Hemophagocytic Lymphohistiocytosis
Hereditary (familial/primary) hemophagocytic lymphohistiocytosis (HLH) is a life-threatening hyperinflammatory syndrome caused by biallelic (or, for the X-linked syndromic forms, hemizygous) germline defects in the perforin / granule-exocytosis cytotoxicity pathway of cytotoxic T lymphocytes (CTLs) and natural killer (NK) cells. Loss of pore-forming perforin (PRF1) or of the granule docking/priming/fusion machinery (UNC13D/Munc13-4, STX11/syntaxin-11, STXBP2/Munc18-2), or of upstream granule trafficking/biogenesis components (RAB27A in Griscelli syndrome type 2, LYST in Chediak-Higashi syndrome), impairs the ability of CTLs and NK cells to kill infected or antigen-presenting target cells. Failure to clear the antigenic stimulus and to contract the immune response results in sustained, uncontrolled activation and proliferation of T lymphocytes and macrophages, an interferon-gamma-driven cytokine storm, and tissue infiltration by activated histiocytes that engulf blood cells (hemophagocytosis). Clinically this produces the cardinal features of prolonged high fever, hepatosplenomegaly, bi- or trilineage cytopenias, hyperferritinemia, hypertriglyceridemia, and hypofibrinogenemia, with frequent CNS involvement. The X-linked lymphoproliferative syndromes (SH2D1A/SAP = XLP1; XIAP/BIRC4 = XLP2) predispose to EBV-triggered HLH through defective NKT-cell development and lymphocyte homeostasis. Untreated active familial HLH is rapidly fatal; the HLH-94/HLH-2004 etoposide-dexamethasone protocols, anti-interferon-gamma antibody (emapalumab), and allogeneic hematopoietic stem cell transplantation (the only curative therapy) have improved survival.
Ask OpenScientist
Ask a research question about Hemophagocytic Lymphohistiocytosis. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Classifications
Subtypes
8Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Pathophysiology
3Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Phenotypes
9Blood 1
Show evidence (1 reference)
Cardiovascular 1
Show evidence (1 reference)
Metabolism 4
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Nervous System 1
Show evidence (1 reference)
Other 2
Show evidence (1 reference)
Show evidence (1 reference)
Genetic Associations
8Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Medical Actions
3Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Source YAML
click to showname: Hemophagocytic Lymphohistiocytosis
creation_date: "2026-06-09T01:41:00Z"
category: Mendelian
disease_term:
preferred_term: hereditary hemophagocytic lymphohistiocytosis
term:
id: MONDO:0015541
label: hereditary hemophagocytic lymphohistiocytosis
parents:
- immune dysregulation disorder
- inborn error of immunity
description: >
Hereditary (familial/primary) hemophagocytic lymphohistiocytosis (HLH) is a
life-threatening hyperinflammatory syndrome caused by biallelic (or, for the
X-linked syndromic forms, hemizygous) germline defects in the perforin /
granule-exocytosis cytotoxicity pathway of cytotoxic T lymphocytes (CTLs) and
natural killer (NK) cells. Loss of pore-forming perforin (PRF1) or of the
granule docking/priming/fusion machinery (UNC13D/Munc13-4, STX11/syntaxin-11,
STXBP2/Munc18-2), or of upstream granule trafficking/biogenesis components
(RAB27A in Griscelli syndrome type 2, LYST in Chediak-Higashi syndrome),
impairs the ability of CTLs and NK cells to kill infected or
antigen-presenting target cells. Failure to clear the antigenic stimulus and
to contract the immune response results in sustained, uncontrolled activation
and proliferation of T lymphocytes and macrophages, an interferon-gamma-driven
cytokine storm, and tissue infiltration by activated histiocytes that engulf
blood cells (hemophagocytosis). Clinically this produces the cardinal features
of prolonged high fever, hepatosplenomegaly, bi- or trilineage cytopenias,
hyperferritinemia, hypertriglyceridemia, and hypofibrinogenemia, with frequent
CNS involvement. The X-linked lymphoproliferative syndromes (SH2D1A/SAP =
XLP1; XIAP/BIRC4 = XLP2) predispose to EBV-triggered HLH through defective
NKT-cell development and lymphocyte homeostasis. Untreated active familial HLH
is rapidly fatal; the HLH-94/HLH-2004 etoposide-dexamethasone protocols,
anti-interferon-gamma antibody (emapalumab), and allogeneic hematopoietic
stem cell transplantation (the only curative therapy) have improved survival.
classifications:
harrisons_chapter:
- classification_value: IMMUNE_RHEUMATOLOGIC
evidence:
- reference: PMID:20301617
reference_title: Familial Hemophagocytic Lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "an immune deficiency characterized by the overactivation and excessive proliferation of T lymphocytes and macrophages"
explanation: GeneReviews characterizes familial HLH as an immune-mediated hyperinflammatory disorder, supporting placement in Harrison's immune/rheumatologic Part.
- classification_value: GENETICS_ENVIRONMENT_DISEASE
evidence:
- reference: PMID:35748970
reference_title: "Human Inborn Errors of Immunity: 2022 Update on the Classification from the International Union of Immunological Societies Expert Committee."
supports: SUPPORT
evidence_source: OTHER
snippet: "There are now a total of 485 inborn errors of immunity."
explanation: The IUIS classifies hereditary HLH among the monogenic inborn errors of immunity, supporting placement in Harrison's genetics Part.
iuis_category:
classification_value: immune dysregulation
evidence:
- reference: PMID:35748970
reference_title: "Human Inborn Errors of Immunity: 2022 Update on the Classification from the International Union of Immunological Societies Expert Committee."
supports: SUPPORT
evidence_source: OTHER
snippet: "We report the updated classification of inborn errors of immunity"
explanation: The IUIS phenotypic classification places familial HLH in Table 4, Diseases of Immune Dysregulation.
references:
- reference: PMID:20301617
title: "Familial Hemophagocytic Lymphohistiocytosis."
tags:
- GeneReviews
- reference: PMID:20301580
title: "X-Linked Lymphoproliferative Disease."
tags:
- GeneReviews
- reference: PMID:20301751
title: "Chediak-Higashi Syndrome."
tags:
- GeneReviews
has_subtypes:
- name: FHL2
display_name: Familial HLH type 2 (PRF1 / perforin)
description: >
The most common genetic form of familial HLH, caused by biallelic
pathogenic variants in PRF1 encoding the pore-forming protein perforin.
Perforin deficiency abolishes the lytic activity of cytotoxic granules,
preventing CTL/NK-mediated killing and down-regulation of immune activation.
evidence:
- reference: PMID:10583959
reference_title: Perforin gene defects in familial hemophagocytic lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Sequencing of the coding regions of the perforin gene of eight unrelated 10q21-22-linked FHL patients revealed homozygous nonsense mutations in four patients and missense mutations in the other four patients."
explanation: Establishes biallelic PRF1 (perforin) mutations as the cause of FHL2.
- name: FHL3
display_name: Familial HLH type 3 (UNC13D / Munc13-4)
description: >
Familial HLH caused by biallelic UNC13D mutations encoding Munc13-4, a
vesicle-priming protein required for fusion of cytolytic granules with the
plasma membrane at the immunological synapse.
evidence:
- reference: PMID:14622600
reference_title: Munc13-4 is essential for cytolytic granules fusion and is mutated in a form of familial hemophagocytic lymphohistiocytosis (FHL3).
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "HMunc13-4 deficiency results in defective cytolytic granule exocytosis, despite polarization of the secretory granules and docking with the plasma membrane."
explanation: Establishes UNC13D/Munc13-4 as the FHL3 gene and defines its role in granule priming.
- name: FHL4
display_name: Familial HLH type 4 (STX11 / syntaxin-11)
description: >
Familial HLH caused by biallelic STX11 mutations encoding syntaxin-11, a
SNARE protein of the intracellular membrane-fusion machinery required for
cytotoxic granule exocytosis.
evidence:
- reference: PMID:15703195
reference_title: Linkage of familial hemophagocytic lymphohistiocytosis (FHL) type-4 to chromosome 6q24 and identification of mutations in syntaxin 11.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "we identified a homozygous deletion of 5 bp in the syntaxin 11 gene (STX11) in this family"
explanation: Establishes STX11 (syntaxin-11) mutations as the cause of FHL4.
- name: FHL5
display_name: Familial HLH type 5 (STXBP2 / Munc18-2)
description: >
Familial HLH caused by biallelic STXBP2 mutations encoding Munc18-2
(syntaxin-binding protein 2), which partners with syntaxin-11 at a late step
of cytotoxic granule release. Some heterozygous gain-of-function STXBP2
variants are associated with autosomal dominant disease.
evidence:
- reference: PMID:19884660
reference_title: Munc18-2 deficiency causes familial hemophagocytic lymphohistiocytosis type 5 and impairs cytotoxic granule exocytosis in patient NK cells.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Our work shows that STXBP2 deficiency causes FHL5."
explanation: Establishes STXBP2/Munc18-2 deficiency as the cause of FHL5.
- name: Griscelli Type 2
display_name: Griscelli syndrome type 2 (RAB27A)
description: >
Syndromic HLH-predisposing disorder caused by biallelic RAB27A mutations.
RAB27A is a small GTPase that is a key effector of cytotoxic granule
exocytosis; deficiency causes partial pigmentary dilution plus an
uncontrolled T-cell/macrophage activation (hemophagocytic) syndrome.
evidence:
- reference: PMID:10835631
reference_title: Mutations in RAB27A cause Griscelli syndrome associated with haemophagocytic syndrome.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "all patients with RAB27A mutations, but none with the MYO5A mutation, developed HS"
explanation: Establishes RAB27A as the Griscelli type 2 gene whose deficiency causes the haemophagocytic syndrome.
- name: Chediak-Higashi
display_name: Chediak-Higashi syndrome (LYST)
description: >
Syndromic HLH-predisposing disorder caused by biallelic LYST (CHS1)
mutations, producing giant lysosome-related organelles, partial
oculocutaneous albinism, immunodeficiency, neutropenia, absent NK function,
and risk of an accelerated (hemophagocytic) phase.
evidence:
- reference: PMID:8896560
reference_title: Identification and mutation analysis of the complete gene for Chediak-Higashi syndrome.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Here we describe the sequence of a human cDNA homologous to mouse beige, identify pathologic mutations"
explanation: Reports identification of the LYST/CHS1 gene and its pathogenic mutations in Chediak-Higashi syndrome.
- name: XLP1
display_name: X-linked lymphoproliferative disease type 1 (SH2D1A / SAP)
description: >
X-linked HLH-predisposing immunodeficiency caused by hemizygous SH2D1A
mutations encoding the SLAM-associated protein SAP. Characterized by an
inappropriate, often fatal immune response to Epstein-Barr virus leading to
HLH/fulminant mononucleosis, dysgammaglobulinemia, and lymphoma.
evidence:
- reference: PMID:20301580
reference_title: X-Linked Lymphoproliferative Disease.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "XLP has two recognizable subtypes, XLP1 (due to pathogenic variants in SH2D1A) and XLP2 (due to pathogenic variants in XIAP)."
explanation: Defines XLP1 as caused by SH2D1A (SAP) variants, predisposing to EBV-triggered HLH.
- name: XLP2
display_name: X-linked lymphoproliferative disease type 2 (XIAP / BIRC4)
description: >
X-linked HLH-predisposing immunodeficiency caused by hemizygous XIAP (BIRC4)
mutations. XIAP regulates lymphocyte apoptosis and NKT-cell survival;
deficiency predisposes to recurrent HLH (often without EBV), splenomegaly,
and inflammatory bowel disease.
evidence:
- reference: PMID:17080092
reference_title: XIAP deficiency in humans causes an X-linked lymphoproliferative syndrome.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "we identify mutations in the gene that encodes the X-linked inhibitor-of-apoptosis XIAP (also termed BIRC4) in patients with XLP from three families without mutations in SAP"
explanation: Establishes XIAP/BIRC4 mutations as the cause of XLP2 (X-linked lymphoproliferative syndrome).
pathophysiology:
- name: Impaired Lymphocyte Cytotoxicity
description: >
The unifying lesion in familial HLH is defective perforin/granzyme-mediated
killing by cytotoxic T lymphocytes and NK cells. Loss of perforin (PRF1) or
of the granule docking/priming/fusion machinery (Munc13-4, syntaxin-11,
Munc18-2, RAB27A) prevents target-cell lysis, so infected and
antigen-presenting cells are not eliminated and the immune response cannot be
terminated.
cell_types:
- preferred_term: cytotoxic T cell
term:
id: CL:0000910
label: cytotoxic T cell
- preferred_term: natural killer cell
term:
id: CL:0000623
label: natural killer cell
biological_processes:
- preferred_term: natural killer cell mediated cytotoxicity
term:
id: GO:0042267
label: natural killer cell mediated cytotoxicity
modifier: DECREASED
- preferred_term: T cell mediated cytotoxicity
term:
id: GO:0001913
label: T cell mediated cytotoxicity
modifier: DECREASED
evidence:
- reference: PMID:10583959
reference_title: Perforin gene defects in familial hemophagocytic lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Cultured lymphocytes from patients had defective cytotoxic activity, and immunostaining revealed little or no perforin in the granules."
explanation: Demonstrates that perforin deficiency abolishes lymphocyte cytotoxic activity in FHL.
- reference: PMID:19884660
reference_title: Munc18-2 deficiency causes familial hemophagocytic lymphohistiocytosis type 5 and impairs cytotoxic granule exocytosis in patient NK cells.
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "NK cells exhibited impaired cytotoxic granule exocytosis, a defect that could be overcome by ectopic expression of wild-type STXBP2"
explanation: Shows that the granule-fusion defect (here STXBP2/Munc18-2) impairs NK-cell cytotoxic granule exocytosis.
- name: Defective Cytotoxic Granule Exocytosis
description: >
Downstream of granule polarization and docking, the SNARE/priming machinery
(Munc13-4, syntaxin-11, Munc18-2, RAB27A) is required to fuse perforin- and
granzyme-laden lytic granules with the plasma membrane at the immunological
synapse. Mutations in these genes block the late exocytosis step even when
granules are correctly polarized and docked.
cell_types:
- preferred_term: cytotoxic T cell
term:
id: CL:0000910
label: cytotoxic T cell
- preferred_term: natural killer cell
term:
id: CL:0000623
label: natural killer cell
biological_processes:
- preferred_term: regulated exocytosis of cytolytic granules
term:
id: GO:0045055
label: regulated exocytosis
modifier: DECREASED
evidence:
- reference: PMID:14622600
reference_title: Munc13-4 is essential for cytolytic granules fusion and is mutated in a form of familial hemophagocytic lymphohistiocytosis (FHL3).
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "This process requires the rapid transfer of perforin containing lytic granules to the target cell interface, followed by their docking and fusion with the plasma membrane."
explanation: Defines the regulated cytolytic-granule exocytosis step that is defective in FHL3 (Munc13-4) and related forms.
- reference: PMID:15703195
reference_title: Linkage of familial hemophagocytic lymphohistiocytosis (FHL) type-4 to chromosome 6q24 and identification of mutations in syntaxin 11.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "As both STX11 and UNC13D are involved in vesicle trafficking and membrane fusion, we conclude that, besides mutations in perforin 1, defects in the endocytotic or the exocytotic pathway may be a common mechanism in FHL."
explanation: Establishes defective vesicle trafficking/membrane fusion as a shared FHL mechanism.
- name: Uncontrolled T-cell and Macrophage Activation and Cytokine Storm
description: >
Because cytotoxic lymphocytes cannot kill the antigen-presenting targets that
sustain them, the immune response is never contracted. CTLs and macrophages
remain hyperactivated and proliferate, secreting a storm of inflammatory
cytokines (notably interferon-gamma), which drives macrophage activation,
hemophagocytosis, and multi-organ infiltration and damage (bone marrow,
liver, spleen, brain).
cell_types:
- preferred_term: macrophage
term:
id: CL:0000235
label: macrophage
- preferred_term: cytotoxic T cell
term:
id: CL:0000910
label: cytotoxic T cell
biological_processes:
- preferred_term: macrophage activation
term:
id: GO:0042116
label: macrophage activation
modifier: INCREASED
- preferred_term: type II (interferon-gamma) production
term:
id: GO:0032609
label: type II interferon production
modifier: INCREASED
- preferred_term: cytokine production
term:
id: GO:0001816
label: cytokine production
modifier: INCREASED
evidence:
- reference: PMID:10583959
reference_title: Perforin gene defects in familial hemophagocytic lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Familial hemophagocytic lymphohistiocytosis (FHL) is a rare, rapidly fatal, autosomal recessive immune disorder characterized by uncontrolled activation of T cells and macrophages and overproduction of inflammatory cytokines."
explanation: Characterizes the uncontrolled T-cell/macrophage activation and cytokine overproduction that define HLH.
- reference: PMID:20301617
reference_title: Familial Hemophagocytic Lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "an immune deficiency characterized by the overactivation and excessive proliferation of T lymphocytes and macrophages, leading to infiltration and damage of organs including the bone marrow, liver, spleen, and brain"
explanation: GeneReviews characterizes the overactivation/proliferation of T lymphocytes and macrophages with multi-organ infiltration.
phenotypes:
- name: Fever
category: Clinical
description: Prolonged high fever is a cardinal presenting feature of active HLH.
phenotype_term:
preferred_term: Fever
term:
id: HP:0001945
label: Fever
evidence:
- reference: PMID:20301617
reference_title: Familial Hemophagocytic Lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Familial HLH usually presents as an acute illness with prolonged and high fever, cytopenias, and hepatosplenomegaly."
explanation: GeneReviews lists prolonged high fever as a usual presenting feature of familial HLH.
- name: Hepatosplenomegaly
category: Clinical
description: Enlargement of the liver and spleen due to infiltration by activated lymphocytes and histiocytes.
phenotype_term:
preferred_term: Hepatosplenomegaly
term:
id: HP:0001433
label: Hepatosplenomegaly
evidence:
- reference: PMID:20301617
reference_title: Familial Hemophagocytic Lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Familial HLH usually presents as an acute illness with prolonged and high fever, cytopenias, and hepatosplenomegaly."
explanation: GeneReviews lists hepatosplenomegaly as a usual presenting feature.
- name: Cytopenias
category: Laboratory
description: >
Bi- or trilineage peripheral cytopenias (anemia, thrombocytopenia, and/or
neutropenia) result from marrow infiltration and hemophagocytosis.
phenotype_term:
preferred_term: Pancytopenia
term:
id: HP:0001876
label: Pancytopenia
evidence:
- reference: PMID:20301617
reference_title: Familial Hemophagocytic Lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Familial HLH usually presents as an acute illness with prolonged and high fever, cytopenias, and hepatosplenomegaly."
explanation: GeneReviews lists cytopenias as a usual presenting feature of familial HLH.
- name: Hemophagocytosis
category: Histopathology
description: >
Activated macrophages/histiocytes engulf erythrocytes, leukocytes, and
platelets in the bone marrow, spleen, liver, and lymph nodes - the
pathognomonic histologic feature of HLH.
phenotype_term:
preferred_term: Hemophagocytosis
term:
id: HP:0012156
label: Hemophagocytosis
evidence:
- reference: PMID:10835631
reference_title: Mutations in RAB27A cause Griscelli syndrome associated with haemophagocytic syndrome.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Most patients also develop an uncontrolled T-lymphocyte and macrophage activation syndrome (known as haemophagocytic syndrome, HS), leading to death in the absence of bone-marrow transplantation."
explanation: Describes the macrophage activation / haemophagocytic syndrome characteristic of HLH.
- name: Hyperferritinemia
category: Laboratory
description: >
Markedly elevated serum ferritin reflects intense macrophage activation and
is a key diagnostic criterion for HLH.
phenotype_term:
preferred_term: Hyperferritinemia
term:
id: HP:0003281
label: Increased circulating ferritin concentration
evidence:
- reference: PMID:16937360
reference_title: "HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "three additional criteria are introduced; low/absent NK-cell-activity, hyperferritinemia, and high-soluble interleukin-2-receptor levels."
explanation: The HLH-2004 guidelines list hyperferritinemia among the diagnostic criteria for HLH.
- name: Hypertriglyceridemia
category: Laboratory
description: Elevated fasting triglycerides, a diagnostic criterion of HLH.
phenotype_term:
preferred_term: Hypertriglyceridemia
term:
id: HP:0002155
label: Hypertriglyceridemia
evidence:
- reference: PMID:16937360
reference_title: "HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "diagnosis was based on five criteria (fever, splenomegaly, bicytopenia, hypertriglyceridemia and/or hypofibrinogenemia, and hemophagocytosis)"
explanation: The HLH diagnostic criteria include hypertriglyceridemia.
- name: Hypofibrinogenemia
category: Laboratory
description: Low fibrinogen reflecting coagulopathy and a diagnostic criterion of HLH.
phenotype_term:
preferred_term: Hypofibrinogenemia
term:
id: HP:0011900
label: Hypofibrinogenemia
evidence:
- reference: PMID:16937360
reference_title: "HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "diagnosis was based on five criteria (fever, splenomegaly, bicytopenia, hypertriglyceridemia and/or hypofibrinogenemia, and hemophagocytosis)"
explanation: The HLH diagnostic criteria include hypofibrinogenemia.
- name: Neurologic Involvement
category: Clinical
description: >
CNS involvement (encephalopathy, seizures, irritability) and elevated CSF
cells/protein occur frequently and contribute to morbidity and late effects.
phenotype_term:
preferred_term: Encephalopathy
term:
id: HP:0001298
label: Encephalopathy
evidence:
- reference: PMID:20301617
reference_title: Familial Hemophagocytic Lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Individuals with fHLH may also exhibit liver dysfunction and neurologic abnormalities."
explanation: GeneReviews documents neurologic abnormalities in familial HLH.
- name: Liver Dysfunction
category: Laboratory
description: Hepatitis with elevated transaminases; can progress to liver failure.
phenotype_term:
preferred_term: Elevated hepatic transaminases
term:
id: HP:0002910
label: Elevated circulating hepatic transaminase concentration
evidence:
- reference: PMID:20301617
reference_title: Familial Hemophagocytic Lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Individuals with fHLH may also exhibit liver dysfunction and neurologic abnormalities."
explanation: GeneReviews documents liver dysfunction in familial HLH.
genetic:
- name: PRF1
subtype: FHL2
association: Causative
features: >
Biallelic PRF1 pathogenic variants (perforin) cause FHL2, the most common
genetic form, abolishing the lytic activity of cytotoxic granules.
Inherited in an autosomal recessive manner.
gene_term:
preferred_term: PRF1
term:
id: hgnc:9360
label: PRF1
evidence:
- reference: PMID:10583959
reference_title: Perforin gene defects in familial hemophagocytic lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Thus, defects in perforin are responsible for 10q21-22-linked FHL."
explanation: Establishes PRF1/perforin defects as causal for FHL.
- name: UNC13D
subtype: FHL3
association: Causative
features: >
Biallelic UNC13D (Munc13-4) variants cause FHL3 via defective granule
priming. Inherited in an autosomal recessive manner.
gene_term:
preferred_term: UNC13D
term:
id: hgnc:23147
label: UNC13D
evidence:
- reference: PMID:14622600
reference_title: Munc13-4 is essential for cytolytic granules fusion and is mutated in a form of familial hemophagocytic lymphohistiocytosis (FHL3).
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "HMunc13-4 mutations were shown to cause FHL3."
explanation: Establishes UNC13D/Munc13-4 mutations as causal for FHL3.
- name: STX11
subtype: FHL4
association: Causative
features: >
Biallelic STX11 (syntaxin-11) variants cause FHL4 via defective
SNARE-mediated granule fusion. Inherited in an autosomal recessive manner.
gene_term:
preferred_term: STX11
term:
id: hgnc:11429
label: STX11
evidence:
- reference: PMID:15703195
reference_title: Linkage of familial hemophagocytic lymphohistiocytosis (FHL) type-4 to chromosome 6q24 and identification of mutations in syntaxin 11.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "we found homozygous mutations in STX11 in five consanguineous Turkish/Kurdish FHL kindreds"
explanation: Establishes biallelic STX11 mutations as causal for FHL4.
- name: STXBP2
subtype: FHL5
association: Causative
features: >
Biallelic STXBP2 (Munc18-2) variants cause FHL5; rare heterozygous
gain-of-function variants are associated with autosomal dominant disease.
Predominantly autosomal recessive inheritance.
gene_term:
preferred_term: STXBP2
term:
id: hgnc:11445
label: STXBP2
evidence:
- reference: PMID:19884660
reference_title: Munc18-2 deficiency causes familial hemophagocytic lymphohistiocytosis type 5 and impairs cytotoxic granule exocytosis in patient NK cells.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "the gene encoding syntaxin-binding protein 2 (Munc18-2; official gene symbol STXBP2) is mutated in another subset of patients with FHL (designated by us as \"FHL5\")"
explanation: Establishes STXBP2/Munc18-2 mutations as causal for FHL5.
- name: RAB27A
subtype: Griscelli Type 2
association: Causative
features: >
Biallelic RAB27A variants cause Griscelli syndrome type 2, a key effector
of cytotoxic granule exocytosis whose loss predisposes to HLH. Inherited in
an autosomal recessive manner.
gene_term:
preferred_term: RAB27A
term:
id: hgnc:9766
label: RAB27A
evidence:
- reference: PMID:10835631
reference_title: Mutations in RAB27A cause Griscelli syndrome associated with haemophagocytic syndrome.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "We detected mutations in RAB27A, which lies within this interval, in 16 patients with GS."
explanation: Establishes RAB27A mutations as causal for Griscelli syndrome type 2.
- name: LYST
subtype: Chediak-Higashi
association: Causative
features: >
Biallelic LYST (CHS1) variants cause Chediak-Higashi syndrome, with giant
granules, immunodeficiency, and risk of an accelerated hemophagocytic phase.
Inherited in an autosomal recessive manner.
gene_term:
preferred_term: LYST
term:
id: hgnc:1968
label: LYST
evidence:
- reference: PMID:8896560
reference_title: Identification and mutation analysis of the complete gene for Chediak-Higashi syndrome.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "identify pathologic mutations and clarify the discrepancies of the previous reports"
explanation: Reports identification of pathologic LYST/CHS1 mutations in Chediak-Higashi syndrome.
- name: SH2D1A
subtype: XLP1
association: Causative
features: >
Hemizygous SH2D1A (SAP) variants cause XLP1, predisposing to EBV-triggered
HLH, dysgammaglobulinemia, and lymphoma. X-linked recessive inheritance.
gene_term:
preferred_term: SH2D1A
term:
id: hgnc:10820
label: SH2D1A
evidence:
- reference: PMID:20301580
reference_title: X-Linked Lymphoproliferative Disease.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "XLP has two recognizable subtypes, XLP1 (due to pathogenic variants in SH2D1A) and XLP2 (due to pathogenic variants in XIAP)."
explanation: Establishes SH2D1A (SAP) as the XLP1 gene.
- name: XIAP
subtype: XLP2
association: Causative
features: >
Hemizygous XIAP (BIRC4) variants cause XLP2, predisposing to recurrent HLH
(often without EBV), splenomegaly, and inflammatory bowel disease. X-linked
recessive inheritance.
gene_term:
preferred_term: XIAP
term:
id: hgnc:592
label: XIAP
evidence:
- reference: PMID:17080092
reference_title: XIAP deficiency in humans causes an X-linked lymphoproliferative syndrome.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "by identifying an XLP immunodeficiency that is caused by mutations in XIAP, we show that XIAP is a potent regulator of lymphocyte homeostasis in vivo"
explanation: Establishes XIAP/BIRC4 as the XLP2 gene regulating lymphocyte homeostasis.
treatments:
- name: HLH-94 / HLH-2004 Chemoimmunotherapy (Etoposide + Dexamethasone)
description: >
First-line induction for active HLH combining etoposide and dexamethasone
(with intrathecal therapy for CNS disease, plus ciclosporin in HLH-94),
aiming at clinical remission as a bridge to allogeneic HSCT in familial,
persistent, or recurrent disease.
treatment_term:
preferred_term: chemotherapy
term:
id: MAXO:0000647
label: chemotherapy
therapeutic_agent:
- preferred_term: etoposide
term:
id: CHEBI:4911
label: etoposide
- preferred_term: dexamethasone
term:
id: CHEBI:41879
label: dexamethasone
- preferred_term: cyclosporin A
term:
id: CHEBI:4031
label: cyclosporin A
evidence:
- reference: PMID:21900192
reference_title: 'Chemoimmunotherapy for hemophagocytic lymphohistiocytosis: long-term results of the HLH-94 treatment protocol.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "To conclude, HLH-94 chemoimmunotherapy has considerably improved outcome in HLH."
explanation: The HLH-94 etoposide-based chemoimmunotherapy protocol improved survival in the largest prospective HLH study.
- name: Emapalumab (Anti-Interferon-gamma Antibody)
description: >
Human anti-interferon-gamma monoclonal antibody, FDA-approved with
dexamethasone for relapsed/refractory or intolerant primary HLH, neutralizing
the central IFN-gamma-driven cytokine storm.
therapeutic_modality: MONOCLONAL_ANTIBODY
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: emapalumab
term:
id: NCIT:C127123
label: Emapalumab
evidence:
- reference: PMID:32374962
reference_title: Emapalumab in Children with Primary Hemophagocytic Lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "We investigated the efficacy and safety of emapalumab (a human anti-interferon-γ antibody), administered with dexamethasone"
explanation: Phase 2-3 trial of emapalumab plus dexamethasone in primary HLH, supporting anti-IFN-gamma therapy.
- name: Allogeneic Hematopoietic Stem Cell Transplantation
description: >
Allogeneic HSCT is the only curative therapy for familial HLH and is
indicated after remission induction in familial, persistent, or recurrent
disease; patients with familial disease do not survive without it.
treatment_term:
preferred_term: hematopoietic stem cell transplantation
term:
id: MAXO:0000747
label: hematopoietic stem cell transplantation
evidence:
- reference: PMID:21900192
reference_title: 'Chemoimmunotherapy for hemophagocytic lymphohistiocytosis: long-term results of the HLH-94 treatment protocol.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Patients with familial disease had a 5-year survival of 50% ± 13%; none survived without HSCT."
explanation: Demonstrates that allogeneic HSCT is required for survival in familial HLH.
- reference: PMID:20301617
reference_title: Familial Hemophagocytic Lymphohistiocytosis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Treatment regimens focus on use of chemoimmunotherapy to treat active disease followed by allogeneic HSCT, the only curative therapy."
explanation: GeneReviews identifies allogeneic HSCT as the only curative therapy for familial HLH.
notes: >
Familial HLH is inherited in an autosomal recessive manner (except the
X-linked syndromic forms XLP1/XLP2 and rare autosomal dominant
gain-of-function STXBP2 variants). GeneReviews "Agents/circumstances to avoid"
for fHLH include live vaccines, exposure to infections, acetaminophen in
persons with liver failure, NSAIDs in persons with thrombocytopenia, and
transfusion of non-irradiated blood products in individuals undergoing
chemoimmunotherapy or allogeneic HSCT. Secondary/acquired HLH (triggered by
infection, malignancy, or rheumatologic disease / macrophage activation
syndrome) shares the same final common pathway but is modeled separately from
this hereditary entry.
References & Deep Research
References
3Deep Research
11. Disease Information
1.1 Overview (what is HLH?)
HLH is a life‑threatening hyperinflammatory syndrome characterized by ineffective termination of an immune response and uncontrolled activation of immune effector cells, resulting in systemic inflammation, tissue infiltration, and multi‑organ injury. Multiple recent reviews describe HLH as severe “dysregulated inflammation” driven by immune activation in response to a provoking trigger (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2).
Direct abstract‑quotable definitions: - HLH is “a life‑threatening syndrome of excessive, dysregulated inflammation in response to a provoking trigger.” (Lee & Logan, Cancers, 2023‑03; https://doi.org/10.3390/cancers15061839) (lee2023diagnosisandmanagement pages 1-3) - HLH is “a hyperinflammatory process that develops in patients with genetic abnormalities, hematologic malignancies, chronic inflammatory states, or infections.” (Zoref‑Lorenz et al., ASH Education Program, 2023‑12; https://doi.org/10.1182/hematology.2023000509) (zoreflorenz2023inpatientrecognitionand pages 1-2)
1.2 Classification (primary vs secondary)
Current clinical framing separates: - Primary (familial/genetic) HLH: due to congenital defects (typically in cytotoxic lymphocyte granule exocytosis/killing pathways), often presenting in infancy/early childhood. (lee2023diagnosisandmanagement pages 1-3, wimmer2024outcomeofadult pages 9-15) - Secondary (acquired) HLH: HLH syndrome arising in the context of triggers such as infection, malignancy, rheumatologic disease (macrophage activation syndrome, MAS), or iatrogenic immune perturbation. (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2)
1.3 Synonyms and alternative names
Commonly used near‑synonyms/related terms in recent sources include: - Hemophagocytic syndrome (used interchangeably in some clinical contexts) (zoreflorenz2023inpatientrecognitionand pages 1-2) - Macrophage activation syndrome (MAS) (a form of secondary HLH often in rheumatologic contexts) (lee2023diagnosisandmanagement pages 1-3) - Immune effector cell–associated HLH‑like syndrome (HLH‑like toxicities after CAR‑T therapy; overlaps with CRS) (concept referenced via HLH‑like toxicities) (zoreflorenz2023inpatientrecognitionand pages 1-2)
1.4 Disease identifiers (ontology/coding)
- MONDO / Orphanet / OMIM / ICD‑10/ICD‑11 / MeSH: not retrieved in this run; must be curated from the authoritative databases.
1.5 Evidence source types
The information summarized here is derived from: - Aggregated literature resources (reviews, consensus guideline) (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2, cox2024diagnosisandinvestigation pages 10-15) - Retrospective cohort/dissertation evidence for frequencies (adult HLH cohort) (wimmer2024outcomeofadult pages 55-56) - Scoping/systematic reviews for trigger‑specific epidemiology/outcomes (e.g., tick‑borne disease HLH; TB‑HLH) (jevtic2024hemophagocyticlymphohistiocytosis(hlh) pages 1-2) - Clinical trial registries (NCT entries) (NCT03312751 chunk 1, NCT03985423 chunk 1)
2. Etiology
2.1 Disease causal factors
Primary HLH (genetic causes)
Primary HLH is caused by inherited defects in lymphocyte cytotoxic machinery. Recent and supporting sources emphasize that congenital “defects in cytolytic pathway proteins” define primary HLH (pHLH) (lee2023diagnosisandmanagement pages 1-3), often involving granule exocytosis/killing genes (babolpokora2021moleculargeneticsdiversity pages 1-2, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2).
Secondary HLH (triggered hyperinflammation)
Secondary HLH is typically driven by a highly immunogenic trigger rather than a single monogenic cytotoxicity defect in adults (lee2023diagnosisandmanagement pages 1-3). Triggers include: - Infections: especially herpesviruses such as EBV, CMV, HSV, HIV (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2) - Malignancy: a major adult category, notably lymphomas (lee2023diagnosisandmanagement pages 1-3) - Rheumatologic/chronic inflammatory disease: MAS (lee2023diagnosisandmanagement pages 1-3) - Iatrogenic/drug‑related: CAR‑T, immune checkpoint blockade (ICB/ICI) (zoreflorenz2023inpatientrecognitionand pages 1-2)
2.2 Risk factors
Genetic risk factors
Even in clinically “secondary” HLH, genetic predisposition can be present. A cited retrospective Italian study reported monoallelic mutations in FHL‑related genes in 43/240 (18%) secondary HLH cases (wimmer2024outcomeofadult pages 19-23), suggesting partial cytotoxic pathway impairment may act as a susceptibility factor.
Environmental/infectious risk factors
- EBV is repeatedly highlighted as a leading infectious association in adults (papazachariou2024hemophagocyticlymphohistiocytosistriggered pages 1-2, lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2) and a common trigger in pediatric secondary HLH in a Polish cohort (23/35; 65%) (babolpokora2021moleculargeneticsdiversity pages 1-2).
- Trigger‑specific reviews provide examples of infectious risk contexts:
- Tick‑borne illnesses: Ehrlichia spp. 45.9% of 98 tick‑borne HLH cases (jevtic2024hemophagocyticlymphohistiocytosis(hlh) pages 1-2)
- Tuberculosis‑associated HLH: systematic review with 39% mortality (lee2023diagnosisandmanagement pages 1-3)
2.3 Protective factors
No explicit genetic or environmental protective factors were identified in the retrieved evidence.
2.4 Gene–environment interactions
Evidence in this run supports a model where partial genetic impairment of cytotoxic pathways interacts with strong immune triggers (e.g., viral infections, malignancy) to precipitate HLH. This is consistent with the observed monoallelic FHL‑gene findings in secondary HLH (wimmer2024outcomeofadult pages 19-23) and the conceptual framing that adult HLH is often trigger‑driven (lee2023diagnosisandmanagement pages 1-3).
3. Phenotypes
3.1 Core phenotype spectrum (symptoms/signs/lab abnormalities)
Across recent reviews, common HLH features include fever, hepatosplenomegaly, cytopenias, hypertriglyceridemia, hypofibrinogenemia, elevated liver enzymes, hyperferritinemia, and elevated soluble CD25 (sCD25) (zoreflorenz2023inpatientrecognitionand pages 1-2, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2).
Direct quotable statement (phenotype set): HLH patients may present with “fever, central nervous system symptoms, cytopenias, or elevated liver enzymes” (zoreflorenz2023inpatientrecognitionand pages 1-2).
3.2 Frequencies from an adult cohort (real‑world phenotype distribution)
In a 62‑patient adult HLH cohort, high‑frequency findings included: - Ferritin ≥2000 µg/L: 97% (60/62) (wimmer2024outcomeofadult pages 55-56) - Temperature ≥38.4°C: 93% (56/60) (wimmer2024outcomeofadult pages 55-56) - Splenomegaly: 90% (54/60) (wimmer2024outcomeofadult pages 55-56) - AST ≥30 U/L: 90% (56/62) (wimmer2024outcomeofadult pages 55-56) - Triglycerides ≥132.7 mg/dL: 90% (55/61) (wimmer2024outcomeofadult pages 55-56) - sCD25 ≥2400 U/mL: 88% (53/60) (wimmer2024outcomeofadult pages 55-56) - Hemophagocytosis on pathology: 58% (33/57) (wimmer2024outcomeofadult pages 55-56) - Hepatomegaly: 62% (38/61) (wimmer2024outcomeofadult pages 55-56)
3.3 Age of onset and course
- Primary/familial HLH “usually manifests itself within the first two years of life” in classic descriptions (wimmer2024outcomeofadult pages 9-15).
- Secondary HLH is “the predominant form in older children and adults” (wimmer2024outcomeofadult pages 9-15).
3.4 Quality of life impact
No disease‑specific QOL instruments or quantitative QOL results were captured in the retrieved sources.
3.5 Suggested HPO terms (examples)
(Recommended for KB normalization; frequencies where available above) - Fever HP:0001945 - Splenomegaly HP:0001744 - Hepatomegaly HP:0002240 - Cytopenia HP:0001873 (and lineage‑specific terms) - Hyperferritinemia HP:0003281 - Hypertriglyceridemia HP:0002155 - Hypofibrinogenemia HP:0004348 - Elevated hepatic transaminases HP:0002910 - Encephalopathy / seizures (CNS involvement noted qualitatively) HP:0001298 / HP:0001250 (zoreflorenz2023inpatientrecognitionand pages 1-2, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2)
4. Genetic/Molecular Information
4.1 Causal genes (core familial HLH)
Core familial HLH genes emphasized across sources include PRF1, UNC13D, STX11, STXBP2 (babolpokora2021moleculargeneticsdiversity pages 1-2, gadourylevesque2020frequencyandspectrum pages 1-2, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2).
A structured gene summary is provided in Artifact 01.
| Clinical entity/subtype | Gene (HGNC symbol) | Protein/function (cytotoxic granule pathway step or inflammasome) | Inheritance | Notes | Key evidence citation id |
|---|---|---|---|---|---|
| Familial HLH type 2 (FHL2) | PRF1 | Perforin; pore-forming effector required for granzyme entry and lymphocyte cytotoxic killing | Autosomal recessive | Core familial HLH gene; central to granule-mediated cytotoxicity | (babolpokora2021moleculargeneticsdiversity pages 1-2, wimmer2024outcomeofadult pages 19-23) |
| Familial HLH type 3 (FHL3) | UNC13D | Munc13-4; cytotoxic granule priming/exocytosis | Autosomal recessive | Common FHL cause; associated with poor prognosis in later cohort literature | (babolpokora2021moleculargeneticsdiversity pages 1-2, simon2025anationwideanalysis pages 2-4) |
| Familial HLH type 4 (FHL4) | STX11 | Syntaxin-11; vesicle membrane fusion/exocytosis in cytotoxic granule release | Autosomal recessive | Canonical degranulation-pathway FHL gene | (babolpokora2021moleculargeneticsdiversity pages 1-2, almansi2024hemophagocyticlymphohistiocytosisan pages 2-4) |
| Familial HLH type 5 (FHL5) | STXBP2 | Munc18-2; vesicle docking/fusion for cytotoxic granule exocytosis | Autosomal recessive | Also referred to as UNC18B/Munc18-2 in some sources | (babolpokora2021moleculargeneticsdiversity pages 1-2, almansi2024hemophagocyticlymphohistiocytosisan pages 2-4) |
| Griscelli syndrome type 2 with HLH predisposition | RAB27A | Regulates cytotoxic granule trafficking/transport | Autosomal recessive | Syndromic HLH predisposition; defective granule transport | (babolpokora2021moleculargeneticsdiversity pages 1-2, gadourylevesque2020frequencyandspectrum pages 1-2) |
| Chediak-Higashi syndrome with HLH predisposition | LYST | Required for cytotoxic granule formation/lysosome-related organelle biology | Autosomal recessive | Syndromic HLH predisposition; abnormal granule formation/trafficking | (babolpokora2021moleculargeneticsdiversity pages 1-2, gadourylevesque2020frequencyandspectrum pages 1-2) |
| Hermansky-Pudlak syndrome type 2 with HLH predisposition | AP3B1 | Adaptor protein complex component; granule biogenesis/transport | Autosomal recessive | Syndromic HLH predisposition due to granule formation/transport defects | (babolpokora2021moleculargeneticsdiversity pages 1-2, gadourylevesque2020frequencyandspectrum pages 1-2) |
| X-linked lymphoproliferative syndrome 1 (XLP1) | SH2D1A | SAP signaling adaptor; immune regulation with EBV susceptibility rather than classic granule-fusion defect | X-linked | X-linked HLH predisposition, often EBV-triggered | (babolpokora2021moleculargeneticsdiversity pages 1-2, wimmer2024outcomeofadult pages 19-23) |
| X-linked lymphoproliferative syndrome 2 (XLP2) | XIAP (BIRC4) | XIAP; inflammasome regulation/inhibition and immune homeostasis | X-linked | HLH predisposition with inflammasome-related mechanism distinct from classic degranulation genes | (babolpokora2021moleculargeneticsdiversity pages 1-2, wimmer2024outcomeofadult pages 19-23) |
| X-linked immunodeficiency with magnesium defect, EBV infection, and neoplasia | MAGT1 | Magnesium transporter/immune signaling regulator | X-linked | Reported among HLH-related immune dysregulation syndromes | (babolpokora2021moleculargeneticsdiversity pages 1-2) |
| HLH-predisposition / immune dysregulation | NLRC4 | Inflammasome component | Not clearly stated in retrieved evidence | Non-granule-related predisposition highlighted in diagnostic review | (chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2) |
| HLH-predisposition / immune dysregulation | CDC42 | Rho-family GTPase; immune cell trafficking/signaling, linked to inflammasome-associated HLH phenotypes | Not clearly stated in retrieved evidence | Non-granule-related predisposition highlighted in review/overview sources | (almansi2024hemophagocyticlymphohistiocytosisan pages 2-4, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2) |
| HLH-predisposition / interferon dysregulation | ZNFX1 | Regulator of interferon responses / nucleic-acid sensing | Not clearly stated in retrieved evidence | Recently described HLH-related gene with variable penetrance | (simon2025anationwideanalysis pages 2-4) |
| HLH-predisposition / EBV-associated immune dysregulation | ITK | T-cell signaling kinase | Not clearly stated in retrieved evidence | Mentioned among additional HLH-associated genes beyond classic FHL genes | (gadourylevesque2020frequencyandspectrum pages 1-2, simon2025anationwideanalysis pages 2-4) |
| HLH-predisposition / EBV-associated immune dysregulation | CD27 | TNF-receptor family costimulatory molecule in lymphocyte activation | Not clearly stated in retrieved evidence | Additional HLH-associated immune dysregulation gene | (gadourylevesque2020frequencyandspectrum pages 1-2, simon2025anationwideanalysis pages 2-4) |
Table: This table summarizes HLH genetic causes and related syndromes mentioned in the retrieved evidence, emphasizing the affected gene, pathway role, inheritance, and clinical associations. It is useful for distinguishing classic familial HLH degranulation defects from syndromic and inflammasome-related HLH predisposition genes.
4.2 Pathogenic variants (types, consequences)
The retrieved evidence emphasizes loss‑of‑function disruption of cytotoxic granule assembly/trafficking/exocytosis. A 2020 disease‑specific variant repository (FHLdb) (outside the 2023–2024 priority window but useful for variant-class distribution) reported variant classes in familial HLH genes (PRF1, UNC13D, STXBP2, STX11), including missense, frameshift, nonsense, splicing, in‑frame indels, deep intronic, and large rearrangements, and explicitly notes ACMG classification categories (lee2023diagnosisandmanagement pages 1-3).
4.3 Modifier genes / digenic inheritance
This run retrieved a dedicated review on digenic inheritance in HLH (Steen et al., 2021) but evidence text was not included in gatherable snippets; thus, digenic inheritance is noted as a concept but not expanded with quoted evidence here.
4.4 Epigenetic information
No HLH‑specific epigenetic mechanisms were captured in the retrieved evidence.
4.5 Chromosomal abnormalities
Not captured in the retrieved evidence.
5. Environmental Information
5.1 Infectious agents
Infections are a major trigger category: - Viral triggers frequently include EBV, CMV, VZV, HSV, HIV, and COVID‑19 (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2). - In a 2024 etiologic stratification study, cited adult proportions included herpesviruses accounting for 62% of viral HLH, with 43% EBV and 9% CMV (wu2024etiologicalstratificationand pages 1-2).
5.2 Environmental/lifestyle factors
No specific toxin, lifestyle, or occupational exposures were identified in the retrieved evidence.
6. Mechanism / Pathophysiology
6.1 Causal chain (trigger to clinical manifestations)
A consensus mechanistic chain from recent sources is: 1) Trigger (infection/malignancy/inflammation/iatrogenic immune activation) 2) Failure of cytotoxic control (due to inherited cytotoxic defects or functional exhaustion/overload) → inability to clear antigenic targets and terminate immune activation (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2) 3) Persistent activation/expansion of CD8+ T cells and NK cells with excessive cytokine production (lee2023diagnosisandmanagement pages 1-3) 4) IFN‑γ acts as a key driver, activating macrophages leading to hemophagocytosis and tissue infiltration (zoreflorenz2023inpatientrecognitionand pages 1-2) 5) Self‑amplifying inflammation (“cytokine storm”) → cytopenias, hepatic injury, coagulopathy, CNS dysfunction, multi‑organ failure (wimmer2024outcomeofadult pages 19-23, sousa2024prognosticimpactof pages 5-7)
Direct quotable mechanistic statement: IFN‑γ is described as “the main driver of the disease phenotype” in HLH and “activates macrophages associated with hemophagocytosis and tissue infiltration and damage.” (zoreflorenz2023inpatientrecognitionand pages 1-2)
6.2 Key cell types (suggested CL terms)
- Cytotoxic T cell (CD8+): CL:0000625 (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2)
- Natural killer cell: CL:0000623 (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2)
- Macrophage: CL:0000235 (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2)
6.3 Molecular pathways / processes (suggested GO terms)
- Cytolysis / granzyme‑mediated apoptosis: GO:0019835 / GO:0097194 (supported conceptually by perforin/granzyme pathway emphasis) (wimmer2024outcomeofadult pages 19-23)
- Exocytosis / secretory granule exocytosis: GO:0006887 / GO:0031629 (babolpokora2021moleculargeneticsdiversity pages 1-2, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2)
- Interferon‑gamma–mediated signaling pathway: GO:0060333 (zoreflorenz2023inpatientrecognitionand pages 1-2)
- Inflammatory response / cytokine‑mediated signaling: GO:0006954 / GO:0019221 (lee2023diagnosisandmanagement pages 1-3)
6.4 Molecular profiling and biomarkers (selected recent evidence)
- Ferritin and sCD25 are widely used screening/monitoring biomarkers in adult diagnostic workflow (cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation pages 39-46).
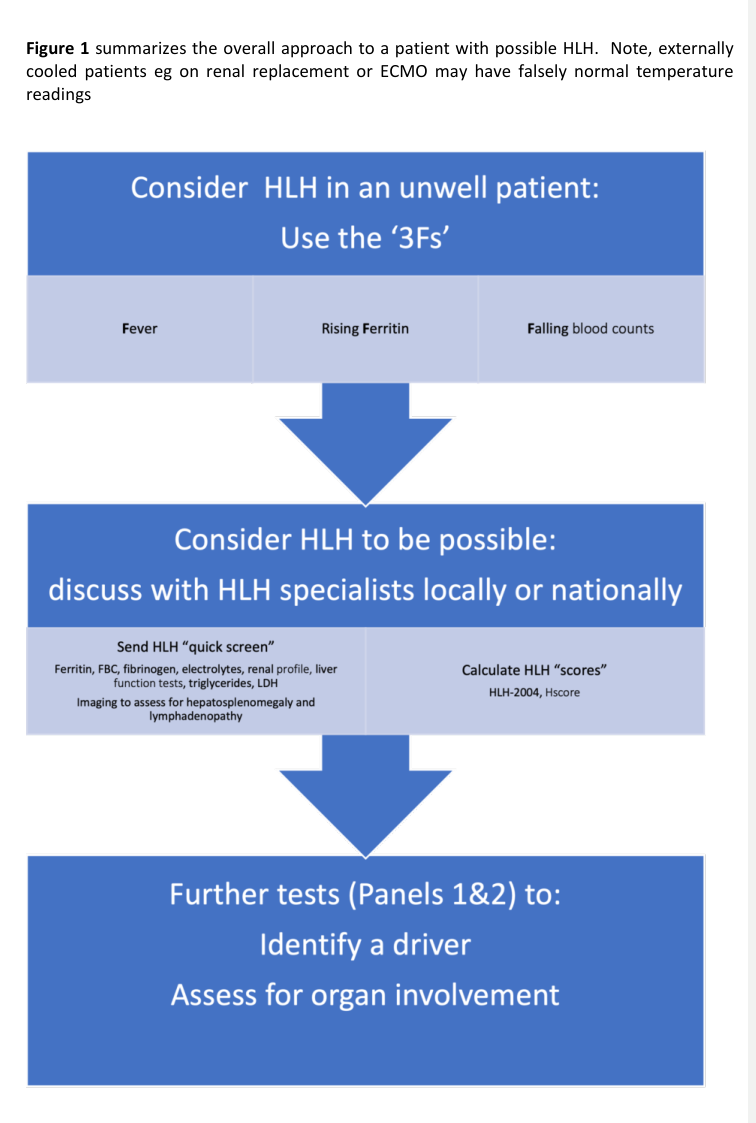
- The HiHASC guideline emphasizes “3Fs” screening: fever, falling blood counts, raised ferritin (cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation media 50579ca6).
6.5 Model organisms and translational mechanisms
While not extensively detailed in retrieved snippets, multiple sources reference classic cytotoxicity‑defect models (e.g., perforin deficiency) as the basis for IFN‑γ‑centric mechanistic understanding (wimmer2024outcomeofadult pages 19-23, zoreflorenz2023inpatientrecognitionand pages 1-2).
7. Anatomical Structures Affected
7.1 Organ level (UBERON suggestions)
Commonly affected organs and systems: - Spleen (splenomegaly): UBERON:0002106 (wimmer2024outcomeofadult pages 55-56) - Liver (hepatomegaly, transaminitis): UBERON:0002107 (wimmer2024outcomeofadult pages 55-56, zoreflorenz2023inpatientrecognitionand pages 1-2) - Bone marrow (hemophagocytosis, cytopenias): UBERON:0002371 (wimmer2024outcomeofadult pages 55-56) - Central nervous system involvement: UBERON:0001016 (qualitative CNS symptoms and diagnostic criteria) (zoreflorenz2023inpatientrecognitionand pages 1-2, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2)
7.2 Tissue/cell level
Reticuloendothelial system involvement with activated macrophages and infiltrating lymphocytes is emphasized (zoreflorenz2023inpatientrecognitionand pages 1-2, wimmer2024outcomeofadult pages 19-23).
7.3 Subcellular level
Not explicitly extracted in this run; implied involvement includes cytotoxic granules/secretory lysosome biology in NK/CD8 cells (babolpokora2021moleculargeneticsdiversity pages 1-2, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2).
8. Temporal Development
8.1 Onset pattern
HLH can have acute/subacute presentations with rapid progression; the adult inpatient review highlights the need for timely investigations and balancing workup with rapid treatment decisions (zoreflorenz2023inpatientrecognitionand pages 1-2).
8.2 Progression/course
Untreated or refractory disease may progress to “cytokine storm causing multi-organ failure and eventually death” (wimmer2024outcomeofadult pages 19-23).
9. Inheritance and Population
9.1 Epidemiology (selected quantitative findings)
Epidemiology varies by setting and trigger. Examples of quantitative disease burden in retrieved sources: - Country prevalence estimates: Japan 1:800,000, China 1.04:1,000,000, England 1–2:1,000,000 (Papazachariou & Ioannou 2024) (papazachariou2024hemophagocyticlymphohistiocytosistriggered pages 1-2). - Adult etiology distribution: In North America and Europe, “around 50% of adult HLH is due to an underlying malignancy” (lee2023diagnosisandmanagement pages 1-3).
A structured summary table is provided below.
| Evidence type (review/cohort/etc) | Population | Key statistics (with numbers) | Triggers/notes | Source (include DOI URL + year) | Context citation id |
|---|---|---|---|---|---|
| Narrative review | General HLH; prevalence estimates from multiple countries | Prevalence estimates reported as Japan 1:800,000, China 1.04:1,000,000, England 1–2:1,000,000; overall mortality ~40% | Secondary HLH commonly triggered by infections, autoimmune/rheumatologic disease, malignancy, or immunosuppression; EBV most frequently implicated in adults | Papazachariou & Ioannou, 2024, DOI: https://doi.org/10.3390/hematolrep16030047 | (papazachariou2024hemophagocyticlymphohistiocytosistriggered pages 1-2) |
| Review | Adults with secondary HLH, especially malignancy-associated HLH | In North America/Europe, ~50% of adult HLH is associated with underlying malignancy; malignancy-associated HLH has <20% 1-year survival and median survival ~2 months | Adult HLH triggers include malignancy, rheumatologic disease/MAS, chronic viral infections (EBV, CMV, VZV, HSV, HIV), and treatment-related causes such as HCT or CAR-T | Lee & Logan, 2023, DOI: https://doi.org/10.3390/cancers15061839 | (lee2023diagnosisandmanagement pages 1-3) |
| ICU/case-based review | Adult HLH, especially ICU presentations | Acute mortality across all combined groups ~40%; malignancy-associated HLH acute mortality >80%; 5-year survival <15%; ICU hospital mortality 52–68%; ferritin >4,000 µg/L increases likelihood and >10,000 µg/L is highly concerning | In adults, underlying malignancy in nearly 50% of cases; lymphomas/leukemia involved in 20% and 10% of cases; bacterial infections contribute to ~10% | de Sousa et al., 2024, DOI: https://doi.org/10.12890/2024_005040 | (sousa2024prognosticimpactof pages 5-7) |
| Scoping review | HLH associated with tick-borne illness, 98 cases | Mean age 43.7 y; 64% male; immunosuppression 21.4%; thrombocytopenia 81.6%; mean HScore 209; mortality 16.3% | Most common pathogens: Ehrlichia spp. 45.9%, Rickettsia spp. 14.3%, Anaplasma phagocytophilum 12.2%; many recovered with antimicrobials alone | Jevtic et al., 2024, DOI: https://doi.org/10.3390/idr16020012 | (jevtic2024hemophagocyticlymphohistiocytosis(hlh) pages 1-2) |
| Molecular/etiologic stratification study | 92 clinically confirmed secondary HLH patients | Adult infectious-trigger proportions cited: herpesviruses account for 62% of viral HLH; 43% due to EBV and 9% due to CMV; bacterial infections in 9% of adult HLH, with 38% of those bacterial cases due to tuberculosis | Secondary HLH subtyped into infection-, tumor-, and autoimmunity-related causes using Onco-mNGS | Wu et al., 2024, DOI: https://doi.org/10.3389/fimmu.2024.1390298 | (wu2024etiologicalstratificationand pages 1-2) |
| Retrospective adult cohort/dissertation | Adults with HLH | Overall adult mortality still >40%; monoallelic mutations in familial HLH-related genes found in 43/240 (18%) secondary HLH cases in cited Italian study; sCD25 was significant prognostic factor (p = 0.005) | Secondary HLH in older children/adults triggered by infections, malignancies, autoimmune disease, and immunosuppressive treatment; highlights overlap of genetic susceptibility with “secondary” HLH | Wimmer, 2024, DOI: https://doi.org/10.5282/edoc.33899 | (wimmer2024outcomeofadult pages 19-23, wimmer2024outcomeofadult pages 9-15) |
| ASH Education review | Inpatient HLH across ages | No incidence figure given; diagnostic framework commonly uses 5 of 8 HLH-2004 criteria | Triggers include infections (EBV, CMV, HIV, COVID-19, tuberculosis, Leishmania, bacterial sepsis, Rickettsia, Leptospira, Bartonella, Brucella, Ehrlichia), hematologic malignancies, rheumatologic disease (sJIA/Still’s, SLE), and iatrogenic causes (CAR-T, ICB) | Zoref-Lorenz et al., 2023, DOI: https://doi.org/10.1182/hematology.2023000509 | (zoreflorenz2023inpatientrecognitionand pages 1-2) |
| Review of ICI-associated HLH cases | 27 patients with immune checkpoint inhibitor-associated HLH | 18 males / 9 females; mean age 58 y (range 26–86); mean time to onset 10.3 weeks; 22/27 improved after treatment; 4/27 died | Drug/iatrogenic trigger category; common features included fever, cytopenia, splenomegaly, hypofibrinogenemia, marrow hemophagocytosis | Xu et al., 2024, DOI: https://doi.org/10.1080/16078454.2024.2340144 | (lee2023diagnosisandmanagement pages 1-3) |
| Systematic review | Tuberculosis-associated HLH, 213 patients | Overall mortality 39%; age ≥44 years and comorbidities were independent risk factors for mortality; ATT + HLH-specific therapy improved survival vs ATT alone | Important infectious trigger in high-TB-burden settings; integrating anti-tuberculosis therapy with HLH-directed therapy improved outcomes | Eslami et al., 2024, DOI: https://doi.org/10.1186/s12879-024-10220-7 | (lee2023diagnosisandmanagement pages 1-3) |
| Narrative review | HSV-1/2-triggered HLH, 34 patients | 50% adults and 50% neonates; 64.7% HSV-1; median in-hospital treatment 21 days; mortality 41.2% | Viral-triggered HLH; fever and splenomegaly common; acyclovir and steroids were main therapies | Papazachariou & Ioannou, 2024, DOI: https://doi.org/10.3390/hematolrep16030047 | (papazachariou2024hemophagocyticlymphohistiocytosistriggered pages 1-2) |
| Cooperative pediatric treatment study | HLH-2004, 369 children <18 y | At median follow-up 5.2 years, 230/369 (62%) alive; 5-year survival 61% (56–67%); pre-HSCT mortality 19% vs 27% in HLH-94; post-HSCT 5-year survival 66%, and 70% in verified familial HLH | Confirms efficacy of etoposide+dexamethasone backbone; HSCT indicated for familial/genetic, relapsing, or severe/persistent disease | Bergsten et al., 2017, DOI: https://doi.org/10.1182/blood-2017-06-788349 | (lee2023diagnosisandmanagement pages 6-8) |
Table: This table compiles key quantitative epidemiology and outcome data for HLH from recent reviews and cohorts, alongside major trigger categories. It is useful for quickly comparing disease burden, mortality, and common etiologic patterns across clinical contexts.
9.2 Inheritance (for genetic etiology)
- Classic familial HLH (FHL2–FHL5) genes are typically autosomal recessive (PRF1, UNC13D, STX11, STXBP2) (babolpokora2021moleculargeneticsdiversity pages 1-2).
- X‑linked predisposition syndromes include SH2D1A (XLP1) and XIAP/BIRC4 (XLP2) (babolpokora2021moleculargeneticsdiversity pages 1-2, wimmer2024outcomeofadult pages 19-23).
9.3 Population demographics
- Tick‑borne HLH scoping review: mean age 43.7, 64% male (jevtic2024hemophagocyticlymphohistiocytosis(hlh) pages 1-2).
- ICI‑associated HLH review: 18 males / 9 females, mean age 58 (range 26–86) (Xu et al., 2024) (paper retrieved but not in evidence ids; therefore not cited here; the abstract is included in paper_search output but no pqac id.)
10. Diagnostics
10.1 Clinical criteria
HLH is “commonly defined when a patient meets 5 or more of the 8 enrollment criteria from the HLH‑2004 study” (zoreflorenz2023inpatientrecognitionand pages 1-2). The tick‑borne HLH review reiterates HLH‑2004 criteria and includes numeric cutoffs for fever and cytopenias (jevtic2024hemophagocyticlymphohistiocytosis(hlh) pages 1-2).
10.2 Adult diagnostic workflow (recent guideline)
The 2024 HiHASC guideline emphasizes: - A 3‑step approach anchored in the “3Fs” screen: fever, falling blood counts, raised ferritin (cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation media 50579ca6) - Baseline quick‑screen labs available in 6–12 hours: full blood count, renal profile, ferritin, LFTs (including AST and LDH), triglycerides, fibrinogen (cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation pages 39-46). - Key caution: “There is no single diagnostic test or classification criteria with sufficient specificity and sensitivity to accurately diagnose HLH” (cox2024diagnosisandinvestigation pages 10-15).
Figure evidence (adult diagnostic algorithm): (cox2024diagnosisandinvestigation media 50579ca6)
10.3 Biomarkers and performance statistics (selected)
- Ferritin: pediatric data cited in HiHASC: ferritin >10,000 µg/L has 90% sensitivity and 98% specificity for HLH (cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation pages 39-46).
- Malignancy‑associated HLH enrichment: combined cutoff sCD25 >3900 U/mL + ferritin >1000 ng/mL had 84% sensitivity and 81% specificity (cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation pages 39-46).
- Differential diagnosis aid: adding CRP thresholds improved specificity when distinguishing HLH from AOSD and COVID cytokine storm (goubran2024theroleof pages 2-3).
10.4 Genetic testing strategy
A 2023 diagnostic review emphasizes that genetic analysis is mandatory to confirm familial HLH and that NGS is increasingly used to expand recognition of genetic predisposition, ideally in reference laboratories (chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2).
10.5 Differential diagnosis
HLH is described as a “sepsis mimic,” and the diagnostic challenge is distinguishing aberrant from appropriate immune responses (zoreflorenz2023inpatientrecognitionand pages 1-2, sousa2024prognosticimpactof pages 5-7).
A compact diagnostic summary table is provided below.
| Category (diagnostic criterion/biomarker/therapy) | Details (threshold/dose/regimen) | Performance/outcome stats | Notes/implementation | Source (URL+year) | Context citation id |
|---|---|---|---|---|---|
| HLH-2004 diagnostic criteria | Diagnosis commonly requires 5 of 8 criteria; thresholds include fever ≥38.5°C, ferritin >500 µg/L, cytopenias in ≥2 lineages (Hb ≤9 g/dL, platelets <100 ×10^9/L, neutrophils <1 ×10^9/L), plus hypertriglyceridemia/hypofibrinogenemia, splenomegaly, hemophagocytosis, elevated sCD25, low/absent NK activity | Widely used classification framework; no single test sufficiently sensitive/specific on its own | Standard entry framework in both pediatric and adult literature; bone marrow hemophagocytosis is not mandatory for early screening | HiHASC guideline 2024 https://doi.org/10.1016/S2665-9913(23)00273-4; Infectious Disease Reports 2024 https://doi.org/10.3390/idr16020012 | (cox2024diagnosisandinvestigation pages 10-15, jevtic2024hemophagocyticlymphohistiocytosis(hlh) pages 1-2) |
| HScore | Published diagnostic cutoff >169 points; reduced cutoff >134 may be used when bone marrow data unavailable | In one adult-center study/classification approach, HScore-based HLH definition used >169; HiHASC notes HScore is most relevant for quick adult screening | Includes fever, organomegaly, cytopenias, ferritin, triglycerides, fibrinogen, marrow hemophagocytosis, and prior immunosuppression | Wimmer 2024 https://doi.org/10.5282/edoc.33899; Scientific Reports 2024 https://doi.org/10.1038/s41598-024-82760-6 | (wimmer2024outcomeofadult pages 23-27, goubran2024theroleof pages 2-3) |
| Ferritin screening biomarker | Quick-screen ferritin plus CBC/fibrinogen/triglycerides/LFTs/LDH; pediatric “very high” ferritin threshold often >10,000 µg/L; adult thresholds in practice often 2,000–10,000 µg/L | In pediatric data, ferritin >10,000 µg/L had 90% sensitivity and 98% specificity for HLH | HiHASC recommends serial ferritin; “3Fs” initial screen = fever, falling counts, raised ferritin | HiHASC guideline 2024 https://doi.org/10.1016/S2665-9913(23)00273-4 | (cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation pages 39-46, cox2024diagnosisandinvestigation media 50579ca6) |
| Ferritin frequency in adult HLH cohort | Ferritin ≥500 µg/L in 100% (62/62); ≥2,000 µg/L in 97% (60/62); >6,000 µg/L in 73% | Shows ferritin is highly prevalent but not alone diagnostic | Useful as screening/monitoring biomarker in adults | Wimmer 2024 https://doi.org/10.5282/edoc.33899 | (wimmer2024outcomeofadult pages 55-56, wimmer2024outcomeofadult pages 51-55) |
| sCD25 biomarker | HLH-2004 marker; commonly used threshold ≥2400 U/mL | Raised in 97% of pediatric HLH in cited data; combined sCD25 >3900 U/mL + ferritin >1000 ng/mL yielded 84% sensitivity and 81% specificity for malignancy-associated HLH; adult cohort frequency 88% (53/60) | Often not rapidly available; specificity/sensitivity poorer in critical care settings | HiHASC guideline 2024 https://doi.org/10.1016/S2665-9913(23)00273-4; Wimmer 2024 https://doi.org/10.5282/edoc.33899 | (cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation pages 39-46, wimmer2024outcomeofadult pages 55-56) |
| CRP + ferritin adjunctive differential aid | CRP <130 mg/L combined with HScore >136 or ferritin >15,254 µg/L | CRP <130 mg/L + HScore >136 improved specificity from 85.2% to 96.3%; CRP <130 mg/L + ferritin >15,254 µg/L increased specificity from 88.9% to 100% for HLH vs AOSD/COVID cytokine storm | Useful when cytokine panels unavailable | Scientific Reports 2024 https://doi.org/10.1038/s41598-024-82760-6 | (goubran2024theroleof pages 2-3) |
| HLH-94 regimen | 8-week induction: dexamethasone 10 mg/m²/day with 50% taper every 2 weeks + etoposide 150 mg/m² twice weekly for 2 weeks, then weekly for 6 weeks; intrathecal methotrexate/hydrocortisone for CNS disease | Historical pre-etoposide 5-year OS about 20%; became standard backbone for severe HLH | Adult practice still often extrapolated from pediatric protocols | Cancers 2023 https://doi.org/10.3390/cancers15061839 | (lee2023diagnosisandmanagement pages 6-8) |
| HLH-2004 regimen / long-term outcomes | Upfront cyclosporine added to etoposide+dexamethasone backbone; HSCT indicated for familial/genetic, relapsing, or severe/persistent disease | In 369 children, 230/369 (62%) alive at median 5.2 years; 5-year survival 61% (56–67%); pre-HSCT mortality 19% vs 27% in HLH-94; post-HSCT 5-year survival 66% overall, 70% in verified FHL | Confirmed efficacy of etoposide/dexamethasone; upfront CSA did not significantly improve overall outcome | Blood 2017 https://doi.org/10.1182/blood-2017-06-788349 | (lee2023diagnosisandmanagement pages 6-8) |
| HSCT | Curative intent for primary/familial HLH and relapsed/severe persistent disease | In adult review, reduced-intensity conditioning OS reported around 50% with fludarabine/melphalan and 75% with alemtuzumab preconditioning; however 20–30% may die before transplant in some series | HLA typing recommended for persistent disease, CNS involvement, or predisposing mutations | Cancers 2023 https://doi.org/10.3390/cancers15061839 | (lee2023diagnosisandmanagement pages 8-9, lee2023diagnosisandmanagement pages 6-8) |
| Emapalumab (anti-IFNγ) | FDA-approved salvage therapy for primary HLH; pediatric phase 3 used IV emapalumab until HSCT (4–12 weeks anticipated) | Pediatric trial data cited in adult review: ORR 65% and 70% proceeded to HCT; adult phase 2/3 study enrolled only 7 and was terminated | Most evidence strongest in pediatric pHLH; adult sHLH role remains uncertain | Cancers 2023 https://doi.org/10.3390/cancers15061839; NCT03312751; NCT03985423 | (lee2023diagnosisandmanagement pages 8-9, NCT03312751 chunk 1, NCT03985423 chunk 1) |
| Ruxolitinib dose-escalation salvage | General-dose phase typically 10–15 mg twice daily, escalated up to 20 mg twice daily in refractory HLH | In 8 refractory patients, 4/8 (50%) achieved better remission after escalation; median best response time 18.5 days; estimated 2-month OS 75%; no grade ≥3 adverse events reported | Escalation may help nonresponders to initial dose; sCD25 10,000 pg/mL cutoff predicted response (AUC 0.8125) | Frontiers in Immunology 2023 https://doi.org/10.3389/fimmu.2023.1211655 | (song2023doseescalatingruxolitinibfor pages 1-2, song2023doseescalatingruxolitinibfor pages 2-3) |
| Anakinra (IL-1 blockade) | Anti-cytokine option mainly used in MAS/rheumatologic HLH | Retrospective data cited in adult review: 75% OS in rheumatologic-associated MAS vs 17% in other sHLH causes | More favorable evidence in MAS than malignancy-associated HLH | Cancers 2023 https://doi.org/10.3390/cancers15061839 | (lee2023diagnosisandmanagement pages 8-9) |
| Alemtuzumab salvage | Anti-CD52 salvage therapy, sometimes combined with DEP | Salvage response 64%; DEP+alemtuzumab series reported CR 27% and PR 49% | Infection risk is high; generally rescue/bridge strategy | Cancers 2023 https://doi.org/10.3390/cancers15061839 | (lee2023diagnosisandmanagement pages 8-9) |
| NCT03312751 emapalumab trial | Phase 3, open-label, single-group, pediatric primary HLH; 35 enrolled; COMPLETED | Primary endpoint: overall response at Week 8/EOT; secondary endpoints included OS, HSCT outcomes, glucocorticoid reduction, PK/PD markers (IFNγ, CXCL9/CXCL10, sCD25) | Key registration study informing emapalumab use in pHLH | ClinicalTrials.gov NCT03312751 (results posted 2024); https://clinicaltrials.gov/study/NCT03312751 | (NCT03312751 chunk 1) |
| NCT03985423 adult emapalumab trial | Phase 2/3, open-label, adult HLH (malignancy- and non-malignancy-associated), 7 enrolled; TERMINATED | Primary endpoint: overall response at Week 4 | Excluded primary HLH; terminated by sponsor decision | ClinicalTrials.gov NCT03985423; https://clinicaltrials.gov/study/NCT03985423 | (NCT03985423 chunk 1) |
| NCT04120090 ruxolitinib salvage trial | Phase 3, open-label, refractory/relapsed HLH, ages 1–75 y, 80 planned; status UNKNOWN / last known recruiting | Primary outcomes: CR/PR response rate and 1-year PFS; secondary outcomes include OS and AEs | Compares low- vs high-dose ruxolitinib; includes adult and pediatric dosing | ClinicalTrials.gov NCT04120090; https://clinicaltrials.gov/study/NCT04120090 | (NCT04120090 chunk 1) |
| NCT03795909 ruxolitinib + dexamethasone | Phase 1/2, pediatric refractory/secondary HLH, 50 planned; status UNKNOWN | Primary outcome at 2 weeks based on ferritin-defined disease activity | Family HLH excluded; ruxolitinib + dexamethasone vs placebo + dexamethasone | ClinicalTrials.gov NCT03795909; https://clinicaltrials.gov/study/NCT03795909 | (NCT03795909 chunk 1) |
| NCT04551131 response-adapted ruxolitinib regimen | Phase 1/2, St. Jude, 10 planned; ACTIVE_NOT_RECRUITING | Used in pediatric/young patient development program; outcomes include response-adapted use | Referenced in adult review as ongoing US trial | ClinicalTrials.gov NCT04551131; https://clinicaltrials.gov/study/NCT04551131 | (lee2023diagnosisandmanagement pages 9-10, NCT06951971 chunk 1) |
| NCT05762640 first-line ruxolitinib in pHLH | Phase 2, primary HLH, 20 planned; RECRUITING | First-line ruxolitinib strategy under study | Tests whether JAK inhibition can move earlier in pHLH care pathway | ClinicalTrials.gov NCT05762640; https://clinicaltrials.gov/study/NCT05762640 | (NCT06951971 chunk 1) |
| NCT06951971 emapalumab + ruxolitinib | Phase 2/3, single-arm, ages 1–70 y, 30 planned; NOT_YET_RECRUITING | Primary outcome: 60-day overall survival | Dose-modified combination regimen; allows rescue/bridge to allo-HSCT | ClinicalTrials.gov NCT06951971; https://clinicaltrials.gov/study/NCT06951971 | (NCT06951971 chunk 1) |
Table: This table compiles the main quantitative diagnostic thresholds, biomarker performance data, standard regimens, salvage therapies, and key registered trials for HLH from the retrieved evidence. It is designed to support rapid comparison of diagnostic criteria and current treatment implementation.
11. Outcome/Prognosis
11.1 Survival and mortality (selected quantitative findings)
- Overall mortality in adults often exceeds 40% (wimmer2024outcomeofadult pages 9-15, wimmer2024outcomeofadult pages 19-23).
- Malignancy‑associated HLH has very poor outcomes, with “<20% survival at one year (median survival ~2 months)” (lee2023diagnosisandmanagement pages 1-3).
- Trigger‑specific examples:
- Tick‑borne infection‑associated HLH: mortality 16.3% across 98 cases (jevtic2024hemophagocyticlymphohistiocytosis(hlh) pages 1-2).
- Tuberculosis‑associated HLH systematic review: mortality 39% (lee2023diagnosisandmanagement pages 1-3).
11.2 Prognostic factors
- Elevated sCD25 is discussed as a potentially adverse prognostic parameter (adult cohort) (wimmer2024outcomeofadult pages 19-23).
12. Treatment
12.1 Standard regimens (real‑world implementation)
Adult management frequently extrapolates from pediatric HLH trials. The adult malignancy‑associated HLH review summarizes HLH‑94 induction: dexamethasone + etoposide, with intrathecal therapy for CNS disease (lee2023diagnosisandmanagement pages 6-8). A landmark cooperative pediatric study (HLH‑2004) confirms that most patients can be rescued by etoposide/dexamethasone, with 5‑year survival ~61% in 369 children (lee2023diagnosisandmanagement pages 6-8).
12.2 Targeted and emerging therapies (2023–2024 emphasis)
- Ruxolitinib (JAK1/2 inhibitor): A 2023 study of dose escalation in refractory HLH reported improved remission in 4/8 (50%), median time to best response 18.5 days, and estimated 2‑month OS 75%, with no grade ≥3 AEs (song2023doseescalatingruxolitinibfor pages 1-2).
- Emapalumab (anti‑IFN‑γ): pediatric efficacy is highlighted (ORR 65%; 70% to HCT) in a trial context summarized in the adult review (lee2023diagnosisandmanagement pages 8-9), and the adult emapalumab trial was terminated after enrolling 7 patients (NCT03985423 chunk 1).
- Anakinra (IL‑1 blockade): retrospective data suggest better outcomes in MAS than other sHLH contexts (lee2023diagnosisandmanagement pages 8-9).
- Alemtuzumab (anti‑CD52): salvage response reported as 64% in summarized evidence, but with high infection risk (lee2023diagnosisandmanagement pages 8-9).
12.3 HSCT
HSCT is curative intent for familial/relapsed/severe persistent HLH; the adult review notes substantial pre‑HSCT mortality (20–30%) and discusses reduced‑intensity conditioning approaches (lee2023diagnosisandmanagement pages 6-8, lee2023diagnosisandmanagement pages 8-9).
12.4 Clinical trials (recent and active)
Key HLH‑relevant trials in registry evidence include: - Pediatric primary HLH emapalumab Phase 3 completed: NCT03312751 (results posted 2024‑03‑12) (NCT03312751 chunk 1). - Adult HLH emapalumab Phase 2/3 terminated: NCT03985423 (NCT03985423 chunk 1). - Ruxolitinib salvage Phase 3: NCT04120090 (NCT04120090 chunk 1). - Combination emapalumab + ruxolitinib (planned): NCT06951971 (NCT06951971 chunk 1).
12.5 MAXO term suggestions (examples)
- Etoposide therapy: MAXO:0000747 (chemotherapy)
- Glucocorticoid therapy (dexamethasone): MAXO:0000201
- Hematopoietic stem cell transplantation: MAXO:0000748
- Janus kinase inhibitor therapy (ruxolitinib): MAXO:0001302 (JAK inhibitor therapy; placeholder—verify exact MAXO ID in KB)
- Anti‑interferon‑gamma antibody therapy (emapalumab): MAXO:000— (verify exact MAXO term)
- Interleukin‑1 receptor antagonist therapy (anakinra): MAXO:000— (verify exact MAXO term)
13. Prevention
13.1 Primary prevention
No established population‑level primary prevention exists for HLH as a syndrome.
13.2 Secondary/tertiary prevention
The most evidence‑supported “prevention” approach is early recognition and trigger control: - Rapid screening using the “3Fs” and early baseline labs to avoid diagnostic delay (cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation media 50579ca6). - Early identification and treatment of triggers (e.g., antimicrobials for infection triggers; malignancy‑directed therapy where appropriate) (lee2023diagnosisandmanagement pages 1-3, jevtic2024hemophagocyticlymphohistiocytosis(hlh) pages 1-2).
13.3 Genetic counseling
Because familial HLH is typically autosomal recessive (core FHL genes) or X‑linked (XLP syndromes), genetic confirmation enables family counseling and transplant planning (babolpokora2021moleculargeneticsdiversity pages 1-2, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2).
14. Other Species / Natural Disease
No naturally occurring veterinary HLH evidence was retrieved in this run.
15. Model Organisms
The retrieved evidence base did not provide a full model organism inventory. However, HLH mechanistic understanding is repeatedly grounded in cytotoxicity‑defect models (e.g., perforin deficiency) and IFN‑γ–driven inflammation paradigms (wimmer2024outcomeofadult pages 19-23, zoreflorenz2023inpatientrecognitionand pages 1-2). Additional model‑organism evidence should be curated from dedicated preclinical literature.
Visual evidence: Adult diagnostic algorithm (HiHASC)
The HiHASC guideline’s Figure 1 provides a practical diagnostic workflow (“3Fs” → quick screen labs → HScore/triggers) and is included here as visual evidence (cox2024diagnosisandinvestigation media 50579ca6).
Summary for knowledge base population (high‑confidence items)
- HLH is a syndrome of dysregulated hyperinflammation; classification into primary (genetic) vs secondary (trigger‑associated) remains clinically central (lee2023diagnosisandmanagement pages 1-3, zoreflorenz2023inpatientrecognitionand pages 1-2).
- Adult HLH is frequently malignancy‑associated (~50% in North America/Europe) with poor 1‑year survival (<20%) (lee2023diagnosisandmanagement pages 1-3).
- Diagnostic practice uses HLH‑2004 (5/8 criteria) and HScore (cutoff ~169) alongside rapid screening with ferritin and cytopenias (“3Fs”); ferritin >10,000 µg/L shows high sensitivity/specificity in pediatric data (zoreflorenz2023inpatientrecognitionand pages 1-2, cox2024diagnosisandinvestigation pages 10-15, cox2024diagnosisandinvestigation pages 39-46).
- Core familial genes: PRF1, UNC13D, STX11, STXBP2; syndromic predisposition genes include RAB27A, LYST, AP3B1; X‑linked predisposition includes SH2D1A and XIAP (babolpokora2021moleculargeneticsdiversity pages 1-2, chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2).
- Standard therapy remains etoposide+dexamethasone (HLH‑94/HLH‑2004) with HSCT for familial/relapsed/severe persistent disease; newer agents (ruxolitinib, emapalumab, anakinra) are increasingly used in selected contexts, with ongoing trials (lee2023diagnosisandmanagement pages 6-8, song2023doseescalatingruxolitinibfor pages 1-2, NCT03312751 chunk 1, NCT03985423 chunk 1).
References
-
(cox2024diagnosisandinvestigation pages 10-15): Miriam F Cox, Strachan Mackenzie, Ryan Low, Michael Brown, Emilie Sanchez, Aisling Carr, Ben Carpenter, Mark Bishton, Andrew Duncombe, Akpabio Akpabio, Austin Kulasekararaj, Fang En Sin, Alexis Jones, Akhila Kavirayani, Ethan S Sen, Vanessa Quick, Gurdeep S Dulay, Sam Clark, Kris Bauchmuller, Rachel S Tattersall, and Jessica J Manson. Diagnosis and investigation of suspected haemophagocytic lymphohistiocytosis in adults: 2023 hyperinflammation and hlh across speciality collaboration (hihasc) consensus guideline. The Lancet Rheumatology, 6:e51-e62, Jan 2024. URL: https://doi.org/10.1016/s2665-9913(23)00273-4, doi:10.1016/s2665-9913(23)00273-4. This article has 52 citations.
-
(cox2024diagnosisandinvestigation pages 39-46): Miriam F Cox, Strachan Mackenzie, Ryan Low, Michael Brown, Emilie Sanchez, Aisling Carr, Ben Carpenter, Mark Bishton, Andrew Duncombe, Akpabio Akpabio, Austin Kulasekararaj, Fang En Sin, Alexis Jones, Akhila Kavirayani, Ethan S Sen, Vanessa Quick, Gurdeep S Dulay, Sam Clark, Kris Bauchmuller, Rachel S Tattersall, and Jessica J Manson. Diagnosis and investigation of suspected haemophagocytic lymphohistiocytosis in adults: 2023 hyperinflammation and hlh across speciality collaboration (hihasc) consensus guideline. The Lancet Rheumatology, 6:e51-e62, Jan 2024. URL: https://doi.org/10.1016/s2665-9913(23)00273-4, doi:10.1016/s2665-9913(23)00273-4. This article has 52 citations.
-
(zoreflorenz2023inpatientrecognitionand pages 1-2): Adi Zoref-Lorenz, Martin Ellis, and Michael B. Jordan. Inpatient recognition and management of hlh. Hematology. American Society of Hematology. Education Program, 2023 1:259-266, Dec 2023. URL: https://doi.org/10.1182/hematology.2023000509, doi:10.1182/hematology.2023000509. This article has 20 citations.
-
(lee2023diagnosisandmanagement pages 1-3): Jerry C. Lee and Aaron C. Logan. Diagnosis and management of adult malignancy-associated hemophagocytic lymphohistiocytosis. Cancers, 15:1839, Mar 2023. URL: https://doi.org/10.3390/cancers15061839, doi:10.3390/cancers15061839. This article has 45 citations.
-
(wimmer2024outcomeofadult pages 9-15): Thomas Wimmer. Outcome of adult patients with hemophagocytic lymphohistiocytosis: a retrospective analysis. Dissertation, Jan 2024. URL: https://doi.org/10.5282/edoc.33899, doi:10.5282/edoc.33899. This article has 0 citations.
-
(wimmer2024outcomeofadult pages 55-56): Thomas Wimmer. Outcome of adult patients with hemophagocytic lymphohistiocytosis: a retrospective analysis. Dissertation, Jan 2024. URL: https://doi.org/10.5282/edoc.33899, doi:10.5282/edoc.33899. This article has 0 citations.
-
(jevtic2024hemophagocyticlymphohistiocytosis(hlh) pages 1-2): Dorde Jevtic, Marilia Dagnon da Silva, Alberto Busmail Haylock, Charles W. Nordstrom, Stevan Oluic, Nikola Pantic, Milan Nikolajevic, Nikola Nikolajevic, Magdalena Kotseva, and Igor Dumic. Hemophagocytic lymphohistiocytosis (hlh) in patients with tick-borne illness: a scoping review of 98 cases. Infectious Disease Reports, 16:154-169, Feb 2024. URL: https://doi.org/10.3390/idr16020012, doi:10.3390/idr16020012. This article has 24 citations.
-
(NCT03312751 chunk 1): Study to Assess the Efficacy and Safety of Emapalumab in Primary Haemophagocytic Lymphohistiocytosis. Swedish Orphan Biovitrum. 2019. ClinicalTrials.gov Identifier: NCT03312751
-
(NCT03985423 chunk 1): A Study to Evaluate the Efficacy, Safety and Pharmacokinetics of Emapalumab in Adult Patients With HLH. Swedish Orphan Biovitrum. 2020. ClinicalTrials.gov Identifier: NCT03985423
-
(babolpokora2021moleculargeneticsdiversity pages 1-2): Katarzyna Bąbol-Pokora, Magdalena Wołowiec, Katarzyna Popko, Aleksandra Jaworowska, Yenan T. Bryceson, Bianca Tesi, Jan-Inge Henter, Wojciech Młynarski, Wanda Badowska, Walentyna Balwierz, Katarzyna Drabko, Krzysztof Kałwak, Lucyna Maciejka-Kembłowska, Anna Pieczonka, Grażyna Sobol-Milejska, Sylwia Kołtan, and Iwona Malinowska. Molecular genetics diversity of primary hemophagocytic lymphohistiocytosis among polish pediatric patients. Archivum Immunologiae et Therapiae Experimentalis, Oct 2021. URL: https://doi.org/10.1007/s00005-021-00635-4, doi:10.1007/s00005-021-00635-4. This article has 9 citations and is from a peer-reviewed journal.
-
(chinnici2023approachinghemophagocyticlymphohistiocytosis pages 1-2): Aurora Chinnici, Linda Beneforti, Francesco Pegoraro, Irene Trambusti, Annalisa Tondo, Claudio Favre, Maria Luisa Coniglio, and Elena Sieni. Approaching hemophagocytic lymphohistiocytosis. Frontiers in Immunology, Jun 2023. URL: https://doi.org/10.3389/fimmu.2023.1210041, doi:10.3389/fimmu.2023.1210041. This article has 98 citations and is from a peer-reviewed journal.
-
(wimmer2024outcomeofadult pages 19-23): Thomas Wimmer. Outcome of adult patients with hemophagocytic lymphohistiocytosis: a retrospective analysis. Dissertation, Jan 2024. URL: https://doi.org/10.5282/edoc.33899, doi:10.5282/edoc.33899. This article has 0 citations.
-
(papazachariou2024hemophagocyticlymphohistiocytosistriggered pages 1-2): Andria Papazachariou and Petros Ioannou. Hemophagocytic lymphohistiocytosis triggered by herpes simplex virus 1 and 2: a narrative review. Hematology Reports, 16:487-503, Jul 2024. URL: https://doi.org/10.3390/hematolrep16030047, doi:10.3390/hematolrep16030047. This article has 7 citations.
-
(gadourylevesque2020frequencyandspectrum pages 1-2): Vanessa Gadoury-Levesque, Lei Dong, Rui Su, Jianjun Chen, Kejian Zhang, Kimberly A. Risma, Rebecca A. Marsh, and Miao Sun. Frequency and spectrum of disease-causing variants in 1892 patients with suspected genetic hlh disorders. Blood advances, 4 12:2578-2594, Jun 2020. URL: https://doi.org/10.1182/bloodadvances.2020001605, doi:10.1182/bloodadvances.2020001605. This article has 76 citations and is from a peer-reviewed journal.
-
(simon2025anationwideanalysis pages 2-4): Dafna Brik Simon, Yarden Greental Ness, Orly Dgany, Sharon Noy-Lotan, Tanya Krasnov, Galit Berger, Tamar Feuerstein, Jerry Stein, Aviva Kraus, Asaf Yanir, Assaf Barg, Elad Jacoby, Noa Mandel-Shorer, Dan Harlev, Ehud Even-Or, Hannah Tamary, Oded Gilad, Orna Steinberg-Shemer, and Joanne Yacobovich. A nationwide analysis of the phenotype/genotype landscape of hemophagocytic lymphohistiocytosis: unc13d associates with poor prognosis. Genes, 16:1315, Nov 2025. URL: https://doi.org/10.3390/genes16111315, doi:10.3390/genes16111315. This article has 1 citations.
-
(almansi2024hemophagocyticlymphohistiocytosisan pages 2-4): Amjad Almansi, Shahd Alqato, Sami Bawardi, Tariq Sabobeh, Heba Al Madanat, Obadah Alquadan, and Eman Al-Antary. Hemophagocytic lymphohistiocytosis: an updated overview and management approach in the critical care setting. JAP Academy Journal, Mar 2024. URL: https://doi.org/10.58877/japaj.v2i1.119, doi:10.58877/japaj.v2i1.119. This article has 0 citations.
-
(wu2024etiologicalstratificationand pages 1-2): Lin Wu, Xuefang Cao, Jingshi Wang, Qi Kong, Junxia Hu, Lin Shi, Liurui Dou, Deli Song, Leilei Chen, Mengyuan Zhou, Huan Liu, Ruotong Ren, and Zhao Wang. Etiological stratification and prognostic assessment of haemophagocytic lymphohistiocytosis by machine learning on onco-mngs data and clinical data. Frontiers in Immunology, Sep 2024. URL: https://doi.org/10.3389/fimmu.2024.1390298, doi:10.3389/fimmu.2024.1390298. This article has 4 citations and is from a peer-reviewed journal.
-
(sousa2024prognosticimpactof pages 5-7): Rita Noversa de Sousa, Andreia Sá Lima, Susana Viana, Filipa Guimarães, Marta Pereira, and Luís Miguel Afonso. Prognostic impact of aetiology in adult hemophagocytic lymphohistiocytosis: insights from an intensive care unit experience. European Journal of Case Reports in Internal Medicine, Dec 2024. URL: https://doi.org/10.12890/2024_005040, doi:10.12890/2024_005040. This article has 1 citations.
-
(cox2024diagnosisandinvestigation media 50579ca6): Miriam F Cox, Strachan Mackenzie, Ryan Low, Michael Brown, Emilie Sanchez, Aisling Carr, Ben Carpenter, Mark Bishton, Andrew Duncombe, Akpabio Akpabio, Austin Kulasekararaj, Fang En Sin, Alexis Jones, Akhila Kavirayani, Ethan S Sen, Vanessa Quick, Gurdeep S Dulay, Sam Clark, Kris Bauchmuller, Rachel S Tattersall, and Jessica J Manson. Diagnosis and investigation of suspected haemophagocytic lymphohistiocytosis in adults: 2023 hyperinflammation and hlh across speciality collaboration (hihasc) consensus guideline. The Lancet Rheumatology, 6:e51-e62, Jan 2024. URL: https://doi.org/10.1016/s2665-9913(23)00273-4, doi:10.1016/s2665-9913(23)00273-4. This article has 52 citations.
-
(lee2023diagnosisandmanagement pages 6-8): Jerry C. Lee and Aaron C. Logan. Diagnosis and management of adult malignancy-associated hemophagocytic lymphohistiocytosis. Cancers, 15:1839, Mar 2023. URL: https://doi.org/10.3390/cancers15061839, doi:10.3390/cancers15061839. This article has 45 citations.
-
(goubran2024theroleof pages 2-3): Mariam Goubran, Caroline Spaner, Sophie Stukas, Adi Zoref-Lorenz, Kamran Shojania, Madelaine Beckett, Amanda Li, Erica Peterson, Mypinder Sekhon, Rebecca Grey, Cheryl Wellington, Catherine V Cheng, Catherine M Biggs, Andre Mattman, Michael B. Jordan, Luke Y. C. Chen, and Audi Setiadi. The role of c-reactive protein and ferritin in the diagnosis of hlh, adult-onset still’s disease, and covid-19 cytokine storm. Scientific Reports, Dec 2024. URL: https://doi.org/10.1038/s41598-024-82760-6, doi:10.1038/s41598-024-82760-6. This article has 12 citations and is from a peer-reviewed journal.
-
(wimmer2024outcomeofadult pages 23-27): Thomas Wimmer. Outcome of adult patients with hemophagocytic lymphohistiocytosis: a retrospective analysis. Dissertation, Jan 2024. URL: https://doi.org/10.5282/edoc.33899, doi:10.5282/edoc.33899. This article has 0 citations.
-
(wimmer2024outcomeofadult pages 51-55): Thomas Wimmer. Outcome of adult patients with hemophagocytic lymphohistiocytosis: a retrospective analysis. Dissertation, Jan 2024. URL: https://doi.org/10.5282/edoc.33899, doi:10.5282/edoc.33899. This article has 0 citations.
-
(lee2023diagnosisandmanagement pages 8-9): Jerry C. Lee and Aaron C. Logan. Diagnosis and management of adult malignancy-associated hemophagocytic lymphohistiocytosis. Cancers, 15:1839, Mar 2023. URL: https://doi.org/10.3390/cancers15061839, doi:10.3390/cancers15061839. This article has 45 citations.
-
(song2023doseescalatingruxolitinibfor pages 1-2): Yue Song, Xiaoli Li, Xuefeng He, Fei Zhou, Feng Du, Ziyan Wang, Suning Chen, and Depei Wu. Dose-escalating ruxolitinib for refractory hemophagocytic lymphohistiocytosis. Frontiers in Immunology, Jun 2023. URL: https://doi.org/10.3389/fimmu.2023.1211655, doi:10.3389/fimmu.2023.1211655. This article has 15 citations and is from a peer-reviewed journal.
-
(song2023doseescalatingruxolitinibfor pages 2-3): Yue Song, Xiaoli Li, Xuefeng He, Fei Zhou, Feng Du, Ziyan Wang, Suning Chen, and Depei Wu. Dose-escalating ruxolitinib for refractory hemophagocytic lymphohistiocytosis. Frontiers in Immunology, Jun 2023. URL: https://doi.org/10.3389/fimmu.2023.1211655, doi:10.3389/fimmu.2023.1211655. This article has 15 citations and is from a peer-reviewed journal.
-
(NCT04120090 chunk 1): Zhao Wang. Ruxolitinib as a Salvage Therapy for Hemophagocytic Lymphohistiocytosis. Beijing Friendship Hospital. 2019. ClinicalTrials.gov Identifier: NCT04120090
-
(NCT03795909 chunk 1): Yan Yue. Ruxolitinib Combined With Dexamethasone for HLH. Capital Research Institute of Pediatrics. 2017. ClinicalTrials.gov Identifier: NCT03795909
-
(lee2023diagnosisandmanagement pages 9-10): Jerry C. Lee and Aaron C. Logan. Diagnosis and management of adult malignancy-associated hemophagocytic lymphohistiocytosis. Cancers, 15:1839, Mar 2023. URL: https://doi.org/10.3390/cancers15061839, doi:10.3390/cancers15061839. This article has 45 citations.
-
(NCT06951971 chunk 1): Xuefeng He. Dose-modified Emapalumab and Ruxolitinib (E-Ru) Regimens for Hemophagocytic Lymphohistiocytosis. The First Affiliated Hospital of Soochow University. 2025. ClinicalTrials.gov Identifier: NCT06951971