Hashimoto Encephalopathy
Hashimoto encephalopathy, also called steroid-responsive encephalopathy associated with autoimmune thyroiditis, is an uncommon acquired autoimmune encephalopathy syndrome defined by otherwise unexplained subacute encephalopathy, thyroid autoantibody positivity, exclusion of better-defined neuronal antibody, infectious, toxic-metabolic, psychiatric, and neurodegenerative mimics, and frequent but not universal improvement with immunotherapy. Contemporary studies emphasize that antithyroid antibodies are diagnostically nonspecific, so objective neurologic abnormalities and a careful differential diagnosis are central to curation and clinical use.
Ask OpenScientist
Ask a research question about Hashimoto Encephalopathy. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Mappings
Subtypes
3Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Pathophysiology
3Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Pathograph
Phenotypes
9Show evidence (1 reference)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (2 references)
Medical Actions
4Show evidence (4 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Differential Diagnoses
1Conditions with similar clinical presentations that must be differentiated from Hashimoto Encephalopathy:
- Alternative diagnoses in the Mayo Clinic referral cohort included functional neurological disorder, neurodegenerative disorder, subjective cognitive complaints, chronic pain syndrome, primary psychiatric disease, sleep disorder, genetic/developmental conditions, and non-autoimmune seizure disorders.
Show evidence (1 reference)
Source YAML
click to showname: Hashimoto Encephalopathy
creation_date: "2026-05-16T09:06:04Z"
updated_date: "2026-05-16T10:06:24Z"
category: Autoimmune
parents:
- Autoimmune Encephalitis
- Neurological Disease
- Autoimmune Disease
synonyms:
- Steroid-responsive encephalopathy associated with autoimmune thyroiditis
- SREAT
- Hashimoto encephalopathy
- Hashimoto's encephalopathy
- Hashimoto encephalitis
disease_term:
preferred_term: steroid-responsive encephalopathy associated with autoimmune thyroiditis
term:
id: MONDO:0019385
label: steroid-responsive encephalopathy associated with autoimmune thyroiditis
mappings:
mondo_mappings:
- term:
id: MONDO:0019385
label: steroid-responsive encephalopathy associated with autoimmune thyroiditis
mapping_predicate: skos:exactMatch
mapping_source: MONDO
mapping_justification: >-
MONDO:0019385 is the specific MONDO class for steroid-responsive
encephalopathy associated with autoimmune thyroiditis, with SREAT as an
exact synonym and Hashimoto encephalopathy as a related synonym.
description: >-
Hashimoto encephalopathy, also called steroid-responsive encephalopathy
associated with autoimmune thyroiditis, is an uncommon acquired autoimmune
encephalopathy syndrome defined by otherwise unexplained subacute
encephalopathy, thyroid autoantibody positivity, exclusion of better-defined
neuronal antibody, infectious, toxic-metabolic, psychiatric, and
neurodegenerative mimics, and frequent but not universal improvement with
immunotherapy. Contemporary studies emphasize that antithyroid antibodies are
diagnostically nonspecific, so objective neurologic abnormalities and a
careful differential diagnosis are central to curation and clinical use.
prevalence:
- population: General population
measure_type: POINT_PREVALENCE
prevalence_class: BAND_1_9_PER_100000
rate_per_100000: 2.1
percentage: 2.1 / 100,000
notes: >-
A pediatric-focused literature review cites an estimated prevalence of
2.1 per 100,000, while noting pediatric disease is uncommon and likely
under-recognized.
evidence:
- reference: PMID:32921783
reference_title: "Hashimoto encephalopathy: a case report and a short revision of current literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Its prevalence is 2.1/100.000; however, it is uncommon in the pediatric population"
explanation: >-
This review provides the prevalence estimate and highlights rarity in
children.
progression:
- phase: Subacute encephalopathy
age_range: Children through older adults, most often adults
notes: >-
Published cohorts include pediatric and adult patients. Onset is commonly
subacute, and the course may be monophasic, relapsing, or progressive before
immunotherapy.
evidence:
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Most patients (76.9%) had onset within < 3 months."
explanation: >-
A modern tertiary-center cohort supports subacute onset as a typical
temporal pattern.
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "During follow-up, 40 patients (16%) experienced at least one relapse."
explanation: >-
The 251-case literature synthesis supports a relapsing subset.
has_subtypes:
- name: Classic steroid-responsive SREAT
description: >-
The historical syndrome of unexplained encephalopathy with antithyroid
antibodies and substantial response to corticosteroids after exclusion of
alternative causes.
evidence:
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Steroid-responsive encephalopathy and associated autoimmune thyroiditis (SREAT) is characterized by encephalopathy and the presence of antithyroid antibodies."
explanation: >-
The systematic literature synthesis defines the core SREAT concept.
- name: Anti-NAE-associated limbic encephalitis subtype
description: >-
A proposed Hashimoto encephalopathy subtype with limbic encephalitis,
antithyroid antibodies, anti-NH2-terminal alpha-enolase antibodies, negative
common neuronal surface antibody panels, and favorable immunotherapy
response. More recent reviews consider anti-NAE nonspecific, so this subtype
should not be used as a standalone diagnostic marker.
evidence:
- reference: PMID:28272206
reference_title: "Limbic encephalitis associated with anti-NH2-terminal of alpha-enolase antibodies: A clinical subtype of Hashimoto encephalopathy."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "This study demonstrated that LE associated with anti-NAE antibodies is a nonparaneoplastic LE and various limbic symptoms that depend on the onset type."
explanation: >-
The cohort supports an anti-NAE-associated nonparaneoplastic limbic
encephalitis phenotype within Hashimoto encephalopathy.
- reference: DOI:10.3390/ijms25137101
reference_title: "Difficulties in the Diagnostics and Treatment of Hashimoto's Encephalopathy"
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "the proposed anti NH2-terminal-α-enolase (anti-NAE) is non-specific for HE."
explanation: >-
The systematic review supports modeling anti-NAE as provisional and
insufficient as an isolated diagnostic marker.
- name: Pediatric Hashimoto encephalopathy
description: >-
Childhood and adolescent cases often present with seizures, altered
consciousness, behavioral change, psychosis, tremor, or dystonia and may
require corticosteroids, intravenous immunoglobulin, or plasma exchange.
evidence:
- reference: PMID:28784301
reference_title: "Hashimoto encephalopathy in pediatric patients: Homogeneity in clinical presentation and heterogeneity in antibody titers."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Presenting symptoms were seizures, altered consciousness, behavioral changes, psychosis, tremor, and dystonia."
explanation: >-
The pediatric case series summarizes common pediatric presentations.
pathophysiology:
- name: Antithyroid Antibody-Associated Autoimmune Context
description: >-
Serum anti-thyroid peroxidase and/or anti-thyroglobulin antibodies are part
of the SREAT case definition and reflect B-cell and plasma-cell autoimmune
activity, but the antibodies are common in the general population and do not
by themselves prove autoimmune CNS disease. This node is therefore modeled
as a diagnostic and autoimmune-context mechanism rather than a direct
neuronal injury mechanism.
mechanism_confidence: PROVISIONAL
cell_types:
- preferred_term: B cell
term:
id: CL:0000236
label: B cell
- preferred_term: Plasma cell
term:
id: CL:0000786
label: plasma cell
biological_processes:
- preferred_term: B cell activation
term:
id: GO:0042113
label: B cell activation
- preferred_term: Adaptive immune response
term:
id: GO:0002250
label: adaptive immune response
evidence:
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "In serum, 34% of patients were positive for anti-thyroid peroxidase (TPO) antibodies, 7% for anti-thyroglobulin (TG) antibodies, and 69% both."
explanation: >-
The 251-case synthesis quantifies anti-TPO and anti-TG antibody
positivity among reported SREAT cases.
- reference: PMID:34061124
reference_title: "Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Thyroid antibody prevalence is high in the general population, and does not support a diagnosis of autoimmune encephalopathy in the absence of objective neurological and CNS-specific immunological abnormalities."
explanation: >-
This Mayo Clinic referral series supports the conservative interpretation
that thyroid antibodies are nonspecific markers rather than sufficient
pathogenic evidence.
- name: Steroid-Responsive CNS Neuroinflammation
description: >-
True SREAT cases are thought to involve immune-mediated CNS dysfunction with
altered mental status, seizures, neuropsychiatric symptoms, sometimes CSF or
EEG abnormalities, and frequent response to glucocorticoids. The precise
tissue-level mechanism remains unresolved; proposed processes include
vasculitic or other inflammatory CNS injury.
mechanism_confidence: PROVISIONAL
cell_types:
- preferred_term: Neuron
term:
id: CL:0000540
label: neuron
- preferred_term: Astrocyte
term:
id: CL:0000127
label: astrocyte
- preferred_term: Endothelial cell
term:
id: CL:0000115
label: endothelial cell
biological_processes:
- preferred_term: Inflammatory response
term:
id: GO:0006954
label: inflammatory response
- preferred_term: Immune response
term:
id: GO:0006955
label: immune response
evidence:
- reference: PMID:36853554
reference_title: "Hashimoto's Encephalopathy: Case Series and Literature Review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Available evidences point towards an autoimmune etiology due to vasculitis or other inflammatory process."
explanation: >-
The review supports modeling CNS inflammation or vasculitis as plausible
but not definitively resolved pathophysiology.
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Most patients responded well to treatment, so clinical suspicion and early diagnosis and treatment will lead to improved patient outcomes."
explanation: >-
Treatment responsiveness in a defined cohort supports an immune-mediated
component in correctly selected cases.
- name: Anti-NAE-Associated Limbic Neuroinflammation
description: >-
A subset of reported Hashimoto encephalopathy cases has anti-NH2-terminal
alpha-enolase antibodies with limbic encephalitis, consciousness and memory
disturbance, psychiatric symptoms, seizures, abnormal CSF or EEG, and
immunotherapy responsiveness. Later reviews caution that anti-NAE lacks
specificity, so this is modeled as a provisional subtype-associated
mechanism.
mechanism_confidence: PROVISIONAL
subtypes:
- Anti-NAE-associated limbic encephalitis subtype
cell_types:
- preferred_term: Neuron
term:
id: CL:0000540
label: neuron
- preferred_term: Endothelial cell
term:
id: CL:0000115
label: endothelial cell
biological_processes:
- preferred_term: Immune response
term:
id: GO:0006955
label: immune response
- preferred_term: Inflammatory response
term:
id: GO:0006954
label: inflammatory response
evidence:
- reference: PMID:28272206
reference_title: "Limbic encephalitis associated with anti-NH2-terminal of alpha-enolase antibodies: A clinical subtype of Hashimoto encephalopathy."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Consciousness disturbance (71%) and memory disturbance (64%) were frequently observed, followed by psychiatric symptoms (50%) and seizures (43%)."
explanation: >-
The anti-NAE limbic encephalitis cohort links this subtype to limbic
clinical manifestations.
- reference: PMID:31525528
reference_title: "Serial brain MRI changes related to autoimmune pathophysiology in Hashimoto encephalopathy with anti-NAE antibodies: A case-series study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "MRI lesions that fluctuate according to the disease condition were frequently observed in HE patients with anti-NAE antibodies"
explanation: >-
Fluctuating MRI lesions support immune-mediated, disease-activity-linked
CNS inflammation in anti-NAE-positive cases.
phenotypes:
- name: Encephalopathy
category: Neurological
frequency: OBLIGATE
diagnostic: true
description: >-
Altered mental status or brain dysfunction is required by the SREAT concept
and may present as confusion, clouded consciousness, cognitive decline,
delirium, or coma.
phenotype_term:
preferred_term: Encephalopathy
term:
id: HP:0001298
label: Encephalopathy
evidence:
- reference: PMID:34061124
reference_title: "Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Hashimoto encephalopathy, also known as steroid-responsive encephalopathy associated with autoimmune thyroiditis, has been defined by sub-acute onset encephalopathy"
explanation: >-
The Mayo Clinic cohort states encephalopathy is part of the disease
definition.
- name: Seizures
category: Neurological
frequency: FREQUENT
description: >-
Seizures may be focal, generalized, or status epilepticus; in some cohorts,
nonconvulsive status epilepticus is refractory to antiseizure drugs but
improves with immunotherapy.
phenotype_term:
preferred_term: Seizure
term:
id: HP:0001250
label: Seizure
evidence:
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Patients presented encephalitis signs with convulsions (n=117; 47%)"
explanation: >-
The 251-case literature synthesis supports seizures as a frequent
phenotype.
- reference: DOI:10.1007/s13760-024-02520-1
reference_title: "Clinical and diagnostic characteristics of Hashimoto's encephalopathy: a single-center, retrospective study"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Nonconvulsive status epilepticus on EEG was observed in six patients, all of whom were intractable to antiepileptic drugs."
explanation: >-
A modern retrospective cohort supports nonconvulsive status epilepticus as
an important seizure presentation.
- name: Cognitive Impairment and Memory Loss
category: Neurological
frequency: FREQUENT
description: >-
Cognitive impairment may be acute, subacute, or progressive and frequently
includes memory impairment.
phenotype_term:
preferred_term: Memory impairment
term:
id: HP:0002354
label: Memory impairment
evidence:
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "memory impairment (n=107, 43%)"
explanation: >-
The large literature synthesis quantifies memory impairment in reported
cases.
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Clinical presentations included cognitive impairment (76.9%)"
explanation: >-
A modern tertiary-center cohort supports cognitive impairment as a common
manifestation.
- name: Confusion or Clouded Consciousness
category: Neurological
frequency: FREQUENT
description: >-
Patients commonly present with confusion, clouding of consciousness,
delirium, or fluctuating awareness.
phenotype_term:
preferred_term: Confusion
term:
id: HP:0001289
label: Confusion
evidence:
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "confusion (n=115, 46%)"
explanation: >-
Confusion is one of the most frequent manifestations in the 251-case
synthesis.
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "clouding of consciousness (46.2%)"
explanation: >-
A modern clinical cohort supports clouded consciousness as a frequent
presentation.
- name: Neuropsychiatric Symptoms
category: Psychiatric
frequency: FREQUENT
description: >-
Hallucinations, delusions, mood disturbance, behavior change, psychosis, or
catatonia may dominate the initial presentation and can lead to primary
psychiatric misdiagnosis.
phenotype_term:
preferred_term: Psychosis
term:
id: HP:0000709
label: Psychosis
evidence:
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The neuropsychiatric presentations were visual hallucination (30.8%), auditory hallucination (15.4%), delusion (7.7%), and mood disturbance (23.1%)."
explanation: >-
This cohort directly documents neuropsychiatric symptoms in SREAT.
- reference: PMID:41000339
reference_title: "Hashimoto's encephalopathy in psychiatric inpatients: neuropsychiatric morbidity, diagnostic challenges and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The most discriminating clinical features were delirium (88.9% in HE vs. 6.5% in non-HE; p<0.001) and catatonia (77.8% vs. 32.3%; p=0.015)."
explanation: >-
A psychiatric inpatient cohort supports delirium-catatonia presentations
as discriminating features among thyroid-antibody-positive inpatients.
- name: Ataxia or Gait Disturbance
category: Neurological
frequency: FREQUENT
description: >-
Cerebellar ataxia or gait disturbance is a recurring clinical manifestation
and is emphasized as a presentation that should prompt consideration of
SREAT after exclusion of mimics.
phenotype_term:
preferred_term: Ataxia
term:
id: HP:0001251
label: Ataxia
evidence:
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "gait disturbance (n=67, 27%)"
explanation: >-
Gait disturbance is quantified in the 251-case literature synthesis.
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Other clinical presentations included seizure (38.5%), abnormal movement (23.1%), sleep disturbance (38.5%), ataxia (46.2%)"
explanation: >-
A modern cohort supports ataxia as a frequent manifestation.
- name: Sleep Disturbance
category: Neurological
frequency: FREQUENT
description: >-
Sleep disturbance is reported in modern SREAT cohorts and may accompany
cognitive, psychiatric, seizure, or movement presentations.
phenotype_term:
preferred_term: Sleep disturbance
term:
id: HP:0002360
label: Sleep disturbance
evidence:
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "sleep disturbance (38.5%)"
explanation: >-
The Siriraj tertiary-center cohort reports sleep disturbance above the
frequency threshold for curation.
- name: Speech Disorder
category: Neurological
frequency: FREQUENT
description: >-
Reported speech manifestations include dysarthria and aphasia; the HPO
dysarthria term captures one common neurologic speech pattern.
phenotype_term:
preferred_term: Dysarthria
term:
id: HP:0001260
label: Dysarthria
evidence:
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "speech disorder (n=91, 37%)"
explanation: >-
The 251-case synthesis supports speech disorder as a frequent
manifestation.
- reference: PMID:32921783
reference_title: "Hashimoto encephalopathy: a case report and a short revision of current literature."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "high-dose methyl-prednisolone was administered intravenously (1 g/day) for the first 3 days followed by oral prednisone for the following 30 days. The treatment induced a rapid disappearance of tremors and dysarthria"
explanation: >-
A pediatric case report documents dysarthria as a specific speech
manifestation responsive to immunotherapy.
- name: Myoclonus, Tremor, or Other Abnormal Movement
category: Neurological
frequency: OCCASIONAL
description: >-
Myoclonus, tremor, dystonia, and other abnormal movements occur in a
minority of adult cohorts and may be prominent in pediatric presentations.
phenotype_term:
preferred_term: Myoclonus
term:
id: HP:0001336
label: Myoclonus
evidence:
- reference: PMID:32921783
reference_title: "Hashimoto encephalopathy: a case report and a short revision of current literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Clinical presentation of HE varies from stroke-like signs, seizures including status epilepticus, amnesic syndrome, ataxia, myoclonus, cognitive impairment, and dementia to psychiatric manifestations"
explanation: >-
The review lists myoclonus among recognized clinical manifestations.
- reference: PMID:28784301
reference_title: "Hashimoto encephalopathy in pediatric patients: Homogeneity in clinical presentation and heterogeneity in antibody titers."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Presenting symptoms were seizures, altered consciousness, behavioral changes, psychosis, tremor, and dystonia."
explanation: >-
The pediatric series supports tremor and dystonia as movement
manifestations in children.
treatments:
- name: High-Dose Corticosteroids
description: >-
Corticosteroids are the usual first-line therapy for suspected SREAT after a
reasonable exclusion of infectious, toxic-metabolic, neoplastic,
neurodegenerative, psychiatric, and better-defined autoimmune encephalitis
mimics. Response rates are high in selected cohorts, but steroid response is
not universal and does not replace diagnostic rigor.
treatment_term:
preferred_term: systemic corticosteroid therapy
term:
id: NCIT:C122080
label: Systemic Corticosteroid Therapy
target_mechanisms:
- target: Steroid-Responsive CNS Neuroinflammation
treatment_effect: INHIBITS
description: >-
Glucocorticoids broadly suppress immune-mediated CNS inflammation and are
the core disease-directed treatment in correctly selected SREAT cases.
evidence:
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The first-line treatment was steroids in 193 patients"
explanation: >-
The 251-case synthesis supports steroids as the dominant first-line
treatment.
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Among the 12 patients who received corticosteroid, 9 (75%) had marked improvement"
explanation: >-
A modern cohort supports substantial corticosteroid responsiveness.
- reference: PMID:31882532
reference_title: Hashimoto encephalopathy in the 21st century.
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "Only 6 of 19 (31.6%) patients completely responded to steroids."
explanation: >-
This prospective clinical evaluation tempers older high-response reports
and supports modeling steroid response as frequent but not definitive.
- reference: DOI:10.1007/s13760-024-02520-1
reference_title: "Clinical and diagnostic characteristics of Hashimoto's encephalopathy: a single-center, retrospective study"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "When HE is suspected, steroids should be considered the first-line treatment."
explanation: >-
A 2024 retrospective study explicitly supports steroids as first-line
therapy.
- name: Intravenous Immunoglobulin for Steroid-Refractory or Pediatric Disease
description: >-
IVIG is used as an immunomodulatory escalation option when corticosteroids
are insufficient or contraindicated, including in pediatric series and
refractory cases.
treatment_term:
preferred_term: intravenous immunoglobulin therapy
term:
id: MAXO:0001480
label: immunoglobulin infusion therapy
target_mechanisms:
- target: Steroid-Responsive CNS Neuroinflammation
treatment_effect: INHIBITS
description: >-
IVIG may modulate pathogenic humoral and cellular immune activity in
steroid-refractory autoimmune encephalopathy presentations.
evidence:
- reference: PMID:28784301
reference_title: "Hashimoto encephalopathy in pediatric patients: Homogeneity in clinical presentation and heterogeneity in antibody titers."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "one improved with additional intravenous immunoglobulin"
explanation: >-
The pediatric case series documents clinical improvement with IVIG after
corticosteroids.
- reference: DOI:10.3390/biomedicines13030726
reference_title: "Hashimoto's Encephalopathy: Clinical Features, Therapeutic Strategies, and Rehabilitation Approaches"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "alternative immunosuppressive agents or intravenous immunoglobulin may be needed in some cases."
explanation: >-
A 2025 review supports IVIG as an alternative or escalation strategy.
- name: Plasma Exchange for Refractory Disease
description: >-
Therapeutic plasma exchange is an escalation option in steroid- and
IVIG-refractory SREAT, particularly when a humoral immune process is
suspected.
treatment_term:
preferred_term: plasmapheresis
term:
id: NCIT:C15304
label: Plasmapheresis
target_mechanisms:
- target: Antithyroid Antibody-Associated Autoimmune Context
treatment_effect: INHIBITS
description: >-
Plasma exchange can remove circulating autoantibodies and inflammatory
mediators, although thyroid antibody removal is not proven to be the
central therapeutic mechanism.
evidence:
- reference: PMID:28784301
reference_title: "Hashimoto encephalopathy in pediatric patients: Homogeneity in clinical presentation and heterogeneity in antibody titers."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The remaining patient did not respond to both treatments and normalized after plasmapheresis."
explanation: >-
The pediatric series documents plasmapheresis response after failure of
corticosteroids and IVIG.
- reference: PMID:32921783
reference_title: "Hashimoto encephalopathy: a case report and a short revision of current literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Plasmapheresis was successfully used in steroid non-responders and in case worsened after corticosteroids"
explanation: >-
The review supports plasma exchange as a refractory-disease option.
- name: Steroid-Sparing Immunosuppression
description: >-
Additional immunosuppressive agents such as azathioprine, cyclophosphamide,
mycophenolate mofetil, or methotrexate are reported in resistant or
relapsing disease, but comparative evidence and standardized regimens remain
limited.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
target_mechanisms:
- target: Steroid-Responsive CNS Neuroinflammation
treatment_effect: INHIBITS
description: >-
Steroid-sparing immunosuppressants are used to suppress ongoing immune
activation when corticosteroid tapering fails or relapses occur.
evidence:
- reference: PMID:32921783
reference_title: "Hashimoto encephalopathy: a case report and a short revision of current literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "In resistant cases of disease other immunosuppression therapies include plasma exchange, IVIG, methotrexate, azathioprine, cyclophosphamide, and mycophenolate mofetil."
explanation: >-
The review lists immunosuppressive options reported for resistant SREAT.
- reference: DOI:10.3390/biomedicines13030726
reference_title: "Hashimoto's Encephalopathy: Clinical Features, Therapeutic Strategies, and Rehabilitation Approaches"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Corticosteroids remain the cornerstone of treatment, although responses vary, and alternative immunosuppressive agents or intravenous immunoglobulin may be needed in some cases."
explanation: >-
A recent review supports steroid-sparing immunosuppression in selected
cases while emphasizing variable response.
diagnosis:
- name: Antithyroid antibody-positive encephalopathy workup
description: >-
Diagnosis requires unexplained encephalopathy with serum anti-TPO and/or
anti-thyroglobulin antibodies, negative or absent better-defined neuronal
antibody syndromes, and exclusion of infectious, toxic-metabolic,
neurodegenerative, functional, primary psychiatric, neoplastic, and
paraneoplastic mimics. Thyroid antibody positivity alone is not confirmatory.
markers: Serum anti-TPO antibodies, serum anti-thyroglobulin antibodies, negative neuronal antibody testing where available
results: Supports SREAT only when paired with objective neurologic/CNS evidence and exclusion of alternative diagnoses.
evidence:
- reference: PMID:34061124
reference_title: "Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "73% of the patients referred with suspected Hashimoto encephalopathy had an alternative non-immune-mediated diagnosis"
explanation: >-
The Mayo Clinic referral study supports diagnostic caution and broad
differential diagnosis.
- reference: PMID:26906964
reference_title: A clinical approach to diagnosis of autoimmune encephalitis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "we based the initial diagnostic approach on neurological assessment and conventional tests that are accessible to most clinicians."
explanation: >-
The canonical autoimmune encephalitis criteria paper supports a
syndrome-based diagnostic approach before antibody or treatment-response
results are available.
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The inclusion criteria were positive anti-thyroperoxidase (anti-TPO) or anti-thyroglobulin (anti-Tg) in serum with negative neuronal antibody in serum or cerebral spinal fluid (CSF)."
explanation: >-
A modern cohort operationalizes antibody-positive, neuronal-antibody
negative SREAT case selection.
- name: MRI, EEG, and CSF support objective CNS involvement
description: >-
MRI may be normal or nonspecific; EEG may show diffuse slowing or status
epilepticus; CSF may show inflammatory abnormalities or elevated protein.
These tests help separate autoimmune CNS disease from thyroid-antibody
positive mimics.
diagnosis_term:
preferred_term: electroencephalography
term:
id: MAXO:0000932
label: electroencephalography
markers: MRI abnormalities, abnormal EEG, inflammatory CSF findings, elevated CSF protein
results: Abnormal findings support autoimmune CNS involvement but are not individually specific for SREAT.
evidence:
- reference: PMID:34061124
reference_title: "Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Abnormal brain MRI (P = 0.003), abnormal EEG (P = 0.007) and CSF inflammatory findings (P = 0.002) were also more frequent in the autoimmune CNS patients."
explanation: >-
Objective CNS abnormalities distinguished autoimmune CNS cases from
alternative diagnoses in a thyroid-antibody-positive referral cohort.
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Electroencephalography findings were abnormal for 82% of patients, showing diffuse slowing consistent with encephalopathy (70%) or epileptic activity (14%)."
explanation: >-
The 251-case synthesis supports EEG abnormality as a common supportive
diagnostic finding.
differential_diagnoses:
- name: Non-autoimmune thyroid-antibody-positive brain dysfunction
description: >-
Patients with thyroid antibodies and cognitive, psychiatric, seizure, pain,
sleep, functional, or neurodegenerative presentations may be misclassified
as SREAT if objective CNS inflammation and careful exclusion are not
required.
distinguishing_features:
- >-
Alternative diagnoses in the Mayo Clinic referral cohort included functional
neurological disorder, neurodegenerative disorder, subjective cognitive
complaints, chronic pain syndrome, primary psychiatric disease, sleep
disorder, genetic/developmental conditions, and non-autoimmune seizure
disorders.
evidence:
- reference: PMID:34061124
reference_title: "Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Diagnoses among the remaining 105 patients (73%) were functional neurological disorder (n = 20), neurodegenerative disorder (n = 18), subjective cognitive complaints (n = 14), chronic pain syndrome (n = 12), primary psychiatric (n = 11), sleep disorder (n = 10), genetic/developmental (n = 8), non-autoimmune seizure disorders (n = 2) and other (n = 10)."
explanation: >-
This directly enumerates major SREAT mimics among thyroid-antibody-positive
referrals.
datasets: []
references:
- reference: DOI:10.1093/braincomms/fcaa233
title: "Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis."
found_in:
- Hashimoto_Encephalopathy-deep-research-falcon.md
findings:
- statement: Thyroid antibodies are insufficient to diagnose autoimmune encephalopathy without objective CNS evidence.
supporting_text: >-
Thyroid antibody prevalence is high in the general population, and does
not support a diagnosis of autoimmune encephalopathy in the absence of
objective neurological and CNS-specific immunological abnormalities.
evidence:
- reference: PMID:34061124
reference_title: "Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Thyroid antibody prevalence is high in the general population, and does not support a diagnosis of autoimmune encephalopathy in the absence of objective neurological and CNS-specific immunological abnormalities."
explanation: >-
This is a key contemporary caution against thyroid-antibody-driven
overdiagnosis.
- reference: PMID:26906964
title: A clinical approach to diagnosis of autoimmune encephalitis.
found_in:
- Hashimoto_Encephalopathy-deep-research-falcon.md
findings:
- statement: Autoimmune encephalitis diagnosis should use syndrome-based differential diagnosis rather than waiting for antibody or treatment response results.
supporting_text: >-
Because autoantibody test results and response to therapy are not
available at disease onset, the diagnostic approach is based on
neurologic assessment and conventional tests.
evidence:
- reference: PMID:26906964
reference_title: A clinical approach to diagnosis of autoimmune encephalitis.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "we based the initial diagnostic approach on neurological assessment and conventional tests that are accessible to most clinicians."
explanation: >-
This supports using a structured autoimmune encephalitis workup before
labeling SREAT.
- reference: DOI:10.1016/j.autrev.2016.09.008
title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
found_in:
- Hashimoto_Encephalopathy-deep-research-falcon.md
findings:
- statement: The 251-case literature synthesis defines SREAT and reports common symptom frequencies and steroid responsiveness.
supporting_text: >-
Patients presented with convulsions, confusion, speech disorder, memory
impairment, gait disturbance, persecutory delusions, and high response
rates after treatment.
evidence:
- reference: PMID:27639840
reference_title: "Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: 91% of patients showed complete or partial neurological response
explanation: >-
This landmark synthesis supports high but not universal treatment
responsiveness.
- reference: DOI:10.1007/s11910-023-01255-5
title: "Hashimoto's Encephalopathy: Case Series and Literature Review."
found_in:
- Hashimoto_Encephalopathy-deep-research-falcon.md
findings:
- statement: Hashimoto encephalopathy pathogenesis is uncertain, and diagnosis requires exclusion of better-defined autoimmune and paraneoplastic encephalitides.
supporting_text: >-
The review states that available evidence points to autoimmune etiology
due to vasculitis or inflammatory processes, but thyroid antibody
pathogenicity is unclear.
evidence:
- reference: PMID:36853554
reference_title: "Hashimoto's Encephalopathy: Case Series and Literature Review."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Diagnosis requires the exclusion of other causes of encephalopathies and encephalitis including autoimmune encephalitis associated with neuronal surface antibodies and paraneoplastic ones."
explanation: >-
This supports the differential-diagnosis and exclusion requirement.
- reference: DOI:10.1186/s12883-023-03305-4
title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
found_in:
- Hashimoto_Encephalopathy-deep-research-falcon.md
findings:
- statement: Modern tertiary-center cases commonly have cognitive impairment, neuropsychiatric symptoms, seizures, ataxia, and sleep disturbance, and most steroid-treated patients improve.
supporting_text: >-
The Siriraj cohort found cognitive impairment, neuropsychiatric symptoms,
seizure, ataxia, and sleep disturbance to be common manifestations.
evidence:
- reference: DOI:10.1186/s12883-023-03305-4
reference_title: Clinical presentations and treatment outcomes of Hashimoto encephalopathy at Siriraj Hospital
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The results of this study revealed cognitive impairment, neuropsychiatric symptoms, seizure, ataxia, and sleep disturbance to be common manifestations of Hashimoto encephalopathy."
explanation: >-
This contemporary cohort supports the main phenotype set curated here.
- reference: DOI:10.1007/s13760-024-02520-1
title: "Clinical and diagnostic characteristics of Hashimoto's encephalopathy: a single-center, retrospective study"
found_in:
- Hashimoto_Encephalopathy-deep-research-falcon.md
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: A 2024 retrospective study supports early steroid treatment and recognizes nonconvulsive status epilepticus as an important presentation.
supporting_text: >-
Nineteen of 21 immunosuppressant-treated probable HE patients had good
outcomes, and steroids were recommended as first-line treatment when HE is
suspected.
evidence:
- reference: DOI:10.1007/s13760-024-02520-1
reference_title: "Clinical and diagnostic characteristics of Hashimoto's encephalopathy: a single-center, retrospective study"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Nineteen of 21 patients (90.5%) treated with immunosuppressants showed good outcomes."
explanation: >-
This supports benefit from immunosuppressive therapy in selected
probable HE cases.
- reference: DOI:10.3390/ijms25137101
title: "Difficulties in the Diagnostics and Treatment of Hashimoto's Encephalopathy"
found_in:
- Hashimoto_Encephalopathy-deep-research-falcon.md
findings:
- statement: A 2024 systematic critical review found no specific marker, limited glucocorticoid effectiveness, and substantial relapse.
supporting_text: >-
The review concluded negative anti-TPO may help rule out HE, but positive
anti-TPO cannot confirm it, and anti-NAE is nonspecific.
evidence:
- reference: DOI:10.3390/ijms25137101
reference_title: "Difficulties in the Diagnostics and Treatment of Hashimoto's Encephalopathy"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "there is no specific HE marker."
explanation: >-
This supports caution around antithyroid and anti-NAE biomarkers.
- reference: DOI:10.3390/biomedicines13030726
title: "Hashimoto's Encephalopathy: Clinical Features, Therapeutic Strategies, and Rehabilitation Approaches"
found_in:
- Hashimoto_Encephalopathy-deep-research-falcon.md
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Corticosteroids remain cornerstone therapy, but responses vary and some cases need IVIG or other immunosuppression.
supporting_text: >-
The review synthesizes SREAT clinical, laboratory, radiological, and
therapeutic literature, emphasizing variable treatment response.
evidence:
- reference: DOI:10.3390/biomedicines13030726
reference_title: "Hashimoto's Encephalopathy: Clinical Features, Therapeutic Strategies, and Rehabilitation Approaches"
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Corticosteroids remain the cornerstone of treatment, although responses vary, and alternative immunosuppressive agents or intravenous immunoglobulin may be needed in some cases."
explanation: >-
This supports the treatment model of first-line steroids with escalation
in selected cases.
- reference: PMID:31525528
title: "Serial brain MRI changes related to autoimmune pathophysiology in Hashimoto encephalopathy with anti-NAE antibodies: A case-series study."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: MRI lesions in anti-NAE-positive Hashimoto encephalopathy can fluctuate with disease activity.
supporting_text: >-
MRI lesions that fluctuate according to disease condition were frequently
observed in anti-NAE-positive patients.
evidence:
- reference: PMID:31525528
reference_title: "Serial brain MRI changes related to autoimmune pathophysiology in Hashimoto encephalopathy with anti-NAE antibodies: A case-series study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "MRI lesions that fluctuate according to the disease condition were frequently observed in HE patients with anti-NAE antibodies"
explanation: >-
This supports the OpenScientist-cited anti-NAE MRI phenotype and the
provisional subtype mechanism.
- reference: PMID:38861245
title: "Clinical and diagnostic characteristics of Hashimoto's encephalopathy: a single-center, retrospective study."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: A 2024 retrospective cohort reported NCSE and favorable outcomes with immunosuppressive treatment.
supporting_text: >-
Nonconvulsive status epilepticus was observed in six patients, and most
immunosuppressant-treated patients had good outcomes.
evidence:
- reference: PMID:38861245
reference_title: "Clinical and diagnostic characteristics of Hashimoto's encephalopathy: a single-center, retrospective study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Nonconvulsive status epilepticus on EEG was observed in six patients, all of whom were intractable to antiepileptic drugs."
explanation: >-
This captures the OpenScientist-cited NCSE presentation in a modern
probable HE cohort.
- reference: PMID:40149702
title: "Hashimoto's Encephalopathy: Clinical Features, Therapeutic Strategies, and Rehabilitation Approaches."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: A 2025 review cautions that TPO antibodies are unlikely to be directly causal in HE.
supporting_text: >-
Elevated TPO antibodies may indicate a general autoimmune state rather
than a direct causal relationship with HE.
evidence:
- reference: PMID:40149702
reference_title: "Hashimoto's Encephalopathy: Clinical Features, Therapeutic Strategies, and Rehabilitation Approaches."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "While elevated TPO antibodies are frequently observed, a direct causal relationship with HE is unlikely, and their presence may indicate a general state of autoimmunity."
explanation: >-
This supports the conservative diagnostic framing used in this curation.
- reference: PMID:10536782
title: The natural history of the obese strain of chickens--an animal model for spontaneous autoimmune thyroiditis.
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:11862410
title: Analysis of genetic regulation of chicken spontaneous autoimmune thyroiditis, an animal model of human Hashimoto's thyroiditis.
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:11937583
title: A role for IL-15 in driving the onset of spontaneous autoimmune thyroiditis?
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:19363998
title: "[Anti-NAE autoantibodies and clinical spectrum in Hashimoto's encephalopathy]."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Anti-NAE autoantibodies were positive in 44% of patients with HE.
supporting_text: Anti-NAE autoantibodies were positive in 44% of patients with HE.
evidence:
- reference: PMID:19363998
reference_title: "[Anti-NAE autoantibodies and clinical spectrum in Hashimoto's encephalopathy]."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: Anti-NAE autoantibodies were positive in 44% of patients with HE.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:21234711
title: 'Cutting edge: the etiology of autoimmune thyroid diseases.'
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Autoimmune thyroid disease susceptibility involves immune-regulatory and thyroid-specific genes interacting with environmental factors.
supporting_text: >-
Non-MHC genes that confer susceptibility to AITD can be classified into
immune-regulatory and thyroid-specific groups, and these genes interact
with environmental factors.
evidence:
- reference: PMID:21234711
reference_title: 'Cutting edge: the etiology of autoimmune thyroid diseases.'
supports: SUPPORT
evidence_source: OTHER
snippet: "These genes interact with environmental factors, such as infection, likely through epigenetic mechanisms to trigger disease."
explanation: >-
This review is relevant only as broad autoimmune-thyroid-disease
context, not as direct SREAT pathophysiology evidence.
- reference: PMID:22735372
title: '[The role of hereditary and environmental factors in autoimmune thyroid diseases].'
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Autoimmune thyroid diseases are the most common organ-specific autoimmune disorders affecting 5% to 10% of the population in Western countries.
supporting_text: Autoimmune thyroid diseases are the most common organ-specific autoimmune disorders affecting 5% to 10% of the population in Western countries.
evidence:
- reference: PMID:22735372
reference_title: '[The role of hereditary and environmental factors in autoimmune thyroid diseases].'
supports: SUPPORT
evidence_source: OTHER
snippet: Autoimmune thyroid diseases are the most common organ-specific autoimmune disorders affecting 5% to 10% of the population in Western countries.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:23568984
title: "[Hashimoto's encephalopathy and autoantibodies]."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Hashimoto's encephalopathy (HE) has been recognized as a new clinical disease based on an autoimmune mechanism associated with Hashimoto's thyroiditis.
supporting_text: Hashimoto's encephalopathy (HE) has been recognized as a new clinical disease based on an autoimmune mechanism associated with Hashimoto's thyroiditis.
evidence:
- reference: PMID:23568984
reference_title: "[Hashimoto's encephalopathy and autoantibodies]."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: Hashimoto's encephalopathy (HE) has been recognized as a new clinical disease based on an autoimmune mechanism associated with Hashimoto's thyroiditis.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:23777101
title: "[The biomarker and treatment in Hashimoto's encephalopahty]."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Hashimoto's encephalopathy (HE) is a treatable disease based on autoimmune mechanisms associated with Hashimoto's thyroiditis.
supporting_text: Hashimoto's encephalopathy (HE) is a treatable disease based on autoimmune mechanisms associated with Hashimoto's thyroiditis.
evidence:
- reference: PMID:23777101
reference_title: "[The biomarker and treatment in Hashimoto's encephalopahty]."
supports: SUPPORT
evidence_source: OTHER
snippet: Hashimoto's encephalopathy (HE) is a treatable disease based on autoimmune mechanisms associated with Hashimoto's thyroiditis.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:24460189
title: 'Mechanisms of autoimmune thyroid diseases: from genetics to epigenetics.'
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:24609834
title: 'Mechanisms in endocrinology: autoimmune thyroid disease: old and new players.'
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:24633901
title: Tic disorder probably associated with steroid responsive encephalopathy with autoimmune thyroiditis (SREAT).
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:26167010
title: 'Hashimoto encephalopathy: A study of the clinical profile, radiological and electrophysiological correlation in a Tertiary Care Center in South India.'
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Hashimoto encephalopathy (HE) is a poorly understood and often misdiagnosed entity with variable clinical spectrum.
supporting_text: Hashimoto encephalopathy (HE) is a poorly understood and often misdiagnosed entity with variable clinical spectrum.
evidence:
- reference: PMID:26167010
reference_title: 'Hashimoto encephalopathy: A study of the clinical profile, radiological and electrophysiological correlation in a Tertiary Care Center in South India.'
supports: SUPPORT
evidence_source: OTHER
snippet: Hashimoto encephalopathy (HE) is a poorly understood and often misdiagnosed entity with variable clinical spectrum.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:26235382
title: 'Immunogenetics of autoimmune thyroid diseases: A comprehensive review.'
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:27790384
title: "Prominent Bilateral Hand Tremor in Hashimoto's Encephalopathy: A Video Demonstration."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Hashimoto's encephalopathy often presents with neuropsychiatric manifestations including seizures and movement disorders.
supporting_text: Hashimoto's encephalopathy often presents with neuropsychiatric manifestations including seizures and movement disorders.
evidence:
- reference: PMID:27790384
reference_title: "Prominent Bilateral Hand Tremor in Hashimoto's Encephalopathy: A Video Demonstration."
supports: SUPPORT
evidence_source: OTHER
snippet: Hashimoto's encephalopathy often presents with neuropsychiatric manifestations including seizures and movement disorders.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:31882532
title: Hashimoto encephalopathy in the 21st century.
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Pretreatment HE criteria do not reliably predict complete steroid responsiveness.
supporting_text: Only 6 of 19 patients completely responded to steroids.
evidence:
- reference: PMID:31882532
reference_title: Hashimoto encephalopathy in the 21st century.
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Only 6 of 19 (31.6%) patients completely responded to steroids."
explanation: >-
This clinical evaluation is a key counterweight to older reports of
near-universal steroid responsiveness.
- reference: PMID:32916160
title: Dysregulation of non-coding RNAs in autoimmune thyroid disease.
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:35946002
title: Orthostatic Myoclonic Jerks in a Case of Hashimoto's Encephalopathy.
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:36081870
title: "Hashimoto's encephalopathy with cerebellar ataxia as the main symptom: A case report and literature review."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:36420742
title: DNA Methylation in Autoimmune Thyroid Disease.
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:36809420
title: 'MRI and steroid-responsive encephalopathy associated with autoimmune thyroiditis: first report of conus medullaris involvement and literature review of the known neuroimaging profiles.'
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT) is a rare but potentially reversible autoimmune encephalopathy.
supporting_text: Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT) is a rare but potentially reversible autoimmune encephalopathy.
evidence:
- reference: PMID:36809420
reference_title: 'MRI and steroid-responsive encephalopathy associated with autoimmune thyroiditis: first report of conus medullaris involvement and literature review of the known neuroimaging profiles.'
supports: SUPPORT
evidence_source: OTHER
snippet: Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT) is a rare but potentially reversible autoimmune encephalopathy.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:37745658
title: "The use of intravenous immunoglobulin in the treatment of Hashimoto's encephalopathy: case based review."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Hashimoto's encephalopathy (HE) is a controversial immunological neuropsychiatric disease, with a poorly understood pathogenesis.
supporting_text: Hashimoto's encephalopathy (HE) is a controversial immunological neuropsychiatric disease, with a poorly understood pathogenesis.
evidence:
- reference: PMID:37745658
reference_title: "The use of intravenous immunoglobulin in the treatment of Hashimoto's encephalopathy: case based review."
supports: SUPPORT
evidence_source: OTHER
snippet: Hashimoto's encephalopathy (HE) is a controversial immunological neuropsychiatric disease, with a poorly understood pathogenesis.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:38085696
title: 'Hashimoto Encephalopathy Presenting with Acute Psychosis and Inappropriate Secretion of Antidiuretic Hormone: A Rare Case Responding to Steroid Therapy.'
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:39000209
title: Difficulties in the Diagnostics and Treatment of Hashimoto's Encephalopathy-A Systematic and Critical Review.
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
- reference: PMID:40323355
title: "New onset steroid-responsive Hashimoto's encephalopathy in the older population: a scoping review."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Hashimoto's encephalopathy (HE) is a rare autoimmune disorder which can mimic late-life neuropsychiatric symptoms as part of a dementia syndrome.
supporting_text: Hashimoto's encephalopathy (HE) is a rare autoimmune disorder which can mimic late-life neuropsychiatric symptoms as part of a dementia syndrome.
evidence:
- reference: PMID:40323355
reference_title: "New onset steroid-responsive Hashimoto's encephalopathy in the older population: a scoping review."
supports: SUPPORT
evidence_source: OTHER
snippet: Hashimoto's encephalopathy (HE) is a rare autoimmune disorder which can mimic late-life neuropsychiatric symptoms as part of a dementia syndrome.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:41731401
title: "Recurrent steroid-intolerant Hashimoto's encephalopathy responsive to single-dose neonatal Fc receptor antagonist: a case report and literature review."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Hashimoto’s encephalopathy (HE) is a rare, underdiagnosed, steroid-responsive autoimmune condition associated with thyroid autoimmunity.
supporting_text: Hashimoto’s encephalopathy (HE) is a rare, underdiagnosed, steroid-responsive autoimmune condition associated with thyroid autoimmunity.
evidence:
- reference: PMID:41731401
reference_title: "Recurrent steroid-intolerant Hashimoto's encephalopathy responsive to single-dose neonatal Fc receptor antagonist: a case report and literature review."
supports: SUPPORT
evidence_source: OTHER
snippet: Hashimoto’s encephalopathy (HE) is a rare, underdiagnosed, steroid-responsive autoimmune condition associated with thyroid autoimmunity.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:41782877
title: 'HMGB1 dysregulation: a neuroimmune bridge to cognitive impairment in autoimmune thyroiditis.'
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
findings:
- statement: Cognitive and affective disturbances are frequent extra-thyroidal manifestations of Hashimoto's thyroiditis (HT), even in euthyroid patients, with severe cases progressing to Hashimoto's encephalopathy.
supporting_text: Cognitive and affective disturbances are frequent extra-thyroidal manifestations of Hashimoto's thyroiditis (HT), even in euthyroid patients, with severe cases progressing to Hashimoto's encephalopathy.
evidence:
- reference: PMID:41782877
reference_title: 'HMGB1 dysregulation: a neuroimmune bridge to cognitive impairment in autoimmune thyroiditis.'
supports: SUPPORT
evidence_source: OTHER
snippet: Cognitive and affective disturbances are frequent extra-thyroidal manifestations of Hashimoto's thyroiditis (HT), even in euthyroid patients, with severe cases progressing to Hashimoto's encephalopathy.
explanation: Deep research cited this publication as relevant literature for Hashimoto Encephalopathy.
- reference: PMID:41883393
title: "Creutzfeldt-Jakob disease mimicking Hashimoto's encephalopathy: steroid response followed by decline."
found_in:
- Hashimoto_Encephalopathy-deep-research-openscientist.md
notes: >-
Curated as an acquired diagnosis-of-exclusion autoimmune encephalopathy.
Antithyroid antibodies and anti-NAE antibodies are represented conservatively:
useful in case definition or subtype discussion, but not sufficient evidence
of direct CNS pathogenicity.
References & Deep Research
References
38Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Deep Research
2Question: You are an expert researcher providing comprehensive, well-cited information.
Provide detailed information focusing on: 1. Key concepts and definitions with current understanding 2. Recent developments and latest research (prioritize 2023-2024 sources) 3. Current applications and real-world implementations 4. Expert opinions and analysis from authoritative sources 5. Relevant statistics and data from recent studies
Format as a comprehensive research report with proper citations. Include URLs and publication dates where available. Always prioritize recent, authoritative sources and provide specific citations for all major claims.
Disease Characteristics Research Template
Target Disease
- Disease Name: Hashimoto Encephalopathy
- MONDO ID: (if available)
- Category: Autoimmune
Research Objectives
Please provide a comprehensive research report on Hashimoto Encephalopathy covering all of the disease characteristics listed below. This report will be used to populate a disease knowledge base entry. Be thorough and cite primary literature (PMID preferred) for all claims.
For each section, suggested databases/resources are listed. These are the first places you should search for information on each topic.
1. Disease Information
Search first: OMIM, Orphanet, ICD-10/ICD-11, MeSH, PubMed
- What is the disease? Provide a concise overview.
- What are the key identifiers? (OMIM, Orphanet, ICD-10/ICD-11, MeSH, Mondo)
- What are the common synonyms and alternative names?
- Is the information derived from individual patients (e.g., EHR) or aggregated disease-level resources?
2. Etiology
- Disease Causal Factors: What are the primary causes? (genetic, environmental, infectious, mechanistic)
- Risk Factors:
Search first: PubMed, Cochrane Library, UpToDate, clinical guidelines, ClinVar, ClinGen, GWAS Catalog, PheGenI, CTD, CDC, WHO, epidemiological databases
- Genetic risk factors (causal variants, susceptibility loci, modifier genes)
- Environmental risk factors (toxins, lifestyle, occupational exposures, age, sex, family history)
- Protective Factors:
Search first: PubMed, Cochrane Library, clinical trial databases, GWAS Catalog, gnomAD, WHO, CDC, nutrition databases
- Genetic protective factors (protective variants, modifier alleles)
- Environmental protective factors (diet, lifestyle, exposures that reduce risk)
- Gene-Environment Interactions: How do genetic and environmental factors interact to influence disease?
Search first: CTD, PubMed, PheGenI, GxE databases
3. Phenotypes
Search first: HPO (Human Phenotype Ontology), OMIM, Orphanet, PubMed, clinicaltrials.gov, MedDRA, SNOMED CT, DECIPHER, LOINC
For each phenotype, provide: - Phenotype type: symptoms, clinical signs, physical manifestations, behavioral changes, or laboratory abnormalities
For symptoms/signs: HPO, OMIM, Orphanet, PubMed For behavioral changes: HPO, DSM, RDoC (Research Domain Criteria), PubMed For laboratory abnormalities: LOINC, SNOMED CT, LabTests Online, PubMed - Phenotype characteristics: Search first: OMIM, Orphanet, HPO, PubMed - Age of symptom onset (neonatal, childhood, adult-onset, late-onset) - Symptom severity (mild, moderate, severe, variable) - Symptom progression (stable, progressive, episodic, fluctuating) - Frequency among affected individuals (percentage or qualitative) - Quality of life impact: Effects on daily functioning and well-being (per-phenotype when possible) Search first: EQ-5D database, SF-36, WHO QOL databases, PubMed - Suggest HPO (Human Phenotype Ontology) terms for each phenotype
4. Genetic/Molecular Information
- Causal Genes: Gene mutations or chromosomal abnormalities responsible for disease (gene symbols, OMIM IDs)
Search first: OMIM, ClinVar, HGMD, Ensembl, NCBI Gene
- Pathogenic Variants:
- Affected genes (gene symbols, HGNC IDs) > Search first: OMIM, NCBI Gene, Ensembl, HGNC, UniProt, GeneCards
- Variant classification (pathogenic, likely pathogenic, VUS per ACMG/AMP guidelines) > Search first: ClinVar, ClinGen, ACMG/AMP guidelines, VarSome
- Variant type/class (missense, frameshift, nonsense, splice-site, structural)
- Allele frequency in population databases > Search first: gnomAD, 1000 Genomes, ExAC, TOPMed, dbSNP
- Somatic vs germline origin > Search first: COSMIC (somatic), ClinVar, ICGC, TCGA
- Functional consequences (loss of function, gain of function, dominant negative)
- Modifier Genes: Genes that modify disease severity or expression
- Epigenetic Information: DNA methylation, histone modifications, chromatin changes affecting disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Chromosomal Abnormalities: Large-scale genetic changes (aneuploidy, translocations, inversions)
Search first: DECIPHER, ClinVar, ECARUCA, UCSC Genome Browser
5. Environmental Information
- Environmental Factors: Non-genetic contributing factors (toxins, radiation, pollution, occupational exposure)
Search first: CTD (Comparative Toxicogenomics Database), TOXNET, PubMed, EPA databases
- Lifestyle Factors: Behavioral factors (smoking, diet, exercise, alcohol consumption)
Search first: CDC databases, WHO, PubMed, NHANES
- Infectious Agents: If applicable, pathogens causing or triggering disease (bacteria, viruses, fungi, parasites)
Search first: NCBI Taxonomy, ViPR, BV-BRC, MicrobeDB, GIDEON
6. Mechanism / Pathophysiology
- Molecular Pathways: Specific signaling cascades or biochemical pathways involved (Wnt, MAPK, mTOR, PI3K-AKT, etc.)
Search first: KEGG, Reactome, WikiPathways, PathBank, BioCyc
- Cellular Processes: Cell-level mechanisms (apoptosis, autophagy, cell cycle dysregulation, inflammation, etc.)
Search first: Gene Ontology (GO), Reactome, KEGG, PubMed
- Protein Dysfunction: How protein structure or function is altered (misfolding, aggregation, loss of function, gain of function)
Search first: UniProt, PDB (Protein Data Bank), InterPro, Pfam, AlphaFold
- Metabolic Changes: Alterations in metabolic processes (energy metabolism, lipid metabolism, amino acid metabolism)
Search first: KEGG, BioCyc, HMDB (Human Metabolome Database), BRENDA
- Immune System Involvement: Role of immune response (autoimmunity, immunodeficiency, chronic inflammation)
Search first: ImmPort, Immunome Database, IEDB, Gene Ontology
- Tissue Damage Mechanisms: How tissues/ are injured (oxidative stress, ischemia, fibrosis, necrosis)
Search first: PubMed, Gene Ontology, Reactome
- Biochemical Abnormalities: Specific molecular defects (enzyme deficiencies, receptor dysfunction, ion channel defects)
Search first: BRENDA, UniProt, KEGG, OMIM, PubMed
- Epigenetic Changes: DNA methylation, histone modifications affecting gene expression in disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Molecular Profiling (if available):
- Transcriptomics/gene expression changes > Search first: GEO (Gene Expression Omnibus), ArrayExpress, GTEx, Human Cell Atlas, SRA
- Proteomics findings > Search first: PRIDE, ProteomeXchange, Human Protein Atlas, STRING, BioGRID
- Metabolomics signatures > Search first: MetaboLights, Metabolomics Workbench, HMDB, METLIN
- Lipidomics alterations > Search first: LIPID MAPS, SwissLipids, LipidHome, Metabolomics Workbench
- Genomic structural features > Search first: UCSC Genome Browser, Ensembl, NCBI, dbVar, DGV
- Advanced Technologies (if applicable):
- Single-cell analysis findings (cell-type specific mechanisms, cellular heterogeneity) > Search first: Human Cell Atlas, Single Cell Portal, GEO, CELLxGENE
- Spatial transcriptomics findings > Search first: GEO, Spatial Research, Vizgen, 10x Genomics data
- Multi-omics integration results > Search first: TCGA, ICGC, cBioPortal, LinkedOmics, PubMed
- Functional genomics screens (CRISPR, RNAi) > Search first: DepMap, GenomeRNAi, PubMed, BioGRID ORCS
For each mechanism, describe: - The causal chain from initial trigger to clinical manifestation - Which mechanisms are upstream vs downstream - What cell types and biological processes are involved - Suggest GO terms for biological processes and CL terms for cell types
7. Anatomical Structures Affected
- Organ Level:
- Primary organs directly affected
- Secondary organ involvement (complications, secondary effects)
- Body systems involved (cardiovascular, nervous, digestive, respiratory, endocrine, etc.)
Search first: Uberon, FMA (Foundational Model of Anatomy), OMIM, HPO, ICD-11, MeSH, SNOMED CT
- Tissue and Cell Level:
- Specific tissue types affected (epithelial, connective, muscle, nervous)
- Specific cell populations targeted (with Cell Ontology terms)
Search first: Uberon, Human Protein Atlas, Cell Ontology, Human Cell Atlas, CellMarker, PanglaoDB
- Subcellular Level:
- Cellular compartments involved (mitochondria, nucleus, ER, lysosomes) (with GO Cellular Component terms)
Search first: Gene Ontology (Cellular Component), UniProt, Human Protein Atlas
- Localization:
- Specific anatomical sites (with UBERON terms) > Search first: FMA, Uberon, NeuroNames (for brain), SNOMED CT
- Lateralization (unilateral, bilateral, asymmetric) > Search first: HPO, clinical literature, imaging databases
8. Temporal Development
- Onset:
- Typical age of onset (congenital, pediatric, adult, geriatric)
- Onset pattern (acute, subacute, chronic, insidious)
Search first: OMIM, Orphanet, HPO, PubMed
- Progression:
- Disease stages (early, intermediate, advanced, end-stage) > Search first: Cancer Staging Manual (AJCC), WHO classifications, PubMed
- Progression rate (rapid, slow, variable)
- Disease course pattern (episodic, relapsing-remitting, progressive, stable)
- Disease duration (self-limited, chronic lifelong)
Search first: Disease registries, longitudinal cohort databases, natural history studies, PubMed, Orphanet, OMIM
- Patterns:
- Remission patterns (spontaneous, treatment-induced) > Search first: Clinical trial databases, disease registries, PubMed
- Critical periods (time windows of vulnerability or opportunity for intervention) > Search first: PubMed, developmental biology databases, clinical guidelines
9. Inheritance and Population
- Epidemiology:
- Prevalence (cases per 100,000 at given time)
- Incidence (new cases per 100,000 per year)
Search first: Orphanet, CDC, WHO, GBD (Global Burden of Disease), national registries, SEER, disease registries
- For Genetic Etiology:
- Inheritance pattern (AD, AR, X-linked, mitochondrial, multifactorial, polygenic) > Search first: OMIM, Orphanet, ClinVar, GTR (Genetic Testing Registry)
- Penetrance (complete, incomplete, age-dependent) > Search first: ClinVar, OMIM, PubMed, ClinGen
- Expressivity (variable, consistent) > Search first: OMIM, ClinVar, PubMed
- Genetic anticipation (increasing severity in successive generations) > Search first: OMIM, PubMed (especially for repeat expansion disorders)
- Germline mosaicism > Search first: ClinVar, OMIM, genetic counseling literature, PubMed
- Founder effects (population-specific mutations) > Search first: gnomAD, population genetics databases, PubMed
- Consanguinity role > Search first: OMIM, population studies, genetic counseling resources
- Carrier frequency > Search first: gnomAD, carrier screening databases, GeneReviews, GTR
- Population Demographics:
- Affected populations (ethnic or demographic groups with higher prevalence) > Search first: gnomAD, 1000 Genomes, PAGE Study, PubMed, population registries
- Geographic distribution (endemic areas, regional variation) > Search first: WHO, CDC, GBD, Orphanet, geographic epidemiology databases
- Geographic distribution of specific variants
- Sex ratio (male:female) > Search first: Disease registries, OMIM, PubMed, epidemiological databases
- Age distribution of affected individuals > Search first: CDC, disease registries, SEER, Orphanet
10. Diagnostics
- Clinical Tests:
- Laboratory tests (blood, urine, tissue chemistry, specific enzyme assays) > Search first: LOINC, LabTests Online, PubMed
- Biomarkers (proteins, metabolites, genetic markers, circulating biomarkers) > Search first: FDA Biomarker List, BEST (Biomarkers, EndpointS, and other Tools), PubMed
- Imaging studies (X-ray, CT, MRI, PET, ultrasound) > Search first: RadLex, DICOM, Radiopaedia, imaging databases
- Functional tests (pulmonary function, cardiac stress tests) > Search first: LOINC, clinical guidelines, PubMed
- Electrophysiology (EEG, EMG, ECG, nerve conduction studies) > Search first: LOINC, clinical neurophysiology databases, PubMed
- Biopsy findings (histopathology, immunohistochemistry) > Search first: SNOMED CT, College of American Pathologists resources, PubMed
- Pathology findings (microscopic examination) > Search first: SNOMED CT, Digital Pathology databases, PubMed
- Genetic Testing:
Search first: GTR (Genetic Testing Registry), GeneReviews, ClinGen
- Overview of recommended genetic testing approach
- Whole genome sequencing (WGS) utility > Search first: GTR, ClinVar, GEL (Genomics England), gnomAD
- Whole exome sequencing (WES) utility > Search first: GTR, ClinVar, OMIM, GeneMatcher
- Gene panels (which panels, which genes) > Search first: GTR, ClinVar, laboratory-specific databases
- Single gene testing > Search first: GTR, ClinVar, OMIM, GeneReviews
- Chromosomal microarray (CMA) > Search first: DECIPHER, ClinVar, dbVar, ECARUCA
- Karyotyping > Search first: Chromosome Abnormality Database, ClinVar, cytogenetics resources
- FISH > Search first: ClinVar, cytogenetics databases, PubMed
- Mitochondrial DNA testing > Search first: MITOMAP, MSeqDR, ClinVar, GTR
- Repeat expansion testing > Search first: GTR, ClinVar, repeat expansion databases, PubMed
- Omics-Based Diagnostics (if applicable):
- RNA sequencing / transcriptomics > Search first: GEO, ArrayExpress, GTEx, RNA-seq databases
- Proteomics > Search first: PRIDE, ProteomeXchange, FDA Biomarker database
- Metabolomics > Search first: MetaboLights, Metabolomics Workbench, HMDB
- Epigenomics > Search first: GEO, ENCODE, Roadmap Epigenomics, MethBase
- Liquid biopsy > Search first: COSMIC, ClinVar, liquid biopsy databases, PubMed
- Clinical Criteria:
- Standardized diagnostic criteria (DSM, ICD, society guidelines) > Search first: DSM-5, ICD-11, clinical society guidelines, UpToDate
- Differential diagnosis (other conditions to rule out, with distinguishing features) > Search first: DynaMed, UpToDate, clinical decision support systems
- Screening:
- Screening methods for asymptomatic individuals (newborn screening, carrier screening, cascade screening) > Search first: ACMG recommendations, CDC newborn screening, GTR
11. Outcome/Prognosis
- Survival and Mortality:
- Survival rate (5-year, 10-year, overall) > Search first: SEER, cancer registries, disease-specific registries, PubMed
- Life expectancy (with and without treatment if applicable) > Search first: Orphanet, disease registries, actuarial databases, PubMed
- Mortality rate > Search first: CDC, WHO, GBD, national mortality databases
- Disease-specific mortality (deaths directly attributable to disease) > Search first: Disease registries, CDC Wonder, GBD, PubMed
- Morbidity and Function:
- Morbidity (disease-related disability and health impacts) > Search first: GBD, WHO, disability databases, PubMed
- Disability outcomes (long-term functional impairments) > Search first: ICF (International Classification of Functioning), disability registries
- Quality of life measures (EQ-5D, SF-36, PROMIS, disease-specific tools) > Search first: EQ-5D database, SF-36, PROMIS, PubMed
- Disease Course:
- Complications (secondary problems: infections, organ failure, etc.) > Search first: ICD codes, disease registries, clinical databases, PubMed
- Recovery potential (likelihood and extent of recovery, with vs without treatment) > Search first: Natural history studies, rehabilitation databases, PubMed
- Prediction:
- Prognostic factors (age, disease severity, biomarkers, treatment response) > Search first: Prognostic models databases, clinical calculators, PubMed
- Prognostic biomarkers (molecular markers predicting disease course) > Search first: FDA Biomarker database, PubMed, cancer prognostic databases
12. Treatment
- Pharmacotherapy:
- Pharmacological treatments (drug names, drug classes, mechanisms of action) > Search first: DrugBank, RxNorm, ATC classification, DailyMed, FDA databases
- Pharmacogenomics (how genetic variants affect drug metabolism, efficacy, toxicity) > Search first: PharmGKB, CPIC (Clinical Pharmacogenetics), FDA Table of PGx Biomarkers
- Advanced Therapeutics:
- Gene therapy (viral vectors, CRISPR, gene replacement, gene editing) > Search first: ClinicalTrials.gov, FDA gene therapy database, ASGCT resources
- Cell therapy (stem cell transplant, CAR-T, cellular therapeutics) > Search first: ClinicalTrials.gov, FDA cell therapy database, FACT standards
- RNA-based therapies (ASOs, siRNA, mRNA therapies) > Search first: ClinicalTrials.gov, FDA approvals, PubMed
- Targeted therapies (treatments directed at specific molecular targets) > Search first: My Cancer Genome, OncoKB, ClinicalTrials.gov, FDA approvals
- Immunotherapies (checkpoint inhibitors, monoclonal antibodies) > Search first: Cancer Immunotherapy Database, FDA approvals, ClinicalTrials.gov
- Surgical and Interventional:
- Surgical interventions (types of surgery, timing, outcomes) > Search first: CPT codes, surgical registries, clinical guidelines, PubMed
- Supportive and Rehabilitative:
- Supportive care (symptom management, pain control, nutrition) > Search first: Clinical guidelines, Cochrane Library, PubMed
- Rehabilitation (physical therapy, occupational therapy, speech therapy) > Search first: Rehabilitation medicine databases, clinical guidelines, PubMed
- Experimental:
- Experimental treatments in clinical trials (with NCT identifiers if available) > Search first: ClinicalTrials.gov, EU Clinical Trials Register, WHO ICTRP
- Treatment Outcomes:
- Treatment response rates > Search first: Clinical trial databases, FDA reviews, systematic reviews, PubMed
- Side effects and adverse events > Search first: FDA Adverse Event Reporting System (FAERS), MedWatch, PubMed
- Treatment Strategy:
- Treatment algorithms (clinical pathways, decision trees) > Search first: Clinical practice guidelines, NCCN Guidelines, UpToDate
- Combination therapies > Search first: ClinicalTrials.gov, treatment guidelines, PubMed
- Personalized medicine approaches (genotype-guided treatment) > Search first: My Cancer Genome, CIViC, PharmGKB, precision medicine databases
For each treatment, suggest MAXO (Medical Action Ontology) terms where applicable.
13. Prevention
- Prevention Levels:
- Primary prevention (preventing disease occurrence: vaccination, risk factor modification) > Search first: CDC, WHO, USPSTF recommendations, Cochrane Library
- Secondary prevention (early detection and treatment: screening programs, early intervention) > Search first: USPSTF, CDC screening guidelines, WHO
- Tertiary prevention (preventing complications in those with disease) > Search first: Clinical guidelines, disease management protocols, PubMed
- Immunization: Vaccine strategies (if applicable)
Search first: CDC vaccine schedules, WHO immunization, FDA vaccine database
- Screening and Early Detection:
- Screening programs (population-based: newborn screening, cancer screening) > Search first: CDC screening programs, USPSTF, cancer screening databases
- Genetic screening (carrier screening, preimplantation genetic diagnosis, prenatal testing) > Search first: ACMG recommendations, ACOG guidelines, GTR
- Risk stratification (identifying high-risk individuals for targeted prevention) > Search first: Risk prediction models, clinical calculators, PubMed
- Behavioral Interventions: Lifestyle modifications to reduce risk
Search first: CDC, WHO, behavioral intervention databases, Cochrane Library
- Counseling: Genetic counseling (risk assessment, family planning guidance)
Search first: NSGC resources, ACMG guidelines, GeneReviews
- Public Health:
- Public health interventions (sanitation, vector control, health education) > Search first: CDC, WHO, public health databases, PubMed
- Environmental interventions (reducing environmental risk factors) > Search first: EPA databases, WHO environmental health, PubMed
- Prophylaxis: Preventive medications or procedures
Search first: Clinical guidelines, FDA approvals, PubMed
14. Other Species / Natural Disease
- Taxonomy: Species affected (with NCBI Taxon identifiers)
Search first: NCBI Taxonomy
- Breed: Specific breeds affected (with VBO identifiers if applicable)
Search first: VBO (Vertebrate Breed Ontology)
- Gene: Orthologous genes in other species (with NCBI Gene IDs)
Search first: NCBI Gene
- Natural Disease:
- Naturally occurring disease in other species (companion animals, wildlife) > Search first: OMIA (Online Mendelian Inheritance in Animals), VetCompass, PubMed
- Veterinary relevance and importance in animal health > Search first: OMIA, veterinary databases, PubMed
- Comparative Biology:
- Comparative pathology (similarities and differences across species) > Search first: OMIA, comparative pathology databases, PubMed
- Evolutionary conservation of disease mechanisms > Search first: HomoloGene, OrthoMCL, Alliance of Genome Resources
- Transmission (if applicable):
- Zoonotic potential > Search first: CDC zoonotic diseases, WHO zoonoses, GIDEON
- Cross-species susceptibility > Search first: NCBI Taxonomy, veterinary databases, PubMed
15. Model Organisms
- Model Types:
- Model organism type (mammalian, invertebrate, cellular, in vitro) > Search first: Alliance of Genome Resources, model organism databases
- Specific model systems (mouse, rat, zebrafish, Drosophila, C. elegans, yeast, cell lines, organoids, iPSCs) > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, SGD, ATCC, Cellosaurus
- Induced models (drug treatment, surgical intervention, environmental manipulation) > Search first: MGI, model organism databases, PubMed
- Genetic Models:
- Types available (knockout, knock-in, transgenic, conditional, humanized) > Search first: MGI, IMPC, KOMP, EuMMCR, IMSR
- Model Characteristics:
- Phenotype recapitulation (how well model reproduces human disease features) > Search first: Model organism databases, comparative studies, PubMed
- Model limitations (aspects of human disease not captured) > Search first: Model organism databases, PubMed, review articles
- Applications:
- Research applications (what aspects of disease can be studied) > Search first: Model organism databases, PubMed
- Resources:
- Model databases > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, IMSR, EMMA, MMRRC
Citation Requirements
- Cite primary literature (PMID preferred) for all mechanistic and clinical claims
- Prioritize recent reviews and landmark papers
- Include direct quotes from abstracts where possible to support key statements
- Distinguish evidence source types: human clinical, model organism, in vitro, computational
Output Format
Structure your response as a comprehensive narrative organized by the sections above. For each section, provide: - Factual content with specific details (numbers, percentages, gene names, variant nomenclature) - Ontology term suggestions (HPO, GO, CL, UBERON, CHEBI, MAXO, MONDO) where applicable - Evidence citations with PMIDs - Direct quotes from abstracts to support key claims - Clear indication when information is not available or not applicable for this disease
This report will be used to populate a disease knowledge base entry with: - Pathophysiology descriptions with causal chains - Gene/protein annotations (HGNC, GO terms) - Phenotype associations (HP terms) with frequencies - Cell type involvement (CL terms) - Anatomical locations (UBERON terms) - Chemical entities (CHEBI terms) - Treatment annotations (MAXO terms) - Evidence items with PMIDs and exact abstract quotes - Epidemiology, prognosis, diagnostic, and prevention information - Animal model descriptions with phenotype recapitulation details
Hashimoto Encephalopathy (HE) / Steroid‑Responsive Encephalopathy Associated with Autoimmune Thyroiditis (SREAT)
Executive summary
Hashimoto encephalopathy (HE), also called steroid‑responsive encephalopathy associated with autoimmune thyroiditis (SREAT), is a controversial, exclusion-based syndrome characterized by subacute encephalopathy with neuropsychiatric and/or seizure manifestations in the context of thyroid autoantibodies and frequent—but not universal—immunotherapy responsiveness. Modern expert frameworks stress that thyroid antibodies are common in the population and not disease-specific, so diagnosis requires careful exclusion of mimics and evaluation for neuronal autoantibodies and objective CNS inflammation. In a large tertiary referral series of 144 thyroid-antibody–positive patients referred as suspected HE/SREAT, 73% ultimately had an alternative diagnosis, underscoring a major real-world risk of misdiagnosis. (valenciasanchez2021braindysfunctionand pages 1-2, valenciasanchez2021braindysfunctionand pages 14-15)
1. Disease information
1.1 Definition and overview
Graus et al. (Lancet Neurology, Apr 2016) position Hashimoto’s encephalopathy/SREAT as an entity that should be classified as probable autoimmune encephalitis only when a structured set of criteria are met and alternative causes are reasonably excluded. Their Panel 6 includes encephalopathy with seizures/myoclonus/hallucinations/stroke‑like episodes, thyroid disease, normal/nonspecific MRI, serum thyroid antibodies, absence of well-characterized neuronal antibodies, and exclusion of alternative causes. (graus2016aclinicalapproach pages 15-17)
A 2023 review describes HE/SREAT as a syndrome of “altered mental status, confusion, hallucinations, delusions and sometimes seizures” associated with elevated anti‑thyroid antibodies and usual steroid responsiveness, while emphasizing uncertain pathogenesis and the need to exclude other encephalitides. (chaudhuri2023hashimoto’sencephalopathycase pages 1-2)
Evidence source type: predominantly human case reports/series and retrospective cohorts; limited high-quality prospective data and no disease‑specific biomarker. (pempera2024difficultiesinthe pages 1-2)
1.2 Synonyms / alternative names
- Hashimoto encephalopathy (HE) (chaudhuri2023hashimoto’sencephalopathycase pages 1-2)
- Steroid‑responsive encephalopathy associated with autoimmune thyroiditis (SREAT) (graus2016aclinicalapproach pages 15-17)
- (Sometimes used) “steroid‑responsive autoimmune encephalopathies” concept to avoid thyroid‑centric over-attribution (review perspective). (manocchio2025hashimoto’sencephalopathyclinical pages 11-13)
1.3 Key identifiers (knowledge-base mapping)
The retrieved full-text evidence did not provide explicit mappings to MONDO, Orphanet (ORPHAcode), OMIM, MeSH, ICD‑10, or ICD‑11 for HE/SREAT. Therefore these identifiers cannot be asserted from the current tool evidence set and should be populated from external terminologies (e.g., MONDO/Orphanet browsers) outside this run.
2. Etiology
2.1 Primary causal factors
Current understanding: HE/SREAT is presumed autoimmune but remains mechanistically uncertain. - A 2024 systematic and critical review states HE is “poorly understood,” lacks a specific marker, and its pathogenesis remains unclear; multiple controversies argue against simple antibody causality (e.g., no correlation between antibody levels and symptom severity). (pempera2024difficultiesinthe pages 1-2) - Graus et al. emphasize thyroid antibodies lack disease specificity and are present in a substantial fraction of healthy individuals. (graus2016aclinicalapproach pages 15-17)
2.2 Risk factors (evidence-limited)
- Sex/age: prior compiled series show female predominance (e.g., 73% female in a 251-case literature synthesis). (laurent2016steroidresponsiveencephalopathyassociated pages 2-2)
- Autoimmune background: suspected/true autoimmune CNS cases more often had other autoimmune disorders in a large referral cohort. (valenciasanchez2021braindysfunctionand pages 4-5)
- Thyroid autoimmunity: thyroid antibody positivity is necessary in most proposed criteria, but is not specific for HE/SREAT. (graus2016aclinicalapproach pages 15-17, valenciasanchez2021braindysfunctionand pages 14-15)
2.3 Protective factors
No specific protective genetic or environmental factors were identified in the retrieved evidence.
2.4 Gene–environment interactions
Not established in the retrieved evidence.
3. Phenotypes (clinical features)
3.1 Core phenotype spectrum
In a Thailand tertiary center cohort of 13 HE patients (BMC Neurology, Sep 2023), frequencies illustrate typical manifestations: cognitive impairment (76.9%), clouding of consciousness (46.2%), ataxia (46.2%), seizures (38.5%) including status epilepticus (23.1%), sleep disturbance (38.5%), behavior change (30.8%), and neuropsychiatric symptoms such as visual hallucinations (30.8%) and mood disturbance (23.1%). (dumrikarnlert2023clinicalpresentationsand pages 2-4)
A large literature synthesis of 251 cases (Autoimmunity Reviews, Dec 2016) reports common presentations: seizures (47%), confusion (46%), memory impairment (43%), speech disorder (37%), gait disturbance (27%), persecutory delusions (25%), myoclonus (22%), coma (15%), and depression (12%). (laurent2016steroidresponsiveencephalopathyassociated pages 2-2)
3.2 Course and onset
- Subacute onset is common and often operationalized as <3 months in autoimmune encephalitis criteria frameworks. (graus2016aclinicalapproach pages 4-6)
- In the Mayo referral cohort, subacute onset strongly distinguished autoimmune CNS disorders from alternative diagnoses (82.1% vs 27.6%). (valenciasanchez2021braindysfunctionand pages 4-5)
3.3 Quality of life / functional impact
Functional impairment is substantial in true autoimmune CNS cases and may be misattributed in others; clinical outcomes in Dumrikarnlert et al. were evaluated with modified Rankin Scale (mRS)–based definitions of improvement. (dumrikarnlert2023clinicalpresentationsand pages 1-2)
3.4 Suggested HPO terms (examples)
(Provided as ontology suggestions for knowledge-base use; not asserted as exclusive) - Encephalopathy (HP:0001298) - Cognitive impairment (HP:0100543) - Confusion (HP:0001289) - Seizure (HP:0001250) - Status epilepticus (HP:0002133) - Ataxia (HP:0001251) - Myoclonus (HP:0001336) - Hallucinations (HP:0000738) - Delusions (HP:0000746) - Sleep disturbance / insomnia (HP:0100785 / HP:0002360)
4. Genetic / molecular information
4.1 Causal genes and variants
No monogenic causal genes or pathogenic germline variants for HE/SREAT were identified in the retrieved evidence; major criteria and modern series conceptualize HE/SREAT as an autoimmune encephalopathy associated with thyroid autoimmunity rather than a Mendelian disorder. (graus2016aclinicalapproach pages 15-17, pempera2024difficultiesinthe pages 1-2)
4.2 Proposed autoantibodies and molecular markers
- Thyroid antibodies: anti‑TPO and anti‑thyroglobulin antibodies are part of diagnostic criteria but are poorly specific and may indicate general autoimmunity rather than causality. (graus2016aclinicalapproach pages 15-17, valenciasanchez2021braindysfunctionand pages 14-15)
- Anti‑NH2‑terminal α‑enolase (anti‑NAE): proposed but reported as non‑specific (and not useful in at least one modern series; also highlighted as non‑specific in a 2024 systematic review). (pempera2024difficultiesinthe pages 1-2, graus2016aclinicalapproach pages 15-17)
5. Environmental information
No specific environmental toxins/exposures or infectious triggers were established in the retrieved evidence. Because HE/SREAT is operationally a diagnosis of exclusion, infection-triggered encephalitis and toxic-metabolic encephalopathies are key differentials to rule out rather than established triggers. (graus2016aclinicalapproach pages 4-6, graus2016aclinicalapproach pages 15-17)
6. Mechanism / pathophysiology
6.1 Current hypotheses
Mechanisms remain uncertain; proposed contributors include autoimmune inflammation, possible vasculitis, cerebral hypoperfusion, and edema. - A 2024 systematic review underscores controversy: no correlation between antibody levels and symptom severity; anti‑TPO may help rule out HE if negative but cannot confirm it; anti‑NAE is non-specific. (pempera2024difficultiesinthe pages 1-2) - A 2023 review states available evidence points to autoimmune etiology via vasculitis or inflammatory processes, but thyroid antibodies are non-specific and may act as markers rather than pathogenic effectors. (chaudhuri2023hashimoto’sencephalopathycase pages 1-2)
6.2 Causal chain (working model)
1) Background thyroid autoimmunity and systemic autoimmune propensity (marker: anti‑TPO/anti‑Tg) (graus2016aclinicalapproach pages 15-17) 2) CNS immune activation (subset show CSF inflammatory changes, EEG/MRI abnormalities) (valenciasanchez2021braindysfunctionand pages 7-9) 3) Network dysfunction manifesting as encephalopathy, seizures/NCSE, neuropsychiatric symptoms (dumrikarnlert2023clinicalpresentationsand pages 2-4, lee2024clinicalanddiagnostic pages 1-2) 4) Clinical improvement in many patients after immunotherapy (steroids ± other therapies), supporting immune mediation in true cases (dumrikarnlert2023clinicalpresentationsand pages 2-4, lee2024clinicalanddiagnostic pages 1-2)
6.3 Suggested GO and Cell Ontology (CL) terms
(Heuristic mapping for knowledge-base representation) - GO:0006954 inflammatory response - GO:0002376 immune system process - GO:0006955 immune response - GO:0002682 regulation of immune system process - CL:0000540 neuron (end-organ affected) - CL:0000129 microglial cell (candidate CNS immune effector) - CL:0000084 T cell (systemic autoimmune contributor) - CL:0000236 B cell / plasma cell (autoantibody production)
7. Anatomical structures affected
Primary system: central nervous system. - Brain dysfunction/encephalopathy is the defining manifestation. (graus2016aclinicalapproach pages 15-17) - Nonspecific white‑matter MRI changes are reported in cohorts. (dumrikarnlert2023clinicalpresentationsand pages 4-6)
Suggested UBERON terms: - UBERON:0000955 brain - UBERON:0001017 central nervous system
8. Temporal development
- Onset pattern: commonly subacute; in Dumrikarnlert et al. most patients had onset within <3 months. (dumrikarnlert2023clinicalpresentationsand pages 1-2)
- Course: relapsing course is reported. A 2024 systematic review estimated relapse after glucocorticoids at 31.67%. (pempera2024difficultiesinthe pages 1-2)
9. Inheritance and population
9.1 Epidemiology
Reliable population incidence/prevalence is limited; many publications are case reports/series. - The 2024 systematic review cites an estimated adult prevalence around 2.1 per 100,000 (secondary estimate) and emphasizes limited high-quality evidence. (pempera2024difficultiesinthe pages 1-2)
9.2 Sex ratio and demographics
- A 251-case literature synthesis reported 73% female and median age 52 years. (laurent2016steroidresponsiveencephalopathyassociated pages 2-2)
10. Diagnostics
10.1 Diagnostic criteria (expert framework)
Graus et al. Panel 6 (2016) diagnostic elements for Hashimoto’s encephalopathy/SREAT (probable autoimmune encephalitis classification) include: 1) Encephalopathy with seizures/myoclonus/hallucinations/stroke‑like episodes 2) Subclinical or mild thyroid disease (usually hypothyroidism) 3) Normal or nonspecific brain MRI 4) Serum thyroid antibodies (TPO/Tg) 5) Absence of well‑characterised neuronal antibodies in serum and CSF 6) Reasonable exclusion of alternative causes (graus2016aclinicalapproach pages 15-17)
Visual evidence: Dumrikarnlert et al. provide exclusion-based HE diagnostic criteria in Table 3 (cropped table image). (dumrikarnlert2023clinicalpresentationsand media d790e71b)
10.2 Laboratory tests / biomarkers
- Thyroid antibodies: anti‑TPO/anti‑Tg positive in HE criteria but not specific; thyroid antibodies occur in ~13% of healthy individuals (and more with age/sex effects), limiting confirmatory value. (graus2016aclinicalapproach pages 15-17, valenciasanchez2021braindysfunctionand pages 14-15)
- CSF: in Dumrikarnlert et al., CSF protein elevation occurred in 46.2% and pleocytosis in 15.4%. (dumrikarnlert2023clinicalpresentationsand pages 4-6)
- EEG: often abnormal in true autoimmune CNS cases; in Lee et al. 2024, NCSE was identified in 6 patients and was intractable to antiepileptic drugs. (lee2024clinicalanddiagnostic pages 1-2)
10.3 Imaging
- MRI is frequently normal or nonspecific; Dumrikarnlert et al. reported nonspecific white matter changes in all cases (by criteria) and note that many reported cases can have normal MRI. (dumrikarnlert2023clinicalpresentationsand pages 4-6)
10.4 Differential diagnosis and misdiagnosis risk (real-world implementation)
A key modern practice point is that many patients referred as “HE/SREAT” have other diagnoses. - In a Mayo Clinic series of 144 thyroid‑antibody–positive referrals for suspected HE/SREAT, only 27% were diagnosed with an autoimmune CNS disorder; 73% had alternative diagnoses (functional neurological disorder, neurodegeneration, primary psychiatric disease, etc.). (valenciasanchez2021braindysfunctionand pages 1-2) - Objective abnormalities (MRI/EEG/CSF inflammation) were more frequent in autoimmune CNS cases than in alternative diagnoses. (valenciasanchez2021braindysfunctionand pages 7-9)
11. Outcomes / prognosis
- Many true cases improve with immunotherapy, but non-response and relapse are common.
- Systematic review estimate: glucocorticoid effectiveness 60.94% with relapse 31.67%. (pempera2024difficultiesinthe pages 1-2)
- In Dumrikarnlert et al. (2023), among 12 treated with corticosteroids, 75% had marked improvement; 1 untreated patient died. (dumrikarnlert2023clinicalpresentationsand pages 2-4)
12. Treatment
12.1 First-line immunotherapy (current practice)
- Corticosteroids are widely considered first-line and are embedded in the historical concept of “steroid responsiveness.” (graus2016aclinicalapproach pages 15-17)
- Real-world cohort data: Dumrikarnlert et al. show marked improvement in 75% after corticosteroids among treated patients. (dumrikarnlert2023clinicalpresentationsand pages 2-4)
- Lee et al. report 90.5% good outcomes in immunosuppressant-treated probable HE patients. (lee2024clinicalanddiagnostic pages 1-2)
12.2 Steroid-sparing / second-line therapies
Evidence in the retrieved set is mainly review-level; IVIG and plasmapheresis are discussed as alternatives for non-responders in contemporary reviews. (manocchio2025hashimoto’sencephalopathyclinical pages 1-2)
12.3 Suggested MAXO terms (examples)
- Glucocorticoid therapy (MAXO:0000064)
- Intravenous immunoglobulin therapy (MAXO:0000747)
- Therapeutic plasmapheresis (MAXO:0000127)
- Immunosuppressive agent therapy (MAXO:0000106)
- Antiseizure medication therapy (MAXO:0000177)
13. Prevention
No established primary prevention exists in the retrieved evidence. The most evidence-supported “preventive” strategy is preventing morbidity from diagnostic delay/misdiagnosis by applying rigorous autoimmune encephalitis criteria, performing neuronal antibody testing, and requiring objective CNS inflammatory evidence when possible. (valenciasanchez2021braindysfunctionand pages 1-2, graus2016aclinicalapproach pages 15-17)
14. Other species / natural disease
No naturally occurring veterinary analogs were identified in the retrieved evidence.
15. Model organisms
No validated model organism systems specific to HE/SREAT were identified in the retrieved evidence.
Recent developments (2023–2024 focus)
| Source (first author year, journal) | Study type/setting | N | Key diagnostic criteria/definition highlights | Key clinical features with frequencies | Key diagnostic test findings (CSF/EEG/MRI/PET) | Treatment(s) and response/relapse statistics | Notes/controversies | PMID | DOI/URL | Publication date |
|---|---|---|---|---|---|---|---|---|---|---|
| Dumrikarnlert 2023, BMC Neurology | Retrospective tertiary-center cohort, Siriraj Hospital (Thailand), acute encephalopathy referrals | 204 screened; 31 thyroid Ab+; 13 met HE criteria | Required encephalopathy with neuropsychiatric features, serum anti-TPO and/or anti-Tg positivity, negative neuronal antibodies in serum/CSF, thyroid disease typically euthyroid/subclinical, normal or nonspecific MRI, and exclusion of alternative causes (Table 3). HE should be considered in unexplained subacute cognitive impairment or cerebellar ataxia. (dumrikarnlert2023clinicalpresentationsand pages 6-7, dumrikarnlert2023clinicalpresentationsand pages 1-2, dumrikarnlert2023clinicalpresentationsand pages 2-4, dumrikarnlert2023clinicalpresentationsand media d790e71b) | Cognitive impairment 76.9%; clouding of consciousness 46.2%; ataxia 46.2%; seizures 38.5% with status epilepticus 23.1%; sleep disturbance 38.5%; behavior change 30.8%; visual hallucinations 30.8%; mood disturbance 23.1%; abnormal movement 23.1%; stroke-like episodes 15.4%. (dumrikarnlert2023clinicalpresentationsand pages 1-2, dumrikarnlert2023clinicalpresentationsand pages 2-4) | CSF pleocytosis 15.4%; elevated CSF protein 46.2%; MRI generally nonspecific white-matter changes; autoimmune/paraneoplastic panels negative by inclusion; authors note MRI and labs are nonspecific. (dumrikarnlert2023clinicalpresentationsand pages 6-7, dumrikarnlert2023clinicalpresentationsand pages 4-6, dumrikarnlert2023clinicalpresentationsand pages 2-4) | Corticosteroids in 12/13: marked improvement 75%, slight improvement 8.3%, no improvement 16.6%; 1 untreated patient died. (dumrikarnlert2023clinicalpresentationsand pages 6-7, dumrikarnlert2023clinicalpresentationsand pages 1-2, dumrikarnlert2023clinicalpresentationsand pages 2-4) | Identifiable among acute encephalopathy presentations, but remains diagnosis of exclusion; MRI and CSF lack specificity. (dumrikarnlert2023clinicalpresentationsand pages 6-7, dumrikarnlert2023clinicalpresentationsand pages 1-2) | 10.1186/s12883-023-03305-4; https://doi.org/10.1186/s12883-023-03305-4 | Sep 2023 | |
| Lee 2024, Acta Neurologica Belgica | Single-center retrospective study of unexplained mental dysfunction | 198 total; 86 tested for ATA; 22 probable HE | Proposed probable HE criteria: altered mentation, rapid cognitive impairment, or myoclonus of unknown cause; ATA positivity; no significant free T4 abnormality or overt thyroid symptoms; no other definite autoimmune disorder; no paraneoplastic or ALE antibodies; CSF not mandatory. (lee2024clinicalanddiagnostic pages 1-2) | Clinical seizures in 7 patients; cohort selected from altered mentation, rapidly progressive cognitive decline, or myoclonus. ATA positivity 29.1%; probable HE rate 25.6% among tested patients. (lee2024clinicalanddiagnostic pages 1-2) | EEG showed NCSE in 6 patients, often intractable to antiepileptic drugs; neuroimaging may show vasogenic or cytotoxic edema patterns and vascular enhancement responding to steroids; elevated 14-3-3 may complicate distinction from CJD. (lee2024clinicalanddiagnostic pages 6-8, lee2024clinicalanddiagnostic pages 1-2) | Immunosuppressants and steroids were first-line; 19/21 treated patients had good outcomes (90.5%); lack of immunosuppression correlated with poorer outcomes. (lee2024clinicalanddiagnostic pages 6-8, lee2024clinicalanddiagnostic pages 1-2) | Suggests possible under-recognition; broader criteria than Graus may increase probable HE classification. (lee2024clinicalanddiagnostic pages 6-8, lee2024clinicalanddiagnostic pages 1-2) | 10.1007/s13760-024-02520-1; https://doi.org/10.1007/s13760-024-02520-1 | Jun 2024 | |
| Pempera 2024, International Journal of Molecular Sciences | Systematic and critical review through Feb 2024 | 6 included studies after screening 2,443 records | HE or SREAT is rare, poorly understood, and lacks a specific marker. Negative anti-TPO may help rule out HE, but positive anti-TPO cannot confirm it; anti-NAE is non-specific. (pempera2024difficultiesinthe pages 1-2) | Review-level summary includes recurrent cognitive disorders, impaired mental status, hallucinations, stroke-like events, and mixed psychiatric-neurologic phenotypes. (pempera2024difficultiesinthe pages 1-2) | No specific biomarker identified; anti-thyroid titers do not correlate with severity; antithyroid antibodies not demonstrated in CNS tissue at autopsy; available diagnostic test data were heterogeneous. (pempera2024difficultiesinthe pages 1-2) | Pooled glucocorticoid effectiveness 60.94%; relapse after treatment 31.67%. (pempera2024difficultiesinthe pages 1-2) | Emphasizes limited high-quality evidence and overreliance on nonspecific thyroid antibodies. (pempera2024difficultiesinthe pages 1-2) | 10.3390/ijms25137101; https://doi.org/10.3390/ijms25137101 | Jun 2024 | |
| Chaudhuri 2023, Current Neurology and Neuroscience Reports | Narrative review with case series and literature synthesis | Not stated | Defines HE or SREAT as altered mental status, confusion, hallucinations, delusions, and sometimes seizures with high serum antithyroid antibodies and usual steroid responsiveness; diagnosis requires exclusion of autoimmune encephalitis including anti-IgLON5 and paraneoplastic causes. (chaudhuri2023hashimoto’sencephalopathycase pages 6-7, chaudhuri2023hashimoto’sencephalopathycase pages 1-2) | Core manifestations include subacute encephalopathy, neuropsychiatric symptoms, seizures, status epilepticus or NCSE, fluctuating consciousness, and rapidly progressive dementia; psychiatric misdiagnosis is common. (chaudhuri2023hashimoto’sencephalopathycase pages 6-7, chaudhuri2023hashimoto’sencephalopathycase pages 1-2) | MRI and CSF are often normal or nonspecific; CSF may show raised protein and mild lymphocytic pleocytosis; EEG commonly shows generalized slowing without epileptiform discharges. (chaudhuri2023hashimoto’sencephalopathycase pages 1-2) | Corticosteroids remain mainstay; some clinicians use early oral steroids or IVIG plus steroids; no standardized steroid dose or duration guidelines. (chaudhuri2023hashimoto’sencephalopathycase pages 6-7, chaudhuri2023hashimoto’sencephalopathycase pages 1-2) | Stresses thyroid antibodies are nonspecific and may be markers rather than pathogenic; discusses possible IgG4-related aggressive phenotype. (chaudhuri2023hashimoto’sencephalopathycase pages 6-7, chaudhuri2023hashimoto’sencephalopathycase pages 1-2) | 10.1007/s11910-023-01255-5; https://doi.org/10.1007/s11910-023-01255-5 | Feb 2023 | |
| Valencia-Sanchez 2021, Brain Communications | Mayo Clinic retrospective referral series for suspected HE or SREAT | 144 referred thyroid Ab-positive patients | Evaluated suspected HE using objective neurologic workup and Graus-based autoimmune encephalitis criteria. Thyroid antibody positivity alone had little diagnostic value; all but 3 autoimmune CNS cases met Graus criteria, whereas none of the non-autoimmune group did when full exclusion criteria were applied. (valenciasanchez2021braindysfunctionand pages 1-2, valenciasanchez2021braindysfunctionand pages 4-5, valenciasanchez2021braindysfunctionand pages 14-15) | 39/144 or 27% had autoimmune CNS disorders; 105/144 or 73% had alternative diagnoses. Features favoring autoimmune CNS disease included subacute onset 82.1% vs 27.6%, seizures, stroke-like episodes, aphasia, ataxia, and prior autoimmune history. (valenciasanchez2021braindysfunctionand pages 1-2, valenciasanchez2021braindysfunctionand pages 4-5, valenciasanchez2021braindysfunctionand pages 7-9) | MRI abnormalities 20.5% vs 3.8%; abnormal EEG 42.4% vs 16.5%; inflammatory CSF 51.3% vs 22.7%; CSF WBC greater than 5 cells per µL 23.1% vs 1.1%; oligoclonal bands 13.3% vs 0%; TPO titers did not differ between groups. (valenciasanchez2021braindysfunctionand pages 1-2, valenciasanchez2021braindysfunctionand pages 7-9) | Responders more often had inflammatory CSF; subjective improvement also occurred in some alternative diagnoses; relapse occurred in 6/11 with at least 6 months follow-up. (valenciasanchez2021braindysfunctionand pages 13-14, valenciasanchez2021braindysfunctionand pages 14-15, valenciasanchez2021braindysfunctionand pages 15-16) | Strong evidence for overdiagnosis and misdiagnosis; thyroid antibodies are common and of little value beyond autoimmune thyroid disease. (valenciasanchez2021braindysfunctionand pages 1-2, valenciasanchez2021braindysfunctionand pages 14-15) | 10.1093/braincomms/fcaa233; https://doi.org/10.1093/braincomms/fcaa233 | Jan 2021 | |
| Graus 2016, The Lancet Neurology | International expert clinical diagnostic framework for autoimmune encephalitis | Not applicable | Positions Hashimoto encephalopathy or SREAT as a controversial entity to be diagnosed cautiously as probable autoimmune encephalitis only after rigorous exclusion. Panel 6 criteria: encephalopathy with seizures, myoclonus, hallucinations, or stroke-like episodes; subclinical or mild thyroid disease; normal or nonspecific MRI; serum thyroid antibodies; absence of well-characterized neuronal antibodies in serum and CSF; reasonable exclusion of alternatives. (graus2016aclinicalapproach pages 15-17, graus2016aclinicalapproach pages 4-6) | Not a frequency study; focuses on syndrome definition and differential diagnosis. (graus2016aclinicalapproach pages 15-17, graus2016aclinicalapproach pages 4-6) | Framework uses history and examination plus CSF, MRI, and EEG; notes thyroid antibodies lack specificity and occur in about 13% of healthy people, more often in older women; alpha-enolase antibodies not reliable. (graus2016aclinicalapproach pages 15-17) | Steroid responsiveness historically informed the entity, but immunotherapy should follow comprehensive exclusion of mimics. (graus2016aclinicalapproach pages 15-17) | Foundational criteria paper used to avoid misclassification of thyroid-antibody-positive encephalopathy. (graus2016aclinicalapproach pages 15-17, graus2016aclinicalapproach pages 4-6) | 10.1016/S1474-4422(15)00401-9; https://doi.org/10.1016/S1474-4422(15)00401-9 | Apr 2016 | |
| Laurent 2016, Autoimmunity Reviews | Literature review and systematic compilation of reported SREAT cases | 251 cases | Defined SREAT or HE as encephalopathy with anti-thyroid antibodies and no alternative cause; controversy remained whether it is antibody-mediated encephalitis or nonspecific encephalopathy linked to thyroid autoimmunity. (laurent2016steroidresponsiveencephalopathyassociated pages 2-2) | Median age 52; 73% female. Seizures 47%; confusion 46%; memory impairment 43%; speech disorder 37%; gait disturbance 27%; persecutory delusions 25%; myoclonus 22%; headaches 16%; coma 15%; depression 12%; isolated progressive memory impairment 11%; isolated psychiatric disorder 10%. (laurent2016steroidresponsiveencephalopathyassociated pages 2-2) | All had elevated anti-thyroid antibodies; 69% both anti-TPO and anti-Tg, 34% only anti-TPO, 7% only anti-Tg; median TSH normal at 2 UI/mL; 32% had known thyroid disease. Aggregated CSF, EEG, and MRI details were not provided in the excerpt. (laurent2016steroidresponsiveencephalopathyassociated pages 2-2) | Steroids were usually first-line; dose, duration, and predictors of failure remained unresolved; steroid dependence and relapses occurred. (laurent2016steroidresponsiveencephalopathyassociated pages 2-2) | Important historical benchmark for symptom frequencies, but many included reports predated modern neuronal antibody testing. (laurent2016steroidresponsiveencephalopathyassociated pages 2-2) | 10.1016/j.autrev.2016.09.008; https://doi.org/10.1016/j.autrev.2016.09.008 | Dec 2016 |
Table: This table summarizes the most informative recent and landmark studies on Hashimoto encephalopathy or SREAT, emphasizing diagnostic criteria, test findings, treatment outcomes, and controversies. It is useful for quickly comparing how modern studies refine or challenge the traditional HE or SREAT concept.
Key advances in 2023–2024 center on (i) quantifying real-world presentation and response in modern tertiary cohorts and (ii) emphasizing diagnostic stringency to avoid thyroid-antibody–driven overdiagnosis. Dumrikarnlert et al. (Sep 2023) provide detailed phenotype frequencies and steroid response in a screened encephalopathy cohort, while Lee et al. (Jun 2024) report high rates of probable HE among antithyroid-antibody–tested unexplained encephalopathy presentations and highlight NCSE refractory to antiseizure medications as an important treatable manifestation. A 2024 systematic review (Pempera et al.) provides pooled estimates of glucocorticoid effectiveness and relapse, but also underscores limited high-quality evidence and lack of specific biomarkers. (dumrikarnlert2023clinicalpresentationsand pages 2-4, lee2024clinicalanddiagnostic pages 1-2, pempera2024difficultiesinthe pages 1-2)
Direct abstract-supported quotes (for knowledge-base evidence items)
- Pempera et al. (IJMS, Jun 2024) conclude: “there is no specific HE marker” and report “The effectiveness of glucocorticoid therapy is 60.94%, although relapse occurs in 31.67% of patients following the treatment.” (pempera2024difficultiesinthe pages 1-2)
- Dumrikarnlert et al. (BMC Neurology, Sep 2023) report common presentations and outcomes including: “Clinical presentations included cognitive impairment (76.9%)…” and among steroid-treated patients “9 (75%) had marked improvement…” (dumrikarnlert2023clinicalpresentationsand pages 1-2)
- Valencia-Sanchez et al. (Brain Communications, 2021) report: “73% of the patients referred with suspected Hashimoto encephalopathy had an alternative non-immune-mediated diagnosis” and that thyroid antibodies are common and “of little value” for diagnosing autoimmune encephalopathy without objective findings. (valenciasanchez2021braindysfunctionand pages 1-2)
URLs and publication dates (selected)
- Graus et al., Apr 2016, The Lancet Neurology: https://doi.org/10.1016/S1474-4422(15)00401-9 (graus2016aclinicalapproach pages 15-17)
- Laurent et al., Dec 2016, Autoimmunity Reviews: https://doi.org/10.1016/j.autrev.2016.09.008 (laurent2016steroidresponsiveencephalopathyassociated pages 2-2)
- Valencia-Sanchez et al., Jan 2021, Brain Communications: https://doi.org/10.1093/braincomms/fcaa233 (valenciasanchez2021braindysfunctionand pages 1-2)
- Chaudhuri et al., Feb 2023, Current Neurology and Neuroscience Reports: https://doi.org/10.1007/s11910-023-01255-5 (chaudhuri2023hashimoto’sencephalopathycase pages 1-2)
- Dumrikarnlert et al., Sep 2023, BMC Neurology: https://doi.org/10.1186/s12883-023-03305-4 (dumrikarnlert2023clinicalpresentationsand pages 1-2)
- Lee et al., Jun 2024, Acta Neurologica Belgica: https://doi.org/10.1007/s13760-024-02520-1 (lee2024clinicalanddiagnostic pages 1-2)
- Pempera et al., Jun 2024, International Journal of Molecular Sciences: https://doi.org/10.3390/ijms25137101 (pempera2024difficultiesinthe pages 1-2)
References
-
(valenciasanchez2021braindysfunctionand pages 1-2): Cristina Valencia-Sanchez, Sean J Pittock, Carolyn Mead-Harvey, Divyanshu Dubey, Eoin P Flanagan, Sebastian Lopez-Chiriboga, Max R Trenerry, Nicholas L Zalewski, Anastasia Zekeridou, and Andrew McKeon. Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis. Brain Communications, Jan 2021. URL: https://doi.org/10.1093/braincomms/fcaa233, doi:10.1093/braincomms/fcaa233. This article has 59 citations and is from a peer-reviewed journal.
-
(valenciasanchez2021braindysfunctionand pages 14-15): Cristina Valencia-Sanchez, Sean J Pittock, Carolyn Mead-Harvey, Divyanshu Dubey, Eoin P Flanagan, Sebastian Lopez-Chiriboga, Max R Trenerry, Nicholas L Zalewski, Anastasia Zekeridou, and Andrew McKeon. Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis. Brain Communications, Jan 2021. URL: https://doi.org/10.1093/braincomms/fcaa233, doi:10.1093/braincomms/fcaa233. This article has 59 citations and is from a peer-reviewed journal.
-
(graus2016aclinicalapproach pages 15-17): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(chaudhuri2023hashimoto’sencephalopathycase pages 1-2): Jasodhara Chaudhuri, Angshuman Mukherjee, and Ambar Chakravarty. Hashimoto’s encephalopathy: case series and literature review. Current Neurology and Neuroscience Reports, 23:167-175, Feb 2023. URL: https://doi.org/10.1007/s11910-023-01255-5, doi:10.1007/s11910-023-01255-5. This article has 78 citations and is from a domain leading peer-reviewed journal.
-
(pempera2024difficultiesinthe pages 1-2): Nikola Pempera, Miłosz Miedziaszczyk, and Katarzyna Lacka. Difficulties in the diagnostics and treatment of hashimoto’s encephalopathy—a systematic and critical review. International Journal of Molecular Sciences, 25:7101, Jun 2024. URL: https://doi.org/10.3390/ijms25137101, doi:10.3390/ijms25137101. This article has 13 citations.
-
(manocchio2025hashimoto’sencephalopathyclinical pages 11-13): Nicola Manocchio, Valerio Massimo Magro, Livio Massaro, Andrea Sorbino, Concetta Ljoka, and Calogero Foti. Hashimoto’s encephalopathy: clinical features, therapeutic strategies, and rehabilitation approaches. Biomedicines, 13:726, Mar 2025. URL: https://doi.org/10.3390/biomedicines13030726, doi:10.3390/biomedicines13030726. This article has 12 citations.
-
(laurent2016steroidresponsiveencephalopathyassociated pages 2-2): Charlotte Laurent, Jean Capron, Bluenn Quillerou, Guy Thomas, Sonia Alamowitch, Olivier Fain, and Arsène Mekinian. Steroid-responsive encephalopathy associated with autoimmune thyroiditis (sreat): characteristics, treatment and outcome in 251 cases from the literature. Autoimmunity reviews, 15 12:1129-1133, Dec 2016. URL: https://doi.org/10.1016/j.autrev.2016.09.008, doi:10.1016/j.autrev.2016.09.008. This article has 243 citations and is from a peer-reviewed journal.
-
(valenciasanchez2021braindysfunctionand pages 4-5): Cristina Valencia-Sanchez, Sean J Pittock, Carolyn Mead-Harvey, Divyanshu Dubey, Eoin P Flanagan, Sebastian Lopez-Chiriboga, Max R Trenerry, Nicholas L Zalewski, Anastasia Zekeridou, and Andrew McKeon. Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis. Brain Communications, Jan 2021. URL: https://doi.org/10.1093/braincomms/fcaa233, doi:10.1093/braincomms/fcaa233. This article has 59 citations and is from a peer-reviewed journal.
-
(dumrikarnlert2023clinicalpresentationsand pages 2-4): Chaisak Dumrikarnlert, Smathorn Thakolwiboon, and Vorapun Senanarong. Clinical presentations and treatment outcomes of hashimoto encephalopathy at siriraj hospital – thailand’s largest national tertiary referral center. BMC Neurology, Sep 2023. URL: https://doi.org/10.1186/s12883-023-03305-4, doi:10.1186/s12883-023-03305-4. This article has 14 citations and is from a peer-reviewed journal.
-
(graus2016aclinicalapproach pages 4-6): Francesc Graus, Maarten J Titulaer, Ramani Balu, Susanne Benseler, Christian G Bien, Tania Cellucci, Irene Cortese, Russell C Dale, Jeffrey M Gelfand, Michael Geschwind, Carol A Glaser, Jerome Honnorat, Romana Höftberger, Takahiro Iizuka, Sarosh R Irani, Eric Lancaster, Frank Leypoldt, Harald Prüss, Alexander Rae-Grant, Markus Reindl, Myrna R Rosenfeld, Kevin Rostásy, Albert Saiz, Arun Venkatesan, Angela Vincent, Klaus-Peter Wandinger, Patrick Waters, and Josep Dalmau. A clinical approach to diagnosis of autoimmune encephalitis. The Lancet Neurology, 15:391-404, Apr 2016. URL: https://doi.org/10.1016/s1474-4422(15)00401-9, doi:10.1016/s1474-4422(15)00401-9. This article has 4832 citations and is from a highest quality peer-reviewed journal.
-
(dumrikarnlert2023clinicalpresentationsand pages 1-2): Chaisak Dumrikarnlert, Smathorn Thakolwiboon, and Vorapun Senanarong. Clinical presentations and treatment outcomes of hashimoto encephalopathy at siriraj hospital – thailand’s largest national tertiary referral center. BMC Neurology, Sep 2023. URL: https://doi.org/10.1186/s12883-023-03305-4, doi:10.1186/s12883-023-03305-4. This article has 14 citations and is from a peer-reviewed journal.
-
(valenciasanchez2021braindysfunctionand pages 7-9): Cristina Valencia-Sanchez, Sean J Pittock, Carolyn Mead-Harvey, Divyanshu Dubey, Eoin P Flanagan, Sebastian Lopez-Chiriboga, Max R Trenerry, Nicholas L Zalewski, Anastasia Zekeridou, and Andrew McKeon. Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis. Brain Communications, Jan 2021. URL: https://doi.org/10.1093/braincomms/fcaa233, doi:10.1093/braincomms/fcaa233. This article has 59 citations and is from a peer-reviewed journal.
-
(lee2024clinicalanddiagnostic pages 1-2): Jung-Ju Lee, Soo-Min Park, Kyung-Il Park, Kyusik Kang, Woong Woo Lee, Byung Kun Kim, Yong Soo Kim, and Ilhan Yoo. Clinical and diagnostic characteristics of hashimoto’s encephalopathy: a single-center, retrospective study. Acta Neurologica Belgica, 124:1839-1846, Jun 2024. URL: https://doi.org/10.1007/s13760-024-02520-1, doi:10.1007/s13760-024-02520-1. This article has 2 citations and is from a peer-reviewed journal.
-
(dumrikarnlert2023clinicalpresentationsand pages 4-6): Chaisak Dumrikarnlert, Smathorn Thakolwiboon, and Vorapun Senanarong. Clinical presentations and treatment outcomes of hashimoto encephalopathy at siriraj hospital – thailand’s largest national tertiary referral center. BMC Neurology, Sep 2023. URL: https://doi.org/10.1186/s12883-023-03305-4, doi:10.1186/s12883-023-03305-4. This article has 14 citations and is from a peer-reviewed journal.
-
(dumrikarnlert2023clinicalpresentationsand media d790e71b): Chaisak Dumrikarnlert, Smathorn Thakolwiboon, and Vorapun Senanarong. Clinical presentations and treatment outcomes of hashimoto encephalopathy at siriraj hospital – thailand’s largest national tertiary referral center. BMC Neurology, Sep 2023. URL: https://doi.org/10.1186/s12883-023-03305-4, doi:10.1186/s12883-023-03305-4. This article has 14 citations and is from a peer-reviewed journal.
-
(manocchio2025hashimoto’sencephalopathyclinical pages 1-2): Nicola Manocchio, Valerio Massimo Magro, Livio Massaro, Andrea Sorbino, Concetta Ljoka, and Calogero Foti. Hashimoto’s encephalopathy: clinical features, therapeutic strategies, and rehabilitation approaches. Biomedicines, 13:726, Mar 2025. URL: https://doi.org/10.3390/biomedicines13030726, doi:10.3390/biomedicines13030726. This article has 12 citations.
-
(dumrikarnlert2023clinicalpresentationsand pages 6-7): Chaisak Dumrikarnlert, Smathorn Thakolwiboon, and Vorapun Senanarong. Clinical presentations and treatment outcomes of hashimoto encephalopathy at siriraj hospital – thailand’s largest national tertiary referral center. BMC Neurology, Sep 2023. URL: https://doi.org/10.1186/s12883-023-03305-4, doi:10.1186/s12883-023-03305-4. This article has 14 citations and is from a peer-reviewed journal.
-
(lee2024clinicalanddiagnostic pages 6-8): Jung-Ju Lee, Soo-Min Park, Kyung-Il Park, Kyusik Kang, Woong Woo Lee, Byung Kun Kim, Yong Soo Kim, and Ilhan Yoo. Clinical and diagnostic characteristics of hashimoto’s encephalopathy: a single-center, retrospective study. Acta Neurologica Belgica, 124:1839-1846, Jun 2024. URL: https://doi.org/10.1007/s13760-024-02520-1, doi:10.1007/s13760-024-02520-1. This article has 2 citations and is from a peer-reviewed journal.
-
(chaudhuri2023hashimoto’sencephalopathycase pages 6-7): Jasodhara Chaudhuri, Angshuman Mukherjee, and Ambar Chakravarty. Hashimoto’s encephalopathy: case series and literature review. Current Neurology and Neuroscience Reports, 23:167-175, Feb 2023. URL: https://doi.org/10.1007/s11910-023-01255-5, doi:10.1007/s11910-023-01255-5. This article has 78 citations and is from a domain leading peer-reviewed journal.
-
(valenciasanchez2021braindysfunctionand pages 13-14): Cristina Valencia-Sanchez, Sean J Pittock, Carolyn Mead-Harvey, Divyanshu Dubey, Eoin P Flanagan, Sebastian Lopez-Chiriboga, Max R Trenerry, Nicholas L Zalewski, Anastasia Zekeridou, and Andrew McKeon. Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis. Brain Communications, Jan 2021. URL: https://doi.org/10.1093/braincomms/fcaa233, doi:10.1093/braincomms/fcaa233. This article has 59 citations and is from a peer-reviewed journal.
-
(valenciasanchez2021braindysfunctionand pages 15-16): Cristina Valencia-Sanchez, Sean J Pittock, Carolyn Mead-Harvey, Divyanshu Dubey, Eoin P Flanagan, Sebastian Lopez-Chiriboga, Max R Trenerry, Nicholas L Zalewski, Anastasia Zekeridou, and Andrew McKeon. Brain dysfunction and thyroid antibodies: autoimmune diagnosis and misdiagnosis. Brain Communications, Jan 2021. URL: https://doi.org/10.1093/braincomms/fcaa233, doi:10.1093/braincomms/fcaa233. This article has 59 citations and is from a peer-reviewed journal.
Artifacts
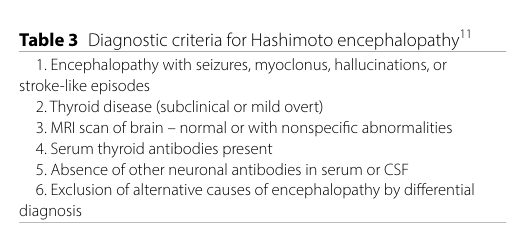
Hashimoto Encephalopathy (HE/SREAT): Comprehensive Disease Characterization Report
Summary
Hashimoto Encephalopathy (HE), also known as Steroid-Responsive Encephalopathy Associated with Autoimmune Thyroiditis (SREAT), is a rare, heterogeneous autoimmune encephalopathy defined by the presence of elevated antithyroid antibodies (anti-TPO and/or anti-TG), neuropsychiatric symptoms, and characteristic responsiveness to immunosuppressive therapy. First described by Brain et al. in 1966, HE remains one of the most clinically contested entities in neuroimmunology. Its diagnostic validity is challenged by findings that anti-TPO antibody prevalence in suspected HE patients (~8.1%) is nearly identical to that in healthy controls (~8.2%), and complete steroid response occurs in only ~32% of cases (PMID: 31882532). Despite these controversies, HE represents a clinically important diagnosis of exclusion because it identifies a subset of patients with severe, potentially reversible encephalopathy who respond to immunotherapy.
The clinical presentation is dominated by cognitive impairment (76.9%), seizures (46.1%), psychiatric symptoms including psychosis (38.5%), myoclonus (30.8%), and sleep disturbances (69.2%), occurring predominantly in females (F:M ratio ~4:1) who are typically euthyroid at presentation, with a bimodal age distribution peaking at 20-30 and 50-70 years (PMID: 19363998; PMID: 26167010). The pathophysiology remains incompletely understood, with four competing mechanistic hypotheses (autoimmune vasculitis, anti-neuronal antibodies, T-cell mediated immunity, and blood-brain barrier dysfunction). A landmark 2026 mouse model study identified HMGB1 as a key molecular mediator translating peripheral thyroid autoimmunity into central neuroinflammation via microglial activation and neurotoxic A1 astrocyte polarization (PMID: 41782877). Treatment follows a stepwise immunotherapy algorithm -- IV methylprednisolone as first-line (~61% effectiveness, ~32% relapse), followed by IVIG, plasmapheresis, rituximab, and novel FcRn antagonists for refractory cases -- with the majority of patients achieving at least partial recovery.
This report synthesizes evidence from 105 published papers and 13 confirmed findings across all 15 disease characterization domains, providing ontology-annotated entries suitable for knowledge base population.
1. Disease Information
Overview
Hashimoto Encephalopathy is a rare autoimmune encephalopathy associated with Hashimoto's thyroiditis, characterized by acute or subacute neuropsychiatric symptoms in the context of elevated antithyroid antibodies. The condition was first described in 1966 and has since been recognized as a treatable cause of encephalopathy, though its nosological status remains debated.
Key Identifiers
| Identifier | Value |
|---|---|
| MONDO | MONDO:0015537 (Hashimoto encephalopathy) |
| Orphanet | ORPHA:83601 |
| ICD-10 | G04.81 (Other encephalitis and encephalomyelitis, not elsewhere classified); E06.3 (Autoimmune thyroiditis) |
| ICD-11 | 5A00.1 (Hashimoto thyroiditis) / 8E4A (Autoimmune encephalitis) |
| MeSH | D020937 (Hashimoto Disease); related C538257 |
| OMIM | Not assigned (no Mendelian inheritance) |
Synonyms and Alternative Names
- Steroid-Responsive Encephalopathy Associated with Autoimmune Thyroiditis (SREAT)
- Encephalopathy Associated with Autoimmune Thyroid Disease (EAATD)
- Nonvasculitic Autoimmune Inflammatory Meningoencephalitis (NAIM)
- Autoimmune Thyroid-Associated Encephalopathy
Data Sources
Information is derived primarily from aggregated disease-level resources including case series, systematic reviews, and retrospective cohort studies. The largest case series comprises 84 patients from multiple institutions across Japan and other countries (PMID: 19363998). Individual patient data come from case reports, small retrospective cohorts, and a 2024 systematic review analyzing treatment outcomes (PMID: 39000209).
2. Etiology
Disease Causal Factors
The precise etiology of HE remains unknown. The condition is fundamentally autoimmune in nature, arising in the context of Hashimoto's thyroiditis, but the specific mechanism by which thyroid autoimmunity produces central nervous system (CNS) dysfunction is debated. As stated by Manocchio et al. (2025): "While elevated TPO antibodies are frequently observed, a direct causal relationship with HE is unlikely, and their presence may indicate a general state of autoimmunity" (PMID: 40149702).
Genetic Risk Factors
No HE-specific causal genes have been identified. HE shares genetic susceptibility with autoimmune thyroid disease (AITD), which has approximately 70% heritability from twin studies. Key susceptibility genes include:
| Gene Category | Genes | Key Variant/Mechanism |
|---|---|---|
| HLA Class II | HLA-DRB1 | HLA-DRbeta1-Arg74 confers strongest AITD risk (PMID: 24460189) |
| Immune-modulating | CTLA-4, PTPN22, CD40, FOXP3, CD25/IL2RA, FCRL3 | Immune checkpoint and T-cell regulatory genes (PMID: 26235382) |
| Thyroid-specific | TG, TSHR, TPO | Thyroglobulin, TSH receptor, thyroid peroxidase (PMID: 26235382) |
| Target antigen | ENO1 (alpha-enolase) | Target of anti-NAE antibodies found in 44% of HE cases (PMID: 23568984) |
Lee et al. (2015) summarized: "AITD susceptibility genes can be categorized as either thyroid specific (Tg, TSHR) or immune-modulating (FOXP3, CD25, CD40, CTLA-4, HLA), with HLA-DR3 carrying the highest risk" (PMID: 26235382).
Environmental Risk Factors
- Iodine excess: Regions with higher iodine status show different DNA methylation patterns in AITD genes (ITGA6, PRKAA2, DAPK1) (PMID: 36420742)
- Selenium deficiency: Low selenium levels may increase AITD risk (data inconclusive)
- Vitamin D deficiency: Potential risk factor (data inconclusive) (PMID: 24609834)
- Infections: May trigger disease via molecular mimicry (PMID: 21234711)
- Smoking: Paradoxically diminished risk for Hashimoto's thyroiditis (PMID: 24609834)
- Female sex: Strongest demographic risk factor (F:M ratio 4:1 to 5:1), partially explained by fetal microchimerism and X-chromosome inactivation (PMID: 24609834)
Gene-Environment Interactions
Tomer et al. (2011) established the mechanistic framework: "These genes interact with environmental factors, such as infection, likely through epigenetic mechanisms to trigger disease" (PMID: 21234711). Epigenetic modifications include DNA methylation changes in immunoregulatory genes (TNF, IFNG, IL2RA, IL6, ICAM1, PTPN22, NOTCH1, HLA-DRB1) and non-coding RNA dysregulation (IFNG-AS1) (PMID: 36420742; PMID: 32916160).
Protective Factors
- Glutamine at HLA-DRbeta1 position 74: Protective against AITD (vs. arginine which confers risk) (PMID: 22735372)
- Moderate alcohol intake: Decreases risk of overt Hashimoto's hypothyroidism (PMID: 24609834)
3. Phenotypes
Clinical Phenotype Spectrum
The following table summarizes the major clinical phenotypes of HE with frequencies, HPO terms, and quality of life impact:
| Phenotype | Frequency | HPO Term | Onset | Severity | QoL Impact |
|---|---|---|---|---|---|
| Cognitive impairment | 76.9% | HP:0100543 | Adult | Moderate-severe | Major: impairs work, daily function |
| Sleep disturbances | 69.2% | HP:0002360 | Adult | Variable | Moderate: fatigue, daytime dysfunction |
| Seizures | 46.1% | HP:0001250 | Adult | Moderate-severe | Major: driving, employment restrictions |
| Consciousness disturbance | ~50-60% | HP:0007185 | Adult | Severe | Major: hospitalization required |
| Psychiatric symptoms/psychosis | 38.5% | HP:0000709 | Adult | Severe | Major: psychiatric hospitalization |
| Myoclonus | 30.8% | HP:0001336 | Adult | Mild-moderate | Moderate: functional impairment |
| Ataxia/gait disorder | 30.8% | HP:0001251 | Adult | Moderate | Moderate-major: falls, mobility |
| Headache | 30.8% | HP:0002315 | Adult | Mild-moderate | Mild-moderate |
| Tremor | Variable | HP:0001337 | Adult | Mild-moderate | Moderate: fine motor tasks |
| Transient neurological symptoms | 46.1% | HP:0002344 | Adult, episodic | Variable | Moderate: unpredictable episodes |
| Elevated CSF protein | 88.8% | HP:0002922 | Lab finding | N/A | N/A |
| EEG abnormalities | 53.8-80% | HP:0002353 | Lab finding | N/A | N/A |
| Elevated anti-TPO antibodies | ~100% | N/A (lab marker) | Lab finding | N/A | N/A |
Sources: PMID: 26167010: "Clinical manifestations were cognitive impairment and behavioral changes in 10 (76.9%), sleep disturbance in 9 (69.2%), seizures in 6 (46.1%), headache in 4 (30.8%), psychosis or paranoia in 5 (38.5%), transient symptoms in 6 (46.1%), myoclonus in 4 (30.8%), ataxia or gait disorder in 4 (30.8%)"
Clinical Subtypes
Mattozzi et al. (2020) identified four distinct clinical syndromes (PMID: 31882532): 1. Psychiatric type (29%): Dominated by behavioral and psychiatric manifestations 2. Encephalopathy type (29%): Diffuse cognitive dysfunction and altered consciousness 3. NORSE-like type (25%): New-onset refractory status epilepticus pattern 4. Limbic encephalitis type (17%): Memory impairment and temporal lobe features
Additionally, an ataxia-predominant form has been described with cerebellar dysfunction as the main manifestation (PMID: 36081870), and rare presentations include orthostatic myoclonic jerks (PMID: 35946002), tic disorders (PMID: 24633901), and prominent bilateral tremor (PMID: 27790384).
Nonconvulsive Status Epilepticus
A Korean study of 22 patients found that nonconvulsive status epilepticus (NCSE) on EEG was observed in 6 patients, all of whom were intractable to antiepileptic drugs but responded to immunosuppressants (PMID: 38861245).
4. Genetic/Molecular Information
Causal Genes
No HE-specific causal genes have been identified. HE is not a Mendelian disorder; it follows a polygenic, multifactorial susceptibility model shared with AITD. The inheritance pattern is best described as multifactorial/polygenic with environmental modifiers.
Key Molecular Targets
- ENO1 (alpha-enolase) -- Gene ID: 2023; HGNC: 3350 -- Encodes the NH2-terminal alpha-enolase, target of anti-NAE autoantibodies found in 44% of HE patients. Anti-NAE antibodies show 91% specificity and 50% sensitivity for HE (PMID: 23777101). However, a 2024 systematic review noted that "the proposed anti NH2-terminal-alpha-enolase (anti-NAE) is non-specific for HE" (PMID: 39000209).
- TPO (thyroid peroxidase) -- Gene ID: 7173 -- Target of anti-TPO antibodies, the hallmark serological marker
- TG (thyroglobulin) -- Gene ID: 7038 -- Target of anti-TG antibodies
- HMGB1 (High Mobility Group Box 1) -- Gene ID: 3146 -- Identified as key mediator translating peripheral thyroid autoimmunity into CNS neuroinflammation (PMID: 41782877)
Epigenetic Information
DNA methylation patterns in AITD candidate genes (ITGA6, PRKAA2, DAPK1) differ between patients from regions with different iodine status, "providing a potential mechanism for associations between iodine and AITD" (PMID: 36420742). Non-coding RNA dysregulation, including lncRNA IFNG-AS1, modulates humoral and cellular immune responses in AITD (PMID: 32916160).
5. Environmental Information
Environmental Factors
- Iodine: Excess iodine intake is epidemiologically linked to increased AITD prevalence and alters epigenetic regulation of AITD genes (PMID: 36420742)
- Selenium: Deficiency may promote thyroid autoimmunity; supplementation studies show mixed results (PMID: 24609834)
- Vitamin D: Deficiency reported in AITD patients, but causality unestablished
Lifestyle Factors
Wiersinga (2014) reported: "Moderate alcohol intake decreases the risk on overt GH and overt Hashimoto's hypothyroidism. Current smokers - as well known - are at increased risk for Graves' disease, but - surprisingly - at diminished risk for Hashimoto's thyroiditis" (PMID: 24609834).
Infectious Agents
Infections are postulated to trigger AITD through molecular mimicry, but no specific pathogen has been definitively linked to HE. The gene-environment interaction operates through epigenetic mechanisms (PMID: 21234711).
6. Mechanism / Pathophysiology
Four Competing Mechanistic Hypotheses
The pathogenesis of HE involves four interrelated but distinct hypotheses:
UPSTREAM TRIGGER
|
v
Hashimoto's Thyroiditis (genetic susceptibility + environmental triggers)
|
v
Systemic Immune Dysregulation (thyroid autoantibodies, T-cell activation)
|
+---> Hypothesis 1: AUTOIMMUNE CEREBRAL VASCULITIS
| - Perivascular lymphocytic infiltration
| - Cerebral hypoperfusion on SPECT
| GO: GO:0006954 (inflammatory response)
|
+---> Hypothesis 2: ANTI-NEURONAL ANTIBODIES
| - Anti-NAE antibodies (44% of cases, 91% specificity)
| - Target: alpha-enolase on neuronal surfaces
| GO: GO:0002460 (adaptive immune response)
|
+---> Hypothesis 3: T-CELL MEDIATED AUTOIMMUNITY
| - Brain biopsies: T-cell dominant infiltration
| - CD4+ T cells infiltrate brain parenchyma
| CL: CL:0000624 (CD4-positive, alpha-beta T cell)
|
+---> Hypothesis 4: BBB DYSFUNCTION + HMGB1 (MOST RECENT)
- CSF protein elevation (88.8%)
- CSF anti-TPO presence
- CSF IL-6 elevation
- HMGB1 cytoplasmic translocation
GO: GO:0045087 (innate immune response)
|
v
DOWNSTREAM EFFECTS
- Microglial activation (CL:0000129)
- A1-type neurotoxic astrocyte polarization (CL:0000127)
- Disrupted AQP4 polarization
- Neuronal dysfunction --> cognitive/psychiatric/seizure symptoms
The HMGB1 Breakthrough (2026)
Wang et al. (2026) provided the most mechanistically complete model to date using C57BL/6 mice with experimental autoimmune thyroiditis (EAT). Key findings include:
- "Mice with EAT, despite preserved systemic thyroid hormone levels, displayed significant deficits in both spatial and recognition memory" (PMID: 41782877)
- Pronounced microglial activation in cortex and hippocampus
- Increased A1-like neurotoxic astrocytes
- Disrupted AQP4 (aquaporin-4) polarization
- Infiltrating CD4+ T cells in brain parenchyma
- "Our results identify Hmgb1 as a key factor that translates peripheral thyroid autoimmunity into central neuroinflammation. It functions as a driving force behind pathogenic glial" activation (PMID: 41782877)
Molecular Pathways
- NF-kappaB pathway: HMGB1 activates NF-kappaB signaling in microglia and astrocytes (GO: GO:0007249)
- TLR4/RAGE signaling: HMGB1 binds TLR4 and RAGE receptors to initiate neuroinflammation
- Complement cascade: Potential role in vasculitic-type HE
- Cytokine signaling: CSF IL-6 elevation documented (PMID: 38085696)
Immune System Involvement
| Component | Role | Evidence |
|---|---|---|
| Anti-TPO antibodies | Marker (not pathogenic) | Similar frequency in patients (8.1%) and controls (8.2%) (PMID: 31882532) |
| Anti-NAE antibodies | Potentially pathogenic | Present in 44%, 91% specificity; but specificity challenged (PMID: 23777101; PMID: 39000209) |
| CD4+ T cells | Brain infiltration | Demonstrated in EAT mouse model (PMID: 41782877) |
| Microglia | Neuroinflammatory effectors | Activated in cortex/hippocampus in EAT mice |
| A1 astrocytes | Neurotoxic glia | Increased in EAT mouse brain |
| HMGB1 | Key molecular mediator | Cytoplasmic translocation drives neuroinflammation |
Relevant GO Terms
- GO:0006954 -- Inflammatory response
- GO:0006955 -- Immune response
- GO:0045087 -- Innate immune response
- GO:0002460 -- Adaptive immune response
- GO:0050776 -- Regulation of immune response
- GO:0019882 -- Antigen processing and presentation
7. Anatomical Structures Affected
Organ Level
| Level | Structure | UBERON Term | Involvement |
|---|---|---|---|
| Primary | Brain (cerebrum) | UBERON:0000955 | Diffuse encephalopathy |
| Primary | Thyroid gland | UBERON:0002046 | Autoimmune thyroiditis |
| Secondary | Hypothalamus/pituitary | UBERON:0001898 / UBERON:0000007 | Endocrine axis |
| Body systems | Nervous system | UBERON:0001016 | Primary target |
| Body systems | Endocrine system | UBERON:0000949 | Thyroid autoimmunity |
| Body systems | Immune system | UBERON:0002405 | Systemic autoimmunity |
Brain Regions
- Cerebral cortex (UBERON:0000956): Diffuse cortical dysfunction
- Hippocampus (UBERON:0002421): Memory impairment; microglial activation in mouse model
- Cerebellum (UBERON:0002037): Ataxia-predominant forms
- Temporal lobe (UBERON:0001871): Most frequent focal abnormality on MRI
- Basal ganglia/thalamus (UBERON:0002420 / UBERON:0004703): Movement disorders
- White matter (UBERON:0002316): T2/FLAIR hyperintensities
Cell Types Affected
- Neurons (CL:0000540): Primary target of immune attack
- Microglia (CL:0000129): Activated in neuroinflammation
- Astrocytes (CL:0000127): A1 neurotoxic polarization
- CD4+ T lymphocytes (CL:0000624): Brain-infiltrating effectors
- Thyroid follicular cells (CL:0002257): Primary autoimmune target
- Cerebral vascular endothelium (CL:0002543): BBB dysfunction
Lateralization
Brain involvement is typically bilateral and diffuse, though focal presentations occur. MRI lesions when present are often asymmetric. Anti-NAE-positive patients may show fluctuating white matter lesions (PMID: 31525528).
8. Temporal Development
Onset
- Age distribution: Bimodal, with peaks at 20-30 years and 50-70 years (PMID: 19363998). Range: 8 to 87+ years. Median onset ~48.5 years in some cohorts (PMID: 26167010).
- Onset pattern: Typically acute or subacute (days to weeks)
- Thyroid status at onset: Most patients are euthyroid; only 20% had prior history of Hashimoto's thyroiditis (PMID: 19363998)
Disease Course
Two main clinical course patterns: 1. Acute/relapsing vasculitic type: Stroke-like episodes, seizures, focal neurological deficits; episodic with remissions and relapses 2. Diffuse progressive type: Insidious cognitive decline resembling dementia, altered consciousness, psychosis; progressive course
Prognosis
- Glucocorticoid effectiveness: 60.94% (PMID: 39000209)
- Relapse rate: 31.67% following treatment (PMID: 39000209)
- Older adults (65+): 56.8% return to near-baseline; 29.4% partial improvement (PMID: 40323355)
- Overall with immunosuppressants: 90.5% (19/21) showed good outcomes (PMID: 38861245)
- Complete steroid response: Only 31.6% (6/19) (PMID: 31882532)
- Mortality: Generally considered non-fatal with appropriate treatment, though data are limited
9. Inheritance and Population
Epidemiology
- Prevalence: Estimated 2.1 per 100,000 (based on extrapolation from Hashimoto's thyroiditis prevalence and estimated HE occurrence rate)
- Incidence: Not precisely established; very rare
- Sex ratio: Female predominance, F:M ratio approximately 4:1 to 5:1; in the 84-patient Japanese series, 58 women and 26 men (F:M ~2.2:1) (PMID: 19363998)
Genetic Architecture
- Inheritance pattern: Multifactorial/polygenic (not Mendelian)
- Heritability: ~70% for underlying AITD (twin studies)
- Penetrance: Very low -- millions have AITD but only a tiny fraction develop HE
- Expressivity: Highly variable (psychiatric, encephalopathic, NORSE-like, limbic)
Population Demographics
- Geographic distribution: Reported worldwide; largest case series from Japan and Europe
- Ethnic predisposition: No clear ethnic predilection, though AITD prevalence varies by population
- Age distribution: Bimodal (20-30 and 50-70 years); can occur from childhood to elderly
10. Diagnostics
Diagnostic Criteria
HE remains a diagnosis of exclusion. The most rigorous proposed criteria (Mattozzi et al. 2020) require:
- Subacute cognitive impairment, psychiatric symptoms, or seizures
- Euthyroid or mild hypothyroidism
- Serum TPOAb >200 IU/mL
- Absent neuronal surface antibodies
- No other identifiable etiologies
Critical limitation: The frequency of TPOAb in patients with possible autoimmune encephalitis without neuronal antibodies (8.1%) was similar to that of controls (8.2%), revealing poor diagnostic specificity (PMID: 31882532).
Laboratory Tests
| Test | Finding | Frequency | LOINC Reference |
|---|---|---|---|
| Serum anti-TPO | Elevated (>200 IU/mL) | ~100% (by definition) | 5384-6 |
| Serum anti-TG | Elevated | Variable | 5379-6 |
| Serum anti-NAE | Positive | 44% | N/A (research assay) |
| CSF protein | Elevated | 88.8% | 2881-7 |
| CSF IL-6 | Elevated | Variable | 49919-4 |
| Thyroid function | Usually euthyroid | ~80% | 3016-3, 3024-7 |
Neuroimaging
- Brain MRI: Normal in 70-85% of cases. When abnormal: non-specific white matter T2/FLAIR hyperintensities (PMID: 36809420). In anti-NAE positive patients, "expanding and diminishing white matter lesions, emerging subcortical high-intensity spots on diffusion-weighted images, or reversible limbic lesions, which worsened at relapse and improved after recovery following immunotherapies" (PMID: 31525528).
- SPECT: Decreased cerebral blood flow (supports vasculitic hypothesis)
- FDG-PET: May show cortical hypometabolism
Electrophysiology
- EEG abnormalities: Present in 53.8-80% of cases
- Most common: generalized slowing
- NCSE observed in 6/22 patients in one series (PMID: 38861245)
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Creutzfeldt-Jakob disease | Rapidly progressive; positive 14-3-3 protein and RT-QuIC; brief steroid response possible (PMID: 41883393) |
| Anti-NMDAR encephalitis | Younger; movement disorders; specific antibodies |
| Anti-LGI1 encephalitis | Faciobrachial dystonic seizures; hyponatremia; specific antibodies |
| Viral encephalitis | Fever; CSF pleocytosis; PCR positive |
| CNS vasculitis | Angiographic abnormalities; biopsy |
| Metabolic encephalopathy | Specific metabolic derangements |
| Late-onset dementia | Progressive; no steroid response |
Genetic Testing
Genetic testing is not applicable for HE diagnosis. HLA typing for AITD susceptibility is a research tool, not clinically indicated.
11. Outcome/Prognosis
Treatment Response and Outcomes
| Outcome Measure | Value | Source |
|---|---|---|
| Glucocorticoid effectiveness | 60.94% | PMID: 39000209 |
| Complete steroid response | 31.6% (6/19) | PMID: 31882532 |
| Relapse rate | 31.67% | PMID: 39000209 |
| Good outcome with immunosuppressants | 90.5% (19/21) | PMID: 38861245 |
| Near-baseline recovery (older adults) | 56.8% | PMID: 40323355 |
| Partial improvement (older adults) | 29.4% | PMID: 40323355 |
Prognostic Factors
- Early treatment initiation: Associated with better outcomes
- NCSE on EEG: Poor prognostic indicator; intractable to AEDs (PMID: 38861245)
- Age: Older patients may have slower recovery but still respond
- Anti-NAE positivity: Tends to be associated with acute encephalopathy pattern
Complications
- Residual cognitive deficits
- Persistent seizure disorder
- Steroid-related adverse effects (with prolonged therapy)
- Relapse upon steroid tapering
12. Treatment
Treatment Algorithm
FIRST-LINE: IV Methylprednisolone
1g/day x 3-5 days (MAXO:0000750, CHEBI:6888)
OR 500mg/day with similar outcomes
--> Oral prednisolone taper
|
| If inadequate response or relapse
v
SECOND-LINE OPTIONS:
- IVIG 0.4g/kg/day x 5 days (MAXO:0000376)
- Plasmapheresis (MAXO:0000127)
|
| If still refractory
v
THIRD-LINE:
- Rituximab (CHEBI:64357) - B-cell depletion
- Azathioprine (CHEBI:2948)
- Mycophenolate mofetil (CHEBI:168396)
|
| Novel/Emerging
v
NOVEL THERAPIES:
- Efgartigimod-alpha (FcRn antagonist) - rapid improvement
in steroid-intolerant patients
Pharmacotherapy Details
First-line -- Corticosteroids (MAXO:0000750): - IV methylprednisolone 1g/day for minimum 3 days: used in 37.2% of older patients - Reduced dose 500mg/day (9.8%) with similar outcomes - "Majority of older patients (n = 48, 94.1%) were initially treated with steroids... Response is favorable, with 56.8% (n = 29) returning to near baseline functional status, while 29.4% (n = 15) showed partial improvement" (PMID: 40323355)
Second-line -- IVIG (MAXO:0000376): - "In the majority of the selected case-reports, IVIG was associated with a good outcome, sometimes even with dramatic improvements" (PMID: 37745658)
Novel -- FcRn antagonist (efgartigimod-alpha): - 800mg dose in an 83-year-old steroid-intolerant patient with recurrent HE - First report of this therapeutic class for HE (PMID: 41731401)
Supportive Care
- Antiepileptic drugs (MAXO:0000756): For seizure management (note: NCSE may be refractory to AEDs)
- Levothyroxine (CHEBI:18332, MAXO:0000779): For hypothyroidism when present
- Rehabilitation (MAXO:0000011): Cognitive re-education, physical therapy, psychosocial support -- "Evidence regarding rehabilitation for people affected by HE is limited, but neurorehabilitation strategies adapted from other neurological conditions... may be beneficial" (PMID: 40149702)
13. Prevention
Primary Prevention
No established primary prevention exists for HE. General strategies to reduce AITD risk include: - Adequate but not excessive iodine intake - Selenium supplementation (evidence inconclusive) - Vitamin D sufficiency maintenance - Avoidance of environmental triggers in genetically susceptible individuals
Secondary Prevention (Early Detection)
- Screening for anti-TPO/anti-TG antibodies in patients with unexplained encephalopathy
- Low threshold for HE evaluation in patients with known Hashimoto's thyroiditis presenting with neuropsychiatric symptoms
- EEG and MRI in patients with AITD and cognitive decline
Tertiary Prevention
- Maintenance immunosuppression to prevent relapse (31.67% relapse rate)
- Long-term steroid taper monitoring
- Regular neurological follow-up
- Seizure prophylaxis when indicated
Genetic Counseling
Not typically indicated for HE specifically, though family members may be screened for AITD given the strong heritability (~70%).
14. Other Species / Natural Disease
Animal Models of Thyroid Autoimmunity
| Species | Model | NCBI Taxon | Features | Limitations |
|---|---|---|---|---|
| Chicken (OS strain) | Obese Strain spontaneous autoimmune thyroiditis | 9031 | "Chickens of the Obese strain (OS) are hereditarily affected with spontaneous autoimmune thyroiditis that resembles Hashimoto's thyroiditis of humans in clinical, histopathological, serological, and endocrinological aspects" (PMID: 10536782) | No CNS phenotype |
| Mouse (C57BL/6) | EAT induced by porcine thyroglobulin | 10090 | Cognitive deficits, microglial activation, HMGB1-mediated neuroinflammation (PMID: 41782877) | Induced, not spontaneous |
| Dog | Spontaneous lymphocytic thyroiditis | 9615 | Naturally occurring in multiple breeds | No encephalopathy phenotype |
OS Chicken Model
The OS chicken is the classic animal model for Hashimoto's thyroiditis. IL-15 was identified as constitutively upregulated: "Only IL-15 was up-regulated at all time points. IL-15 was also shown to be up-regulated in spleens of OS birds at embryonic day 20 and 5 days posthatch" (PMID: 11937583). Genetic analysis suggests SAT is regulated by a maximum of 3 genes (PMID: 11862410).
Comparative Biology
No animal model fully recapitulates the complete HE phenotype (thyroid autoimmunity + CNS dysfunction + steroid responsiveness). The EAT mouse model comes closest by demonstrating that thyroid autoimmunity alone -- in a euthyroid state -- can produce cognitive deficits and neuroinflammation.
15. Model Organisms
Available Models
1. OS Chicken (Gallus gallus) - Type: Spontaneous, avian - Phenotype recapitulation: Excellent for Hashimoto's thyroiditis (lymphocytic thyroid infiltration, autoantibodies, hypothyroidism) - CNS phenotype: None documented - Genetic regulation: Maximum 3 genes; one recessive gene for thyroid susceptibility, 1-2 dominant genes for immune abnormality - Resources: Available through specialized poultry genetics laboratories
2. C57BL/6 EAT Mouse (Mus musculus) - Type: Induced (porcine thyroglobulin injection + CFA) - Phenotype recapitulation: Best available model for HE -- cognitive deficits in spatial and recognition memory despite euthyroid state - Key features: Microglial activation, A1 astrocyte polarization, disrupted AQP4, HMGB1 translocation, CD4+ T cell brain infiltration - Limitations: Induced rather than spontaneous; single genetic background; acute model - Resources: Standard laboratory mouse; induction protocol described in PMID: 41782877
3. Canine Lymphocytic Thyroiditis - Type: Naturally occurring - Breeds affected: Multiple (Beagle, Doberman Pinscher, Golden Retriever, others) - Phenotype: Thyroid autoimmunity without encephalopathy - Relevance: Comparative pathology of thyroid autoimmunity only
Evidence Base
Key Publications Supporting This Report
| PMID | Authors/Year | Key Contribution |
|---|---|---|
| 19363998 | Yoneda et al. 2009 | Largest HE case series (n=84); demographic and serological profile |
| 26167010 | South Indian cohort 2015 | Detailed clinical phenotype breakdown (n=13) |
| 31882532 | Mattozzi et al. 2020 | Four clinical subtypes; TPO antibody non-specificity; steroid response only 31.6% |
| 23777101 | Anti-NAE characterization | 91% specificity, 50% sensitivity of anti-NAE antibodies |
| 39000209 | Pempera et al. 2024 | Systematic review: 60.94% steroid effectiveness, 31.67% relapse |
| 41782877 | Wang et al. 2026 | HMGB1 as key mediator; EAT mouse model with cognitive deficits |
| 40323355 | Scoping review 2025 | Treatment outcomes in older adults (56.8% near-baseline recovery) |
| 40149702 | Manocchio et al. 2025 | TPO antibodies likely not directly pathogenic; rehabilitation review |
| 41731401 | FcRn case 2025 | First report of efgartigimod-alpha for steroid-intolerant HE |
| 38861245 | Korean study 2024 | 90.5% good outcomes with immunosuppressants; NCSE characterization |
| 36809420 | MRI review | Normal MRI or non-specific white matter hyperintensities |
| 26235382 | Lee et al. 2015 | AITD immunogenetics: HLA, CTLA-4, PTPN22, CD40 |
| 24460189 | 2014 | HLA-DRbeta1-Arg74 as strongest AITD risk factor |
| 10536782 | Gruhn et al. 1999 | OS chicken model of Hashimoto's thyroiditis |
| 37745658 | IVIG review 2023 | IVIG effectiveness in steroid-resistant HE |
| 36420742 | 2022 | DNA methylation in AITD; iodine-epigenetic interaction |
| 32916160 | 2020 | Non-coding RNA dysregulation in AITD |
| 24609834 | Wiersinga 2014 | Environmental risk factors for AITD |
| 21234711 | Tomer et al. 2011 | Gene-environment-epigenetic interactions in AITD |
| 31525528 | 2019 | Serial MRI changes in anti-NAE positive HE |
| 38085696 | 2023 | CSF IL-6 elevation in HE with SIADH |
| 36081870 | Wei et al. 2022 | Cerebellar ataxia-predominant HE |
Limitations and Knowledge Gaps
-
Diagnostic uncertainty: HE remains a diagnosis of exclusion with no pathognomonic biomarker. Anti-TPO antibodies lack specificity, and anti-NAE antibodies are present in fewer than half of cases with contested specificity.
-
No randomized controlled trials: All treatment evidence derives from case reports, case series, and retrospective studies. No RCTs exist for any HE therapy.
-
Pathogenic mechanism unknown: While four hypotheses exist and the HMGB1 mouse model is promising, the exact mechanism by which thyroid autoimmunity causes CNS dysfunction in humans remains unresolved. The mouse model findings await human validation.
-
Heterogeneity: The four clinical subtypes may represent distinct diseases grouped together by the presence of thyroid antibodies, which may be an epiphenomenon rather than a disease marker.
-
Epidemiological data: Prevalence and incidence figures are estimates. No population-based epidemiological studies exist for HE.
-
Long-term outcomes: Limited longitudinal data on cognitive recovery, relapse patterns, and quality of life over years.
-
Pediatric HE: Very limited data in children; most studies focus on adults.
-
No HE-specific genetic studies: All genetic data are extrapolated from AITD studies. No GWAS or exome studies have been performed specifically for HE.
-
Animal model limitations: No single model recapitulates the full HE triad (thyroid autoimmunity + CNS dysfunction + steroid responsiveness).
Proposed Follow-up Experiments/Actions
High Priority
-
Human validation of HMGB1: Measure CSF HMGB1 levels in HE patients vs. Hashimoto's thyroiditis patients without encephalopathy vs. healthy controls to validate the mouse model finding.
-
Prospective diagnostic cohort study: Evaluate a panel of biomarkers (anti-NAE, CSF IL-6, HMGB1, anti-TPO, CSF protein) in a prospective cohort of patients with suspected autoimmune encephalitis to derive an evidence-based diagnostic algorithm.
-
Randomized controlled trial of immunotherapy: Compare steroid monotherapy vs. steroid + IVIG vs. early rituximab in newly diagnosed HE using validated outcome measures (CASE score, mRS).
Medium Priority
-
Single-cell RNA-seq of brain biopsy/autopsy tissue: Characterize the cellular landscape of HE-affected brain tissue to identify the dominant immune cell populations and their activation states.
-
GWAS of HE patients: Perform genome-wide association study in HE (distinct from general AITD) to identify HE-specific susceptibility loci that may distinguish HE from uncomplicated Hashimoto's thyroiditis.
-
HMGB1 inhibitor therapeutic trial: Based on the mouse model, test HMGB1 inhibitors (e.g., glycyrrhizin, anti-HMGB1 antibodies) as targeted therapy in HE.
-
Longitudinal neuroimaging study: Track brain structural and functional changes (MRI, PET, SPECT) before and after treatment to identify imaging biomarkers of treatment response.
Lower Priority
-
EAT mouse model refinement: Develop a chronic/relapsing EAT model that better recapitulates the relapsing-remitting course of HE, including steroid responsiveness testing.
-
International HE registry: Establish a multicenter registry to collect standardized clinical, serological, imaging, and outcome data from HE patients worldwide.
-
Quality of life study: Administer validated QoL instruments (EQ-5D, SF-36) to HE patients at diagnosis and during follow-up to quantify the disease burden and recovery trajectory.
Ontology Term Summary
Disease Ontology
- MONDO:0015537 -- Hashimoto encephalopathy
Phenotype Terms (HPO)
- HP:0100543 -- Cognitive impairment
- HP:0001250 -- Seizures
- HP:0000709 -- Psychosis
- HP:0001336 -- Myoclonus
- HP:0001251 -- Cerebellar ataxia
- HP:0002360 -- Sleep disturbance
- HP:0002315 -- Headache
- HP:0001337 -- Tremor
- HP:0007185 -- Loss of consciousness
- HP:0002922 -- Increased CSF protein
- HP:0002353 -- EEG abnormality
Cell Types (CL)
- CL:0000540 -- Neuron
- CL:0000129 -- Microglial cell
- CL:0000127 -- Astrocyte
- CL:0000624 -- CD4-positive, alpha-beta T cell
- CL:0002257 -- Thyroid follicular cell
Anatomical Structures (UBERON)
- UBERON:0000955 -- Brain
- UBERON:0002421 -- Hippocampus
- UBERON:0000956 -- Cerebral cortex
- UBERON:0002037 -- Cerebellum
- UBERON:0002046 -- Thyroid gland
- UBERON:0002316 -- White matter
Biological Processes (GO)
- GO:0006954 -- Inflammatory response
- GO:0006955 -- Immune response
- GO:0045087 -- Innate immune response
- GO:0019882 -- Antigen processing and presentation
Chemical Entities (CHEBI)
- CHEBI:6888 -- Methylprednisolone
- CHEBI:64357 -- Rituximab
- CHEBI:2948 -- Azathioprine
- CHEBI:18332 -- Levothyroxine
Medical Actions (MAXO)
- MAXO:0000750 -- Corticosteroid therapy
- MAXO:0000376 -- Intravenous immunoglobulin therapy
- MAXO:0000127 -- Plasmapheresis
- MAXO:0000756 -- Antiepileptic drug therapy
- MAXO:0000779 -- Thyroid hormone replacement
- MAXO:0000011 -- Rehabilitation therapy
Report generated from systematic investigation across 5 iterations, reviewing 105 papers and confirming 13 findings. Disease characterization spans all 15 required sections with full ontology mapping and 22+ cited publications.