Congenital Dyserythropoietic Anemia
Congenital dyserythropoietic anemia (CDA) is a heterogeneous group of inherited disorders of late erythropoiesis characterized by ineffective erythropoiesis, distinctive morphological abnormalities of bone-marrow erythroid precursors (including bi- and multinucleated erythroblasts), and a variable hemolytic component. Anemia ranges from mild to transfusion dependent, and secondary iron overload develops even in non-transfused patients through erythroferrone-mediated suppression of hepcidin. The major subtypes are defined by causal gene and marrow morphology: CDA I (CDAN1, CDIN1/C15orf41), CDA II (SEC23B, the most common type), CDA III (KIF23), and the transcription-factor-related forms (GATA1, KLF1).
Ask OpenScientist
Ask a research question about Congenital Dyserythropoietic Anemia. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Inheritance
3Show evidence (1 reference)
Subtypes
4Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Pathophysiology
5Show evidence (2 references)
Show evidence (2 references)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (3 references)
Pathograph
Phenotypes
17Blood 5
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Cardiovascular 1
Show evidence (1 reference)
Digestive 3
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Metabolism 2
Show evidence (1 reference)
Show evidence (1 reference)
Growth 1
Show evidence (1 reference)
Other 5
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Genetic Associations
6Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (1 reference)
Medical Actions
6Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Show evidence (1 reference)
Clinical Trials
1Show evidence (1 reference)
Source YAML
click to showname: Congenital Dyserythropoietic Anemia
creation_date: "2026-06-05T12:00:00Z"
category: Mendelian
description: >-
Congenital dyserythropoietic anemia (CDA) is a heterogeneous group of
inherited disorders of late erythropoiesis characterized by ineffective
erythropoiesis, distinctive morphological abnormalities of bone-marrow
erythroid precursors (including bi- and multinucleated erythroblasts), and
a variable hemolytic component. Anemia ranges from mild to transfusion
dependent, and secondary iron overload develops even in non-transfused
patients through erythroferrone-mediated suppression of hepcidin. The major
subtypes are defined by causal gene and marrow morphology: CDA I (CDAN1,
CDIN1/C15orf41), CDA II (SEC23B, the most common type), CDA III (KIF23),
and the transcription-factor-related forms (GATA1, KLF1).
disease_term:
preferred_term: Congenital Dyserythropoietic Anemia
term:
id: MONDO:0019403
label: congenital dyserythropoietic anemia
synonyms:
- CDA
- congenital dyshematopoietic anemia
- anemia, congenital dyserythropoietic
references:
- reference: PMID:20301759
title: "Congenital Dyserythropoietic Anemia Type I."
tags:
- GeneReviews
has_subtypes:
- name: CDA I
display_name: CDA Type I (CDAN1 / CDIN1)
description: >-
Autosomal recessive CDA caused by biallelic variants in CDAN1 (codanin-1)
or CDIN1 (formerly C15orf41). Characterized by moderate-to-severe
macrocytic anemia with pathognomonic "spongy" (Swiss-cheese)
heterochromatin and internuclear chromatin bridges in erythroblasts.
Interferon-alpha can reduce transfusion requirements.
subtype_term:
preferred_term: congenital dyserythropoietic anemia type I
term:
id: MONDO:0020337
label: congenital dyserythropoietic anemia type 1
genes:
- preferred_term: CDAN1
term:
id: hgnc:1713
label: CDAN1
- preferred_term: CDIN1
term:
id: hgnc:26929
label: CDIN1
inheritance:
- name: Autosomal recessive inheritance
inheritance_term:
preferred_term: Autosomal recessive inheritance
term:
id: HP:0000007
label: Autosomal recessive inheritance
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Congenital dyserythropoietic anemia type I (CDA I) is characterized by moderate-to-severe macrocytic anemia presenting occasionally in utero as severe anemia associated with hydrops fetalis but more commonly in neonates as hepatomegaly, early jaundice, and intrauterine growth restriction."
explanation: GeneReviews defines CDA I as a distinct macrocytic-anemia subtype.
- reference: PMID:34234691
reference_title: "Cdan1 Is Essential for Primitive Erythropoiesis."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "Congenital dyserythropoietic anemia type I (CDA I) is an autosomal recessive disease characterized by moderate to severe macrocytic anemia and pathognomonic morphologic abnormalities of the erythroid precursors, including spongy heterochromatin."
explanation: Defines CDA I morphology and inheritance, supporting it as a subtype.
- name: CDA II
display_name: CDA Type II (SEC23B)
description: >-
The most common major CDA type. Autosomal recessive disorder caused by
biallelic SEC23B variants affecting COPII-dependent endoplasmic-reticulum-
to-Golgi vesicular trafficking, producing mild-to-severe normocytic
anemia, hemolysis, jaundice, and splenomegaly with band-3
hypoglycosylation and bi/multinucleated mature erythroblasts on marrow
examination.
subtype_term:
preferred_term: congenital dyserythropoietic anemia type II
term:
id: MONDO:0009134
label: congenital dyserythropoietic anemia type 2
genes:
- preferred_term: SEC23B
term:
id: hgnc:10702
label: SEC23B
inheritance:
- name: Autosomal recessive inheritance
inheritance_term:
preferred_term: Autosomal recessive inheritance
term:
id: HP:0000007
label: Autosomal recessive inheritance
evidence:
- reference: PMID:37373084
reference_title: "New Cases and Mutations in SEC23B Gene Causing Congenital Dyserythropoietic Anemia Type II."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Congenital dyserythropoietic anemia type II (CDA II) is an inherited autosomal recessive blood disorder which belongs to the wide group of ineffective erythropoiesis conditions. It is characterized by mild to severe normocytic anemia, jaundice, and splenomegaly owing to the hemolytic component."
explanation: Defines CDA II as the autosomal recessive SEC23B subtype and its hallmark features.
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "This mini-review illustrates the challenges involved in the diagnosis and management of the most common CDA, which is type II."
explanation: Establishes CDA II as the most common CDA subtype.
- name: CDA III
display_name: CDA Type III (KIF23)
description: >-
Rare CDA subtype characterized by giant multinucleated erythroblasts in
the bone marrow. Associated with variants in KIF23, which encodes a
kinesin-family motor protein (mitotic kinesin-like protein 1, MKLP1)
required for cytokinesis; impaired cytokinesis underlies the
multinuclearity of erythroid precursors.
subtype_term:
preferred_term: congenital dyserythropoietic anemia type III
term:
id: MONDO:0007109
label: congenital dyserythropoietic anemia type 3
genes:
- preferred_term: KIF23
term:
id: hgnc:6392
label: KIF23
inheritance:
- name: Autosomal dominant inheritance
inheritance_term:
preferred_term: Autosomal dominant inheritance
term:
id: HP:0000006
label: Autosomal dominant inheritance
evidence:
- reference: PMID:32702750
reference_title: "Congenital dyserythropoietic anemias."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "CDAs are classified into the 3 major types (I, II, III), plus the transcription factor-related CDAs, and the CDA variants, on the basis of the distinctive morphological, clinical, and genetic features."
explanation: Establishes CDA III as one of the three major morphology-defined CDA types.
- name: CDA transcription-factor-related
display_name: Transcription-factor-related CDA (GATA1, KLF1)
description: >-
Transcription-factor-related CDA forms caused by variants in the erythroid
master regulators GATA1 (X-linked) and KLF1. These produce dyserythropoiesis
as part of a broader phenotype; GATA1-related disease often combines
dyserythropoietic anemia with thrombocytopenia, and KLF1 underlies CDA IV.
genes:
- preferred_term: GATA1
term:
id: hgnc:4170
label: GATA1
- preferred_term: KLF1
term:
id: hgnc:6345
label: KLF1
evidence:
- reference: PMID:32702750
reference_title: "Congenital dyserythropoietic anemias."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "CDAs are classified into the 3 major types (I, II, III), plus the transcription factor-related CDAs, and the CDA variants, on the basis of the distinctive morphological, clinical, and genetic features."
explanation: Establishes the transcription-factor-related CDAs (including GATA1/KLF1) as a recognized class within the CDA classification.
inheritance:
- name: Autosomal recessive inheritance
inheritance_term:
preferred_term: Autosomal recessive inheritance
term:
id: HP:0000007
label: Autosomal recessive inheritance
description: >-
CDA I and CDA II are inherited in an autosomal recessive manner. The
transcription-factor form due to GATA1 is X-linked, and CDA III is often
autosomal dominant or sporadic.
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "CDA I is inherited in an autosomal recessive manner."
explanation: GeneReviews documents autosomal recessive inheritance for CDA I; CDA II is similarly autosomal recessive.
- name: Autosomal dominant inheritance
inheritance_term:
preferred_term: Autosomal dominant inheritance
term:
id: HP:0000006
label: Autosomal dominant inheritance
description: >-
CDA III (KIF23) is inherited in an autosomal dominant manner, as
described in the original Swedish family (KIF23 p.P916R). KLF1-related
CDA IV is also autosomal dominant (dominant-negative E325K).
- name: X-linked inheritance
inheritance_term:
preferred_term: X-linked inheritance
term:
id: HP:0001417
label: X-linked inheritance
description: >-
The transcription-factor-related CDA caused by GATA1 variants is X-linked.
pathophysiology:
- name: Ineffective erythropoiesis
description: >-
The unifying mechanism of all CDA subtypes is ineffective erythropoiesis:
erythropoietin-driven expansion of erythroid precursors with apoptosis and
maturation arrest of late-stage erythroblasts, so that the bone marrow
shows erythroid hyperplasia and dyserythropoiesis while the peripheral
reticulocyte response is inadequate for the degree of anemia. Subtype-
specific molecular lesions (CDAN1/CDIN1 chromatin and nucleolar defects,
SEC23B COPII trafficking defects, KIF23 cytokinesis defects) all converge
on failed terminal erythroid maturation.
cell_types:
- preferred_term: erythroblast
term:
id: CL:0000765
label: erythroblast
- preferred_term: erythroid lineage cell
term:
id: CL:0000764
label: erythroid lineage cell
biological_processes:
- preferred_term: erythrocyte differentiation
term:
id: GO:0030218
label: erythrocyte differentiation
modifier: DECREASED
- preferred_term: erythrocyte maturation
term:
id: GO:0043249
label: erythrocyte maturation
modifier: DECREASED
- preferred_term: apoptotic process
term:
id: GO:0006915
label: apoptotic process
modifier: INCREASED
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Congenital dyserythropoietic anemia (CDA) is characterized by anemia—mild to severe, hemolysis, ineffective erythropoiesis, and in some cases, iron overload."
explanation: Defines ineffective erythropoiesis as the central feature of CDA.
- reference: PMID:32702750
reference_title: "Congenital dyserythropoietic anemias."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Congenital dyserythropoietic anemias (CDAs) are a heterogeneous group of inherited anemias that affect the normal differentiation-proliferation pathways of the erythroid lineage. They belong to the wide group of ineffective erythropoiesis conditions that mainly result in monolinear cytopenia."
explanation: Establishes that CDAs perturb erythroid differentiation/proliferation and are ineffective erythropoiesis conditions.
downstream:
- target: Secondary iron overload
description: >-
Ineffective erythropoiesis drives erythroferrone overexpression, which
suppresses hepcidin and increases intestinal iron absorption.
evidence:
- reference: PMID:32702750
reference_title: "Congenital dyserythropoietic anemias."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The erythroblast-derived hormone erythroferrone specifically inhibits hepcidin production, and its role in the mediation of hepatic iron overload has been dissected out."
explanation: Links ineffective erythropoiesis to iron overload via the erythroferrone-hepcidin axis.
- target: Anemia
description: >-
Failed terminal erythroid maturation reduces effective red-cell output,
producing chronic anemia.
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Congenital dyserythropoietic anemia (CDA) is characterized by anemia—mild to severe, hemolysis, ineffective erythropoiesis, and in some cases, iron overload."
explanation: Links ineffective erythropoiesis to the resulting anemia.
- target: Macrocytic anemia
causal_link_type: DIRECT
- target: Hemolytic anemia
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- target: Abnormal erythroid morphology
causal_link_type: DIRECT
- target: Erythroid hyperplasia
causal_link_type: DIRECT
- target: Jaundice
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- target: Splenomegaly
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- target: Hepatomegaly
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- target: Cholelithiasis
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- target: Unconjugated hyperbilirubinemia
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- target: Hydrops fetalis
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- target: Extramedullary hematopoiesis
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- target: Failure to thrive
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- name: CDA I chromatin and nucleolar dysfunction
description: >-
In CDA I, biallelic CDAN1 (codanin-1) or CDIN1 variants disrupt erythroid
chromatin organization and nucleolar structure/function. Codanin-1
physically interacts with CDIN1, so CDAN1 and CDIN1 variants cause CDA I
through a common pathway. Affected erythroblasts show delayed terminal
differentiation, widespread changes in chromatin accessibility, increased
proliferation and apoptosis, and the pathognomonic "spongy"
heterochromatin seen on electron microscopy.
cell_types:
- preferred_term: erythroblast
term:
id: CL:0000765
label: erythroblast
biological_processes:
- preferred_term: chromatin organization
term:
id: GO:0006325
label: chromatin organization
modifier: ABNORMAL
evidence:
- reference: PMID:33121234
reference_title: "Recapitulation of erythropoiesis in congenital dyserythropoietic anaemia type I (CDA-I) identifies defects in differentiation and nucleolar abnormalities."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "erythroid cells in this condition show a delay during terminal erythroid differentiation, associated with increased proliferation and widespread changes in chromatin accessibility. We also show that the proteins encoded by CDAN1 and CDIN1 are enriched in nucleoli which are structurally and functionally abnormal in CDA-I."
explanation: Demonstrates the chromatin-accessibility and nucleolar abnormalities underlying CDA I in a patient-derived culture system.
- reference: PMID:35441598
reference_title: "The congenital dyserythropoieitic anemias: genetics and pathophysiology."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Codanin-1 was found to physically interact with CDIN1, suggesting that mutations in CDAN1 and CDIN1 result in CDAI via a common mechanism."
explanation: Supports a shared CDAN1/CDIN1 mechanism for CDA I.
downstream:
- target: Ineffective erythropoiesis
description: >-
Chromatin and nucleolar dysfunction blocks terminal erythroid
maturation, feeding into ineffective erythropoiesis.
- target: Distal limb anomalies
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- name: CDA II COPII trafficking and hypoglycosylation defect
description: >-
In CDA II, biallelic SEC23B variants impair the COPII coat component
required for endoplasmic-reticulum-to-Golgi vesicular transport. Disrupted
secretory trafficking alters glycosylation of erythrocyte membrane
proteins (e.g., band 3 hypoglycosylation), and patient erythroblasts show
an additional membrane of residual endoplasmic reticulum beneath the
plasma membrane. Patient-derived cells show reduced SEC23B protein without
compensatory SEC23A upregulation, consistent with a loss-of-function
mechanism.
cell_types:
- preferred_term: erythroblast
term:
id: CL:0000765
label: erythroblast
biological_processes:
- preferred_term: endoplasmic reticulum to Golgi vesicle-mediated transport
term:
id: GO:0006888
label: endoplasmic reticulum to Golgi vesicle-mediated transport
modifier: DECREASED
cellular_components:
- preferred_term: COPII vesicle coat
term:
id: GO:0030134
label: COPII-coated ER to Golgi transport vesicle
evidence:
- reference: PMID:37373084
reference_title: "New Cases and Mutations in SEC23B Gene Causing Congenital Dyserythropoietic Anemia Type II."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "Analysis of SEC23B protein levels done in patient-derived lymphoblastoid cell lines (LCLs) showed a significant decrease in SEC23B protein expression, in the absence of SEC23A compensation."
explanation: Supports loss of SEC23B protein function as the CDA II molecular lesion.
- reference: PMID:37455305
reference_title: "Development of High-Resolution Melting Curve Analysis for rapid detection of SEC23B gene mutation causing Congenital Dyserythropoietic Anemia type II in Indian population."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "CDA II is caused by mutations in the SEC23B gene. The most common mutation reported in India is c.1385 A > G, p.Y462C."
explanation: Identifies SEC23B as the CDA II gene and documents a recurrent founder variant.
downstream:
- target: Ineffective erythropoiesis
description: >-
COPII trafficking/glycosylation failure impairs erythroblast maturation,
contributing to ineffective erythropoiesis.
- name: CDA III impaired erythroblast cytokinesis
description: >-
CDA III is associated with KIF23, encoding mitotic kinesin-like protein 1
(MKLP1), a motor protein essential for cytokinesis. Defective cytokinesis
prevents complete division of maturing erythroblasts, producing the
characteristic giant multinucleated erythroblasts of CDA III and
contributing to ineffective erythropoiesis.
cell_types:
- preferred_term: erythroblast
term:
id: CL:0000765
label: erythroblast
biological_processes:
- preferred_term: cytokinesis
term:
id: GO:0000910
label: cytokinesis
modifier: ABNORMAL
evidence:
- reference: PMID:32702750
reference_title: "Congenital dyserythropoietic anemias."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "CDAs are classified into the 3 major types (I, II, III), plus the transcription factor-related CDAs, and the CDA variants, on the basis of the distinctive morphological, clinical, and genetic features."
explanation: Supports CDA III as a distinct morphology/genetic CDA type; KIF23/cytokinesis mechanistic detail is from the disease classification literature and gene function.
downstream:
- target: Ineffective erythropoiesis
causal_link_type: INDIRECT_UNKNOWN_INTERMEDIATES
- target: Multinucleated erythroblasts
causal_link_type: DIRECT
- name: Secondary iron overload
description: >-
Ineffective erythropoiesis stimulates erythroblast-derived erythroferrone,
which inhibits hepcidin. Reduced hepcidin increases intestinal iron
absorption, producing progressive hepatic and systemic iron overload
(secondary hemochromatosis) even in patients who are not transfused.
biological_processes:
- preferred_term: intracellular iron ion homeostasis
term:
id: GO:0006879
label: intracellular iron ion homeostasis
modifier: ABNORMAL
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "complete iron panel (serum iron, ferritin, and iron saturation), which may suggest iron overload."
explanation: Documents iron overload as a clinical feature of CDA requiring iron-panel monitoring.
- reference: PMID:32702750
reference_title: "Congenital dyserythropoietic anemias."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The erythroblast-derived hormone erythroferrone specifically inhibits hepcidin production, and its role in the mediation of hepatic iron overload has been dissected out."
explanation: Establishes the erythroferrone-hepcidin axis driving hepatic iron overload in CDA.
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Secondary hemochromatosis develops with age as a result of increased iron absorption even in those who are not transfused."
explanation: Documents non-transfusional iron overload from increased absorption in CDA I.
downstream:
- target: Iron overload
causal_link_type: DIRECT
- target: Elevated hepatic iron concentration
causal_link_type: DIRECT
phenotypes:
- name: Anemia
description: Chronic anemia ranging from mild to transfusion dependent.
phenotype_term:
preferred_term: Anemia
term:
id: HP:0001903
label: Anemia
temporality: CHRONIC
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Congenital dyserythropoietic anemia (CDA) is characterized by anemia—mild to severe, hemolysis, ineffective erythropoiesis, and in some cases, iron overload."
explanation: Documents anemia as a defining feature of CDA.
- name: Macrocytic anemia
description: CDA I characteristically presents with moderate-to-severe macrocytic anemia.
subtype: CDA I
phenotype_term:
preferred_term: Macrocytic anemia
term:
id: HP:0001972
label: Macrocytic anemia
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Congenital dyserythropoietic anemia type I (CDA I) is characterized by moderate-to-severe macrocytic anemia"
explanation: GeneReviews documents macrocytic anemia in CDA I.
- name: Hemolytic anemia
description: Hemolysis with jaundice contributes to the anemia, especially in CDA II.
subtype: CDA II
phenotype_term:
preferred_term: Hemolytic anemia
term:
id: HP:0001878
label: Hemolytic anemia
evidence:
- reference: PMID:37373084
reference_title: "New Cases and Mutations in SEC23B Gene Causing Congenital Dyserythropoietic Anemia Type II."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "It is characterized by mild to severe normocytic anemia, jaundice, and splenomegaly owing to the hemolytic component."
explanation: Documents the hemolytic component of CDA II.
- name: Multinucleated erythroblasts
description: >-
Bi- and multinucleated mature erythroblasts in the bone marrow are a
morphologic hallmark of CDA; CDA II marrow characteristically shows >10%
bi/multinucleated mature erythroblasts and CDA III shows giant
multinucleated forms.
category: Cellular
phenotype_term:
preferred_term: Multinucleated erythroblast
term:
id: HP:0034278
label: Multinucleated erythroblast
evidence:
- reference: PMID:38765414
reference_title: "Congenital Dyserythropoietic Anemia Type II With Myelofibrosis in an Adult Patient."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The bone marrow examination showed hyperplasia in the erythroid series with dyserythropoiesis"
explanation: Documents dyserythropoietic erythroid morphology on marrow examination in CDA II.
- reference: PMID:38090446
reference_title: "Congenital Dyserythropoietic Anemia Type I: A Rare Case Report."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "These disorders are characterized by anemia, primarily caused by inefficient erythropoiesis, as well as distinctive morphological abnormalities observed in most erythroblasts in the bone marrow."
explanation: Documents distinctive erythroblast morphological abnormalities as a defining CDA feature.
- name: Abnormal erythroid morphology
description: Distinctive morphological abnormalities of bone-marrow erythroid precursors.
category: Cellular
phenotype_term:
preferred_term: Abnormal erythroid lineage cell morphology
term:
id: HP:0012130
label: Abnormal erythroid lineage cell morphology
evidence:
- reference: PMID:34234691
reference_title: "Cdan1 Is Essential for Primitive Erythropoiesis."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "pathognomonic morphologic abnormalities of the erythroid precursors, including spongy heterochromatin."
explanation: Documents pathognomonic erythroid precursor morphologic abnormalities in CDA I.
- name: Erythroid hyperplasia
description: Bone marrow shows erythroid hyperplasia with dyserythropoiesis.
category: Cellular
phenotype_term:
preferred_term: Erythroid hyperplasia
term:
id: HP:0012132
label: Erythroid hyperplasia
evidence:
- reference: PMID:38765414
reference_title: "Congenital Dyserythropoietic Anemia Type II With Myelofibrosis in an Adult Patient."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "The bone marrow examination showed hyperplasia in the erythroid series with dyserythropoiesis"
explanation: Documents erythroid hyperplasia with dyserythropoiesis in a CDA II patient.
- name: Jaundice
description: Jaundice from unconjugated hyperbilirubinemia accompanies the hemolytic component.
phenotype_term:
preferred_term: Jaundice
term:
id: HP:0000952
label: Jaundice
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "most affected individuals have lifelong moderate anemia, usually accompanied by jaundice and splenomegaly."
explanation: GeneReviews documents jaundice in CDA I.
- name: Splenomegaly
description: Splenomegaly is a common complication across CDA subtypes.
phenotype_term:
preferred_term: Splenomegaly
term:
id: HP:0001744
label: Splenomegaly
evidence:
- reference: PMID:37373084
reference_title: "New Cases and Mutations in SEC23B Gene Causing Congenital Dyserythropoietic Anemia Type II."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "It is characterized by mild to severe normocytic anemia, jaundice, and splenomegaly owing to the hemolytic component."
explanation: Documents splenomegaly in CDA II.
- name: Hepatomegaly
description: Neonatal hepatomegaly is part of the CDA I presentation.
subtype: CDA I
phenotype_term:
preferred_term: Hepatomegaly
term:
id: HP:0002240
label: Hepatomegaly
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "more commonly in neonates as hepatomegaly, early jaundice, and intrauterine growth restriction."
explanation: GeneReviews documents neonatal hepatomegaly in CDA I.
- name: Iron overload
description: >-
Secondary iron overload / hemochromatosis develops from increased iron
absorption (erythroferrone-hepcidin axis) and transfusion, even in
non-transfused patients.
phenotype_term:
preferred_term: Increased circulating iron concentration
term:
id: HP:0003452
label: Increased circulating iron concentration
clinical_course: PROGRESSIVE
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Secondary hemochromatosis develops with age as a result of increased iron absorption even in those who are not transfused."
explanation: GeneReviews documents progressive secondary iron overload in CDA I.
- name: Elevated hepatic iron concentration
description: Iron loading of the liver, assessed by MRI, is a key monitoring target.
phenotype_term:
preferred_term: Elevated hepatic iron concentration
term:
id: HP:0012465
label: Elevated hepatic iron concentration
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Evaluation includes basic laboratory testing, magnetic resonance imaging of organs for assessment of iron overload, bone marrow assessment, and genetic testing."
explanation: Documents MRI assessment of organ (including hepatic) iron overload in CDA.
- name: Cholelithiasis
description: Gallstones are a frequent complication of the chronic hemolytic state.
phenotype_term:
preferred_term: Cholelithiasis
term:
id: HP:0001081
label: Cholelithiasis
evidence:
- reference: PMID:38765414
reference_title: "Congenital Dyserythropoietic Anemia Type II With Myelofibrosis in an Adult Patient."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Patients with CDA type II generally present with variable degrees of anemia along with pallor, icterus, splenomegaly, gallstones, and iron overload."
explanation: Documents gallstones as a typical CDA II complication.
- name: Unconjugated hyperbilirubinemia
description: Indirect (unconjugated) hyperbilirubinemia reflects the hemolytic component.
phenotype_term:
preferred_term: Unconjugated hyperbilirubinemia
term:
id: HP:0008282
label: Unconjugated hyperbilirubinemia
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "Laboratory tests to evaluate for ineffective erythropoiesis include indirect bilirubin level, which can be normal or increased"
explanation: Documents elevated indirect (unconjugated) bilirubin as a laboratory marker of ineffective erythropoiesis in CDA.
- name: Hydrops fetalis
description: Rare severe in-utero presentation of CDA I.
subtype: CDA I
frequency: VERY_RARE
phenotype_term:
preferred_term: Hydrops fetalis
term:
id: HP:0001789
label: Hydrops fetalis
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "presenting occasionally in utero as severe anemia associated with hydrops fetalis"
explanation: GeneReviews documents hydrops fetalis as a rare severe in-utero CDA I presentation.
- name: Distal limb anomalies
description: >-
Distal limb anomalies are a recognized minor feature of CDA I, occurring
in a minority of affected individuals.
subtype: CDA I
frequency: OCCASIONAL
phenotype_term:
preferred_term: Distal limb anomalies
term:
id: HP:0002813
label: Abnormal limb bone morphology
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Distal limb anomalies occur in 4%-14% of affected individuals."
explanation: GeneReviews documents distal limb anomalies in 4-14% of CDA I patients, supporting an OCCASIONAL frequency band.
- name: Extramedullary hematopoiesis
description: >-
Extramedullary hematopoiesis is a complication of CDA requiring directed
management (transfusion, surgical debulking, or low-dose radiation).
phenotype_term:
preferred_term: Extramedullary hematopoiesis
term:
id: HP:0001978
label: Extramedullary hematopoiesis
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "treatment of extramedullary hematopoiesis"
explanation: GeneReviews lists treatment of extramedullary hematopoiesis among CDA I management measures, documenting it as a recognized complication.
- name: Failure to thrive
description: Infantile presentation may include failure to thrive.
subtype: CDA I
phenotype_term:
preferred_term: Failure to thrive
term:
id: HP:0001508
label: Failure to thrive
evidence:
- reference: PMID:38090446
reference_title: "Congenital Dyserythropoietic Anemia Type I: A Rare Case Report."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "A male infant, aged four months, who had signs of vomiting, weight loss, and failure to thrive, was diagnosed with CDA-I"
explanation: Case report documents failure to thrive at CDA I presentation.
genetic:
- name: CDAN1
gene_term:
preferred_term: CDAN1
term:
id: hgnc:1713
label: CDAN1
association: Causal
subtype: CDA I
inheritance:
- name: Autosomal recessive inheritance
inheritance_term:
preferred_term: Autosomal recessive inheritance
term:
id: HP:0000007
label: Autosomal recessive inheritance
notes: >-
CDAN1 encodes codanin-1 and is the main CDA I gene. Codanin-1 physically
interacts with CDIN1.
evidence:
- reference: PMID:34234691
reference_title: "Cdan1 Is Essential for Primitive Erythropoiesis."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "The disease is mainly caused by mutations in CDAN1 (encoding for Codanin-1)."
explanation: Identifies CDAN1 as the principal CDA I gene.
- name: CDIN1
gene_term:
preferred_term: CDIN1
term:
id: hgnc:26929
label: CDIN1
association: Causal
subtype: CDA I
inheritance:
- name: Autosomal recessive inheritance
inheritance_term:
preferred_term: Autosomal recessive inheritance
term:
id: HP:0000007
label: Autosomal recessive inheritance
notes: >-
CDIN1 (formerly C15orf41) is a second CDA I gene; CDAN1 and CDIN1 cause
CDA I via a shared mechanism.
evidence:
- reference: PMID:33121234
reference_title: "Recapitulation of erythropoiesis in congenital dyserythropoietic anaemia type I (CDA-I) identifies defects in differentiation and nucleolar abnormalities."
supports: SUPPORT
evidence_source: IN_VITRO
snippet: "Congenital Dyserythropoietic Anaemia type 1 (CDA-I) is a rare form of anaemia caused by mutations in two genes of unknown function: CDAN1 and CDIN1 (previously called C15orf41)"
explanation: Identifies CDIN1 (C15orf41) as a CDA I gene alongside CDAN1.
- name: SEC23B
gene_term:
preferred_term: SEC23B
term:
id: hgnc:10702
label: SEC23B
association: Causal
subtype: CDA II
inheritance:
- name: Autosomal recessive inheritance
inheritance_term:
preferred_term: Autosomal recessive inheritance
term:
id: HP:0000007
label: Autosomal recessive inheritance
notes: >-
SEC23B encodes a COPII coat component; biallelic loss-of-function variants
cause CDA II. A recurrent Indian founder variant is c.1385A>G (p.Y462C).
evidence:
- reference: PMID:37373084
reference_title: "New Cases and Mutations in SEC23B Gene Causing Congenital Dyserythropoietic Anemia Type II."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "CDA II is caused by biallelic mutations in the SEC23B gene. In this study, we report 9 new CDA II cases and identify 16 pathogenic variants, 6 of which are novel."
explanation: Identifies SEC23B as the causative CDA II gene and documents pathogenic variants.
- name: KIF23
gene_term:
preferred_term: KIF23
term:
id: hgnc:6392
label: KIF23
association: Causal
subtype: CDA III
inheritance:
- name: Autosomal dominant inheritance
inheritance_term:
preferred_term: Autosomal dominant inheritance
term:
id: HP:0000006
label: Autosomal dominant inheritance
notes: >-
KIF23 encodes mitotic kinesin-like protein 1 (MKLP1), required for
cytokinesis; it is associated with CDA III and its giant multinucleated
erythroblasts. CDA III is inherited in an autosomal dominant manner (the
original Swedish family, KIF23 p.P916R).
evidence:
- reference: PMID:32702750
reference_title: "Congenital dyserythropoietic anemias."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "CDAs are classified into the 3 major types (I, II, III), plus the transcription factor-related CDAs, and the CDA variants"
explanation: Supports CDA III as a recognized type; KIF23 is its established gene from the CDA classification literature.
- name: GATA1
gene_term:
preferred_term: GATA1
term:
id: hgnc:4170
label: GATA1
association: Causal
subtype: CDA transcription-factor-related
inheritance:
- name: X-linked inheritance
inheritance_term:
preferred_term: X-linked inheritance
term:
id: HP:0001417
label: X-linked inheritance
notes: >-
GATA1 is an X-linked erythroid transcription factor; variants cause a
transcription-factor-related CDA, often with thrombocytopenia.
evidence:
- reference: PMID:32702750
reference_title: "Congenital dyserythropoietic anemias."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "plus the transcription factor-related CDAs, and the CDA variants, on the basis of the distinctive morphological, clinical, and genetic features."
explanation: Supports the transcription-factor-related CDA class to which GATA1 belongs.
- name: KLF1
gene_term:
preferred_term: KLF1
term:
id: hgnc:6345
label: KLF1
association: Causal
subtype: CDA transcription-factor-related
inheritance:
- name: Autosomal dominant inheritance
inheritance_term:
preferred_term: Autosomal dominant inheritance
term:
id: HP:0000006
label: Autosomal dominant inheritance
notes: >-
KLF1 is an erythroid Krüppel-like transcription factor; variants cause a
transcription-factor-related CDA (CDA IV), inherited in an autosomal
dominant manner via the dominant-negative E325K variant.
evidence:
- reference: PMID:32702750
reference_title: "Congenital dyserythropoietic anemias."
supports: PARTIAL
evidence_source: HUMAN_CLINICAL
snippet: "plus the transcription factor-related CDAs, and the CDA variants, on the basis of the distinctive morphological, clinical, and genetic features."
explanation: Supports the transcription-factor-related CDA class to which KLF1 belongs.
treatments:
- name: Red blood cell transfusion
description: >-
Blood transfusion supports patients with severe anemia; some patients are
transfusion dependent.
treatment_term:
preferred_term: blood transfusion
term:
id: MAXO:0000756
label: blood transfusion
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "some severe cases may require blood transfusion, iron chelation therapy, splenectomy, and in extreme cases, hematopoietic stem cell transplant may be necessary."
explanation: Documents transfusion as a management option for severe CDA.
- name: Iron chelation therapy
description: >-
Iron chelation (e.g., deferasirox) treats secondary iron overload from
increased absorption and transfusion. GeneReviews advises avoiding
iron-containing preparations.
treatment_term:
preferred_term: pharmacotherapy
term:
id: MAXO:0000058
label: pharmacotherapy
therapeutic_agent:
- preferred_term: deferasirox
term:
id: CHEBI:49005
label: deferasirox
target_mechanisms:
- target: Secondary iron overload
description: Iron chelation removes excess iron accumulated from increased absorption and transfusion.
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "some severe cases may require blood transfusion, iron chelation therapy, splenectomy, and in extreme cases, hematopoietic stem cell transplant may be necessary."
explanation: Documents iron chelation therapy as a CDA management option.
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Agents/circumstances to avoid: Any preparation containing iron."
explanation: GeneReviews drug-safety warning to avoid iron-containing preparations in CDA I.
- name: Splenectomy
description: Splenectomy may be used in selected patients with hemolysis/hypersplenism.
treatment_term:
preferred_term: splenectomy
term:
id: MAXO:0001077
label: splenectomy
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "some severe cases may require blood transfusion, iron chelation therapy, splenectomy, and in extreme cases, hematopoietic stem cell transplant may be necessary."
explanation: Documents splenectomy as a CDA management option.
- name: Hematopoietic stem cell transplantation
description: >-
Allogeneic HSCT is a potentially curative option reserved for severe,
transfusion-dependent disease (e.g., interferon-resistant CDA I).
treatment_term:
preferred_term: hematopoietic stem cell transplantation
term:
id: MAXO:0000747
label: hematopoietic stem cell transplantation
evidence:
- reference: DOI:10.3389/frhem.2024.1389820
reference_title: "Congenital dyserythropoietic anemia type II and ineffective erythropoiesis: challenges in diagnosis and management."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "in extreme cases, hematopoietic stem cell transplant may be necessary."
explanation: Documents HSCT as a treatment for the most severe CDA cases.
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Allogeneic bone marrow transplantation should be considered only in transfusion-dependent persons who are resistant to IFN therapy."
explanation: GeneReviews reserves HSCT for transfusion-dependent, interferon-resistant CDA I.
- name: Interferon-alpha therapy
description: >-
In CDA I, interferon-alpha (IFN-alpha2a/2b or peginterferon-alpha2b)
increases hemoglobin and decreases iron overload, reducing transfusion
dependence.
treatment_term:
preferred_term: pharmacotherapy
term:
id: MAXO:0000058
label: pharmacotherapy
therapeutic_agent:
- preferred_term: recombinant interferon alfa
term:
id: NCIT:C225
label: Recombinant Interferon Alfa
target_mechanisms:
- target: Secondary iron overload
description: Interferon-alpha decreases iron overload in CDA I.
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Intramuscular or subcutaneous injections of interferon IFN-α2a or IFN-α2b are given two or three times a week or peginterferon-α2b once a week to increase hemoglobin and decrease iron overload."
explanation: GeneReviews documents interferon-alpha as CDA I treatment that raises hemoglobin and reduces iron overload.
- name: Genetic counseling
description: >-
Genetic counseling supports families; once familial pathogenic variants
are identified, carrier testing and prenatal/preimplantation testing are
possible.
treatment_term:
preferred_term: Genetic Counseling
term:
id: NCIT:C15240
label: Genetic Counseling
evidence:
- reference: PMID:20301759
reference_title: "Congenital Dyserythropoietic Anemia Type I."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: "Once the pathogenic variants have been identified in an affected family member, carrier testing for at-risk relatives and prenatal and preimplantation genetic testing are possible."
explanation: GeneReviews supports genetic counseling and family-based testing in CDA.
animal_models:
- species: Mus musculus
genotype: Erythroid-specific Cdan1 deletion (CdanΔEry)
description: >-
Erythroid-specific deletion of Cdan1 (using ErGFPcre) causes mid-gestation
embryonic lethality from severe anemia and recapitulates the pathognomonic
spongy heterochromatin and increased erythroblast apoptosis of CDA I.
evidence:
- reference: PMID:34234691
reference_title: "Cdan1 Is Essential for Primitive Erythropoiesis."
supports: SUPPORT
evidence_source: MODEL_ORGANISM
snippet: "The resulting CdanΔEry transgenic embryos died at mid-gestation (E12.5-E13.5) from severe anemia, with very low numbers of circulating erythroblast. Transmission electron microscopy studies of primitive erythroblasts (E9.5) revealed the pathognomonic spongy heterochromatin."
explanation: Mouse model recapitulates CDA I severe anemia and the pathognomonic spongy heterochromatin.
clinical_trials:
- name: NCT02964494
status: RECRUITING
description: >-
The Congenital Dyserythropoietic Anemia Registry (CDAR), a North American
registry collecting long-term natural history, complications, and treatment
effects.
evidence:
- reference: clinicaltrials:NCT02964494
reference_title: "The Congenital Dyserythropoietic Anemia Registry (CDAR)"
supports: SUPPORT
snippet: "The goal of this registry is to collect long-term confidential data on patients with CDA in the US, Canada, and Mexico"
explanation: Establishes the CDAR registry as an active CDA natural-history study.
References & Deep Research
References
1Deep Research
1Congenital Dyserythropoietic Anemia (CDA) — Comprehensive Disease Characteristics Report
Target disease
- Disease name: Congenital dyserythropoietic anemia (CDA)
- Category: Mendelian / inherited anemia
- MONDO ID: MONDO_0019403 (OpenTargets) (OpenTargets Search: congenital dyserythropoietic anemia)
1. Disease information
1.1 Concise overview / definition
Congenital dyserythropoietic anemias are inherited disorders of erythropoiesis characterized by ineffective erythropoiesis with distinctive morphologic abnormalities of erythroid precursors and variable hemolysis and iron overload. A recent CDA type II mini-review states: “Congenital dyserythropoietic anemia (CDA) is characterized by anemia—mild to severe, hemolysis, ineffective erythropoiesis, and in some cases, iron overload.” (published 2024-07-05) (akpan2024congenitaldyserythropoieticanemia pages 1-2). A Blood review further frames CDAs as “a heterogeneous group of inherited anemias” affecting erythroid differentiation–proliferation and classified by morphology/clinical/genetic features (published 2020-07, URL below) (iolascon2020congenitaldyserythropoieticanemias. pages 1-1).
1.2 Key identifiers (with availability notes)
- MONDO: MONDO_0019403 (OpenTargets) (OpenTargets Search: congenital dyserythropoietic anemia)
- MeSH term (ClinicalTrials.gov condition browse): Anemia, Dyserythropoietic, Congenital (MeSH tree includes genetic/congenital anemia terms) (NCT03983629 chunk 1)
- OMIM (examples explicitly present in retrieved sources):
- CDA II: OMIM 224100 (saptarshi2023developmentofhighresolution pages 1-2, musri2023newcasesand pages 1-2)
- SEC23B: OMIM 610512 (saptarshi2023developmentofhighresolution pages 1-2)
- ICD-10 / ICD-11 / Orphanet: Not directly available in the retrieved source set; should be added from Orphanet/ICD resources in a follow-on curation step.
1.3 Common synonyms / alternative names
- “Congenital dyserythropoietic anemias (CDAs)” (plural group term) (iolascon2020congenitaldyserythropoieticanemias. pages 1-1)
- “CDA type I/II/III/IV”; “transcription factor–related CDA”; “X-linked thrombocytopenia with dyserythropoietic anemia (XLTDA)” (saptarshi2023developmentofhighresolution pages 1-2, musri2023newcasesand pages 1-2, iolascon2020congenitaldyserythropoieticanemias. pages 1-1)
1.4 Evidence provenance (patient-level vs aggregated)
The information summarized here derives from both: - Aggregated disease-level reviews and mechanistic synthesis (e.g., Blood review; Curr Opin Hematol review) (iolascon2020congenitaldyserythropoieticanemias. pages 1-1, king2022thecongenitaldyserythropoieitic pages 1-3) - Patient-series / molecular cohorts (e.g., 9-case SEC23B cohort; 11-case Indian diagnostic cohort) (musri2023newcasesand pages 1-2, saptarshi2023developmentofhighresolution pages 1-2) - Registries (real-world evidence infrastructure): North American CDA registry (CDAR) and French national registry initiative (ClinicalTrials.gov) (NCT02964494 chunk 1, NCT03983629 chunk 1)
Key recent sources prioritized (2023–2024): Akpan 2024 (Frontiers in Hematology), Musri 2023 (IJMS), Saptarshi 2023 (Italian J Pediatrics) (akpan2024congenitaldyserythropoieticanemia pages 1-2, musri2023newcasesand pages 1-2, saptarshi2023developmentofhighresolution pages 1-2).
2. Etiology
2.1 Primary causes
CDA is genetic (Mendelian) and caused by pathogenic variants in genes required for erythroblast maturation, vesicular trafficking/glycosylation, cytokinesis, or transcriptional control of erythropoiesis.
Examples in retrieved evidence: - CDA I: mutations in CDAN1 and CDIN1 (previously C15orf41) (scott2020recapitulationoferythropoiesis pages 1-2, king2022thecongenitaldyserythropoieitic pages 1-3) - CDA II: biallelic pathogenic variants in SEC23B (akpan2024congenitaldyserythropoieticanemia pages 1-2, musri2023newcasesand pages 1-2) - Additional/rare CDA genes are noted in disease–target association resources (OpenTargets) including KIF23, RACGAP1, GATA1, KLF1, LPIN2 (OpenTargets Search: congenital dyserythropoietic anemia).
2.2 Risk factors
- Family history / inherited genotype is the dominant risk factor.
- Population-specific recurrent variants: In India, a common SEC23B mutation is c.1385A>G (p.Y462C) (saptarshi2023developmentofhighresolution pages 1-2).
2.3 Protective factors
No specific genetic or environmental protective factors were identified in the retrieved sources.
2.4 Gene–environment interactions
No specific CDA gene–environment interaction studies were identified in the retrieved sources.
3. Phenotypes
3.1 Shared clinical/laboratory phenotype across CDAs
Across CDA subtypes, a consistent pattern is chronic anemia with hemolysis markers and suboptimal reticulocytosis for the severity of anemia (ineffective erythropoiesis). A review notes that CDA is characterized by elevated LDH/indirect bilirubin (hemolysis) while the reticulocyte count is “normal or suboptimally elevated” because of ineffective erythropoiesis (king2022thecongenitaldyserythropoieitic pages 1-3). The French registry summary similarly describes anemia that is “non-regenerative or inappropriate regarding anaemia” with “moderate unconjugated hyperbilirubinemia” and frequent splenomegaly/jaundice (NCT03983629 chunk 1).
Common complications: gallstones, splenomegaly/hypersplenism, and iron overload/hemochromatosis even without transfusions (akpan2024congenitaldyserythropoieticanemia pages 1-2, musri2023newcasesand pages 1-2, king2022thecongenitaldyserythropoieitic pages 1-3, NCT03983629 chunk 1).
3.2 CDA II phenotype (examples of 2023–2024 data)
- Akpan 2024 describes CDA II as autosomal recessive hemolytic disease due to SEC23B variants, and notes peripheral smear anisopoikilocytosis with basophilic stippling and rare binucleated mature erythroblasts, and hemolytic anemia with inadequate reticulocytosis (akpan2024congenitaldyserythropoieticanemia pages 1-2).
- Musri 2023 additionally lists complications such as “leg ulcers,” “aplastic crisis,” and “bulky extramedullary erythropoiesis,” and notes marrow with >10% bi/multinucleated erythroblasts, and an EM feature of an “additional membrane consisting of residual endoplasmic reticulum beneath the cytoplasmic membrane” (musri2023newcasesand pages 1-2).
- A severe adult case report (2024) illustrates the clinical range (Hb 3.7 g/dL; ferritin 1,880 ng/mL; transferrin saturation 96.08%) and emphasizes negative Coombs and the role of gene panels in delayed diagnosis (shemawat2024congenitaldyserythropoieticanemia pages 1-2).
3.3 CDA I phenotype (examples)
CDA I is described as an autosomal recessive disease with macrocytic anemia and a pathognomonic “spongy heterochromatin” in erythroblasts (noylotan2021cdan1isessential pages 1-2). In cultured patient erythroid cells, a Haematologica study states CDA-I is caused by mutations in CDAN1 and CDIN1, and reports defects including delayed terminal erythroid differentiation and nucleolar abnormalities (scott2020recapitulationoferythropoiesis pages 1-2).
3.4 Phenotype characteristics (onset, progression, severity)
- Typical onset: infancy/childhood; however delayed diagnoses into adulthood occur in milder disease (king2022thecongenitaldyserythropoieitic pages 1-3, NCT03983629 chunk 1, shemawat2024congenitaldyserythropoieticanemia pages 1-2).
- Severity: ranges from mild/asymptomatic to transfusion dependence and rare hydrops fetalis (king2022thecongenitaldyserythropoieitic pages 1-3, musri2023newcasesand pages 1-2).
- Progression: chronic disease; iron overload may be progressive and can occur without transfusion due to increased absorption (NCT03983629 chunk 1, king2022thecongenitaldyserythropoieitic pages 1-3).
3.5 Quality-of-life impact
No disease-specific QoL instrument results (e.g., SF-36, PROMIS, EQ-5D) were identified in the retrieved sources. Clinically, persistent anemia, transfusion dependence, iron overload management, and complications (splenomegaly, gallstones, extramedullary hematopoiesis) plausibly impair daily functioning; however, quantitative QoL data should be added from dedicated QoL studies not captured in this retrieval.
3.6 Suggested HPO terms (non-exhaustive)
(Ontology suggestions for knowledge base mapping; not all are explicitly labeled as HPO in the retrieved sources.) - HP:0001903 Anemia - HP:0001878 Hemolytic anemia - HP:0002188 Elevated indirect bilirubin / unconjugated hyperbilirubinemia - HP:0000980 Jaundice - HP:0001744 Splenomegaly - HP:0003270 Iron overload / hemochromatosis - HP:0003155 Elevated serum ferritin - HP:0002240 Hepatomegaly - HP:0001082 Abnormality of bone marrow morphology (dyserythropoiesis) - HP:0004396 Cholelithiasis / gallstones - HP:0001764 Aplastic crisis (CDA II complication reported) (musri2023newcasesand pages 1-2)
4. Genetic / molecular information
4.1 Causal genes and inheritance (core)
- CDA I: CDAN1 and CDIN1 (C15orf41); autosomal recessive (scott2020recapitulationoferythropoiesis pages 1-2, noylotan2021cdan1isessential pages 1-2, king2022thecongenitaldyserythropoieitic pages 1-3).
- CDA II: SEC23B; autosomal recessive; “biallelic” pathogenic variants (akpan2024congenitaldyserythropoieticanemia pages 1-2, musri2023newcasesand pages 1-2).
- CDA III and other genetic types: Multiple genes exist; OpenTargets lists disease–gene associations including KIF23, RACGAP1, GATA1, KLF1, among others (OpenTargets Search: congenital dyserythropoietic anemia). The French registry notes: “The transmission mode for Type I and II is autosomal recessive, while it is autosomal dominant or sporadic for Type III.” (NCT03983629 chunk 1).
4.2 Pathogenic variants (examples with HGVS nomenclature; 2023 priority)
SEC23B variants in a 9-case cohort (Musri 2023; published 2023-06-09): - The abstract states: “we report 9 new CDA II cases and identify 16 pathogenic variants, 6 of which are novel.” (musri2023newcasesand pages 1-2). - Novel variants reported include: p.Thr445Arg, p.Tyr579Cys, p.Arg701His, p.Asp693GlyfsTer2, c.1512-2A>G, and complex intronic c.1512-3delinsTT linked to c.1512-16_1512-7delACTCTGGAAT (musri2023newcasesand pages 1-2).
Indian recurrent variant and diagnostic screening (Saptarshi 2023; published 2023-07-07): - Abstract reports: “The most common mutation reported in India is c.1385 A>G, p.Y462C.” and describes 11 patients with homozygous p.Y462C, with heterozygous parents (saptarshi2023developmentofhighresolution pages 1-2).
4.3 Variant classes and functional consequences (SEC23B examples)
Musri 2023 reports computational and patient-derived cell evidence consistent with loss-of-function/protein deficiency: “Analysis of SEC23B protein levels done in patient-derived lymphoblastoid cell lines (LCLs) showed a significant decrease in SEC23B protein expression, in the absence of SEC23A compensation.” (musri2023newcasesand pages 1-2). RT-PCR/Sanger data showed aberrant splicing for complex intronic alleles (exon 13–14 skipping) (musri2023newcasesand pages 1-2).
4.4 Modifier genes / variants (iron overload severity)
A Blood review summarizes modifier concepts for iron overload in CDA II, including genetic modifiers such as HFE variants and an erythroferrone (ERFE) coding variant (p.A260S) associated with altered iron regulation (iolascon2020congenitaldyserythropoieticanemias. pages 12-13).
4.5 Epigenetic information
No CDA-specific epigenetic (methylation/histone modification) findings were identified in the retrieved sources.
4.6 Chromosomal abnormalities
No recurrent chromosomal abnormalities were identified in the retrieved sources.
5. Environmental information
CDA is primarily genetic. No specific environmental toxins, lifestyle factors, or infectious triggers were identified as causal in the retrieved sources.
6. Mechanism / pathophysiology
6.1 Unifying mechanism: ineffective erythropoiesis → anemia ± hemolysis
Akpan 2024 defines ineffective erythropoiesis as inadequate reticulocytosis in the presence of immature precursors, with an “erythropoietin-driven expansion of erythroid precursors and apoptosis of late-stage erythroid precursors” (akpan2024congenitaldyserythropoieticanemia pages 1-2). This links upstream erythroid maturation failure to downstream anemia/hemolysis phenotypes.
Suggested GO biological process terms (examples): - erythrocyte differentiation; erythrocyte maturation; regulation of erythropoiesis; apoptotic process
Suggested CL cell types: - erythroblast; late erythroid precursor; reticulocyte
6.2 Iron overload: ERFE–hepcidin axis (central downstream pathway)
Akpan 2024 states that ineffective erythropoiesis causes “overexpression of erythroferrone” that “suppresses hepcidin leading to increased iron absorption and progressive iron overload” (akpan2024congenitaldyserythropoieticanemia pages 1-2). The Blood review similarly highlights erythroferrone as an erythroblast-derived inhibitor of hepcidin in CDA II (iolascon2020congenitaldyserythropoieticanemias. pages 1-1).
Causal chain (simplified): Genetic subtype defect → ineffective erythropoiesis → ↑EPO drive/precursor expansion and apoptosis → ↑erythroferrone (ERFE) → ↓hepcidin → ↑intestinal iron absorption → hepatic/systemic iron overload (akpan2024congenitaldyserythropoieticanemia pages 1-2, iolascon2020congenitaldyserythropoieticanemias. pages 1-1).
6.3 CDA II mechanism: SEC23B / COPII trafficking and hypoglycosylation
- CDA II is caused by biallelic SEC23B variants affecting COPII-dependent trafficking (akpan2024congenitaldyserythropoieticanemia pages 1-2, musri2023newcasesand pages 1-2).
- The Indian diagnostic paper explains that SEC23B is a COPII component and that ER-to-Golgi trafficking disruption affects glycosylation pathways, accounting for CDA II cellular phenotype (saptarshi2023developmentofhighresolution pages 1-2).
- A case report describes defective glycosylation of red cell membrane proteins (band 3 and band 4.5) as part of CDA II pathogenesis (shemawat2024congenitaldyserythropoieticanemia pages 1-2).
Suggested GO cellular component terms (examples): - endoplasmic reticulum; Golgi apparatus; COPII-coated vesicle
6.4 CDA I mechanism: CDAN1/CDIN1 and erythroid nuclear/chromatin pathology
A CDA-I model paper states CDA I is “mainly caused by mutations in CDAN1” and demonstrates erythroid-lineage deletion causes severe embryonic anemia with the pathognomonic “spongy heterochromatin” and increased apoptotic erythroblasts (noylotan2021cdan1isessential pages 1-2). In human CDA-I erythroid culture, cells show delayed terminal differentiation and chromatin accessibility changes, with CDAN1/CDIN1 enrichment in abnormal nucleoli (scott2020recapitulationoferythropoiesis pages 1-2).
7. Anatomical structures affected
7.1 Organ-level
- Bone marrow (primary): erythroid hyperplasia with dyserythropoiesis (musri2023newcasesand pages 1-2, NCT03983629 chunk 1)
- Spleen: splenomegaly (extramedullary hematopoiesis / hypersplenism) (akpan2024congenitaldyserythropoieticanemia pages 1-2, NCT03983629 chunk 1)
- Liver: iron overload; secondary hemochromatosis (musri2023newcasesand pages 1-2, NCT03983629 chunk 1)
- Gallbladder: gallstones (musri2023newcasesand pages 1-2, NCT03983629 chunk 1)
Suggested UBERON terms (examples): bone marrow; spleen; liver; gallbladder
7.2 Tissue/cell level
- Erythroid lineage-restricted defect in most CDAs (king2022thecongenitaldyserythropoieitic pages 1-3)
- Cell type focus: erythroblasts / erythroid precursors (musri2023newcasesand pages 1-2, NCT03983629 chunk 1)
7.3 Subcellular level
- CDA II: ER-to-Golgi trafficking; residual ER beneath plasma membrane on EM (musri2023newcasesand pages 1-2, saptarshi2023developmentofhighresolution pages 1-2)
- CDA I: nuclear chromatin ultrastructure (“spongy heterochromatin”) (noylotan2021cdan1isessential pages 1-2, scott2020recapitulationoferythropoiesis pages 1-2)
8. Temporal development
8.1 Onset
Diagnosis is commonly made in childhood, but can be delayed for years; French registry summary explicitly notes heterogeneity can delay diagnosis (NCT03983629 chunk 1). A 30-year-old adult CDA II case demonstrates late diagnosis in practice (shemawat2024congenitaldyserythropoieticanemia pages 1-2).
8.2 Progression and course
Chronic course with variable anemia severity; progressive iron loading can occur even without transfusions due to increased absorption (NCT03983629 chunk 1, akpan2024congenitaldyserythropoieticanemia pages 1-2).
9. Inheritance and population
9.1 Epidemiology (statistics)
- A 2022 review provides estimated prevalence: CDA II ~0.71 cases/million and CDA I ~0.24 cases/million, with underdiagnosis suspected; it also cites a more recent estimate of CDA I incidence of 5 cases/million live births (king2022thecongenitaldyserythropoieitic pages 1-3).
- The French registry protocol summary reports international variation: “varies between countries from 0.08 million in Scandinavia to 2.6 cases/million inhabitants in Italy” (NCT03983629 chunk 1).
9.2 Inheritance patterns
- CDA I and II: autosomal recessive (noylotan2021cdan1isessential pages 1-2, akpan2024congenitaldyserythropoieticanemia pages 1-2, NCT03983629 chunk 1).
- CDA III: often autosomal dominant or sporadic (registry description) (NCT03983629 chunk 1).
9.3 Population distribution / founder effects
- India: SEC23B c.1385A>G (p.Y462C) highlighted as common; 11-patient cohort used for rapid screening assay development (saptarshi2023developmentofhighresolution pages 1-2).
- European/Mediterranean enrichment noted in a 2024 case report background (shemawat2024congenitaldyserythropoieticanemia pages 1-2).
10. Diagnostics
10.1 Core clinical tests and morphology
A 2024 mini-review states evaluation “includes basic laboratory testing… MRI… bone marrow assessment, and genetic testing” (akpan2024congenitaldyserythropoieticanemia pages 1-2). It also specifies labs useful for ineffective erythropoiesis evaluation (indirect bilirubin, reticulocyte production index <2, and iron panel) (akpan2024congenitaldyserythropoieticanemia pages 1-2).
Key morphologic criteria (examples): - CDA II marrow: “more than 10% of mature bi- or multi-nucleated erythroblasts” (musri2023newcasesand pages 1-2).
10.2 Specialized assays for CDA II vs membrane disorders
Saptarshi 2023 explains that CDA II has band 3 hypoglycosylation and can show decreased mean channel fluorescence on EMA testing (a pitfall with hereditary spherocytosis), and uses anti-CD44 antibody binding plus molecular confirmation (saptarshi2023developmentofhighresolution pages 1-2).
10.3 Genetic testing strategy and real-world implementations
- Akpan 2024: “Genetic testing is crucial for CDA diagnosis and includes next-generation sequencing.” (akpan2024congenitaldyserythropoieticanemia pages 1-2)
- Musri 2023: patients diagnosed using targeted NGS panels with Sanger validation (musri2023newcasesand pages 1-2).
- Registries explicitly incorporate WES/WGS for mutation characterization (French registry protocol) (NCT03983629 chunk 1).
10.4 Differential diagnosis
Registries and reviews note overlap with hereditary hemolytic anemias and acquired dyserythropoiesis, complicating diagnosis (NCT02964494 chunk 1, akpan2024congenitaldyserythropoieticanemia pages 1-2).
11. Outcome / prognosis
Robust survival and cause-specific mortality statistics were not identified in the retrieved sources. Registry protocols explicitly highlight these as unanswered questions (median survival, causes of death) and motivate long-term follow-up registries (NCT03983629 chunk 1). Prognosis is therefore best represented as variable, driven by anemia severity and iron overload burden, with registries designed to quantify long-term outcomes (NCT02964494 chunk 1, NCT03983629 chunk 1).
12. Treatment
12.1 Supportive care and escalation (real-world standard practice)
A 2024 mini-review states management is phenotype-dependent and “some severe cases may require blood transfusion, iron chelation therapy, splenectomy, and in extreme cases, hematopoietic stem cell transplant may be necessary.” (akpan2024congenitaldyserythropoieticanemia pages 1-2). The Blood review describes routine monitoring and includes transfusion support for severe anemia and HSCT in severe cases (iolascon2020congenitaldyserythropoieticanemias. pages 12-13).
12.2 Interferon-α for CDA I
A CDA I model paper notes: “for some patients, administration of interferon-α (INF-α) improves anemia and normalizes erythroid morphology… although this treatment has significant toxicities.” (noylotan2021cdan1isessential pages 1-2). Registry endpoints also track interferon efficacy (NCT03983629 chunk 1).
12.3 Iron overload management
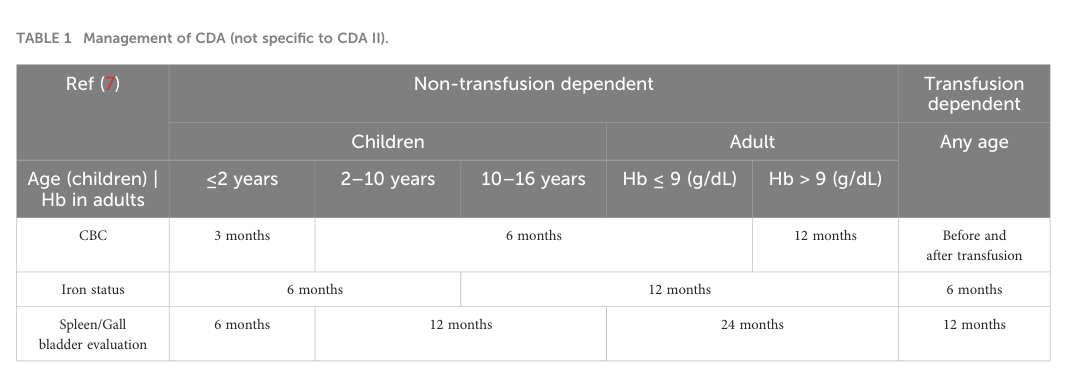
Given ERFE–hepcidin-driven absorption and transfusional exposure, iron monitoring and treatment are core (akpan2024congenitaldyserythropoieticanemia pages 1-2, NCT03983629 chunk 1). Akpan 2024 provides a management monitoring summary table (Table 1) (akpan2024congenitaldyserythropoieticanemia media 60f6d3ed).
12.4 Curative therapy: hematopoietic stem cell transplantation (HSCT)
HSCT is described as a curative option for severe CDA cases in review-level evidence (iolascon2020congenitaldyserythropoieticanemias. pages 12-13, akpan2024congenitaldyserythropoieticanemia pages 1-2).
12.5 Suggested MAXO terms (examples)
- Red blood cell transfusion
- Iron chelation therapy
- Splenectomy
- Hematopoietic stem cell transplantation
- Genetic counseling
12.6 Clinical trials / registries (current applications)
- NCT02964494 (CDAR): North American CDA registry; recruiting; started 2016-08-29, updated 2025-05-15; collects long-term natural history, complications, and treatment effects (NCT02964494 chunk 1).
- URL: https://clinicaltrials.gov/study/NCT02964494 (NCT02964494 chunk 1)
- NCT03983629: French national registry; first posted 2019-06-12; includes WES/WGS and tracks interferon efficacy and survival-related outcomes (NCT03983629 chunk 1).
- URL: https://clinicaltrials.gov/study/NCT03983629 (NCT03983629 chunk 1)
13. Prevention
Primary prevention is not generally feasible because CDA is genetic; however, secondary/tertiary prevention focuses on early diagnosis, transfusion/iron overload management, and family planning. - Prenatal and preimplantation testing become feasible once familial pathogenic variants are identified (noted in CDA literature; and consistent with genetic testing emphasis and registry inclusion of genetic analyses) (NCT03983629 chunk 1, akpan2024congenitaldyserythropoieticanemia pages 1-2).
14. Other species / natural disease
No naturally occurring CDA in non-human species was identified in the retrieved sources.
15. Model organisms
15.1 CDA I models
A 2021 study reports erythroid-specific deletion of Cdan1 causes embryonic lethality from severe anemia and recapitulates ultrastructural “spongy heterochromatin”; it also reports increased apoptosis and impaired maturation marker dynamics (noylotan2021cdan1isessential pages 1-2).
15.2 CDA II models (review evidence)
A 2022 review summarizes that SEC23B overlaps functionally with SEC23A in mice and that erythroid-specific reduction of Sec23 alleles can produce CDAII-like features, with rescue by increasing SEC23A expression (king2022thecongenitaldyserythropoieitic pages 1-3).
Key concepts & expert synthesis (authoritative analysis)
- CDA is best approached as a genetic disease group, not a single disorder, with subtype classification anchored in marrow morphology but increasingly confirmed/defined by molecular testing (NGS/WES/WGS) (iolascon2020congenitaldyserythropoieticanemias. pages 1-1, akpan2024congenitaldyserythropoieticanemia pages 1-2, NCT02964494 chunk 1).
- Iron overload is not merely transfusional in CDA; it can be mechanistically downstream of ineffective erythropoiesis via ERFE-mediated hepcidin suppression, producing progressive overload even in non-transfused individuals—an important clinical pitfall for monitoring and management (akpan2024congenitaldyserythropoieticanemia pages 1-2, iolascon2020congenitaldyserythropoieticanemias. pages 1-1, NCT03983629 chunk 1).
- Real-world implementation is increasingly registry-driven, with multicenter long-term registries explicitly designed to resolve gaps in survival, complications, genotype–phenotype correlations, and treatment effects (NCT02964494 chunk 1, NCT03983629 chunk 1).
Summary table of CDA subtypes
| Subtype | Key causal gene(s) | Inheritance | Hallmark bone marrow morphology | Key clinical features / complications | Key management notes |
|---|---|---|---|---|---|
| CDA (group); MONDO: MONDO_0019403 | Major associated genes include CDAN1, CDIN1, SEC23B, KIF23, RACGAP1, GATA1, KLF1 (OpenTargets disease–target associations) (OpenTargets Search: congenital dyserythropoietic anemia) | Heterogeneous; includes autosomal recessive and X-linked/TF-related forms depending on subtype (OpenTargets Search: congenital dyserythropoietic anemia, iolascon2020congenitaldyserythropoieticanemias. pages 1-1) | Bone marrow usually shows erythroid hyperplasia with subtype-specific dyserythropoiesis (iolascon2020congenitaldyserythropoieticanemias. pages 24-25) | Inherited anemias with ineffective erythropoiesis; iron overload can occur even without heavy transfusion burden due to erythroferrone-mediated hepcidin suppression; differential diagnosis overlaps with hereditary hemolytic anemias and acquired dyserythropoiesis (iolascon2020congenitaldyserythropoieticanemias. pages 12-13, iolascon2020congenitaldyserythropoieticanemias. pages 1-1, iolascon2020congenitaldyserythropoieticanemias. pages 24-25) | Monitoring includes CBC and iron parameters; severe anemia may require transfusion; iron overload should be treated/monitored carefully, especially before HSCT (iolascon2020congenitaldyserythropoieticanemias. pages 12-13, akpan2024congenitaldyserythropoieticanemia media 60f6d3ed) |
| CDA I | CDAN1, CDIN1/C15orf41 (OpenTargets Search: congenital dyserythropoietic anemia) | Autosomal recessive (nagar2023congenitaldyserythropoieticanemia pages 10-11) | Internuclear chromatin bridges; EM shows “Swiss cheese” / spongy heterochromatin (iolascon2020congenitaldyserythropoieticanemias. pages 24-25, nagar2023congenitaldyserythropoieticanemia pages 10-11) | Moderate to severe anemia; hepatosplenomegaly; macrocytosis; hyperbilirubinemia; gallstones; iron overload/hemosiderosis may develop even in non-transfused patients (nagar2023congenitaldyserythropoieticanemia pages 10-11) | Mainly supportive care; RBC transfusions as needed; interferon therapy can reduce transfusion dependence; cholecystectomy for symptomatic gallstones; phlebotomy or chelation for iron overload; prenatal/preimplantation testing possible once familial variants are known (iolascon2020congenitaldyserythropoieticanemias. pages 12-13, nagar2023congenitaldyserythropoieticanemia pages 10-11) |
| CDA II (most common major type) | SEC23B (biallelic pathogenic variants) (akpan2024congenitaldyserythropoieticanemia pages 1-2, OpenTargets Search: congenital dyserythropoietic anemia) | Autosomal recessive (akpan2024congenitaldyserythropoieticanemia pages 1-2) | Binucleate erythroid precursors / erythroblasts with two or more nuclei (iolascon2020congenitaldyserythropoieticanemias. pages 24-25) | Mild to severe normocytic anemia, hemolysis, jaundice, splenomegaly, gallstones, liver iron overload; inadequate reticulocytosis despite anemia; ineffective erythropoiesis with ERFE overexpression → hepcidin suppression → increased iron absorption (akpan2024congenitaldyserythropoieticanemia pages 1-2, iolascon2020congenitaldyserythropoieticanemias. pages 12-13) | Diagnostic workup: CBC/reticulocytes, bilirubin/haptoglobin, iron studies, MRI for organ iron, bone marrow exam, and genetic testing/NGS; management may include transfusions, iron chelation, splenectomy in selected cases, and HSCT for very severe disease (akpan2024congenitaldyserythropoieticanemia pages 1-2, iolascon2020congenitaldyserythropoieticanemias. pages 12-13, akpan2024congenitaldyserythropoieticanemia media 60f6d3ed) |
| CDA II: example SEC23B variants | Examples reported in recent cohort: c.1334C>G (p.Thr445Arg), c.1736A>G (p.Tyr579Cys), c.2102G>A (p.Arg701His), c.2074_2077dupGATG (p.Asp693GlyfsTer2), c.1512-2A>G, c.1512-3delinsTT with c.1512-16_1512-7delACTCTGGAAT, c.325G>A (p.Glu109Lys), c.40C>T (p.Arg14Trp) (musri2023newcasesand pages 2-4, musri2023newcasesand pages 1-2, musri2023newcasesand pages 4-6, musri2023newcasesand pages 12-13, musri2023newcasesand pages 6-7) | Autosomal recessive; variants often occur as homozygous or compound heterozygous alleles (musri2023newcasesand pages 2-4, musri2023newcasesand pages 6-7) | Same CDA II morphology; some patients also had abnormal membrane protein electrophoresis / band 3 and EM membrane abnormalities in reported series (musri2023newcasesand pages 4-6) | Reported cohorts showed chronic Coombs-negative hemolytic anemia, hepatosplenomegaly, cholelithiasis, iron overload, and transfusion history in some patients (musri2023newcasesand pages 4-6, musri2023newcasesand pages 6-7) | Functional studies showed reduced SEC23B protein, limited SEC23A compensation in LCLs, and exon 13–14 skipping for complex intronic alleles; findings support loss-of-function disease mechanism (musri2023newcasesand pages 1-2, musri2023newcasesand pages 9-12, musri2023newcasesand pages 12-13) |
| CDA III | KIF23, RACGAP1 (OpenTargets Search: congenital dyserythropoietic anemia) | Not specified in gathered evidence for all forms; genetically distinct subtype (OpenTargets Search: congenital dyserythropoietic anemia, iolascon2020congenitaldyserythropoieticanemias. pages 1-1) | Giant multinucleated erythroblasts (iolascon2020congenitaldyserythropoieticanemias. pages 24-25) | Rare major subtype within CDA classification; specific phenotype details not fully captured in gathered excerpts (iolascon2020congenitaldyserythropoieticanemias. pages 1-1, iolascon2020congenitaldyserythropoieticanemias. pages 24-25) | Supportive care and iron monitoring principles from CDA group apply; subtype-specific evidence in gathered set is limited (iolascon2020congenitaldyserythropoieticanemias. pages 12-13, iolascon2020congenitaldyserythropoieticanemias. pages 24-25) |
| CDA IV / transcription factor–related and variant forms | KLF1, GATA1; broader CDA-associated list in OpenTargets also includes LPIN2 and other rare associations (OpenTargets Search: congenital dyserythropoietic anemia) | X-linked or other subtype-specific inheritance may apply for TF-related cytopenias; not fully resolved in gathered excerpts (OpenTargets Search: congenital dyserythropoietic anemia, iolascon2020congenitaldyserythropoieticanemias. pages 24-25) | Multinucleate erythroblasts reported for CDA IV; GATA1-related disorders may present as dyserythropoietic anemia with thrombocytopenia rather than classic isolated CDA (iolascon2020congenitaldyserythropoieticanemias. pages 24-25) | Includes GATA1-related cytopenias and KLF1-related CDA IV within modern classification; clinical manifestations are heterogeneous and may extend beyond isolated anemia (iolascon2020congenitaldyserythropoieticanemias. pages 1-1, iolascon2020congenitaldyserythropoieticanemias. pages 24-25, OpenTargets Search: congenital dyserythropoietic anemia) | No subtype-specific standard therapy detailed in gathered excerpts; diagnosis relies increasingly on molecular testing/NGS and expert hematopathology review (iolascon2020congenitaldyserythropoieticanemias. pages 1-1, iolascon2020congenitaldyserythropoieticanemias. pages 24-25) |
Table: This table summarizes major congenital dyserythropoietic anemia subtypes and selected additional/transcription-factor-related forms using only the gathered evidence. It highlights the causal genes, inheritance, hallmark marrow morphology, major clinical features, and practical management points most relevant for a disease knowledge base.
Management monitoring table (image evidence)
Akpan 2024 includes a management/monitoring table (Table 1) summarizing recommended monitoring frequencies across age groups and transfusion status (akpan2024congenitaldyserythropoieticanemia media 60f6d3ed).
Key source URLs and publication dates (from retrieved evidence)
- Akpan IJ et al. Frontiers in Hematology — published 2024-07-05. https://doi.org/10.3389/frhem.2024.1389820 (akpan2024congenitaldyserythropoieticanemia pages 1-2)
- Musri MM et al. International Journal of Molecular Sciences — published 2023-06-09. https://doi.org/10.3390/ijms24129935 (musri2023newcasesand pages 1-2)
- Saptarshi AN et al. Italian Journal of Pediatrics — published 2023-07 (article shows 2023, open access). https://doi.org/10.1186/s13052-023-01493-w (saptarshi2023developmentofhighresolution pages 1-2)
- King R et al. Current Opinion in Hematology — published 2022-05-01. https://doi.org/10.1097/MOH.0000000000000697 (king2022thecongenitaldyserythropoieitic pages 1-3)
- Noy-Lotan S et al. Frontiers in Physiology — published 2021-06-21. https://doi.org/10.3389/fphys.2021.685242 (noylotan2021cdan1isessential pages 1-2)
- Scott C et al. Haematologica — published in volume 2021; prepublished 2020; doi below. https://doi.org/10.3324/haematol.2020.260158 (scott2020recapitulationoferythropoiesis pages 1-2)
- ClinicalTrials.gov CDA registries:
- NCT02964494: https://clinicaltrials.gov/study/NCT02964494 (NCT02964494 chunk 1)
- NCT03983629: https://clinicaltrials.gov/study/NCT03983629 (NCT03983629 chunk 1)
Notable gaps in retrieved evidence (for follow-on curation)
- ICD-10/ICD-11 and Orphanet identifiers were not captured in the retrieved set.
- Quantitative QoL outcomes and robust long-term survival statistics were not found; ongoing registries aim to address these (NCT03983629 chunk 1, NCT02964494 chunk 1).
References
-
(OpenTargets Search: congenital dyserythropoietic anemia): Open Targets Query (congenital dyserythropoietic anemia, 18 results). Buniello, A. et al. (2025). Open Targets Platform: facilitating therapeutic hypotheses building in drug discovery. Nucleic Acids Research.
-
(akpan2024congenitaldyserythropoieticanemia pages 1-2): Imo J. Akpan, Kelsie Bogyo, Rebecca J. Leeman-Neill, Julia Wattacheril, and Richard O. Francis. Congenital dyserythropoietic anemia type ii and ineffective erythropoiesis: challenges in diagnosis and management. Frontiers in Hematology, Jul 2024. URL: https://doi.org/10.3389/frhem.2024.1389820, doi:10.3389/frhem.2024.1389820. This article has 1 citations.
-
(iolascon2020congenitaldyserythropoieticanemias. pages 1-1): Achille Iolascon, Roberta Russo, and Jean Delaunay. Congenital dyserythropoietic anemias. Blood, 18:146-151, Jul 2020. URL: https://doi.org/10.1182/blood.2019000948, doi:10.1182/blood.2019000948. This article has 128 citations and is from a highest quality peer-reviewed journal.
-
(NCT03983629 chunk 1): Registry of Congenital Dyserythropoietic Anemia. Lille Catholic University. 2017. ClinicalTrials.gov Identifier: NCT03983629
-
(saptarshi2023developmentofhighresolution pages 1-2): Arati Nandan Saptarshi, Rashmi K. Dongerdiye, Tejashree Anil More, and Prabhakar S. Kedar. Development of high-resolution melting curve analysis for rapid detection of sec23b gene mutation causing congenital dyserythropoietic anemia type ii in indian population. Italian Journal of Pediatrics, Jul 2023. URL: https://doi.org/10.1186/s13052-023-01493-w, doi:10.1186/s13052-023-01493-w. This article has 4 citations and is from a peer-reviewed journal.
-
(musri2023newcasesand pages 1-2): Melina Mara Musri, Veronica Venturi, Xènia Ferrer-Cortès, Lídia Romero-Cortadellas, Gonzalo Hernández, Pilar Leoz, María Pilar Ricard Andrés, Marta Morado, María del Carmen Fernández Valle, David Beneitez Pastor, Ana Ortuño Cabrero, Maite Moreno Gamiz, Leonor Senent Peris, Amanda Isabel Perez-Valencia, Santiago Pérez-Montero, Cristian Tornador, and Mayka Sánchez. New cases and mutations in sec23b gene causing congenital dyserythropoietic anemia type ii. International Journal of Molecular Sciences, 24:9935, Jun 2023. URL: https://doi.org/10.3390/ijms24129935, doi:10.3390/ijms24129935. This article has 8 citations.
-
(king2022thecongenitaldyserythropoieitic pages 1-3): Richard King, Patrick J. Gallagher, and Rami Khoriaty. The congenital dyserythropoieitic anemias: genetics and pathophysiology. Current Opinion in Hematology, 29:126-136, Dec 2022. URL: https://doi.org/10.1097/moh.0000000000000697, doi:10.1097/moh.0000000000000697. This article has 22 citations and is from a peer-reviewed journal.
-
(NCT02964494 chunk 1): The Congenital Dyserythropoietic Anemia Registry (CDAR). Children's Hospital Medical Center, Cincinnati. 2016. ClinicalTrials.gov Identifier: NCT02964494
-
(scott2020recapitulationoferythropoiesis pages 1-2): Caroline Scott, Damien J. Downes, Jill M. Brown, Robert Beagrie, Aude-Anais Olijnik, Matthew Gosden, Ron Schwessinger, Christopher A. Fisher, Anna Rose, David J.P Ferguson, Errin Johnson, Quentin A. Hill, Steven Okoli, Raffaele Renella, Kate Ryan, Marjorie Brand, Jim Hughes, Noemi B.A. Roy, Douglas R. Higgs, Christian Babbs, and Veronica J. Buckle. Recapitulation of erythropoiesis in congenital dyserythropoietic anemia type i (cda-i) identifies defects in differentiation and nucleolar abnormalities. Haematologica, 106:2960-2970, Oct 2020. URL: https://doi.org/10.3324/haematol.2020.260158, doi:10.3324/haematol.2020.260158. This article has 14 citations.
-
(shemawat2024congenitaldyserythropoieticanemia pages 1-2): Shruti Shemawat, Shweta A. Bansal, Arpita Mathur, Anjana Mittal, and Manoj Sharma. Congenital dyserythropoietic anemia type ii with myelofibrosis in an adult patient: a report of a rare case with a brief review. Cureus, Apr 2024. URL: https://doi.org/10.7759/cureus.58515, doi:10.7759/cureus.58515. This article has 0 citations.
-
(noylotan2021cdan1isessential pages 1-2): Sharon Noy-Lotan, Orly Dgany, Nathaly Marcoux, Ayelet Atkins, Gary M. Kupfer, Linette Bosques, Christine Gottschalk, Orna Steinberg-Shemer, Benny Motro, and Hannah Tamary. Cdan1 is essential for primitive erythropoiesis. Frontiers in Physiology, Jun 2021. URL: https://doi.org/10.3389/fphys.2021.685242, doi:10.3389/fphys.2021.685242. This article has 14 citations.
-
(iolascon2020congenitaldyserythropoieticanemias. pages 12-13): Achille Iolascon, Roberta Russo, and Jean Delaunay. Congenital dyserythropoietic anemias. Blood, 18:146-151, Jul 2020. URL: https://doi.org/10.1182/blood.2019000948, doi:10.1182/blood.2019000948. This article has 128 citations and is from a highest quality peer-reviewed journal.
-
(akpan2024congenitaldyserythropoieticanemia media 60f6d3ed): Imo J. Akpan, Kelsie Bogyo, Rebecca J. Leeman-Neill, Julia Wattacheril, and Richard O. Francis. Congenital dyserythropoietic anemia type ii and ineffective erythropoiesis: challenges in diagnosis and management. Frontiers in Hematology, Jul 2024. URL: https://doi.org/10.3389/frhem.2024.1389820, doi:10.3389/frhem.2024.1389820. This article has 1 citations.
-
(iolascon2020congenitaldyserythropoieticanemias. pages 24-25): Achille Iolascon, Roberta Russo, and Jean Delaunay. Congenital dyserythropoietic anemias. Blood, 18:146-151, Jul 2020. URL: https://doi.org/10.1182/blood.2019000948, doi:10.1182/blood.2019000948. This article has 128 citations and is from a highest quality peer-reviewed journal.
-
(nagar2023congenitaldyserythropoieticanemia pages 10-11): V Nagar, NJ Patil, and NJ Patil IV. Congenital dyserythropoietic anemia type i: a rare case report. Cureus, Nov 2023. URL: https://doi.org/10.7759/cureus.48594, doi:10.7759/cureus.48594. This article has 0 citations.
-
(musri2023newcasesand pages 2-4): Melina Mara Musri, Veronica Venturi, Xènia Ferrer-Cortès, Lídia Romero-Cortadellas, Gonzalo Hernández, Pilar Leoz, María Pilar Ricard Andrés, Marta Morado, María del Carmen Fernández Valle, David Beneitez Pastor, Ana Ortuño Cabrero, Maite Moreno Gamiz, Leonor Senent Peris, Amanda Isabel Perez-Valencia, Santiago Pérez-Montero, Cristian Tornador, and Mayka Sánchez. New cases and mutations in sec23b gene causing congenital dyserythropoietic anemia type ii. International Journal of Molecular Sciences, 24:9935, Jun 2023. URL: https://doi.org/10.3390/ijms24129935, doi:10.3390/ijms24129935. This article has 8 citations.
-
(musri2023newcasesand pages 4-6): Melina Mara Musri, Veronica Venturi, Xènia Ferrer-Cortès, Lídia Romero-Cortadellas, Gonzalo Hernández, Pilar Leoz, María Pilar Ricard Andrés, Marta Morado, María del Carmen Fernández Valle, David Beneitez Pastor, Ana Ortuño Cabrero, Maite Moreno Gamiz, Leonor Senent Peris, Amanda Isabel Perez-Valencia, Santiago Pérez-Montero, Cristian Tornador, and Mayka Sánchez. New cases and mutations in sec23b gene causing congenital dyserythropoietic anemia type ii. International Journal of Molecular Sciences, 24:9935, Jun 2023. URL: https://doi.org/10.3390/ijms24129935, doi:10.3390/ijms24129935. This article has 8 citations.
-
(musri2023newcasesand pages 12-13): Melina Mara Musri, Veronica Venturi, Xènia Ferrer-Cortès, Lídia Romero-Cortadellas, Gonzalo Hernández, Pilar Leoz, María Pilar Ricard Andrés, Marta Morado, María del Carmen Fernández Valle, David Beneitez Pastor, Ana Ortuño Cabrero, Maite Moreno Gamiz, Leonor Senent Peris, Amanda Isabel Perez-Valencia, Santiago Pérez-Montero, Cristian Tornador, and Mayka Sánchez. New cases and mutations in sec23b gene causing congenital dyserythropoietic anemia type ii. International Journal of Molecular Sciences, 24:9935, Jun 2023. URL: https://doi.org/10.3390/ijms24129935, doi:10.3390/ijms24129935. This article has 8 citations.
-
(musri2023newcasesand pages 6-7): Melina Mara Musri, Veronica Venturi, Xènia Ferrer-Cortès, Lídia Romero-Cortadellas, Gonzalo Hernández, Pilar Leoz, María Pilar Ricard Andrés, Marta Morado, María del Carmen Fernández Valle, David Beneitez Pastor, Ana Ortuño Cabrero, Maite Moreno Gamiz, Leonor Senent Peris, Amanda Isabel Perez-Valencia, Santiago Pérez-Montero, Cristian Tornador, and Mayka Sánchez. New cases and mutations in sec23b gene causing congenital dyserythropoietic anemia type ii. International Journal of Molecular Sciences, 24:9935, Jun 2023. URL: https://doi.org/10.3390/ijms24129935, doi:10.3390/ijms24129935. This article has 8 citations.
-
(musri2023newcasesand pages 9-12): Melina Mara Musri, Veronica Venturi, Xènia Ferrer-Cortès, Lídia Romero-Cortadellas, Gonzalo Hernández, Pilar Leoz, María Pilar Ricard Andrés, Marta Morado, María del Carmen Fernández Valle, David Beneitez Pastor, Ana Ortuño Cabrero, Maite Moreno Gamiz, Leonor Senent Peris, Amanda Isabel Perez-Valencia, Santiago Pérez-Montero, Cristian Tornador, and Mayka Sánchez. New cases and mutations in sec23b gene causing congenital dyserythropoietic anemia type ii. International Journal of Molecular Sciences, 24:9935, Jun 2023. URL: https://doi.org/10.3390/ijms24129935, doi:10.3390/ijms24129935. This article has 8 citations.