Appendiceal Neuroendocrine Tumor
Appendiceal neuroendocrine tumors (appendiceal NETs, historically "appendiceal carcinoids") are well-differentiated neoplasms arising from the diffuse neuroendocrine cells of the appendix, predominantly serotonin-producing enterochromaffin (EC) cells. They are the most common neoplasm of the appendix and are usually discovered incidentally in appendectomy specimens removed for presumed acute appendicitis. Most are small (<1 cm), low-grade (G1), and behave indolently with excellent prognosis after simple appendectomy. Tumor size, histologic grade (Ki-67 proliferation index and mitotic count), and depth of mesoappendiceal invasion are the principal determinants of metastatic risk and guide the decision between appendectomy alone and completion right hemicolectomy. Functional carcinoid syndrome (flushing, secretory diarrhea, bronchospasm, carcinoid heart disease) is rare and essentially confined to the minority of patients with hepatic metastases, because serotonin and other vasoactive amines secreted into the portal circulation are normally inactivated by the liver. Appendiceal NETs are overwhelmingly sporadic. They must be distinguished from goblet cell adenocarcinoma (formerly "goblet cell carcinoid"), an amphicrine epithelial neoplasm with mixed neuroendocrine and mucinous/glandular differentiation that is biologically more aggressive and is staged and treated as an adenocarcinoma rather than as a neuroendocrine tumor.
Ask OpenScientist
Ask a research question about Appendiceal Neuroendocrine Tumor. OpenScientist will conduct autonomous deep research using the Disorder Mechanisms Knowledge Base and PubMed literature (typically 10-30 minutes).
Do not include personal health information in your question. Questions and results are cached in your browser's local storage.
Subtypes
3Pathophysiology
4Show evidence (1 reference)
Show evidence (1 reference)
Show evidence (2 references)
Show evidence (1 reference)
Pathograph
Phenotypes
7Digestive 1
Show evidence (1 reference)
Integument 1
Show evidence (1 reference)
Growth 1
Other 4
Show evidence (1 reference)
Show evidence (1 reference)
Medical Actions
3Show evidence (2 references)
Show evidence (1 reference)
Show evidence (2 references)
Source YAML
click to showname: Appendiceal Neuroendocrine Tumor
creation_date: "2026-06-08T00:00:00Z"
description: >-
Appendiceal neuroendocrine tumors (appendiceal NETs, historically "appendiceal
carcinoids") are well-differentiated neoplasms arising from the diffuse
neuroendocrine cells of the appendix, predominantly serotonin-producing
enterochromaffin (EC) cells. They are the most common neoplasm of the appendix
and are usually discovered incidentally in appendectomy specimens removed for
presumed acute appendicitis. Most are small (<1 cm), low-grade (G1), and behave
indolently with excellent prognosis after simple appendectomy. Tumor size,
histologic grade (Ki-67 proliferation index and mitotic count), and depth of
mesoappendiceal invasion are the principal determinants of metastatic risk and
guide the decision between appendectomy alone and completion right hemicolectomy.
Functional carcinoid syndrome (flushing, secretory diarrhea, bronchospasm,
carcinoid heart disease) is rare and essentially confined to the minority of
patients with hepatic metastases, because serotonin and other vasoactive amines
secreted into the portal circulation are normally inactivated by the liver.
Appendiceal NETs are overwhelmingly sporadic. They must be distinguished from
goblet cell adenocarcinoma (formerly "goblet cell carcinoid"), an amphicrine
epithelial neoplasm with mixed neuroendocrine and mucinous/glandular
differentiation that is biologically more aggressive and is staged and treated as
an adenocarcinoma rather than as a neuroendocrine tumor.
categories:
- Solid Tumor
- Gastrointestinal Cancer
- Neuroendocrine Neoplasm
parents:
- neuroendocrine tumor
- appendix cancer
disease_term:
preferred_term: appendiceal neuroendocrine tumor
term:
id: MONDO:0015066
label: neuroendocrine tumor of the appendix, well differentiated, low or intermediate grade
has_subtypes:
- name: G1 NET
display_name: Grade 1 (G1) well-differentiated NET
description: >-
Well-differentiated appendiceal neuroendocrine tumor with low proliferative
activity (Ki-67 <3% and mitotic count <2 per 2 mm^2). The most common grade;
typically small, incidentally discovered, and cured by appendectomy alone.
- name: G2 NET
display_name: Grade 2 (G2) well-differentiated NET
description: >-
Well-differentiated appendiceal neuroendocrine tumor with intermediate
proliferative activity (Ki-67 3-20% or mitotic count 2-20 per 2 mm^2). Higher
grade and larger size correlate with increased risk of nodal and distant spread.
- name: Goblet Cell Adenocarcinoma
display_name: Goblet cell adenocarcinoma (distinct entity)
description: >-
Amphicrine appendiceal neoplasm composed of goblet-like mucinous cells with
variable neuroendocrine differentiation, formerly termed "goblet cell carcinoid."
The 2019 WHO classification reclassified it as an adenocarcinoma; it behaves more
aggressively than conventional appendiceal NET and is staged and managed as an
adenocarcinoma. Included here to document its distinction from true appendiceal
neuroendocrine tumors, not as a neuroendocrine subtype.
pathophysiology:
- name: Neoplastic Proliferation of Appendiceal Enterochromaffin Cells
description: >-
Appendiceal NETs arise from the diffuse neuroendocrine cell compartment of the
appendiceal mucosa, predominantly serotonin-producing enterochromaffin (EC)
cells. Clonal neoplastic proliferation of these cells produces a
well-differentiated tumor expressing neuroendocrine markers (chromogranin A,
synaptophysin) and frequently arises in a subepithelial/submucosal location.
cell_types:
- preferred_term: enterochromaffin cell
term:
id: CL:0000577
label: type EC enteroendocrine cell
- preferred_term: serotonin secreting cell
term:
id: CL:0000458
label: serotonin secreting cell
locations:
- preferred_term: vermiform appendix
term:
id: UBERON:0001154
label: vermiform appendix
biological_processes:
- preferred_term: cell population proliferation
modifier: INCREASED
term:
id: GO:0008283
label: cell population proliferation
evidence:
- reference: PMID:33754384
reference_title: "Risk factors for progression of appendiceal neuroendocrine tumours: low-stage tumours <5 mm appear to be overwhelmingly indolent and may merit a separate designation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Appendiceal well-differentiated neuroendocrine tumours (NETs) are usually
incidental and clinically benign.
explanation: >-
Establishes appendiceal NET as a well-differentiated neuroendocrine neoplasm
that is usually incidental and clinically benign.
downstream:
- target: Serotonin Secretion and Storage in Neurosecretory Granules
description: >-
Neoplastic EC cells retain serotonin biosynthetic machinery and secretory
granules.
- target: Size-, Grade-, and Invasion-Dependent Metastatic Progression
description: >-
Tumor growth and acquisition of invasive potential drive metastatic risk.
- name: Serotonin Secretion and Storage in Neurosecretory Granules
description: >-
Tumor EC cells synthesize serotonin from L-tryptophan and store it, along with
other bioactive amines and peptides, in dense-core secretory (neurosecretory)
granules. Serotonin and its metabolites underlie the biochemical hallmarks of
serotonin-producing NETs; urinary 5-hydroxyindoleacetic acid (5-HIAA), the major
serotonin metabolite, is the principal biochemical marker.
cell_types:
- preferred_term: enterochromaffin cell
term:
id: CL:0000577
label: type EC enteroendocrine cell
biological_processes:
- preferred_term: serotonin biosynthetic process
modifier: INCREASED
term:
id: GO:0042427
label: serotonin biosynthetic process
- preferred_term: serotonin secretion
modifier: INCREASED
term:
id: GO:0001820
label: serotonin secretion
cellular_components:
- preferred_term: secretory granule
term:
id: GO:0030141
label: secretory granule
evidence:
- reference: PMID:28904734
reference_title: "A 17-year-old male with a Small Bowel Neuroendocrine Tumor: flushing differential diagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Small bowel NETs (SB-NETs) are related to serotonin hypersecretion which
causes: flushing, diarrhea, abdominal pain, bronchoconstriction and heart
involvement, also known as carcinoid syndrome (CS).
explanation: >-
Documents that serotonin hypersecretion by midgut/small-bowel NETs (the same
EC-cell biology as appendiceal NET) drives the carcinoid syndrome.
downstream:
- target: Hepatic Metastasis and Carcinoid Syndrome
description: >-
Systemic serotonin escape from first-pass hepatic clearance produces the
carcinoid syndrome only once liver metastases are present.
- name: Size-, Grade-, and Invasion-Dependent Metastatic Progression
description: >-
The metastatic risk of an appendiceal NET is governed chiefly by tumor size,
histologic grade (Ki-67 index and mitotic count), and depth of mesoappendiceal
invasion. Small (<1 cm) low-grade tumors confined to the appendix rarely
metastasize and are cured by appendectomy, whereas larger tumors, higher grade,
and deep mesoappendiceal invasion increase the likelihood of lymph node and
distant spread and prompt consideration of right hemicolectomy.
cell_types:
- preferred_term: enterochromaffin cell
term:
id: CL:0000577
label: type EC enteroendocrine cell
biological_processes:
- preferred_term: negative regulation of apoptotic process
modifier: INCREASED
term:
id: GO:0043066
label: negative regulation of apoptotic process
evidence:
- reference: PMID:33754384
reference_title: "Risk factors for progression of appendiceal neuroendocrine tumours: low-stage tumours <5 mm appear to be overwhelmingly indolent and may merit a separate designation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Increasing tumour size was associated with an increased risk of nodal disease
explanation: >-
Demonstrates that larger tumor size predicts nodal metastasis, supporting
size as a key determinant of metastatic risk.
- reference: PMID:33754384
reference_title: "Risk factors for progression of appendiceal neuroendocrine tumours: low-stage tumours <5 mm appear to be overwhelmingly indolent and may merit a separate designation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Small (<5 mm) App-NETs that do not invade the serosa or mesoappendix appear
to be overwhelmingly benign and low-grade
explanation: >-
Confirms that small tumors without mesoappendiceal/serosal invasion are
overwhelmingly indolent, supporting size and invasion depth as risk factors.
downstream:
- target: Hepatic Metastasis and Carcinoid Syndrome
description: >-
Distant spread to the liver is the prerequisite for systemic serotonin effects.
- name: Hepatic Metastasis and Carcinoid Syndrome
description: >-
Under normal portal anatomy, serotonin and other vasoactive amines secreted by
a primary gut NET are cleared during first-pass hepatic metabolism, so systemic
symptoms do not occur. Once liver metastases secrete vasoactive products directly
into the systemic (hepatic venous) circulation, patients develop the carcinoid
syndrome: episodic flushing, secretory diarrhea, bronchospasm, and, over time,
fibrotic right-sided (tricuspid/pulmonary) carcinoid heart disease. Carcinoid
syndrome is rare in appendiceal NET because most tumors are small and never
metastasize.
locations:
- preferred_term: vermiform appendix
term:
id: UBERON:0001154
label: vermiform appendix
biological_processes:
- preferred_term: serotonin secretion
modifier: INCREASED
term:
id: GO:0001820
label: serotonin secretion
evidence:
- reference: PMID:28904734
reference_title: "A 17-year-old male with a Small Bowel Neuroendocrine Tumor: flushing differential diagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Hepatic and intestinal biopsies reported a well-differentiated NET of the
ileocecal valve with hepatic metastasis. He was started on octreotide
explanation: >-
Illustrates that carcinoid syndrome from a midgut serotonin-secreting NET
accompanies hepatic metastasis (with elevated urinary 5-HIAA), the same
mechanism by which appendiceal NET produces carcinoid syndrome only when
liver metastases are present.
phenotypes:
- name: Carcinoid Tumor
category: Neoplasm
description: >-
Appendiceal NET is a well-differentiated carcinoid (neuroendocrine) tumor of the
appendix.
phenotype_term:
preferred_term: Carcinoid tumor
term:
id: HP:0100570
label: Carcinoid tumor
- name: Acute Appendicitis Presentation
category: Clinical
description: >-
Most appendiceal NETs are clinically silent and are found incidentally in
appendectomy specimens removed for symptoms of acute appendicitis, sometimes
because a tumor at the appendiceal base obstructs the lumen.
phenotype_term:
preferred_term: Appendicitis
term:
id: HP:6000143
label: Appendicitis
evidence:
- reference: PMID:33754384
reference_title: "Risk factors for progression of appendiceal neuroendocrine tumours: low-stage tumours <5 mm appear to be overwhelmingly indolent and may merit a separate designation."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Appendiceal well-differentiated neuroendocrine tumours (NETs) are usually
incidental and clinically benign.
explanation: >-
Most appendiceal NETs are incidental findings, typically in appendectomy
specimens removed for presumed appendicitis.
- name: Flushing
category: Clinical
description: >-
Episodic cutaneous flushing is a cardinal feature of the carcinoid syndrome,
occurring in appendiceal NET essentially only in the setting of hepatic
metastases.
phenotype_term:
preferred_term: Flushing
term:
id: HP:0031284
label: Flushing
temporality: RECURRENT
evidence:
- reference: PMID:28904734
reference_title: "A 17-year-old male with a Small Bowel Neuroendocrine Tumor: flushing differential diagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Small bowel NETs (SB-NETs) are related to serotonin hypersecretion which
causes: flushing, diarrhea, abdominal pain, bronchoconstriction and heart
involvement, also known as carcinoid syndrome (CS).
explanation: >-
Flushing is a cardinal feature of the serotonin-driven carcinoid syndrome
seen with metastatic midgut/appendiceal NETs.
- name: Secretory Diarrhea
category: Clinical
description: >-
Chronic secretory diarrhea is a major component of the carcinoid syndrome driven
by serotonin and other secretagogues released by metastatic tumor.
phenotype_term:
preferred_term: Diarrhea
term:
id: HP:0002014
label: Diarrhea
temporality: CHRONIC
evidence:
- reference: PMID:28904734
reference_title: "A 17-year-old male with a Small Bowel Neuroendocrine Tumor: flushing differential diagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Small bowel NETs (SB-NETs) are related to serotonin hypersecretion which
causes: flushing, diarrhea, abdominal pain, bronchoconstriction and heart
involvement, also known as carcinoid syndrome (CS).
explanation: >-
Diarrhea is a defining feature of serotonin-mediated carcinoid syndrome in
midgut/appendiceal NETs.
- name: Elevated Urinary 5-HIAA
category: Laboratory
description: >-
24-hour urinary 5-hydroxyindoleacetic acid (5-HIAA), the principal serotonin
metabolite, is elevated in serotonin-secreting NETs with carcinoid syndrome and
serves as the main biochemical marker.
phenotype_term:
preferred_term: Elevated urinary 5-hydroxyindoleacetic acid level
term:
id: HP:6000756
label: Elevated urinary 5-hydroxyindoleacetic acid level
evidence:
- reference: PMID:28904734
reference_title: "A 17-year-old male with a Small Bowel Neuroendocrine Tumor: flushing differential diagnosis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
The 24-h urinary 5-hydroxyindoleacetic acid (5-HIAA) excretion was elevated.
explanation: >-
Elevated 24-hour urinary 5-HIAA is the principal biochemical marker of
serotonin-secreting NETs with carcinoid syndrome.
- name: Carcinoid Heart Disease (Tricuspid Regurgitation)
category: Clinical
description: >-
Chronic serotonin exposure causes plaque-like fibrous thickening of right-sided
endocardium and valves, producing tricuspid regurgitation and pulmonary valve
disease in long-standing metastatic carcinoid syndrome.
phenotype_term:
preferred_term: Tricuspid regurgitation
term:
id: HP:0005180
label: Tricuspid regurgitation
- name: Weight Loss
category: Clinical
description: >-
Weight loss may accompany advanced or metastatic disease and chronic carcinoid
syndrome.
phenotype_term:
preferred_term: Weight loss
term:
id: HP:0001824
label: Weight loss
treatments:
- name: Appendectomy
description: >-
Simple appendectomy is curative for the majority of appendiceal NETs, which are
small (<1 cm), low-grade, and confined to the appendix.
treatment_term:
preferred_term: appendectomy
term:
id: MAXO:0001032
label: appendectomy
therapeutic_modality: SURGERY
evidence:
- reference: PMID:42057320
reference_title: "De-Escalating Surgery for 1-2 cm Appendiceal Neuroendocrine Tumors: A North American Multi-Center Analysis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
NCCN guidelines recommend right hemicolectomy (RHC) for appendiceal
neuroendocrine tumors (aNETs) > 2 cm and observation for < 1 cm.
explanation: >-
NCCN guidance reserves more extensive surgery for larger tumors; small aNETs
are managed with appendectomy/observation.
- reference: PMID:42057320
reference_title: "De-Escalating Surgery for 1-2 cm Appendiceal Neuroendocrine Tumors: A North American Multi-Center Analysis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Among patients with 1-2 cm aNETs, RHC conferred no survival benefit over APY.
explanation: >-
Appendectomy alone (APY) conferred outcomes equivalent to right hemicolectomy
for 1-2 cm appendiceal NETs, supporting appendectomy as adequate treatment in
many cases.
- name: Right Hemicolectomy
description: >-
Completion right hemicolectomy with mesenteric lymphadenectomy is considered for
appendiceal NETs with higher-risk features such as size >2 cm, deep
mesoappendiceal invasion, higher grade, or positive/uncertain margins.
treatment_term:
preferred_term: right colectomy
term:
id: NCIT:C51623
label: Right Colectomy
therapeutic_modality: SURGERY
evidence:
- reference: PMID:42057320
reference_title: "De-Escalating Surgery for 1-2 cm Appendiceal Neuroendocrine Tumors: A North American Multi-Center Analysis."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
NCCN guidelines recommend right hemicolectomy (RHC) for appendiceal
neuroendocrine tumors (aNETs) > 2 cm and observation for < 1 cm.
explanation: >-
Completion right hemicolectomy is the guideline-recommended option for larger
(>2 cm) appendiceal NETs.
- name: Somatostatin Analogue Therapy
description: >-
Long-acting somatostatin analogues (e.g., octreotide, lanreotide) control
carcinoid-syndrome symptoms (flushing, diarrhea) and provide antiproliferative
benefit in advanced, somatostatin-receptor-positive well-differentiated NETs.
treatment_term:
preferred_term: Pharmacotherapy
term:
id: NCIT:C15986
label: Pharmacotherapy
therapeutic_agent:
- preferred_term: octreotide
term:
id: CHEBI:7726
label: octreotide
therapeutic_modality: PEPTIDE
evidence:
- reference: PMID:28286921
reference_title: "Treatment Strategies for Metastatic Neuroendocrine Tumors of the Gastrointestinal Tract."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
Current and emerging treatment options include somatostatin analogs,
radiolabeled somatostatin analogs, the mTOR inhibitor everolimus, and the
tyrosine kinase inhibitor sunitinib.
explanation: >-
Somatostatin analogues are a standard treatment option for metastatic
gastrointestinal NETs, including for symptom control and antiproliferative
effect.
- reference: PMID:37682701
reference_title: "European Neuroendocrine Tumor Society (ENETS) 2023 guidance paper for appendiceal neuroendocrine tumours (aNET)."
supports: SUPPORT
evidence_source: HUMAN_CLINICAL
snippet: >-
practical guidance for the diagnosis and management of appendiceal NET (aNET)
explanation: >-
The ENETS 2023 guidance paper provides evidence-based recommendations for the
diagnosis and management of appendiceal NET, including the role of somatostatin
analogues in advanced disease.
References & Deep Research
Deep Research
1Appendiceal Neuroendocrine Tumor (aNET/ANET) — Disease Characteristics Research Report
Target Disease
- Disease Name: Appendiceal Neuroendocrine Tumor (appendiceal neuroendocrine neoplasm)
- MONDO ID: Not identified from the retrieved sources in this run (see “Key identifiers” below).
- Category: Gastrointestinal neuroendocrine neoplasm (appendix primary).
Executive summary (current understanding)
Appendiceal neuroendocrine neoplasms (ANENs) are uncommon tumors of the appendix, most often sporadic, non-functioning, well-differentiated NETs (G1–G2) that are incidentally discovered in appendectomy specimens obtained for suspected appendicitis. Management is primarily surgical, with appendectomy adequate for most tumors <1 cm and right hemicolectomy (RHC) generally recommended for tumors ≥2 cm; however, the benefit of completion RHC for 1–2 cm tumors has been challenged by a large Europe-wide pooled cohort study showing no survival advantage and no metachronous metastases after complete resection. (andrini2023anupdateon pages 1-3, mohamed2022managementofappendix pages 1-2, nesti2023hemicolectomyversusappendectomy pages 5-12)
| Topic | Key finding (with numbers) | Source (author/year/journal) | URL/DOI | Evidence type |
|---|---|---|---|---|
| Definition / classification | Appendiceal neuroendocrine neoplasms include well-differentiated NETs (formerly “carcinoid tumors”), poorly differentiated NECs, and MiNENs; ~70–75% are well-differentiated NETs graded G1–G3 by Ki-67 and/or mitotic index. (mohamed2022managementofappendix pages 1-2, mohamed2022managementofappendix pages 2-4) | Mohamed et al., 2022, Cancers | https://doi.org/10.3390/cancers15010295 | Review/guideline synthesis |
| Epidemiology / incidence | aNET annual incidence reported at ~0.15–0.6 per 100,000; peak age 38–51 years; female predominance ~2:1; found in ~3–5 per 1,000 appendectomies; most arise at the appendix tip (~70%). (andrini2023anupdateon pages 1-3) | Andrini et al., 2023, Current Treatment Options in Oncology | https://doi.org/10.1007/s11864-023-01093-0 | Review |
| Epidemiology / incidence trends | In SEER 2000–2017, appendiceal NET incidence increased from 0.03 to 0.90 per 100,000 person-years, with the largest increase in localized disease; survival also improved over time. (wang2023incidencetrendsand pages 13-14) | Wang et al., 2023, PLOS ONE | https://doi.org/10.1371/journal.pone.0294153 | Population-based registry study |
| Stage at diagnosis | SEER (1973–2004) distribution: 60% localized, 28% regional, 12% distant at presentation. (mohamed2022managementofappendix pages 1-2) | Mohamed et al., 2022, Cancers | https://doi.org/10.3390/cancers15010295 | Review of registry data |
| Nodal metastasis by size | Reported nodal metastasis rates rise with size: ~2.5% for <1 cm, 31% for 1–2 cm, and 64% for ≥2 cm. (andrini2023anupdateon pages 1-3) | Andrini et al., 2023, Current Treatment Options in Oncology | https://doi.org/10.1007/s11864-023-01093-0 | Review |
| Nodal metastasis by size (alternative dataset) | SEER analyses summarized rates of 15% (<1 cm), 47% (1.0–1.9 cm), and 86% (>2 cm); another series reported 31% for 1.1–2 cm and 64% for >2 cm. (mohamed2022managementofappendix pages 4-5) | Mohamed et al., 2022, Cancers | https://doi.org/10.3390/cancers15010295 | Review of registry studies |
| Distant metastasis / carcinoid syndrome | Carcinoid syndrome is very rare (<1%) and generally occurs only with metastases. (andrini2023anupdateon pages 1-3) | Andrini et al., 2023, Current Treatment Options in Oncology | https://doi.org/10.1007/s11864-023-01093-0 | Review |
| Surgery threshold: appendectomy | Consensus summarized by guidelines supports appendectomy for tumors <1 cm, and for 1.0–1.9 cm tumors without high-risk features. (mohamed2022managementofappendix pages 4-5) | Mohamed et al., 2022, Cancers | https://doi.org/10.3390/cancers15010295 | Review/guideline synthesis |
| Surgery threshold: right hemicolectomy | Most guidelines recommend right hemicolectomy for tumors >2 cm; high-risk features include deep mesoappendiceal invasion >3 mm, positive/unclear margins, lymphovascular invasion, and higher proliferative rate. (mohamed2022managementofappendix pages 4-5) | Mohamed et al., 2022, Cancers | https://doi.org/10.3390/cancers15010295 | Review/guideline synthesis |
| Intermediate tumors (1–2 cm) | Authors suggest considering right hemicolectomy when tumor size is >15 mm and/or G2 and/or lymphovascular invasion, ideally after multidisciplinary review. (andrini2023anupdateon pages 1-3, andrini2023anupdateon pages 7-9) | Andrini et al., 2023, Current Treatment Options in Oncology | https://doi.org/10.1007/s11864-023-01093-0 | Expert review/opinion |
| Hemicolectomy vs appendectomy outcomes (1–2 cm) | Europe-wide pooled cohort of 278 patients: 163 appendectomy vs 115 hemicolectomy; median follow-up 13.0 years; regional nodal metastases in 22/115 (19.6%); estimated occult nodal disease after appendectomy 12.8% (95% CI 6.5–21.1%); no new metastases during >10 years follow-up; adjusted OS HR 0.88 (95% CI 0.36–2.17; p=0.71), supporting no routine hemicolectomy after complete appendectomy for 1–2 cm aNETs. (nesti2023hemicolectomyversusappendectomy pages 16-21, nesti2023hemicolectomyversusappendectomy pages 5-12, nesti2023hemicolectomyversusappendectomy pages 30-36) | Nesti et al., 2023, The Lancet Oncology | https://doi.org/10.1016/S1470-2045(22)00750-1 | Multicenter pooled retrospective cohort |
| Recent metastasis study | In an institutional series of 124 appendiceal NETs, only 10 had stage IV disease; 8/10 were synchronous, and among 114 early-stage patients none developed distant metastases during follow-up; authors concluded surveillance after resection is unlikely to help and tumors <2 cm should not receive completion hemicolectomy. (altoubah2025doappendicealneuroendocrine pages 1-2, altoubah2025doappendicealneuroendocrine pages 2-3, altoubah2025doappendicealneuroendocrine pages 3-4) | Al-Toubah et al., 2025, JNCCN | https://doi.org/10.6004/jnccn.2024.7069 | Institutional retrospective cohort |
| Recent completion-surgery study | Single-center cohort of 82 patients: lymph-node metastases in 7/82 (8.5%), distant metastases in 3/82 (3.6%); 27/82 (33%) underwent completion hemicolectomy, but only 6/27 (22%) had nodal metastases and none had distant metastases, implying overtreatment in 21/27 (75%); tumor size >2 cm was the only significant predictor of nodal metastasis. (wachter2025retrospectiveanalysisof pages 1-2, wachter2025retrospectiveanalysisof pages 2-4) | Wächter et al., 2025, Langenbeck's Archives of Surgery | https://doi.org/10.1007/s00423-024-03603-6 | Single-center retrospective cohort |
| Imaging recommendations | For NETs >2 cm, incomplete resection, or positive nodes/margins, recommend contrast-enhanced triple-phase CT or MRI; somatostatin-receptor PET with Ga-68 or Cu-64 DOTATATE is preferred and considered the diagnostic/surveillance gold standard for SSTR-positive disease. (mohamed2022managementofappendix pages 4-5) | Mohamed et al., 2022, Cancers | https://doi.org/10.3390/cancers15010295 | Review/guideline synthesis |
| Imaging in high-grade disease | Poorly differentiated/high-grade NECs are better evaluated with 18F-FDG PET plus CT/MRI rather than SSTR-based imaging. (mohamed2022managementofappendix pages 4-5) | Mohamed et al., 2022, Cancers | https://doi.org/10.3390/cancers15010295 | Review/guideline synthesis |
| Biomarkers | Chromogranin A may be elevated but is nonspecific; 5-HIAA (plasma or 24-h urine) is mainly useful in serotonin-producing tumors with carcinoid features or liver metastases. (mohamed2022managementofappendix pages 2-4, mohamed2022managementofappendix pages 4-5) | Mohamed et al., 2022, Cancers | https://doi.org/10.3390/cancers15010295 | Review/guideline synthesis |
| Survival / prognosis | Localized well-differentiated NETs have median OS >20 years; NCDB 5-year survival for ANETs was 86.3% (95% CI 81.4–89.9); 5-year survival by size was 89.9% (≤2 cm), 70.6% (2–4 cm), and 58.2% (>4 cm). (mohamed2022managementofappendix pages 2-4) | Mohamed et al., 2022, Cancers | https://doi.org/10.3390/cancers15010295 | Review of registry data |
| Follow-up / surveillance | Most well-differentiated appendiceal NETs <2 cm with negative margins and mesoappendiceal invasion <3 mm have low recurrence risk and often need no surveillance; postoperative surveillance is unlikely to benefit resected small tumors in recent retrospective data. (mohamed2022managementofappendix pages 4-5, altoubah2025doappendicealneuroendocrine pages 1-2, altoubah2025doappendicealneuroendocrine pages 3-4) | Mohamed et al., 2022, Cancers; Al-Toubah et al., 2025, JNCCN | https://doi.org/10.3390/cancers15010295; https://doi.org/10.6004/jnccn.2024.7069 | Review/guideline synthesis; retrospective cohort |
Table: This table compiles key evidence-backed facts about appendiceal neuroendocrine tumors/neoplasms from the retrieved literature, emphasizing incidence, metastatic risk by tumor size, management thresholds, diagnostics, and recent outcome studies. It is designed as a compact reference for evidence-supported knowledge base population.
1. Disease information
What is the disease?
- Definition / scope: Appendiceal neuroendocrine neoplasms include well-differentiated neuroendocrine tumors (NETs; historically called “carcinoid tumors”), poorly differentiated neuroendocrine carcinomas (NECs), and mixed neuroendocrine–non-neuroendocrine neoplasms (MiNENs) arising in the appendix. (mohamed2022managementofappendix pages 1-2, mohamed2022managementofappendix pages 2-4)
- Most appendiceal NENs are well-differentiated NETs; a 2022 guideline-synthesis review states ~70–75% are well-differentiated NETs. (mohamed2022managementofappendix pages 1-2)
Key identifiers (OMIM, Orphanet, ICD-10/ICD-11, MeSH, MONDO)
- Not recovered from the retrieved documents in this run (no ICD/MeSH/MONDO/Orphanet codes were present in accessible excerpts). (mohamed2022managementofappendix pages 1-2)
Synonyms / alternative names
- Appendiceal neuroendocrine tumor (aNET/ANET)
- Appendiceal neuroendocrine neoplasm (ANEN)
- Appendiceal carcinoid tumor (legacy term for well-differentiated appendiceal NET) (mohamed2022managementofappendix pages 1-2)
Evidence provenance
- The synthesized disease understanding here is derived primarily from aggregated disease-level resources (reviews, guideline syntheses, registry-based cohort studies) plus large pooled/retrospective clinical cohorts. (mohamed2022managementofappendix pages 4-5, nesti2023hemicolectomyversusappendectomy pages 5-12, wachter2025retrospectiveanalysisof pages 1-2)
2. Etiology
Disease causal factors
- ANENs are described as “usually sporadic tumors” in a guideline-synthesis review. (mohamed2022managementofappendix pages 1-2)
Risk factors
- Evidence gap in retrieved sources: The retrieved texts emphasize sporadic presentation and incidental detection but do not provide well-supported, tumor-specific environmental or inherited risk factors for appendiceal NET. (mohamed2022managementofappendix pages 1-2)
Protective factors / gene–environment interactions
- Not identified in the retrieved evidence set. (mohamed2022managementofappendix pages 1-2)
3. Phenotypes (clinical presentation) + suggested HPO terms
Typical presentation
- Incidental diagnosis after appendectomy for suspected appendicitis is the dominant presentation pattern. (mohamed2022managementofappendix pages 1-2)
- Tumors are most often located at the distal tip of the appendix. (mohamed2022managementofappendix pages 1-2)
- Functional syndromes are rare: a 2023 review reports carcinoid syndrome is very rare (<1%), generally occurring only with metastases. (andrini2023anupdateon pages 1-3)
Phenotype characteristics (age of onset, severity, progression)
- Demographics from a 2023 review: peak age reported as ~38–51 years with female predominance (~2:1). (andrini2023anupdateon pages 1-3)
- Clinical course is typically indolent for localized well-differentiated tumors, consistent with high long-term survival in registry/retrospective datasets. (mohamed2022managementofappendix pages 2-4, nesti2023hemicolectomyversusappendectomy pages 5-12)
HPO term suggestions (non-exhaustive)
- Abdominal pain (HPO: Abdominal pain)
- Acute appendicitis-like presentation (HPO: Appendicitis or Abdominal pain with acute onset)
- Incidental finding (HPO: Incidental finding)
- If functional/metastatic:
- Carcinoid syndrome (HPO: Carcinoid syndrome)
- Diarrhea (HPO: Diarrhea)
- Flushing (HPO: Flushing)
Biomarker phenotype links (laboratory abnormalities)
- Chromogranin A may be elevated but is nonspecific (confounded by renal/hepatic disease and medications). (mohamed2022managementofappendix pages 2-4)
- 5-HIAA (plasma or 24-hour urine) is mainly useful when serotonin excess is suspected (carcinoid features or liver metastases). (mohamed2022managementofappendix pages 4-5, mohamed2022managementofappendix pages 2-4)
4. Genetic / molecular information
Causal genes / germline predisposition
- Not identified for appendiceal NET specifically in the retrieved sources. The main high-confidence statements available were that ANENs are typically sporadic. (mohamed2022managementofappendix pages 1-2)
Pathophysiology-linked molecular features (clinically used)
- Proliferation index (Ki-67) and mitotic rate are central to grading well-differentiated NETs and correlate with behavior. (mohamed2022managementofappendix pages 1-2, mohamed2022managementofappendix pages 2-4)
- Somatostatin receptor (SSTR) biology is clinically actionable: SSTR-targeted PET is described as preferred and a “gold standard” approach for SSTR-positive disease evaluation/surveillance in guideline syntheses. (mohamed2022managementofappendix pages 4-5)
Proposed ontology annotations
- Cell types (Cell Ontology; CL) — suggestions:
- Enteroendocrine cell (CL: enteroendocrine cell; as the relevant neuroendocrine lineage of the gut)
- GO biological process — suggestions (non-exhaustive):
- Regulation of cell proliferation
- Neuroendocrine differentiation
- Hormone secretion / regulated exocytosis
5. Environmental information
No appendiceal-NET-specific toxin, lifestyle, or infectious triggers were supported in the retrieved evidence set. (mohamed2022managementofappendix pages 1-2)
6. Mechanism / pathophysiology
Mechanistic chain (clinically grounded)
- Neuroendocrine neoplastic transformation in appendiceal neuroendocrine lineage cells results in a well-differentiated NET in most cases. (mohamed2022managementofappendix pages 1-2)
- Growth and invasion are typically limited in small tumors; however, increasing tumor size and adverse histopathologic features associate with higher probability of regional lymph node metastasis and (rarely) distant spread. (mohamed2022managementofappendix pages 4-5, wachter2025retrospectiveanalysisof pages 1-2)
- Systemic functional symptoms (carcinoid syndrome) are uncommon and generally reflect metastatic disease. (andrini2023anupdateon pages 1-3)
Key pathways and cellular processes
- The retrieved sources did not provide appendiceal-NET-specific pathway alterations (e.g., MAPK/PI3K driver mutations) with primary molecular evidence; thus, pathway-level claims are not made here. (mohamed2022managementofappendix pages 1-2)
7. Anatomical structures affected
Primary organ
- Appendix (UBERON suggestion: vermiform appendix).
Localization
- Most tumors arise at the appendiceal tip/distal appendix. (andrini2023anupdateon pages 1-3, mohamed2022managementofappendix pages 1-2)
Metastatic spread (when present)
- In a large institutional cohort (2008–2023), stage IV disease was rare and, among metastatic cases, common sites included peritoneum and liver, with ovarian involvement noted among females in metastatic subset. (altoubah2025doappendicealneuroendocrine pages 2-3)
8. Temporal development
Onset and course
- Often detected in young to middle-aged adults and diagnosed after acute presentation leading to appendectomy. (andrini2023anupdateon pages 1-3, mohamed2022managementofappendix pages 1-2)
Progression
- For completely resected 1–2 cm tumors, a Europe-wide pooled cohort with median 13 years follow-up reported no metachronous distant metastases and no tumor-related deaths. (nesti2023hemicolectomyversusappendectomy pages 5-12)
9. Inheritance and population
Epidemiology (recent data prioritized)
- Incidence trend (SEER 2000–2017): appendiceal NET incidence increased from 0.03 to 0.90 per 100,000 person-years, with the most pronounced increase in localized disease. (Wang et al., PLOS ONE, published Nov 2023; https://doi.org/10.1371/journal.pone.0294153) (wang2023incidencetrendsand pages 13-14)
- Reported incidence range: a 2023 review reports annual incidence ~0.15–0.6 per 100,000 and that aNETs are found in approximately 3–5 per 1,000 appendectomies. (Andrini et al., Current Treatment Options in Oncology, May 2023; https://doi.org/10.1007/s11864-023-01093-0) (andrini2023anupdateon pages 1-3)
- Stage distribution (historical SEER 1973–2004): 60% localized, 28% regional, 12% distant at diagnosis. (mohamed2022managementofappendix pages 1-2)
Inheritance
- No Mendelian inheritance pattern or specific causal genes were supported by the retrieved appendiceal-NET-focused evidence; tumors are generally described as sporadic. (mohamed2022managementofappendix pages 1-2)
10. Diagnostics
Histopathology / immunohistochemistry
- Diagnostic confirmation typically relies on postoperative pathology with neuroendocrine immunophenotype markers (e.g., synaptophysin, chromogranin A variably, CD56) and Ki-67 assessment for grading. (vasile2025neuroendocrinetumorsof pages 3-4, kim2025appendicealneuroendocrinetumor pages 4-6)
Imaging
Guideline-synthesis evidence indicates imaging choice depends on risk features and differentiation: - For higher-risk localized disease (e.g., >2 cm, incomplete resection, positive nodes/margins), guidelines recommend contrast-enhanced triple-phase CT or MRI. (mohamed2022managementofappendix pages 4-5) - Somatostatin receptor PET (Ga-68 or Cu-64 DOTATATE) is described as preferred, “gold standard” for SSTR-positive lesions; lesions considered SSTR-positive if uptake exceeds liver background in the cited synthesis. (mohamed2022managementofappendix pages 4-5) - For high-grade NEC, FDG-PET is favored. (mohamed2022managementofappendix pages 4-5) - Reported imaging performance in the 2022 synthesis: FDG-PET/CT sensitivity/specificity 61.9%/100%, and 68Ga-DOTATATE PET/CT sensitivity/specificity approximately 100–81% and 90–80% across studies summarized there (with reported false positives 0–38%). (mohamed2022managementofappendix pages 4-5)
Differential diagnosis
- The retrieved evidence set did not provide a structured differential diagnosis list; however, the classification framework distinguishes well-differentiated NET from poorly differentiated NEC and MiNEN, which has major prognostic and therapeutic implications. (mohamed2022managementofappendix pages 1-2, mohamed2022managementofappendix pages 2-4)
Visual evidence (staging/management)
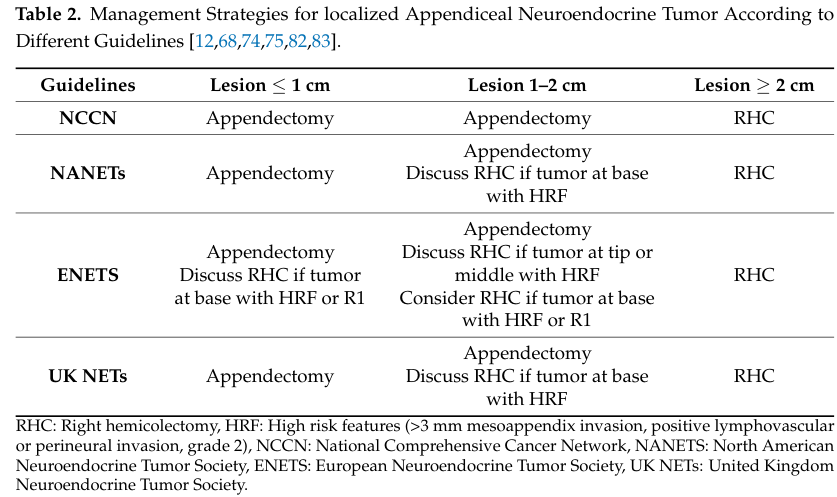
- TNM staging with survival estimates and guideline comparisons for appendectomy vs RHC indications are shown in extracted figures/tables from Mohamed et al. 2022. (mohamed2022managementofappendix media 6bf50e49, mohamed2022managementofappendix media 58ffb4ea, mohamed2022managementofappendix media 5c304756)
11. Outcome / prognosis
Survival and prognostic factors
- Prognosis is strongly related to tumor size, differentiation/grade, margins, and metastatic stage. (mohamed2022managementofappendix pages 2-4)
- A guideline-synthesis review summarizing NCDB data reports:
- 5-year survival for ANETs ~86.3% (95% CI 81.4–89.9). (mohamed2022managementofappendix pages 2-4)
- Size-stratified 5-year survival: 89.9% (≤2 cm), 70.6% (2–4 cm), 58.2% (>4 cm). (mohamed2022managementofappendix pages 2-4)
- Stage IV disease appears extremely uncommon in specialty-center populations: an institutional series identified 10 stage IV cases among 124 appendiceal NET patients, and most were synchronous at diagnosis. (altoubah2025doappendicealneuroendocrine pages 1-2)
Nodal metastases and clinical relevance
- Lymph-node metastasis probability increases with tumor size in registry-based summaries and cohorts. (mohamed2022managementofappendix pages 4-5, wachter2025retrospectiveanalysisof pages 1-2)
- Importantly, long-term outcomes suggest nodal disease in 1–2 cm tumors may be clinically less consequential: in the Europe-wide pooled cohort, there were no metachronous metastases and no tumor-related deaths after complete resection despite ~20% nodal positivity in the hemicolectomy group. (nesti2023hemicolectomyversusappendectomy pages 5-12)
12. Treatment
Surgical management (real-world implementation + recent developments)
Surgery is the mainstay: - <1 cm: appendectomy is generally considered curative when margins are negative. (mohamed2022managementofappendix pages 4-5, andrini2023anupdateon pages 1-3) - ≥2 cm: most guidelines recommend right hemicolectomy with lymphadenectomy due to higher nodal metastasis risk. (mohamed2022managementofappendix pages 4-5, andrini2023anupdateon pages 1-3) - 1–2 cm: management is controversial; recent high-quality evidence supports de-escalation: - Nesti et al., The Lancet Oncology (Feb 2023, DOI: https://doi.org/10.1016/S1470-2045(22)00750-1) pooled 278 patients (1–2 cm aNET): appendectomy vs hemicolectomy showed no OS benefit (adjusted HR 0.88; p=0.71), and “All metastases were diagnosed synchronously with no tumour-related deaths during the follow-up” (quote from study summary evidence). (nesti2023hemicolectomyversusappendectomy pages 5-12) - A single-center ENETS center retrospective analysis (2025) reported that guideline-based completion RHC may lead to substantial overtreatment: 27/82 (33%) had completion surgery but only 6/27 (22%) had nodal metastases and 0 had distant metastases in completion specimens; tumor size >2 cm was the only significant predictor of nodal metastasis. (Wächter et al., Jan 2025; https://doi.org/10.1007/s00423-024-03603-6) (wachter2025retrospectiveanalysisof pages 1-2)
Guideline comparison and algorithm (visual): Table 2 and Figure 2 extracted from Mohamed et al. summarize across NCCN/NANETS/ENETS/UK NET guidance when to recommend appendectomy versus RHC and show a post-appendectomy surgical algorithm. (mohamed2022managementofappendix media 6bf50e49, mohamed2022managementofappendix media 58ffb4ea, mohamed2022managementofappendix media 5c304756)
Systemic therapy (advanced disease)
- For well-differentiated metastatic NENs, the evidence set primarily supports SSTR-based imaging and implies feasibility of SSTR-targeted approaches (SSAs/PRRT) when SSTR-positive; appendiceal-specific systemic trial evidence was not directly retrieved. (mohamed2022managementofappendix pages 4-5)
- For poorly differentiated NECs, platinum–etoposide is noted as a standard approach in the guideline synthesis. (mohamed2022managementofappendix pages 14-16)
Treatment outcomes and surveillance
- The 2022 guideline-synthesis review notes that many well-differentiated appendiceal NETs <2 cm with negative margins and limited mesoappendiceal invasion have low recurrence risk and often do not require surveillance. (mohamed2022managementofappendix pages 4-5)
- A 2025 institutional analysis similarly concluded that for tumors <2 cm, completion hemicolectomy is overtreatment and “postoperative surveillance is unlikely to be of benefit” (quote captured in evidence). (altoubah2025doappendicealneuroendocrine pages 1-2)
MAXO term suggestions (non-exhaustive)
- Appendectomy; right hemicolectomy; lymphadenectomy (surgical)
- Contrast-enhanced CT; MRI; somatostatin receptor PET (diagnostic)
- Somatostatin analogue therapy; peptide receptor radionuclide therapy (PRRT) (advanced disease; where applicable)
13. Prevention
No primary prevention strategies specific to appendiceal NET were supported in the retrieved sources; the dominant theme is incidental detection during appendectomy rather than screening. (mohamed2022managementofappendix pages 1-2)
14. Other species / natural disease
No cross-species naturally occurring appendiceal NET evidence was identified in the retrieved documents. (mohamed2022managementofappendix pages 1-2)
15. Model organisms
No appendiceal-NET-specific animal models, organoids, or cell lines were identified in the retrieved evidence set; any discussion of model systems would require additional targeted searches outside the current corpus. (mohamed2022managementofappendix pages 1-2)
Recent developments (2023–2025 highlights)
- Incidence escalation in the US: SEER-based analysis documents a strong rise in aNET incidence (0.03→0.90 per 100,000 person-years, 2000–2017), likely reflecting stage migration and detection. (Nov 2023; https://doi.org/10.1371/journal.pone.0294153) (wang2023incidencetrendsand pages 13-14)
- Surgical de-escalation evidence for 1–2 cm tumors: large pooled cohort demonstrates no survival benefit to hemicolectomy and no metachronous metastases after complete resection. (Feb 2023; https://doi.org/10.1016/S1470-2045(22)00750-1) (nesti2023hemicolectomyversusappendectomy pages 5-12)
- Reassessment of completion surgery criteria: single-center cohort quantifies potential overtreatment when applying guideline criteria broadly; tumor size >2 cm emerges as the dominant predictor of nodal disease. (Jan 2025; https://doi.org/10.1007/s00423-024-03603-6) (wachter2025retrospectiveanalysisof pages 1-2)
- Metastasis rarity and questionable value of surveillance: institutional series suggests stage IV disease is exceptionally rare and usually synchronous; surveillance benefit after resection of small tumors appears minimal. (Jan 2025; https://doi.org/10.6004/jnccn.2024.7069) (altoubah2025doappendicealneuroendocrine pages 1-2)
Clinical trials and real-world studies (selected; clinicaltrials.gov)
- NCT05919758 (Recruiting): “Value of Right-sided Hemicolectomy for Children With High-risk Neuroendocrine Tumors of the Appendix” (observational; large target enrollment). (clinicaltrials.gov record retrieved in this run) (NCT05919758 chunk 1)
- NCT02730104 (Completed): “Community-based Neuroendocrine Tumor (NET) Research Study” (observational). (NCT02730104 chunk 1)
Notes on evidence limitations for knowledge-base population
- Ontology identifiers (MONDO/Orphanet/MeSH/ICD) were not recoverable from retrieved texts; additional targeted retrieval (e.g., MeSH browser, MONDO, Orphanet, ICD-11 MMS) is required.
- Appendiceal-NET-specific genomics and model organism resources were not present in the current evidence set; these should be populated via targeted molecular studies (e.g., sequencing cohorts) and model-system literature.
Key “direct abstract” quotes captured in this evidence set
- On management controversy and size thresholds (review): “Simple appendectomy is curative for appendiceal NETs (G1–G2) < 1 cm… whereas RHC… is recommended in tumors ≥ 2 cm…” (May 2023) (andrini2023anupdateon pages 1-3)
- On incidence and stage migration (registry study): “the annual incidence of appendiceal neuroendocrine tumors (aNETs) increased significantly, from 0.03 to 0.90 per 100,000 person-years…” (Nov 2023) (wang2023incidencetrendsand pages 13-14)
- On pooled cohort outcomes (study summary evidence): “All metastases were diagnosed synchronously with no tumour-related deaths during the follow-up.” (Feb 2023) (nesti2023hemicolectomyversusappendectomy pages 5-12)
References
-
(andrini2023anupdateon pages 1-3): Elisa Andrini, Giuseppe Lamberti, Laura Alberici, Claudio Ricci, and Davide Campana. An update on appendiceal neuroendocrine tumors. Current Treatment Options in Oncology, 24:742-756, May 2023. URL: https://doi.org/10.1007/s11864-023-01093-0, doi:10.1007/s11864-023-01093-0. This article has 26 citations and is from a peer-reviewed journal.
-
(mohamed2022managementofappendix pages 1-2): Amr Mohamed, Sulin Wu, Mohamed Hamid, Amit Mahipal, Sakti Cjakrabarti, David Bajor, J. Eva Selfridge, and Sylvia L. Asa. Management of appendix neuroendocrine neoplasms: insights on the current guidelines. Cancers, 15:295, Dec 2022. URL: https://doi.org/10.3390/cancers15010295, doi:10.3390/cancers15010295. This article has 55 citations.
-
(nesti2023hemicolectomyversusappendectomy pages 5-12): Cédric Nesti, Konstantin Bräutigam, Marta Benavent, Laura Bernal, Hessa Boharoon, Johan Botling, Antonin Bouroumeau, Iva Brcic, Maximilian Brunner, Guillaume Cadiot, Maria Camara, Emanuel Christ, Thomas Clerici, Ashley K Clift, Hamish Clouston, Lorenzo Cobianchi, Jarosław B Ćwikła, Kosmas Daskalakis, Andrea Frilling, Rocio Garcia-Carbonero, Simona Grozinsky-Glasberg, Jorge Hernando, Valérie Hervieu, Johannes Hofland, Pernille Holmager, Frediano Inzani, Henning Jann, Paula Jimenez-Fonseca, Enes Kaçmaz, Daniel Kaemmerer, Gregory Kaltsas, Branislav Klimacek, Ulrich Knigge, Agnieszka Kolasińska-Ćwikła, Walter Kolb, Beata Kos-Kudła, Catarina Alisa Kunze, Stefania Landolfi, Stefano La Rosa, Carlos López López, Kerstin Lorenz, Maurice Matter, Peter Mazal, Claudia Mestre-Alagarda, Patricia Morales del Burgo, Els J M Nieveen van Dijkum, Kira Oleinikov, Lorenzo A Orci, Francesco Panzuto, Marianne Pavel, Marine Perrier, Henrik Mikael Reims, Guido Rindi, Anja Rinke, Maria Rinzivillo, Xavier Sagaert, Ilker Satiroglu, Andreas Selberherr, Alexander R Siebenhüner, Margot E T Tesselaar, Michael J Thalhammer, Espen Thiis-Evensen, Christos Toumpanakis, Timon Vandamme, José G van den Berg, Alessandro Vanoli, Marie-Louise F van Velthuysen, Chris Verslype, Stephan A Vorburger, Alessandro Lugli, John Ramage, Marcel Zwahlen, Aurel Perren, and Reto M Kaderli. Hemicolectomy versus appendectomy for patients with appendiceal neuroendocrine tumours 1–2 cm in size: a retrospective, europe-wide, pooled cohort study. The Lancet Oncology, 24:187-194, Feb 2023. URL: https://doi.org/10.1016/s1470-2045(22)00750-1, doi:10.1016/s1470-2045(22)00750-1. This article has 90 citations and is from a highest quality peer-reviewed journal.
-
(mohamed2022managementofappendix pages 2-4): Amr Mohamed, Sulin Wu, Mohamed Hamid, Amit Mahipal, Sakti Cjakrabarti, David Bajor, J. Eva Selfridge, and Sylvia L. Asa. Management of appendix neuroendocrine neoplasms: insights on the current guidelines. Cancers, 15:295, Dec 2022. URL: https://doi.org/10.3390/cancers15010295, doi:10.3390/cancers15010295. This article has 55 citations.
-
(wang2023incidencetrendsand pages 13-14): Dan Wang, Heming Ge, Yebin Lu, and Xuejun Gong. Incidence trends and survival analysis of appendiceal tumors in the united states: primarily changes in appendiceal neuroendocrine tumors. PLOS ONE, 18:e0294153, Nov 2023. URL: https://doi.org/10.1371/journal.pone.0294153, doi:10.1371/journal.pone.0294153. This article has 31 citations and is from a peer-reviewed journal.
-
(mohamed2022managementofappendix pages 4-5): Amr Mohamed, Sulin Wu, Mohamed Hamid, Amit Mahipal, Sakti Cjakrabarti, David Bajor, J. Eva Selfridge, and Sylvia L. Asa. Management of appendix neuroendocrine neoplasms: insights on the current guidelines. Cancers, 15:295, Dec 2022. URL: https://doi.org/10.3390/cancers15010295, doi:10.3390/cancers15010295. This article has 55 citations.
-
(andrini2023anupdateon pages 7-9): Elisa Andrini, Giuseppe Lamberti, Laura Alberici, Claudio Ricci, and Davide Campana. An update on appendiceal neuroendocrine tumors. Current Treatment Options in Oncology, 24:742-756, May 2023. URL: https://doi.org/10.1007/s11864-023-01093-0, doi:10.1007/s11864-023-01093-0. This article has 26 citations and is from a peer-reviewed journal.
-
(nesti2023hemicolectomyversusappendectomy pages 16-21): Cédric Nesti, Konstantin Bräutigam, Marta Benavent, Laura Bernal, Hessa Boharoon, Johan Botling, Antonin Bouroumeau, Iva Brcic, Maximilian Brunner, Guillaume Cadiot, Maria Camara, Emanuel Christ, Thomas Clerici, Ashley K Clift, Hamish Clouston, Lorenzo Cobianchi, Jarosław B Ćwikła, Kosmas Daskalakis, Andrea Frilling, Rocio Garcia-Carbonero, Simona Grozinsky-Glasberg, Jorge Hernando, Valérie Hervieu, Johannes Hofland, Pernille Holmager, Frediano Inzani, Henning Jann, Paula Jimenez-Fonseca, Enes Kaçmaz, Daniel Kaemmerer, Gregory Kaltsas, Branislav Klimacek, Ulrich Knigge, Agnieszka Kolasińska-Ćwikła, Walter Kolb, Beata Kos-Kudła, Catarina Alisa Kunze, Stefania Landolfi, Stefano La Rosa, Carlos López López, Kerstin Lorenz, Maurice Matter, Peter Mazal, Claudia Mestre-Alagarda, Patricia Morales del Burgo, Els J M Nieveen van Dijkum, Kira Oleinikov, Lorenzo A Orci, Francesco Panzuto, Marianne Pavel, Marine Perrier, Henrik Mikael Reims, Guido Rindi, Anja Rinke, Maria Rinzivillo, Xavier Sagaert, Ilker Satiroglu, Andreas Selberherr, Alexander R Siebenhüner, Margot E T Tesselaar, Michael J Thalhammer, Espen Thiis-Evensen, Christos Toumpanakis, Timon Vandamme, José G van den Berg, Alessandro Vanoli, Marie-Louise F van Velthuysen, Chris Verslype, Stephan A Vorburger, Alessandro Lugli, John Ramage, Marcel Zwahlen, Aurel Perren, and Reto M Kaderli. Hemicolectomy versus appendectomy for patients with appendiceal neuroendocrine tumours 1–2 cm in size: a retrospective, europe-wide, pooled cohort study. The Lancet Oncology, 24:187-194, Feb 2023. URL: https://doi.org/10.1016/s1470-2045(22)00750-1, doi:10.1016/s1470-2045(22)00750-1. This article has 90 citations and is from a highest quality peer-reviewed journal.
-
(nesti2023hemicolectomyversusappendectomy pages 30-36): Cédric Nesti, Konstantin Bräutigam, Marta Benavent, Laura Bernal, Hessa Boharoon, Johan Botling, Antonin Bouroumeau, Iva Brcic, Maximilian Brunner, Guillaume Cadiot, Maria Camara, Emanuel Christ, Thomas Clerici, Ashley K Clift, Hamish Clouston, Lorenzo Cobianchi, Jarosław B Ćwikła, Kosmas Daskalakis, Andrea Frilling, Rocio Garcia-Carbonero, Simona Grozinsky-Glasberg, Jorge Hernando, Valérie Hervieu, Johannes Hofland, Pernille Holmager, Frediano Inzani, Henning Jann, Paula Jimenez-Fonseca, Enes Kaçmaz, Daniel Kaemmerer, Gregory Kaltsas, Branislav Klimacek, Ulrich Knigge, Agnieszka Kolasińska-Ćwikła, Walter Kolb, Beata Kos-Kudła, Catarina Alisa Kunze, Stefania Landolfi, Stefano La Rosa, Carlos López López, Kerstin Lorenz, Maurice Matter, Peter Mazal, Claudia Mestre-Alagarda, Patricia Morales del Burgo, Els J M Nieveen van Dijkum, Kira Oleinikov, Lorenzo A Orci, Francesco Panzuto, Marianne Pavel, Marine Perrier, Henrik Mikael Reims, Guido Rindi, Anja Rinke, Maria Rinzivillo, Xavier Sagaert, Ilker Satiroglu, Andreas Selberherr, Alexander R Siebenhüner, Margot E T Tesselaar, Michael J Thalhammer, Espen Thiis-Evensen, Christos Toumpanakis, Timon Vandamme, José G van den Berg, Alessandro Vanoli, Marie-Louise F van Velthuysen, Chris Verslype, Stephan A Vorburger, Alessandro Lugli, John Ramage, Marcel Zwahlen, Aurel Perren, and Reto M Kaderli. Hemicolectomy versus appendectomy for patients with appendiceal neuroendocrine tumours 1–2 cm in size: a retrospective, europe-wide, pooled cohort study. The Lancet Oncology, 24:187-194, Feb 2023. URL: https://doi.org/10.1016/s1470-2045(22)00750-1, doi:10.1016/s1470-2045(22)00750-1. This article has 90 citations and is from a highest quality peer-reviewed journal.
-
(altoubah2025doappendicealneuroendocrine pages 1-2): Taymeyah Al-Toubah, Mintallah Haider, Eleonora Pelle, Maria Grazia Maratta, and Jonathan Strosberg. Do appendiceal neuroendocrine tumors metastasize post appendectomy or right hemicolectomy? Jan 2025. URL: https://doi.org/10.6004/jnccn.2024.7069, doi:10.6004/jnccn.2024.7069. This article has 5 citations and is from a domain leading peer-reviewed journal.
-
(altoubah2025doappendicealneuroendocrine pages 2-3): Taymeyah Al-Toubah, Mintallah Haider, Eleonora Pelle, Maria Grazia Maratta, and Jonathan Strosberg. Do appendiceal neuroendocrine tumors metastasize post appendectomy or right hemicolectomy? Jan 2025. URL: https://doi.org/10.6004/jnccn.2024.7069, doi:10.6004/jnccn.2024.7069. This article has 5 citations and is from a domain leading peer-reviewed journal.
-
(altoubah2025doappendicealneuroendocrine pages 3-4): Taymeyah Al-Toubah, Mintallah Haider, Eleonora Pelle, Maria Grazia Maratta, and Jonathan Strosberg. Do appendiceal neuroendocrine tumors metastasize post appendectomy or right hemicolectomy? Jan 2025. URL: https://doi.org/10.6004/jnccn.2024.7069, doi:10.6004/jnccn.2024.7069. This article has 5 citations and is from a domain leading peer-reviewed journal.
-
(wachter2025retrospectiveanalysisof pages 1-2): Sabine Wächter, Dimitrios Panidis, Moritz Jesinghaus, Anja Rinke, Monika Heinzel-Gutenbrunner, Elisabeth Maurer, and Detlef K. Bartsch. Retrospective analysis of criteria for oncological completion surgery of neuroendocrine tumors of the appendix. Langenbeck's Archives of Surgery, Jan 2025. URL: https://doi.org/10.1007/s00423-024-03603-6, doi:10.1007/s00423-024-03603-6. This article has 1 citations.
-
(wachter2025retrospectiveanalysisof pages 2-4): Sabine Wächter, Dimitrios Panidis, Moritz Jesinghaus, Anja Rinke, Monika Heinzel-Gutenbrunner, Elisabeth Maurer, and Detlef K. Bartsch. Retrospective analysis of criteria for oncological completion surgery of neuroendocrine tumors of the appendix. Langenbeck's Archives of Surgery, Jan 2025. URL: https://doi.org/10.1007/s00423-024-03603-6, doi:10.1007/s00423-024-03603-6. This article has 1 citations.
-
(vasile2025neuroendocrinetumorsof pages 3-4): Liviu Vasile, Laurenţiu Augustus Barbu, Gabriel Florin Răzvan Mogoş, Valeriu Şurlin, Ionică Daniel Vîlcea, Liliana Cercelaru, Stelian Ştefăniţă Mogoantă, Nicolae-Dragoş Mărgăritescu, and Victor Nimigean. Neuroendocrine tumors of the appendix: a comprehensive review of the literature and case presentation. Romanian Journal of Morphology and Embryology, 66:269-278, Aug 2025. URL: https://doi.org/10.47162/rjme.66.2.01, doi:10.47162/rjme.66.2.01. This article has 4 citations and is from a peer-reviewed journal.
-
(kim2025appendicealneuroendocrinetumor pages 4-6): YESEUL KIM, YOU-NA SUNG, ANNA THERESE DATUIN, INHO JANG, and JONGMIN SIM. Appendiceal neuroendocrine tumor: clinicopathologic characteristics of six cases and review of the literature. In Vivo, 39:559-565, Dec 2025. URL: https://doi.org/10.21873/invivo.13860, doi:10.21873/invivo.13860. This article has 4 citations and is from a peer-reviewed journal.
-
(mohamed2022managementofappendix media 6bf50e49): Amr Mohamed, Sulin Wu, Mohamed Hamid, Amit Mahipal, Sakti Cjakrabarti, David Bajor, J. Eva Selfridge, and Sylvia L. Asa. Management of appendix neuroendocrine neoplasms: insights on the current guidelines. Cancers, 15:295, Dec 2022. URL: https://doi.org/10.3390/cancers15010295, doi:10.3390/cancers15010295. This article has 55 citations.
-
(mohamed2022managementofappendix media 58ffb4ea): Amr Mohamed, Sulin Wu, Mohamed Hamid, Amit Mahipal, Sakti Cjakrabarti, David Bajor, J. Eva Selfridge, and Sylvia L. Asa. Management of appendix neuroendocrine neoplasms: insights on the current guidelines. Cancers, 15:295, Dec 2022. URL: https://doi.org/10.3390/cancers15010295, doi:10.3390/cancers15010295. This article has 55 citations.
-
(mohamed2022managementofappendix media 5c304756): Amr Mohamed, Sulin Wu, Mohamed Hamid, Amit Mahipal, Sakti Cjakrabarti, David Bajor, J. Eva Selfridge, and Sylvia L. Asa. Management of appendix neuroendocrine neoplasms: insights on the current guidelines. Cancers, 15:295, Dec 2022. URL: https://doi.org/10.3390/cancers15010295, doi:10.3390/cancers15010295. This article has 55 citations.
-
(mohamed2022managementofappendix pages 14-16): Amr Mohamed, Sulin Wu, Mohamed Hamid, Amit Mahipal, Sakti Cjakrabarti, David Bajor, J. Eva Selfridge, and Sylvia L. Asa. Management of appendix neuroendocrine neoplasms: insights on the current guidelines. Cancers, 15:295, Dec 2022. URL: https://doi.org/10.3390/cancers15010295, doi:10.3390/cancers15010295. This article has 55 citations.