture guidance, and orthopedic follow-up; useful across lifespan because physical HRQoL declines with age in MED. | physical therapy; rehabilitation therapy | (dikova2024multipleepiphysealdysplasia pages 5-10, matsushita2021healthrelatedqualityof pages 3-6, white2020bestpracticeguidelines pages 5-7) |
| Activity modification and weight management | Reduce joint loading and slow symptom progression in weight-bearing joints | Recommended as pragmatic supportive care; no direct interventional MED outcome trial identified. | Particularly relevant because hips and knees are heavily affected and early osteoarthritis is common; often implemented with NSAIDs and physiotherapy. | lifestyle modification; weight reduction counseling; activity modification | (dikova2024multipleepiphysealdysplasia pages 5-10, white2020bestpracticeguidelines pages 5-7) |
| Guided growth / hemiepiphysiodesis / temporary epiphysiodesis for genu valgum | Correct lower-limb malalignment during growth, especially genu valgum | In the 2025 cohort, surgical procedures included bilateral femur hemiepiphysiodesis and bilateral medial distal femur guided growth with tension-band plates for genu valgum; overall 7/25 genetically resolved patients (28%) underwent orthopedic surgery. Dikova 2024 reports temporary medial epiphysiodesis with hinge plates/screws for valgus deformity. | Best suited to skeletally immature patients with open physes; real-world implementation includes plates/screws or tension-band plates. Outcomes were described qualitatively rather than with standardized angular correction data in retrieved text. | hemiepiphysiodesis; guided growth procedure; lower limb deformity correction | (dasar2025recognizingmultipleepiphyseal pages 2-4, dikova2024multipleepiphysealdysplasia pages 1-5) |
| Proximal femoral osteotomy / distal femoral correction osteotomy | Correct coxa/proximal femoral deformity or distal femoral malalignment; improve gait and joint mechanics | The 2025 cohort reported 2 proximal femoral osteotomies and 2 distal femoral correction osteotomies with plate fixation among operated patients; quantitative pre/post functional scores were not reported for these procedures. | Used in real-world orthopedic management for progressive deformity and symptomatic malalignment. Often individualized based on hip/knee morphology and growth status. | femoral osteotomy; corrective osteotomy | (dasar2025recognizingmultipleepiphyseal pages 2-4) |
| Bernese periacetabular osteotomy (PAO) | Joint-preserving treatment for acetabular dysplasia / hip undercoverage and early hip osteoarthritis | In 6 hips from 3 patients, mean age 14.3 years, mean follow-up 1.7 years: LCEA improved 3.8°→47.1° (p=0.02), ACEA 7.3°→35.1° (p=0.02), acetabular index 27.8°→14.6° (p=0.04), femoral head coverage 66.8%→100% (p=0.02), and Harris Hip Score 67.3→86.7 (p=0.05). No major complications reported; all osteotomies united by 6 months. | Staged bilateral PAO was performed with average 104-day interval; immediate rehab with toe-touch ambulation, weight-bearing as tolerated at 1 month, full weight-bearing by 6 months. Image-based tables with these outcomes were retrieved. | periacetabular osteotomy; hip preservation surgery | (chang2023thefavorableoutcome pages 1-2, chang2023thefavorableoutcome pages 2-4, chang2023thefavorableoutcome pages 4-6, chang2023thefavorableoutcome media 2150d8bc, chang2023thefavorableoutcome media ea36e400) |
| Total hip arthroplasty (THA) | End-stage hip osteoarthritis / severe pain and functional limitation | In the 2025 cohort, 1 patient underwent total hip arthroplasty; quantitative implant survival or PROM data were not reported. Adult MED is associated with premature hip OA and joint replacement may be required relatively young. | Represents salvage treatment after progressive degenerative joint disease. Often follows years of dysplasia-related abnormal loading. | total hip arthroplasty; joint replacement surgery | (dasar2025recognizingmultipleepiphyseal pages 2-4, mazzotti2024multipleosteochondritisdissecans pages 7-8, matsushita2021healthrelatedqualityof pages 1-2) |
| Spine surveillance and management in skeletal dysplasia care | Detect spinal stenosis, deformity progression, instability, and myelopathy; prevent irreversible neurologic injury | White et al. consensus produced 31 best-practice guidelines. Surveillance recommendations include routine clinical spinal exam plus radiographic follow-up, regular neurological assessment, and further evaluation for any myelopathic signs. Surgical thresholds cited in literature include thoracolumbar kyphosis >60° with >10°/year progression; complication rates in growth-friendly instrumentation reports included dural tear ~30% and neurologic injury ~20%. | Although not MED-specific, guidance is relevant for MED patients with scoliosis/kyphosis or spine symptoms. Pre-op MRI/advanced imaging is recommended for “spine-at-risk” anatomy; avoid prophylactic C1–C2 fusion without cord compression/myelopathy. Conservative measures include posture guidance, bracing/casting for flexible kyphosis, NSAIDs, physical therapy, and timely surgery when progression persists. | spinal monitoring; neurologic monitoring; spinal radiography; magnetic resonance imaging; spinal fusion; spinal decompression | (white2020bestpracticeguidelines pages 2-4, white2020bestpracticeguidelines pages 4-5, white2020bestpracticeguidelines pages 5-7, white2020bestpracticeguidelines pages 8-9, white2020bestpracticeguidelines pages 7-8) |
| Posterior spinal instrumentation and fusion | Treat progressive scoliosis / spinal deformity with instability or neurologic risk | In the 2025 MED cohort, 1 patient underwent posterior spinal instrumentation and fusion; no MED-specific quantitative follow-up metrics were provided. | Should be individualized and informed by skeletal dysplasia spine guidelines, including pre-operative advanced imaging and assessment of cord compression / sagittal balance. | posterior spinal fusion; spinal instrumentation | (dasar2025recognizingmultipleepiphyseal pages 2-4, white2020bestpracticeguidelines pages 2-4, white2020bestpracticeguidelines pages 8-9) |
| Experimental pain therapy related to COMP-spectrum disease: oral resveratrol in pseudoachondroplasia | Reduce joint pain in COMP-related skeletal dysplasia spectrum (related, not MED-specific) | Phase 2 randomized, triple-masked crossover trial NCT03866200 enrolled 6 participants; resveratrol 125 mg/day vs placebo for 90 days with 30-day washout. Primary endpoint: Numeric Pain Rating Scale; secondary endpoint: SF-36. Trial status: TERMINATED due to inability to recruit target number, so no efficacy outcome was established. | Not a MED trial, but relevant because pseudoachondroplasia and COMP-MED share COMP-related pathobiology and pain burden. Suggests translational interest in symptom-modifying therapy for COMP disorders. | resveratrol administration; pain management clinical trial | (NCT03866200 chunk 1) |
Table: This table summarizes current treatment and management approaches for multiple epiphyseal dysplasia, including supportive care, orthopedic procedures, spine surveillance, and a related experimental pain trial in the COMP-spectrum disorder pseudoachondroplasia. It emphasizes real-world implementation details and the limited but useful quantitative surgical evidence currently available.
12.1 Orthopedic interventions (real-world implementations)
Bernese PAO has short-term evidence in a small series of three female MED patients (6 hips) demonstrating improved hip coverage angles and improved Harris Hip Score at 1 year; the pre/post changes are also captured in the retrieved tables (image citations). (chang2023thefavorableoutcome pages 1-2, chang2023thefavorableoutcome media 2150d8bc, chang2023thefavorableoutcome media ea36e400)
12.2 Pharmacotherapy and disease-modifying treatments
No disease-modifying pharmacotherapy for MED was supported in retrieved evidence; pain management is supportive. A related Phase 2 resveratrol pain trial was conducted in pseudoachondroplasia (COMP-spectrum) but terminated due to recruitment failure and therefore provides no efficacy conclusion. (NCT03866200 chunk 1)
13. Prevention
No primary prevention strategies were retrieved beyond genetic causation recognition. Tertiary prevention includes reducing joint load and proactive orthopedic surveillance/treatment to prevent progression of deformity and joint degeneration. (dikova2024multipleepiphysealdysplasia pages 5-10, dasar2025recognizingmultipleepiphyseal pages 1-2)
Evidence for carrier screening, prenatal diagnosis, or preimplantation testing was not present in retrieved texts.
14. Other species / natural disease
No naturally occurring MED in other species was identified in the retrieved evidence.
15. Model organisms
Evidence in the retrieved corpus includes: * Slc26a2−/− mouse (model of severe SLC26A2-related disorders) with FGFR3 overactivation and impaired collagen II/IX deposition. (li2024biallelicvariantsin pages 1-2) * Cellular models: human primary chondrocytes transfected with wild-type vs mutant SLC26A2 constructs; HEK-293 and Xenopus oocyte systems referenced for transporter functional studies. (li2024biallelicvariantsin pages 8-9, li2024biallelicvariantsin pages 1-2)
No COMP-MED knock-in mouse model data were directly retrieved; a 2024 case report calls for targeted mouse models to dissect phenotypic variability (e.g., OCD). (mazzotti2024multipleosteochondritisdissecans pages 7-8)
Recent developments (prioritizing 2023–2024)
- SLC26A2 MED-4 mechanism in human chondrocytes (2024-07-xx; Orphanet J Rare Dis; DOI:10.1186/s13023-024-03228-4): functional data linking disease variants to altered SLC26A2 expression/localization and chondrocyte differentiation marker shifts. (li2024biallelicvariantsin pages 1-2)
- COMP-MED phenotype expansion to multiple OCD (2024-11; Genes; DOI:10.3390/genes15111490): first reported COMP-MED case in which multiple OCD was the main manifestation, expanding clinical surveillance considerations and mechanistic hypotheses. (mazzotti2024multipleosteochondritisdissecans pages 7-8)
- Orthopedic hip-preservation evidence (2023-10; Orphanet J Rare Dis; DOI:10.1186/s13023-023-02920-1): short-term PAO outcomes with large improvements in acetabular coverage angles and functional scores. (chang2023thefavorableoutcome pages 1-2, chang2023thefavorableoutcome media 2150d8bc, chang2023thefavorableoutcome media ea36e400)
- Nosology update (2023-02; Am J Med Genet A; DOI:10.1002/ajmg.a.63132): restructured gene-linked naming system and expanded catalog (771 disorders/552 genes) relevant to MED differential diagnosis and NGS interpretation pipelines. (unger2023nosologyofgenetic pages 6-8)
Key statistics extracted (recent studies)
- Gene distribution in a genetically resolved MED cohort (n=25): COMP 52%, MATN3 20%, SLC26A2 20%, COL9A2 8%. (dasar2025recognizingmultipleepiphyseal pages 1-2)
- Symptom frequency in the same cohort: joint pain 68%, short stature 36%, orthopedic surgery 28%. (dasar2025recognizingmultipleepiphyseal pages 1-2)
- PAO radiographic correction (6 hips): LCEA 3.8°→47.1°, ACEA 7.3°→35.1°, acetabular index 27.8°→14.6°, head coverage 66.8%→100%; HHS 67.3→86.7. (chang2023thefavorableoutcome pages 1-2, chang2023thefavorableoutcome media 2150d8bc, chang2023thefavorableoutcome media ea36e400)
- SLC26A2-related MED imaging sign: double-layered patella ~60% (as reported in a mechanistic MED-4 paper). (li2024biallelicvariantsin pages 1-2)
Notes on abstract quotes and PMID requirements
The retrieved evidence is largely full-text snippets and registry entries; explicit abstract-quote extraction and PMID mapping were not available in the tool outputs for the core MED papers. Where the retrieved evidence included abstract-like language (e.g., mechanistic description and definitions), it has been paraphrased with citations. DOI/URLs and publication months are provided as available.
References
-
(dasar2025recognizingmultipleepiphyseal pages 1-2): Tuğba Daşar, Gözde İmren, Adalet Elçin Yıldız, Gizem Ürel Demir, Gülen Eda Utine, Güney Yılmaz, and Pelin Özlem Şimşek Kiper. Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia. European Journal of Pediatrics, May 2025. URL: https://doi.org/10.1007/s00431-025-06176-8, doi:10.1007/s00431-025-06176-8. This article has 2 citations and is from a peer-reviewed journal.
-
(li2024biallelicvariantsin pages 1-2): Shan Li, Yueyang Sheng, Xinyu Wang, Qianqian Wang, Ying Wang, Yanzhuo Zhang, Chengai Wu, and Xu Jiang. Biallelic variants in slc26a2 cause multiple epiphyseal dysplasia-4 by disturbing chondrocyte homeostasis. Orphanet Journal of Rare Diseases, Jul 2024. URL: https://doi.org/10.1186/s13023-024-03228-4, doi:10.1186/s13023-024-03228-4. This article has 6 citations and is from a peer-reviewed journal.
-
(mazzotti2024multipleosteochondritisdissecans pages 7-8): Antonio Mazzotti, Elena Artioli, Evelise Brizola, Alice Moroni, Morena Tremosini, Alessia Di Cecco, Salvatore Gallone, Cesare Faldini, Luca Sangiorgi, and Maria Gnoli. Multiple osteochondritis dissecans as main manifestation of multiple epiphyseal dysplasia caused by a novel cartilage oligomeric matrix protein pathogenic variant: a clinical report. Genes, 15:1490, Nov 2024. URL: https://doi.org/10.3390/genes15111490, doi:10.3390/genes15111490. This article has 2 citations.
-
(unger2023nosologyofgenetic pages 6-8): Sheila Unger, Carlos R. Ferreira, Geert R. Mortier, Houda Ali, Débora R. Bertola, Alistair Calder, Daniel H. Cohn, Valerie Cormier‐Daire, Katta M. Girisha, Christine Hall, Deborah Krakow, Outi Makitie, Stefan Mundlos, Gen Nishimura, Stephen P. Robertson, Ravi Savarirayan, David Sillence, Marleen Simon, V. Reid Sutton, Matthew L. Warman, and Andrea Superti‐Furga. Nosology of genetic skeletal disorders: 2023 revision. American Journal of Medical Genetics Part A, 191:1164-1209, Feb 2023. URL: https://doi.org/10.1002/ajmg.a.63132, doi:10.1002/ajmg.a.63132. This article has 495 citations.
-
(dasar2025recognizingmultipleepiphyseal pages 2-4): Tuğba Daşar, Gözde İmren, Adalet Elçin Yıldız, Gizem Ürel Demir, Gülen Eda Utine, Güney Yılmaz, and Pelin Özlem Şimşek Kiper. Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia. European Journal of Pediatrics, May 2025. URL: https://doi.org/10.1007/s00431-025-06176-8, doi:10.1007/s00431-025-06176-8. This article has 2 citations and is from a peer-reviewed journal.
-
(dikova2024multipleepiphysealdysplasia pages 5-10): Milka Dikova, Mihaela Blazheva, Oleg Mladenov, and Darina Kachakova. Multiple epiphyseal dysplasia with contribution of two cases with a mutation in the comp gene. THE JOURNAL OF THE BULGARIAN ORTHOPAEDICS AND TRAUMA ASSOCIATION, 61:202-212, Sep 2024. URL: https://doi.org/10.58542/jbota.v61i4.154, doi:10.58542/jbota.v61i4.154. This article has 0 citations.
-
(white2020bestpracticeguidelines pages 2-4): Klane K. White, Michael B. Bober, Tae-Joon Cho, Michael J. Goldberg, Julie Hoover-Fong, Melita Irving, Shawn E. Kamps, William G. Mackenzie, Cathleen Raggio, Samantha A. Spencer, Viviana Bompadre, and Ravi Savarirayan. Best practice guidelines for management of spinal disorders in skeletal dysplasia. Orphanet Journal of Rare Diseases, Jun 2020. URL: https://doi.org/10.1186/s13023-020-01415-7, doi:10.1186/s13023-020-01415-7. This article has 43 citations and is from a peer-reviewed journal.
-
(savarirayan2021bestpracticeguidelines pages 1-2): Ravi Savarirayan, David E. Tunkel, Laura M. Sterni, Michael B. Bober, Tae-Joon Cho, Michael J. Goldberg, Julie Hoover-Fong, Melita Irving, Shawn E. Kamps, William G. Mackenzie, Cathleen Raggio, Samantha A. Spencer, Viviana Bompadre, and Klane K. White. Best practice guidelines in managing the craniofacial aspects of skeletal dysplasia. Orphanet Journal of Rare Diseases, Jan 2021. URL: https://doi.org/10.1186/s13023-021-01678-8, doi:10.1186/s13023-021-01678-8. This article has 32 citations and is from a peer-reviewed journal.
-
(dasar2025recognizingmultipleepiphyseal pages 5-7): Tuğba Daşar, Gözde İmren, Adalet Elçin Yıldız, Gizem Ürel Demir, Gülen Eda Utine, Güney Yılmaz, and Pelin Özlem Şimşek Kiper. Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia. European Journal of Pediatrics, May 2025. URL: https://doi.org/10.1007/s00431-025-06176-8, doi:10.1007/s00431-025-06176-8. This article has 2 citations and is from a peer-reviewed journal.
-
(dikova2024multipleepiphysealdysplasia pages 1-5): Milka Dikova, Mihaela Blazheva, Oleg Mladenov, and Darina Kachakova. Multiple epiphyseal dysplasia with contribution of two cases with a mutation in the comp gene. THE JOURNAL OF THE BULGARIAN ORTHOPAEDICS AND TRAUMA ASSOCIATION, 61:202-212, Sep 2024. URL: https://doi.org/10.58542/jbota.v61i4.154, doi:10.58542/jbota.v61i4.154. This article has 0 citations.
-
(dasar2025recognizingmultipleepiphyseal pages 4-5): Tuğba Daşar, Gözde İmren, Adalet Elçin Yıldız, Gizem Ürel Demir, Gülen Eda Utine, Güney Yılmaz, and Pelin Özlem Şimşek Kiper. Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia. European Journal of Pediatrics, May 2025. URL: https://doi.org/10.1007/s00431-025-06176-8, doi:10.1007/s00431-025-06176-8. This article has 2 citations and is from a peer-reviewed journal.
-
(matsushita2021healthrelatedqualityof pages 1-2): Masaki Matsushita, Kenichi Mishima, Yasunari Kamiya, Nobuhiko Haga, Sayaka Fujiwara, Keiichi Ozono, Takuo Kubota, Taichi Kitaoka, Shiro Imagama, and Hiroshi Kitoh. Health-related quality of life in adult patients with multiple epiphyseal dysplasia and spondyloepiphyseal dysplasia. Progress in Rehabilitation Medicine, 6:n/a, Dec 2021. URL: https://doi.org/10.2490/prm.20210048, doi:10.2490/prm.20210048. This article has 3 citations.
-
(mazzotti2024multipleosteochondritisdissecans pages 5-7): Antonio Mazzotti, Elena Artioli, Evelise Brizola, Alice Moroni, Morena Tremosini, Alessia Di Cecco, Salvatore Gallone, Cesare Faldini, Luca Sangiorgi, and Maria Gnoli. Multiple osteochondritis dissecans as main manifestation of multiple epiphyseal dysplasia caused by a novel cartilage oligomeric matrix protein pathogenic variant: a clinical report. Genes, 15:1490, Nov 2024. URL: https://doi.org/10.3390/genes15111490, doi:10.3390/genes15111490. This article has 2 citations.
-
(matsushita2021healthrelatedqualityof pages 3-6): Masaki Matsushita, Kenichi Mishima, Yasunari Kamiya, Nobuhiko Haga, Sayaka Fujiwara, Keiichi Ozono, Takuo Kubota, Taichi Kitaoka, Shiro Imagama, and Hiroshi Kitoh. Health-related quality of life in adult patients with multiple epiphyseal dysplasia and spondyloepiphyseal dysplasia. Progress in Rehabilitation Medicine, 6:n/a, Dec 2021. URL: https://doi.org/10.2490/prm.20210048, doi:10.2490/prm.20210048. This article has 3 citations.
-
(silveira2022slc26a2dtdstspectruma pages 3-4): Cynthia Silveira, Karina da Costa Silveira, Maria D. Lacarrubba-Flores, Maurício T. Sakata, Silvia N. Carbognani, Juan Llerena Jr., Carolina A. Moreno, and Denise P. Cavalcanti. Slc26a2/dtdst spectrum: a cohort of 12 patients associated with a comprehensive review of the genotype-phenotype correlation. Molecular Syndromology, 13:485-495, Jun 2022. URL: https://doi.org/10.1159/000525020, doi:10.1159/000525020. This article has 10 citations and is from a peer-reviewed journal.
-
(li2024biallelicvariantsin pages 9-10): Shan Li, Yueyang Sheng, Xinyu Wang, Qianqian Wang, Ying Wang, Yanzhuo Zhang, Chengai Wu, and Xu Jiang. Biallelic variants in slc26a2 cause multiple epiphyseal dysplasia-4 by disturbing chondrocyte homeostasis. Orphanet Journal of Rare Diseases, Jul 2024. URL: https://doi.org/10.1186/s13023-024-03228-4, doi:10.1186/s13023-024-03228-4. This article has 6 citations and is from a peer-reviewed journal.
-
(dasar2025recognizingmultipleepiphyseal pages 10-11): Tuğba Daşar, Gözde İmren, Adalet Elçin Yıldız, Gizem Ürel Demir, Gülen Eda Utine, Güney Yılmaz, and Pelin Özlem Şimşek Kiper. Recognizing multiple epiphyseal dysplasia in children presenting with joint pain: a commonly overlooked skeletal dysplasia. European Journal of Pediatrics, May 2025. URL: https://doi.org/10.1007/s00431-025-06176-8, doi:10.1007/s00431-025-06176-8. This article has 2 citations and is from a peer-reviewed journal.
-
(white2020bestpracticeguidelines pages 5-7): Klane K. White, Michael B. Bober, Tae-Joon Cho, Michael J. Goldberg, Julie Hoover-Fong, Melita Irving, Shawn E. Kamps, William G. Mackenzie, Cathleen Raggio, Samantha A. Spencer, Viviana Bompadre, and Ravi Savarirayan. Best practice guidelines for management of spinal disorders in skeletal dysplasia. Orphanet Journal of Rare Diseases, Jun 2020. URL: https://doi.org/10.1186/s13023-020-01415-7, doi:10.1186/s13023-020-01415-7. This article has 43 citations and is from a peer-reviewed journal.
-
(chang2023thefavorableoutcome pages 1-2): Yao-Yuan Chang, Chia-Che Lee, Sheng-Chieh Lin, Ken N. Kuo, Jia-Feng Chang, Kuan-Wen Wu, and Ting-Ming Wang. The favorable outcome of bernese periacetabular osteotomy for the hip osteoarthritis in multiple epiphyseal dysplasia. Orphanet Journal of Rare Diseases, Oct 2023. URL: https://doi.org/10.1186/s13023-023-02920-1, doi:10.1186/s13023-023-02920-1. This article has 2 citations and is from a peer-reviewed journal.
-
(chang2023thefavorableoutcome pages 2-4): Yao-Yuan Chang, Chia-Che Lee, Sheng-Chieh Lin, Ken N. Kuo, Jia-Feng Chang, Kuan-Wen Wu, and Ting-Ming Wang. The favorable outcome of bernese periacetabular osteotomy for the hip osteoarthritis in multiple epiphyseal dysplasia. Orphanet Journal of Rare Diseases, Oct 2023. URL: https://doi.org/10.1186/s13023-023-02920-1, doi:10.1186/s13023-023-02920-1. This article has 2 citations and is from a peer-reviewed journal.
-
(chang2023thefavorableoutcome pages 4-6): Yao-Yuan Chang, Chia-Che Lee, Sheng-Chieh Lin, Ken N. Kuo, Jia-Feng Chang, Kuan-Wen Wu, and Ting-Ming Wang. The favorable outcome of bernese periacetabular osteotomy for the hip osteoarthritis in multiple epiphyseal dysplasia. Orphanet Journal of Rare Diseases, Oct 2023. URL: https://doi.org/10.1186/s13023-023-02920-1, doi:10.1186/s13023-023-02920-1. This article has 2 citations and is from a peer-reviewed journal.
-
(chang2023thefavorableoutcome media 2150d8bc): Yao-Yuan Chang, Chia-Che Lee, Sheng-Chieh Lin, Ken N. Kuo, Jia-Feng Chang, Kuan-Wen Wu, and Ting-Ming Wang. The favorable outcome of bernese periacetabular osteotomy for the hip osteoarthritis in multiple epiphyseal dysplasia. Orphanet Journal of Rare Diseases, Oct 2023. URL: https://doi.org/10.1186/s13023-023-02920-1, doi:10.1186/s13023-023-02920-1. This article has 2 citations and is from a peer-reviewed journal.
-
(chang2023thefavorableoutcome media ea36e400): Yao-Yuan Chang, Chia-Che Lee, Sheng-Chieh Lin, Ken N. Kuo, Jia-Feng Chang, Kuan-Wen Wu, and Ting-Ming Wang. The favorable outcome of bernese periacetabular osteotomy for the hip osteoarthritis in multiple epiphyseal dysplasia. Orphanet Journal of Rare Diseases, Oct 2023. URL: https://doi.org/10.1186/s13023-023-02920-1, doi:10.1186/s13023-023-02920-1. This article has 2 citations and is from a peer-reviewed journal.
-
(white2020bestpracticeguidelines pages 4-5): Klane K. White, Michael B. Bober, Tae-Joon Cho, Michael J. Goldberg, Julie Hoover-Fong, Melita Irving, Shawn E. Kamps, William G. Mackenzie, Cathleen Raggio, Samantha A. Spencer, Viviana Bompadre, and Ravi Savarirayan. Best practice guidelines for management of spinal disorders in skeletal dysplasia. Orphanet Journal of Rare Diseases, Jun 2020. URL: https://doi.org/10.1186/s13023-020-01415-7, doi:10.1186/s13023-020-01415-7. This article has 43 citations and is from a peer-reviewed journal.
-
(white2020bestpracticeguidelines pages 8-9): Klane K. White, Michael B. Bober, Tae-Joon Cho, Michael J. Goldberg, Julie Hoover-Fong, Melita Irving, Shawn E. Kamps, William G. Mackenzie, Cathleen Raggio, Samantha A. Spencer, Viviana Bompadre, and Ravi Savarirayan. Best practice guidelines for management of spinal disorders in skeletal dysplasia. Orphanet Journal of Rare Diseases, Jun 2020. URL: https://doi.org/10.1186/s13023-020-01415-7, doi:10.1186/s13023-020-01415-7. This article has 43 citations and is from a peer-reviewed journal.
-
(white2020bestpracticeguidelines pages 7-8): Klane K. White, Michael B. Bober, Tae-Joon Cho, Michael J. Goldberg, Julie Hoover-Fong, Melita Irving, Shawn E. Kamps, William G. Mackenzie, Cathleen Raggio, Samantha A. Spencer, Viviana Bompadre, and Ravi Savarirayan. Best practice guidelines for management of spinal disorders in skeletal dysplasia. Orphanet Journal of Rare Diseases, Jun 2020. URL: https://doi.org/10.1186/s13023-020-01415-7, doi:10.1186/s13023-020-01415-7. This article has 43 citations and is from a peer-reviewed journal.
-
(NCT03866200 chunk 1): Karen Posey. Resveratrol Trial for Relief of Pain in Pseudoachondroplasia. The University of Texas Health Science Center, Houston. 2019. ClinicalTrials.gov Identifier: NCT03866200
-
(li2024biallelicvariantsin pages 8-9): Shan Li, Yueyang Sheng, Xinyu Wang, Qianqian Wang, Ying Wang, Yanzhuo Zhang, Chengai Wu, and Xu Jiang. Biallelic variants in slc26a2 cause multiple epiphyseal dysplasia-4 by disturbing chondrocyte homeostasis. Orphanet Journal of Rare Diseases, Jul 2024. URL: https://doi.org/10.1186/s13023-024-03228-4, doi:10.1186/s13023-024-03228-4. This article has 6 citations and is from a peer-reviewed journal.