Limbic Encephalitis
Limbic encephalitis is an autoimmune or paraneoplastic encephalitis syndrome centered on medial temporal and other limbic regions. It typically presents with short-term memory impairment, seizures, confusion or psychiatric and behavioral symptoms, and may be supported by neuronal antibody testing, CSF inflammation, temporal-lobe EEG abnormalities, and medial temporal MRI T2/FLAIR hyperintensity. Treatment depends on antibody and tumor context and commonly combines immunotherapy with tumor-directed therapy when a neoplasm is identified.
Ask OpenScientist
Ask a research question about Limbic Encephalitis. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Mappings
Definitions
1- Memory impairment Short-term or working memory impairment.
- Seizure Focal temporal-lobe seizures, generalized seizures, or status epilepticus.
- Confusion Confusion or disorientation.
- Psychosis Psychiatric symptoms may include psychosis, hallucinations, anxiety, or mood symptoms.
Show evidence (2 references)
Show evidence (1 reference)
Subtypes
6Show evidence (1 reference)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Pathophysiology
6Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Pathograph
Phenotypes
12Metabolism 1
Show evidence (2 references)
Nervous System 8
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Other 3
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Medical Actions
7Show evidence (3 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (3 references)
Show evidence (2 references)
Show evidence (1 reference)
Environmental Factors
3Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Biochemical Markers
5Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Clinical Trials
1Show evidence (1 reference)
Source YAML
click to showname: Limbic Encephalitis
creation_date: "2026-05-16T08:20:21Z"
updated_date: "2026-05-16T08:53:06Z"
category: Autoimmune
parents:
- Autoimmune Encephalitis
- Neurological Disease
- Autoimmune Disease
synonyms:
- Autoimmune limbic encephalitis
- Paraneoplastic limbic encephalitis
- LE
disease_term:
preferred_term: limbic encephalitis
term:
id: MONDO:0015588
label: limbic encephalitis
mappings:
mondo_mappings:
- term:
id: MONDO:0015588
label: limbic encephalitis
mapping_predicate: skos:exactMatch
mapping_source: MONDO
mapping_justification: Primary MONDO disease term for this broad limbic encephalitis entry.
description: >-
Limbic encephalitis is an autoimmune or paraneoplastic encephalitis syndrome
centered on medial temporal and other limbic regions. It typically presents
with short-term memory impairment, seizures, confusion or psychiatric and
behavioral symptoms, and may be supported by neuronal antibody testing, CSF
inflammation, temporal-lobe EEG abnormalities, and medial temporal MRI
T2/FLAIR hyperintensity. Treatment depends on antibody and tumor context and
commonly combines immunotherapy with tumor-directed therapy when a neoplasm is
identified.
has_subtypes:
- name: Autoimmune Limbic Encephalitis
subtype_term:
preferred_term: autoimmune limbic encephalitis
term:
id: MONDO:0850097
label: autoimmune limbic encephalitis
description: >-
Autoimmune limbic encephalitis is the antibody-associated or
seronegative autoimmune subgroup involving mesial temporal structures, with
subacute memory, seizure, psychiatric, CSF, EEG, MRI, or antibody evidence.
evidence:
- reference: PMID:26906964
reference_title: "A clinical approach to diagnosis of autoimmune encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "we based the initial diagnostic approach on neurological assessment and conventional tests that are accessible to most clinicians."
explanation: >
The Graus consensus framework supports diagnosing autoimmune
encephalitis syndromes using clinical and conventional paraclinical tests
rather than waiting for antibody or treatment-response results.
- name: Classic Paraneoplastic Limbic Encephalitis
subtype_term:
preferred_term: classic paraneoplastic limbic encephalitis
term:
id: MONDO:0015590
label: classic paraneoplastic limbic encephalitis
description: >-
A cancer-associated limbic encephalitis subgroup, often linked to
intracellular/onconeural antibodies such as Hu, Ma2, amphiphysin, or
CV2/CRMP5 and commonly requiring combined antineoplastic and
immunomodulatory treatment.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Some patients develop limbic encephalitis as a paraneoplastic manifestation of systemic cancer, where immune tolerance is thought to be lost."
explanation: >
The review supports paraneoplastic limbic encephalitis as a major
disease subgroup.
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Patients with antibodies to intracellular neuronal antigens (onconeuronal antibodies: Hu, Ma2, amphiphysin, CV2/CRMP5) almost invariably have an underlying neoplasm (lung, testis, breast, etc.)"
explanation: >
Intracellular/onconeural antibody-associated limbic encephalitis is
strongly linked to underlying neoplasia.
- name: Limbic Encephalitis with LGI1 Antibodies
subtype_term:
preferred_term: limbic encephalitis with LGI1 antibodies
term:
id: MONDO:0015592
label: limbic encephalitis with LGI1 antibodies
description: >-
LGI1-antibody limbic encephalitis is a common neuronal-surface antibody
subtype, usually non-paraneoplastic, often affecting older adults and
associated with cognitive symptoms, seizures, faciobrachial dystonic
seizures, and hyponatremia.
evidence:
- reference: DOI:10.3389/fneur.2021.674368
reference_title: "Clinical Characteristics and Long-Term Prognosis of Anti-LGI1 Encephalitis: A Single-Center Cohort Study in Beijing, China"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients presented with seizures at the initial consultation. Other common manifestations included cognitive dysfunction (82.2%), psychiatric disturbance (66.7%), sleep disorder (54.5%), and hyponatremia (66.7%)."
explanation: >
This LGI1 cohort supports seizures, cognitive and psychiatric symptoms,
sleep disturbance, and hyponatremia as common anti-LGI1 encephalitis
features.
- reference: PMID:20663977
reference_title: "Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan's syndrome and acquired neuromyotonia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "leucine-rich, glioma inactivated 1 protein-antibody positive patients (P < 0.0001), who predominantly had limbic encephalitis."
explanation: >
This antibody-characterization cohort supports LGI1 antibodies as a
major marker of limbic encephalitis.
- name: Limbic Encephalitis with CASPR2 Antibodies
subtype_term:
preferred_term: limbic encephalitis with caspr2 antibodies
term:
id: MONDO:0017179
label: limbic encephalitis with caspr2 antibodies
description: >-
CASPR2-antibody limbic encephalitis overlaps with peripheral nerve
hyperexcitability and Morvan syndrome and has a stronger tumor and poorer
prognosis signal than LGI1-antibody disease in early VGKC-complex cohorts.
evidence:
- reference: PMID:20663977
reference_title: "Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan's syndrome and acquired neuromyotonia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "detection of contactin-associated protein-2 antibodies should help identify the risk of an underlying tumour and a poor prognosis in future patients."
explanation: >
The study distinguishes CASPR2-antibody disease from LGI1-antibody
limbic encephalitis by tumor and prognosis associations.
- name: GABAB Receptor Autoimmune Limbic Encephalitis
description: >-
A neuronal-surface antibody subtype characterized by prominent seizures and
frequent association with small-cell lung cancer, although non-paraneoplastic
cases also occur.
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "GABA(B) receptor autoimmune encephalitis is a potentially treatable disorder characterised by seizures and, in some patients, associated with small-cell lung cancer and with other autoantibodies."
explanation: >
The case series defines the GABAB receptor antibody-associated limbic
encephalitis phenotype.
- name: AMPAR Autoimmune Limbic Encephalitis
description: >-
A GluR1/GluR2 AMPA receptor antibody-associated subtype that is often
paraneoplastic, treatment responsive, and relapse prone.
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Antibodies to GluR1/2 associate with LE that is often paraneoplastic, treatment responsive, and has a tendency to relapse."
explanation: >
The AMPAR antibody study supports a distinct antibody-defined limbic
encephalitis subtype.
definitions:
- name: Limbic encephalitis clinical syndrome
definition_type: CASE_DEFINITION
description: >-
Limbic encephalitis is recognized clinically by an encephalitic syndrome
centered on limbic structures, especially subacute short-term memory
impairment, seizures, confusion, psychiatric or behavioral symptoms, and
supportive MRI, EEG, CSF, or antibody evidence after exclusion of competing
causes.
criteria_sets:
- name: Core limbic syndrome features
core_clinical_characteristics:
- preferred_term: Memory impairment
term:
id: HP:0002354
label: Memory impairment
description: Short-term or working memory impairment.
- preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
description: Focal temporal-lobe seizures, generalized seizures, or status epilepticus.
- preferred_term: Confusion
term:
id: HP:0001289
label: Confusion
description: Confusion or disorientation.
- preferred_term: Psychosis
term:
id: HP:0000709
label: Psychosis
description: Psychiatric symptoms may include psychosis, hallucinations, anxiety, or mood symptoms.
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Limbic encephalitis (LE) is an inflammatory disorder that predominantly affects the grey matter of the medial temporal lobes, amygdala, and orbitofrontal cortex."
explanation: >
The full-text introduction defines the anatomical limbic syndrome.
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "As a result patients develop short-term memory deficits, emotional and behavioral disturbances, seizures, and sometimes dementia."
explanation: >
This statement supports the core clinical features used in the criteria
set.
evidence:
- reference: PMID:26906964
reference_title: "A clinical approach to diagnosis of autoimmune encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Through logical differential diagnosis, levels of evidence for autoimmune encephalitis (possible, probable, or definite) are achieved, which can lead to prompt immunotherapy."
explanation: >
The consensus review supports a graded syndrome-based diagnostic
approach that can guide early treatment.
pathophysiology:
- name: Limbic Gray Matter Inflammation
description: >-
Inflammation predominates in medial temporal and limbic gray matter,
explaining the memory, seizure, psychiatric, and behavioral syndrome.
locations:
- preferred_term: hippocampal formation
term:
id: UBERON:0002421
label: hippocampal formation
- preferred_term: brain
term:
id: UBERON:0000955
label: brain
biological_processes:
- preferred_term: immune response
modifier: INCREASED
term:
id: GO:0006955
label: immune response
downstream:
- target: Limbic Network Dysfunction
description: >
Limbic inflammation disrupts memory and seizure-prone temporal-lobe
networks.
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "As a result patients develop short-term memory deficits, emotional and behavioral disturbances, seizures, and sometimes dementia."
explanation: >
The clinical consequences of limbic gray matter inflammation support
the downstream link to network dysfunction.
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Limbic encephalitis (LE) is an inflammatory disorder that predominantly affects the grey matter of the medial temporal lobes, amygdala, and orbitofrontal cortex."
explanation: >
The paper defines the primary anatomical inflammatory substrate of limbic
encephalitis.
- name: Neuronal Antigen Humoral Autoimmunity
description: >-
Serum or CSF antibodies against neuronal intracellular or cell-surface
antigens identify major mechanistic and prognostic subgroups.
cell_types:
- preferred_term: B cell
term:
id: CL:0000236
label: B cell
- preferred_term: plasma cell
term:
id: CL:0000786
label: plasma cell
biological_processes:
- preferred_term: immunoglobulin production
modifier: INCREASED
term:
id: GO:0002377
label: immunoglobulin production
downstream:
- target: Limbic Network Dysfunction
description: >
Cell-surface antibody subtypes can alter synaptic receptor localization,
receptor signaling, or neuronal excitability.
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "patients' antibodies alter the synaptic localization and number of AMPARs."
explanation: >
AMPAR antibody effects provide direct mechanistic support for the
downstream synaptic-receptor edge.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Serum and cerebrospinal antibodies against neuronal antigens can be detected in most patients."
explanation: >
Detection of neuronal antibodies in serum or CSF supports humoral
autoimmunity as a major organizing mechanism.
- name: LGI1-CASPR2 VGKC-Complex Autoimmunity
description: >-
Many patients formerly classified by high voltage-gated potassium channel
complex antibodies have antibodies to LGI1 or CASPR2, which correlate with
distinct limbic encephalitis, Morvan/neuromyotonia, tumor, and prognosis
phenotypes.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
locations:
- preferred_term: hippocampal formation
term:
id: UBERON:0002421
label: hippocampal formation
biological_processes:
- preferred_term: chemical synaptic transmission
modifier: ABNORMAL
term:
id: GO:0007268
label: chemical synaptic transmission
downstream:
- target: Limbic Network Dysfunction
description: >
LGI1-antibody-positive patients predominantly manifest limbic
encephalitis.
evidence:
- reference: PMID:20663977
reference_title: "Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan's syndrome and acquired neuromyotonia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "leucine-rich, glioma inactivated 1 protein-antibody positive patients (P < 0.0001), who predominantly had limbic encephalitis."
explanation: >
The cohort links LGI1 antibodies to the limbic encephalitis clinical
syndrome.
evidence:
- reference: PMID:20663977
reference_title: "Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan's syndrome and acquired neuromyotonia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The identification of leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 as the major targets of potassium channel antibodies, and their associations with different clinical features, begins to explain the diversity of these syndromes"
explanation: >
The study identifies LGI1 and CASPR2 as the key antigenic targets behind
diverse VGKC-complex antibody syndromes.
- name: AMPAR Synaptic Cluster Loss
description: >-
AMPAR autoantibodies bind GluR1/GluR2-containing receptors on hippocampal
neurons and reduce synaptic AMPAR cluster number and localization, producing
potentially reversible limbic dysfunction.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
locations:
- preferred_term: hippocampal formation
term:
id: UBERON:0002421
label: hippocampal formation
biological_processes:
- preferred_term: glutamate receptor signaling pathway
modifier: DECREASED
term:
id: GO:0007215
label: glutamate receptor signaling pathway
- preferred_term: synapse organization
modifier: ABNORMAL
term:
id: GO:0050808
label: synapse organization
downstream:
- target: Limbic Network Dysfunction
description: >
Reduced synaptic AMPAR localization impairs hippocampal excitatory
signaling involved in memory and seizures.
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "AMPAR are ionotropic glutamate receptors that are highly conserved among mammals, and mediate most of the fast excitatory neurotransmission in the brain."
explanation: >
AMPAR localization effects can disrupt excitatory neurotransmission in
limbic circuitry.
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "Application of antibodies to cultures of neurons significantly decreased the number of GluR2-containing AMPAR clusters at synapses with a smaller decrease in overall AMPAR cluster density; these effects were reversed after antibody removal."
explanation: >
Patient antibodies directly altered AMPAR synaptic clusters in neuronal
culture.
- name: GABAB Receptor Autoimmunity and Neuronal Hyperexcitability
description: >-
GABAB receptor antibodies target inhibitory GABAB1 receptors and are linked
to prominent seizures, temporal-lobe EEG abnormalities, and memory
dysfunction.
cell_types:
- preferred_term: neuron
term:
id: CL:0000540
label: neuron
locations:
- preferred_term: hippocampal formation
term:
id: UBERON:0002421
label: hippocampal formation
biological_processes:
- preferred_term: chemical synaptic transmission
modifier: ABNORMAL
term:
id: GO:0007268
label: chemical synaptic transmission
downstream:
- target: Limbic Network Dysfunction
description: >
Disrupted GABAB receptor function can produce seizure-prone temporal-lobe
networks.
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients presented with early or prominent seizures; other symptoms, MRI, and electroencephalography findings were consistent with predominant limbic dysfunction."
explanation: >
The GABAB antibody series directly links this immune target with
seizure-predominant limbic dysfunction.
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "Confocal microscopy showed colocalisation of the antibody with GABA(B) receptors."
explanation: >
Colocalization of patient antibodies with GABAB receptors supports direct
receptor targeting.
- name: Limbic Network Dysfunction
description: >-
Limbic-region inflammation and synaptic antibody effects converge on
temporal-lobe networks, producing memory impairment, seizures, confusion,
psychiatric symptoms, EEG abnormalities, and MRI signal changes.
locations:
- preferred_term: hippocampal formation
term:
id: UBERON:0002421
label: hippocampal formation
biological_processes:
- preferred_term: chemical synaptic transmission
modifier: ABNORMAL
term:
id: GO:0007268
label: chemical synaptic transmission
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients had seizures, confusion, and memory deficits."
explanation: >
The GABAB receptor antibody cohort illustrates the core limbic network
clinical syndrome.
phenotypes:
- name: Memory Impairment
category: Neurologic
diagnostic: true
phenotype_term:
preferred_term: Memory impairment
term:
id: HP:0002354
label: Memory impairment
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "As a result patients develop short-term memory deficits, emotional and behavioral disturbances, seizures, and sometimes dementia."
explanation: >
Short-term memory deficits are a core limbic encephalitis manifestation.
- name: Seizure
category: Neurologic
diagnostic: true
phenotype_term:
preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "As a result patients develop short-term memory deficits, emotional and behavioral disturbances, seizures, and sometimes dementia."
explanation: >
Seizures are part of the core syndrome of limbic encephalitis.
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients presented with early or prominent seizures; other symptoms, MRI, and electroencephalography findings were consistent with predominant limbic dysfunction."
explanation: >
GABAB receptor antibody-associated limbic encephalitis is especially
seizure prominent.
- name: Faciobrachial Dystonic Seizures
subtype: Limbic Encephalitis with LGI1 Antibodies
category: Neurologic
diagnostic: true
phenotype_term:
preferred_term: Faciobrachial dystonic seizures
term:
id: HP:0001250
label: Seizure
notes: >
HPO does not currently expose a specific faciobrachial dystonic seizure
term; the broader seizure term is used for brief dystonic seizures involving
face and arm in LGI1-antibody disease.
evidence:
- reference: PMID:24014519
reference_title: "Faciobrachial dystonic seizures: the influence of immunotherapy on seizure control and prevention of cognitive impairment in a broadening phenotype."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Voltage-gated potassium channel complex antibodies, particularly those directed against leucine-rich glioma inactivated 1, are associated with a common form of limbic encephalitis that presents with cognitive impairment and seizures."
explanation: >
The study places LGI1/VGKC-complex antibody disease in the limbic
encephalitis spectrum with cognitive impairment and seizures.
- reference: PMID:24014519
reference_title: "Faciobrachial dystonic seizures: the influence of immunotherapy on seizure control and prevention of cognitive impairment in a broadening phenotype."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Faciobrachial dystonic seizures have recently been reported as immunotherapy-responsive, brief, frequent events that often predate the cognitive impairment associated with this limbic encephalitis."
explanation: >
This directly supports faciobrachial dystonic seizures as an
LGI1-associated limbic encephalitis phenotype and diagnostic clue.
- name: Confusion
category: Neurologic
phenotype_term:
preferred_term: Confusion
term:
id: HP:0001289
label: Confusion
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients had seizures, confusion, and memory deficits."
explanation: >
Confusion was universal in this GABAB receptor antibody limbic
encephalitis series.
- name: Psychiatric Symptoms
category: Psychiatric
diagnostic: true
phenotype_term:
preferred_term: Psychosis
term:
id: HP:0000709
label: Psychosis
notes: >
HPO psychosis is used as the closest structured term for the psychiatric
limbic syndrome; individual presentations may include hallucinations,
anxiety, mood symptoms, agitation, or broader behavioral changes.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "encephalitis, combining psychiatric symptoms, seizures, dyskinesias, catatonia and central hypoventilation (NMDAR-encephalitis)."
explanation: >
The review identifies psychiatric symptoms as part of the autoimmune
encephalitis spectrum overlapping limbic/cortical syndromes.
- name: Personality Changes
category: Psychiatric
phenotype_term:
preferred_term: Personality changes
term:
id: HP:0000751
label: Personality changes
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Nine patients presented with subacute (< 8 weeks) confusion, disorientation and memory loss, classic of LE; 1 patient presented with a 4 month history of progressive memory loss, behavioral change and agitation"
explanation: >
Behavioral change and agitation in the AMPAR cohort support the
personality/behavioral phenotype.
- name: Status Epilepticus
category: Neurologic
phenotype_term:
preferred_term: Status epilepticus
term:
id: HP:0002133
label: Status epilepticus
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "After further clinical assessment most seizures appeared to have a temporal-lobe onset with secondary generalisation, and three patients had status epilepticus."
explanation: >
Status epilepticus occurred in a subset of the GABAB receptor antibody
limbic encephalitis cohort.
- name: Abnormal Hippocampus Morphology
category: Radiologic
diagnostic: true
phenotype_term:
preferred_term: Abnormal hippocampus morphology
term:
id: HP:0025100
label: Abnormal hippocampus morphology
notes: >
Used to represent medial temporal/hippocampal T2 or FLAIR signal change on
MRI, which is central to many limbic encephalitis diagnostic workflows.
evidence:
- reference: PMID:38497971
reference_title: "Magnetic Resonance Imaging Characteristics of LGI1-Antibody and CASPR2-Antibody Encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "T2 and/or FLAIR hyperintensities confined to the temporal lobes, without diffusion restriction or contrast enhancement, robustly distinguished LGI1/CASPR2-Ab-E from key differential diagnoses."
explanation: >
Temporal-lobe T2/FLAIR hyperintensity is a characteristic imaging pattern
in LGI1/CASPR2 antibody encephalitis.
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Ten patients had unilateral or bilateral increases in medial temporal lobe FLAIR/T2 signal consistent with limbic encephalitis, and one had a small area of increased FLAIR signal in the corpus callosum (table 2)."
explanation: >
Medial temporal FLAIR/T2 abnormalities occurred in most GABAB receptor
antibody cases with available MRI.
- name: EEG Abnormality
category: Neurologic
phenotype_term:
preferred_term: EEG abnormality
term:
id: HP:0002353
label: EEG abnormality
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "EEG results were available from 12 patients: nine had temporal-lobe seizures, epileptiform discharges, or temporal-lobe slowing; two had generalised slowing; and one had no abnormalities."
explanation: >
Temporal-lobe epileptiform or slowing abnormalities support EEG
abnormality as a supportive diagnostic feature.
- name: CSF Pleocytosis
category: Laboratory
phenotype_term:
preferred_term: CSF pleocytosis
term:
id: HP:0012229
label: CSF pleocytosis
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "CSF was abnormal in nine of ten patients for whom data were available. The most common CSF abnormality was lymphocytic pleocytosis in eight patients."
explanation: >
CSF pleocytosis is a common inflammatory CSF finding in this GABAB
receptor antibody cohort.
- name: Hyponatremia
category: Laboratory
phenotype_term:
preferred_term: Hyponatremia
term:
id: HP:0002902
label: Hyponatremia
notes: >
Hyponatremia is especially associated with LGI1-antibody limbic
encephalitis rather than all antibody subtypes.
evidence:
- reference: DOI:10.3389/fneur.2021.674368
reference_title: "Clinical Characteristics and Long-Term Prognosis of Anti-LGI1 Encephalitis: A Single-Center Cohort Study in Beijing, China"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Other common manifestations included cognitive dysfunction (82.2%), psychiatric disturbance (66.7%), sleep disorder (54.5%), and hyponatremia (66.7%)."
explanation: >
Hyponatremia occurred in two thirds of this anti-LGI1 encephalitis cohort,
supporting it as a subtype-associated laboratory phenotype.
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The patient had hyponatraemia (119 mEq/L) caused by syndrome of inappropriate antidiuretic hormone secretion."
explanation: >
The GABAB receptor paper documents hyponatremia in an index limbic
encephalitis case; MONDO also identifies hyponatremia in LGI1-antibody
limbic encephalitis.
- name: Sleep Disturbance
category: Neurologic
phenotype_term:
preferred_term: Sleep disturbance
term:
id: HP:0002360
label: Sleep disturbance
notes: >
Sleep disturbance is particularly supported for anti-LGI1 encephalitis and
may include insomnia, hypersomnia, or other sleep-wake disruption depending
on antibody subtype.
evidence:
- reference: DOI:10.3389/fneur.2021.674368
reference_title: "Clinical Characteristics and Long-Term Prognosis of Anti-LGI1 Encephalitis: A Single-Center Cohort Study in Beijing, China"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Other common manifestations included cognitive dysfunction (82.2%), psychiatric disturbance (66.7%), sleep disorder (54.5%), and hyponatremia (66.7%)."
explanation: >
Sleep disorder affected 54.5% of this anti-LGI1 encephalitis cohort.
biochemical:
- name: Serum or CSF Neuronal Antigen Antibodies
presence: Positive in many cases
context: Serum or cerebrospinal fluid
notes: >
Neuronal antibodies define many autoimmune and paraneoplastic limbic
encephalitis subgroups, although antibody-negative autoimmune limbic
encephalitis is recognized clinically.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Serum and cerebrospinal antibodies against neuronal antigens can be detected in most patients."
explanation: >
The review supports neuronal antibody testing in serum and CSF as a key
biomarker domain.
- reference: DOI:10.3390/cells13010015
reference_title: Pathophysiological Effects of Autoantibodies in Autoimmune Encephalitides
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "There are many subtypes of autoimmune encephalitides, which now entails both diseases with autoantibodies targeting extracellular antigens and classical paraneoplastic syndromes with autoantibodies targeting intracellular antigens."
explanation: >
This review supports the split between extracellular neuronal
antigen-associated disease and intracellular paraneoplastic antibody
syndromes.
- name: LGI1 Antibodies
presence: Positive in subtype
context: Serum or cerebrospinal fluid
evidence:
- reference: PMID:20663977
reference_title: "Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan's syndrome and acquired neuromyotonia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Antibodies to Kv1 subunits were found in three sera, to contactin-associated protein-2 in 19 sera, to leucine-rich, glioma inactivated 1 protein in 55 sera and to contactin-2 in five sera"
explanation: >
The cohort identifies LGI1 antibodies as the largest VGKC-complex target
group.
- name: CASPR2 Antibodies
presence: Positive in subtype
context: Serum or cerebrospinal fluid
evidence:
- reference: PMID:20663977
reference_title: "Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan's syndrome and acquired neuromyotonia."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Antibodies to Kv1 subunits were found in three sera, to contactin-associated protein-2 in 19 sera, to leucine-rich, glioma inactivated 1 protein in 55 sera and to contactin-2 in five sera"
explanation: >
CASPR2 antibodies define one VGKC-complex antibody subgroup relevant to
limbic encephalitis and Morvan/neuromyotonia phenotypes.
- name: GABAB Receptor Antibodies
presence: Positive in subtype
context: Serum or cerebrospinal fluid
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients had antibodies (mainly IgG1) against a neuronal cell-surface antigen; in three patients antibodies were detected only in CSF."
explanation: >
The GABAB receptor case series demonstrates subtype-defining neuronal
cell-surface antibodies, including CSF-only detection in some patients.
- name: AMPAR GluR1/GluR2 Antibodies
presence: Positive in subtype
context: Serum or cerebrospinal fluid
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "All patients had antibodies against neuronal cell surface antigens that by immunoprecipitation were found to be the glutamate receptor 1 (GluR1) and GluR2 subunits"
explanation: >
The AMPAR subtype is defined by GluR1/GluR2 neuronal surface antibodies.
environmental:
- name: Underlying Neoplasm
description: >-
Limbic encephalitis can be paraneoplastic; tumor type and antibody class
affect prognosis, evaluation, and treatment.
effect: Triggers or sustains paraneoplastic autoimmunity
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Some patients develop limbic encephalitis as a paraneoplastic manifestation of systemic cancer, where immune tolerance is thought to be lost."
explanation: >
The review supports systemic cancer as a trigger for paraneoplastic limbic
encephalitis.
- name: Small-Cell Lung Cancer
description: >-
Small-cell lung cancer is a major tumor association, particularly in
classic paraneoplastic limbic encephalitis and GABAB receptor antibody
limbic encephalitis.
effect: Paraneoplastic trigger
evidence:
- reference: PMID:19962348
reference_title: "Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Seven of 15 patients had tumours, five of which were small-cell lung cancer, and seven patients had non-neuronal autoantibodies."
explanation: >
The GABAB receptor antibody series shows small-cell lung cancer was the
dominant tumor association.
- name: Thymus, Breast, or Lung Tumor
description: >-
AMPAR antibody limbic encephalitis is often associated with tumors of the
thymus, breast, or lung.
effect: Paraneoplastic trigger
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Seven had tumors of the lung, breast, or thymus."
explanation: >
The AMPAR antibody cohort identifies lung, breast, and thymus tumors as
important paraneoplastic associations.
progression:
- phase: Subacute limbic syndrome onset
notes: >
Limbic encephalitis commonly begins over weeks with memory impairment,
confusion, behavioral or psychiatric change, and seizures.
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Nine patients presented with subacute (< 8 weeks) confusion, disorientation and memory loss, classic of LE; 1 patient presented with a 4 month history of progressive memory loss, behavioral change and agitation"
explanation: >
The AMPAR cohort illustrates the usual subacute limbic presentation.
- phase: Diagnostic evaluation and antibody/tumor stratification
notes: >
Workup integrates MRI, EEG, CSF, serum/CSF antibody testing, and malignancy
screening because antibody subtype and tumor status shape prognosis and
treatment.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "According to the type of antibodies found, patients may be classified into two broad groups, with implications for neurological and cancer diagnosis, treatment and prognosis."
explanation: >
Antibody grouping is central to diagnostic and prognostic stratification.
- reference: PMID:38497971
reference_title: "Magnetic Resonance Imaging Characteristics of LGI1-Antibody and CASPR2-Antibody Encephalitis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "These observations should assist clinical decision-making toward expediting immunotherapy."
explanation: >
MRI patterns can help distinguish autoimmune limbic encephalitis from
infectious and degenerative mimics while antibody results are pending.
- phase: Treatment response, recovery, or relapse
notes: >
Cell-surface antibody-associated disease is often immunotherapy responsive,
but relapse and residual cognitive or behavioral deficits can occur,
especially if relapses are not promptly controlled.
evidence:
- reference: PMID:19338055
reference_title: "AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Antibodies to GluR1/2 associate with LE that is often paraneoplastic, treatment responsive, and has a tendency to relapse."
explanation: >
AMPAR antibody limbic encephalitis illustrates both treatment response
and relapse risk.
- reference: PMID:26559389
reference_title: "Immune therapy in autoimmune encephalitis: a systematic review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "patients given immune therapy do better and relapse less than patients given no treatment."
explanation: >
The systematic review supports immune therapy as improving outcomes and
reducing relapse across autoimmune encephalitis.
treatments:
- name: First-Line Immunotherapy
description: >-
First-line treatment commonly uses high-dose corticosteroids, intravenous
immunoglobulin, plasma exchange, or combinations, with escalation based on
severity, antibody subtype, and tumor context.
treatment_term:
preferred_term: immunotherapy
term:
id: MAXO:0001002
label: immunotherapy procedure
target_mechanisms:
- target: Neuronal Antigen Humoral Autoimmunity
treatment_effect: INHIBITS
description: >
Immunotherapy suppresses or removes pathogenic antibody-mediated immune
activity.
evidence:
- reference: PMID:26559389
reference_title: "Immune therapy in autoimmune encephalitis: a systematic review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "patients given immune therapy do better and relapse less than patients given no treatment."
explanation: >
Better outcomes after immunotherapy support targeting the autoimmune
mechanism.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "First-line immunotherapies include high dose steroids, intravenous immunoglobulins and plasma exchange."
explanation: >
The limbic encephalitis treatment review lists the main first-line
immunotherapy options.
- reference: PMID:26559389
reference_title: "Immune therapy in autoimmune encephalitis: a systematic review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Most clinicians use first-line therapy (steroids, intravenous immunoglobulin, plasma exchange), and if severe or refractory, second-line therapy (rituximab, cyclophosphamide)."
explanation: >
The autoimmune encephalitis systematic review supports the same first-line
and escalation framework.
- reference: DOI:10.1055/s-0044-1788586
reference_title: Brazilian consensus recommendations on the diagnosis and treatment of autoimmune encephalitis in the adult and pediatric populations
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Treatment should be started within the first 4 weeks of symptoms. The first-line option is methylprednisolone plus intravenous immunoglobulin (IVIG) or plasmapheresis, the second-line includes rituximab and/or cyclophosphamide, while third-line treatment options are bortezomib and tocilizumab."
explanation: >
The 2024 consensus recommendation supports early treatment timing and the
first-line treatment combination options.
- name: High-Dose Corticosteroid Therapy
description: >-
High-dose systemic corticosteroids are a core first-line
immunosuppressive treatment for autoimmune limbic encephalitis.
treatment_term:
preferred_term: systemic corticosteroid therapy
term:
id: NCIT:C122080
label: Systemic Corticosteroid Therapy
target_mechanisms:
- target: Limbic Gray Matter Inflammation
treatment_effect: INHIBITS
description: Corticosteroids suppress acute CNS inflammation.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "First-line immunotherapies include high dose steroids, intravenous immunoglobulins and plasma exchange."
explanation: >
High-dose steroids are a first-line immunotherapy used to suppress
active inflammatory limbic encephalitis.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "First-line immunotherapies include high dose steroids, intravenous immunoglobulins and plasma exchange."
explanation: >
High-dose steroids are explicitly listed among first-line limbic
encephalitis immunotherapies.
- name: Intravenous Immunoglobulin
description: >-
Intravenous immunoglobulin is used as first-line immune modulation alone or
in combination with corticosteroids or plasma exchange.
treatment_term:
preferred_term: intravenous immunoglobulin therapy
term:
id: NCIT:C121331
label: Intravenous Immunoglobulin Therapy
target_mechanisms:
- target: Neuronal Antigen Humoral Autoimmunity
treatment_effect: MODULATES
description: IVIG modulates pathogenic antibody and immune effector activity.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "First-line immunotherapies include high dose steroids, intravenous immunoglobulins and plasma exchange."
explanation: >
Intravenous immunoglobulin is a first-line immunotherapy that modulates
antibody-mediated immune activity.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "First-line immunotherapies include high dose steroids, intravenous immunoglobulins and plasma exchange."
explanation: >
Intravenous immunoglobulin is explicitly listed among first-line
immunotherapies.
- name: Plasma Exchange
description: >-
Plasma exchange is used to remove pathogenic circulating antibodies in
antibody-mediated limbic encephalitis.
treatment_term:
preferred_term: plasmapheresis
term:
id: NCIT:C15304
label: Plasmapheresis
target_mechanisms:
- target: Neuronal Antigen Humoral Autoimmunity
treatment_effect: INHIBITS
description: Plasma exchange reduces circulating pathogenic antibody burden.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "First-line immunotherapies include high dose steroids, intravenous immunoglobulins and plasma exchange."
explanation: >
Plasma exchange is a first-line immunotherapy option consistent with
removing circulating antibody-mediated immune factors.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "First-line immunotherapies include high dose steroids, intravenous immunoglobulins and plasma exchange."
explanation: >
Plasma exchange is explicitly listed among first-line immunotherapies.
- name: Rituximab or Cyclophosphamide Second-Line Immunotherapy
description: >-
Severe, refractory, or relapsing autoimmune limbic encephalitis can be
escalated to second-line B-cell-directed or cytotoxic immunotherapy.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: rituximab
term:
id: NCIT:C1702
label: Rituximab
- preferred_term: cyclophosphamide
term:
id: CHEBI:4027
label: cyclophosphamide
target_mechanisms:
- target: Neuronal Antigen Humoral Autoimmunity
treatment_effect: INHIBITS
description: >
B-cell depletion or cytotoxic immunosuppression suppresses persistent
autoreactive lymphocyte and antibody responses.
evidence:
- reference: PMID:26559389
reference_title: "Immune therapy in autoimmune encephalitis: a systematic review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "when patients fail first-line therapy, second-line therapy improves outcomes and reduces relapses."
explanation: >
Improved outcomes after second-line immunotherapy support escalation to
suppress persistent autoimmune activity.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Second-line drugs include Rituximab and Cyclophosphamide."
explanation: >
Rituximab and cyclophosphamide are named second-line agents in the limbic
encephalitis treatment review.
- reference: PMID:26559389
reference_title: "Immune therapy in autoimmune encephalitis: a systematic review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "when patients fail first-line therapy, second-line therapy improves outcomes and reduces relapses."
explanation: >
The systematic review supports escalation when first-line therapy fails.
- reference: DOI:10.1055/s-0044-1788586
reference_title: Brazilian consensus recommendations on the diagnosis and treatment of autoimmune encephalitis in the adult and pediatric populations
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The first-line option is methylprednisolone plus intravenous immunoglobulin (IVIG) or plasmapheresis, the second-line includes rituximab and/or cyclophosphamide, while third-line treatment options are bortezomib and tocilizumab."
explanation: >
The consensus statement directly names rituximab and cyclophosphamide as
second-line autoimmune encephalitis therapies.
- name: Tumor Removal and Antineoplastic Therapy
description: >-
Tumor-directed treatment is required when limbic encephalitis is
paraneoplastic or a tumor is identified alongside a neuronal antibody
syndrome.
treatment_term:
preferred_term: surgical procedure
term:
id: MAXO:0000004
label: surgical procedure
target_mechanisms:
- target: Neuronal Antigen Humoral Autoimmunity
treatment_effect: INHIBITS
description: >
Removing or treating a tumor can remove the antigen source sustaining a
paraneoplastic immune response.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "are likely to improve with immunomodulatory treatment (and tumor removal for paraneoplastic cases) and have, overall, a better prognosis."
explanation: >
Tumor removal in paraneoplastic cases supports targeting the neoplasm
as an upstream driver of autoimmune limbic disease.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "are likely to improve with immunomodulatory treatment (and tumor removal for paraneoplastic cases) and have, overall, a better prognosis."
explanation: >
The limbic encephalitis review links paraneoplastic cases to tumor
removal plus immunomodulatory treatment.
- reference: PMID:26559389
reference_title: "Immune therapy in autoimmune encephalitis: a systematic review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "When present, tumours should be removed."
explanation: >
The autoimmune encephalitis treatment review supports tumor removal when
a tumor is present.
- name: Maintenance Immunosuppression
description: >-
Selected relapsing or deteriorating cases may require maintenance
immunosuppression after acute treatment.
treatment_term:
preferred_term: immunotherapy
term:
id: MAXO:0001002
label: immunotherapy procedure
target_mechanisms:
- target: Neuronal Antigen Humoral Autoimmunity
treatment_effect: INHIBITS
description: Maintenance immunosuppression suppresses ongoing autoimmune activity.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "For some patients, maintenance treatment with immunosuppressants might be required to prevent deterioration or relapses."
explanation: >
Maintenance treatment is used to prevent deterioration or relapse by
continuing suppression of autoimmune activity.
evidence:
- reference: PMID:23250843
reference_title: "Limbic encephalitis and related cortical syndromes."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "For some patients, maintenance treatment with immunosuppressants might be required to prevent deterioration or relapses."
explanation: >
The limbic encephalitis review supports maintenance immunosuppression in
selected patients.
clinical_trials:
- name: NCT05503264
phase: PHASE_III
status: RECRUITING
description: >-
Phase III randomized, double-blind, placebo-controlled basket trial of
satralizumab in participants with anti-NMDAR or anti-LGI1 encephalitis.
target_phenotypes:
- preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
- preferred_term: Memory impairment
term:
id: HP:0002354
label: Memory impairment
evidence:
- reference: clinicaltrials:NCT05503264
reference_title: "A Phase III, Randomized, Double-blind, Placebo-controlled, Multicenter Basket Study to Evaluate the Efficacy, Safety, Pharmacokinetics, and Pharmacodynamics of Satralizumab in Patients With Anti-N-methyl-D-aspartic Acid Receptor (NMDAR) or Anti-leucine-rich Glioma-inactivated 1 (LGI1) Encephalitis"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The purpose of this study is to assess the efficacy, safety, PK, and PD of satralizumab in participants with NMDAR and LGI1 encephalitis."
explanation: >
ClinicalTrials.gov documents an active Phase III satralizumab trial that
includes LGI1 encephalitis, a major autoimmune limbic encephalitis subtype.
datasets: []
references:
- reference: DOI:10.1017/cjn.2024.16
title: "Canadian Consensus Guidelines for the Diagnosis and Treatment of Autoimmune Encephalitis in Adults"
found_in:
- Limbic_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1055/s-0044-1788586
title: "Brazilian consensus recommendations on the diagnosis and treatment of autoimmune encephalitis in the adult and pediatric populations"
found_in:
- Limbic_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1055/s-0044-1793933
title: "Recent advances in autoimmune encephalitis"
found_in:
- Limbic_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1186/s12883-023-03514-x
title: "Clinical characteristics of autoimmune encephalitis with co-existence of multiple anti-neuronal antibodies"
found_in:
- Limbic_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.1212/nxi.0000000000200225
title: "Risk of Seizure Recurrence Due to Autoimmune Encephalitis With NMDAR, LGI1, CASPR2, and GABAB Receptor Antibodies"
found_in:
- Limbic_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.3389/fneur.2021.674368
title: "Clinical Characteristics and Long-Term Prognosis of Anti-LGI1 Encephalitis: A Single-Center Cohort Study in Beijing, China"
found_in:
- Limbic_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.3389/fneur.2024.1437913
title: "Innovation and optimization in autoimmune encephalitis trials: the design and rationale for the Phase 3, randomized study of satralizumab in patients with NMDAR-IgG-antibody-positive or LGI1-IgG-antibody-positive autoimmune encephalitis (CIELO)"
found_in:
- Limbic_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.3389/fneur.2024.1474888
title: "Clinical characteristics and prognosis analysis of acute symptomatic seizures secondary to autoimmune encephalitis"
found_in:
- Limbic_Encephalitis-deep-research-falcon.md
findings: []
- reference: DOI:10.3390/cells13010015
title: "Pathophysiological Effects of Autoantibodies in Autoimmune Encephalitides"
found_in:
- Limbic_Encephalitis-deep-research-falcon.md
findings: []
References & Deep Research
References
9Deep Research
1Limbic Encephalitis (Autoimmune) — Comprehensive Disease Characteristics Report
Target Disease
- Disease name: Limbic encephalitis (LE)
- Category: Autoimmune (often antibody-mediated; can be paraneoplastic)
- MONDO ID: Not retrieved in the tool-accessible evidence for this run (explicit MONDO mapping not available from the sources accessed).
Executive summary (current understanding)
Autoimmune limbic encephalitis is a subacute inflammatory syndrome affecting limbic structures (especially the medial temporal lobes) that commonly presents with memory deficits, seizures, and/or psychiatric symptoms. A widely used operational definition is the 2016 Graus et al. “definite autoimmune limbic encephalitis” criteria, which integrates clinical syndrome, medial temporal MRI (or FDG-PET) abnormalities, supportive CSF/EEG evidence, and exclusion of alternative causes. Autoimmune LE encompasses both (i) neuronal cell-surface/synaptic antibody–associated disease (often treatment-responsive) and (ii) paraneoplastic/intracellular onconeural antibody–associated disease (more often cancer-associated and less responsive to immunotherapy). (graus2016aclinicalapproach pages 6-7, graus2016aclinicalapproach pages 7-9)
1. Disease information
1.1 What is the disease?
Definite autoimmune limbic encephalitis (Graus 2016) requires all four of the following: (1) subacute onset (<3 months) of working memory deficits, seizures, or psychiatric symptoms suggesting limbic involvement; (2) bilateral medial temporal lobe abnormalities on T2/FLAIR MRI (or FDG-PET substitute); (3) at least one of CSF pleocytosis (>5 cells/mm³) or EEG with temporal epileptic/slow activity; and (4) reasonable exclusion of alternative causes. (graus2016aclinicalapproach pages 6-7)
Clinical concept: LE is a syndrome that can arise from infectious encephalitis (notably HSV) or autoimmune mechanisms; the Graus framework is intended to support early diagnosis and empiric immunotherapy once infectious causes are reasonably excluded because delays can worsen outcomes. (graus2016aclinicalapproach pages 2-4)
1.2 Key identifiers (OMIM, Orphanet, ICD-10/ICD-11, MeSH, MONDO)
In the retrieved tool-accessible full texts for this run, specific codes/IDs (OMIM, Orphanet, ICD-10/ICD-11, MeSH, MONDO) for limbic encephalitis were not explicitly provided. Accordingly, this report does not assert specific identifiers without evidence.
1.3 Common synonyms / alternative names
- Autoimmune limbic encephalitis
- Paraneoplastic limbic encephalitis (when associated with high-risk intracellular/onconeural antibodies and cancer)
- Antibody-mediated encephalitis with limbic involvement (used in some reviews/guidelines) (graus2016aclinicalapproach pages 7-9)
1.4 Evidence provenance
Information in this report is derived from aggregated disease-level resources (international diagnostic criteria and national consensus guidelines) and cohort studies (multicenter and single-center), plus mechanistic reviews synthesizing in vitro and in vivo models. (graus2016aclinicalapproach pages 6-7, hahn2024canadianconsensusguidelines pages 8-9, dutra2024brazilianconsensusrecommendations pages 1-2, rada2024riskofseizure pages 1-2, ryding2023pathophysiologicaleffectsof pages 4-5)
2. Etiology
2.1 Disease causal factors
Autoimmune mechanisms dominate “autoimmune LE,” frequently mediated by autoantibodies against neuronal cell-surface/synaptic proteins (e.g., LGI1, CASPR2, GABABR, AMPAR, NMDAR) that can directly perturb synaptic function. (li2024clinicalcharacteristicsand pages 1-2, graus2016aclinicalapproach pages 29-29, ryding2023pathophysiologicaleffectsof pages 4-5)
Paraneoplastic etiologies occur when LE is associated with intracellular/onconeural antibodies (e.g., Hu, Ma2) and underlying cancer; these forms are generally less responsive to immunotherapy and require tumor-directed care. (graus2016aclinicalapproach pages 7-9, hahn2024canadianconsensusguidelines pages 8-9)
2.2 Risk factors
- Neoplasm/cancer association: In multi-antibody AE (which can include LE phenotypes), ~46.9% (39/83) were confirmed/suspected to have a tumor; lung cancer was most common (33.7%, 28/83). (zhou2024clinicalcharacteristicsof pages 1-2)
- Autoantibody subtype: Certain antibodies have high tumor associations per Graus’ summary table (e.g., AMPAR ~65% with thymoma/SCLC; GABABR ~50% with SCLC). (graus2016aclinicalapproach pages 29-29)
2.3 Protective factors
No protective factors (genetic or environmental) were identified in the retrieved sources for this run.
2.4 Gene–environment interactions
Not specifically addressed in retrieved sources for this run.
3. Phenotypes
3.1 Core phenotype spectrum and suggested HPO terms
Syndromic core (Graus 2016): subacute onset of - Memory deficits / working memory impairment (HPO: HP:0002354 Memory impairment) - Seizures (HPO: HP:0001250 Seizures) - Psychiatric symptoms (e.g., psychosis, behavioral change) (HPO: HP:0000708 Behavioral abnormality; HP:0000738 Hallucinations) (graus2016aclinicalapproach pages 6-7)
Seizure-related phenotypes: Seizures are common early in autoimmune encephalitis, reported in 42–100% of patients; <15% may develop chronic epilepsy. (li2024clinicalcharacteristicsand pages 1-2)
Subtype-linked phenotype example (LGI1): In an anti-LGI1 cohort (n=45), seizures occurred in 100%; cognitive dysfunction 82.2%; psychiatric disturbance 66.7%; sleep disorder 54.5%; hyponatremia 66.7%. Suggested HPO additions: HP:0002360 Sleep disturbance; HP:0002902 Hyponatremia. (li2021clinicalcharacteristicsand pages 1-2)
EEG phenotype: “Extreme delta brush” is noted in up to 30% of NMDAR antibody encephalitis cases. (hahn2024canadianconsensusguidelines pages 6-7)
3.2 Age of onset / progression patterns
LE typically presents with subacute onset (criterion: <3 months). (graus2016aclinicalapproach pages 6-7) Late-onset anti-NMDAR encephalitis (>45 years in one series) may be oligosymptomatic, has different tumor associations, and worse outcomes in some reports summarized in a 2024 review. (ferreira2024recentadvancesin pages 1-2)
3.3 Quality-of-life and functional impact
Long-term morbidity is substantial in anti-LGI1 encephalitis (a leading LE cause): residual moderate-to-severe cognitive impairment reported in 28.0–66.7%; only 24–43% returned to premorbid activities in cited series; visually detectable hippocampal atrophy in 77.8–88.9%. (li2021clinicalcharacteristicsand pages 1-2)
4. Genetic / molecular information
4.1 Causal genes / pathogenic variants
Autoimmune LE is not typically a monogenic disorder in the retrieved sources. Instead, disease is defined by autoantibody specificity (e.g., anti-LGI1, anti-CASPR2, anti-GABABR, anti-AMPAR, anti-NMDAR) and immune dysregulation.
4.2 Susceptibility genetics
A 2024 review notes HLA associations for anti-LGI1, anti-CASPR2, anti-IgLON5, and anti-GAD syndromes. (ferreira2024recentadvancesin pages 1-2)
4.3 Molecular targets (key “genes” as antigen names)
See antibody table artifact below for major targets, tumor links, and mechanisms.
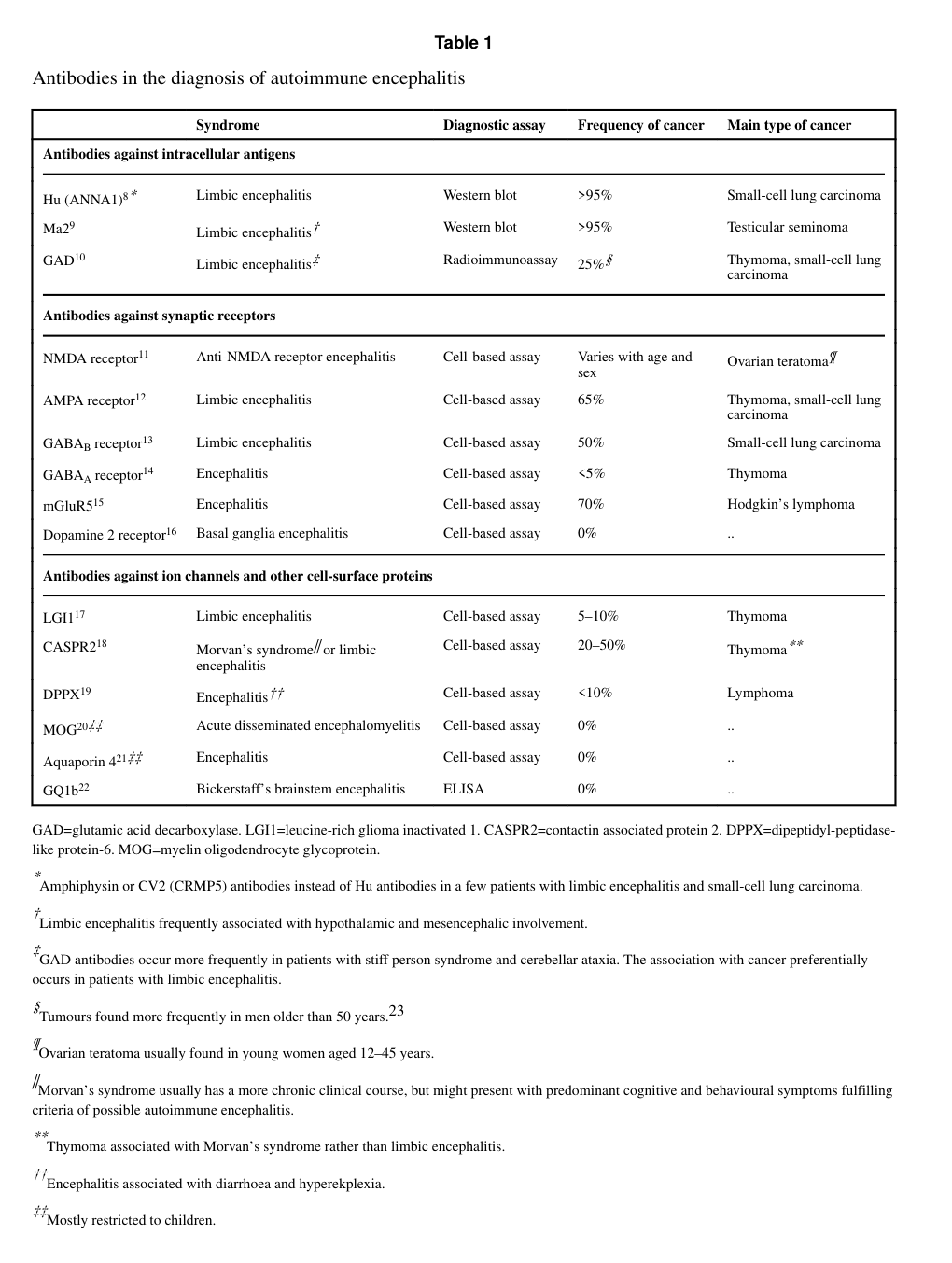
| Antibody/target | Antigen location | Typical syndrome/notes | Common tumor associations and approximate positivity rates if provided | Key mechanistic effect | Key evidence type | Primary sources |
|---|---|---|---|---|---|---|
| LGI1 | Cell-surface/synaptic VGKC-complex–associated protein | Classic autoimmune limbic encephalitis; prominent seizures, memory impairment, psychiatric/behavioral change; faciobrachial dystonic seizures (FBDS) are highly specific; hyponatremia common (graus2016aclinicalapproach pages 6-7, li2021clinicalcharacteristicsand pages 1-2) | Thymoma reported; approximate tumor positivity 5–10% in Graus table (graus2016aclinicalapproach pages 29-29) | Predominantly IgG4-mediated disruption of LGI1–ADAM22/ADAM23 interactions; reduction of synaptic AMPAR and Kv1 channel clusters; impaired LTP; increased excitability; some models suggest BBB tight-junction breakdown and possible complement/inflammatory effects (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 8-10, ryding2023pathophysiologicaleffectsof pages 6-8) | Human clinical cohorts + in vitro/in vivo mechanistic models | Graus 2016, doi: https://doi.org/10.1016/S1474-4422(15)00401-9; Li 2021, doi: https://doi.org/10.3389/fneur.2021.674368; Ryding 2023, doi: https://doi.org/10.3390/cells13010015 (graus2016aclinicalapproach pages 6-7, li2021clinicalcharacteristicsand pages 1-2, ryding2023pathophysiologicaleffectsof pages 4-5) |
| CASPR2 | Cell-surface/paranodal-synaptic protein | Limbic encephalitis spectrum with seizures/cognitive symptoms; can overlap with Morvan syndrome; relevant limbic involvement in autoimmune encephalitis panels (graus2016aclinicalapproach pages 29-29, rada2024riskofseizure pages 1-2) | Thymoma reported; approximate tumor positivity 20–50% in Graus table (graus2016aclinicalapproach pages 29-29) | Disruption of CASPR2–contactin-2 interactions and/or CASPR2 internalization; altered Kv1.2 surface expression, neuronal hyperexcitability, reduced AMPAR currents/LTP, memory impairment; glial activation and increased complement C3 in models (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 10-11, ryding2023pathophysiologicaleffectsof pages 8-10) | Human clinical cohorts + in vitro/in vivo mechanistic models | Graus 2016, doi: https://doi.org/10.1016/S1474-4422(15)00401-9; Rada 2024, doi: https://doi.org/10.1212/NXI.0000000000200225; Ryding 2023, doi: https://doi.org/10.3390/cells13010015 (graus2016aclinicalapproach pages 29-29, rada2024riskofseizure pages 1-2, ryding2023pathophysiologicaleffectsof pages 10-11) |
| GABABR | Cell-surface/synaptic receptor | Autoimmune limbic encephalitis with early and prominent seizures; often included among core limbic AE antibodies (graus2016aclinicalapproach pages 29-29, rada2024riskofseizure pages 1-2) | Small-cell lung carcinoma common; approximate tumor positivity ~50% in Graus table (graus2016aclinicalapproach pages 29-29) | Evidence supports direct inhibition/signaling blockade of receptor function rather than major receptor-expression loss (ryding2023pathophysiologicaleffectsof pages 5-6) | Human clinical association + mechanistic in vitro evidence/review synthesis | Graus 2016, doi: https://doi.org/10.1016/S1474-4422(15)00401-9; Rada 2024, doi: https://doi.org/10.1212/NXI.0000000000200225; Ryding 2023, doi: https://doi.org/10.3390/cells13010015 (graus2016aclinicalapproach pages 29-29, rada2024riskofseizure pages 1-2, ryding2023pathophysiologicaleffectsof pages 5-6) |
| AMPAR | Cell-surface/synaptic glutamate receptor | Limbic encephalitis with memory disturbance, seizures, psychiatric symptoms; important cell-surface limbic AE subtype (graus2016aclinicalapproach pages 29-29) | Thymoma and small-cell lung cancer reported; approximate tumor positivity ~65% in Graus table (graus2016aclinicalapproach pages 29-29) | Receptor internalization and lysosomal degradation, reduced AMPAR-mediated currents, impaired LTP, memory deficits (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 10-11, ryding2023pathophysiologicaleffectsof pages 8-10) | Human clinical association + in vitro/in vivo mechanistic models | Graus 2016, doi: https://doi.org/10.1016/S1474-4422(15)00401-9; Ryding 2023, doi: https://doi.org/10.3390/cells13010015 (graus2016aclinicalapproach pages 29-29, ryding2023pathophysiologicaleffectsof pages 10-11) |
| NMDAR (NR1) | Cell-surface/synaptic glutamate receptor | Broader autoimmune encephalitis phenotype; may involve limbic symptoms including memory deficits, seizures, psychiatric symptoms; anti-NMDAR is a major AE subtype and included in limbic differential/criteria (graus2016aclinicalapproach pages 6-7, ferreira2024recentadvancesin pages 1-2) | Ovarian teratoma association; positivity varies with age/sex in Graus table; review notes ovarian teratoma in nearly 50% of cases in some series, with lower tumor rates (~10%) in some countries (graus2016aclinicalapproach pages 29-29, ferreira2024recentadvancesin pages 1-2) | IgG1-mediated cross-linking, internalization, and lysosomal degradation of NMDAR; suppression of NMDAR-dependent plasticity/LTP; altered excitability and receptor trafficking (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 6-8) | Human clinical cohorts + strong in vitro/in vivo mechanistic evidence | Graus 2016, doi: https://doi.org/10.1016/S1474-4422(15)00401-9; Ferreira 2024, doi: https://doi.org/10.1055/s-0044-1793933; Ryding 2023, doi: https://doi.org/10.3390/cells13010015 (graus2016aclinicalapproach pages 29-29, ferreira2024recentadvancesin pages 1-2, ryding2023pathophysiologicaleffectsof pages 6-8) |
| Ma2 | Intracellular/onconeural antigen | Paraneoplastic limbic encephalitis; intracellular-antibody subgroup generally less responsive to immunotherapy than cell-surface forms (graus2016aclinicalapproach pages 7-9, graus2016aclinicalapproach pages 29-29) | Testicular seminoma; Graus table reports positivity >95% by Western blot (graus2016aclinicalapproach pages 29-29) | Primarily a marker of T-cell–mediated paraneoplastic autoimmunity rather than a directly pathogenic surface-antibody mechanism (ryding2023pathophysiologicaleffectsof pages 1-2, graus2016aclinicalapproach pages 7-9) | Human clinical/paraneoplastic evidence | Graus 2016, doi: https://doi.org/10.1016/S1474-4422(15)00401-9; Ryding 2023, doi: https://doi.org/10.3390/cells13010015 (graus2016aclinicalapproach pages 7-9, graus2016aclinicalapproach pages 29-29, ryding2023pathophysiologicaleffectsof pages 1-2) |
| Hu (ANNA-1) | Intracellular/onconeural antigen | Classic paraneoplastic limbic encephalitis/encephalomyelitis spectrum; intracellular high-risk antibody category with poorer response to immunotherapy (graus2016aclinicalapproach pages 7-9, hahn2024canadianconsensusguidelines pages 8-9) | Strongly cancer-associated; Graus identifies Hu as an onconeuronal antibody linked to cancer, though the supplied excerpt does not give a percentage for Hu specifically (graus2016aclinicalapproach pages 7-9) | Mainly reflects cytotoxic T-cell–mediated neuronal injury rather than receptor internalization/signaling blockade (ryding2023pathophysiologicaleffectsof pages 1-2, graus2016aclinicalapproach pages 7-9) | Human clinical/paraneoplastic evidence | Graus 2016, doi: https://doi.org/10.1016/S1474-4422(15)00401-9; Canadian guideline 2024, doi: https://doi.org/10.1017/cjn.2024.16; Ryding 2023, doi: https://doi.org/10.3390/cells13010015 (graus2016aclinicalapproach pages 7-9, hahn2024canadianconsensusguidelines pages 8-9, ryding2023pathophysiologicaleffectsof pages 1-2) |
| GAD65 | Intracellular enzyme antigen | Limbic encephalitis/autoimmune epilepsy subgroup with predominant seizures; often younger median age in Graus discussion; usually no cancer, but cancer risk higher in older patients or with coexisting GABABR antibodies (graus2016aclinicalapproach pages 7-9) | Graus table reports approximate positivity ~25% and associations with thymoma and small-cell lung carcinoma (graus2016aclinicalapproach pages 29-29) | Intracellular target; direct pathogenicity less established than for surface antibodies, often treated as part of broader autoimmune process rather than classic receptor-internalization mechanism (ryding2023pathophysiologicaleffectsof pages 2-4, ryding2023pathophysiologicaleffectsof pages 1-2) | Human clinical evidence; mechanistic evidence less definitive | Graus 2016, doi: https://doi.org/10.1016/S1474-4422(15)00401-9; Ryding 2023, doi: https://doi.org/10.3390/cells13010015 (graus2016aclinicalapproach pages 7-9, graus2016aclinicalapproach pages 29-29, ryding2023pathophysiologicaleffectsof pages 2-4) |
Table: This table summarizes major antibody-defined subtypes relevant to autoimmune limbic encephalitis, including antigen class, typical clinical patterns, tumor associations, and supported mechanisms. It is useful for comparing cell-surface/synaptic versus intracellular paraneoplastic forms and linking subtype to diagnosis and management.
5. Environmental information
5.1 Infectious triggers
Infectious encephalitis (notably HSV) is a major differential; HSV PCR may be falsely negative early (<24h) and repeat testing is emphasized in diagnostic reasoning. (graus2016aclinicalapproach pages 6-7) The Canadian guideline notes an infectious prodrome is common in autoimmune encephalitis broadly. (hahn2024canadianconsensusguidelines pages 1-2)
5.2 Lifestyle/other exposures
Not identified in retrieved sources for this run.
6. Mechanism / pathophysiology
6.1 Causal chains (examples)
Cell-surface/synaptic antibody LE (often more treatment-responsive): 1) Immune activation leads to production of IgG autoantibodies against neuronal surface/synaptic targets (e.g., NMDAR, AMPAR, LGI1, CASPR2). (li2024clinicalcharacteristicsand pages 1-2, ryding2023pathophysiologicaleffectsof pages 1-2) 2) Antibodies bind accessible extracellular epitopes → functional effects including receptor cross-linking/internalization (NMDAR/AMPAR), disruption of protein–protein interactions (LGI1/CASPR2), or direct signaling blockade (GABABR). (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 6-8, ryding2023pathophysiologicaleffectsof pages 5-6) 3) Synaptic dysfunction (impaired LTP, altered excitability) → limbic symptoms: memory deficits, seizures, psychiatric changes. (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 6-8)
Intracellular/onconeural paraneoplastic LE (often less treatment-responsive): 1) Tumor expression of neuronal antigens → immune response; intracellular antibodies serve as markers of paraneoplastic autoimmunity. 2) Strong cancer association and poorer immunotherapy response relative to cell-surface forms; tumor resection/oncologic therapy becomes central. (graus2016aclinicalapproach pages 7-9, hahn2024canadianconsensusguidelines pages 8-9)
6.2 Antibody-specific mechanistic highlights (selected)
- NMDAR: IgG1-mediated cross-linking → internalization and lysosomal degradation → reduced surface NMDARs; suppression of NMDAR-dependent synaptic plasticity/LTP. (ryding2023pathophysiologicaleffectsof pages 6-8)
- LGI1: antibodies (often IgG4) disrupt LGI1–ADAM22/23 interactions; reduce synaptic AMPAR and Kv1 channel clusters; impair LTP and increase excitability; BBB tight-junction breakdown has been observed in models. (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 8-10)
- CASPR2: disrupt CASPR2–contactin-2 interactions and/or internalize CASPR2; can increase excitability (Kv1.2 changes), associate with glial activation and complement C3 in models. (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 8-10)
- AMPAR: internalization and lysosomal degradation, reduced AMPAR currents, impaired LTP. (ryding2023pathophysiologicaleffectsof pages 10-11)
- GABABR: direct inhibition of receptor function without major receptor-expression change (reviewed evidence). (ryding2023pathophysiologicaleffectsof pages 5-6)
6.3 Suggested ontology terms (mechanisms, cells)
GO biological processes (suggested, based on mechanisms described): - Synaptic signaling / glutamatergic transmission; synaptic plasticity / long-term potentiation (LTP) (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 6-8) - Receptor-mediated endocytosis / receptor internalization (NMDAR/AMPAR) (ryding2023pathophysiologicaleffectsof pages 10-11, ryding2023pathophysiologicaleffectsof pages 6-8) - Complement activation / innate immune response (subset of AE mechanisms) (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 1-2)
Cell Ontology (CL) cell types (suggested): - Hippocampal pyramidal neurons (inferred from hippocampal involvement and LTP mechanisms) (ryding2023pathophysiologicaleffectsof pages 6-8) - Microglia (glial activation in CASPR2 models) (ryding2023pathophysiologicaleffectsof pages 4-5) - Astrocytes (morphologic changes in CASPR2 models) (ryding2023pathophysiologicaleffectsof pages 10-11) - Oligodendrocytes (NMDAR effects on oligodendrocyte GLUT1 described) (ryding2023pathophysiologicaleffectsof pages 6-8)
7. Anatomical structures affected
7.1 Primary localization
- Medial temporal lobes (limbic structures) as the key imaging localization: bilateral medial temporal T2/FLAIR abnormalities are a defining criterion for definite autoimmune LE. (graus2016aclinicalapproach pages 6-7)
7.2 Suggested UBERON terms
- Hippocampus (UBERON:0001954)
- Temporal lobe (UBERON:0001874) (These are ontology suggestions; explicit UBERON IDs were not provided in the retrieved sources.)
8. Temporal development
8.1 Onset pattern
- Subacute onset required by criteria: <3 months. (graus2016aclinicalapproach pages 6-7)
8.2 Course patterns
- Seizures are common in the acute stage; many cases improve with immunotherapy and do not develop chronic epilepsy. (li2024clinicalcharacteristicsand pages 1-2)
- Relapses occur in anti-LGI1 encephalitis; literature range 12.5%–35.3% and in one cohort (n=45) ~13% relapsed over ~33 months. (li2021clinicalcharacteristicsand pages 1-2)
9. Inheritance and population
9.1 Epidemiology
- Encephalitis overall incidence (high-income countries): ~5–10 per 100,000 per year (all-cause encephalitis). (graus2016aclinicalapproach pages 2-4)
- Autoimmune encephalitis (AE) incidence cited in a 2024 review: ~1.2 per 100,000 per year. (ferreira2024recentadvancesin pages 1-2)
- Canadian guideline cites AIE incidence range 0.2–0.8 per 100,000 person-years and notes similar prevalence to infectious encephalitis. (hahn2024canadianconsensusguidelines pages 1-2)
9.2 Population/subtype demographics
Anti-NMDAR encephalitis commonly affects young women and may be associated with ovarian teratoma in nearly 50% of cases in some series; other series report up to 40% male and ~10% neoplasia rates. (ferreira2024recentadvancesin pages 1-2)
10. Diagnostics
10.1 Standardized criteria and core workup
The Graus criteria provide a widely used framework for definite autoimmune limbic encephalitis (see Section 1). (graus2016aclinicalapproach pages 6-7)
National consensus guidelines emphasize a pragmatic workup incorporating MRI/EEG/CSF, paired serum+CSF antibody testing, and malignancy screening.
| Framework/source | Intended diagnosis level | Criteria/workup elements | Notes/thresholds | Source URL + publication month/year |
|---|---|---|---|---|
| Graus et al. 2016, A clinical approach to diagnosis of autoimmune encephalitis | Definite autoimmune limbic encephalitis | 1) Subacute onset of working memory deficits, seizures, or psychiatric symptoms suggesting limbic system involvement; 2) Bilateral brain abnormalities on T2-weighted FLAIR MRI highly restricted to the medial temporal lobes; 3) At least one of: CSF pleocytosis or EEG with epileptic/slow-wave activity involving temporal lobes; 4) Reasonable exclusion of alternative causes (graus2016aclinicalapproach pages 6-7, graus2016aclinicalapproach pages 2-4) | Symptom onset should be <3 months; CSF pleocytosis threshold >5 cells/mm³; 18F-FDG-PET can substitute for criterion 2 if MRI unavailable/negative in some cases; if one of first 3 criteria is missing, diagnosis of definite LE requires detection of antibodies against cell-surface, synaptic, or onconeural proteins (graus2016aclinicalapproach pages 6-7, graus2016aclinicalapproach pages 7-9) | https://doi.org/10.1016/S1474-4422(15)00401-9 — Apr 2016 (graus2016aclinicalapproach pages 6-7, graus2016aclinicalapproach pages 2-4) |
| Graus et al. 2016, syndrome-based AE approach | Possible autoimmune encephalitis / early diagnostic framework | Use clinical syndrome + conventional tests rather than waiting for antibody confirmation: neurologic assessment, MRI, CSF, EEG, differential diagnosis, and staged evidence levels (possible/probable/definite) (graus2016aclinicalapproach pages 2-4) | Designed to avoid over-reliance on antibody tests and treatment response; supports early immunotherapy once mimics are excluded because delayed treatment worsens outcomes (graus2016aclinicalapproach pages 2-4) | https://doi.org/10.1016/S1474-4422(15)00401-9 — Apr 2016 (graus2016aclinicalapproach pages 2-4) |
| Canadian Consensus Guidelines 2024 | Adult AE diagnostic workup in acute care | Core workup includes MRI brain, EEG, CSF, neural antibody testing, repeat/follow-up MRI if initial imaging is unrevealing, and consideration of FDG-PET and malignancy screening where appropriate (hahn2024canadianconsensusguidelines pages 1-2, hahn2024canadianconsensusguidelines pages 6-7) | FDG-PET reported as more sensitive than MRI (87% vs 25–50%) but should not be used alone for diagnosis; whole-body FDG-PET is useful for occult malignancy, especially with intermediate-/high-risk antibodies; EEG contributes to definite limbic AIE criteria (hahn2024canadianconsensusguidelines pages 6-7) | https://doi.org/10.1017/cjn.2024.16 — Feb 2024 (hahn2024canadianconsensusguidelines pages 1-2, hahn2024canadianconsensusguidelines pages 6-7) |
| Canadian Consensus Guidelines 2024 | Ancillary test interpretation | EEG abnormalities support diagnosis; specific recognition of extreme delta brush in anti-NMDAR encephalitis; imaging and antibody results should be interpreted in clinical context (hahn2024canadianconsensusguidelines pages 6-7) | Extreme delta brush occurs in up to 30% of anti-NMDAR encephalitis cases; clinicians should contact testing laboratories for unexpected antibody results and consider confirmatory testing ("TIIF/IHC") for broad neural antibody panels (hahn2024canadianconsensusguidelines pages 6-7) | https://doi.org/10.1017/cjn.2024.16 — Feb 2024 (hahn2024canadianconsensusguidelines pages 6-7) |
| Brazilian Consensus Recommendations 2024 | Possible or definite AE diagnostic workup | Initial investigations should include brain MRI, EEG, CSF analysis, oligoclonal bands, IgG index, and CSF PCR for herpesviruses; collect paired serum and CSF for antineuronal antibody testing before treatment when feasible (dutra2024brazilianconsensusrecommendations pages 7-8) | MRI findings suggestive of AIE include medial temporal T2/FLAIR hyperintensities and multifocal inflammatory/demyelinating changes; herpes simplex and other herpesvirus encephalitides should be excluded with CSF PCR (dutra2024brazilianconsensusrecommendations pages 7-8) | https://doi.org/10.1055/s-0044-1788586 — Jul 2024 (dutra2024brazilianconsensusrecommendations pages 7-8) |
| Brazilian Consensus Recommendations 2024 | Antibody-confirmed AE / comprehensive laboratory workup | Test serum and CSF using both tissue-based assay (TBA) and cell-based assay (CBA); CBA specifically recommended for anti-MOG and anti-glycine receptor antibodies; children should also be screened for anti-MOG (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) | Combined TBA + CBA improves sensitivity/specificity; TBA (rat-brain immunohistochemistry) may detect noncommercial/novel antibodies; the panel recommended against anti-VGKC testing; low-titer serum-only antibodies and low-titer anti-CASPR2 require cautious interpretation (dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) | https://doi.org/10.1055/s-0044-1788586 — Jul 2024 (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) |
| Brazilian Consensus Recommendations 2024 | Cancer/paraneoplastic workup | Perform neoplasm screening at presentation and repeat surveillance for antibodies linked to cancer; use contrast-enhanced CT chest/abdomen/pelvis or MRI if CT contraindicated; consider whole-body FDG-PET if CT is negative (dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) | Screening at presentation had 100% panel agreement; CT chest/abdomen/pelvis 92% agreement; whole-body FDG-PET after negative CT 84% agreement; repeat cancer screening annually for 4 years for tumor-associated antibodies (dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) | https://doi.org/10.1055/s-0044-1788586 — Jul 2024 (dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) |
| Practical cross-framework synthesis | Real-world diagnostic implementation for autoimmune limbic encephalitis | Suspected limbic encephalitis should be approached with rapid syndrome recognition, MRI/EEG/CSF, paired serum+CSF antibody testing, selective FDG-PET when MRI is negative or malignancy is suspected, and prompt exclusion of infectious mimics (graus2016aclinicalapproach pages 6-7, hahn2024canadianconsensusguidelines pages 6-7, dutra2024brazilianconsensusrecommendations pages 7-8) | Key thresholds/features: subacute <3 months, CSF >5 cells/mm³, bilateral medial temporal FLAIR lesions, temporal EEG slow waves/epileptiform activity, extreme delta brush mainly in anti-NMDAR, and annual tumor surveillance for high-risk antibodies (graus2016aclinicalapproach pages 6-7, hahn2024canadianconsensusguidelines pages 6-7, dutra2024brazilianconsensusrecommendations pages 10-11) | Graus 2016: https://doi.org/10.1016/S1474-4422(15)00401-9 (Apr 2016); Canadian 2024: https://doi.org/10.1017/cjn.2024.16 (Feb 2024); Brazilian 2024: https://doi.org/10.1055/s-0044-1788586 (Jul 2024) (graus2016aclinicalapproach pages 6-7, hahn2024canadianconsensusguidelines pages 6-7, dutra2024brazilianconsensusrecommendations pages 10-11) |
Table: This table condenses the core diagnostic criteria for definite autoimmune limbic encephalitis from Graus 2016 and aligns them with 2024 Canadian and Brazilian consensus diagnostic workup recommendations. It is useful for quickly comparing formal criteria, practical testing steps, thresholds, and malignancy-screening guidance.
10.2 Imaging
- MRI: bilateral medial temporal T2/FLAIR hyperintensity is central to definite LE criteria. (graus2016aclinicalapproach pages 6-7)
- FDG-PET: Canadian guideline reports brain FDG-PET may be more sensitive than MRI (87% vs 25–50%) but should not be used alone for diagnosis; whole-body FDG-PET is useful for occult malignancy in higher-risk antibody contexts. (hahn2024canadianconsensusguidelines pages 6-7)
10.3 CSF / EEG
- CSF pleocytosis threshold in definite LE criteria: >5 cells/mm³; mild-to-moderate lymphocytic pleocytosis occurs in 60–80% of AE; IgG index/OCBs in ~50% (Graus). (graus2016aclinicalapproach pages 6-7)
- EEG: temporal epileptic/slow-wave activity supports definite LE. (graus2016aclinicalapproach pages 6-7)
- Extreme delta brush: up to 30% of anti-NMDAR encephalitis. (hahn2024canadianconsensusguidelines pages 6-7)
10.4 Antibody testing (real-world implementation)
Brazilian 2024 consensus recommends testing paired serum and CSF using both tissue-based assay (TBA) and cell-based assay (CBA); TBA can detect noncommercial/novel antibodies; and it recommends against anti-VGKC testing. (dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11)
10.5 Differential diagnosis
HSV and other infections are key mimics; Graus notes HSV PCR can be falsely negative if performed within 24 hours. (graus2016aclinicalapproach pages 6-7)
11. Outcome / prognosis
11.1 Seizure outcomes (quantitative)
A multicenter cohort (n=981 across NMDAR/LGI1/CASPR2/GABABR) estimated the probability of remaining seizure-free for 12 months after achieving 3 months seizure freedom as: NMDAR 0.89, LGI1 0.84, CASPR2 0.82, GABABR 0.76 (Kaplan–Meier). (rada2024riskofseizure pages 1-2)
11.2 Mortality / severe outcomes
In a cohort of AE patients with co-existing multiple neuronal antibodies (n=83), 31.3% (26/83) died during treatment or follow-up; 68.6% had partial/complete recovery. (zhou2024clinicalcharacteristicsof pages 1-2)
11.3 Relapse
Anti-LGI1 relapse rates in literature are reported as 12.5%–35.3%; in one cohort (n=45), ~13% relapsed over follow-up 32.8±13.5 months. (li2021clinicalcharacteristicsand pages 1-2)
11.4 Prognostic factors
A 2024 seizure-focused cohort study in AE found poor prognosis associated with status epilepticus, complications, intubation, higher mRS at discharge, and higher APE2/RITE2 scores; intensive care and higher albumin were associated with reduced risk. (li2024clinicalcharacteristicsand pages 1-2)
12. Treatment
12.1 Consensus treatment algorithms (real-world practice)
Both Canadian (2024) and Brazilian (2024) guidance emphasize early empiric immunotherapy once infection is reasonably excluded and recommend tiered escalation (first-line → second-line → third-line), incorporating cancer treatment when appropriate.
| Framework/source | Treatment tier / decision point | Recommended strategy | Timing for escalation / treatment failure | Dosing examples provided | Neoplasm / other key management notes | Source URL + publication date |
|---|---|---|---|---|---|---|
| Canadian consensus guidelines | Empiric initiation | Start early empiric immunotherapy for suspected autoimmune encephalitis once infectious causes are reasonably excluded; do not delay while awaiting neural antibody results (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7) | Treatment should begin promptly in the acute setting; delay is associated with worse prognosis in guideline rationale (hahn2024canadianconsensusguidelines pages 1-2, hahn2024canadianconsensusguidelines pages 6-7) | Severe AIE combination therapy example: IV methylprednisolone 1 g daily for 5 days plus IVIG 2 g/kg over 2–5 days (hahn2024canadianconsensusguidelines pages 6-7) | Early tumor removal in paraneoplastic encephalitis is crucial; malignancy search is part of workup, especially with intermediate/high-risk neural antibodies (hahn2024canadianconsensusguidelines pages 6-7) | https://doi.org/10.1017/cjn.2024.16; Feb 2024 (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7) |
| Canadian consensus guidelines | First-line therapy | Steroids, IVIG, and/or plasma exchange (PLEX); in severe disease, guideline supports combination therapy rather than waiting for monotherapy failure (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7) | First-line failure defined as lack of improvement or worsening at 5–10 days in severe AIE and 2–4 weeks in mild/moderate AIE; objective measures such as seizure frequency and cognitive testing recommended (hahn2024canadianconsensusguidelines pages 8-9) | IV methylprednisolone 1 g/day ×5 days; IVIG 2 g/kg over 2–5 days; repeat high-dose steroids or repeat PLEX/IVIG can be considered if previously effective (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7) | Follow-up MRI if initial MRI negative but suspicion remains; FDG-PET may be more sensitive than MRI but should not be used alone for diagnosis (hahn2024canadianconsensusguidelines pages 6-7) | https://doi.org/10.1017/cjn.2024.16; Feb 2024 (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7) |
| Canadian consensus guidelines | Second-line therapy: cell-surface antibody or antibody-negative AIE | Prefer rituximab because of efficacy/safety profile in cell-surface antibody disease and antibody-negative AIE (hahn2024canadianconsensusguidelines pages 8-9) | Escalate after first-line failure using above timing windows; failure after second-line is harder to define because onset of action is variable and treatments overlap (hahn2024canadianconsensusguidelines pages 8-9) | Specific rituximab dose not stated in extracted Canadian text (hahn2024canadianconsensusguidelines pages 8-9) | Can use rituximab when cyclophosphamide is contraindicated (hahn2024canadianconsensusguidelines pages 8-9) | https://doi.org/10.1017/cjn.2024.16; Feb 2024 (hahn2024canadianconsensusguidelines pages 8-9) |
| Canadian consensus guidelines | Second-line therapy: paraneoplastic / intracellular high-risk antibody AIE | Prefer cyclophosphamide for paraneoplastic cases and intracellular high-risk antibodies such as Hu or Yo (hahn2024canadianconsensusguidelines pages 8-9) | Escalate after first-line failure; specialist input recommended in severe/refractory disease (hahn2024canadianconsensusguidelines pages 8-9) | Specific cyclophosphamide dose not stated in extracted Canadian text (hahn2024canadianconsensusguidelines pages 8-9) | Strong recommendation for tumor resection and oncology involvement in paraneoplastic encephalitis (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7) | https://doi.org/10.1017/cjn.2024.16; Feb 2024 (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7) |
| Canadian consensus guidelines | Third-line / refractory disease | Tocilizumab or bortezomib used for refractory disease after failure of second-line therapy; myeloablative cyclophosphamide may be considered in selected severe cases with specialist input (hahn2024canadianconsensusguidelines pages 8-9) | No fixed universal failure interval after second-line because response kinetics vary (hahn2024canadianconsensusguidelines pages 8-9) | Specific tocilizumab/bortezomib doses not stated in extracted Canadian text (hahn2024canadianconsensusguidelines pages 8-9) | Guideline notes evidence base is limited and largely observational/consensus-driven, except one positive RCT for IVIG in LGI1/CASPR2-seropositive patients (hahn2024canadianconsensusguidelines pages 6-7) | https://doi.org/10.1017/cjn.2024.16; Feb 2024 (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7) |
| Brazilian consensus recommendations | Empiric initiation | Treat possible or definite AIE; consensus states treatment should be started within the first 4 weeks of symptoms and should not wait for complete antibody confirmation when suspicion is high (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) | If there is no satisfactory clinical/functional improvement within 10–14 days, start second-line therapy (dutra2024brazilianconsensusrecommendations pages 7-8) | First-line usually combines methylprednisolone with IVIG or plasmapheresis (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 8-10) | Prognosis is associated with treatment within the first 4 weeks; panel recommends neoplasm screening at presentation (dutra2024brazilianconsensusrecommendations pages 10-11) | https://doi.org/10.1055/s-0044-1788586; Jul 2024 (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) |
| Brazilian consensus recommendations | First-line therapy | Preferred first-line is combination therapy: methylprednisolone + IVIG or methylprednisolone + plasmapheresis; MP, IVIG, and PLEX may be given concomitantly depending on availability/experience (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) | Assess for clinical/functional response over 10–14 days (dutra2024brazilianconsensusrecommendations pages 7-8) | IVIG 2 g/kg over 2–5 days; IV methylprednisolone adults 1,000 mg/day for 3–5 days; children 20–30 mg/kg/day, max 1 g/day for 3–5 days; plasmapheresis 5–7 sessions over 7–14 days (dutra2024brazilianconsensusrecommendations pages 8-10) | Rule out herpesvirus encephalitis with CSF PCR; MRI/EEG/CSF are part of parallel workup (dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 7-8) | https://doi.org/10.1055/s-0044-1788586; Jul 2024 (dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 7-8) |
| Brazilian consensus recommendations | Second-line therapy | Rituximab and/or cyclophosphamide for refractory disease or inadequate response to first-line therapy (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 10-11) | Start after 10–14 days without satisfactory improvement (dutra2024brazilianconsensusrecommendations pages 7-8) | Rituximab: acceptable regimens include 500–1,000 mg twice 2 weeks apart or 375 mg/m² weekly ×4; cyclophosphamide 500–1,000 mg/m² IV monthly pulses (dutra2024brazilianconsensusrecommendations pages 8-10) | Rituximab supported by better functional outcomes and fewer relapses, especially in anti-NMDAR; cyclophosphamide favored when rituximab unavailable or in selected refractory patients >16 years (dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 10-11) | https://doi.org/10.1055/s-0044-1788586; Jul 2024 (dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 10-11) |
| Brazilian consensus recommendations | Third-line therapy | Tocilizumab and bortezomib are third-line options for refractory disease (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 10-11) | Used after failure of second-line therapy in refractory cases (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 8-10) | Tocilizumab: monthly IV dosing with pediatric/adult weight-based regimens; bortezomib: 3 cycles of 21 days, given subcutaneously on days 1, 4, 8, 11 (dutra2024brazilianconsensusrecommendations pages 8-10) | Intended for highly refractory disease; evidence base remains limited compared with first-/second-line treatments (dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 10-11) | https://doi.org/10.1055/s-0044-1788586; Jul 2024 (dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 10-11) |
| Brazilian consensus recommendations | Maintenance / long-term therapy | Maintenance may include monthly IVIG in selected cases; routine long-term azathioprine/mycophenolate is not supported by current evidence, and oral immunosuppressants should not be used in anti-NMDAR according to panel consensus (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) | Long-term strategy individualized after acute response (dutra2024brazilianconsensusrecommendations pages 7-8) | No standardized dose extracted for monthly IVIG maintenance (dutra2024brazilianconsensusrecommendations pages 7-8) | ASMs are for seizure control; most seizures are acute symptomatic and may be weaned after acute stage (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 10-11) | https://doi.org/10.1055/s-0044-1788586; Jul 2024 (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 8-10, dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) |
| Brazilian consensus recommendations | Neoplasm management | Screen for neoplasia at presentation in all patients; for antibodies commonly linked to cancer, continue surveillance (dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) | Repeat screening annually for 4 years when antibodies are commonly tumor-associated (dutra2024brazilianconsensusrecommendations pages 7-8, dutra2024brazilianconsensusrecommendations pages 10-11) | Initial screening examples: contrast-enhanced CT chest/abdomen/pelvis; MRI if CT contraindicated; consider whole-body FDG-PET if CT is negative (dutra2024brazilianconsensusrecommendations pages 10-11) | Integrates AE care with oncology; parallels Canadian emphasis on early tumor treatment in paraneoplastic disease (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7, dutra2024brazilianconsensusrecommendations pages 10-11) | https://doi.org/10.1055/s-0044-1788586; Jul 2024; https://doi.org/10.1017/cjn.2024.16; Feb 2024 (hahn2024canadianconsensusguidelines pages 8-9, hahn2024canadianconsensusguidelines pages 6-7, dutra2024brazilianconsensusrecommendations pages 10-11) |
Table: This table summarizes consensus treatment pathways for autoimmune encephalitis and limbic encephalitis from the 2024 Canadian and Brazilian guidelines. It highlights empiric treatment timing, escalation thresholds, drug tiers, dosing examples where available, and tumor-management recommendations.
12.2 Key guideline points (selected)
- Canadian guideline: do not delay immunotherapy waiting for antibody results; severe AIE example: IV methylprednisolone 1 g/day ×5 days + IVIG 2 g/kg over 2–5 days. (hahn2024canadianconsensusguidelines pages 6-7)
- Canadian guideline: first-line failure defined as no improvement/worsening at 5–10 days (severe) or 2–4 weeks (mild/moderate). (hahn2024canadianconsensusguidelines pages 8-9)
- Brazilian guideline: start treatment within first 4 weeks of symptoms; first-line combination MP + IVIG or MP + plasmapheresis; second-line rituximab/cyclophosphamide; third-line tocilizumab/bortezomib; provides dosing regimens. (dutra2024brazilianconsensusrecommendations pages 1-2, dutra2024brazilianconsensusrecommendations pages 8-10)
12.3 MAXO (suggested) terms
- High-dose intravenous corticosteroid therapy
- Intravenous immunoglobulin therapy
- Therapeutic plasma exchange
- B-cell depletion therapy (rituximab)
- Alkylating agent immunosuppression (cyclophosphamide)
- IL-6 receptor inhibitor therapy (tocilizumab; satralizumab investigational)
- Proteasome inhibitor therapy (bortezomib) (These are ontology suggestions; MAXO IDs were not provided in retrieved sources.)
12.4 Recent developments / latest research (2023–2024 prioritized)
Targeted cytokine pathway therapy in trials: The Phase 3 basket RCT CIELO (NCT05503264) evaluates satralizumab (IL-6R inhibition) in NMDAR-IgG+ or LGI1-IgG+ autoimmune encephalitis; primary endpoint includes ≥1-point mRS improvement and no rescue at Week 24; the design allows background immunosuppression and rescue therapies to mirror real-world care. (lee2024innovationandoptimization pages 1-2, lee2024innovationandoptimization pages 3-4)
13. Prevention
There are no established primary prevention strategies for autoimmune LE in the retrieved sources. Secondary/tertiary prevention in practice centers on: - Early recognition and early immunotherapy (avoid delayed treatment). (graus2016aclinicalapproach pages 2-4, hahn2024canadianconsensusguidelines pages 6-7) - Cancer screening and surveillance in tumor-associated antibody contexts (annual for 4 years in Brazilian consensus). (dutra2024brazilianconsensusrecommendations pages 10-11)
14. Other species / natural disease
Not addressed in retrieved sources for this run.
15. Model organisms
Mechanistic understanding is supported by in vitro neuronal culture models, passive transfer approaches, and in vivo mouse models showing receptor internalization, synaptic dysfunction, memory deficits, and seizure phenotypes for several antibody types (e.g., NMDAR, LGI1, CASPR2, AMPAR). (ryding2023pathophysiologicaleffectsof pages 4-5, ryding2023pathophysiologicaleffectsof pages 10-11, ryding2023pathophysiologicaleffectsof pages 6-8)
Figures / tables (visual evidence)
- Diagnostic criteria and antibody–tumor association table from Graus 2016 were retrieved as cropped images supporting (i) possible AE criteria, (ii) definite autoimmune limbic encephalitis criteria, and (iii) antibody/tumor associations. (graus2016aclinicalapproach media eb6ebeb5, graus2016aclinicalapproach media fdd6abe4, graus2016aclinicalapproach media be8b1f92, graus2016aclinicalapproach media 2946d09a)
Evidence gaps and limitations for knowledge-base population
- Disease identifiers (MONDO/MeSH/ICD/Orphanet/OMIM): not present in the retrieved full texts; therefore not asserted.
- PMIDs: The tool outputs provided DOIs/URLs and bibliographic metadata but did not provide PMIDs; therefore PMIDs are not asserted.
- Environmental/lifestyle risk and protective factors, gene–environment interactions, and cross-species models: not supported by retrieved evidence in this run.
References
-
(graus2016aclinicalapproach pages 6-7): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(graus2016aclinicalapproach pages 7-9): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(graus2016aclinicalapproach pages 2-4): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(hahn2024canadianconsensusguidelines pages 8-9): Christopher Hahn, Adrian Budhram, Katayoun Alikhani, Nasser AlOhaly, Grayson Beecher, Gregg Blevins, John Brooks, Robert Carruthers, Jacynthe Comtois, Juthaporn Cowan, Paula de Robles, Julien Hébert, Ronak K. Kapadia, Sarah Lapointe, Aaron Mackie, Warren Mason, Brienne McLane, Alexandra Muccilli, Ilia Poliakov, Penelope Smyth, Kimberly G. Williams, Christopher Uy, and Jennifer A. McCombe. Canadian consensus guidelines for the diagnosis and treatment of autoimmune encephalitis in adults. Canadian Journal of Neurological Sciences / Journal Canadien des Sciences Neurologiques, 51:734-754, Feb 2024. URL: https://doi.org/10.1017/cjn.2024.16, doi:10.1017/cjn.2024.16. This article has 33 citations.
-
(dutra2024brazilianconsensusrecommendations pages 1-2): Lívia Almeida Dutra, Pedro Victor de Castro Silva, João Henrique Fregadolli Ferreira, Alexandre Coelho Marques, Fabio Fieni Toso, Claudia Cristina Ferreira Vasconcelos, Doralina Guimarães Brum, Samira Luisa dos Apóstolos Pereira, Tarso Adoni, Leticia Januzi de Almeida Rocha, Leticia Pereira de Brito Sampaio, Nise Alessandra de Carvalho Sousa, Renata Barbosa Paolilo, Angélica Dal Pizzol, Bruna Klein da Costa, Caio César Diniz Disserol, Camila Pupe, Daniel Almeida do Valle, Denise Sisterolli Diniz, Fabiano Ferreira de Abrantes, Felipe da Rocha Schmidt, Fernando Cendes, Francisco Tomaz Meneses de Oliveira, Gabriela Joca Martins, Guilherme Diogo Silva, Katia Lin, Lécio Figueira Pinto, Mara Lúcia Schimtz Ferreira Santos, Marcus Vinícius Magno Gonçalves, Mariana Braatz Krueger, Michel Elyas Jung Haziot, Orlando Graziani Povoas Barsottini, Osvaldo José Moreira do Nascimento, Paulo Ribeiro Nóbrega, Priscilla Mara Proveti, Raphael Machado do Castilhos, Vanessa Daccach, and Felipe von Glehn. Brazilian consensus recommendations on the diagnosis and treatment of autoimmune encephalitis in the adult and pediatric populations. Arquivos de Neuro-Psiquiatria, 82:001-015, Jul 2024. URL: https://doi.org/10.1055/s-0044-1788586, doi:10.1055/s-0044-1788586. This article has 11 citations and is from a peer-reviewed journal.
-
(rada2024riskofseizure pages 1-2): Anna Rada, Anne Hagemann, Charlotte Aaberg Poulsen, Tobias Baumgartner, Timea Berki, Morten Blaabjerg, Juliette Brenner, Jeffrey W. Britton, Andrew Christiana, Nicolás L. Ciano-Petersen, Yvette Crijnen, Martin Elišák, Antonio Farina, Alec R. Friedman, Zsófia Hayden, Julien Hébert, Martin Holtkamp, Zhen Hong, Jerome Honnorat, Maria Ilyas-Feldmann, Sarosh R. Irani, Stjepana Kovac, Petr Marusic, Sergio Muñiz-Castrillo, Sudarshini Ramanathan, Kelsey M. Smith, Claude Steriade, Christine Strippel, Rainer Surges, Maarten J. Titulaer, Christopher E. Uy, Juna M. de Vries, Christian G. Bien, and Ulrich Specht. Risk of seizure recurrence due to autoimmune encephalitis with nmdar, lgi1, caspr2, and gaba b r antibodies. Neurology Neuroimmunology & Neuroinflammation, Jul 2024. URL: https://doi.org/10.1212/nxi.0000000000200225, doi:10.1212/nxi.0000000000200225. This article has 13 citations.
-
(ryding2023pathophysiologicaleffectsof pages 4-5): Matias Ryding, Anne With Mikkelsen, Mette Scheller Nissen, Anna Christine Nilsson, and Morten Blaabjerg. Pathophysiological effects of autoantibodies in autoimmune encephalitides. Cells, 13:15, Dec 2023. URL: https://doi.org/10.3390/cells13010015, doi:10.3390/cells13010015. This article has 16 citations.
-
(li2024clinicalcharacteristicsand pages 1-2): Mengyun Li, Qing Zhang, Xu Wang, Bofei Tan, and Qiang Liu. Clinical characteristics and prognosis analysis of acute symptomatic seizures secondary to autoimmune encephalitis. Frontiers in Neurology, Oct 2024. URL: https://doi.org/10.3389/fneur.2024.1474888, doi:10.3389/fneur.2024.1474888. This article has 4 citations and is from a peer-reviewed journal.
-
(graus2016aclinicalapproach pages 29-29): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(zhou2024clinicalcharacteristicsof pages 1-2): Yiyi Zhou, Hao Chen, Min Zhu, Menghua Li, Lianqun Wang, Zunchun Xie, Mei-hong Zhou, Xiaomu Wu, and Daojun Hong. Clinical characteristics of autoimmune encephalitis with co-existence of multiple anti-neuronal antibodies. BMC Neurology, Jan 2024. URL: https://doi.org/10.1186/s12883-023-03514-x, doi:10.1186/s12883-023-03514-x. This article has 7 citations and is from a peer-reviewed journal.
-
(li2021clinicalcharacteristicsand pages 1-2): Tao-Ran Li, Yu-Di Zhang, Qun Wang, Xiao-Qiu Shao, Di-Yang Lyu, and Rui-Juan Lv. Clinical characteristics and long-term prognosis of anti-lgi1 encephalitis: a single-center cohort study in beijing, china. Frontiers in Neurology, Jun 2021. URL: https://doi.org/10.3389/fneur.2021.674368, doi:10.3389/fneur.2021.674368. This article has 37 citations and is from a peer-reviewed journal.
-
(hahn2024canadianconsensusguidelines pages 6-7): Christopher Hahn, Adrian Budhram, Katayoun Alikhani, Nasser AlOhaly, Grayson Beecher, Gregg Blevins, John Brooks, Robert Carruthers, Jacynthe Comtois, Juthaporn Cowan, Paula de Robles, Julien Hébert, Ronak K. Kapadia, Sarah Lapointe, Aaron Mackie, Warren Mason, Brienne McLane, Alexandra Muccilli, Ilia Poliakov, Penelope Smyth, Kimberly G. Williams, Christopher Uy, and Jennifer A. McCombe. Canadian consensus guidelines for the diagnosis and treatment of autoimmune encephalitis in adults. Canadian Journal of Neurological Sciences / Journal Canadien des Sciences Neurologiques, 51:734-754, Feb 2024. URL: https://doi.org/10.1017/cjn.2024.16, doi:10.1017/cjn.2024.16. This article has 33 citations.
-
(ferreira2024recentadvancesin pages 1-2): João Henrique Fregadolli Ferreira, Caio César Diniz Disserol, Bruna de Freitas Dias, Alexandre Coelho Marques, Marina Driemeier Cardoso, Pedro Victor de Castro Silva, Fabio Fieni Toso, and Lívia Almeida Dutra. Recent advances in autoimmune encephalitis. Arquivos de Neuro-Psiquiatria, 82:001-013, Dec 2024. URL: https://doi.org/10.1055/s-0044-1793933, doi:10.1055/s-0044-1793933. This article has 6 citations and is from a peer-reviewed journal.
-
(ryding2023pathophysiologicaleffectsof pages 8-10): Matias Ryding, Anne With Mikkelsen, Mette Scheller Nissen, Anna Christine Nilsson, and Morten Blaabjerg. Pathophysiological effects of autoantibodies in autoimmune encephalitides. Cells, 13:15, Dec 2023. URL: https://doi.org/10.3390/cells13010015, doi:10.3390/cells13010015. This article has 16 citations.
-
(ryding2023pathophysiologicaleffectsof pages 6-8): Matias Ryding, Anne With Mikkelsen, Mette Scheller Nissen, Anna Christine Nilsson, and Morten Blaabjerg. Pathophysiological effects of autoantibodies in autoimmune encephalitides. Cells, 13:15, Dec 2023. URL: https://doi.org/10.3390/cells13010015, doi:10.3390/cells13010015. This article has 16 citations.
-
(ryding2023pathophysiologicaleffectsof pages 10-11): Matias Ryding, Anne With Mikkelsen, Mette Scheller Nissen, Anna Christine Nilsson, and Morten Blaabjerg. Pathophysiological effects of autoantibodies in autoimmune encephalitides. Cells, 13:15, Dec 2023. URL: https://doi.org/10.3390/cells13010015, doi:10.3390/cells13010015. This article has 16 citations.
-
(ryding2023pathophysiologicaleffectsof pages 5-6): Matias Ryding, Anne With Mikkelsen, Mette Scheller Nissen, Anna Christine Nilsson, and Morten Blaabjerg. Pathophysiological effects of autoantibodies in autoimmune encephalitides. Cells, 13:15, Dec 2023. URL: https://doi.org/10.3390/cells13010015, doi:10.3390/cells13010015. This article has 16 citations.
-
(ryding2023pathophysiologicaleffectsof pages 1-2): Matias Ryding, Anne With Mikkelsen, Mette Scheller Nissen, Anna Christine Nilsson, and Morten Blaabjerg. Pathophysiological effects of autoantibodies in autoimmune encephalitides. Cells, 13:15, Dec 2023. URL: https://doi.org/10.3390/cells13010015, doi:10.3390/cells13010015. This article has 16 citations.
-
(ryding2023pathophysiologicaleffectsof pages 2-4): Matias Ryding, Anne With Mikkelsen, Mette Scheller Nissen, Anna Christine Nilsson, and Morten Blaabjerg. Pathophysiological effects of autoantibodies in autoimmune encephalitides. Cells, 13:15, Dec 2023. URL: https://doi.org/10.3390/cells13010015, doi:10.3390/cells13010015. This article has 16 citations.
-
(hahn2024canadianconsensusguidelines pages 1-2): Christopher Hahn, Adrian Budhram, Katayoun Alikhani, Nasser AlOhaly, Grayson Beecher, Gregg Blevins, John Brooks, Robert Carruthers, Jacynthe Comtois, Juthaporn Cowan, Paula de Robles, Julien Hébert, Ronak K. Kapadia, Sarah Lapointe, Aaron Mackie, Warren Mason, Brienne McLane, Alexandra Muccilli, Ilia Poliakov, Penelope Smyth, Kimberly G. Williams, Christopher Uy, and Jennifer A. McCombe. Canadian consensus guidelines for the diagnosis and treatment of autoimmune encephalitis in adults. Canadian Journal of Neurological Sciences / Journal Canadien des Sciences Neurologiques, 51:734-754, Feb 2024. URL: https://doi.org/10.1017/cjn.2024.16, doi:10.1017/cjn.2024.16. This article has 33 citations.
-
(dutra2024brazilianconsensusrecommendations pages 7-8): Lívia Almeida Dutra, Pedro Victor de Castro Silva, João Henrique Fregadolli Ferreira, Alexandre Coelho Marques, Fabio Fieni Toso, Claudia Cristina Ferreira Vasconcelos, Doralina Guimarães Brum, Samira Luisa dos Apóstolos Pereira, Tarso Adoni, Leticia Januzi de Almeida Rocha, Leticia Pereira de Brito Sampaio, Nise Alessandra de Carvalho Sousa, Renata Barbosa Paolilo, Angélica Dal Pizzol, Bruna Klein da Costa, Caio César Diniz Disserol, Camila Pupe, Daniel Almeida do Valle, Denise Sisterolli Diniz, Fabiano Ferreira de Abrantes, Felipe da Rocha Schmidt, Fernando Cendes, Francisco Tomaz Meneses de Oliveira, Gabriela Joca Martins, Guilherme Diogo Silva, Katia Lin, Lécio Figueira Pinto, Mara Lúcia Schimtz Ferreira Santos, Marcus Vinícius Magno Gonçalves, Mariana Braatz Krueger, Michel Elyas Jung Haziot, Orlando Graziani Povoas Barsottini, Osvaldo José Moreira do Nascimento, Paulo Ribeiro Nóbrega, Priscilla Mara Proveti, Raphael Machado do Castilhos, Vanessa Daccach, and Felipe von Glehn. Brazilian consensus recommendations on the diagnosis and treatment of autoimmune encephalitis in the adult and pediatric populations. Arquivos de Neuro-Psiquiatria, 82:001-015, Jul 2024. URL: https://doi.org/10.1055/s-0044-1788586, doi:10.1055/s-0044-1788586. This article has 11 citations and is from a peer-reviewed journal.
-
(dutra2024brazilianconsensusrecommendations pages 10-11): Lívia Almeida Dutra, Pedro Victor de Castro Silva, João Henrique Fregadolli Ferreira, Alexandre Coelho Marques, Fabio Fieni Toso, Claudia Cristina Ferreira Vasconcelos, Doralina Guimarães Brum, Samira Luisa dos Apóstolos Pereira, Tarso Adoni, Leticia Januzi de Almeida Rocha, Leticia Pereira de Brito Sampaio, Nise Alessandra de Carvalho Sousa, Renata Barbosa Paolilo, Angélica Dal Pizzol, Bruna Klein da Costa, Caio César Diniz Disserol, Camila Pupe, Daniel Almeida do Valle, Denise Sisterolli Diniz, Fabiano Ferreira de Abrantes, Felipe da Rocha Schmidt, Fernando Cendes, Francisco Tomaz Meneses de Oliveira, Gabriela Joca Martins, Guilherme Diogo Silva, Katia Lin, Lécio Figueira Pinto, Mara Lúcia Schimtz Ferreira Santos, Marcus Vinícius Magno Gonçalves, Mariana Braatz Krueger, Michel Elyas Jung Haziot, Orlando Graziani Povoas Barsottini, Osvaldo José Moreira do Nascimento, Paulo Ribeiro Nóbrega, Priscilla Mara Proveti, Raphael Machado do Castilhos, Vanessa Daccach, and Felipe von Glehn. Brazilian consensus recommendations on the diagnosis and treatment of autoimmune encephalitis in the adult and pediatric populations. Arquivos de Neuro-Psiquiatria, 82:001-015, Jul 2024. URL: https://doi.org/10.1055/s-0044-1788586, doi:10.1055/s-0044-1788586. This article has 11 citations and is from a peer-reviewed journal.
-
(dutra2024brazilianconsensusrecommendations pages 8-10): Lívia Almeida Dutra, Pedro Victor de Castro Silva, João Henrique Fregadolli Ferreira, Alexandre Coelho Marques, Fabio Fieni Toso, Claudia Cristina Ferreira Vasconcelos, Doralina Guimarães Brum, Samira Luisa dos Apóstolos Pereira, Tarso Adoni, Leticia Januzi de Almeida Rocha, Leticia Pereira de Brito Sampaio, Nise Alessandra de Carvalho Sousa, Renata Barbosa Paolilo, Angélica Dal Pizzol, Bruna Klein da Costa, Caio César Diniz Disserol, Camila Pupe, Daniel Almeida do Valle, Denise Sisterolli Diniz, Fabiano Ferreira de Abrantes, Felipe da Rocha Schmidt, Fernando Cendes, Francisco Tomaz Meneses de Oliveira, Gabriela Joca Martins, Guilherme Diogo Silva, Katia Lin, Lécio Figueira Pinto, Mara Lúcia Schimtz Ferreira Santos, Marcus Vinícius Magno Gonçalves, Mariana Braatz Krueger, Michel Elyas Jung Haziot, Orlando Graziani Povoas Barsottini, Osvaldo José Moreira do Nascimento, Paulo Ribeiro Nóbrega, Priscilla Mara Proveti, Raphael Machado do Castilhos, Vanessa Daccach, and Felipe von Glehn. Brazilian consensus recommendations on the diagnosis and treatment of autoimmune encephalitis in the adult and pediatric populations. Arquivos de Neuro-Psiquiatria, 82:001-015, Jul 2024. URL: https://doi.org/10.1055/s-0044-1788586, doi:10.1055/s-0044-1788586. This article has 11 citations and is from a peer-reviewed journal.
-
(lee2024innovationandoptimization pages 1-2): Soon-Tae Lee, Hesham Abboud, Sarosh R. Irani, Hideto Nakajima, Amanda L. Piquet, Sean J. Pittock, E. Ann Yeh, Jiawei Wang, Sharmila Rajan, James Overell, Jillian Smith, Jane St Lambert, Muna El-Khairi, Marina Gafarova, and Jeffrey M. Gelfand. Innovation and optimization in autoimmune encephalitis trials: the design and rationale for the phase 3, randomized study of satralizumab in patients with nmdar-igg-antibody-positive or lgi1-igg-antibody-positive autoimmune encephalitis (cielo). Frontiers in Neurology, Aug 2024. URL: https://doi.org/10.3389/fneur.2024.1437913, doi:10.3389/fneur.2024.1437913. This article has 20 citations and is from a peer-reviewed journal.
-
(lee2024innovationandoptimization pages 3-4): Soon-Tae Lee, Hesham Abboud, Sarosh R. Irani, Hideto Nakajima, Amanda L. Piquet, Sean J. Pittock, E. Ann Yeh, Jiawei Wang, Sharmila Rajan, James Overell, Jillian Smith, Jane St Lambert, Muna El-Khairi, Marina Gafarova, and Jeffrey M. Gelfand. Innovation and optimization in autoimmune encephalitis trials: the design and rationale for the phase 3, randomized study of satralizumab in patients with nmdar-igg-antibody-positive or lgi1-igg-antibody-positive autoimmune encephalitis (cielo). Frontiers in Neurology, Aug 2024. URL: https://doi.org/10.3389/fneur.2024.1437913, doi:10.3389/fneur.2024.1437913. This article has 20 citations and is from a peer-reviewed journal.
-
(graus2016aclinicalapproach media eb6ebeb5): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(graus2016aclinicalapproach media fdd6abe4): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(graus2016aclinicalapproach media be8b1f92): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(graus2016aclinicalapproach media 2946d09a): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.