MALT Lymphoma
MALT lymphoma (extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue) is an indolent mature B-cell non-Hodgkin lymphoma that arises at extranodal sites of chronic antigenic stimulation. Sustained antigen drive, most classically by Helicobacter pylori in the stomach, or by autoimmune inflammation (Sjogren syndrome, Hashimoto thyroiditis) and other infections, promotes clonal expansion of marginal-zone-derived B cells. A subset acquires recurrent chromosomal translocations that constitutively activate the NF-kB pathway, most notably t(11;18)(q21;q21)/BIRC3::MALT1, t(14;18)(q32;q21)/IGH::MALT1, and t(1;14)(p22;q32)/BCL10::IGH, rendering tumor growth independent of the original antigenic stimulus. Early antigen-dependent disease (e.g. gastric MALT lymphoma without t(11;18)) often regresses after eradication of the driving infection, whereas translocation-positive disease typically requires radiotherapy, anti-CD20 immunotherapy, or systemic therapy.
Ask OpenScientist
Ask a research question about MALT Lymphoma. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Subtypes
5Show evidence (1 reference)
Show evidence (1 reference)
Pathophysiology
4Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Pathograph
Phenotypes
3Cardiovascular 1
Show evidence (1 reference)
Constitutional 1
Show evidence (1 reference)
Other 1
Show evidence (1 reference)
Genetic Associations
2Show evidence (1 reference)
Show evidence (1 reference)
Medical Actions
3Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Clinical Trials
1Show evidence (1 reference)
Source YAML
click to showname: MALT Lymphoma
creation_date: "2026-06-08T00:00:00Z"
description: >-
MALT lymphoma (extranodal marginal zone lymphoma of mucosa-associated lymphoid
tissue) is an indolent mature B-cell non-Hodgkin lymphoma that arises at
extranodal sites of chronic antigenic stimulation. Sustained antigen drive,
most classically by Helicobacter pylori in the stomach, or by autoimmune
inflammation (Sjogren syndrome, Hashimoto thyroiditis) and other infections,
promotes clonal expansion of marginal-zone-derived B cells. A subset acquires
recurrent chromosomal translocations that constitutively activate the NF-kB
pathway, most notably t(11;18)(q21;q21)/BIRC3::MALT1, t(14;18)(q32;q21)/IGH::MALT1,
and t(1;14)(p22;q32)/BCL10::IGH, rendering tumor growth independent of the
original antigenic stimulus. Early antigen-dependent disease (e.g. gastric MALT
lymphoma without t(11;18)) often regresses after eradication of the driving
infection, whereas translocation-positive disease typically requires
radiotherapy, anti-CD20 immunotherapy, or systemic therapy.
categories:
- Hematologic Malignancy
- B-cell Neoplasm
- Non-Hodgkin Lymphoma
parents:
- B-cell non-Hodgkin lymphoma
- marginal zone lymphoma
disease_term:
preferred_term: MALT lymphoma
term:
id: MONDO:0007650
label: MALT lymphoma
has_subtypes:
- name: Gastric MALT
display_name: Gastric MALT Lymphoma (H. pylori-driven)
description: >-
Most common form, arising in gastric mucosa acquired as MALT in response to
chronic Helicobacter pylori infection. Early-stage, t(11;18)-negative disease
commonly regresses after H. pylori eradication.
- name: t(11;18) MALT
display_name: t(11;18) BIRC3::MALT1 MALT Lymphoma
description: >-
Translocation-defined subset carrying t(11;18)(q21;q21) generating the
BIRC3::MALT1 (API2-MALT1) fusion oncoprotein. Associated with disseminated
disease and resistance to H. pylori eradication.
evidence:
- reference: PMID:21568677
reference_title: "Protease activity of the API2-MALT1 fusion oncoprotein in MALT lymphoma development and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The recurrent translocation t(11;18)(q21;q21) is associated with failure to respond to antibiotic therapy and increased rate of dissemination."
explanation: Defines the t(11;18) subtype by its antibiotic resistance and increased dissemination.
- name: Pulmonary MALT
display_name: Pulmonary / BALT Lymphoma
description: >-
MALT lymphoma of bronchus-associated lymphoid tissue, the most common primary
pulmonary lymphoma. Frequently indolent and often associated with t(11;18).
- name: Ocular Adnexal MALT
display_name: Ocular Adnexal MALT Lymphoma
description: >-
MALT lymphoma of the conjunctiva, orbit, and lacrimal gland, in some regions
associated with Chlamydia psittaci infection.
- name: Salivary Gland MALT
display_name: Salivary Gland MALT Lymphoma
description: >-
MALT lymphoma of salivary gland tissue, strongly associated with Sjogren
syndrome and chronic lymphoepithelial sialadenitis.
evidence:
- reference: PMID:28288723
reference_title: "Clinical features and management of non-gastrointestinal non-ocular extranodal mucosa associated lymphoid tissue (ENMALT) marginal zone lymphomas."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "These lymphomas usually arise in a setting of inflammation due to a persistent infection or autoimmune diseases such as Sjogren syndrome in salivary MALT lymphomas and Hashimoto's thryroiditis in thyroid lymphomas."
explanation: Links salivary gland MALT lymphoma to Sjogren syndrome-associated chronic inflammation.
pathophysiology:
- name: Chronic Antigenic Stimulation
conforms_to: "tumor_promoting_inflammation#Chronic Inflammatory Stimulus"
description: >-
Persistent infection (most classically H. pylori in the stomach) or chronic
autoimmune inflammation drives sustained antigen-dependent stimulation of
B cells at extranodal sites, creating acquired mucosa-associated lymphoid
tissue and a microenvironment that promotes B-cell proliferation and survival.
evidence:
- reference: PMID:21568677
reference_title: "Protease activity of the API2-MALT1 fusion oncoprotein in MALT lymphoma development and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Gastric mucosa-associated lymphoid tissue (MALT) lymphoma is a prototypical cancer that occurs in the setting of chronic inflammation and an important model for understanding how deregulated NF-κB transcriptional activity contributes to malignancy."
explanation: Review establishes that gastric MALT lymphoma arises in the setting of chronic inflammation.
cell_types:
- preferred_term: marginal zone B cell
term:
id: CL:0009060
label: marginal zone B cell of lymph node
biological_processes:
- preferred_term: inflammatory response
modifier: INCREASED
term:
id: GO:0006954
label: inflammatory response
downstream:
- target: Antigen-Driven Clonal B-cell Expansion
description: Sustained antigenic and T-cell help drives clonal selection of marginal-zone B cells
- name: Antigen-Driven Clonal B-cell Expansion
description: >-
Chronic B-cell receptor signaling and T-helper-cell-derived signals select
and expand a clonal population of marginal-zone-derived memory B cells. At
this stage proliferation remains dependent on the antigenic stimulus, which
is why early gastric MALT lymphoma can regress after antigen removal.
evidence:
- reference: PMID:21568677
reference_title: "Protease activity of the API2-MALT1 fusion oncoprotein in MALT lymphoma development and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Most gastric MALT lymphomas require ongoing antigenic stimulation for continued tumor growth, and Stage I disease is usually cured by eradicating the causative microorganism, Helicobacter pylori, with antibiotics."
explanation: Establishes that early MALT lymphoma growth remains dependent on ongoing antigenic stimulation.
cell_types:
- preferred_term: marginal zone B cell
term:
id: CL:0009060
label: marginal zone B cell of lymph node
biological_processes:
- preferred_term: B cell receptor signaling pathway
modifier: INCREASED
term:
id: GO:0050853
label: B cell receptor signaling pathway
- preferred_term: B cell proliferation
modifier: INCREASED
term:
id: GO:0042100
label: B cell proliferation
downstream:
- target: NF-kB-Activating Translocations
description: Genetic instability during chronic proliferation favors acquisition of NF-kB-activating translocations
- name: NF-kB-Activating Translocations
description: >-
A subset of tumors acquires recurrent chromosomal translocations that
converge on the BCL10-MALT1 signaling axis and constitutively activate NF-kB:
t(11;18)(q21;q21)/BIRC3::MALT1, t(14;18)(q32;q21)/IGH::MALT1, and
t(1;14)(p22;q32)/BCL10::IGH. These lesions render lymphoma growth independent
of the original antigenic stimulus.
evidence:
- reference: PMID:15694184
reference_title: "Update on MALT lymphomas."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Three translocations, t(11;18)(q21;q21), t(1;14)(p22;q32) and t(14;18)(q32;q21) are specifically associated with MALT lymphoma and the genes involved have been identified."
explanation: Identifies the three recurrent MALT lymphoma translocations.
- reference: PMID:15694184
reference_title: "Update on MALT lymphomas."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "These three chromosomal translocations that involve different genes appear to share common oncogenic properties by targeting the same nuclear factor kappa B (NF kappa B) oncogenic pathway."
explanation: Establishes that the translocations converge on constitutive NF-kB activation.
cell_types:
- preferred_term: marginal zone B cell
term:
id: CL:0009060
label: marginal zone B cell of lymph node
biological_processes:
- preferred_term: canonical NF-kappaB signal transduction
modifier: INCREASED
term:
id: GO:0007249
label: canonical NF-kappaB signal transduction
downstream:
- target: Antigen-Independent Lymphoma Growth
description: Constitutive NF-kB signaling sustains proliferation and survival without antigen
- name: Antigen-Independent Lymphoma Growth
description: >-
Constitutive NF-kB activation drives expression of anti-apoptotic and
proliferative target genes, sustaining tumor B-cell survival and growth
independent of the original antigenic stimulus. This explains the failure of
antigen/antibiotic-directed therapy in translocation-positive disease.
evidence:
- reference: PMID:21568677
reference_title: "Protease activity of the API2-MALT1 fusion oncoprotein in MALT lymphoma development and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "in a subset of MALT lymphomas, chromosomal translocations are acquired that render the lymphoma antigen-independent. The recurrent translocation t(11;18)(q21;q21) is associated with failure to respond to antibiotic therapy and increased rate of dissemination."
explanation: Establishes that translocation-positive MALT lymphoma becomes antigen-independent and resistant to antibiotic therapy.
cell_types:
- preferred_term: marginal zone B cell
term:
id: CL:0009060
label: marginal zone B cell of lymph node
biological_processes:
- preferred_term: B cell proliferation
modifier: INCREASED
term:
id: GO:0042100
label: B cell proliferation
- preferred_term: apoptotic process
modifier: DECREASED
term:
id: GO:0006915
label: apoptotic process
phenotypes:
- category: Clinical
name: Lymphadenopathy
description: Regional or disseminated lymph node involvement in advanced disease.
phenotype_term:
preferred_term: Lymphadenopathy
term:
id: HP:0002716
label: Lymphadenopathy
evidence:
- reference: PMID:28288723
reference_title: "Clinical features and management of non-gastrointestinal non-ocular extranodal mucosa associated lymphoid tissue (ENMALT) marginal zone lymphomas."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "Patients often present with localised stage I or II although disseminated disease may be present at diagnosis or relapse in a third of the cases."
explanation: Supports nodal/disseminated involvement in a subset of MALT lymphoma patients.
- category: Clinical
name: Epigastric Pain
description: >-
Nonspecific epigastric pain is the most common presenting symptom of gastric
MALT lymphoma.
phenotype_term:
preferred_term: Epigastric pain
term:
id: HP:0410019
label: Epigastric pain
evidence:
- reference: PMID:9646819
reference_title: "Gastric mucosa-associated lymphoid tissue lymphoma: radiographic findings in six patients."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The most common clinical findings at presentation included epigastric pain (n = 6), dyspepsia (n = 4), and nausea and vomiting (n = 4)."
explanation: Epigastric pain was the most frequent presenting symptom in gastric MALT lymphoma patients.
- category: Clinical
name: Dyspepsia
description: >-
Dyspepsia is a common nonspecific presenting symptom of gastric MALT
lymphoma, reflecting the indolent mucosal involvement of the stomach.
phenotype_term:
preferred_term: Dyspepsia
term:
id: HP:0410281
label: Dyspepsia
evidence:
- reference: PMID:9646819
reference_title: "Gastric mucosa-associated lymphoid tissue lymphoma: radiographic findings in six patients."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The most common clinical findings at presentation included epigastric pain (n = 6), dyspepsia (n = 4), and nausea and vomiting (n = 4)."
explanation: Dyspepsia was a common presenting symptom in gastric MALT lymphoma patients.
genetic:
- name: BIRC3/MALT1 Translocation
gene_term:
preferred_term: MALT1
term:
id: hgnc:6819
label: MALT1
association: Defining Genetic Lesion
notes: >-
t(11;18)(q21;q21) fuses BIRC3 (API2) to MALT1, generating a chimeric
oncoprotein that constitutively activates NF-kB.
evidence:
- reference: PMID:21568677
reference_title: "Protease activity of the API2-MALT1 fusion oncoprotein in MALT lymphoma development and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "This translocation creates the API2-MALT1 fusion oncoprotein, which comprises the amino terminus of inhibitor of apoptosis 2 (API2 or cIAP2) fused to the carboxy terminus of MALT1."
explanation: Describes the BIRC3 (API2)-MALT1 fusion oncoprotein created by t(11;18).
- name: BCL10 Translocation
gene_term:
preferred_term: BCL10
term:
id: hgnc:989
label: BCL10
association: Recurrent Genetic Lesion
notes: >-
t(1;14)(p22;q32) juxtaposes BCL10 to the IGH locus, deregulating BCL10
expression and constitutively activating the BCL10-MALT1-NF-kB axis.
evidence:
- reference: PMID:15694184
reference_title: "Update on MALT lymphomas."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "T(1;14) and t(14;18) deregulate BCL10 and MALT1 expression, respectively."
explanation: Identifies t(1;14)-mediated deregulation of BCL10 expression in MALT lymphoma.
treatments:
- name: Helicobacter pylori Eradication
description: >-
Antibiotic-based H. pylori eradication is first-line therapy for early-stage
gastric MALT lymphoma and induces lymphoma regression in a majority of
t(11;18)-negative cases.
treatment_term:
preferred_term: antibiotic therapy
term:
id: NCIT:C15620
label: Antibiotic Therapy
evidence:
- reference: PMID:37122607
reference_title: "Effectiveness of Helicobacter pylori eradication in the treatment of early-stage gastric mucosa-associated lymphoid tissue lymphoma: An up-to-date meta-analysis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The pooled CR of H. pylori-positive early-stage GML after bacterial eradication was 75.18% (95%CI: 70.45%-79.91%)."
explanation: Meta-analysis quantifies complete remission of early-stage gastric MALT lymphoma after H. pylori eradication.
- reference: PMID:37122607
reference_title: "Effectiveness of Helicobacter pylori eradication in the treatment of early-stage gastric mucosa-associated lymphoid tissue lymphoma: An up-to-date meta-analysis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Meta-regression analysis identified statistically significant effect modifiers, including the proportion of patients with t(11;18)(q21;q21)-positive GML and the risk of bias in each study."
explanation: Shows that t(11;18) positivity modifies the response to eradication therapy.
- name: Radiotherapy
description: >-
Involved-site radiotherapy is highly effective for localized MALT lymphoma,
including antibiotic-unresponsive gastric disease and non-gastric sites.
treatment_term:
preferred_term: radiation therapy
term:
id: MAXO:0000014
label: radiation therapy
evidence:
- reference: PMID:39448038
reference_title: "Reduced-dose Radiation Therapy for Stage IE Gastric Mucosa-Associated Lymphoid Tissue Lymphoma: A Multi-Institutional Prospective Study (KROG 16-18)."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Definitive radiation therapy (RT) of 30 Gy or higher is commonly recommended to treat Helicobacter pylori-independent gastric mucosa-associated lymphoid tissue (MALT) lymphoma with an excellent disease control rate."
explanation: Establishes radiotherapy as standard therapy for H. pylori-independent gastric MALT lymphoma with excellent control.
- reference: PMID:39448038
reference_title: "Reduced-dose Radiation Therapy for Stage IE Gastric Mucosa-Associated Lymphoid Tissue Lymphoma: A Multi-Institutional Prospective Study (KROG 16-18)."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The 6-month CR rate was 96.7%."
explanation: Prospective trial demonstrates high complete remission rate with radiotherapy for stage IE gastric MALT lymphoma.
- name: Rituximab
description: >-
Anti-CD20 monoclonal antibody used alone or with chemotherapy for
disseminated or relapsed MALT lymphoma.
therapeutic_modality: MONOCLONAL_ANTIBODY
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: rituximab
term:
id: NCIT:C1702
label: Rituximab
evidence:
- reference: PMID:28355112
reference_title: "Final Results of the IELSG-19 Randomized Trial of Mucosa-Associated Lymphoid Tissue Lymphoma: Improved Event-Free and Progression-Free Survival With Rituximab Plus Chlorambucil Versus Either Chlorambucil or Rituximab Monotherapy."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Rituximab in combination with chlorambucil demonstrated superior efficacy in mucosa-associated lymphoid tissue lymphoma"
explanation: Randomized IELSG-19 trial shows rituximab plus chlorambucil improves outcomes in MALT lymphoma.
clinical_trials:
- name: NCT00210353
phase: PHASE_III
status: COMPLETED
description: >-
IELSG-19, a multicenter randomized phase III trial comparing chlorambucil
monotherapy, rituximab monotherapy, and the chlorambucil plus rituximab
combination as first-line systemic therapy for extranodal marginal zone
(MALT) lymphoma.
evidence:
- reference: clinicaltrials:NCT00210353
supports: SUPPORT
snippet: "determine whether the addition of Rituximab to Chlorambucil will improve the outcome of MALT lymphoma in comparison to treatment with Chlorambucil alone"
explanation: ClinicalTrials.gov summary confirms IELSG-19 tested adding rituximab to chlorambucil in MALT lymphoma.
References & Deep Research
Deep Research
1Question: You are an expert researcher providing comprehensive, well-cited information.
Provide detailed information focusing on: 1. Key concepts and definitions with current understanding 2. Recent developments and latest research (prioritize 2023-2024 sources) 3. Current applications and real-world implementations 4. Expert opinions and analysis from authoritative sources 5. Relevant statistics and data from recent studies
Format as a comprehensive research report with proper citations. Include URLs and publication dates where available. Always prioritize recent, authoritative sources and provide specific citations for all major claims.
Disease Characteristics Research Template
Target Disease
- Disease Name: MALT Lymphoma
- MONDO ID: (if available)
- Category:
Research Objectives
Please provide a comprehensive research report on MALT Lymphoma covering all of the disease characteristics listed below. This report will be used to populate a disease knowledge base entry. Be thorough and cite primary literature (PMID preferred) for all claims.
For each section, suggested databases/resources are listed. These are the first places you should search for information on each topic.
1. Disease Information
Search first: OMIM, Orphanet, ICD-10/ICD-11, MeSH, PubMed
- What is the disease? Provide a concise overview.
- What are the key identifiers? (OMIM, Orphanet, ICD-10/ICD-11, MeSH, Mondo)
- What are the common synonyms and alternative names?
- Is the information derived from individual patients (e.g., EHR) or aggregated disease-level resources?
2. Etiology
- Disease Causal Factors: What are the primary causes? (genetic, environmental, infectious, mechanistic)
- Risk Factors:
Search first: PubMed, Cochrane Library, UpToDate, clinical guidelines, ClinVar, ClinGen, GWAS Catalog, PheGenI, CTD, CDC, WHO, epidemiological databases
- Genetic risk factors (causal variants, susceptibility loci, modifier genes)
- Environmental risk factors (toxins, lifestyle, occupational exposures, age, sex, family history)
- Protective Factors:
Search first: PubMed, Cochrane Library, clinical trial databases, GWAS Catalog, gnomAD, WHO, CDC, nutrition databases
- Genetic protective factors (protective variants, modifier alleles)
- Environmental protective factors (diet, lifestyle, exposures that reduce risk)
- Gene-Environment Interactions: How do genetic and environmental factors interact to influence disease?
Search first: CTD, PubMed, PheGenI, GxE databases
3. Phenotypes
Search first: HPO (Human Phenotype Ontology), OMIM, Orphanet, PubMed, clinicaltrials.gov, MedDRA, SNOMED CT, DECIPHER, LOINC
For each phenotype, provide: - Phenotype type: symptoms, clinical signs, physical manifestations, behavioral changes, or laboratory abnormalities
For symptoms/signs: HPO, OMIM, Orphanet, PubMed For behavioral changes: HPO, DSM, RDoC (Research Domain Criteria), PubMed For laboratory abnormalities: LOINC, SNOMED CT, LabTests Online, PubMed - Phenotype characteristics: Search first: OMIM, Orphanet, HPO, PubMed - Age of symptom onset (neonatal, childhood, adult-onset, late-onset) - Symptom severity (mild, moderate, severe, variable) - Symptom progression (stable, progressive, episodic, fluctuating) - Frequency among affected individuals (percentage or qualitative) - Quality of life impact: Effects on daily functioning and well-being (per-phenotype when possible) Search first: EQ-5D database, SF-36, WHO QOL databases, PubMed - Suggest HPO (Human Phenotype Ontology) terms for each phenotype
4. Genetic/Molecular Information
- Causal Genes: Gene mutations or chromosomal abnormalities responsible for disease (gene symbols, OMIM IDs)
Search first: OMIM, ClinVar, HGMD, Ensembl, NCBI Gene
- Pathogenic Variants:
- Affected genes (gene symbols, HGNC IDs) > Search first: OMIM, NCBI Gene, Ensembl, HGNC, UniProt, GeneCards
- Variant classification (pathogenic, likely pathogenic, VUS per ACMG/AMP guidelines) > Search first: ClinVar, ClinGen, ACMG/AMP guidelines, VarSome
- Variant type/class (missense, frameshift, nonsense, splice-site, structural)
- Allele frequency in population databases > Search first: gnomAD, 1000 Genomes, ExAC, TOPMed, dbSNP
- Somatic vs germline origin > Search first: COSMIC (somatic), ClinVar, ICGC, TCGA
- Functional consequences (loss of function, gain of function, dominant negative)
- Modifier Genes: Genes that modify disease severity or expression
- Epigenetic Information: DNA methylation, histone modifications, chromatin changes affecting disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Chromosomal Abnormalities: Large-scale genetic changes (aneuploidy, translocations, inversions)
Search first: DECIPHER, ClinVar, ECARUCA, UCSC Genome Browser
5. Environmental Information
- Environmental Factors: Non-genetic contributing factors (toxins, radiation, pollution, occupational exposure)
Search first: CTD (Comparative Toxicogenomics Database), TOXNET, PubMed, EPA databases
- Lifestyle Factors: Behavioral factors (smoking, diet, exercise, alcohol consumption)
Search first: CDC databases, WHO, PubMed, NHANES
- Infectious Agents: If applicable, pathogens causing or triggering disease (bacteria, viruses, fungi, parasites)
Search first: NCBI Taxonomy, ViPR, BV-BRC, MicrobeDB, GIDEON
6. Mechanism / Pathophysiology
- Molecular Pathways: Specific signaling cascades or biochemical pathways involved (Wnt, MAPK, mTOR, PI3K-AKT, etc.)
Search first: KEGG, Reactome, WikiPathways, PathBank, BioCyc
- Cellular Processes: Cell-level mechanisms (apoptosis, autophagy, cell cycle dysregulation, inflammation, etc.)
Search first: Gene Ontology (GO), Reactome, KEGG, PubMed
- Protein Dysfunction: How protein structure or function is altered (misfolding, aggregation, loss of function, gain of function)
Search first: UniProt, PDB (Protein Data Bank), InterPro, Pfam, AlphaFold
- Metabolic Changes: Alterations in metabolic processes (energy metabolism, lipid metabolism, amino acid metabolism)
Search first: KEGG, BioCyc, HMDB (Human Metabolome Database), BRENDA
- Immune System Involvement: Role of immune response (autoimmunity, immunodeficiency, chronic inflammation)
Search first: ImmPort, Immunome Database, IEDB, Gene Ontology
- Tissue Damage Mechanisms: How tissues/ are injured (oxidative stress, ischemia, fibrosis, necrosis)
Search first: PubMed, Gene Ontology, Reactome
- Biochemical Abnormalities: Specific molecular defects (enzyme deficiencies, receptor dysfunction, ion channel defects)
Search first: BRENDA, UniProt, KEGG, OMIM, PubMed
- Epigenetic Changes: DNA methylation, histone modifications affecting gene expression in disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Molecular Profiling (if available):
- Transcriptomics/gene expression changes > Search first: GEO (Gene Expression Omnibus), ArrayExpress, GTEx, Human Cell Atlas, SRA
- Proteomics findings > Search first: PRIDE, ProteomeXchange, Human Protein Atlas, STRING, BioGRID
- Metabolomics signatures > Search first: MetaboLights, Metabolomics Workbench, HMDB, METLIN
- Lipidomics alterations > Search first: LIPID MAPS, SwissLipids, LipidHome, Metabolomics Workbench
- Genomic structural features > Search first: UCSC Genome Browser, Ensembl, NCBI, dbVar, DGV
- Advanced Technologies (if applicable):
- Single-cell analysis findings (cell-type specific mechanisms, cellular heterogeneity) > Search first: Human Cell Atlas, Single Cell Portal, GEO, CELLxGENE
- Spatial transcriptomics findings > Search first: GEO, Spatial Research, Vizgen, 10x Genomics data
- Multi-omics integration results > Search first: TCGA, ICGC, cBioPortal, LinkedOmics, PubMed
- Functional genomics screens (CRISPR, RNAi) > Search first: DepMap, GenomeRNAi, PubMed, BioGRID ORCS
For each mechanism, describe: - The causal chain from initial trigger to clinical manifestation - Which mechanisms are upstream vs downstream - What cell types and biological processes are involved - Suggest GO terms for biological processes and CL terms for cell types
7. Anatomical Structures Affected
- Organ Level:
- Primary organs directly affected
- Secondary organ involvement (complications, secondary effects)
- Body systems involved (cardiovascular, nervous, digestive, respiratory, endocrine, etc.)
Search first: Uberon, FMA (Foundational Model of Anatomy), OMIM, HPO, ICD-11, MeSH, SNOMED CT
- Tissue and Cell Level:
- Specific tissue types affected (epithelial, connective, muscle, nervous)
- Specific cell populations targeted (with Cell Ontology terms)
Search first: Uberon, Human Protein Atlas, Cell Ontology, Human Cell Atlas, CellMarker, PanglaoDB
- Subcellular Level:
- Cellular compartments involved (mitochondria, nucleus, ER, lysosomes) (with GO Cellular Component terms)
Search first: Gene Ontology (Cellular Component), UniProt, Human Protein Atlas
- Localization:
- Specific anatomical sites (with UBERON terms) > Search first: FMA, Uberon, NeuroNames (for brain), SNOMED CT
- Lateralization (unilateral, bilateral, asymmetric) > Search first: HPO, clinical literature, imaging databases
8. Temporal Development
- Onset:
- Typical age of onset (congenital, pediatric, adult, geriatric)
- Onset pattern (acute, subacute, chronic, insidious)
Search first: OMIM, Orphanet, HPO, PubMed
- Progression:
- Disease stages (early, intermediate, advanced, end-stage) > Search first: Cancer Staging Manual (AJCC), WHO classifications, PubMed
- Progression rate (rapid, slow, variable)
- Disease course pattern (episodic, relapsing-remitting, progressive, stable)
- Disease duration (self-limited, chronic lifelong)
Search first: Disease registries, longitudinal cohort databases, natural history studies, PubMed, Orphanet, OMIM
- Patterns:
- Remission patterns (spontaneous, treatment-induced) > Search first: Clinical trial databases, disease registries, PubMed
- Critical periods (time windows of vulnerability or opportunity for intervention) > Search first: PubMed, developmental biology databases, clinical guidelines
9. Inheritance and Population
- Epidemiology:
- Prevalence (cases per 100,000 at given time)
- Incidence (new cases per 100,000 per year)
Search first: Orphanet, CDC, WHO, GBD (Global Burden of Disease), national registries, SEER, disease registries
- For Genetic Etiology:
- Inheritance pattern (AD, AR, X-linked, mitochondrial, multifactorial, polygenic) > Search first: OMIM, Orphanet, ClinVar, GTR (Genetic Testing Registry)
- Penetrance (complete, incomplete, age-dependent) > Search first: ClinVar, OMIM, PubMed, ClinGen
- Expressivity (variable, consistent) > Search first: OMIM, ClinVar, PubMed
- Genetic anticipation (increasing severity in successive generations) > Search first: OMIM, PubMed (especially for repeat expansion disorders)
- Germline mosaicism > Search first: ClinVar, OMIM, genetic counseling literature, PubMed
- Founder effects (population-specific mutations) > Search first: gnomAD, population genetics databases, PubMed
- Consanguinity role > Search first: OMIM, population studies, genetic counseling resources
- Carrier frequency > Search first: gnomAD, carrier screening databases, GeneReviews, GTR
- Population Demographics:
- Affected populations (ethnic or demographic groups with higher prevalence) > Search first: gnomAD, 1000 Genomes, PAGE Study, PubMed, population registries
- Geographic distribution (endemic areas, regional variation) > Search first: WHO, CDC, GBD, Orphanet, geographic epidemiology databases
- Geographic distribution of specific variants
- Sex ratio (male:female) > Search first: Disease registries, OMIM, PubMed, epidemiological databases
- Age distribution of affected individuals > Search first: CDC, disease registries, SEER, Orphanet
10. Diagnostics
- Clinical Tests:
- Laboratory tests (blood, urine, tissue chemistry, specific enzyme assays) > Search first: LOINC, LabTests Online, PubMed
- Biomarkers (proteins, metabolites, genetic markers, circulating biomarkers) > Search first: FDA Biomarker List, BEST (Biomarkers, EndpointS, and other Tools), PubMed
- Imaging studies (X-ray, CT, MRI, PET, ultrasound) > Search first: RadLex, DICOM, Radiopaedia, imaging databases
- Functional tests (pulmonary function, cardiac stress tests) > Search first: LOINC, clinical guidelines, PubMed
- Electrophysiology (EEG, EMG, ECG, nerve conduction studies) > Search first: LOINC, clinical neurophysiology databases, PubMed
- Biopsy findings (histopathology, immunohistochemistry) > Search first: SNOMED CT, College of American Pathologists resources, PubMed
- Pathology findings (microscopic examination) > Search first: SNOMED CT, Digital Pathology databases, PubMed
- Genetic Testing:
Search first: GTR (Genetic Testing Registry), GeneReviews, ClinGen
- Overview of recommended genetic testing approach
- Whole genome sequencing (WGS) utility > Search first: GTR, ClinVar, GEL (Genomics England), gnomAD
- Whole exome sequencing (WES) utility > Search first: GTR, ClinVar, OMIM, GeneMatcher
- Gene panels (which panels, which genes) > Search first: GTR, ClinVar, laboratory-specific databases
- Single gene testing > Search first: GTR, ClinVar, OMIM, GeneReviews
- Chromosomal microarray (CMA) > Search first: DECIPHER, ClinVar, dbVar, ECARUCA
- Karyotyping > Search first: Chromosome Abnormality Database, ClinVar, cytogenetics resources
- FISH > Search first: ClinVar, cytogenetics databases, PubMed
- Mitochondrial DNA testing > Search first: MITOMAP, MSeqDR, ClinVar, GTR
- Repeat expansion testing > Search first: GTR, ClinVar, repeat expansion databases, PubMed
- Omics-Based Diagnostics (if applicable):
- RNA sequencing / transcriptomics > Search first: GEO, ArrayExpress, GTEx, RNA-seq databases
- Proteomics > Search first: PRIDE, ProteomeXchange, FDA Biomarker database
- Metabolomics > Search first: MetaboLights, Metabolomics Workbench, HMDB
- Epigenomics > Search first: GEO, ENCODE, Roadmap Epigenomics, MethBase
- Liquid biopsy > Search first: COSMIC, ClinVar, liquid biopsy databases, PubMed
- Clinical Criteria:
- Standardized diagnostic criteria (DSM, ICD, society guidelines) > Search first: DSM-5, ICD-11, clinical society guidelines, UpToDate
- Differential diagnosis (other conditions to rule out, with distinguishing features) > Search first: DynaMed, UpToDate, clinical decision support systems
- Screening:
- Screening methods for asymptomatic individuals (newborn screening, carrier screening, cascade screening) > Search first: ACMG recommendations, CDC newborn screening, GTR
11. Outcome/Prognosis
- Survival and Mortality:
- Survival rate (5-year, 10-year, overall) > Search first: SEER, cancer registries, disease-specific registries, PubMed
- Life expectancy (with and without treatment if applicable) > Search first: Orphanet, disease registries, actuarial databases, PubMed
- Mortality rate > Search first: CDC, WHO, GBD, national mortality databases
- Disease-specific mortality (deaths directly attributable to disease) > Search first: Disease registries, CDC Wonder, GBD, PubMed
- Morbidity and Function:
- Morbidity (disease-related disability and health impacts) > Search first: GBD, WHO, disability databases, PubMed
- Disability outcomes (long-term functional impairments) > Search first: ICF (International Classification of Functioning), disability registries
- Quality of life measures (EQ-5D, SF-36, PROMIS, disease-specific tools) > Search first: EQ-5D database, SF-36, PROMIS, PubMed
- Disease Course:
- Complications (secondary problems: infections, organ failure, etc.) > Search first: ICD codes, disease registries, clinical databases, PubMed
- Recovery potential (likelihood and extent of recovery, with vs without treatment) > Search first: Natural history studies, rehabilitation databases, PubMed
- Prediction:
- Prognostic factors (age, disease severity, biomarkers, treatment response) > Search first: Prognostic models databases, clinical calculators, PubMed
- Prognostic biomarkers (molecular markers predicting disease course) > Search first: FDA Biomarker database, PubMed, cancer prognostic databases
12. Treatment
- Pharmacotherapy:
- Pharmacological treatments (drug names, drug classes, mechanisms of action) > Search first: DrugBank, RxNorm, ATC classification, DailyMed, FDA databases
- Pharmacogenomics (how genetic variants affect drug metabolism, efficacy, toxicity) > Search first: PharmGKB, CPIC (Clinical Pharmacogenetics), FDA Table of PGx Biomarkers
- Advanced Therapeutics:
- Gene therapy (viral vectors, CRISPR, gene replacement, gene editing) > Search first: ClinicalTrials.gov, FDA gene therapy database, ASGCT resources
- Cell therapy (stem cell transplant, CAR-T, cellular therapeutics) > Search first: ClinicalTrials.gov, FDA cell therapy database, FACT standards
- RNA-based therapies (ASOs, siRNA, mRNA therapies) > Search first: ClinicalTrials.gov, FDA approvals, PubMed
- Targeted therapies (treatments directed at specific molecular targets) > Search first: My Cancer Genome, OncoKB, ClinicalTrials.gov, FDA approvals
- Immunotherapies (checkpoint inhibitors, monoclonal antibodies) > Search first: Cancer Immunotherapy Database, FDA approvals, ClinicalTrials.gov
- Surgical and Interventional:
- Surgical interventions (types of surgery, timing, outcomes) > Search first: CPT codes, surgical registries, clinical guidelines, PubMed
- Supportive and Rehabilitative:
- Supportive care (symptom management, pain control, nutrition) > Search first: Clinical guidelines, Cochrane Library, PubMed
- Rehabilitation (physical therapy, occupational therapy, speech therapy) > Search first: Rehabilitation medicine databases, clinical guidelines, PubMed
- Experimental:
- Experimental treatments in clinical trials (with NCT identifiers if available) > Search first: ClinicalTrials.gov, EU Clinical Trials Register, WHO ICTRP
- Treatment Outcomes:
- Treatment response rates > Search first: Clinical trial databases, FDA reviews, systematic reviews, PubMed
- Side effects and adverse events > Search first: FDA Adverse Event Reporting System (FAERS), MedWatch, PubMed
- Treatment Strategy:
- Treatment algorithms (clinical pathways, decision trees) > Search first: Clinical practice guidelines, NCCN Guidelines, UpToDate
- Combination therapies > Search first: ClinicalTrials.gov, treatment guidelines, PubMed
- Personalized medicine approaches (genotype-guided treatment) > Search first: My Cancer Genome, CIViC, PharmGKB, precision medicine databases
For each treatment, suggest MAXO (Medical Action Ontology) terms where applicable.
13. Prevention
- Prevention Levels:
- Primary prevention (preventing disease occurrence: vaccination, risk factor modification) > Search first: CDC, WHO, USPSTF recommendations, Cochrane Library
- Secondary prevention (early detection and treatment: screening programs, early intervention) > Search first: USPSTF, CDC screening guidelines, WHO
- Tertiary prevention (preventing complications in those with disease) > Search first: Clinical guidelines, disease management protocols, PubMed
- Immunization: Vaccine strategies (if applicable)
Search first: CDC vaccine schedules, WHO immunization, FDA vaccine database
- Screening and Early Detection:
- Screening programs (population-based: newborn screening, cancer screening) > Search first: CDC screening programs, USPSTF, cancer screening databases
- Genetic screening (carrier screening, preimplantation genetic diagnosis, prenatal testing) > Search first: ACMG recommendations, ACOG guidelines, GTR
- Risk stratification (identifying high-risk individuals for targeted prevention) > Search first: Risk prediction models, clinical calculators, PubMed
- Behavioral Interventions: Lifestyle modifications to reduce risk
Search first: CDC, WHO, behavioral intervention databases, Cochrane Library
- Counseling: Genetic counseling (risk assessment, family planning guidance)
Search first: NSGC resources, ACMG guidelines, GeneReviews
- Public Health:
- Public health interventions (sanitation, vector control, health education) > Search first: CDC, WHO, public health databases, PubMed
- Environmental interventions (reducing environmental risk factors) > Search first: EPA databases, WHO environmental health, PubMed
- Prophylaxis: Preventive medications or procedures
Search first: Clinical guidelines, FDA approvals, PubMed
14. Other Species / Natural Disease
- Taxonomy: Species affected (with NCBI Taxon identifiers)
Search first: NCBI Taxonomy
- Breed: Specific breeds affected (with VBO identifiers if applicable)
Search first: VBO (Vertebrate Breed Ontology)
- Gene: Orthologous genes in other species (with NCBI Gene IDs)
Search first: NCBI Gene
- Natural Disease:
- Naturally occurring disease in other species (companion animals, wildlife) > Search first: OMIA (Online Mendelian Inheritance in Animals), VetCompass, PubMed
- Veterinary relevance and importance in animal health > Search first: OMIA, veterinary databases, PubMed
- Comparative Biology:
- Comparative pathology (similarities and differences across species) > Search first: OMIA, comparative pathology databases, PubMed
- Evolutionary conservation of disease mechanisms > Search first: HomoloGene, OrthoMCL, Alliance of Genome Resources
- Transmission (if applicable):
- Zoonotic potential > Search first: CDC zoonotic diseases, WHO zoonoses, GIDEON
- Cross-species susceptibility > Search first: NCBI Taxonomy, veterinary databases, PubMed
15. Model Organisms
- Model Types:
- Model organism type (mammalian, invertebrate, cellular, in vitro) > Search first: Alliance of Genome Resources, model organism databases
- Specific model systems (mouse, rat, zebrafish, Drosophila, C. elegans, yeast, cell lines, organoids, iPSCs) > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, SGD, ATCC, Cellosaurus
- Induced models (drug treatment, surgical intervention, environmental manipulation) > Search first: MGI, model organism databases, PubMed
- Genetic Models:
- Types available (knockout, knock-in, transgenic, conditional, humanized) > Search first: MGI, IMPC, KOMP, EuMMCR, IMSR
- Model Characteristics:
- Phenotype recapitulation (how well model reproduces human disease features) > Search first: Model organism databases, comparative studies, PubMed
- Model limitations (aspects of human disease not captured) > Search first: Model organism databases, PubMed, review articles
- Applications:
- Research applications (what aspects of disease can be studied) > Search first: Model organism databases, PubMed
- Resources:
- Model databases > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, IMSR, EMMA, MMRRC
Citation Requirements
- Cite primary literature (PMID preferred) for all mechanistic and clinical claims
- Prioritize recent reviews and landmark papers
- Include direct quotes from abstracts where possible to support key statements
- Distinguish evidence source types: human clinical, model organism, in vitro, computational
Output Format
Structure your response as a comprehensive narrative organized by the sections above. For each section, provide: - Factual content with specific details (numbers, percentages, gene names, variant nomenclature) - Ontology term suggestions (HPO, GO, CL, UBERON, CHEBI, MAXO, MONDO) where applicable - Evidence citations with PMIDs - Direct quotes from abstracts to support key claims - Clear indication when information is not available or not applicable for this disease
This report will be used to populate a disease knowledge base entry with: - Pathophysiology descriptions with causal chains - Gene/protein annotations (HGNC, GO terms) - Phenotype associations (HP terms) with frequencies - Cell type involvement (CL terms) - Anatomical locations (UBERON terms) - Chemical entities (CHEBI terms) - Treatment annotations (MAXO terms) - Evidence items with PMIDs and exact abstract quotes - Epidemiology, prognosis, diagnostic, and prevention information - Animal model descriptions with phenotype recapitulation details
Comprehensive Disease Characteristics Report: MALT Lymphoma (Extranodal Marginal Zone Lymphoma of Mucosa‑Associated Lymphoid Tissue)
Target disease
- Disease name: MALT lymphoma (Extranodal marginal zone B‑cell lymphoma of mucosa‑associated lymphoid tissue; EMZL/MALT)
- MONDO ID: Not found in the retrieved full-text evidence (not inferred).
- Category: Indolent B‑cell non‑Hodgkin lymphoma (marginal zone lymphoma subtype) (walewska2023guidelineforthe pages 2-2).
1. Disease information
Overview (current understanding)
MALT lymphoma is an indolent extranodal marginal zone B‑cell lymphoma that arises from marginal zone B cells in acquired mucosa-associated lymphoid tissue that develops under chronic antigenic stimulation (infection or autoimmunity) (raderer2023clinicalrelevanceof pages 1-2, alderuccio2023enhancingprognosticationand pages 1-3, walewska2023guidelineforthe pages 2-2).
- Classification: WHO 5th edition recognizes marginal zone lymphoma subtypes including EMZL/MALT (walewska2023guidelineforthe pages 2-2).
- Relative frequency: EMZL/MALT accounts for >60% of marginal zone lymphomas (walewska2023guidelineforthe pages 2-2). In broader lymphoma epidemiology, MALT lymphoma has been reported as ~5–8% of adult lymphoma diagnoses (raderer2023clinicalrelevanceof pages 1-2).
- Common primary sites (site distribution varies by region): stomach (~30–40%), ocular adnexa (~12–24%), lung (~9–11%), salivary/parotid (~7–11%), and skin (~10%) (raderer2023clinicalrelevanceof pages 1-2, alderuccio2023enhancingprognosticationand pages 1-3).
Synonyms / alternative names
- Extranodal marginal zone lymphoma (EMZL)
- Extranodal marginal zone B‑cell lymphoma of mucosa-associated lymphoid tissue
- MALT lymphoma
- Gastric MALT lymphoma (site-specific form) (matysiakbudnik2023clinicalmanagementof pages 1-2).
Key identifiers (availability in current evidence)
The retrieved papers did not contain specific ICD‑10/ICD‑11, MeSH, OMIM, Orphanet, or MONDO codes in the accessible text excerpts; therefore, identifiers are not reported here to avoid incorrect mapping.
Data provenance
The information summarized is derived from aggregated disease-level resources (guidelines, systematic reviews, multi-center/real-world cohorts, and mechanistic studies) rather than individual EHR extracts (walewska2023guidelineforthe pages 9-9, lemos2023effectivenessofhelicobacter pages 1-3, min2023longtermclinicaloutcomes pages 7-8, tsai2024cooperativeparticipationof pages 1-2).
Representative abstract quote (definition): A 2023 review describes EMZL/MALT as “an indolent lymphoma originating from marginal zone B‑cells and associated with chronic inflammation” (alderuccio2023enhancingprognosticationand pages 1-3).
2. Etiology
Primary causal factors (infectious / inflammatory)
MALT lymphomagenesis is strongly linked to chronic antigenic stimulation at the involved mucosal site, with subsequent acquisition of genetic alterations that often converge on NF‑κB signaling (raderer2023clinicalrelevanceof pages 1-2, alderuccio2023enhancingprognosticationand pages 1-3).
Gastric MALT lymphoma (GML)
- Helicobacter pylori is a central etiologic driver; a British Society of Haematology (BSH) guideline reports H. pylori implicated in ~38–85% of gastric MALT cases (walewska2023guidelineforthe pages 3-3).
- Non‑H. pylori Helicobacter species and other microbial/autoimmune contexts contribute to “true” H. pylori-negative disease, which is reported in ~10–40% of cases (matysiakbudnik2023clinicalmanagementof pages 7-8).
Site-specific infectious associations (examples from guideline synthesis)
- Intestinal MALT: association with Campylobacter jejuni (up to 50%) in some contexts (walewska2023guidelineforthe pages 3-3).
- Ocular adnexal MALT: geographic association with Chlamydia psittaci (variable by region) (alderuccio2023enhancingprognosticationand pages 17-19).
- Hepatic MALT: associations reported with hepatitis C (23%), hepatitis B, and other viral hepatitis (walewska2023guidelineforthe pages 3-3).
Autoimmune risk contexts
Autoimmune disorders create chronic inflammatory niches and are repeatedly cited as associated contexts for EMZL/MALT, including Sjögren’s syndrome and Hashimoto thyroiditis (alderuccio2023enhancingprognosticationand pages 1-3, alderuccio2023enhancingprognosticationand pages 17-19).
Protective factors
The retrieved evidence did not provide validated protective genetic variants or environmental protective factors specific to MALT lymphoma.
Gene–environment interaction (clinically important example)
A major gene–environment interaction in MALT lymphoma is the transition from antigen-dependent (infection-driven) growth to antigen-independent growth mediated by tumor genetics: - t(11;18)(q21;q21)/BIRC3::MALT1 (API2–MALT1) is associated with poor response to H. pylori eradication and more disseminated gastric disease, suggesting reduced dependence on H. pylori-driven stimulation (raderer2023clinicalrelevanceof pages 1-2, matysiakbudnik2023clinicalmanagementof pages 8-9).
3. Phenotypes (clinical presentation) and HPO mapping
General phenotype pattern
MALT lymphoma is typically indolent, often localized, and symptoms may reflect the involved organ rather than systemic B symptoms (alderuccio2023enhancingprognosticationand pages 1-3, matysiakbudnik2023clinicalmanagementof pages 8-9).
Gastric MALT lymphoma
- Symptoms/signs: nonspecific upper GI symptoms such as dyspepsia/ulcer-like symptoms (matysiakbudnik2023clinicalmanagementof pages 1-2).
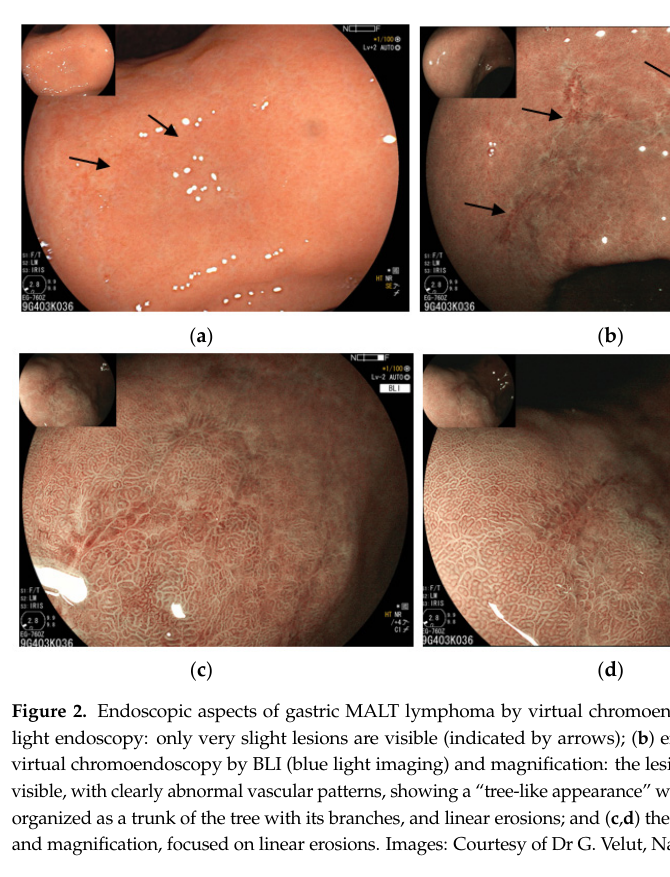
- Endoscopic phenotype: wide range from normal-appearing mucosa to erythema, nodularity, thickened folds, ulcers, or mass-like lesions; advanced imaging may show an abnormal vascular pattern described as “tree-like appearance” (matysiakbudnik2023clinicalmanagementof pages 2-4, matysiakbudnik2023clinicalmanagementof media 18e4f906).
- Stage at diagnosis: most cases are localized; one review notes >90% are stage I–II (matysiakbudnik2023clinicalmanagementof pages 8-9).
Suggested HPO terms (examples): - Dyspepsia (HP:0100749) - Epigastric pain (HP:0030819) - Gastric ulcer (HP:0002592) - Nausea (HP:0002018) - Gastrointestinal hemorrhage (HP:0002239) (when present)
Ocular adnexal / conjunctival MALT lymphoma (high-level)
Ocular adnexal MALT is a common extranodal site; site biology and prognosis vary, and infections/IgG4-related disease can be part of differential/associated context (walewska2023guidelineforthe pages 3-3, alderuccio2023enhancingprognosticationand pages 4-6).
Suggested HPO terms (site-dependent; examples): - Conjunctival mass (HP:0100787) - Proptosis (HP:0000520) - Diplopia (HP:0000651)
Quality-of-life impact
The retrieved evidence did not provide validated QoL instrument data (e.g., EQ‑5D/SF‑36) specific to MALT lymphoma; however, the BSH guideline emphasizes monitoring toxicity via patient-reported outcomes in trials and practice contexts (alderuccio2023enhancingprognosticationand pages 16-17).
4. Genetic / molecular information
Key molecular concept
Across sites, many genetic changes dysregulate pathways leading to NF‑κB activation, consistent with a chronic inflammation/antigen stimulation model (raderer2023clinicalrelevanceof pages 1-2, alderuccio2023enhancingprognosticationand pages 1-3).
Recurrent chromosomal abnormalities (examples)
- t(11;18)(q21;q21)/BIRC3::MALT1 (API2–MALT1): ~24% gastric and ~40% pulmonary in a 2023 critical appraisal; gastric guideline ranges ~6–26% (raderer2023clinicalrelevanceof pages 1-2, walewska2023guidelineforthe pages 3-3).
- t(14;18)(q32;q21)/IGH::MALT1: ~1–5% in gastric disease (walewska2023guidelineforthe pages 3-3).
- Trisomy 3 (~11%) and trisomy 18 (~6%) in gastric disease (walewska2023guidelineforthe pages 3-3).
Somatic mutations and pathway alterations (site-dependent)
The 2023 expert review highlights recurrent alterations in ocular adnexal EMZL (e.g., CABIN1, RHOA, TBL1XR1, CREBBP) and TNFAIP3 inactivation, with frequent concurrent BCR and NF‑κB pathway lesions (alderuccio2023enhancingprognosticationand pages 4-6).
Molecular predictors of therapy response (recent emphasis)
- API2–MALT1 fusion predicts poor response to H. pylori eradication and is an independent predictor in a 2024 cohort examining endoscopic morphology and eradication response (OR ~12.18) (yang2024endoscopicmorphologyof pages 1-2).
- A 2023 critical appraisal notes emerging data suggesting alterations in TNFAIP3 (A20), KMT2D, CARD11 may relate to response to BTK inhibitors (raderer2023clinicalrelevanceof pages 1-2).
Epigenetics
No comprehensive epigenomic profiling (methylation/histone) for MALT lymphoma was retrievable in the current evidence excerpts; Tsai et al. note that some lymphomas show epigenetic suppression of the NFATC1 promoter (contextual statement) (tsai2024cooperativeparticipationof pages 15-16).
Ontology suggestions
- GO biological process: NF‑κB signaling (GO:0043122), B‑cell receptor signaling (GO:0050853), chronic inflammatory response (GO:0002544), lymphocyte proliferation (GO:0046651), regulation of apoptotic process (GO:0042981) (mechanistic convergence described in reviews) (raderer2023clinicalrelevanceof pages 1-2, alderuccio2023enhancingprognosticationand pages 1-3).
- Cell Ontology (CL): marginal zone B cell (CL:0000900), memory B cell (CL:0000787), plasma cell (CL:0000786) (plasma-cell differentiation noted in gastric MALT) (matysiakbudnik2023clinicalmanagementof pages 4-7).
5. Environmental information
Environmental/lifestyle factors
No robust lifestyle/environmental exposure risk factors (e.g., smoking, diet) specific to MALT lymphoma were identified in the retrieved evidence.
Infectious agents (key non-genetic environmental contributors)
Primary environmental drivers are infectious/inflammatory exposures: - Helicobacter pylori (gastric) - Non‑H. pylori Helicobacter species (subset of “true” H. pylori-negative gastric MALT) - Campylobacter jejuni (intestinal) - Chlamydia psittaci (ocular adnexal; geographic variation) - HCV/HBV (hepatic/extranodal contexts) (walewska2023guidelineforthe pages 3-3, matysiakbudnik2023clinicalmanagementof pages 7-8).
6. Mechanism / pathophysiology
Conceptual causal chain (current model)
- Chronic antigenic stimulation (infection/autoimmunity) induces acquired MALT and sustained B‑cell activation via BCR/CD40 signaling.
- Genetic events accumulate (translocations, trisomies, NF‑κB regulators), shifting from antigen-dependent to antigen-independent survival and proliferation.
- NF‑κB pathway dysregulation and related survival programs maintain the malignant clone (raderer2023clinicalrelevanceof pages 1-2, alderuccio2023enhancingprognosticationand pages 1-3).
2024 mechanistic development: CagA–calcineurin–NFATc1 axis (antibiotic-responsive gastric MALT)
A 2024 mechanistic study (Tsai et al., Cancer Cell International, Nov 2024; https://doi.org/10.1186/s12935-024-03552-6) provides a model linking H. pylori virulence factor CagA to host signaling and clinical response: - In vitro co-culture model: B-lymphoma cell lines (MA-1, OCI-Ly3, OCI-Ly7, etc.) exposed to patient-derived H. pylori strains; CagA becomes tyrosine-phosphorylated and translocates to the nucleus, coinciding with NFATc1 dephosphorylation and nuclear translocation; this was linked to signaling (p-SHP-2/p-ERK/Bcl-xL) and induction of p21/p27 with G1 cell-cycle retardation (tsai2024cooperativeparticipationof pages 1-2, tsai2024cooperativeparticipationof pages 4-6). - Drug perturbation: NFATc1 nuclear translocation depended on calcineurin (blocked by cyclosporine A), and clarithromycin reduced CagA/p-CagA and reversed NFATc1 nuclear localization (tsai2024cooperativeparticipationof pages 4-6). - Clinical correlation (n=91): nuclear NFATc1 associated with tumor CagA presence (80% vs 33%, p<0.001) and with H. pylori eradication responsiveness (73% vs 25%, p<0.001); CagA expression independently associated with response (OR ~11.9, p<0.001), with combined CagA+NFATc1 high PPV (~90.5%) and specificity (~87.5%) (tsai2024cooperativeparticipationof pages 1-2, tsai2024cooperativeparticipationof pages 11-13).
Implication: This provides a mechanistic explanation for a subset of “antibiotic-responsive” gastric MALT lymphoma, where bacterial factors directly modulate lymphoma cell signaling and cell-cycle programs, and suggests potential biomarkers (CagA, NFATc1 localization) for predicting eradication response (tsai2024cooperativeparticipationof pages 11-13).
7. Anatomical structures affected
Organ-level sites (common primary sites)
Common primary sites include stomach, ocular adnexa, lung, salivary glands, and skin (raderer2023clinicalrelevanceof pages 1-2, alderuccio2023enhancingprognosticationand pages 1-3).
Suggested UBERON terms (examples): - Stomach (UBERON:0000945) - Conjunctiva (UBERON:0000970) - Lacrimal gland (UBERON:0001817) - Lung (UBERON:0002048) - Major salivary gland (UBERON:0001830) - Skin (UBERON:0002097)
Tissue/cell-level localization
Tumors are composed of heterogeneous small B cells with marginal zone/centrocyte-like morphology (walewska2023guidelineforthe pages 2-2), infiltrating mucosa-associated lymphoid structures (acquired MALT).
Dissemination patterns (available evidence)
- Gastric disease is commonly localized (often stage I/II), and bone marrow involvement is uncommon (~4.3%) (walewska2023guidelineforthe pages 7-7, matysiakbudnik2023clinicalmanagementof pages 8-9).
- t(11;18)/BIRC3::MALT1 is associated with more disseminated gastric disease (raderer2023clinicalrelevanceof pages 1-2).
8. Temporal development
Onset and course
MALT lymphoma is typically indolent, with prolonged natural history and frequent presentation at localized stage (raderer2023clinicalrelevanceof pages 1-2, matysiakbudnik2023clinicalmanagementof pages 8-9).
Staging systems (gastric)
- Lugano (1994) classification is widely used in UK practice (walewska2023guidelineforthe pages 7-7).
- Modified Ann Arbor may be used to incorporate depth of infiltration (walewska2023guidelineforthe pages 7-7).
- A gastroenterology-focused review recommends Paris classification (TNM-like with depth assessed by endoscopic ultrasound) because depth of invasion predicts H. pylori eradication response (matysiakbudnik2023clinicalmanagementof pages 8-9).
Response kinetics after eradication
- Complete remission after eradication may be delayed; guideline notes late responses up to one year (walewska2023guidelineforthe pages 9-9).
9. Inheritance and population
Inheritance
MALT lymphoma is not described as a Mendelian inherited disorder in the retrieved evidence; it is primarily a somatic malignancy driven by acquired genetic lesions in the context of chronic inflammation (raderer2023clinicalrelevanceof pages 1-2).
Epidemiology (available data; limitations)
- Relative frequency among lymphomas: MALT lymphoma represents ~5–8% of adult lymphoma diagnoses (raderer2023clinicalrelevanceof pages 1-2).
- Geography: relatively more frequent in Asia (China/Korea noted) (raderer2023clinicalrelevanceof pages 1-2).
Not available from current evidence: incidence per 100,000/year, prevalence, sex ratio, and age distributions from registries (e.g., SEER/GBD). These are important for a knowledge base but were not extractable from retrieved full text here.
10. Diagnostics
Core diagnostic approach
- Upper endoscopy with biopsy is central for gastric disease; one review recommends ≥10 biopsies from lesions and surrounding mucosa (matysiakbudnik2023clinicalmanagementof pages 4-7).
- Endoscopic appearance is often nonspecific; advanced modalities (NBI/BLI) can show a “tree-like appearance” vascular pattern (matysiakbudnik2023clinicalmanagementof pages 2-4, matysiakbudnik2023clinicalmanagementof media 18e4f906).
Histopathology
Typical gastric MALT histology includes marginal-zone pattern infiltration around B‑cell follicles with confluent sheets and lymphoepithelial lesions; plasma cell differentiation occurs in up to ~33% (matysiakbudnik2023clinicalmanagementof pages 4-7).
Immunophenotype (key markers to include/exclude mimics)
Typical phenotype described for gastric MALT: - CD20+, BCL2+, CD10−, BCL6−, CD5−, cyclin D1−, SOX11−, CD23−, IgD−, usually IgM+; low Ki‑67 (matysiakbudnik2023clinicalmanagementof pages 4-7). Guideline emphasizes IHC is primarily used to exclude other small B‑cell lymphomas because “no widely specific diagnostic markers for MZL” exist (walewska2023guidelineforthe pages 2-2).
Molecular testing
- FISH for t(11;18)(q21;q21)/BIRC3::MALT1 is recommended in all gastric cases in the BSH guideline because it correlates with advanced disease and reduced response to eradication (walewska2023guidelineforthe pages 7-7).
- PCR for clonality can support diagnosis but must be interpreted carefully in chronic inflammation contexts (walewska2023guidelineforthe pages 2-3).
Imaging/staging
- FDG-PET avidity in gastric MALT is variable (~50–60%) and PET is mainly used when transformation is suspected or when baseline FDG avidity is present (walewska2023guidelineforthe pages 7-7).
11. Outcomes / prognosis
Survival
BSH guideline synthesis: overall gastric EMZL/MALT prognosis is excellent with >90% 5‑year survival and ~75–80% 10‑year survival (walewska2023guidelineforthe pages 9-9).
Response and relapse statistics (recent evidence)
- H. pylori eradication (early-stage H. pylori-positive gastric MALT): 2023 proportional meta-analysis (2,936 eradicated patients) reported pooled complete histopathologic remission 75.18% (95% CI 70.45–79.91) (lemos2023effectivenessofhelicobacter pages 1-3).
- Real-world cohort (2023, single-center): complete remission after eradication in localized H. pylori-positive disease 77.8% (112/144) (min2023longtermclinicaloutcomes pages 7-8).
- Radiotherapy (H. pylori-negative or eradication-failure settings): 2023 real-world series reports 100% CR in an H. pylori-negative first-line RT cohort and better long-term PFS than chemotherapy in that dataset (min2023longtermclinicaloutcomes pages 7-8).
Transformation risk (2024 emphasis)
A 2024 prospective cohort and meta-analysis reported pooled histologic transformation cumulative incidence in MZL overall of ~5% at 5 years and ~8% at 10 years; for EMZL/MALT approximately ~3% at 5 years and ~5% at 10 years (bommier2024transformationinmarginal pages 1-2). Transformation was associated with an approximately 3.95-fold increased risk of death (bommier2024transformationinmarginal pages 1-2).
12. Treatment (current practice and real-world implementation)
First-line (localized gastric disease)
- H. pylori eradication is recommended as first-line therapy for localized gastric MALT lymphoma, including in many guidelines even when H. pylori-negative by testing (European guideline perspective described) (matysiakbudnik2023clinicalmanagementof pages 1-2, matysiakbudnik2023clinicalmanagementof pages 8-9).
- BSH guideline reports ~62% CR by 12 months after eradication, with late responses up to one year (walewska2023guidelineforthe pages 9-9).
Second-line / localized H. pylori-negative or eradication-resistant disease
- Involved-site radiotherapy is a key definitive option; guideline notes modern series support dose reduction (e.g., 24 Gy) with low toxicity (walewska2023guidelineforthe pages 9-9).
Systemic therapy (advanced, symptomatic, or refractory)
- Systemic therapy is reserved for disseminated, symptomatic, deeply invasive, or transformed cases (walewska2023guidelineforthe pages 9-9, walewska2023guidelineforthe pages 10-10).
- A 2023 real-world gastric cohort reported first-line R‑CVP chemotherapy CR 81.5%, but with substantial hematologic toxicity (e.g., neutropenia 70.4%) (min2023longtermclinicaloutcomes pages 8-9).
Targeted agents / recent developments
- Recent molecular appraisal suggests TNFAIP3/KMT2D/CARD11 alterations may associate with response to BTK inhibitors, though evidence is not yet sufficient for routine biomarker-driven decisions (raderer2023clinicalrelevanceof pages 1-2).
MAXO (Medical Action Ontology) suggestions
- Helicobacter pylori eradication therapy (antibiotic therapy) (MAXO:0000155; general)
- External beam radiotherapy (MAXO:0000014)
- Anti-CD20 monoclonal antibody therapy (rituximab) (MAXO:0000754; general immunotherapy category)
- Chemoimmunotherapy (MAXO:0000747; general)
13. Prevention
Primary prevention
No population-level primary prevention trials specific to MALT lymphoma were found in the retrieved evidence; however, infection control (H. pylori diagnosis/treatment) is central to reducing chronic gastritis-associated lymphomagenesis in gastric disease contexts (matysiakbudnik2023clinicalmanagementof pages 1-2, matysiakbudnik2023clinicalmanagementof pages 8-9).
Secondary/tertiary prevention (surveillance)
- Gastric MALT lymphoma requires endoscopic and histologic surveillance after therapy; response assessment is endoscopic/histologic (GELA scoring is referenced as surveillance tool after eradication) (matysiakbudnik2023clinicalmanagementof pages 7-8, matysiakbudnik2023clinicalmanagementof pages 8-9).
- BSH guideline recommends repeat OGD and biopsies (often at 3–6 months) to assess response post-eradication; serology can remain positive up to 2 years and is not useful to confirm eradication (walewska2023guidelineforthe pages 9-9).
14. Other species / natural disease
The retrieved evidence did not provide veterinary natural history of MALT lymphoma in other species.
15. Model organisms and experimental systems
In vitro models (2024)
Tsai et al. used B‑lymphoma cell lines co-cultured with patient-derived H. pylori strains to define the CagA–NFATc1 signaling axis and its suppression by clarithromycin or calcineurin inhibition (tsai2024cooperativeparticipationof pages 4-6).
Mouse model context
Tsai et al. note experimental evidence that transgenic mouse expression of CagA can drive gastrointestinal and hematopoietic neoplasms, supporting a causal role for bacterial virulence factors in lymphomagenesis (tsai2024cooperativeparticipationof pages 15-16).
Key visual evidence (endoscopy)
Endoscopic phenotypes of gastric MALT lymphoma, including the “tree-like appearance” vascular pattern under enhanced imaging, are shown in the cited figures (matysiakbudnik2023clinicalmanagementof media 18e4f906).
Structured summary table
| Domain | Key points | Key recent sources (URL; publication date) | Evidence citation IDs |
|---|---|---|---|
| Definition/Identifiers | MALT lymphoma is an indolent extranodal marginal zone B-cell lymphoma arising from marginal zone B cells in acquired mucosa-associated lymphoid tissue under chronic antigenic stimulation. It accounts for >60% of marginal zone lymphomas and up to ~8% of newly diagnosed lymphomas. Common primary sites include stomach (~30–40%), ocular adnexa (~12–24%), skin (~10%), lung (~9–11%), and salivary gland (~7–11%). | Raderer et al., Ther Adv Med Oncol; https://doi.org/10.1177/17588359231183565; Jan 2023. Alderuccio & Lossos, Expert Rev Hematol; https://doi.org/10.1080/17474086.2023.2206557; Apr 2023. Walewska et al., Br J Haematol; https://doi.org/10.1111/bjh.19064; Nov 2023. | (raderer2023clinicalrelevanceof pages 1-2, alderuccio2023enhancingprognosticationand pages 1-3, walewska2023guidelineforthe pages 2-2) |
| Etiology | Strongly linked to chronic inflammation/infection. Gastric disease is associated with Helicobacter pylori in ~38–85% of cases; H. heilmannii <1%. Other site-specific associations include Campylobacter jejuni (up to 50%) in intestinal disease, Chlamydia psittaci in ocular adnexal disease (geographically variable), and autoimmune disorders such as Sjögren syndrome and Hashimoto thyroiditis. HCV is reported in some hepatic/other extranodal cases. | Walewska et al.; https://doi.org/10.1111/bjh.19064; Nov 2023. Alderuccio & Lossos; https://doi.org/10.1080/17474086.2023.2206557; Apr 2023. Matysiak-Budnik et al.; https://doi.org/10.3390/cancers15153811; Jul 2023. | (walewska2023guidelineforthe pages 3-3, alderuccio2023enhancingprognosticationand pages 17-19, matysiakbudnik2023clinicalmanagementof pages 16-17, matysiakbudnik2023clinicalmanagementof pages 1-2) |
| Molecular genetics | Recurrent lesions converge on NF-κB activation. The translocation t(11;18)(q21;q21)/BIRC3::MALT1 (API2-MALT1) is relatively specific and occurs in ~24% of gastric and ~40% of pulmonary MALT lymphoma; in gastric disease guideline tables report ~6–26%. It is associated with more disseminated disease and poor response to H. pylori eradication. Other recurrent abnormalities include t(14;18)(IGH::MALT1) ~1–5%, trisomy 3 ~11%, trisomy 18 ~6%, and TNFAIP3/A20 inactivation ~5–18% in gastric MALT. | Raderer et al.; https://doi.org/10.1177/17588359231183565; Jan 2023. Walewska et al.; https://doi.org/10.1111/bjh.19064; Nov 2023. Yang et al.; https://doi.org/10.1186/s43556-023-00141-3; Sep 2023. | (raderer2023clinicalrelevanceof pages 1-2, walewska2023guidelineforthe pages 3-3, yang2023extranodallymphomapathogenesis pages 28-29, matysiakbudnik2023clinicalmanagementof pages 4-7, walewska2023guidelineforthe pages 7-7) |
| Diagnostics | Diagnosis is biopsy-based. Recommended gastric workup includes upper endoscopy with biopsies; at least 10 biopsies from lesions and surrounding mucosa are suggested. Histology shows marginal-zone pattern infiltration with lymphoepithelial lesions; plasma cell differentiation may be seen in up to ~33%. Typical immunophenotype: CD20+, BCL2+, CD10−, BCL6−, CD5−, cyclin D1−, SOX11−, CD23−, IgD−, usually IgM+. FISH for t(11;18) is recommended in all gastric cases in the BSH guideline. Bone marrow involvement is uncommon (~4.3%), so marrow biopsy is not routine unless cytopenias are present. FDG-PET avidity is variable (~50–60%). | Matysiak-Budnik et al.; https://doi.org/10.3390/cancers15153811; Jul 2023. Walewska et al.; https://doi.org/10.1111/bjh.19064; Nov 2023. Alderuccio & Lossos; https://doi.org/10.1080/17474086.2023.2206557; Apr 2023. | (matysiakbudnik2023clinicalmanagementof pages 4-7, walewska2023guidelineforthe pages 7-7, walewska2023guidelineforthe pages 2-3, alderuccio2023enhancingprognosticationand pages 1-3, matysiakbudnik2023clinicalmanagementof pages 2-4) |
| Treatment/outcomes | For early-stage H. pylori-positive gastric MALT, eradication is first-line. A 2023 meta-analysis of 2,936 successfully eradicated H. pylori-positive patients found pooled complete histopathologic remission 75.18% (95% CI 70.45–79.91). The 2023 BSH guideline notes ~62% CR by 12 months after eradication, with late responses up to 1 year. In a 2023 real-world series, CR after eradication in localized H. pylori-positive disease was 77.8% (112/144). Radiotherapy for H. pylori-independent/localized disease achieved 100% CR in H. pylori-negative first-line cohorts in that study; older referenced RT series reported 5- and 10-year OS 94% and 79%, and the BSH guideline summarizes overall prognosis as >90% 5-year survival and 75–80% 10-year survival. | Lemos et al., World J Gastroenterol; https://doi.org/10.3748/wjg.v29.i14.2202; Apr 2023. Min et al., Ann Hematol; https://doi.org/10.1007/s00277-023-05130-8; Feb 2023. Walewska et al.; https://doi.org/10.1111/bjh.19064; Nov 2023. | (walewska2023guidelineforthe pages 9-9, min2023longtermclinicaloutcomes pages 8-9, lemos2023effectivenessofhelicobacter pages 1-3, min2023longtermclinicaloutcomes pages 7-8) |
| Transformation | Histologic transformation is uncommon but clinically important. In the 2024 prospective cohort/meta-analysis of MZL, pooled cumulative incidence was ~5% at 5 years and ~8% at 10 years overall; for EMZL/MALT, pooled incidence was about ~3% at 5 years and ~5% at 10 years. Transformation was associated with a 3.95-fold increased risk of death. Reported predictors included ≥2 extranodal sites, Ann Arbor stage III/IV, elevated LDH, and MALT-IPI ≥2. | Bommier et al., Blood Advances; https://doi.org/10.1182/bloodadvances.2024013188; Nov 2024. Alderuccio & Lossos; https://doi.org/10.1080/17474086.2023.2206557; Apr 2023. | (bommier2024transformationinmarginal pages 8-9, bommier2024transformationinmarginal pages 5-6, bommier2024transformationinmarginal pages 1-2, alderuccio2023enhancingprognosticationand pages 20-21) |
Table: This table summarizes high-yield, evidence-supported facts on MALT lymphoma across definition, etiology, molecular genetics, diagnosis, treatment, and transformation. It prioritizes 2023–2024 sources and includes quantitative findings and context IDs for traceability.
Expert opinion and analysis (synthesis of authoritative sources)
- Clinical heterogeneity is site-driven: EMZL/MALT is best conceptualized as a family of related indolent lymphomas where infectious/autoimmune context, genomic lesions, and prognosis differ by organ site; therefore, “one-biomarker-fits-all” stratification remains challenging (raderer2023clinicalrelevanceof pages 1-2, alderuccio2023enhancingprognosticationand pages 1-3).
- Antigen dependence versus independence guides management: eradication is first-line even though genetic testing is not mandatory upfront; however, translocations such as t(11;18) explain why a clinically important subset is eradication-refractory and may need RT/systemic therapy (raderer2023clinicalrelevanceof pages 1-2, walewska2023guidelineforthe pages 9-9).
- A 2024 mechanistic advance ties bacterial virulence to treatment response: the CagA–NFATc1 pathway provides a plausible mechanistic basis for “antibiotic-responsive” tumors and suggests biomarker development for precision eradication strategies (tsai2024cooperativeparticipationof pages 11-13, tsai2024cooperativeparticipationof pages 4-6).
Evidence gaps relative to the template (not found in current retrieved evidence)
- MONDO/MeSH/ICD identifiers.
- Population incidence/prevalence per 100,000, sex ratio, and robust age distribution.
- Validated protective factors and formal gene–environment interaction models beyond treatment-resistance genetics.
- Standardized QoL statistics and disease-specific PRO datasets.
- Comprehensive animal-model landscape and naturally occurring veterinary disease reports.
References
-
(walewska2023guidelineforthe pages 2-2): Renata Walewska, Toby A. Eyre, Sally Barrington, Jessica Brady, Paul Fields, Sunil Iyengar, Anurag Joshi, Tobias Menne, Nilima Parry‐Jones, Harriet Walter, Andrew Wotherspoon, and Kim Linton. Guideline for the diagnosis and management of marginal zone lymphomas: a british society of haematology guideline. British Journal of Haematology, 204:107-86, Nov 2023. URL: https://doi.org/10.1111/bjh.19064, doi:10.1111/bjh.19064. This article has 27 citations and is from a domain leading peer-reviewed journal.
-
(raderer2023clinicalrelevanceof pages 1-2): Markus Raderer, Barbara Kiesewetter, and Ming-Qing Du. Clinical relevance of molecular aspects in extranodal marginal zone lymphoma: a critical appraisal. Therapeutic Advances in Medical Oncology, Jan 2023. URL: https://doi.org/10.1177/17588359231183565, doi:10.1177/17588359231183565. This article has 11 citations and is from a peer-reviewed journal.
-
(alderuccio2023enhancingprognosticationand pages 1-3): Juan Pablo Alderuccio and Izidore S. Lossos. Enhancing prognostication and personalizing treatment of extranodal marginal zone lymphoma. Expert Review of Hematology, 16:333-348, Apr 2023. URL: https://doi.org/10.1080/17474086.2023.2206557, doi:10.1080/17474086.2023.2206557. This article has 2 citations and is from a peer-reviewed journal.
-
(matysiakbudnik2023clinicalmanagementof pages 1-2): Tamara Matysiak-Budnik, Kateryna Priadko, Céline Bossard, Nicolas Chapelle, and Agnès Ruskoné-Fourmestraux. Clinical management of patients with gastric malt lymphoma: a gastroenterologist’s point of view. Cancers, 15:3811, Jul 2023. URL: https://doi.org/10.3390/cancers15153811, doi:10.3390/cancers15153811. This article has 26 citations.
-
(walewska2023guidelineforthe pages 9-9): Renata Walewska, Toby A. Eyre, Sally Barrington, Jessica Brady, Paul Fields, Sunil Iyengar, Anurag Joshi, Tobias Menne, Nilima Parry‐Jones, Harriet Walter, Andrew Wotherspoon, and Kim Linton. Guideline for the diagnosis and management of marginal zone lymphomas: a british society of haematology guideline. British Journal of Haematology, 204:107-86, Nov 2023. URL: https://doi.org/10.1111/bjh.19064, doi:10.1111/bjh.19064. This article has 27 citations and is from a domain leading peer-reviewed journal.
-
(lemos2023effectivenessofhelicobacter pages 1-3): Fabian Fellipe Bueno Lemos, Caroline Tianeze de Castro, Mariana Santos Calmon, Marcel Silva Luz, Samuel Luca Rocha Pinheiro, Clara Faria Souza Mendes dos Santos, Gabriel Lima Correa Santos, Hanna Santos Marques, Henrique Affonso Delgado, Kádima Nayara Teixeira, Cláudio Lima Souza, Márcio Vasconcelos Oliveira, and Fabrício Freire de Melo. Effectiveness of helicobacter pylori eradication in the treatment of early-stage gastric mucosa-associated lymphoid tissue lymphoma: an up-to-date meta-analysis. World Journal of Gastroenterology, 29:2202-2221, Apr 2023. URL: https://doi.org/10.3748/wjg.v29.i14.2202, doi:10.3748/wjg.v29.i14.2202. This article has 39 citations.
-
(min2023longtermclinicaloutcomes pages 7-8): Gi-June Min, Donghoon Kang, Han Hee Lee, Seung-Jun Kim, Tong Yoon Kim, Young-Woo Jeon, Joo Hyun O, Byung-Ock Choi, Gyeongsin Park, and Seok-Goo Cho. Long-term clinical outcomes of gastric mucosa-associated lymphoid tissue lymphoma in real-world experience. Annals of Hematology, 102:877-888, Feb 2023. URL: https://doi.org/10.1007/s00277-023-05130-8, doi:10.1007/s00277-023-05130-8. This article has 16 citations and is from a peer-reviewed journal.
-
(tsai2024cooperativeparticipationof pages 1-2): Hui-Jen Tsai, Kun-Huei Yeh, Chung-Wu Lin, Ming-Shiang Wu, Jyh-Ming Liou, Ping-Ning Hsu, Yi-Shin Zeng, Ming-Feng Wei, Chia-Tung Shun, Hsiu-Po Wang, Li-Tzong Chen, Ann-Lii Cheng, and Sung-Hsin Kuo. Cooperative participation of caga and nfatc1 in the pathogenesis of antibiotics-responsive gastric malt lymphoma. Cancer Cell International, Nov 2024. URL: https://doi.org/10.1186/s12935-024-03552-6, doi:10.1186/s12935-024-03552-6. This article has 1 citations and is from a peer-reviewed journal.
-
(walewska2023guidelineforthe pages 3-3): Renata Walewska, Toby A. Eyre, Sally Barrington, Jessica Brady, Paul Fields, Sunil Iyengar, Anurag Joshi, Tobias Menne, Nilima Parry‐Jones, Harriet Walter, Andrew Wotherspoon, and Kim Linton. Guideline for the diagnosis and management of marginal zone lymphomas: a british society of haematology guideline. British Journal of Haematology, 204:107-86, Nov 2023. URL: https://doi.org/10.1111/bjh.19064, doi:10.1111/bjh.19064. This article has 27 citations and is from a domain leading peer-reviewed journal.
-
(matysiakbudnik2023clinicalmanagementof pages 7-8): Tamara Matysiak-Budnik, Kateryna Priadko, Céline Bossard, Nicolas Chapelle, and Agnès Ruskoné-Fourmestraux. Clinical management of patients with gastric malt lymphoma: a gastroenterologist’s point of view. Cancers, 15:3811, Jul 2023. URL: https://doi.org/10.3390/cancers15153811, doi:10.3390/cancers15153811. This article has 26 citations.
-
(alderuccio2023enhancingprognosticationand pages 17-19): Juan Pablo Alderuccio and Izidore S. Lossos. Enhancing prognostication and personalizing treatment of extranodal marginal zone lymphoma. Expert Review of Hematology, 16:333-348, Apr 2023. URL: https://doi.org/10.1080/17474086.2023.2206557, doi:10.1080/17474086.2023.2206557. This article has 2 citations and is from a peer-reviewed journal.
-
(matysiakbudnik2023clinicalmanagementof pages 8-9): Tamara Matysiak-Budnik, Kateryna Priadko, Céline Bossard, Nicolas Chapelle, and Agnès Ruskoné-Fourmestraux. Clinical management of patients with gastric malt lymphoma: a gastroenterologist’s point of view. Cancers, 15:3811, Jul 2023. URL: https://doi.org/10.3390/cancers15153811, doi:10.3390/cancers15153811. This article has 26 citations.
-
(matysiakbudnik2023clinicalmanagementof pages 2-4): Tamara Matysiak-Budnik, Kateryna Priadko, Céline Bossard, Nicolas Chapelle, and Agnès Ruskoné-Fourmestraux. Clinical management of patients with gastric malt lymphoma: a gastroenterologist’s point of view. Cancers, 15:3811, Jul 2023. URL: https://doi.org/10.3390/cancers15153811, doi:10.3390/cancers15153811. This article has 26 citations.
-
(matysiakbudnik2023clinicalmanagementof media 18e4f906): Tamara Matysiak-Budnik, Kateryna Priadko, Céline Bossard, Nicolas Chapelle, and Agnès Ruskoné-Fourmestraux. Clinical management of patients with gastric malt lymphoma: a gastroenterologist’s point of view. Cancers, 15:3811, Jul 2023. URL: https://doi.org/10.3390/cancers15153811, doi:10.3390/cancers15153811. This article has 26 citations.
-
(alderuccio2023enhancingprognosticationand pages 4-6): Juan Pablo Alderuccio and Izidore S. Lossos. Enhancing prognostication and personalizing treatment of extranodal marginal zone lymphoma. Expert Review of Hematology, 16:333-348, Apr 2023. URL: https://doi.org/10.1080/17474086.2023.2206557, doi:10.1080/17474086.2023.2206557. This article has 2 citations and is from a peer-reviewed journal.
-
(alderuccio2023enhancingprognosticationand pages 16-17): Juan Pablo Alderuccio and Izidore S. Lossos. Enhancing prognostication and personalizing treatment of extranodal marginal zone lymphoma. Expert Review of Hematology, 16:333-348, Apr 2023. URL: https://doi.org/10.1080/17474086.2023.2206557, doi:10.1080/17474086.2023.2206557. This article has 2 citations and is from a peer-reviewed journal.
-
(yang2024endoscopicmorphologyof pages 1-2): Bing-Can Yang, Hai-Lin Yan, Xin-Yue Luo, Yu-Qiang Liu, Jin-Lin Yang, and Zhu Wang. Endoscopic morphology of gastric malt lymphoma correlate with api2/malt1 fusion and predict treatment response after helicobacter pylori eradication. BMC Gastroenterology, Oct 2024. URL: https://doi.org/10.1186/s12876-024-03476-5, doi:10.1186/s12876-024-03476-5. This article has 5 citations and is from a peer-reviewed journal.
-
(tsai2024cooperativeparticipationof pages 15-16): Hui-Jen Tsai, Kun-Huei Yeh, Chung-Wu Lin, Ming-Shiang Wu, Jyh-Ming Liou, Ping-Ning Hsu, Yi-Shin Zeng, Ming-Feng Wei, Chia-Tung Shun, Hsiu-Po Wang, Li-Tzong Chen, Ann-Lii Cheng, and Sung-Hsin Kuo. Cooperative participation of caga and nfatc1 in the pathogenesis of antibiotics-responsive gastric malt lymphoma. Cancer Cell International, Nov 2024. URL: https://doi.org/10.1186/s12935-024-03552-6, doi:10.1186/s12935-024-03552-6. This article has 1 citations and is from a peer-reviewed journal.
-
(matysiakbudnik2023clinicalmanagementof pages 4-7): Tamara Matysiak-Budnik, Kateryna Priadko, Céline Bossard, Nicolas Chapelle, and Agnès Ruskoné-Fourmestraux. Clinical management of patients with gastric malt lymphoma: a gastroenterologist’s point of view. Cancers, 15:3811, Jul 2023. URL: https://doi.org/10.3390/cancers15153811, doi:10.3390/cancers15153811. This article has 26 citations.
-
(tsai2024cooperativeparticipationof pages 4-6): Hui-Jen Tsai, Kun-Huei Yeh, Chung-Wu Lin, Ming-Shiang Wu, Jyh-Ming Liou, Ping-Ning Hsu, Yi-Shin Zeng, Ming-Feng Wei, Chia-Tung Shun, Hsiu-Po Wang, Li-Tzong Chen, Ann-Lii Cheng, and Sung-Hsin Kuo. Cooperative participation of caga and nfatc1 in the pathogenesis of antibiotics-responsive gastric malt lymphoma. Cancer Cell International, Nov 2024. URL: https://doi.org/10.1186/s12935-024-03552-6, doi:10.1186/s12935-024-03552-6. This article has 1 citations and is from a peer-reviewed journal.
-
(tsai2024cooperativeparticipationof pages 11-13): Hui-Jen Tsai, Kun-Huei Yeh, Chung-Wu Lin, Ming-Shiang Wu, Jyh-Ming Liou, Ping-Ning Hsu, Yi-Shin Zeng, Ming-Feng Wei, Chia-Tung Shun, Hsiu-Po Wang, Li-Tzong Chen, Ann-Lii Cheng, and Sung-Hsin Kuo. Cooperative participation of caga and nfatc1 in the pathogenesis of antibiotics-responsive gastric malt lymphoma. Cancer Cell International, Nov 2024. URL: https://doi.org/10.1186/s12935-024-03552-6, doi:10.1186/s12935-024-03552-6. This article has 1 citations and is from a peer-reviewed journal.
-
(walewska2023guidelineforthe pages 7-7): Renata Walewska, Toby A. Eyre, Sally Barrington, Jessica Brady, Paul Fields, Sunil Iyengar, Anurag Joshi, Tobias Menne, Nilima Parry‐Jones, Harriet Walter, Andrew Wotherspoon, and Kim Linton. Guideline for the diagnosis and management of marginal zone lymphomas: a british society of haematology guideline. British Journal of Haematology, 204:107-86, Nov 2023. URL: https://doi.org/10.1111/bjh.19064, doi:10.1111/bjh.19064. This article has 27 citations and is from a domain leading peer-reviewed journal.
-
(walewska2023guidelineforthe pages 2-3): Renata Walewska, Toby A. Eyre, Sally Barrington, Jessica Brady, Paul Fields, Sunil Iyengar, Anurag Joshi, Tobias Menne, Nilima Parry‐Jones, Harriet Walter, Andrew Wotherspoon, and Kim Linton. Guideline for the diagnosis and management of marginal zone lymphomas: a british society of haematology guideline. British Journal of Haematology, 204:107-86, Nov 2023. URL: https://doi.org/10.1111/bjh.19064, doi:10.1111/bjh.19064. This article has 27 citations and is from a domain leading peer-reviewed journal.
-
(bommier2024transformationinmarginal pages 1-2): Côme Bommier, Brian K. Link, Brianna J. Gysbers, Matthew J. Maurer, Melissa C. Larson, Arushi Khurana, Yucai Wang, Carrie A. Thompson, Dai Chihara, Juan P. Alderuccio, Jean L. Koff, Narendranath Epperla, Annarita Conconi, Izidore S. Lossos, Grzegorz S. Nowakowski, Andrew L. Feldman, Thomas M. Habermann, Rebecca L. King, and James R. Cerhan. Transformation in marginal zone lymphoma: results from a prospective cohort and a meta-analysis of the literature. Blood Advances, 8:5939-5948, Nov 2024. URL: https://doi.org/10.1182/bloodadvances.2024013188, doi:10.1182/bloodadvances.2024013188. This article has 14 citations and is from a peer-reviewed journal.
-
(walewska2023guidelineforthe pages 10-10): Renata Walewska, Toby A. Eyre, Sally Barrington, Jessica Brady, Paul Fields, Sunil Iyengar, Anurag Joshi, Tobias Menne, Nilima Parry‐Jones, Harriet Walter, Andrew Wotherspoon, and Kim Linton. Guideline for the diagnosis and management of marginal zone lymphomas: a british society of haematology guideline. British Journal of Haematology, 204:107-86, Nov 2023. URL: https://doi.org/10.1111/bjh.19064, doi:10.1111/bjh.19064. This article has 27 citations and is from a domain leading peer-reviewed journal.
-
(min2023longtermclinicaloutcomes pages 8-9): Gi-June Min, Donghoon Kang, Han Hee Lee, Seung-Jun Kim, Tong Yoon Kim, Young-Woo Jeon, Joo Hyun O, Byung-Ock Choi, Gyeongsin Park, and Seok-Goo Cho. Long-term clinical outcomes of gastric mucosa-associated lymphoid tissue lymphoma in real-world experience. Annals of Hematology, 102:877-888, Feb 2023. URL: https://doi.org/10.1007/s00277-023-05130-8, doi:10.1007/s00277-023-05130-8. This article has 16 citations and is from a peer-reviewed journal.
-
(matysiakbudnik2023clinicalmanagementof pages 16-17): Tamara Matysiak-Budnik, Kateryna Priadko, Céline Bossard, Nicolas Chapelle, and Agnès Ruskoné-Fourmestraux. Clinical management of patients with gastric malt lymphoma: a gastroenterologist’s point of view. Cancers, 15:3811, Jul 2023. URL: https://doi.org/10.3390/cancers15153811, doi:10.3390/cancers15153811. This article has 26 citations.
-
(yang2023extranodallymphomapathogenesis pages 28-29): Hua Yang, Yang Xun, Chao Ke, K. Tateishi, and Hua You. Extranodal lymphoma: pathogenesis, diagnosis and treatment. Molecular Biomedicine, Sep 2023. URL: https://doi.org/10.1186/s43556-023-00141-3, doi:10.1186/s43556-023-00141-3. This article has 34 citations and is from a peer-reviewed journal.
-
(bommier2024transformationinmarginal pages 8-9): Côme Bommier, Brian K. Link, Brianna J. Gysbers, Matthew J. Maurer, Melissa C. Larson, Arushi Khurana, Yucai Wang, Carrie A. Thompson, Dai Chihara, Juan P. Alderuccio, Jean L. Koff, Narendranath Epperla, Annarita Conconi, Izidore S. Lossos, Grzegorz S. Nowakowski, Andrew L. Feldman, Thomas M. Habermann, Rebecca L. King, and James R. Cerhan. Transformation in marginal zone lymphoma: results from a prospective cohort and a meta-analysis of the literature. Blood Advances, 8:5939-5948, Nov 2024. URL: https://doi.org/10.1182/bloodadvances.2024013188, doi:10.1182/bloodadvances.2024013188. This article has 14 citations and is from a peer-reviewed journal.
-
(bommier2024transformationinmarginal pages 5-6): Côme Bommier, Brian K. Link, Brianna J. Gysbers, Matthew J. Maurer, Melissa C. Larson, Arushi Khurana, Yucai Wang, Carrie A. Thompson, Dai Chihara, Juan P. Alderuccio, Jean L. Koff, Narendranath Epperla, Annarita Conconi, Izidore S. Lossos, Grzegorz S. Nowakowski, Andrew L. Feldman, Thomas M. Habermann, Rebecca L. King, and James R. Cerhan. Transformation in marginal zone lymphoma: results from a prospective cohort and a meta-analysis of the literature. Blood Advances, 8:5939-5948, Nov 2024. URL: https://doi.org/10.1182/bloodadvances.2024013188, doi:10.1182/bloodadvances.2024013188. This article has 14 citations and is from a peer-reviewed journal.
-
(alderuccio2023enhancingprognosticationand pages 20-21): Juan Pablo Alderuccio and Izidore S. Lossos. Enhancing prognostication and personalizing treatment of extranodal marginal zone lymphoma. Expert Review of Hematology, 16:333-348, Apr 2023. URL: https://doi.org/10.1080/17474086.2023.2206557, doi:10.1080/17474086.2023.2206557. This article has 2 citations and is from a peer-reviewed journal.