Epithelioid Sarcoma
Epithelioid sarcoma is a rare soft-tissue sarcoma of uncertain differentiation characterized by epithelioid and spindled tumor cells co-expressing epithelial (cytokeratin, EMA) and mesenchymal markers. The defining molecular lesion in the large majority of cases is loss of the SWI/SNF (BAF) core subunit SMARCB1 (INI1), producing the diagnostic loss of nuclear INI1 staining. Two clinicopathologic forms are recognized: the more common classic (distal) type, which typically arises in the distal extremities of young adults, and the proximal (large-cell) type, which arises in the trunk, pelvis, perineum, and proximal sites of older adults, is more aggressive, and frequently shows rhabdoid cytomorphology. The EZH2 inhibitor tazemetostat is FDA-approved for advanced INI1-deficient epithelioid sarcoma.
Ask OpenScientist
Ask a research question about Epithelioid Sarcoma. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Classifications
Mappings
Subtypes
2Show evidence (1 reference)
Show evidence (1 reference)
Pathophysiology
4Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Histopathology
3Show evidence (1 reference)
Show evidence (1 reference)
Pathograph
Phenotypes
3Integument 1
Show evidence (1 reference)
Neoplasm 1
Show evidence (1 reference)
Other 1
Show evidence (1 reference)
Genetic Associations
1Show evidence (1 reference)
Medical Actions
3Show evidence (1 reference)
Show evidence (2 references)
Biochemical Markers
1Clinical Trials
1Show evidence (1 reference)
Source YAML
click to showname: Epithelioid Sarcoma
creation_date: '2026-06-17T00:00:00Z'
description: >-
Epithelioid sarcoma is a rare soft-tissue sarcoma of uncertain differentiation
characterized by epithelioid and spindled tumor cells co-expressing epithelial
(cytokeratin, EMA) and mesenchymal markers. The defining molecular lesion in the
large majority of cases is loss of the SWI/SNF (BAF) core subunit SMARCB1 (INI1),
producing the diagnostic loss of nuclear INI1 staining. Two clinicopathologic
forms are recognized: the more common classic (distal) type, which typically
arises in the distal extremities of young adults, and the proximal (large-cell)
type, which arises in the trunk, pelvis, perineum, and proximal sites of older
adults, is more aggressive, and frequently shows rhabdoid cytomorphology. The
EZH2 inhibitor tazemetostat is FDA-approved for advanced INI1-deficient
epithelioid sarcoma.
categories:
- Soft Tissue Sarcoma
- Molecularly Defined Tumor
- SWI/SNF-Deficient Tumor
parents:
- Sarcoma
has_subtypes:
- name: Classic
display_name: Classic (Distal) Type
description: >-
The classic or distal type is the more common form, typically arising in the
distal upper extremity (hand, forearm) of adolescents and young adults as slowly
growing dermal or subcutaneous nodules that may ulcerate and mimic a benign
process or chronic ulcer.
evidence:
- reference: PMID:4014539
reference_title: "Epithelioid sarcoma. Diagnosis, prognostic indicators, and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "A retrospective review of 241 cases of epithelioid sarcoma reaffirmed the propensity of this tumor to occur in the distal extremities of young adults."
explanation: The Chase & Enzinger series confirms the classic (distal) type's predilection for the distal extremities of young adults.
- name: Proximal
display_name: Proximal (Large-Cell) Type
description: >-
The proximal-type (large-cell) variant arises in deep axial soft tissues of the
pelvis, perineum, genital tract, and trunk in older adults. It is composed of
large epithelioid cells with prominent nucleoli and frequent rhabdoid features,
behaves more aggressively, and carries a worse prognosis than the classic type.
evidence:
- reference: PMID:9042279
reference_title: '"Proximal-type" epithelioid sarcoma, a distinctive aggressive neoplasm showing rhabdoid features. Clinicopathologic, immunohistochemical, and ultrastructural study of a series.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "In contrast to the conventional, \"distal-type\" epithelioid sarcoma, the proximal variant is characterized by a predominantly large-cell, epithelioid cytomorphology, marked cytologic atypia, frequent occurrence of rhabdoid features, and lack of a granuloma-like pattern in most cases. It appears to be somewhat more aggressive (or at least metastasizes earlier) than usual epithelioid sarcoma."
explanation: The original clinicopathologic series defining proximal-type epithelioid sarcoma documents its large-cell epithelioid cytomorphology, rhabdoid features, and more aggressive behavior than the conventional distal type.
pathophysiology:
- name: SMARCB1 (INI1) Loss
description: >-
Biallelic inactivation of SMARCB1 (INI1/BAF47/SNF5) disables a core subunit of
the SWI/SNF (BAF) chromatin-remodeling complex. This is the defining molecular
event in the great majority of both classic and proximal-type epithelioid
sarcomas and produces the diagnostic loss of nuclear INI1 immunostaining.
cell_types:
- preferred_term: mesenchymal cell of uncertain differentiation
term:
id: CL:0000134
label: mesenchymal stem cell
protein_complexes:
- preferred_term: BAF complex
term:
id: GO:0016514
label: SWI/SNF complex
biological_processes:
- preferred_term: chromatin remodeling
modifier: ABNORMAL
term:
id: GO:0006338
label: chromatin remodeling
downstream:
- target: EZH2/PRC2 Dependency and H3K27 Hypermethylation
description: >-
Loss of SWI/SNF antagonism of PRC2 leaves EZH2-driven H3K27 methylation
unopposed, creating an oncogenic dependency.
causal_link_type: DIRECT
evidence:
- reference: PMID:19033866
reference_title: "Loss of INI1 expression is characteristic of both conventional and proximal-type epithelioid sarcoma."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "similar to MRT of infancy, loss of INI1 expression is characteristic of both conventional and proximal-type ES, being detected in >90% of cases."
explanation: Immunohistochemical study of 136 epithelioid sarcomas shows loss of INI1 (SMARCB1) expression in over 90% of both conventional and proximal-type cases, establishing SMARCB1 inactivation as the defining molecular lesion.
- name: EZH2/PRC2 Dependency and H3K27 Hypermethylation
description: >-
SWI/SNF normally opposes Polycomb repressive complex 2 (PRC2). When SMARCB1 is
lost, PRC2/EZH2 activity is unopposed, increasing trimethylation of histone H3
at lysine 27 (H3K27me3) and epigenetically repressing differentiation and
tumor-suppressor genes. SMARCB1-deficient tumors become dependent on EZH2
activity, the rationale for therapeutic EZH2 inhibition.
molecular_functions:
- preferred_term: histone H3K27 methyltransferase activity
modifier: INCREASED
term:
id: GO:0046976
label: histone H3K27 methyltransferase activity
biological_processes:
- preferred_term: negative regulation of gene expression, epigenetic
modifier: INCREASED
term:
id: GO:0045814
label: negative regulation of gene expression, epigenetic
downstream:
- target: Aberrant Proliferation and Blocked Differentiation
description: >-
Unopposed PRC2 repression sustains an undifferentiated, proliferative tumor
state.
causal_link_type: DIRECT
evidence:
- reference: PMID:33035459
reference_title: "Tazemetostat in advanced epithelioid sarcoma with loss of INI1/SMARCB1: an international, open-label, phase 2 basket study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Over 90% of tumours have lost INI1 expression, leading to oncogenic dependence on the transcriptional repressor EZH2."
explanation: This phase 2 study states the mechanistic rationale directly - loss of INI1 in over 90% of epithelioid sarcomas creates an oncogenic dependence on the EZH2 transcriptional repressor.
- name: Aberrant Proliferation and Blocked Differentiation
description: >-
The combined loss of SWI/SNF tumor-suppressor function and the resulting
epigenetic repression drive a proliferative, poorly differentiated phenotype
with retained epithelial-mesenchymal hybrid marker expression, manifesting as
progressive locally infiltrative tumor growth.
biological_processes:
- preferred_term: cell population proliferation
modifier: INCREASED
term:
id: GO:0008283
label: cell population proliferation
- preferred_term: cell differentiation
modifier: DECREASED
term:
id: GO:0030154
label: cell differentiation
downstream:
- target: Local Invasion and Metastatic Dissemination
description: >-
The proliferative, infiltrative tumor invades local soft tissues and
disseminates, with a characteristic propensity for regional lymph node and
pulmonary spread.
causal_link_type: INDIRECT_KNOWN_INTERMEDIATES
- target: Soft Tissue Mass
description: >-
Proliferative growth of epithelioid and spindle tumor cells produces the
clinically apparent soft-tissue or dermal mass.
causal_link_type: DIRECT
- name: Local Invasion and Metastatic Dissemination
description: >-
Epithelioid sarcoma is locally infiltrative along fascial planes and tendon
sheaths and metastasizes, with an unusually high rate of regional lymph node
involvement (in addition to pulmonary spread) compared with most soft-tissue
sarcomas. This behavior underlies its high recurrence and metastatic rates.
biological_processes:
- preferred_term: tumor cell migration and invasion
modifier: INCREASED
term:
id: GO:0016477
label: cell migration
downstream:
- target: Skin Ulceration
description: >-
Superficial distal tumor invasion can break down overlying skin and
present as a non-healing ulcer.
causal_link_type: INDIRECT_KNOWN_INTERMEDIATES
- target: Regional Lymph Node Involvement
description: >-
Metastatic dissemination from the primary tumor commonly involves regional
lymph nodes.
causal_link_type: DIRECT
evidence:
- reference: PMID:4014539
reference_title: "Epithelioid sarcoma. Diagnosis, prognostic indicators, and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Follow-up data, available in 202 cases (84%), showed a 77% recurrence and a 45% metastatic rate. The most common initial sites of metastasis were lymph nodes (48%) and lungs (25%)."
explanation: The Chase & Enzinger series quantifies the high recurrence and metastatic rates and identifies lymph nodes as the leading metastatic site, the clinical output of the invasive/disseminating tumor phenotype.
histopathology:
- name: Pseudogranulomatous Nodular Pattern
finding_term:
preferred_term: granuloma-like growth pattern
term:
id: NCIT:C36059
label: Granuloma-Like Growth Pattern
description: >-
Classic distal-type epithelioid sarcoma forms nodules of epithelioid and spindle
cells with central necrosis, producing a pseudogranulomatous appearance that can
mimic a necrotizing granuloma or rheumatoid nodule.
evidence:
- reference: PMID:9042279
reference_title: '"Proximal-type" epithelioid sarcoma, a distinctive aggressive neoplasm showing rhabdoid features. Clinicopathologic, immunohistochemical, and ultrastructural study of a series.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "A granuloma-like pattern reminiscent of that observed in classic epithelioid sarcoma was observed in only two cases."
explanation: The defining proximal-type series notes the granuloma-like (pseudogranulomatous) pattern as a feature characteristic of classic epithelioid sarcoma, contrasting it with the proximal variant.
- name: Spindle Cell Component
finding_term:
preferred_term: spindle cell pattern
term:
id: NCIT:C53643
label: Spindle Cell Pattern
description: >-
A spindle cell component blending with the epithelioid cells is characteristic,
contributing to the epithelial-mesenchymal hybrid phenotype.
- name: Tumor Cell Necrosis
finding_term:
preferred_term: tumor cell necrosis
term:
id: NCIT:C35957
label: Tumor Cell Necrosis
description: >-
Central (geographic) necrosis within tumor nodules is common, especially in the
classic type, contributing to the pseudogranulomatous pattern.
evidence:
- reference: PMID:9042279
reference_title: '"Proximal-type" epithelioid sarcoma, a distinctive aggressive neoplasm showing rhabdoid features. Clinicopathologic, immunohistochemical, and ultrastructural study of a series.'
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Areas of necrosis were often seen."
explanation: The proximal-type series documents frequent tumor necrosis, a recurrent histologic feature across epithelioid sarcoma.
phenotypes:
- category: Musculoskeletal
name: Soft Tissue Mass
diagnostic: true
description: >-
Epithelioid sarcoma presents as a slowly growing soft-tissue or dermal mass;
distal-type lesions are often small superficial nodules of the hand/forearm,
while proximal-type tumors are larger deep masses.
phenotype_term:
preferred_term: Soft tissue neoplasm
term:
id: HP:0031459
label: Soft tissue neoplasm
evidence:
- reference: PMID:4014539
reference_title: "Epithelioid sarcoma. Diagnosis, prognostic indicators, and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The tumor was generally firm and nontender, and involved the dermis, subcutis or deeper soft tissues, particularly fascial planes, aponeuroses, and tendon sheaths."
explanation: The Chase & Enzinger series of 241 cases documents epithelioid sarcoma presenting as a firm soft-tissue mass involving dermis, subcutis, and deeper soft tissues.
- category: Integument
name: Skin Ulceration
subtype: Classic
description: >-
Distal-type lesions frequently ulcerate the overlying skin and can be mistaken
for a non-healing ulcer or infectious process.
phenotype_term:
preferred_term: Skin ulcer
term:
id: HP:0200042
label: Skin ulcer
evidence:
- reference: PMID:29887710
reference_title: "Epithelioid Sarcoma Presenting as Recurrent Thumb Ulcer: a Lesson to Learn."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "We here report a case of left thumb epithelioid sarcoma that presented as an ulcer and subsequently metastasized to forearm, arm, axillary lymph nodes, and lungs."
explanation: This case report documents a distal (thumb) epithelioid sarcoma presenting as a skin ulcer, illustrating the characteristic ulcerative presentation of distal-type disease.
- category: Hematologic
name: Regional Lymph Node Involvement
description: >-
Epithelioid sarcoma has an unusually high propensity for regional lymph node
metastasis compared with most soft-tissue sarcomas, manifesting as abnormal
(involved) regional lymph nodes.
phenotype_term:
preferred_term: Lymph node involvement
term:
id: HP:0002733
label: Abnormal lymph node morphology
evidence:
- reference: PMID:4014539
reference_title: "Epithelioid sarcoma. Diagnosis, prognostic indicators, and treatment."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The most common initial sites of metastasis were lymph nodes (48%) and lungs (25%)."
explanation: The Chase & Enzinger 241-case series establishes lymph nodes as the single most common site of initial metastasis in epithelioid sarcoma, an unusual feature for soft-tissue sarcoma.
genetic:
- name: SMARCB1
gene_term:
preferred_term: SMARCB1
term:
id: hgnc:11103
label: SMARCB1
association: Somatic Loss-of-Function
notes: >-
Inactivation of SMARCB1 (INI1) is the defining genetic event in most epithelioid
sarcomas, mechanistically linking this tumor to the broader family of
SWI/SNF-deficient malignancies.
evidence:
- reference: PMID:19033866
reference_title: "Loss of INI1 expression is characteristic of both conventional and proximal-type epithelioid sarcoma."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "INI1 (hSNF5/SMARCB1), a member of the SWI/SNF chromatin remodeling complex located on chromosome 22q11.2, is deleted or/or mutated in strictly defined malignant rhabdoid tumors (MRT) of infancy. Recent studies suggest that some epithelioid sarcomas (ES) also show inactivation of INI1."
explanation: Establishes SMARCB1/INI1 as a SWI/SNF subunit on 22q11.2 inactivated in epithelioid sarcoma, the shared driver with malignant rhabdoid tumor.
biochemical:
- name: INI1/SMARCB1 Immunohistochemistry
notes: >-
Loss of nuclear INI1/BAF47 staining is the canonical diagnostic biomarker and
reflects biallelic SMARCB1 inactivation; it distinguishes epithelioid sarcoma
from histologic mimics such as carcinoma and melanoma.
treatments:
- name: Wide Surgical Excision
description: >-
Complete wide local excision with negative margins is the mainstay of treatment
for localized disease; regional lymph node evaluation is considered given the
propensity for nodal spread.
treatment_term:
preferred_term: surgical procedure
term:
id: MAXO:0000004
label: surgical procedure
- name: Adjunctive Radiotherapy
description: >-
High-dose radiotherapy to the excision site is used adjunctively for local
control given the high local-recurrence rate of epithelioid sarcoma after
surgery.
treatment_term:
preferred_term: radiation therapy
term:
id: MAXO:0000014
label: radiation therapy
therapeutic_modality: RADIOTHERAPY
evidence:
- reference: PMID:4014539
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "radiotherapy to the excision site may prove to be of additional value"
explanation: >-
Supports adjunctive high-dose radiotherapy to the excision site as a
local-control measure in epithelioid sarcoma.
- name: Tazemetostat (EZH2 Inhibitor)
description: >-
Tazemetostat is an oral EZH2 inhibitor FDA-approved for adults and adolescents
with metastatic or locally advanced INI1-deficient (SMARCB1-deficient)
epithelioid sarcoma not eligible for complete resection, targeting the EZH2
dependency created by SMARCB1 loss.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: tazemetostat
term:
id: NCIT:C107506
label: Tazemetostat
therapeutic_modality: SMALL_MOLECULE
target_mechanisms:
- target: EZH2/PRC2 Dependency and H3K27 Hypermethylation
treatment_effect: INHIBITS
description: >-
Tazemetostat selectively inhibits EZH2 methyltransferase activity, blocking
the H3K27 methylation dependency that SMARCB1-deficient epithelioid sarcomas
acquire when SWI/SNF antagonism of PRC2 is lost.
evidence:
- reference: PMID:33035459
reference_title: "Tazemetostat in advanced epithelioid sarcoma with loss of INI1/SMARCB1: an international, open-label, phase 2 basket study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "we report the clinical activity and safety of tazemetostat, an oral selective EZH2 inhibitor, in patients with epithelioid sarcoma."
explanation: This phase 2 basket study reports the clinical activity of the oral selective EZH2 inhibitor tazemetostat in INI1-negative epithelioid sarcoma, the basis for its FDA approval.
- reference: PMID:33035459
reference_title: "Tazemetostat in advanced epithelioid sarcoma with loss of INI1/SMARCB1: an international, open-label, phase 2 basket study."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "median duration of response was not reached"
explanation: Despite a modest objective response rate, tazemetostat produced durable responses in advanced epithelioid sarcoma (median duration of response not reached), supporting partial but meaningful efficacy.
clinical_trials:
- name: NCT02601950
phase: PHASE_II
status: ACTIVE_NOT_RECRUITING
description: >-
International open-label phase 2 basket study of the EZH2 inhibitor tazemetostat
in INI1-negative tumors, including the epithelioid sarcoma cohort (cohort 5) that
supported regulatory approval.
target_phenotypes:
- preferred_term: Soft tissue neoplasm
term:
id: HP:0031459
label: Soft tissue neoplasm
evidence:
- reference: PMID:33035459
reference_title: "Tazemetostat in advanced epithelioid sarcoma with loss of INI1/SMARCB1: an international, open-label, phase 2 basket study."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "This trial is registered with ClinicalTrials.gov, NCT02601950, and is ongoing."
explanation: The tazemetostat epithelioid sarcoma cohort was conducted under ClinicalTrials.gov registration NCT02601950.
disease_term:
preferred_term: epithelioid sarcoma
term:
id: MONDO:0017387
label: epithelioid sarcoma
mappings:
mondo_mappings:
- term:
id: MONDO:0017387
label: epithelioid sarcoma
mapping_predicate: skos:exactMatch
mapping_source: MONDO
mapping_justification: MONDO provides an exact disease term for epithelioid sarcoma.
classifications:
harrisons_chapter:
- classification_value: ONCOLOGY_HEMATOLOGY
References & Deep Research
Deep Research
1Question: You are an expert researcher providing comprehensive, well-cited information.
Provide detailed information focusing on: 1. Key concepts and definitions with current understanding 2. Recent developments and latest research (prioritize 2023-2024 sources) 3. Current applications and real-world implementations 4. Expert opinions and analysis from authoritative sources 5. Relevant statistics and data from recent studies
Format as a comprehensive research report with proper citations. Include URLs and publication dates where available. Always prioritize recent, authoritative sources and provide specific citations for all major claims.
Disease Characteristics Research Template
Target Disease
- Disease Name: Epithelioid Sarcoma
- MONDO ID: (if available)
- Category:
Research Objectives
Please provide a comprehensive research report on Epithelioid Sarcoma covering all of the disease characteristics listed below. This report will be used to populate a disease knowledge base entry. Be thorough and cite primary literature (PMID preferred) for all claims.
For each section, suggested databases/resources are listed. These are the first places you should search for information on each topic.
1. Disease Information
Search first: OMIM, Orphanet, ICD-10/ICD-11, MeSH, PubMed
- What is the disease? Provide a concise overview.
- What are the key identifiers? (OMIM, Orphanet, ICD-10/ICD-11, MeSH, Mondo)
- What are the common synonyms and alternative names?
- Is the information derived from individual patients (e.g., EHR) or aggregated disease-level resources?
2. Etiology
- Disease Causal Factors: What are the primary causes? (genetic, environmental, infectious, mechanistic)
- Risk Factors:
Search first: PubMed, Cochrane Library, UpToDate, clinical guidelines, ClinVar, ClinGen, GWAS Catalog, PheGenI, CTD, CDC, WHO, epidemiological databases
- Genetic risk factors (causal variants, susceptibility loci, modifier genes)
- Environmental risk factors (toxins, lifestyle, occupational exposures, age, sex, family history)
- Protective Factors:
Search first: PubMed, Cochrane Library, clinical trial databases, GWAS Catalog, gnomAD, WHO, CDC, nutrition databases
- Genetic protective factors (protective variants, modifier alleles)
- Environmental protective factors (diet, lifestyle, exposures that reduce risk)
- Gene-Environment Interactions: How do genetic and environmental factors interact to influence disease?
Search first: CTD, PubMed, PheGenI, GxE databases
3. Phenotypes
Search first: HPO (Human Phenotype Ontology), OMIM, Orphanet, PubMed, clinicaltrials.gov, MedDRA, SNOMED CT, DECIPHER, LOINC
For each phenotype, provide: - Phenotype type: symptoms, clinical signs, physical manifestations, behavioral changes, or laboratory abnormalities
For symptoms/signs: HPO, OMIM, Orphanet, PubMed For behavioral changes: HPO, DSM, RDoC (Research Domain Criteria), PubMed For laboratory abnormalities: LOINC, SNOMED CT, LabTests Online, PubMed - Phenotype characteristics: Search first: OMIM, Orphanet, HPO, PubMed - Age of symptom onset (neonatal, childhood, adult-onset, late-onset) - Symptom severity (mild, moderate, severe, variable) - Symptom progression (stable, progressive, episodic, fluctuating) - Frequency among affected individuals (percentage or qualitative) - Quality of life impact: Effects on daily functioning and well-being (per-phenotype when possible) Search first: EQ-5D database, SF-36, WHO QOL databases, PubMed - Suggest HPO (Human Phenotype Ontology) terms for each phenotype
4. Genetic/Molecular Information
- Causal Genes: Gene mutations or chromosomal abnormalities responsible for disease (gene symbols, OMIM IDs)
Search first: OMIM, ClinVar, HGMD, Ensembl, NCBI Gene
- Pathogenic Variants:
- Affected genes (gene symbols, HGNC IDs) > Search first: OMIM, NCBI Gene, Ensembl, HGNC, UniProt, GeneCards
- Variant classification (pathogenic, likely pathogenic, VUS per ACMG/AMP guidelines) > Search first: ClinVar, ClinGen, ACMG/AMP guidelines, VarSome
- Variant type/class (missense, frameshift, nonsense, splice-site, structural)
- Allele frequency in population databases > Search first: gnomAD, 1000 Genomes, ExAC, TOPMed, dbSNP
- Somatic vs germline origin > Search first: COSMIC (somatic), ClinVar, ICGC, TCGA
- Functional consequences (loss of function, gain of function, dominant negative)
- Modifier Genes: Genes that modify disease severity or expression
- Epigenetic Information: DNA methylation, histone modifications, chromatin changes affecting disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Chromosomal Abnormalities: Large-scale genetic changes (aneuploidy, translocations, inversions)
Search first: DECIPHER, ClinVar, ECARUCA, UCSC Genome Browser
5. Environmental Information
- Environmental Factors: Non-genetic contributing factors (toxins, radiation, pollution, occupational exposure)
Search first: CTD (Comparative Toxicogenomics Database), TOXNET, PubMed, EPA databases
- Lifestyle Factors: Behavioral factors (smoking, diet, exercise, alcohol consumption)
Search first: CDC databases, WHO, PubMed, NHANES
- Infectious Agents: If applicable, pathogens causing or triggering disease (bacteria, viruses, fungi, parasites)
Search first: NCBI Taxonomy, ViPR, BV-BRC, MicrobeDB, GIDEON
6. Mechanism / Pathophysiology
- Molecular Pathways: Specific signaling cascades or biochemical pathways involved (Wnt, MAPK, mTOR, PI3K-AKT, etc.)
Search first: KEGG, Reactome, WikiPathways, PathBank, BioCyc
- Cellular Processes: Cell-level mechanisms (apoptosis, autophagy, cell cycle dysregulation, inflammation, etc.)
Search first: Gene Ontology (GO), Reactome, KEGG, PubMed
- Protein Dysfunction: How protein structure or function is altered (misfolding, aggregation, loss of function, gain of function)
Search first: UniProt, PDB (Protein Data Bank), InterPro, Pfam, AlphaFold
- Metabolic Changes: Alterations in metabolic processes (energy metabolism, lipid metabolism, amino acid metabolism)
Search first: KEGG, BioCyc, HMDB (Human Metabolome Database), BRENDA
- Immune System Involvement: Role of immune response (autoimmunity, immunodeficiency, chronic inflammation)
Search first: ImmPort, Immunome Database, IEDB, Gene Ontology
- Tissue Damage Mechanisms: How tissues/ are injured (oxidative stress, ischemia, fibrosis, necrosis)
Search first: PubMed, Gene Ontology, Reactome
- Biochemical Abnormalities: Specific molecular defects (enzyme deficiencies, receptor dysfunction, ion channel defects)
Search first: BRENDA, UniProt, KEGG, OMIM, PubMed
- Epigenetic Changes: DNA methylation, histone modifications affecting gene expression in disease
Search first: ENCODE, Roadmap Epigenomics, MethBase, DiseaseMeth
- Molecular Profiling (if available):
- Transcriptomics/gene expression changes > Search first: GEO (Gene Expression Omnibus), ArrayExpress, GTEx, Human Cell Atlas, SRA
- Proteomics findings > Search first: PRIDE, ProteomeXchange, Human Protein Atlas, STRING, BioGRID
- Metabolomics signatures > Search first: MetaboLights, Metabolomics Workbench, HMDB, METLIN
- Lipidomics alterations > Search first: LIPID MAPS, SwissLipids, LipidHome, Metabolomics Workbench
- Genomic structural features > Search first: UCSC Genome Browser, Ensembl, NCBI, dbVar, DGV
- Advanced Technologies (if applicable):
- Single-cell analysis findings (cell-type specific mechanisms, cellular heterogeneity) > Search first: Human Cell Atlas, Single Cell Portal, GEO, CELLxGENE
- Spatial transcriptomics findings > Search first: GEO, Spatial Research, Vizgen, 10x Genomics data
- Multi-omics integration results > Search first: TCGA, ICGC, cBioPortal, LinkedOmics, PubMed
- Functional genomics screens (CRISPR, RNAi) > Search first: DepMap, GenomeRNAi, PubMed, BioGRID ORCS
For each mechanism, describe: - The causal chain from initial trigger to clinical manifestation - Which mechanisms are upstream vs downstream - What cell types and biological processes are involved - Suggest GO terms for biological processes and CL terms for cell types
7. Anatomical Structures Affected
- Organ Level:
- Primary organs directly affected
- Secondary organ involvement (complications, secondary effects)
- Body systems involved (cardiovascular, nervous, digestive, respiratory, endocrine, etc.)
Search first: Uberon, FMA (Foundational Model of Anatomy), OMIM, HPO, ICD-11, MeSH, SNOMED CT
- Tissue and Cell Level:
- Specific tissue types affected (epithelial, connective, muscle, nervous)
- Specific cell populations targeted (with Cell Ontology terms)
Search first: Uberon, Human Protein Atlas, Cell Ontology, Human Cell Atlas, CellMarker, PanglaoDB
- Subcellular Level:
- Cellular compartments involved (mitochondria, nucleus, ER, lysosomes) (with GO Cellular Component terms)
Search first: Gene Ontology (Cellular Component), UniProt, Human Protein Atlas
- Localization:
- Specific anatomical sites (with UBERON terms) > Search first: FMA, Uberon, NeuroNames (for brain), SNOMED CT
- Lateralization (unilateral, bilateral, asymmetric) > Search first: HPO, clinical literature, imaging databases
8. Temporal Development
- Onset:
- Typical age of onset (congenital, pediatric, adult, geriatric)
- Onset pattern (acute, subacute, chronic, insidious)
Search first: OMIM, Orphanet, HPO, PubMed
- Progression:
- Disease stages (early, intermediate, advanced, end-stage) > Search first: Cancer Staging Manual (AJCC), WHO classifications, PubMed
- Progression rate (rapid, slow, variable)
- Disease course pattern (episodic, relapsing-remitting, progressive, stable)
- Disease duration (self-limited, chronic lifelong)
Search first: Disease registries, longitudinal cohort databases, natural history studies, PubMed, Orphanet, OMIM
- Patterns:
- Remission patterns (spontaneous, treatment-induced) > Search first: Clinical trial databases, disease registries, PubMed
- Critical periods (time windows of vulnerability or opportunity for intervention) > Search first: PubMed, developmental biology databases, clinical guidelines
9. Inheritance and Population
- Epidemiology:
- Prevalence (cases per 100,000 at given time)
- Incidence (new cases per 100,000 per year)
Search first: Orphanet, CDC, WHO, GBD (Global Burden of Disease), national registries, SEER, disease registries
- For Genetic Etiology:
- Inheritance pattern (AD, AR, X-linked, mitochondrial, multifactorial, polygenic) > Search first: OMIM, Orphanet, ClinVar, GTR (Genetic Testing Registry)
- Penetrance (complete, incomplete, age-dependent) > Search first: ClinVar, OMIM, PubMed, ClinGen
- Expressivity (variable, consistent) > Search first: OMIM, ClinVar, PubMed
- Genetic anticipation (increasing severity in successive generations) > Search first: OMIM, PubMed (especially for repeat expansion disorders)
- Germline mosaicism > Search first: ClinVar, OMIM, genetic counseling literature, PubMed
- Founder effects (population-specific mutations) > Search first: gnomAD, population genetics databases, PubMed
- Consanguinity role > Search first: OMIM, population studies, genetic counseling resources
- Carrier frequency > Search first: gnomAD, carrier screening databases, GeneReviews, GTR
- Population Demographics:
- Affected populations (ethnic or demographic groups with higher prevalence) > Search first: gnomAD, 1000 Genomes, PAGE Study, PubMed, population registries
- Geographic distribution (endemic areas, regional variation) > Search first: WHO, CDC, GBD, Orphanet, geographic epidemiology databases
- Geographic distribution of specific variants
- Sex ratio (male:female) > Search first: Disease registries, OMIM, PubMed, epidemiological databases
- Age distribution of affected individuals > Search first: CDC, disease registries, SEER, Orphanet
10. Diagnostics
- Clinical Tests:
- Laboratory tests (blood, urine, tissue chemistry, specific enzyme assays) > Search first: LOINC, LabTests Online, PubMed
- Biomarkers (proteins, metabolites, genetic markers, circulating biomarkers) > Search first: FDA Biomarker List, BEST (Biomarkers, EndpointS, and other Tools), PubMed
- Imaging studies (X-ray, CT, MRI, PET, ultrasound) > Search first: RadLex, DICOM, Radiopaedia, imaging databases
- Functional tests (pulmonary function, cardiac stress tests) > Search first: LOINC, clinical guidelines, PubMed
- Electrophysiology (EEG, EMG, ECG, nerve conduction studies) > Search first: LOINC, clinical neurophysiology databases, PubMed
- Biopsy findings (histopathology, immunohistochemistry) > Search first: SNOMED CT, College of American Pathologists resources, PubMed
- Pathology findings (microscopic examination) > Search first: SNOMED CT, Digital Pathology databases, PubMed
- Genetic Testing:
Search first: GTR (Genetic Testing Registry), GeneReviews, ClinGen
- Overview of recommended genetic testing approach
- Whole genome sequencing (WGS) utility > Search first: GTR, ClinVar, GEL (Genomics England), gnomAD
- Whole exome sequencing (WES) utility > Search first: GTR, ClinVar, OMIM, GeneMatcher
- Gene panels (which panels, which genes) > Search first: GTR, ClinVar, laboratory-specific databases
- Single gene testing > Search first: GTR, ClinVar, OMIM, GeneReviews
- Chromosomal microarray (CMA) > Search first: DECIPHER, ClinVar, dbVar, ECARUCA
- Karyotyping > Search first: Chromosome Abnormality Database, ClinVar, cytogenetics resources
- FISH > Search first: ClinVar, cytogenetics databases, PubMed
- Mitochondrial DNA testing > Search first: MITOMAP, MSeqDR, ClinVar, GTR
- Repeat expansion testing > Search first: GTR, ClinVar, repeat expansion databases, PubMed
- Omics-Based Diagnostics (if applicable):
- RNA sequencing / transcriptomics > Search first: GEO, ArrayExpress, GTEx, RNA-seq databases
- Proteomics > Search first: PRIDE, ProteomeXchange, FDA Biomarker database
- Metabolomics > Search first: MetaboLights, Metabolomics Workbench, HMDB
- Epigenomics > Search first: GEO, ENCODE, Roadmap Epigenomics, MethBase
- Liquid biopsy > Search first: COSMIC, ClinVar, liquid biopsy databases, PubMed
- Clinical Criteria:
- Standardized diagnostic criteria (DSM, ICD, society guidelines) > Search first: DSM-5, ICD-11, clinical society guidelines, UpToDate
- Differential diagnosis (other conditions to rule out, with distinguishing features) > Search first: DynaMed, UpToDate, clinical decision support systems
- Screening:
- Screening methods for asymptomatic individuals (newborn screening, carrier screening, cascade screening) > Search first: ACMG recommendations, CDC newborn screening, GTR
11. Outcome/Prognosis
- Survival and Mortality:
- Survival rate (5-year, 10-year, overall) > Search first: SEER, cancer registries, disease-specific registries, PubMed
- Life expectancy (with and without treatment if applicable) > Search first: Orphanet, disease registries, actuarial databases, PubMed
- Mortality rate > Search first: CDC, WHO, GBD, national mortality databases
- Disease-specific mortality (deaths directly attributable to disease) > Search first: Disease registries, CDC Wonder, GBD, PubMed
- Morbidity and Function:
- Morbidity (disease-related disability and health impacts) > Search first: GBD, WHO, disability databases, PubMed
- Disability outcomes (long-term functional impairments) > Search first: ICF (International Classification of Functioning), disability registries
- Quality of life measures (EQ-5D, SF-36, PROMIS, disease-specific tools) > Search first: EQ-5D database, SF-36, PROMIS, PubMed
- Disease Course:
- Complications (secondary problems: infections, organ failure, etc.) > Search first: ICD codes, disease registries, clinical databases, PubMed
- Recovery potential (likelihood and extent of recovery, with vs without treatment) > Search first: Natural history studies, rehabilitation databases, PubMed
- Prediction:
- Prognostic factors (age, disease severity, biomarkers, treatment response) > Search first: Prognostic models databases, clinical calculators, PubMed
- Prognostic biomarkers (molecular markers predicting disease course) > Search first: FDA Biomarker database, PubMed, cancer prognostic databases
12. Treatment
- Pharmacotherapy:
- Pharmacological treatments (drug names, drug classes, mechanisms of action) > Search first: DrugBank, RxNorm, ATC classification, DailyMed, FDA databases
- Pharmacogenomics (how genetic variants affect drug metabolism, efficacy, toxicity) > Search first: PharmGKB, CPIC (Clinical Pharmacogenetics), FDA Table of PGx Biomarkers
- Advanced Therapeutics:
- Gene therapy (viral vectors, CRISPR, gene replacement, gene editing) > Search first: ClinicalTrials.gov, FDA gene therapy database, ASGCT resources
- Cell therapy (stem cell transplant, CAR-T, cellular therapeutics) > Search first: ClinicalTrials.gov, FDA cell therapy database, FACT standards
- RNA-based therapies (ASOs, siRNA, mRNA therapies) > Search first: ClinicalTrials.gov, FDA approvals, PubMed
- Targeted therapies (treatments directed at specific molecular targets) > Search first: My Cancer Genome, OncoKB, ClinicalTrials.gov, FDA approvals
- Immunotherapies (checkpoint inhibitors, monoclonal antibodies) > Search first: Cancer Immunotherapy Database, FDA approvals, ClinicalTrials.gov
- Surgical and Interventional:
- Surgical interventions (types of surgery, timing, outcomes) > Search first: CPT codes, surgical registries, clinical guidelines, PubMed
- Supportive and Rehabilitative:
- Supportive care (symptom management, pain control, nutrition) > Search first: Clinical guidelines, Cochrane Library, PubMed
- Rehabilitation (physical therapy, occupational therapy, speech therapy) > Search first: Rehabilitation medicine databases, clinical guidelines, PubMed
- Experimental:
- Experimental treatments in clinical trials (with NCT identifiers if available) > Search first: ClinicalTrials.gov, EU Clinical Trials Register, WHO ICTRP
- Treatment Outcomes:
- Treatment response rates > Search first: Clinical trial databases, FDA reviews, systematic reviews, PubMed
- Side effects and adverse events > Search first: FDA Adverse Event Reporting System (FAERS), MedWatch, PubMed
- Treatment Strategy:
- Treatment algorithms (clinical pathways, decision trees) > Search first: Clinical practice guidelines, NCCN Guidelines, UpToDate
- Combination therapies > Search first: ClinicalTrials.gov, treatment guidelines, PubMed
- Personalized medicine approaches (genotype-guided treatment) > Search first: My Cancer Genome, CIViC, PharmGKB, precision medicine databases
For each treatment, suggest MAXO (Medical Action Ontology) terms where applicable.
13. Prevention
- Prevention Levels:
- Primary prevention (preventing disease occurrence: vaccination, risk factor modification) > Search first: CDC, WHO, USPSTF recommendations, Cochrane Library
- Secondary prevention (early detection and treatment: screening programs, early intervention) > Search first: USPSTF, CDC screening guidelines, WHO
- Tertiary prevention (preventing complications in those with disease) > Search first: Clinical guidelines, disease management protocols, PubMed
- Immunization: Vaccine strategies (if applicable)
Search first: CDC vaccine schedules, WHO immunization, FDA vaccine database
- Screening and Early Detection:
- Screening programs (population-based: newborn screening, cancer screening) > Search first: CDC screening programs, USPSTF, cancer screening databases
- Genetic screening (carrier screening, preimplantation genetic diagnosis, prenatal testing) > Search first: ACMG recommendations, ACOG guidelines, GTR
- Risk stratification (identifying high-risk individuals for targeted prevention) > Search first: Risk prediction models, clinical calculators, PubMed
- Behavioral Interventions: Lifestyle modifications to reduce risk
Search first: CDC, WHO, behavioral intervention databases, Cochrane Library
- Counseling: Genetic counseling (risk assessment, family planning guidance)
Search first: NSGC resources, ACMG guidelines, GeneReviews
- Public Health:
- Public health interventions (sanitation, vector control, health education) > Search first: CDC, WHO, public health databases, PubMed
- Environmental interventions (reducing environmental risk factors) > Search first: EPA databases, WHO environmental health, PubMed
- Prophylaxis: Preventive medications or procedures
Search first: Clinical guidelines, FDA approvals, PubMed
14. Other Species / Natural Disease
- Taxonomy: Species affected (with NCBI Taxon identifiers)
Search first: NCBI Taxonomy
- Breed: Specific breeds affected (with VBO identifiers if applicable)
Search first: VBO (Vertebrate Breed Ontology)
- Gene: Orthologous genes in other species (with NCBI Gene IDs)
Search first: NCBI Gene
- Natural Disease:
- Naturally occurring disease in other species (companion animals, wildlife) > Search first: OMIA (Online Mendelian Inheritance in Animals), VetCompass, PubMed
- Veterinary relevance and importance in animal health > Search first: OMIA, veterinary databases, PubMed
- Comparative Biology:
- Comparative pathology (similarities and differences across species) > Search first: OMIA, comparative pathology databases, PubMed
- Evolutionary conservation of disease mechanisms > Search first: HomoloGene, OrthoMCL, Alliance of Genome Resources
- Transmission (if applicable):
- Zoonotic potential > Search first: CDC zoonotic diseases, WHO zoonoses, GIDEON
- Cross-species susceptibility > Search first: NCBI Taxonomy, veterinary databases, PubMed
15. Model Organisms
- Model Types:
- Model organism type (mammalian, invertebrate, cellular, in vitro) > Search first: Alliance of Genome Resources, model organism databases
- Specific model systems (mouse, rat, zebrafish, Drosophila, C. elegans, yeast, cell lines, organoids, iPSCs) > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, SGD, ATCC, Cellosaurus
- Induced models (drug treatment, surgical intervention, environmental manipulation) > Search first: MGI, model organism databases, PubMed
- Genetic Models:
- Types available (knockout, knock-in, transgenic, conditional, humanized) > Search first: MGI, IMPC, KOMP, EuMMCR, IMSR
- Model Characteristics:
- Phenotype recapitulation (how well model reproduces human disease features) > Search first: Model organism databases, comparative studies, PubMed
- Model limitations (aspects of human disease not captured) > Search first: Model organism databases, PubMed, review articles
- Applications:
- Research applications (what aspects of disease can be studied) > Search first: Model organism databases, PubMed
- Resources:
- Model databases > Search first: MGI, RGD, ZFIN, FlyBase, WormBase, IMSR, EMMA, MMRRC
Citation Requirements
- Cite primary literature (PMID preferred) for all mechanistic and clinical claims
- Prioritize recent reviews and landmark papers
- Include direct quotes from abstracts where possible to support key statements
- Distinguish evidence source types: human clinical, model organism, in vitro, computational
Output Format
Structure your response as a comprehensive narrative organized by the sections above. For each section, provide: - Factual content with specific details (numbers, percentages, gene names, variant nomenclature) - Ontology term suggestions (HPO, GO, CL, UBERON, CHEBI, MAXO, MONDO) where applicable - Evidence citations with PMIDs - Direct quotes from abstracts to support key claims - Clear indication when information is not available or not applicable for this disease
This report will be used to populate a disease knowledge base entry with: - Pathophysiology descriptions with causal chains - Gene/protein annotations (HGNC, GO terms) - Phenotype associations (HP terms) with frequencies - Cell type involvement (CL terms) - Anatomical locations (UBERON terms) - Chemical entities (CHEBI terms) - Treatment annotations (MAXO terms) - Evidence items with PMIDs and exact abstract quotes - Epidemiology, prognosis, diagnostic, and prevention information - Animal model descriptions with phenotype recapitulation details
Comprehensive Disease Characteristics Report: Epithelioid Sarcoma (EpS)
Executive summary
Epithelioid sarcoma (EpS) is an ultra-rare, aggressive soft-tissue sarcoma defined by loss of SMARCB1/INI1 (BAF47) expression, usually from biallelic SMARCB1 inactivation. Two clinicopathologic subtypes are recognized (distal/classic and proximal), and both share the SMARCB1/INI1-deficient biology. Local recurrence and metastatic spread (including lymph node metastasis) are common, and overall survival remains poor in many series. Targeted epigenetic therapy with the EZH2 inhibitor tazemetostat (FDA accelerated approval in 2020) represents a key real-world implementation, though durable benefit occurs in a minority of patients. (grunewald2024translationalaspectsof pages 1-3, grunewald2024translationalaspectsof pages 3-5, czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6)
| Domain | Key finding | Value / summary | Best supporting citation IDs |
|---|---|---|---|
| Ontology identifier | MONDO ID | MONDO:0017387 (epithelioid sarcoma) | (OpenTargets Search: Epithelioid sarcoma) |
| Disease category | Classification | Ultra-rare malignant soft-tissue sarcoma; <1% of all soft-tissue sarcomas; classic/distal and proximal subtypes recognized | (czarnecka2023epithelioidsarcoma pages 1-2, grunewald2024translationalaspectsof pages 3-5) |
| Rarity / prevalence | Prevalence | <2 per 100,000 | (grunewald2024translationalaspectsof pages 3-5) |
| Incidence | Population incidence | ~0.03–0.05 per 100,000 overall; alternatively reported as <0.2 and <0.5 new cases per million/year in EU and US, respectively | (grunewald2024translationalaspectsof pages 3-5, czarnecka2023epithelioidsarcoma pages 1-2) |
| Age distribution | Typical age | Mostly adolescents/young adults in classic descriptions; registry mean age ~46 years with peak in 5th decade in recent consensus | (grunewald2024translationalaspectsof pages 1-3, grunewald2024translationalaspectsof pages 3-5) |
| Sex distribution | Male predominance | Male:female ratio ~1.6 overall; some series report up to 2:1 in distal/classic disease | (grunewald2024translationalaspectsof pages 3-5, tan2023epithelioidsarcomaof pages 1-2) |
| Recurrence | Local recurrence / recurrence risk | 5-year risk of recurrence up to 70%; recurrence rate 63.4% in one large review/SEER-derived summary | (czarnecka2023epithelioidsarcoma pages 2-3, czarnecka2020epithelioidsarcoma—fromgenetics pages 11-13) |
| Nodal metastasis | Regional lymph node involvement | >20% overall in reviews; ~30% in a 2023 review; 12.4% in SEER head/neck/extremity STS analysis; 18% in pediatric/young adult NRSTS cohort | (czarnecka2023epithelioidsarcoma pages 2-3, czarnecka2023epithelioidsarcoma pages 1-2, czarnecka2020epithelioidsarcoma—fromgenetics pages 11-13) |
| Distant metastasis | Hematogenous metastasis | >40% in 2023 review; historical reviews cite 30–75% by 5 years; common sites include lung and liver | (czarnecka2023epithelioidsarcoma pages 1-2, czarnecka2020epithelioidsarcoma—fromgenetics pages 11-13, czarnecka2023epithelioidsarcoma pages 2-3) |
| Survival | Overall prognosis | 5-year relative survival ~50%; 5-year disease-specific survival 55.7% in SEER-derived review; reported 5-year OS ranges ~25–70%; 10-year OS ~60.4% in one review | (grunewald2024translationalaspectsof pages 3-5, czarnecka2020epithelioidsarcoma—fromgenetics pages 11-13) |
| Prognostic factors | Worse outcome associated with | Proximal subtype, tumor >5 cm, multifocality, nodal involvement, vascular invasion, necrosis, high mitotic index/grade, deep axial location, older age, distant metastasis | (czarnecka2023epithelioidsarcoma pages 2-3, czarnecka2020epithelioidsarcoma—fromgenetics pages 11-13, spunt2019clinicalfeaturesand pages 1-3) |
| Hallmark molecular biomarker | SMARCB1 / INI1 loss | Loss of nuclear INI1/SMARCB1 in >90% of cases; biallelic SMARCB1 inactivation drives ~95% of cases in recent consensus | (grunewald2024translationalaspectsof pages 3-5, czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6) |
| Core IHC profile | Positive markers | Cytokeratins, EMA, vimentin; CD34 positive in >50% / about half; ERG positive in ~50% (mostly distal type) | (grunewald2024translationalaspectsof pages 3-5, czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6, czarnecka2023epithelioidsarcoma pages 1-2) |
| Core IHC profile | Typically negative markers | S-100 and CD31 typically negative; desmin/factor VIII usually negative in differential workup | (czarnecka2023epithelioidsarcoma pages 1-2, czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6) |
Table: This table condenses high-yield identifiers, epidemiology, prognosis, and hallmark diagnostic biomarkers for epithelioid sarcoma. It is useful as a quick-reference summary for knowledge base curation and evidence-backed clinical context.
1. Disease information
What is the disease?
EpS is a malignant mesenchymal soft-tissue tumor with epithelioid morphology and epithelial immunophenotype, classically presenting as a slowly growing nodule/mass, but with high risks of recurrence and metastasis. A 2024 expert consensus review describes EpS as an “ultra-rare malignant soft-tissue cancer” and highlights an unfavorable course with fatal outcome in ~50% of cases despite multimodal therapy. (grunewald2024translationalaspectsof pages 1-3, grunewald2024translationalaspectsof pages 3-5)
Direct abstract quote (2024 consensus): “Epithelioid sarcoma (EpS) is an ultra-rare malignant soft-tissue cancer…” (grunewald2024translationalaspectsof pages 1-3)
Key identifiers / ontologies
- MONDO: MONDO:0017387 (via OpenTargets disease mapping) (OpenTargets Search: Epithelioid sarcoma)
- MeSH / ICD-10 / ICD-11 / Orphanet: Not reliably retrievable with the available tool context in this run; these should be filled from authoritative terminologies (Orphanet, ICD-11, MeSH browser) outside the currently retrieved evidence.
Common synonyms / alternative names
- Epithelioid sarcoma (EpS / ES)
- Distal-type (classic/conventional) epithelioid sarcoma
- Proximal-type epithelioid sarcoma (also referred to as “large cell” variant in some pathology literature) (czarnecka2023epithelioidsarcoma pages 1-2, tan2023epithelioidsarcomaof pages 1-2)
Evidence source type
The report integrates aggregated disease-level resources (expert consensus review, reviews) and primary clinical evidence from registries and clinical trials (e.g., ClinicalTrials.gov entries), rather than individual EHR-derived signals. (grunewald2024translationalaspectsof pages 1-3, NCT02601950 chunk 1)
2. Etiology
Disease causal factors
EpS is primarily driven by loss of function of SMARCB1/INI1, a core SWI/SNF chromatin remodeling complex subunit. - 2024 consensus: “biallelic inactivation of the SMARCB1 gene… drives the pathogenesis of 95% EpS.” (grunewald2024translationalaspectsof pages 3-5) - Mechanistically, this defines EpS as a SWI/SNF-deficient cancer with downstream epigenetic dysregulation and dependency on Polycomb/PRC2/EZH2 activity (providing the rationale for EZH2 inhibition). (czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6, kohashi2017oncogenicrolesof pages 1-2)
Risk factors
Genetic risk factors
- Somatic SMARCB1 alterations predominate; most cases show homozygous deletion or other biallelic inactivation. (grunewald2024translationalaspectsof pages 3-5, czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6)
- Germline/constitutional SMARCB1 predisposition appears rare in EpS; 2024 consensus notes only a “rare case with presumed… constitutive heterozygous alteration.” (grunewald2024translationalaspectsof pages 3-5)
Environmental / lifestyle risk factors
No EpS-specific environmental/lifestyle risk factors were identified in the retrieved EpS-focused literature. Available evidence is largely about sarcomas in general and is not subtype-specific.
Protective factors
No established genetic or environmental protective factors are described in the retrieved EpS literature.
Gene–environment interactions
No EpS-specific gene–environment interaction evidence was found in the retrieved corpus.
3. Phenotypes (clinical presentation)
Core clinical phenotype spectrum
EpS often presents as a slowly growing painless mass; symptoms depend on location. Distal/classic EpS often involves distal upper extremities (hands/fingers), while proximal EpS tends to occur in proximal limb girdles, trunk, pelvis, perineum, and genital regions and is more aggressive. (czarnecka2023epithelioidsarcoma pages 1-2, tan2023epithelioidsarcomaof pages 1-2)
Frequency and progression
- High local recurrence risk: 5-year recurrence up to 70% reported in review literature. (czarnecka2023epithelioidsarcoma pages 2-3)
- Metastatic propensity including nodal spread and distant metastases (lung/liver commonly mentioned). (czarnecka2023epithelioidsarcoma pages 2-3)
Suggested HPO terms (examples; mapping requires curation)
Because EpS is a cancer entity, many “phenotypes” are tumor-behavioral and location-specific. Suggested HPO concepts for structured capture include: - HP:0002664 Neoplasm (general) - HP:0002668 Metastasis - HP:0002027 Abdominal pain (for pelvic/peritoneal disease; when present) - HP:0012833 Pain (if painful lesion) - HP:0001250 Seizures / neurologic deficits (only for rare CNS/spinal presentations; case-based) (tan2023epithelioidsarcomaof pages 1-2)
Note: The retrieved evidence does not provide robust phenotype frequency tables with HPO mappings; this would require dedicated HPO/Orphanet extraction.
4. Genetic / molecular information
Causal gene(s)
- SMARCB1 (INI1; BAF47): core SWI/SNF subunit; loss defines EpS. (grunewald2024translationalaspectsof pages 3-5, czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6)
Pathogenic variant classes (tumor / somatic)
- Commonly biallelic inactivation, frequently via homozygous deletion; heterozygous LOF alterations also occur with an uncharacterized second hit in some cases. (grunewald2024translationalaspectsof pages 3-5, czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6)
Epigenetic regulation
INI1 loss is linked to PRC2/EZH2 overactivity and increased H3K27me3, supporting EZH2-targeted therapy. - Quote from mechanistic review: SMARCB1/INI1-deficient tumors show higher EZH2 levels and “elevated levels of H3K27me3…” at polycomb targets. (kohashi2017oncogenicrolesof pages 1-2)
Chromosomal abnormalities
- Extended loss on chromosome 22q around SMARCB1 occurs in about one-third of cases (consensus review). (grunewald2024translationalaspectsof pages 3-5)
Relevant ontology suggestions
- GO (biological process): chromatin remodeling; regulation of transcription; cell cycle control (p16-RB axis)
- GO (molecular function): ATP-dependent chromatin remodeling
- CL (cell types): malignant mesenchymal tumor cell; tumor-associated macrophage (M2); CD8+ T cell (as TME components) (grunewald2024translationalaspectsof pages 11-13)
5. Environmental information
No EpS-specific non-genetic causal exposures were identified in EpS-focused sources retrieved for this report. General sarcoma-level occupational associations exist but cannot be attributed specifically to EpS without subtype-specific studies.
6. Mechanism / pathophysiology
Core causal chain (high-level)
- SMARCB1/INI1 loss → dysfunctional SWI/SNF chromatin remodeling and reduced chromatin occupancy. (grunewald2024translationalaspectsof pages 8-10)
- Downstream epigenetic repression of differentiation/tumor suppressor programs and altered enhancer/promoter activity. (grunewald2024translationalaspectsof pages 8-10)
- PRC2/EZH2 dependency with elevated H3K27me3 at Polycomb targets → rationale for EZH2 inhibition (tazemetostat). (czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6, kohashi2017oncogenicrolesof pages 1-2)
- Additional cooperating alterations (e.g., CDKN2A/B deletions; RB/E2F-axis changes) can affect proliferation and may contribute to drug resistance. (grunewald2024translationalaspectsof pages 3-5, grunewald2024translationalaspectsof pages 10-11)
Key pathways and processes (supported)
- p16–RB–E2F axis: SMARCB1/INI1 impacts cell-cycle control via p16INK4a-RB; loss contributes to proliferation, and CDKN2A/B deletions recur in EpS. (kohashi2017oncogenicrolesof pages 1-2, grunewald2024translationalaspectsof pages 3-5)
- Polycomb/PRC2/EZH2: dependency is a therapeutic vulnerability; EZH2 inhibition may induce apoptosis in INI1-negative tumors and is clinically translated in EpS. (czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6, kohashi2017oncogenicrolesof pages 1-2)
Immune microenvironment
EpS can show immune infiltration despite low TMB; consensus notes PD-L1 expression and cytotoxic T-cell infiltration and suggests potential benefit from immune checkpoint blockade in subsets. (grunewald2024translationalaspectsof pages 8-10, grunewald2024translationalaspectsof pages 11-13)
Suggested GO terms (examples)
- GO:0006338 chromatin remodeling
- GO:0000122 negative regulation of transcription by RNA polymerase II
- GO:0045893 positive regulation of transcription, DNA-templated
- GO:0007049 cell cycle
Suggested CL terms (examples)
- CL:0000084 T cell
- CL:0000625 CD8-positive, alpha-beta T cell
- CL:0000235 macrophage
7. Anatomical structures affected
Organ / site distribution
- Distal/classic EpS: commonly distal extremities (hand/fingers). (czarnecka2023epithelioidsarcoma pages 1-2)
- Proximal EpS: deep soft tissue of proximal limbs, pelvis/perineum, trunk midline, inguinal/genital region. (czarnecka2023epithelioidsarcoma pages 1-2, tan2023epithelioidsarcomaof pages 1-2)
UBERON suggestions (examples)
- Upper limb / hand (UBERON:0002398 / UBERON:0002387)
- Pelvis (UBERON:0001270)
- Trunk (UBERON:0002100)
8. Temporal development
Onset
Often diagnosed in adolescents/young adults, though registry-based data show a peak in the fifth decade (mean ~46 years), reflecting that EpS spans a broad age range. (grunewald2024translationalaspectsof pages 1-3, grunewald2024translationalaspectsof pages 3-5)
Progression
Often indolent initially with diagnostic delays (reported up to 36 months), but with aggressive potential including recurrence and metastasis. (grunewald2024translationalaspectsof pages 1-3, czarnecka2023epithelioidsarcoma pages 1-2)
9. Inheritance and population
Epidemiology
- Prevalence: <2 per 100,000 (2024 consensus). (grunewald2024translationalaspectsof pages 3-5)
- Incidence: 0.03–0.05 per 100,000 (2024 consensus); alternative representation <0.2–0.5 new cases per million/year in EU/US in 2023 review. (grunewald2024translationalaspectsof pages 3-5, czarnecka2023epithelioidsarcoma pages 1-2)
Demographics
- Male predominance (SEER-based summary ~55% male; M:F ~1.6). (grunewald2024translationalaspectsof pages 3-5)
Inheritance
EpS is usually sporadic with somatic SMARCB1 loss; germline predisposition appears rare. (grunewald2024translationalaspectsof pages 3-5)
10. Diagnostics
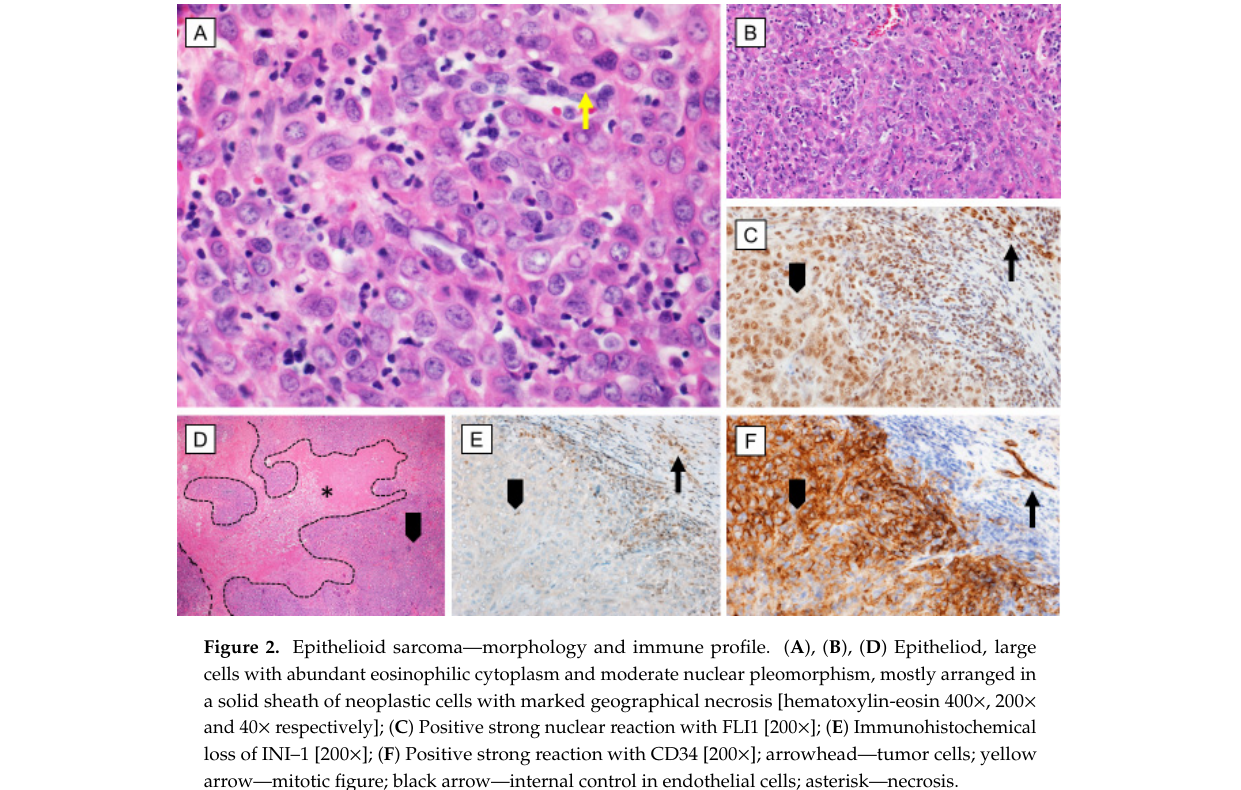
Pathology and immunohistochemistry
Diagnosis relies on histopathology plus IHC. - Typical IHC: cytokeratins and EMA positivity; vimentin positivity; CD34 positive in many cases; negative for S-100 and CD31. (czarnecka2023epithelioidsarcoma pages 1-2, grunewald2024translationalaspectsof pages 3-5) - Hallmark: loss of nuclear INI1/SMARCB1 in >90%. (grunewald2024translationalaspectsof pages 3-5)
Image evidence: Figure showing immunohistochemical loss of INI-1 (SMARCB1) in EpS. (czarnecka2020epithelioidsarcoma—fromgenetics media 68051618)
Differential diagnosis
Broad differential includes benign granulomatous/inflammatory mimics and malignant mimics including synovial sarcoma, melanoma, malignant rhabdoid tumor, and epithelioid MPNST; INI1 loss is helpful but not fully specific because it occurs in other entities. (tan2023epithelioidsarcomaof pages 2-3, czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6)
Molecular testing
Routine molecular testing is often unnecessary if clinicopathologic context + INI1 loss by IHC is convincing; molecular testing is helpful in difficult differentials (e.g., distinguishing from other SMARCB1-deficient tumors). (grunewald2024translationalaspectsof pages 3-5)
11. Outcome / prognosis
Survival
- 5-year relative survival ~50% (consensus). (grunewald2024translationalaspectsof pages 3-5)
- SEER-derived summary: 5-year disease-specific survival 55.7%; 10-year OS 60.4% (review summary). (czarnecka2020epithelioidsarcoma—fromgenetics pages 11-13)
Metastasis and recurrence
- Recurrence: 5-year recurrence up to 70% in review. (czarnecka2023epithelioidsarcoma pages 2-3)
- Distant metastases: >40% in 2023 review; lung/liver common. (czarnecka2023epithelioidsarcoma pages 2-3)
- Nodal involvement: >20% in review sources; EpS is among sarcoma subtypes with notable nodal spread. (czarnecka2023epithelioidsarcoma pages 2-3)
Prognostic factors
Adverse factors: proximal subtype, size >5 cm, multifocality, nodal disease, necrosis, vascular invasion, high mitotic index/grade, deep axial location, older age, distant metastasis. (czarnecka2023epithelioidsarcoma pages 2-3, czarnecka2020epithelioidsarcoma—fromgenetics pages 11-13)
12. Treatment
Local therapy (standard of care)
- Surgery is primary curative treatment: wide excision with clear margins; sometimes amputation; lymph node dissection for nodal disease; sentinel node biopsy considered. (czarnecka2023epithelioidsarcoma pages 2-3, czarnecka2023epithelioidsarcoma pages 1-2)
- Radiotherapy commonly used perioperatively to reduce local recurrence (OS benefit not clearly shown in reviewed summaries). (czarnecka2023epithelioidsarcoma pages 2-3)
MAXO suggestions (examples): surgical excision; radiotherapy; lymph node dissection; sentinel lymph node biopsy.
Systemic therapy
Cytotoxic chemotherapy
Anthracycline-based regimens have modest activity in advanced EpS with ORR around ~22% and median PFS around ~6 months in retrospective series summarized in reviews. (czarnecka2020epithelioidsarcoma—fromgenetics pages 8-10, czarnecka2023epithelioidsarcoma pages 3-5)
Targeted epigenetic therapy: tazemetostat (EZH2 inhibitor)
- FDA accelerated approval for metastatic or locally advanced EpS not eligible for complete resection is noted, with evidence based on ORR and duration of response. (orleni2024pharmacologyandpharmacokinetics pages 1-3)
- In the pivotal phase 2 EpS cohort (NCT02601950), reviewed data report ORR ~15% and DCR ~26% in Cohort 5 with higher ORR in first line vs pretreated; pooled post-hoc median PFS ~3.7 months and median OS ~18 months. (czarnecka2020epithelioidsarcoma—fromgenetics pages 10-11)
ClinicalTrials.gov implementation: - NCT02601950 (completed; open-label phase II, multiple cohorts including EpS): ORR primary endpoint in EpS cohorts; 267 enrolled; dosing 800 mg BID/1600 mg QD across cohorts. (NCT02601950 chunk 1)
Direct abstract quote (2024 consensus): “In 2020, the EZH2 inhibitor tazemetostat was the first targeted therapy approved for EpS…” (grunewald2024translationalaspectsof pages 1-3)
Immunotherapy
EpS may show PD-L1 expression and cytotoxic T cell infiltration, and responses to PD-1/PD-L1 inhibitors have been reported in subsets, but efficacy is inconsistent; immunotherapy remains investigational/selected-use. (grunewald2024translationalaspectsof pages 8-10)
Ongoing/Recent trials: - NCT05407441 (Phase I/II; active not recruiting): tazemetostat + nivolumab + ipilimumab in pediatric INI1-negative/SMARCA4-deficient tumors including EpS. (NCT05407441 chunk 1) - NCT04204941 (tazemetostat + doxorubicin; terminated): termination due to infeasibility/enrollment targets; “No safety concerns.” (NCT04204941 chunk 1)
13. Prevention
No established primary prevention or population screening programs exist for EpS, primarily due to its extreme rarity and predominantly somatic genetic etiology. (grunewald2024translationalaspectsof pages 3-5, grunewald2024translationalaspectsof pages 1-3)
14. Other species / natural disease
No naturally occurring EpS analogs in non-human species were identified in the retrieved evidence.
15. Model organisms / experimental models
Recent consensus emphasizes a developing but still limited model ecosystem. - Many 2D/3D cell lines exist; newer models include PDX and organoid-derived systems (PDO/ODX). Key limitations include over-representation of proximal-type models and lack of immune-competent models. (grunewald2024translationalaspectsof pages 11-13, grunewald2024translationalaspectsof pages 10-11) - Named models include cell lines (e.g., ESX, YCUS-5) and PDX systems used for drug testing and resistance studies. (grunewald2024translationalaspectsof pages 19-20)
Recent developments (2023–2024 emphasis)
2024 translational consensus as a key authoritative synthesis
The 2024 Clinical Cancer Research consensus review is a high-authority, up-to-date synthesis emphasizing: (i) SMARCB1/INI1 loss as defining hallmark; (ii) limits of tazemetostat and immunotherapy efficacy in most patients; (iii) need for new biomarkers, models, and combination strategies. (grunewald2024translationalaspectsof pages 1-3, grunewald2024translationalaspectsof pages 8-10)
2023 clinical and pathology updates
The 2023 ES review reiterates incidence estimates (<0.2–0.5 per million/year) and summarizes recurrence/metastasis patterns and therapeutic approaches, highlighting ongoing reliance on radical surgery and need for referral to sarcoma centers. (czarnecka2023epithelioidsarcoma pages 1-2)
Data gaps and limitations in this run
- Several requested identifiers (Orphanet, ICD-10/11, MeSH) were not directly recoverable from the retrieved evidence corpus.
- Detailed, phenotype-by-phenotype frequencies with HPO terms and validated QoL metrics were not available in the retrieved texts.
- EpS-specific environmental/lifestyle risk factor evidence was not found; the literature appears largely nonspecific to EpS subtype.
Key URLs (publication landing pages)
- Grünewald et al., Clin Cancer Res (2024): https://doi.org/10.1158/1078-0432.ccr-23-2174 (Nov 2024) (grunewald2024translationalaspectsof pages 1-3)
- Czarnecka, Nowotwory J Oncol (2023): https://doi.org/10.5603/njo.a2023.0021 (Jun 2023) (czarnecka2023epithelioidsarcoma pages 1-2)
- Czarnecka et al., Cancers (2020): https://doi.org/10.3390/cancers12082112 (Jul 2020) (czarnecka2020epithelioidsarcoma—fromgenetics pages 1-3)
- Chi et al., JNCI (2023): https://doi.org/10.1093/jnci/djad085 (May 2023) (chi2023tazemetostatfortumors pages 1-2)
- ClinicalTrials.gov NCT02601950: https://clinicaltrials.gov/study/NCT02601950 (NCT02601950 chunk 1)
- ClinicalTrials.gov NCT04204941: https://clinicaltrials.gov/study/NCT04204941 (NCT04204941 chunk 1)
- ClinicalTrials.gov NCT05407441: https://clinicaltrials.gov/study/NCT05407441 (NCT05407441 chunk 1)
References
-
(grunewald2024translationalaspectsof pages 1-3): Thomas G.P. Grünewald, Sophie Postel-Vinay, Robert T. Nakayama, Noah E. Berlow, Andrea Bolzicco, Vincenzo Cerullo, Josephine K. Dermawan, Anna Maria Frezza, Antoine Italiano, Jia Xiang Jin, Francois Le Loarer, Javier Martin-Broto, Andrew Pecora, Antonio Perez-Martinez, Yuen Bun Tam, Franck Tirode, Annalisa Trama, Sandro Pasquali, Mariagrazia Vescia, Lukas Wortmann, Michael Wortmann, Akihiko Yoshida, Kim Webb, Paul H. Huang, Charles Keller, and Cristina R. Antonescu. Translational aspects of epithelioid sarcoma - current consensus. Clinical cancer research : an official journal of the American Association for Cancer Research, 30:1079-1092, Nov 2024. URL: https://doi.org/10.1158/1078-0432.ccr-23-2174, doi:10.1158/1078-0432.ccr-23-2174. This article has 18 citations.
-
(grunewald2024translationalaspectsof pages 3-5): Thomas G.P. Grünewald, Sophie Postel-Vinay, Robert T. Nakayama, Noah E. Berlow, Andrea Bolzicco, Vincenzo Cerullo, Josephine K. Dermawan, Anna Maria Frezza, Antoine Italiano, Jia Xiang Jin, Francois Le Loarer, Javier Martin-Broto, Andrew Pecora, Antonio Perez-Martinez, Yuen Bun Tam, Franck Tirode, Annalisa Trama, Sandro Pasquali, Mariagrazia Vescia, Lukas Wortmann, Michael Wortmann, Akihiko Yoshida, Kim Webb, Paul H. Huang, Charles Keller, and Cristina R. Antonescu. Translational aspects of epithelioid sarcoma - current consensus. Clinical cancer research : an official journal of the American Association for Cancer Research, 30:1079-1092, Nov 2024. URL: https://doi.org/10.1158/1078-0432.ccr-23-2174, doi:10.1158/1078-0432.ccr-23-2174. This article has 18 citations.
-
(czarnecka2020epithelioidsarcoma—fromgenetics pages 3-6): Anna M. Czarnecka, Pawel Sobczuk, Michal Kostrzanowski, Mateusz Spalek, Marzanna Chojnacka, Anna Szumera-Cieckiewicz, and Piotr Rutkowski. Epithelioid sarcoma—from genetics to clinical practice. Cancers, 12:2112, Jul 2020. URL: https://doi.org/10.3390/cancers12082112, doi:10.3390/cancers12082112. This article has 70 citations.
-
(OpenTargets Search: Epithelioid sarcoma): Open Targets Query (Epithelioid sarcoma, 15 results). Buniello, A. et al. (2025). Open Targets Platform: facilitating therapeutic hypotheses building in drug discovery. Nucleic Acids Research.
-
(czarnecka2023epithelioidsarcoma pages 1-2): Anna M. Czarnecka. Epithelioid sarcoma. Nowotwory. Journal of Oncology, 73:154-161, Jun 2023. URL: https://doi.org/10.5603/njo.a2023.0021, doi:10.5603/njo.a2023.0021. This article has 4 citations.
-
(tan2023epithelioidsarcomaof pages 1-2): Yi Liang Tan, Wilson Ong, Jiong Hao Tan, Naresh Kumar, and James Thomas Patrick Decourcy Hallinan. Epithelioid sarcoma of the spine: a review of literature and case report. Journal of Clinical Medicine, 12:5632, Aug 2023. URL: https://doi.org/10.3390/jcm12175632, doi:10.3390/jcm12175632. This article has 5 citations.
-
(czarnecka2023epithelioidsarcoma pages 2-3): Anna M. Czarnecka. Epithelioid sarcoma. Nowotwory. Journal of Oncology, 73:154-161, Jun 2023. URL: https://doi.org/10.5603/njo.a2023.0021, doi:10.5603/njo.a2023.0021. This article has 4 citations.
-
(czarnecka2020epithelioidsarcoma—fromgenetics pages 11-13): Anna M. Czarnecka, Pawel Sobczuk, Michal Kostrzanowski, Mateusz Spalek, Marzanna Chojnacka, Anna Szumera-Cieckiewicz, and Piotr Rutkowski. Epithelioid sarcoma—from genetics to clinical practice. Cancers, 12:2112, Jul 2020. URL: https://doi.org/10.3390/cancers12082112, doi:10.3390/cancers12082112. This article has 70 citations.
-
(spunt2019clinicalfeaturesand pages 1-3): Sheri L. Spunt, Nadine Francotte, Gian Luca De Salvo, Yueh-Yun Chi, Ilaria Zanetti, Andrea Hayes–Jordan, Simon C. Kao, Daniel Orbach, Bernadette Brennan, Aaron R. Weiss, Max M. van Noesel, Lynn Million, Rita Alaggio, David M. Parham, Anna Kelsey, R. Lor Randall, M. Beth McCarville, Gianni Bisogno, Douglas S. Hawkins, and Andrea Ferrari. Clinical features and outcomes of young patients with epithelioid sarcoma: an analysis from the children's oncology group and the european paediatric soft tissue sarcoma study group prospective clinical trials. European Journal of Cancer, 112:98-106, May 2019. URL: https://doi.org/10.1016/j.ejca.2019.02.001, doi:10.1016/j.ejca.2019.02.001. This article has 29 citations and is from a domain leading peer-reviewed journal.
-
(NCT02601950 chunk 1): A Study of Tazemetostat in Adult Participants With Soft Tissue Sarcoma. Epizyme, Inc.. 2015. ClinicalTrials.gov Identifier: NCT02601950
-
(kohashi2017oncogenicrolesof pages 1-2): Kenichi Kohashi and Yoshinao Oda. Oncogenic roles of smarcb1/ini1 and its deficient tumors. Cancer Science, 108:547-552, Apr 2017. URL: https://doi.org/10.1111/cas.13173, doi:10.1111/cas.13173. This article has 250 citations and is from a peer-reviewed journal.
-
(grunewald2024translationalaspectsof pages 11-13): Thomas G.P. Grünewald, Sophie Postel-Vinay, Robert T. Nakayama, Noah E. Berlow, Andrea Bolzicco, Vincenzo Cerullo, Josephine K. Dermawan, Anna Maria Frezza, Antoine Italiano, Jia Xiang Jin, Francois Le Loarer, Javier Martin-Broto, Andrew Pecora, Antonio Perez-Martinez, Yuen Bun Tam, Franck Tirode, Annalisa Trama, Sandro Pasquali, Mariagrazia Vescia, Lukas Wortmann, Michael Wortmann, Akihiko Yoshida, Kim Webb, Paul H. Huang, Charles Keller, and Cristina R. Antonescu. Translational aspects of epithelioid sarcoma - current consensus. Clinical cancer research : an official journal of the American Association for Cancer Research, 30:1079-1092, Nov 2024. URL: https://doi.org/10.1158/1078-0432.ccr-23-2174, doi:10.1158/1078-0432.ccr-23-2174. This article has 18 citations.
-
(grunewald2024translationalaspectsof pages 8-10): Thomas G.P. Grünewald, Sophie Postel-Vinay, Robert T. Nakayama, Noah E. Berlow, Andrea Bolzicco, Vincenzo Cerullo, Josephine K. Dermawan, Anna Maria Frezza, Antoine Italiano, Jia Xiang Jin, Francois Le Loarer, Javier Martin-Broto, Andrew Pecora, Antonio Perez-Martinez, Yuen Bun Tam, Franck Tirode, Annalisa Trama, Sandro Pasquali, Mariagrazia Vescia, Lukas Wortmann, Michael Wortmann, Akihiko Yoshida, Kim Webb, Paul H. Huang, Charles Keller, and Cristina R. Antonescu. Translational aspects of epithelioid sarcoma - current consensus. Clinical cancer research : an official journal of the American Association for Cancer Research, 30:1079-1092, Nov 2024. URL: https://doi.org/10.1158/1078-0432.ccr-23-2174, doi:10.1158/1078-0432.ccr-23-2174. This article has 18 citations.
-
(grunewald2024translationalaspectsof pages 10-11): Thomas G.P. Grünewald, Sophie Postel-Vinay, Robert T. Nakayama, Noah E. Berlow, Andrea Bolzicco, Vincenzo Cerullo, Josephine K. Dermawan, Anna Maria Frezza, Antoine Italiano, Jia Xiang Jin, Francois Le Loarer, Javier Martin-Broto, Andrew Pecora, Antonio Perez-Martinez, Yuen Bun Tam, Franck Tirode, Annalisa Trama, Sandro Pasquali, Mariagrazia Vescia, Lukas Wortmann, Michael Wortmann, Akihiko Yoshida, Kim Webb, Paul H. Huang, Charles Keller, and Cristina R. Antonescu. Translational aspects of epithelioid sarcoma - current consensus. Clinical cancer research : an official journal of the American Association for Cancer Research, 30:1079-1092, Nov 2024. URL: https://doi.org/10.1158/1078-0432.ccr-23-2174, doi:10.1158/1078-0432.ccr-23-2174. This article has 18 citations.
-
(czarnecka2020epithelioidsarcoma—fromgenetics media 68051618): Anna M. Czarnecka, Pawel Sobczuk, Michal Kostrzanowski, Mateusz Spalek, Marzanna Chojnacka, Anna Szumera-Cieckiewicz, and Piotr Rutkowski. Epithelioid sarcoma—from genetics to clinical practice. Cancers, 12:2112, Jul 2020. URL: https://doi.org/10.3390/cancers12082112, doi:10.3390/cancers12082112. This article has 70 citations.
-
(tan2023epithelioidsarcomaof pages 2-3): Yi Liang Tan, Wilson Ong, Jiong Hao Tan, Naresh Kumar, and James Thomas Patrick Decourcy Hallinan. Epithelioid sarcoma of the spine: a review of literature and case report. Journal of Clinical Medicine, 12:5632, Aug 2023. URL: https://doi.org/10.3390/jcm12175632, doi:10.3390/jcm12175632. This article has 5 citations.
-
(czarnecka2020epithelioidsarcoma—fromgenetics pages 8-10): Anna M. Czarnecka, Pawel Sobczuk, Michal Kostrzanowski, Mateusz Spalek, Marzanna Chojnacka, Anna Szumera-Cieckiewicz, and Piotr Rutkowski. Epithelioid sarcoma—from genetics to clinical practice. Cancers, 12:2112, Jul 2020. URL: https://doi.org/10.3390/cancers12082112, doi:10.3390/cancers12082112. This article has 70 citations.
-
(czarnecka2023epithelioidsarcoma pages 3-5): Anna M. Czarnecka. Epithelioid sarcoma. Nowotwory. Journal of Oncology, 73:154-161, Jun 2023. URL: https://doi.org/10.5603/njo.a2023.0021, doi:10.5603/njo.a2023.0021. This article has 4 citations.
-
(orleni2024pharmacologyandpharmacokinetics pages 1-3): Marco Orleni and Jan H. Beumer. Pharmacology and pharmacokinetics of tazemetostat. Cancer chemotherapy and pharmacology, 93:509-517, Mar 2024. URL: https://doi.org/10.1007/s00280-024-04658-4, doi:10.1007/s00280-024-04658-4. This article has 19 citations and is from a peer-reviewed journal.
-
(czarnecka2020epithelioidsarcoma—fromgenetics pages 10-11): Anna M. Czarnecka, Pawel Sobczuk, Michal Kostrzanowski, Mateusz Spalek, Marzanna Chojnacka, Anna Szumera-Cieckiewicz, and Piotr Rutkowski. Epithelioid sarcoma—from genetics to clinical practice. Cancers, 12:2112, Jul 2020. URL: https://doi.org/10.3390/cancers12082112, doi:10.3390/cancers12082112. This article has 70 citations.
-
(NCT05407441 chunk 1): Susan Chi, MD. Tazemetostat+Nivo/Ipi in INI1-Neg/SMARCA4-Def Tumors. Susan Chi, MD. 2023. ClinicalTrials.gov Identifier: NCT05407441
-
(NCT04204941 chunk 1): Tazemetostat in Combination With Doxorubicin as Frontline Therapy for Advanced Epithelioid Sarcoma. Epizyme, Inc.. 2019. ClinicalTrials.gov Identifier: NCT04204941
-
(grunewald2024translationalaspectsof pages 19-20): Thomas G.P. Grünewald, Sophie Postel-Vinay, Robert T. Nakayama, Noah E. Berlow, Andrea Bolzicco, Vincenzo Cerullo, Josephine K. Dermawan, Anna Maria Frezza, Antoine Italiano, Jia Xiang Jin, Francois Le Loarer, Javier Martin-Broto, Andrew Pecora, Antonio Perez-Martinez, Yuen Bun Tam, Franck Tirode, Annalisa Trama, Sandro Pasquali, Mariagrazia Vescia, Lukas Wortmann, Michael Wortmann, Akihiko Yoshida, Kim Webb, Paul H. Huang, Charles Keller, and Cristina R. Antonescu. Translational aspects of epithelioid sarcoma - current consensus. Clinical cancer research : an official journal of the American Association for Cancer Research, 30:1079-1092, Nov 2024. URL: https://doi.org/10.1158/1078-0432.ccr-23-2174, doi:10.1158/1078-0432.ccr-23-2174. This article has 18 citations.
-
(czarnecka2020epithelioidsarcoma—fromgenetics pages 1-3): Anna M. Czarnecka, Pawel Sobczuk, Michal Kostrzanowski, Mateusz Spalek, Marzanna Chojnacka, Anna Szumera-Cieckiewicz, and Piotr Rutkowski. Epithelioid sarcoma—from genetics to clinical practice. Cancers, 12:2112, Jul 2020. URL: https://doi.org/10.3390/cancers12082112, doi:10.3390/cancers12082112. This article has 70 citations.
-
(chi2023tazemetostatfortumors pages 1-2): Susan N Chi, Joanna S Yi, P Mickey Williams, Sinchita Roy-Chowdhuri, David R Patton, Brent D Coffey, Joel M Reid, Jin Piao, Lauren Saguilig, Todd A Alonzo, Stacey L Berg, Nilsa C Ramirez, Alok Jaju, Joyce C Mhlanga, Elizabeth Fox, Douglas S Hawkins, Margaret M Mooney, Naoko Takebe, James V Tricoli, Katherine A Janeway, Nita L Seibel, and D Williams Parsons. Tazemetostat for tumors harboring smarcb1/smarca4 or ezh2 alterations: results from nci-cog pediatric match apec1621c. Journal of the National Cancer Institute, 115:1355-1363, May 2023. URL: https://doi.org/10.1093/jnci/djad085, doi:10.1093/jnci/djad085. This article has 111 citations and is from a highest quality peer-reviewed journal.