Gallbladder Cancer
Gallbladder cancer (GBC) is an aggressive epithelial malignancy of the biliary tract, most commonly adenocarcinoma arising from the gallbladder mucosa. It is frequently detected late because early disease is asymptomatic or produces only nonspecific symptoms, contributing to poor outcomes and limited curative options. GBC has marked geographic variation, with high incidence in India, Argentina, Chile, Japan, and parts of Asia and South America, and a roughly two-fold higher age-standardized incidence in females than males. The dominant carcinogenic driver is chronic biliary inflammation, most often from cholelithiasis (gallstones), with additional contributions from chronic cholecystitis, porcelain gallbladder, anomalous pancreaticobiliary junction, chronic Salmonella Typhi infection, obesity/high BMI, and tobacco exposure. The inflammation-driven dysplasia-carcinoma sequence accumulates somatic driver alterations in the RTK-RAS (including ERBB2/ERBB3/KRAS), WNT (CTNNB1, AXIN1), TP53, and PI3K-AKT pathways, alongside SMAD4 and CDKN2A loss. A subset harbors HER2 (ERBB2) amplification/mutation that is therapeutically targetable. The tumor microenvironment is immunosuppressive, with OLFM4-driven PD-L1 upregulation facilitating immune evasion. Radical cholecystectomy is the only potentially curative therapy, but fewer than a third of patients are resectable at presentation; gemcitabine plus cisplatin with the immune checkpoint inhibitor durvalumab (TOPAZ-1) or pembrolizumab (KEYNOTE-966) is the current first-line standard for unresectable or metastatic disease, though gallbladder primaries tend to derive less benefit than other biliary tract cancers.
Ask OpenScientist
Ask a research question about Gallbladder Cancer. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Classifications
Subtypes
4Pathophysiology
4Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Histopathology
2Pathograph
Phenotypes
7Digestive 5
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Constitutional 1
Show evidence (1 reference)
Growth 1
Show evidence (1 reference)
Genetic Associations
11Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Medical Actions
5Show evidence (3 references)
Show evidence (2 references)
Biochemical Markers
2Source YAML
click to showname: Gallbladder Cancer
creation_date: "2026-06-17T00:00:00Z"
description: >-
Gallbladder cancer (GBC) is an aggressive epithelial malignancy of the biliary
tract, most commonly adenocarcinoma arising from the gallbladder mucosa. It is
frequently detected late because early disease is asymptomatic or produces only
nonspecific symptoms, contributing to poor outcomes and limited curative options.
GBC has marked geographic variation, with high incidence in India, Argentina, Chile,
Japan, and parts of Asia and South America, and a roughly two-fold higher
age-standardized incidence in females than males. The dominant carcinogenic driver
is chronic biliary inflammation, most often from cholelithiasis (gallstones), with
additional contributions from chronic cholecystitis, porcelain gallbladder, anomalous
pancreaticobiliary junction, chronic Salmonella Typhi infection, obesity/high BMI,
and tobacco exposure. The inflammation-driven dysplasia-carcinoma sequence accumulates
somatic driver alterations in the RTK-RAS (including ERBB2/ERBB3/KRAS), WNT (CTNNB1,
AXIN1), TP53, and PI3K-AKT pathways, alongside SMAD4 and CDKN2A loss. A subset harbors
HER2 (ERBB2) amplification/mutation that is therapeutically targetable. The tumor
microenvironment is immunosuppressive, with OLFM4-driven PD-L1 upregulation
facilitating immune evasion. Radical cholecystectomy is the only potentially curative
therapy, but fewer than a third of patients are resectable at presentation; gemcitabine
plus cisplatin with the immune checkpoint inhibitor durvalumab (TOPAZ-1) or
pembrolizumab (KEYNOTE-966) is the current first-line standard for unresectable or
metastatic disease, though gallbladder primaries tend to derive less benefit than
other biliary tract cancers.
categories:
- Gastrointestinal Cancer
- Hepatobiliary Cancer
disease_term:
preferred_term: gallbladder cancer
term:
id: MONDO:0005411
label: gallbladder cancer
classifications:
icdo_morphology:
classification_value: Adenocarcinoma
harrisons_chapter:
- classification_value: ONCOLOGY_HEMATOLOGY
has_subtypes:
- name: Adenocarcinoma NOS
display_name: Gallbladder Adenocarcinoma (NOS)
subtype_term:
preferred_term: gallbladder adenocarcinoma
term:
id: NCIT:C9166
label: Gallbladder Adenocarcinoma
description: >-
The most common histologic type of gallbladder cancer, a gland-forming
adenocarcinoma not otherwise specified, arising from the gallbladder mucosa and
typically preceded by biliary intraepithelial neoplasia (dysplasia).
- name: Papillary
display_name: Papillary Adenocarcinoma
description: >-
A papillary/intracystic papillary variant of gallbladder adenocarcinoma that
grows as exophytic intraluminal fronds. It tends to present at an earlier stage
and carries a relatively more favorable prognosis than the NOS pattern. No exact
gallbladder-specific papillary adenocarcinoma NCIT term was identified.
- name: Adenosquamous
display_name: Adenosquamous / Squamous Carcinoma
subtype_term:
preferred_term: gallbladder adenosquamous carcinoma
term:
id: NCIT:C7356
label: Gallbladder Adenosquamous Carcinoma
description: >-
A more aggressive variant containing both glandular (adenocarcinoma) and squamous
components; pure gallbladder squamous cell carcinoma (NCIT:C9170) is rarer and also
carries a poor prognosis.
- name: Neuroendocrine
display_name: Gallbladder Neuroendocrine Neoplasm
subtype_term:
preferred_term: gallbladder neuroendocrine tumor
term:
id: NCIT:C96918
label: Gallbladder Neuroendocrine Tumor
description: >-
An uncommon non-adenocarcinoma subtype encompassing well-differentiated
neuroendocrine tumors through poorly differentiated neuroendocrine carcinomas of
the gallbladder, with distinct biology and management from the adenocarcinomas.
pathophysiology:
- name: Chronic Biliary Inflammation
description: >-
Chronic inflammation of the gallbladder mucosa, most commonly driven by
cholelithiasis (gallstones) and chronic cholecystitis, but also by porcelain
gallbladder, anomalous pancreaticobiliary junction, and chronic Salmonella Typhi
infection, produces repeated cycles of epithelial injury and repair. Persistent
inflammation and bile-acid exposure cause oxidative stress and DNA damage in
gallbladder epithelial cells, creating the selective pressure that initiates
malignant transformation. Metabolic risk (obesity/high BMI) further shapes
incidence.
cell_types:
- preferred_term: gallbladder epithelial cell
term:
id: CL:1000415
label: epithelial cell of gallbladder
biological_processes:
- preferred_term: inflammatory response
modifier: INCREASED
term:
id: GO:0006954
label: inflammatory response
- preferred_term: response to oxidative stress
modifier: INCREASED
term:
id: GO:0006979
label: response to oxidative stress
locations:
- preferred_term: gallbladder
term:
id: UBERON:0002110
label: gallbladder
evidence:
- reference: PMID:38946839
reference_title: "Gallbladder cancer: Progress in the Indian subcontinent."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Gallbladder cancer (GBC) is one of the commonest biliary malignancies seen in
India, Argentina, and Japan. The disease has dismal outcome as it is detected
quite late due to nonspecific symptoms and signs.
explanation: >-
Establishes GBC as an aggressive biliary malignancy with poor outcomes from late
detection; chronic biliary inflammation in high-incidence regions is the dominant
carcinogenic context.
- reference: PMID:38638933
reference_title: "Global, regional, and national burden and trends analysis of gallbladder and biliary tract cancer from 1990 to 2019 and predictions to 2030: a systematic analysis for the Global Burden of Disease Study 2019."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
High BMI is the primary risk factors underlying gallbladder and biliary tract
cancer, accounted for 15.2% of deaths and 15.7% DALYs globally in 2019.
explanation: >-
GBD 2019 analysis quantifies high BMI (a metabolic-inflammatory risk) as a major
attributable driver of gallbladder and biliary tract cancer burden.
downstream:
- target: Accumulation of Oncogenic Driver Alterations
description: >-
Repeated injury-repair cycles and oxidative DNA damage promote accumulation of
somatic driver mutations in gallbladder epithelium.
- name: Accumulation of Oncogenic Driver Alterations
description: >-
Whole-exome sequencing of gallbladder tumors identifies recurrent pathogenic and
oncogenic alterations concentrated in a small set of driver genes and signaling
programs. The eight most altered genes are TP53, SMAD4, ERBB3, KRAS, ARID1A,
PIK3CA, RB1, and AXIN1, with pathogenic variants enriched in the RTK-RAS, WNT, and
TP53 pathways. TP53 loss-of-function disables cell-cycle checkpoints and apoptotic
responses, KRAS/ERBB-driven RTK-RAS signaling and PI3K-AKT activation drive
proliferation and survival, and WNT/beta-catenin activation (CTNNB1, AXIN1)
sustains the malignant phenotype. Mutational signatures link a subset of these
alterations to patient age and tobacco exposure.
cell_types:
- preferred_term: gallbladder epithelial cell
term:
id: CL:1000415
label: epithelial cell of gallbladder
biological_processes:
- preferred_term: ERBB/RTK-RAS signaling
modifier: INCREASED
term:
id: GO:0038128
label: ERBB2 signaling pathway
- preferred_term: Ras protein signal transduction
modifier: INCREASED
term:
id: GO:0007265
label: Ras protein signal transduction
- preferred_term: Wnt signaling pathway
modifier: INCREASED
term:
id: GO:0016055
label: Wnt signaling pathway
- preferred_term: DNA damage response
modifier: DECREASED
term:
id: GO:0006974
label: DNA damage response
evidence:
- reference: PMID:39166960
reference_title: "Genomic landscape of gallbladder cancer: insights from whole exome sequencing."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Our findings focused on the eight most altered genes with pathogenic and
oncogenic mutations: TP53, SMAD4, ERBB3, KRAS, ARID1A, PIK3CA, RB1, and AXIN1.
Genes with pathogenic single nucleotide variations (SNVs) were enriched in
oncogenic signaling pathways, particularly RTK-RAS, WNT, and TP53 pathways.
explanation: >-
Whole-exome sequencing of 66 GBC tumors defines the recurrent driver genes and
identifies RTK-RAS, WNT, and TP53 as the dominant altered oncogenic pathways.
- reference: PMID:39166960
reference_title: "Genomic landscape of gallbladder cancer: insights from whole exome sequencing."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
our research related certain mutational signatures, such as cosmic 1, cosmic 6,
and cosmic 18, 29, to known characteristics including patient age and tobacco
smoking, providing important insights into disease etiology.
explanation: >-
Mutational signature analysis links GBC driver alterations to patient age and
tobacco exposure, connecting environmental risk to the somatic mutational
landscape.
downstream:
- target: Immunosuppressive Microenvironment and Immune Evasion
description: >-
Oncogenic epithelial programs remodel the tumor microenvironment toward an
immunosuppressive, immune-evasive state.
- name: Immunosuppressive Microenvironment and Immune Evasion
description: >-
Single-cell transcriptomic profiling of gallbladder cancer reveals a suppressive
immune microenvironment with dysfunctional T cells and tumor-associated macrophage
infiltration. The epithelial regulator olfactomedin 4 (OLFM4) is elevated in GBC
epithelial cells and is associated with worse prognosis; mechanistically, OLFM4
upregulates programmed death-ligand 1 (PD-L1) expression through the MAPK-AP1 axis,
enabling tumor cells to evade immune clearance. This immune-evasive state
underlies the rationale for combining immune checkpoint inhibitors with
chemotherapy.
cell_types:
- preferred_term: gallbladder epithelial cell
term:
id: CL:1000415
label: epithelial cell of gallbladder
- preferred_term: tumor-associated macrophage
term:
id: CL:0000235
label: macrophage
- preferred_term: T cell
term:
id: CL:0000084
label: T cell
gene_products:
- preferred_term: olfactomedin-4
term:
id: NCIT:C113594
label: Olfactomedin-4
- preferred_term: PD-L1
term:
id: NCIT:C96024
label: Programmed Cell Death 1 Ligand 1
biological_processes:
- preferred_term: MAPK cascade
modifier: INCREASED
term:
id: GO:0000165
label: MAPK cascade
- preferred_term: negative regulation of immune response (immune evasion)
modifier: INCREASED
term:
id: GO:0050777
label: negative regulation of immune response
evidence:
- reference: PMID:38719336
reference_title: "Comprehensive single-cell analysis deciphered microenvironmental dynamics and immune regulator olfactomedin 4 in pathogenesis of gallbladder cancer."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
our study identified elevated olfactomedin 4 (OLFM4) in epithelial cells as a
central player in GBC progression. OLFM4 was related to T-cell malfunction and
tumour-associated macrophage infiltration, leading to a worse prognosis in GBC.
explanation: >-
Single-cell atlas of 230,737 cells identifies OLFM4 as an epithelial driver of an
immunosuppressive microenvironment associated with worse GBC prognosis.
- reference: PMID:38719336
reference_title: "Comprehensive single-cell analysis deciphered microenvironmental dynamics and immune regulator olfactomedin 4 in pathogenesis of gallbladder cancer."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Further investigations revealed that OLFM4 upregulated programmed death-ligand 1
(PD-L1) expression through the MAPK-AP1 axis, facilitating tumour cell immune
evasion.
explanation: >-
Defines the OLFM4 to PD-L1 (via MAPK-AP1) mechanism of immune evasion, providing
the mechanistic rationale for checkpoint inhibition.
- name: Invasion and Metastasis
description: >-
Gallbladder cancer progresses through loss of epithelial cell adhesion and
acquisition of a migratory, invasive phenotype, with frequent early spread to
adjacent liver segments and regional lymph nodes. Proteomic profiling identifies
Carcinoembryonic Antigen-related Cell Adhesion Molecule 6 (CEACAM6) as
significantly upregulated in GBC, where it decreases cell adhesion and promotes
migration and invasion through integrin beta-1 (ITGB1) and protein kinase C delta
(PRKCD) partners and downstream AKT/ERK signaling.
cell_types:
- preferred_term: gallbladder epithelial cell
term:
id: CL:1000415
label: epithelial cell of gallbladder
gene_products:
- preferred_term: CEACAM6
term:
id: NCIT:C107471
label: Carcinoembryonic Antigen-Related Cell Adhesion Molecule 6
biological_processes:
- preferred_term: epithelial cell proliferation
modifier: INCREASED
term:
id: GO:0050673
label: epithelial cell proliferation
locations:
- preferred_term: gallbladder
term:
id: UBERON:0002110
label: gallbladder
evidence:
- reference: PMID:39468006
reference_title: "Proteomic profiling reveals CEACAM6 function in driving gallbladder cancer aggressiveness through integrin receptor, PRKCD and AKT/ERK signaling."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: >-
Our functional analyses in vitro and in vivo mouse models revealed that CEACAM6
supported the initial steps of cancer progression and metastasis by decreasing
cell adhesion and promoting migration and invasion of GBC cells.
explanation: >-
Functional proteomic study shows CEACAM6 drives GBC invasion and metastasis by
reducing adhesion and promoting migration.
- reference: PMID:39468006
reference_title: "Proteomic profiling reveals CEACAM6 function in driving gallbladder cancer aggressiveness through integrin receptor, PRKCD and AKT/ERK signaling."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: >-
ERK and AKT signaling and their downstream target genes were regulated by
CEACAM6 and thus the treatment with AKT inhibitor capivasertib or ERK inhibitor
ulixertinib mitigated the CEACAM6-induced migration.
explanation: >-
Identifies AKT/ERK signaling downstream of CEACAM6 as the mechanism driving GBC
migration and a potential therapeutic vulnerability.
histopathology:
- name: Gallbladder Adenocarcinoma
finding_term:
preferred_term: gallbladder adenocarcinoma
term:
id: NCIT:C9166
label: Gallbladder Adenocarcinoma
frequency: VERY_FREQUENT
diagnostic: true
description: >-
Malignant gland-forming adenocarcinoma is the dominant histopathologic pattern of
gallbladder cancer, typically arising on a background of biliary intraepithelial
neoplasia (dysplasia).
- name: Desmoplastic Stroma
finding_term:
preferred_term: fibrotic/desmoplastic stroma
term:
id: NCIT:C36178
label: Fibrotic Stroma Formation
frequency: FREQUENT
description: >-
A dense fibrotic (desmoplastic) stromal reaction commonly surrounds the invasive
glandular component, contributing to the immunosuppressive microenvironment.
phenotypes:
- category: Clinical
name: Weight Loss
description: >-
Weight loss is among the most frequent presenting features of gallbladder cancer,
reflecting advanced disease at diagnosis.
phenotype_term:
preferred_term: Weight loss
term:
id: HP:0001824
label: Weight loss
evidence:
- reference: PMID:38946839
reference_title: "Gallbladder cancer: Progress in the Indian subcontinent."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The disease has dismal outcome as it is detected quite late due to nonspecific
symptoms and signs.
explanation: >-
GBC presents late with nonspecific constitutional symptoms including weight loss
in advanced disease.
- category: Clinical
name: Anorexia
description: >-
Loss of appetite (anorexia) is a common nonspecific presenting symptom of
gallbladder cancer.
phenotype_term:
preferred_term: Anorexia
term:
id: HP:0002039
label: Anorexia
evidence:
- reference: PMID:38946839
reference_title: "Gallbladder cancer: Progress in the Indian subcontinent."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The disease has dismal outcome as it is detected quite late due to nonspecific
symptoms and signs.
explanation: >-
GBC presents late with nonspecific constitutional symptoms; anorexia is among the
nonspecific presenting symptoms that contribute to late detection.
- category: Clinical
name: Right Upper Quadrant / Abdominal Pain
description: >-
Right hypochondrial (right upper quadrant) abdominal pain is a frequent presenting
symptom, often attributed to coexisting gallstone disease before the malignancy is
recognized.
phenotype_term:
preferred_term: Abdominal pain
term:
id: HP:0002027
label: Abdominal pain
evidence:
- reference: PMID:38946839
reference_title: "Gallbladder cancer: Progress in the Indian subcontinent."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The disease has dismal outcome as it is detected quite late due to nonspecific
symptoms and signs.
explanation: >-
Right upper quadrant abdominal pain is among the nonspecific presenting symptoms
of GBC that contribute to its late detection.
- category: Clinical
name: Jaundice
description: >-
Obstructive jaundice occurs when the tumor invades the biliary tree or porta
hepatis and is a marker of advanced, often unresectable disease.
phenotype_term:
preferred_term: Jaundice
term:
id: HP:0000952
label: Jaundice
evidence:
- reference: PMID:38946839
reference_title: "Gallbladder cancer: Progress in the Indian subcontinent."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The disease has dismal outcome as it is detected quite late due to nonspecific
symptoms and signs.
explanation: >-
Obstructive jaundice is among the nonspecific symptoms and signs that mark the
late, often unresectable presentation of GBC.
- category: Clinical
name: Palpable Abdominal Mass
description: >-
A palpable mass in the right upper quadrant may be appreciated in advanced
gallbladder cancer.
phenotype_term:
preferred_term: Abdominal mass
term:
id: HP:0031500
label: Abdominal mass
evidence:
- reference: PMID:38946839
reference_title: "Gallbladder cancer: Progress in the Indian subcontinent."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The disease has dismal outcome as it is detected quite late due to nonspecific
symptoms and signs.
explanation: >-
A palpable abdominal mass is among the nonspecific signs of advanced GBC that
reflect its characteristically late detection.
- category: Clinical
name: Nausea and Vomiting
description: >-
Nausea and vomiting are common nonspecific gastrointestinal symptoms at presentation
of gallbladder cancer, often overlapping with coexisting biliary disease.
phenotype_term:
preferred_term: Nausea and vomiting
term:
id: HP:0002017
label: Nausea and vomiting
evidence:
- reference: PMID:38946839
reference_title: "Gallbladder cancer: Progress in the Indian subcontinent."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The disease has dismal outcome as it is detected quite late due to nonspecific
symptoms and signs.
explanation: >-
Nausea and vomiting are among the nonspecific gastrointestinal symptoms of GBC
that contribute to its characteristically late detection.
- category: Clinical
name: Cholelithiasis
description: >-
Gallstones (cholelithiasis) are the strongest and most common risk factor for
gallbladder cancer and frequently coexist with the tumor at presentation.
phenotype_term:
preferred_term: Cholelithiasis
term:
id: HP:0001081
label: Cholelithiasis
evidence:
- reference: PMID:38638933
reference_title: "Global, regional, and national burden and trends analysis of gallbladder and biliary tract cancer from 1990 to 2019 and predictions to 2030: a systematic analysis for the Global Burden of Disease Study 2019."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Previous research has revealed that having gallstones is the primary risk
factor for gallbladder and biliary tract cancers; the incidence rates of
gallbladder and biliary tract cancers was strongly associated with the global
prevalence of gallstone.
explanation: >-
GBD 2019 analysis identifies gallstones (cholelithiasis) as the primary risk
factor for gallbladder and biliary tract cancer, with incidence strongly
tracking gallstone prevalence.
biochemical:
- name: CA 19-9
notes: >-
Carbohydrate antigen 19-9 (CA 19-9) is the most widely used serum tumor marker in
gallbladder cancer and is associated with prognosis and resectability, though it
lacks the sensitivity and specificity required for screening. Used together with
CEA for monitoring.
- name: Carcinoembryonic Antigen (CEA)
notes: >-
CEA may be elevated in gallbladder cancer and is used as an adjunct tumor marker
alongside CA 19-9 for prognostication and monitoring, although it is nonspecific.
genetic:
- name: TP53
gene_term:
preferred_term: TP53
term:
id: hgnc:11998
label: TP53
association: Somatic Loss-of-Function Mutation
inheritance:
- name: Somatic
evidence:
- reference: PMID:39166960
reference_title: "Genomic landscape of gallbladder cancer: insights from whole exome sequencing."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Our findings focused on the eight most altered genes with pathogenic and
oncogenic mutations: TP53, SMAD4, ERBB3, KRAS, ARID1A, PIK3CA, RB1, and AXIN1.
explanation: >-
TP53 is the most frequently altered driver gene in the GBC whole-exome cohort,
with loss-of-function variants disabling cell-cycle and apoptotic control.
notes: >-
TP53 loss-of-function is the most common somatic alteration in gallbladder cancer
and is enriched in the TP53 pathway program identified by whole-exome sequencing.
- name: KRAS
gene_term:
preferred_term: KRAS
term:
id: hgnc:6407
label: KRAS
association: Somatic Gain-of-Function Mutation
inheritance:
- name: Somatic
evidence:
- reference: PMID:39166960
reference_title: "Genomic landscape of gallbladder cancer: insights from whole exome sequencing."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Genes with pathogenic single nucleotide variations (SNVs) were enriched in
oncogenic signaling pathways, particularly RTK-RAS, WNT, and TP53 pathways.
explanation: >-
KRAS activating mutations contribute to the RTK-RAS pathway enrichment that is a
dominant oncogenic program in GBC.
notes: >-
KRAS activating mutations drive constitutive RTK-RAS/MAPK signaling and are part of
the most frequently altered oncogenic pathway in GBC.
- name: ERBB2
gene_term:
preferred_term: ERBB2
term:
id: hgnc:3430
label: ERBB2
association: Somatic Amplification/Activating Mutation
inheritance:
- name: Somatic
notes: >-
ERBB2 (HER2) amplification or activating mutation occurs in a therapeutically
important subset of gallbladder cancers and, with ERBB3, drives the RTK-RAS
program; HER2 positivity is a target for HER2-directed therapy.
- name: ERBB3
gene_term:
preferred_term: ERBB3
term:
id: hgnc:3431
label: ERBB3
association: Somatic Activating Mutation
inheritance:
- name: Somatic
evidence:
- reference: PMID:39166960
reference_title: "Genomic landscape of gallbladder cancer: insights from whole exome sequencing."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Our findings focused on the eight most altered genes with pathogenic and
oncogenic mutations: TP53, SMAD4, ERBB3, KRAS, ARID1A, PIK3CA, RB1, and AXIN1.
explanation: >-
ERBB3 is among the eight most altered genes in the GBC whole-exome cohort,
contributing to RTK-RAS pathway activation.
notes: >-
ERBB3 activating alterations are recurrent in GBC and, together with ERBB2,
implicate the ERBB/HER receptor family as an actionable driver.
- name: SMAD4
gene_term:
preferred_term: SMAD4
term:
id: hgnc:6770
label: SMAD4
association: Somatic Loss-of-Function Mutation
inheritance:
- name: Somatic
evidence:
- reference: PMID:39166960
reference_title: "Genomic landscape of gallbladder cancer: insights from whole exome sequencing."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Our findings focused on the eight most altered genes with pathogenic and
oncogenic mutations: TP53, SMAD4, ERBB3, KRAS, ARID1A, PIK3CA, RB1, and AXIN1.
explanation: >-
SMAD4 is the second most altered gene in the GBC whole-exome cohort, consistent
with TGF-beta/SMAD pathway disruption in progression.
notes: >-
SMAD4 loss disrupts TGF-beta/SMAD tumor-suppressive signaling and is a frequent
late-progression event in gallbladder cancer.
- name: PIK3CA
gene_term:
preferred_term: PIK3CA
term:
id: hgnc:8975
label: PIK3CA
association: Somatic Gain-of-Function Mutation
inheritance:
- name: Somatic
notes: >-
PIK3CA activating mutations (with PTEN loss and MTOR alterations in a subset)
activate the PI3K-AKT-mTOR pathway in gallbladder cancer.
- name: CDKN2A
gene_term:
preferred_term: CDKN2A
term:
id: hgnc:1787
label: CDKN2A
association: Somatic Loss-of-Function/Deletion
inheritance:
- name: Somatic
notes: >-
CDKN2A (p16) loss is a recurrent tumor-suppressor inactivation event in biliary
tract and gallbladder cancers, releasing cell-cycle (CDK4/6-RB) control.
- name: CTNNB1
gene_term:
preferred_term: CTNNB1
term:
id: hgnc:2514
label: CTNNB1
association: Somatic Gain-of-Function Mutation
inheritance:
- name: Somatic
notes: >-
CTNNB1 (beta-catenin) activating alterations, alongside AXIN1 loss, drive the WNT
pathway program that is one of the most frequently altered pathways in GBC.
- name: ARID1A
gene_term:
preferred_term: ARID1A
term:
id: hgnc:11110
label: ARID1A
association: Somatic Loss-of-Function Mutation
inheritance:
- name: Somatic
evidence:
- reference: PMID:39166960
reference_title: "Genomic landscape of gallbladder cancer: insights from whole exome sequencing."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Our findings focused on the eight most altered genes with pathogenic and
oncogenic mutations: TP53, SMAD4, ERBB3, KRAS, ARID1A, PIK3CA, RB1, and AXIN1.
explanation: >-
ARID1A (SWI/SNF chromatin remodeler) is among the eight most altered genes in the
GBC whole-exome cohort, consistent with loss of chromatin-remodeling tumor
suppression.
notes: >-
ARID1A loss-of-function disrupts SWI/SNF chromatin-remodeling tumor-suppressive
function and is a recurrent somatic alteration in gallbladder cancer.
- name: RB1
gene_term:
preferred_term: RB1
term:
id: hgnc:9884
label: RB1
association: Somatic Loss-of-Function Mutation
inheritance:
- name: Somatic
evidence:
- reference: PMID:39166960
reference_title: "Genomic landscape of gallbladder cancer: insights from whole exome sequencing."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Our findings focused on the eight most altered genes with pathogenic and
oncogenic mutations: TP53, SMAD4, ERBB3, KRAS, ARID1A, PIK3CA, RB1, and AXIN1.
explanation: >-
RB1 is among the eight most altered genes in the GBC whole-exome cohort,
consistent with loss of the RB tumor-suppressor cell-cycle checkpoint.
notes: >-
RB1 loss-of-function releases the RB cell-cycle checkpoint and, together with CDKN2A
loss, deregulates the CDK4/6-RB axis in gallbladder cancer.
- name: AXIN1
gene_term:
preferred_term: AXIN1
term:
id: hgnc:903
label: AXIN1
association: Somatic Loss-of-Function Mutation
inheritance:
- name: Somatic
evidence:
- reference: PMID:39166960
reference_title: "Genomic landscape of gallbladder cancer: insights from whole exome sequencing."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Our findings focused on the eight most altered genes with pathogenic and
oncogenic mutations: TP53, SMAD4, ERBB3, KRAS, ARID1A, PIK3CA, RB1, and AXIN1.
explanation: >-
AXIN1 is among the eight most altered genes in the GBC whole-exome cohort, with
loss-of-function alterations driving the WNT pathway program.
notes: >-
AXIN1 loss-of-function removes a negative regulator of the WNT/beta-catenin pathway,
contributing (with CTNNB1 activation) to the WNT program enriched in GBC.
treatments:
- name: Radical Cholecystectomy
description: >-
Radical (extended) cholecystectomy with hepatic resection of the gallbladder fossa
and regional lymphadenectomy is the only potentially curative treatment for
gallbladder cancer. It is feasible in a minority of patients because most present
with advanced, unresectable disease; for incidentally discovered early tumors,
completion radical re-resection is considered when residual disease is suspected.
treatment_term:
preferred_term: cholecystectomy
term:
id: NCIT:C51676
label: Cholecystectomy
therapeutic_modality: SURGERY
- name: Gemcitabine-Cisplatin plus Durvalumab (TOPAZ-1)
description: >-
First-line immuno-chemotherapy combining gemcitabine and cisplatin with the
anti-PD-L1 checkpoint inhibitor durvalumab for unresectable or metastatic biliary
tract cancer, established by the TOPAZ-1 trial and FDA approved 2022-09-02.
Gallbladder primaries appear to derive less benefit than other biliary tract sites.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: durvalumab
term:
id: NCIT:C103194
label: Durvalumab
- preferred_term: gemcitabine
term:
id: CHEBI:175901
label: gemcitabine
- preferred_term: cisplatin
term:
id: CHEBI:27899
label: cisplatin
therapeutic_modality: MONOCLONAL_ANTIBODY
target_mechanisms:
- target: Immunosuppressive Microenvironment and Immune Evasion
treatment_effect: INHIBITS
description: >-
The anti-PD-L1 antibody durvalumab blocks PD-L1-mediated T-cell inhibition,
counteracting the adaptive immune resistance/immune-evasion program (including
OLFM4-driven PD-L1 upregulation) and restoring anti-tumor T-cell activity.
evidence:
- reference: PMID:38856639
reference_title: "FDA Approval Summary: Durvalumab and Pembrolizumab, Immune Checkpoint Inhibitors for the Treatment of Biliary Tract Cancer."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
On September 2, 2022, the Food and Drug Administration (FDA) approved durvalumab
in combination with cisplatin and gemcitabine, for the treatment of patients with
unresectable or metastatic biliary tract cancers (BTC).
explanation: >-
FDA approval summary documents durvalumab plus gemcitabine-cisplatin as first-line
therapy for unresectable/metastatic biliary tract cancer including gallbladder
cancer.
- reference: PMID:38856639
reference_title: "FDA Approval Summary: Durvalumab and Pembrolizumab, Immune Checkpoint Inhibitors for the Treatment of Biliary Tract Cancer."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
In both studies, a statistically significant and clinically meaningful
improvement in OS was demonstrated.
explanation: >-
TOPAZ-1 (durvalumab) and KEYNOTE-966 (pembrolizumab) each demonstrated a
statistically significant overall survival benefit when a checkpoint
inhibitor was added to gemcitabine-cisplatin.
- reference: PMID:39301763
reference_title: "Efficacy, safety and differential outcomes of immune-chemotherapy with gemcitabine, cisplatin and durvalumab in patients with biliary tract cancers: A multicenter real world cohort."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: >-
While extrahepatic and intrahepatic BTC showed similar outcomes, mOS was
significantly shorter in patients with gall bladder cancer (GB-CA) with 9 months
(95% CI 5.5-12.4; p = 0.02).
explanation: >-
Real-world cohort confirms feasibility of gemcitabine-cisplatin-durvalumab but
shows gallbladder cancer is an independent adverse prognostic factor with shorter
survival than other biliary tract cancers.
- name: Gemcitabine-Cisplatin plus Pembrolizumab (KEYNOTE-966)
description: >-
First-line immuno-chemotherapy combining gemcitabine and cisplatin with the
anti-PD-1 checkpoint inhibitor pembrolizumab for unresectable or metastatic biliary
tract cancer, established by the KEYNOTE-966 trial and FDA approved 2023-10-31.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: gemcitabine
term:
id: CHEBI:175901
label: gemcitabine
- preferred_term: cisplatin
term:
id: CHEBI:27899
label: cisplatin
- preferred_term: pembrolizumab
term:
id: NCIT:C106432
label: Pembrolizumab
therapeutic_modality: MONOCLONAL_ANTIBODY
target_mechanisms:
- target: Immunosuppressive Microenvironment and Immune Evasion
treatment_effect: INHIBITS
description: >-
The anti-PD-1 antibody pembrolizumab blocks PD-1/PD-L1 engagement, counteracting
the adaptive immune resistance/immune-evasion program (including OLFM4-driven
PD-L1 upregulation) and reactivating exhausted anti-tumor T cells.
evidence:
- reference: PMID:38856639
reference_title: "FDA Approval Summary: Durvalumab and Pembrolizumab, Immune Checkpoint Inhibitors for the Treatment of Biliary Tract Cancer."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
On October 31, 2023, the FDA approved pembrolizumab in combination with cisplatin
and gemcitabine for the same indication.
explanation: >-
FDA approval summary documents pembrolizumab plus gemcitabine-cisplatin as a
second checkpoint-inhibitor first-line option for biliary tract cancer.
- reference: PMID:38856639
reference_title: "FDA Approval Summary: Durvalumab and Pembrolizumab, Immune Checkpoint Inhibitors for the Treatment of Biliary Tract Cancer."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
In the KEYNOTE-966 trial, the median OS of patients receiving pembrolizumab was
12.7 months (95% CI, 11.5-13.6) and 10.9 months (95% CI, 9.9-11.6) in patients
receiving placebo [HR, 0.83 (95% CI, 0.72-0.95)].
explanation: >-
KEYNOTE-966 demonstrated a statistically significant overall survival benefit for
adding pembrolizumab to gemcitabine-cisplatin.
- name: HER2 (ERBB2)-Targeted Therapy
description: >-
For the subset of gallbladder cancers with HER2 (ERBB2) amplification or activating
mutation, HER2-directed therapy (e.g., trastuzumab-based regimens and HER2 antibody
approaches) targets the ERBB/RTK-RAS driver program. This is part of the rationale
for routine molecular testing in GBC to enable genome-guided therapy.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: trastuzumab
term:
id: CHEBI:231601
label: trastuzumab
therapeutic_modality: MONOCLONAL_ANTIBODY
- name: Systemic Chemotherapy (Gemcitabine-Cisplatin backbone)
description: >-
Gemcitabine plus cisplatin has been the chemotherapy backbone for advanced biliary
tract cancer for over a decade and remains the foundation upon which checkpoint
inhibitors are added. Adjuvant chemotherapy is used in selected resected patients.
treatment_term:
preferred_term: chemotherapy
term:
id: MAXO:0000647
label: chemotherapy
therapeutic_agent:
- preferred_term: gemcitabine
term:
id: CHEBI:175901
label: gemcitabine
- preferred_term: cisplatin
term:
id: CHEBI:27899
label: cisplatin
datasets: []
References & Deep Research
Deep Research
11. Disease Information
1.1 Concise overview / current understanding
Gallbladder cancer is an aggressive malignancy of the biliary tract; it is frequently detected late because early-stage disease is often asymptomatic or nonspecific, contributing to poor outcomes and limited curative options (reuver2023clinicopathologicalandmolecular pages 2-3, kumar2024gallbladdercancerprogress pages 5-7). Contemporary expert synthesis emphasizes that GBC is clinically lethal and molecularly heterogeneous, and that improving outcomes requires high-quality pathology, centralized multidisciplinary care, and routine molecular testing to enable genome-guided therapy and trial enrollment (reuver2023clinicopathologicalandmolecular pages 2-3).
1.2 Synonyms and alternative names
- Gallbladder carcinoma; carcinoma of the gallbladder; GBC; gall bladder cancer (terminology varies across studies and registries) (reuver2023clinicopathologicalandmolecular pages 2-3, su2024globalregionaland pages 2-3).
1.3 Data provenance (individual vs aggregated)
Evidence in this report derives from: - Aggregated disease-level resources (Global Burden of Disease analyses via GBD 2019/2021; large registry studies) (su2024globalregionaland pages 1-2, su2024globalregionaland pages 2-3, zhang2024gallbladdercancerincidence pages 1-2, hu2024ananalysisof pages 1-2). - Human clinical cohorts including multicenter real-world treatment cohorts and surgical cohorts (mitzlaff2024efficacysafetyand pages 1-2, hu2024prognosticfactorsin pages 19-21). - Primary tumor molecular profiling (whole-exome sequencing; single-cell transcriptomics with validation) (awasthi2024genomiclandscapeof pages 1-2, he2024comprehensivesinglecellanalysis pages 1-2).
2. Etiology
2.1 Disease causal factors (mechanistic framing)
GBC etiology is multifactorial, with strong contributions from chronic biliary inflammation and metabolic risk, and with regionally heterogeneous exposures (e.g., gallstones, obesity/high BMI, chronic infections) shaping incidence patterns (su2024globalregionaland pages 17-18, su2024globalregionaland pages 18-19).
2.2 Risk factors (human epidemiology)
Gallstones / cholelithiasis - A GBD-derived synthesis describes gallstones as the “primary risk factor” for gallbladder and biliary tract cancer (su2024globalregionaland pages 17-18). - In imaging series summarized from the Indian subcontinent, gallstones co-occur with gallbladder masses in ~60–90% of cases (sonographic observation; not necessarily causal proof) (kumar2024gallbladdercancerprogress pages 7-8).
Obesity / high body mass index (BMI) - In a GBD 2019-based analysis, high BMI accounted for 15.2% of deaths and 15.7% of DALYs globally in 2019 for gallbladder and biliary tract cancer (su2024globalregionaland pages 1-2). - A GBD 2021-based analysis similarly reports that although age-standardized rates attributable to high BMI decreased from 1990–2021, absolute deaths and DALYs more than doubled, with projected continuation without intervention (hu2024ananalysisof pages 1-2).
Diabetes/metabolic disease - Obesity and diabetes are highlighted among major attributable risks in the GBD-oriented narrative synthesis (su2024globalregionaland pages 17-18).
Infectious exposures (contextual; varies by anatomical subtype) - A GBD-derived synthesis lists chronic infections including HBV, parasites, and Aspergillus flavus among major attributable risks, noting strong geographic clustering of HBV prevalence (su2024globalregionaland pages 17-18). (These statements refer to “gallbladder and biliary tract cancer” and may apply differentially across anatomical subsites.)
2.3 Protective factors
In the retrieved citable excerpts, explicit protective factors (dietary, pharmacologic, or genetic) were not quantified with effect sizes for GBC specifically. The strongest prevention-relevant signal captured here is the population-level impact of lowering BMI, inferred from attributable burden estimates (su2024globalregionaland pages 1-2, hu2024ananalysisof pages 1-2).
2.4 Gene–environment interactions
Direct, statistically tested gene–environment interaction estimates were not provided in the retrieved excerpts. However, tumor mutational signature patterns consistent with tobacco-related mutagen exposure were reported in a 2024 whole-exome cohort (see Section 4/6), providing mechanistic plausibility for exposure–genome coupling (awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof pages 6-8).
3. Phenotypes
3.1 Typical clinical presentation (human)
In a large Indian series summarized in a 2024 review, common presenting features included: - Weight loss: 201/203 (99%) - Loss of appetite/anorexia: 197/203 (97%) - Right hypochondrial pain: 70% - Palpable mass: 53% - Jaundice: 39% - Nausea/vomiting: 10% (kumar2024gallbladdercancerprogress pages 5-7)
3.2 Suggested HPO terms (examples)
- Abdominal pain (HP:0002027)
- Weight loss (HP:0001824)
- Anorexia (HP:0002039)
- Jaundice (HP:0000952)
- Vomiting (HP:0002013)
- Palpable abdominal mass (HP:0001450)
Note: HPO IDs are suggested mappings for phenotypes described in cited clinical series; HPO identifiers themselves were not explicitly listed in the sources and should be validated against the HPO database.
3.3 Phenotype progression / course
GBC often has nonspecific early symptoms and presents later with advanced disease signs (including jaundice, adjacent organ invasion, nodal involvement), consistent with poor resectability rates in many settings (kumar2024gallbladdercancerprogress pages 5-7, hu2024prognosticfactorsin pages 1-2).
4. Genetic/Molecular Information
4.1 Somatic genomic landscape (2024 primary WES evidence)
A 2024 whole-exome sequencing study of 66 tumor–matched blood pairs (India) identified recurrent pathogenic/oncogenic alterations and pathway-level enrichment: - Eight most altered genes: TP53, SMAD4, ERBB3, KRAS, ARID1A, PIK3CA, RB1, AXIN1 (awasthi2024genomiclandscapeof pages 1-2). - Recurrent mutation proportions in this cohort included TP53 21%, SMAD4 16%, ERBB3 11%, KRAS 8%, PIK3CA 7%, ARID1A 5%, RB1 5%, AXIN1 3% (awasthi2024genomiclandscapeof pages 6-8).
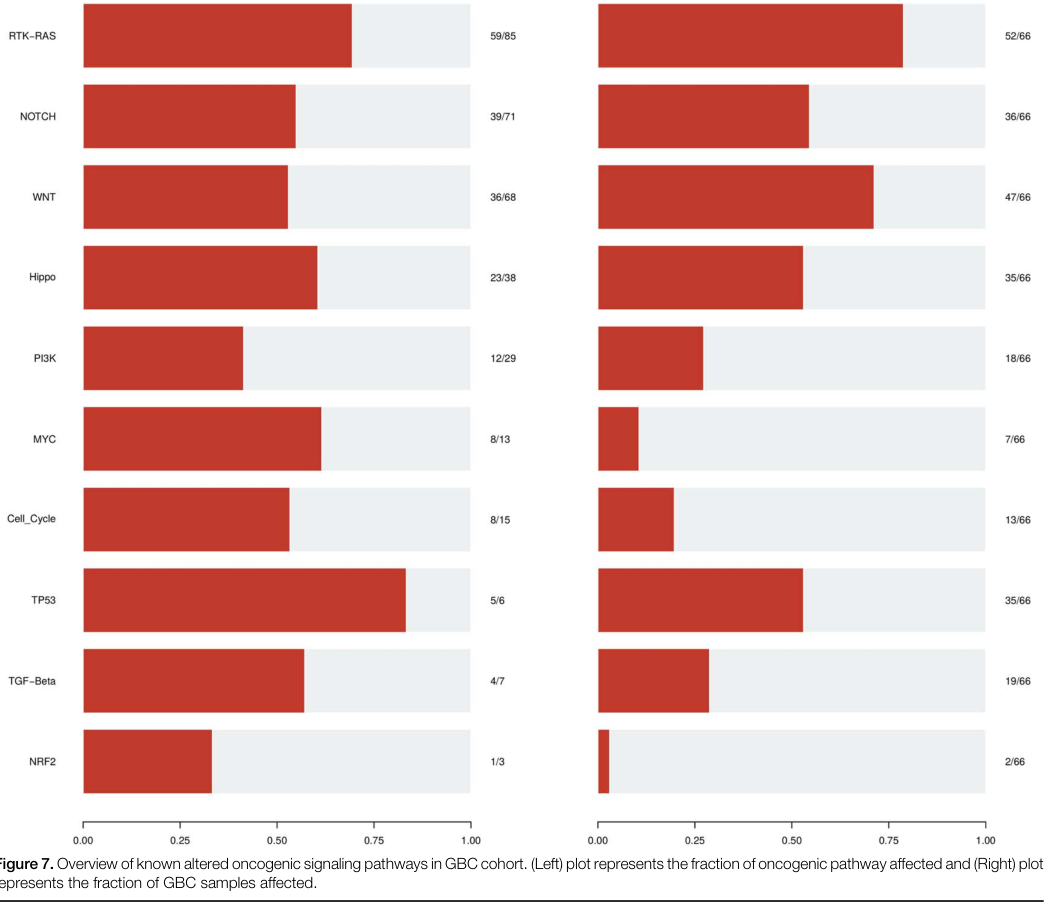
Pathway alteration frequencies (Figure evidence) A pathway summary figure from the same WES study reports the fraction of tumors altered in major oncogenic pathways: - RTK–RAS: 52/66 - WNT: 47/66 - TP53 pathway: 35/66 (awasthi2024genomiclandscapeof media 83e87e83)
Selected pathway component frequencies (WES cohort) - RTK–RAS included ERBB2 26.92%, ERBB3 23.07%, ERBB4 11.53%, KRAS 13.46% (awasthi2024genomiclandscapeof pages 8-11). - WNT included CTNNB1 38.29% and AXIN1 14.89% (awasthi2024genomiclandscapeof pages 8-11). - PI3K-related alterations included PIK3CA, MTOR, and PTEN among affected cases (awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof pages 11-12).
4.2 Mutational signatures / exposure links (2024 WES)
Mutational signature analysis linked COSMIC signatures to clinical characteristics including age and tobacco smoking/chewing (awasthi2024genomiclandscapeof pages 1-2, awasthi2024genomiclandscapeof pages 8-11). APOBEC enrichment (score >2) was observed in 24% of samples and overall tumor mutational burden was low (median 1.6 muts/Mb) (awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof pages 6-8).
4.3 Tumor microenvironment and immune regulation (2024 single-cell + functional)
A 2024 Gut study profiled 230,737 cells across gallbladder cancer and benign gallbladder disease states and identified OLFM4 as elevated in epithelial cells and associated with worse prognosis. Mechanistically, OLFM4 was reported to upregulate PD-L1 via the MAPK–AP1 axis, facilitating immune evasion (he2024comprehensivesinglecellanalysis pages 1-2).
4.4 Suggested ontology terms (GO / CL)
Candidate GO Biological Process terms (examples): - MAPK cascade (GO:0000165) - Regulation of programmed cell death (GO:0043067) - Cell cycle regulation (GO:0051726) - Wnt signaling pathway (GO:0016055) - DNA damage response (GO:0006974) - Immune evasion / regulation of immune response (broad; specific GO selection should match annotated mechanisms)
Candidate Cell Ontology (CL) terms (examples): - Epithelial cell (CL:0000066) - Macrophage (CL:0000235) - T cell (CL:0000084) - Fibroblast (CL:0000057) - Endothelial cell (CL:0000115)
(These are suggested mappings aligned with the single-cell microenvironmental analysis; CL/GO IDs should be validated against the ontologies.)
4.5 Disease–target associations (Open Targets; PMIDs)
Open Targets lists multiple target associations for gallbladder carcinoma, including TP53, KRAS, PIK3CA, ERBB2, SMAD4, CDKN2A, RB1 with supporting PubMed citations (e.g., PMIDs 33115932, 32487254, 34036234, 33563892, 38215750, among others) (OpenTargets Search: Gallbladder carcinoma,Gallbladder cancer).
5. Environmental Information
5.1 Environmental/lifestyle factors captured in current excerpts
- Obesity/high BMI is the dominant quantified modifiable exposure in the retrieved burden analyses (su2024globalregionaland pages 1-2, hu2024ananalysisof pages 1-2).
- Tobacco exposure is implicated indirectly via tobacco-associated mutational signatures in tumor genomes (awasthi2024genomiclandscapeof pages 8-11).
5.2 Infectious agents
Broad BTC risk syntheses mention HBV and parasitic exposures as geographically patterned risks (su2024globalregionaland pages 17-18). Specific gallbladder-carcinoma–specific attributable fractions for infection were not provided in the available excerpts.
6. Mechanism / Pathophysiology
6.1 Causal chain (integrated, evidence-grounded)
- Chronic biliary inflammation/metabolic stress (e.g., gallstones; obesity-driven metabolic milieu) contributes to tissue injury and carcinogenic selection pressure (su2024globalregionaland pages 17-18, kumar2024gallbladdercancerprogress pages 7-8).
- Accumulation of somatic driver alterations in major oncogenic programs (RTK–RAS, WNT, TP53; PI3K pathway; cell-cycle dysregulation) promotes malignant transformation and progression (awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof media 83e87e83).
- Tumor–immune microenvironment remodeling generates immune suppressive states; single-cell analysis implicates OLFM4-driven PD-L1 upregulation via MAPK–AP1 as a mechanism of immune evasion and poor prognosis (he2024comprehensivesinglecellanalysis pages 1-2).
6.2 Key pathways (supported by 2024 WES + figure)
- RTK–RAS (including ERBB2/ERBB3/KRAS) (awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof media 83e87e83)
- WNT/β-catenin signaling (CTNNB1, AXIN1; APC in precursor lesions) (awasthi2024genomiclandscapeof pages 8-11, he2024comprehensivesinglecellanalysis pages 1-2)
- TP53 pathway / DNA damage response (TP53 LOF; ATM, CHEK2 context) (awasthi2024genomiclandscapeof pages 8-11)
- PI3K–AKT–mTOR (PIK3CA, PTEN, MTOR) (awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof pages 11-12)
- Immune checkpoint regulation (PD-L1 induction) (he2024comprehensivesinglecellanalysis pages 1-2)
7. Anatomical Structures Affected
7.1 Primary and secondary anatomy (suggested mappings)
- Primary organ: Gallbladder (UBERON:0005033; suggested mapping)
- Adjacent structures commonly involved in advanced disease: Liver segments adjacent to gallbladder fossa; regional lymph nodes (context for staging and invasion referenced in imaging/staging summaries) (kumar2024gallbladdercancerprogress pages 8-10).
(UBERON IDs are suggested; they were not explicitly listed in sources.)
8. Temporal Development
8.1 Onset
Population data show peak incidence in older age; for example, registry-based analysis in China reported incidence increasing with age and peaking at 70–79 years (zhang2024gallbladdercancerincidence pages 1-2).
8.2 Progression and staging
Advanced-stage presentation is common; a 2024 meta-analysis notes that fewer than 35% of cases are resectable at presentation, recurrence after radical resection is 46–61%, and 5-year overall survival is often <15% (hu2024prognosticfactorsin pages 1-2).
9. Inheritance and Population
9.1 Epidemiology (recent quantified estimates)
Global burden (GBD 2019; all gallbladder and biliary tract cancers) - 2019: 199,211 incident cases; 172,441 deaths; 3,621,473 DALYs (su2024globalregionaland pages 2-3). - Trend 1990→2019: incident cases increased 84.8%, but age-standardized incidence declined ~0.48%/year (su2024globalregionaland pages 2-3).
Sex differences - Age-standardized incidence in 2019 was ~2× higher in females than males (14.0 vs 7.5 per 100,000) (su2024globalregionaland pages 17-18).
Geographic heterogeneity - Higher burden reported in Asia and South America compared with Europe/North America in the GBD synthesis (su2024globalregionaland pages 2-3).
Country-level trend example (China registry) - Age-standardized incidence and mortality decreased from 2005–2017 with AAPC −2.023% (incidence) and −1.603% (mortality) (zhang2024gallbladdercancerincidence pages 1-2).
9.2 Genetic inheritance
GBC is primarily a sporadic cancer driven by somatic alterations; no Mendelian inheritance pattern is established in the evidence retrieved here.
10. Diagnostics
10.1 Cytology/biopsy
- Fine-needle aspiration cytology (FNAC): sensitivity 90.63%, specificity 94.74% in one cited series; ultrasound-guided FNAC diagnostic accuracy reported as ~95% (kumar2024gallbladdercancerprogress pages 5-7).
10.2 Imaging performance (selected statistics)
- MDCT for resectability: sensitivity 72.7%, specificity 100%, accuracy 85% (kumar2024gallbladdercancerprogress pages 8-10).
- CT staging accuracy: 93.3%; high correlation for hepatic/vascular invasion (kumar2024gallbladdercancerprogress pages 8-10).
- Multiparametric MRI (thickened wall): sensitivity 90%, specificity 88% for malignant thickened wall (kumar2024gallbladdercancerprogress pages 8-10).
- PET-CT: detected occult metastases 46.6%; changed management ~25% (resectable) and 30–35% (locally advanced); recurrence sensitivity/specificity 97.6%/90% (kumar2024gallbladdercancerprogress pages 8-10).
10.3 Biomarkers
Tumor markers including CA19-9, CEA, CA125, CA242 were reported to associate with GBC and may help predict resectability/prognosis in some series (kumar2024gallbladdercancerprogress pages 8-10, hu2024prognosticfactorsin pages 19-21).
10.4 Differential diagnosis / mimics
Xanthogranulomatous cholecystitis (XGC) is a recognized mimic; cytologic features include foam cells, histiocytes, bile, multinucleate giant cells, and mixed inflammatory infiltrate (kumar2024gallbladdercancerprogress pages 5-7).
11. Outcome / Prognosis
11.1 Survival statistics (recent summaries)
- A 2024 prognostic meta-analysis reports 5-year overall survival often <15%, with 46–61% recurrence after radical resection (hu2024prognosticfactorsin pages 1-2).
- A GBD 2021-derived high-BMI burden analysis states curative resection is possible in <30% and 5-year overall survival is <10% (hu2024ananalysisof pages 1-2).
11.2 Prognostic factors (meta-analysis)
A 2024 systematic review/meta-analysis (52 studies; 23,174 patients) identified significant factors associated with overall survival: - T stage: HR 2.37 - Lymph node stage: HR 2.03 - Positive/close margins: HR 2.66 - CEA elevated: HR 1.81 - CA19-9 elevated: HR 1.56 - Low LMR: HR 2.17 - Adjuvant chemotherapy: HR 0.75 (benefit) - Radiotherapy: HR 0.56 (benefit) (hu2024prognosticfactorsin pages 1-2)
12. Treatment
12.1 Standard systemic therapy for unresectable/metastatic disease (2023–2024 developments)
Regulatory approvals and pivotal trials (FDA; 2024 summary) - Durvalumab + gemcitabine/cisplatin approved 2022-09-02; TOPAZ-1 median OS 12.8 vs 11.5 months (HR 0.80, 95% CI 0.66–0.97) (casak2024fdaapprovalsummary pages 1-3). - Pembrolizumab + gemcitabine/cisplatin approved 2023-10-31; KEYNOTE-966 median OS 12.7 vs 10.9 months (HR 0.83, 95% CI 0.72–0.95) (casak2024fdaapprovalsummary pages 1-3).
Gallbladder-specific subgroup considerations Exploratory subgroup analyses suggest smaller or absent benefit in the gallbladder cancer subgroup in TOPAZ-1/KEYNOTE-966; one review reports TOPAZ-1 gallbladder subgroup median OS 10.7 vs 11.0 months (HR 0.94, 95% CI 0.65–1.37) (wilbur2024immunotherapyforthe pages 8-9), and the FDA approval summary reports a smaller effect estimate in the gallbladder subgroup (OS HR 0.96) (casak2024fdaapprovalsummary pages 3-4).
12.2 Real-world implementation (2024)
A German multicenter cohort (2021–2024) evaluating gemcitabine/cisplatin/durvalumab (n=165) reported: - Median OS 14 months, median PFS 8 months, ORR 28.5%, DCR 65.5%. - Gallbladder cancer subgroup median OS 9 months and gallbladder cancer was an independent adverse prognostic factor (mitzlaff2024efficacysafetyand pages 1-2).
12.3 Surgery and multimodality therapy
Surgical resection remains the only potentially curative intervention; multiple series emphasize improved survival with resection and the role of adjuvant therapy in selected settings (kumar2024gallbladdercancerprogress pages 13-14, hu2024prognosticfactorsin pages 19-21). Expert commentary supports centralization of care and multidisciplinary decision-making, including consideration of surveillance for very early tumors versus radical re-resection when residual disease is suspected (reuver2023clinicopathologicalandmolecular pages 2-3).
12.4 Suggested MAXO terms (examples)
- Surgical excision (MAXO:0001116; suggested)
- Chemotherapy (MAXO:0000647; suggested)
- Radiotherapy (MAXO:0000008; suggested)
- Immune checkpoint inhibitor therapy (MAXO term mapping should be verified)
(MAXO IDs are suggested; they were not explicitly present in sources.)
13. Prevention
13.1 Primary prevention (evidence captured here)
Because high BMI contributes a substantial attributable fraction of deaths/DALYs, population-level BMI reduction is supported as a prevention strategy (su2024globalregionaland pages 1-2, hu2024ananalysisof pages 1-2). Gallstones are repeatedly emphasized as a major risk factor; however, the retrieved excerpts did not provide evidence-based thresholds for prophylactic cholecystectomy in specific high-risk groups (su2024globalregionaland pages 17-18).
13.2 Secondary prevention (screening/early detection)
A 2024 registry analysis in China recommends exploring “long-term, standardized gallbladder cancer screening programs,” reflecting ongoing uncertainty and need for evidence-based risk stratification (zhang2024gallbladdercancerincidence pages 1-2).
14. Other Species / Natural Disease
The retrieved, citable sources in this run did not provide specific veterinary/natural-disease evidence for gallbladder cancer across other species.
15. Model Organisms
The retrieved, citable excerpts did not enumerate standardized GBC model organism systems (e.g., GEMMs, organoids) in a way that could be cited with specificity here. Mechanistic studies in 2024 include in vitro and in vivo validation linked to single-cell findings (OLFM4 → PD-L1 via MAPK–AP1) (he2024comprehensivesinglecellanalysis pages 1-2), and proteomic studies used functional assays including mouse models to probe invasion/migration programs (sugiyanto2024proteomicprofilingreveals pages 14-14).
Expert opinions / authoritative analysis (2023–2024)
- Expert review recommends synoptic pathology reporting, centralized specialist care, and molecular tumor testing for every GBC patient to enable genome-guided therapy and clinical trial inclusion (reuver2023clinicopathologicalandmolecular pages 2-3).
- Real-world datasets in 2024 demonstrate feasibility and safety of immuno-chemotherapy in routine practice while highlighting that gallbladder primary may have worse outcomes than other BTC sites under similar regimens (mitzlaff2024efficacysafetyand pages 1-2).
Structured evidence summary table
| Domain | Item | Key findings / numeric values | Citations |
|---|---|---|---|
| Epidemiology / burden | Global 2019 burden | 199,211 incident cases (95% UI 166,769–219,615); 256,340 prevalent cases (215,699–282,004); 172,441 deaths (144,899–188,615); 3,621,473 DALYs (3,102,423–3,969,071) worldwide in 2019 | (su2024globalregionaland pages 2-3) |
| Epidemiology / burden | 1990–2019 trends | Incident cases increased 84.8% from 107,787 to 199,211; age-standardized incidence declined by 0.48%/year; age-standardized prevalence declined by 0.27%/year; absolute counts rose 1.85-fold (incidence), 1.92-fold (prevalence), 1.82-fold (deaths), 1.68-fold (DALYs) | (su2024globalregionaland pages 1-2, su2024globalregionaland pages 2-3) |
| Epidemiology / burden | Sex and age patterns | Females had nearly double age-standardized incidence vs males in 2019: 14.0 vs 7.5 per 100,000; older adults and females are more susceptible overall; early-onset burden rose 52.4% from 1990–2019, especially in low-SDI regions | (su2024globalregionaland pages 6-13, su2024globalregionaland pages 17-18, su2024globalregionaland pages 18-19) |
| Epidemiology / burden | High-BMI attributable burden | High BMI accounted for 15.2% of deaths and 15.7% of DALYs globally in 2019; high-BMI-attributable absolute deaths and DALYs more than doubled from 1990–2021 despite declining age-standardized rates | (su2024globalregionaland pages 1-2, hu2024ananalysisof pages 1-2) |
| Risk factors | Gallstones | Gallstones are described as the primary risk factor; gallstones accompanied gallbladder mass in 60–90% of sonographic series | (su2024globalregionaland pages 17-18, kumar2024gallbladdercancerprogress pages 7-8) |
| Risk factors | Obesity / high BMI | Obesity/high BMI is a major attributable risk; burden is higher in high-SDI regions due to obesity prevalence, while low-SDI regions show higher EAPCs | (su2024globalregionaland pages 1-2, su2024globalregionaland pages 18-19, hu2024ananalysisof pages 1-2) |
| Risk factors | Diabetes / metabolic disease | Obesity and diabetes are highlighted among major attributable risks for gallbladder/biliary tract cancer | (su2024globalregionaland pages 17-18) |
| Risk factors | Infectious associations | Chronic infections noted as relevant risks include HBV, parasites, and Aspergillus flavus; HBV prevalence exceeds 8% in parts of Asia/Africa and accounts for nearly 70% of all HBV-infected persons worldwide | (su2024globalregionaland pages 17-18) |
| Genomics / pathways | Top recurrent genes (WES 2024) | Recurrently mutated genes in 66 tumors: TP53 21%, SMAD4 16%, ERBB3 11%, KRAS 8%, PIK3CA 7%, ARID1A 5%, RB1 5%, AXIN1 3% | (awasthi2024genomiclandscapeof pages 1-2, awasthi2024genomiclandscapeof pages 6-8) |
| Genomics / pathways | Most altered genes / drivers | Eight most altered genes highlighted: TP53, SMAD4, ERBB3, KRAS, ARID1A, PIK3CA, RB1, AXIN1; driver genes also included CTNNB1, ELF3, ERBB2 | (awasthi2024genomiclandscapeof pages 1-2, awasthi2024genomiclandscapeof pages 11-12) |
| Genomics / pathways | Pathway frequencies | Figure-based summary in 66 tumors: RTK-RAS 52/66 (78.8%), WNT 47/66 (71.2%), TP53 35/66 (53.0%); other pathways included Notch 54.5%, Hippo ~53%, TGF-β 28.8% | (awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof media 83e87e83) |
| Genomics / pathways | ERBB family | RTK-RAS pathway included ERBB2 26.92%, ERBB3 23.07%, ERBB4 11.53%, KRAS 13.46%; ERBB2/ERBB3 alterations are repeatedly highlighted as actionable/immune-relevant | (awasthi2024genomiclandscapeof pages 8-11, he2024comprehensivesinglecellanalysis pages 14-14) |
| Genomics / pathways | PI3K / PTEN | PI3K pathway altered in 27% overall; among pathway-altered cases PIK3CA 33.3%, MTOR 27.8%, PTEN 22.2%; PIK3CA gain-of-function and PTEN loss emphasized as therapeutically relevant | (awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof pages 12-13, awasthi2024genomiclandscapeof pages 11-12) |
| Genomics / pathways | WNT / CTNNB1 / AXIN1 | WNT pathway altered in 71.2%; CTNNB1 38.29%, AXIN1 14.89%; APC mutations noted in adenomas in single-cell/WGS progression analysis | (awasthi2024genomiclandscapeof pages 8-11, he2024comprehensivesinglecellanalysis pages 1-2) |
| Genomics / pathways | TP53 / SMAD4 / LOF | TP53 pathway altered in 53% with TP53 mutated in 86.11% of TP53-pathway–altered cases; all observed TP53 variants were loss-of-function; SMAD4/TGF-β alterations are prominent after TP53 | (awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof pages 11-12) |
| Genomics / pathways | Mutational signatures / exposures | COSMIC 1, 6, 18, 29 linked to age and tobacco smoking/chewing; Signature 4 linked to tobacco mutagens; APOBEC enrichment score >2 in 24% of samples; median TMB 1.6 muts/Mb | (awasthi2024genomiclandscapeof pages 1-2, awasthi2024genomiclandscapeof pages 8-11, awasthi2024genomiclandscapeof pages 11-12, awasthi2024genomiclandscapeof pages 6-8) |
| Genomics / microenvironment | Single-cell / immune escape | scRNA-seq atlas of 230,737 cells from 15 GBCs and benign lesions identified OLFM4 as elevated; OLFM4 upregulated PD-L1 through MAPK-AP1 axis, linking epithelial programs to immune evasion | (he2024comprehensivesinglecellanalysis pages 14-14, he2024comprehensivesinglecellanalysis pages 1-2) |
| Treatment / standard of care | Historical chemotherapy backbone | Cisplatin + gemcitabine remained SOC for >10 years based on ABC-02: median OS 11.7 vs 8.1 months; HR 0.64 | (casak2024fdaapprovalsummary pages 1-3, wilbur2024immunotherapyforthe pages 1-2) |
| Treatment / pivotal trial | TOPAZ-1 | Durvalumab + gemcitabine/cisplatin: median OS 12.8 vs 11.5 months; OS HR 0.80 (95% CI 0.66–0.97); median PFS 7.2 vs 5.7 months; PFS HR 0.75 (0.63–0.89) | (casak2024fdaapprovalsummary pages 3-4, casak2024fdaapprovalsummary pages 1-3) |
| Treatment / pivotal trial | KEYNOTE-966 | Pembrolizumab + gemcitabine/cisplatin: median OS 12.7 vs 10.9 months; OS HR 0.83 (95% CI 0.72–0.95); median PFS 6.5 vs 5.6 months; BICR PFS HR 0.86 (0.75–1.00) | (casak2024fdaapprovalsummary pages 3-4, casak2024fdaapprovalsummary pages 1-3, storandt2024evaluatingthetherapeutic pages 4-6) |
| Treatment / approvals | FDA approval dates | Durvalumab approved 2022-09-02; pembrolizumab approved 2023-10-31 for unresectable/metastatic biliary tract cancer with gemcitabine/cisplatin | (casak2024fdaapprovalsummary pages 1-3) |
| Treatment / subgroup note | Gallbladder cancer subgroup | Exploratory subgroup analyses suggested smaller benefit in gallbladder cancer: OS HR 0.96 in GBC in FDA review; another review reported GBC subgroup median OS 10.7 vs 11.0 months, HR 0.94 (95% CI 0.65–1.37) | (casak2024fdaapprovalsummary pages 3-4, wilbur2024immunotherapyforthe pages 8-9) |
| Treatment / real-world | Durvalumab + GemCis real-world cohort | German multicenter cohort (n=165): median OS 14.0 months (95% CI 10.3–17.7), PFS 8.0 months (6.8–9.2), ORR 28.5%, DCR 65.5%; gallbladder cancer subgroup median OS 9.0 months (5.5–12.4) and was an independent adverse prognostic factor | (mitzlaff2024efficacysafetyand pages 1-2) |
| Treatment / safety | Durvalumab combination safety | In TOPAZ-1, any-grade AEs 99.4% vs 98.8%; grade 3–4 AEs 75.7% vs 77.8%; immune-related AEs 12.7% vs 4.7% with durvalumab vs placebo | (wilbur2024immunotherapyforthe pages 8-9, storandt2024evaluatingthetherapeutic pages 4-6) |
| Diagnostics | FNAC / cytology | FNAC sensitivity 90.63%, specificity 94.74%; USG-guided FNAC diagnostic accuracy ~95% for confirming diagnosis, especially in locally advanced/metastatic disease | (kumar2024gallbladdercancerprogress pages 5-7) |
| Diagnostics | Ultrasound / sonography | Common sonographic patterns: mass lesion in 87%; intraluminal 59% vs infiltrative 41%; mass replacing gallbladder in 73%; gallstone with mass in 54% in one series | (kumar2024gallbladdercancerprogress pages 7-8) |
| Diagnostics | CT / MRI resectability and staging | MDCT sensitivity 72.7%, specificity 100%, accuracy 85% for resectability; CT staging accuracy 93.3%; multiparametric MRI sensitivity 90% and specificity 88% for malignant thickened wall | (kumar2024gallbladdercancerprogress pages 8-10) |
| Diagnostics | PET-CT / recurrence | PET-CT detected occult metastases in 46.6%; changed management in ~25% of resectable and 30–35% of locally advanced cases; PET/CT sensitivity/specificity for recurrence 97.6% / 90% | (kumar2024gallbladdercancerprogress pages 8-10) |
| Differential diagnosis | Xanthogranulomatous cholecystitis mimic | XGC can mimic malignancy; characteristic cytology includes foam cells, histiocytes, bile, multinucleate giant cells, and mixed inflammatory infiltrate | (kumar2024gallbladdercancerprogress pages 5-7) |
Table: This table condenses high-yield, quantitatively anchored evidence on gallbladder cancer epidemiology, risk factors, molecular landscape, current systemic therapy, and diagnostic performance. It is designed as a reusable reference for a disease knowledge base entry and cites the specific available context IDs supporting each row.
Key visual evidence
A 2024 WES study figure summarizes pathway alteration frequencies in GBC (RTK–RAS 52/66; WNT 47/66; TP53 35/66), supporting statements about dominant oncogenic programs (awasthi2024genomiclandscapeof media 83e87e83).
URLs and publication dates (where available in sources)
- Su et al., Frontiers in Medicine — Apr 2024 — https://doi.org/10.3389/fmed.2024.1384314 (su2024globalregionaland pages 1-2)
- Casak et al., Clinical Cancer Research — Jun 2024 — https://doi.org/10.1158/1078-0432.CCR-24-0517 (casak2024fdaapprovalsummary pages 1-3)
- Awasthi et al., International Journal of Surgery — Aug 2024 — https://doi.org/10.1097/JS9.0000000000002031 (awasthi2024genomiclandscapeof pages 1-2)
- He et al., Gut — May 2024 — https://doi.org/10.1136/gutjnl-2023-331773 (he2024comprehensivesinglecellanalysis pages 1-2)
- Mitzlaff et al., United European Gastroenterology Journal — Sep 2024 — https://doi.org/10.1002/ueg2.12656 (mitzlaff2024efficacysafetyand pages 1-2)
- Kumar et al., World Journal of Clinical Oncology — Jun 2024 — https://doi.org/10.5306/wjco.v15.i6.695 (kumar2024gallbladdercancerprogress pages 5-7)
- Hu et al., Hepatobiliary Surgery and Nutrition — Jan 2024 — https://doi.org/10.21037/hbsn-23-502 (hu2024prognosticfactorsin pages 1-2)
- Zhang et al., BMC Public Health — Nov 2024 — https://doi.org/10.1186/s12889-024-20584-9 (zhang2024gallbladdercancerincidence pages 1-2)
Evidence limitations (important for knowledge base curation)
- The tool-accessible excerpts did not include citable ICD/MeSH/Orphanet IDs, nor many primary PMIDs for 2023–2024 studies (except via Open Targets’ embedded PubMed IDs). Identifier fields should therefore be verified using the relevant terminologies before database population (OpenTargets Search: Gallbladder carcinoma,Gallbladder cancer).
- Many epidemiology estimates in this run are for combined gallbladder and biliary tract cancers (GBD aggregated cause), not gallbladder-only; they still provide useful burden framing but should be labeled accordingly in a knowledge base (su2024globalregionaland pages 1-2, su2024globalregionaland pages 2-3).
References
-
(OpenTargets Search: Gallbladder carcinoma,Gallbladder cancer): Open Targets Query (Gallbladder carcinoma,Gallbladder cancer, 30 results). Buniello, A. et al. (2025). Open Targets Platform: facilitating therapeutic hypotheses building in drug discovery. Nucleic Acids Research.
-
(reuver2023clinicopathologicalandmolecular pages 2-3): Philip R. de Reuver and Rachel S. van der Post. Clinicopathological and molecular insights into gallbladder cancer. Cancers, 15:2728, May 2023. URL: https://doi.org/10.3390/cancers15102728, doi:10.3390/cancers15102728. This article has 5 citations.
-
(casak2024fdaapprovalsummary pages 1-3): Sandra J. Casak, Vaibhav Kumar, Chi Song, Mengdie Yuan, Anup K. Amatya, Joyce Cheng, Pallavi S. Mishra-Kalyani, Shenghui Tang, Steven J. Lemery, Doris Auth, Gina Davis, Paul G. Kluetz, Richard Pazdur, and Lola A. Fashoyin-Aje. Fda approval summary: durvalumab and pembrolizumab, immune checkpoint inhibitors for the treatment of biliary tract cancer. Clinical cancer research : an official journal of the American Association for Cancer Research, 30:3371-3377, Jun 2024. URL: https://doi.org/10.1158/1078-0432.ccr-24-0517, doi:10.1158/1078-0432.ccr-24-0517. This article has 25 citations.
-
(kumar2024gallbladdercancerprogress pages 5-7): Ashok Kumar, Yajnadatta Sarangi, Annapurna Gupta, and Aarti Sharma. Gallbladder cancer: progress in the indian subcontinent. World Journal of Clinical Oncology, 15:695-716, Jun 2024. URL: https://doi.org/10.5306/wjco.v15.i6.695, doi:10.5306/wjco.v15.i6.695. This article has 25 citations.
-
(su2024globalregionaland pages 2-3): Jiao Su, Yuanhao Liang, and Xiaofeng He. Global, regional, and national burden and trends analysis of gallbladder and biliary tract cancer from 1990 to 2019 and predictions to 2030: a systematic analysis for the global burden of disease study 2019. Frontiers in Medicine, Apr 2024. URL: https://doi.org/10.3389/fmed.2024.1384314, doi:10.3389/fmed.2024.1384314. This article has 42 citations.
-
(su2024globalregionaland pages 1-2): Jiao Su, Yuanhao Liang, and Xiaofeng He. Global, regional, and national burden and trends analysis of gallbladder and biliary tract cancer from 1990 to 2019 and predictions to 2030: a systematic analysis for the global burden of disease study 2019. Frontiers in Medicine, Apr 2024. URL: https://doi.org/10.3389/fmed.2024.1384314, doi:10.3389/fmed.2024.1384314. This article has 42 citations.
-
(zhang2024gallbladdercancerincidence pages 1-2): Xinzhou Zhang, Chenyun Xu, Han Zhang, Xinxin Du, Quanyu Zhang, Manman Lu, Yanrong Ma, and Wenjun Ma. Gallbladder cancer incidence and mortality rate trends in china: analysis of data from the population-based cancer registry. BMC Public Health, Nov 2024. URL: https://doi.org/10.1186/s12889-024-20584-9, doi:10.1186/s12889-024-20584-9. This article has 8 citations and is from a peer-reviewed journal.
-
(hu2024ananalysisof pages 1-2): Zhuowen Hu, Xue Wang, Xin Zhang, Wuping Sun, and Jun Mao. An analysis of the global burden of gallbladder and biliary tract cancer attributable to high bmi in 204 countries and territories: 1990–2021. Frontiers in Nutrition, Dec 2024. URL: https://doi.org/10.3389/fnut.2024.1521770, doi:10.3389/fnut.2024.1521770. This article has 17 citations.
-
(mitzlaff2024efficacysafetyand pages 1-2): Katharina Mitzlaff, Martha M. Kirstein, Christian Müller, Marino Venerito, Alexander Olkus, Michael T. Dill, Arndt Weinmann, Lorenz Kocheise, Alina Busch, Kornelius Schulze, Gabriel Allo, Dirk‐Thomas Waldschmidt, Maryam Barsch, Bertram Bengsch, Michael Quante, Maria A. Gonzalez‐Carmona, Vera Himmelsbach, Fabian Finkelmeier, Roman Kloeckner, Peter Schirmacher, Jens U. Marquardt, and Carolin Zimpel. Efficacy, safety and differential outcomes of immune‐chemotherapy with gemcitabine, cisplatin and durvalumab in patients with biliary tract cancers: a multicenter real world cohort. United European Gastroenterology Journal, 12:1230-1242, Sep 2024. URL: https://doi.org/10.1002/ueg2.12656, doi:10.1002/ueg2.12656. This article has 17 citations and is from a peer-reviewed journal.
-
(hu2024prognosticfactorsin pages 19-21): Xiaoqian Hu, Di Zeng, Ningyuan Wen, Yaoqun Wang, Jiong Lu, and Bei Li. Prognostic factors in gallbladder cancer: a comprehensive systematic review and meta-analysis. Hepatobiliary Surgery and Nutrition, 14:374-397, Jan 2024. URL: https://doi.org/10.21037/hbsn-23-502, doi:10.21037/hbsn-23-502. This article has 4 citations and is from a peer-reviewed journal.
-
(awasthi2024genomiclandscapeof pages 1-2): Supriya Awasthi, Rahul Kumar, Dibyabhaba Pradhan, Neetu Rawal, Harsh Goel, Parameswar Sahu, Sandeep Sisodiya, Rashmi Rana, Sunil Kumar, Nihar Ranjan Dash, Prasenjit Das, Usha Agrawal, GK Rath, Tanvir Kaur, RS Dhaliwal, Showket Hussain, Sundeep Singh Saluja, and Pranay Tanwar. Genomic landscape of gallbladder cancer: insights from whole exome sequencing. International Journal of Surgery (London, England), 110:6883-6897, Aug 2024. URL: https://doi.org/10.1097/js9.0000000000002031, doi:10.1097/js9.0000000000002031. This article has 15 citations.
-
(he2024comprehensivesinglecellanalysis pages 1-2): Huisi He, Shuzhen Chen, Yong Yu, Zhecai Fan, Youwen Qian, Yaping Dong, Yuting Song, Caiming Zhong, Xiaojuan Sun, Qiqi Cao, Shiyao Li, Weihan Huang, Wenxin Li, Mingzhu Zhuang, Jinxian Yang, Xianming Wang, Jiaqian Wang, Dongfang Wu, Hongyang Wang, and Wen Wen. Comprehensive single-cell analysis deciphered microenvironmental dynamics and immune regulator olfactomedin 4 in pathogenesis of gallbladder cancer. Gut, 73:1529-1542, May 2024. URL: https://doi.org/10.1136/gutjnl-2023-331773, doi:10.1136/gutjnl-2023-331773. This article has 30 citations and is from a highest quality peer-reviewed journal.
-
(su2024globalregionaland pages 17-18): Jiao Su, Yuanhao Liang, and Xiaofeng He. Global, regional, and national burden and trends analysis of gallbladder and biliary tract cancer from 1990 to 2019 and predictions to 2030: a systematic analysis for the global burden of disease study 2019. Frontiers in Medicine, Apr 2024. URL: https://doi.org/10.3389/fmed.2024.1384314, doi:10.3389/fmed.2024.1384314. This article has 42 citations.
-
(su2024globalregionaland pages 18-19): Jiao Su, Yuanhao Liang, and Xiaofeng He. Global, regional, and national burden and trends analysis of gallbladder and biliary tract cancer from 1990 to 2019 and predictions to 2030: a systematic analysis for the global burden of disease study 2019. Frontiers in Medicine, Apr 2024. URL: https://doi.org/10.3389/fmed.2024.1384314, doi:10.3389/fmed.2024.1384314. This article has 42 citations.
-
(kumar2024gallbladdercancerprogress pages 7-8): Ashok Kumar, Yajnadatta Sarangi, Annapurna Gupta, and Aarti Sharma. Gallbladder cancer: progress in the indian subcontinent. World Journal of Clinical Oncology, 15:695-716, Jun 2024. URL: https://doi.org/10.5306/wjco.v15.i6.695, doi:10.5306/wjco.v15.i6.695. This article has 25 citations.
-
(awasthi2024genomiclandscapeof pages 8-11): Supriya Awasthi, Rahul Kumar, Dibyabhaba Pradhan, Neetu Rawal, Harsh Goel, Parameswar Sahu, Sandeep Sisodiya, Rashmi Rana, Sunil Kumar, Nihar Ranjan Dash, Prasenjit Das, Usha Agrawal, GK Rath, Tanvir Kaur, RS Dhaliwal, Showket Hussain, Sundeep Singh Saluja, and Pranay Tanwar. Genomic landscape of gallbladder cancer: insights from whole exome sequencing. International Journal of Surgery (London, England), 110:6883-6897, Aug 2024. URL: https://doi.org/10.1097/js9.0000000000002031, doi:10.1097/js9.0000000000002031. This article has 15 citations.
-
(awasthi2024genomiclandscapeof pages 6-8): Supriya Awasthi, Rahul Kumar, Dibyabhaba Pradhan, Neetu Rawal, Harsh Goel, Parameswar Sahu, Sandeep Sisodiya, Rashmi Rana, Sunil Kumar, Nihar Ranjan Dash, Prasenjit Das, Usha Agrawal, GK Rath, Tanvir Kaur, RS Dhaliwal, Showket Hussain, Sundeep Singh Saluja, and Pranay Tanwar. Genomic landscape of gallbladder cancer: insights from whole exome sequencing. International Journal of Surgery (London, England), 110:6883-6897, Aug 2024. URL: https://doi.org/10.1097/js9.0000000000002031, doi:10.1097/js9.0000000000002031. This article has 15 citations.
-
(hu2024prognosticfactorsin pages 1-2): Xiaoqian Hu, Di Zeng, Ningyuan Wen, Yaoqun Wang, Jiong Lu, and Bei Li. Prognostic factors in gallbladder cancer: a comprehensive systematic review and meta-analysis. Hepatobiliary Surgery and Nutrition, 14:374-397, Jan 2024. URL: https://doi.org/10.21037/hbsn-23-502, doi:10.21037/hbsn-23-502. This article has 4 citations and is from a peer-reviewed journal.
-
(awasthi2024genomiclandscapeof media 83e87e83): Supriya Awasthi, Rahul Kumar, Dibyabhaba Pradhan, Neetu Rawal, Harsh Goel, Parameswar Sahu, Sandeep Sisodiya, Rashmi Rana, Sunil Kumar, Nihar Ranjan Dash, Prasenjit Das, Usha Agrawal, GK Rath, Tanvir Kaur, RS Dhaliwal, Showket Hussain, Sundeep Singh Saluja, and Pranay Tanwar. Genomic landscape of gallbladder cancer: insights from whole exome sequencing. International Journal of Surgery (London, England), 110:6883-6897, Aug 2024. URL: https://doi.org/10.1097/js9.0000000000002031, doi:10.1097/js9.0000000000002031. This article has 15 citations.
-
(awasthi2024genomiclandscapeof pages 11-12): Supriya Awasthi, Rahul Kumar, Dibyabhaba Pradhan, Neetu Rawal, Harsh Goel, Parameswar Sahu, Sandeep Sisodiya, Rashmi Rana, Sunil Kumar, Nihar Ranjan Dash, Prasenjit Das, Usha Agrawal, GK Rath, Tanvir Kaur, RS Dhaliwal, Showket Hussain, Sundeep Singh Saluja, and Pranay Tanwar. Genomic landscape of gallbladder cancer: insights from whole exome sequencing. International Journal of Surgery (London, England), 110:6883-6897, Aug 2024. URL: https://doi.org/10.1097/js9.0000000000002031, doi:10.1097/js9.0000000000002031. This article has 15 citations.
-
(kumar2024gallbladdercancerprogress pages 8-10): Ashok Kumar, Yajnadatta Sarangi, Annapurna Gupta, and Aarti Sharma. Gallbladder cancer: progress in the indian subcontinent. World Journal of Clinical Oncology, 15:695-716, Jun 2024. URL: https://doi.org/10.5306/wjco.v15.i6.695, doi:10.5306/wjco.v15.i6.695. This article has 25 citations.
-
(wilbur2024immunotherapyforthe pages 8-9): Helen Catherine Wilbur and Nilofer S. Azad. Immunotherapy for the treatment of biliary tract cancer: an evolving landscape. Therapeutic Advances in Medical Oncology, Jan 2024. URL: https://doi.org/10.1177/17588359241235799, doi:10.1177/17588359241235799. This article has 8 citations and is from a peer-reviewed journal.
-
(casak2024fdaapprovalsummary pages 3-4): Sandra J. Casak, Vaibhav Kumar, Chi Song, Mengdie Yuan, Anup K. Amatya, Joyce Cheng, Pallavi S. Mishra-Kalyani, Shenghui Tang, Steven J. Lemery, Doris Auth, Gina Davis, Paul G. Kluetz, Richard Pazdur, and Lola A. Fashoyin-Aje. Fda approval summary: durvalumab and pembrolizumab, immune checkpoint inhibitors for the treatment of biliary tract cancer. Clinical cancer research : an official journal of the American Association for Cancer Research, 30:3371-3377, Jun 2024. URL: https://doi.org/10.1158/1078-0432.ccr-24-0517, doi:10.1158/1078-0432.ccr-24-0517. This article has 25 citations.
-
(kumar2024gallbladdercancerprogress pages 13-14): Ashok Kumar, Yajnadatta Sarangi, Annapurna Gupta, and Aarti Sharma. Gallbladder cancer: progress in the indian subcontinent. World Journal of Clinical Oncology, 15:695-716, Jun 2024. URL: https://doi.org/10.5306/wjco.v15.i6.695, doi:10.5306/wjco.v15.i6.695. This article has 25 citations.
-
(sugiyanto2024proteomicprofilingreveals pages 14-14): Raisatun Nisa Sugiyanto, Carmen Metzger, Aslihan Inal, Felicia Truckenmueller, Kira Gür, Eva Eiteneuer, Thorben Huth, Angelika Fraas, Ivonne Heinze, Joanna Kirkpatrick, Carsten Sticht, Thomas Albrecht, Benjamin Goeppert, Tanja Poth, Stefan Pusch, Arianeb Mehrabi, Peter Schirmacher, Junfang Ji, Alessandro Ori, and Stephanie Roessler. Proteomic profiling reveals ceacam6 function in driving gallbladder cancer aggressiveness through integrin receptor, prkcd and akt/erk signaling. Cell Death & Disease, Oct 2024. URL: https://doi.org/10.1038/s41419-024-07171-x, doi:10.1038/s41419-024-07171-x. This article has 9 citations and is from a peer-reviewed journal.
-
(su2024globalregionaland pages 6-13): Jiao Su, Yuanhao Liang, and Xiaofeng He. Global, regional, and national burden and trends analysis of gallbladder and biliary tract cancer from 1990 to 2019 and predictions to 2030: a systematic analysis for the global burden of disease study 2019. Frontiers in Medicine, Apr 2024. URL: https://doi.org/10.3389/fmed.2024.1384314, doi:10.3389/fmed.2024.1384314. This article has 42 citations.
-
(he2024comprehensivesinglecellanalysis pages 14-14): Huisi He, Shuzhen Chen, Yong Yu, Zhecai Fan, Youwen Qian, Yaping Dong, Yuting Song, Caiming Zhong, Xiaojuan Sun, Qiqi Cao, Shiyao Li, Weihan Huang, Wenxin Li, Mingzhu Zhuang, Jinxian Yang, Xianming Wang, Jiaqian Wang, Dongfang Wu, Hongyang Wang, and Wen Wen. Comprehensive single-cell analysis deciphered microenvironmental dynamics and immune regulator olfactomedin 4 in pathogenesis of gallbladder cancer. Gut, 73:1529-1542, May 2024. URL: https://doi.org/10.1136/gutjnl-2023-331773, doi:10.1136/gutjnl-2023-331773. This article has 30 citations and is from a highest quality peer-reviewed journal.
-
(awasthi2024genomiclandscapeof pages 12-13): Supriya Awasthi, Rahul Kumar, Dibyabhaba Pradhan, Neetu Rawal, Harsh Goel, Parameswar Sahu, Sandeep Sisodiya, Rashmi Rana, Sunil Kumar, Nihar Ranjan Dash, Prasenjit Das, Usha Agrawal, GK Rath, Tanvir Kaur, RS Dhaliwal, Showket Hussain, Sundeep Singh Saluja, and Pranay Tanwar. Genomic landscape of gallbladder cancer: insights from whole exome sequencing. International Journal of Surgery (London, England), 110:6883-6897, Aug 2024. URL: https://doi.org/10.1097/js9.0000000000002031, doi:10.1097/js9.0000000000002031. This article has 15 citations.
-
(wilbur2024immunotherapyforthe pages 1-2): Helen Catherine Wilbur and Nilofer S. Azad. Immunotherapy for the treatment of biliary tract cancer: an evolving landscape. Therapeutic Advances in Medical Oncology, Jan 2024. URL: https://doi.org/10.1177/17588359241235799, doi:10.1177/17588359241235799. This article has 8 citations and is from a peer-reviewed journal.
-
(storandt2024evaluatingthetherapeutic pages 4-6): Michael Storandt, Zhaohui Jin, and Amit Mahipal. Evaluating the therapeutic potential of durvalumab in adults with locally advanced or metastatic biliary tract cancer: evidence to date. OncoTargets and Therapy, 17:383-394, May 2024. URL: https://doi.org/10.2147/ott.s391707, doi:10.2147/ott.s391707. This article has 3 citations.